
Abstract
While concepts such as ‘partnership’ are central to the terminology of private–public mix (PPM), little attention has been paid to how social relations are negotiated among the diverse actors responsible for implementing these inter-sectoral arrangements. India's Revised National Tuberculosis Control Programme (RNTCP) has used intermediary agents to facilitate the involvement of private providers in the expansion of Directly Observed Therapy, Short-Course (DOTS). We examine the roles of tuberculosis health visitors (TB HVs) in mediating working relationships among private providers, programme staff and patients that underpin a PPM-DOTS launched by the RNTCP in western Maharashtra. In addition to observations and informal interactions with the programme and participating health providers, researchers conducted in-depth interviews with senior programme officers and eight TB HVs. Framed by a political discourse of clinical governance, working relationships within the PPM are structured by the pluralistic context, social and professional hierarchies and paternalism of health care in India. TB HVs are at the nexus of these relationships, yet remain undervalued partly because accountability is measured through technical rather than social outcomes of the ‘partnership’. Close attention to the dynamics of power relations in working practices within the health system can improve accountability and sustainability of partnerships.
Introduction
The WHO-recommended DOTS (Directly Observed Treatment, Short-Course) strategy for tuberculosis (TB) control was launched and expanded in the mid-to-late 1990s through the Revised National TB Control Programme (RNTCP) in India (RNTCP, Citation2001). However, growing evidence confirmed that more than half of India's TB patients were likely to seek treatment from a private practitioner (PP) (Kelkar-Khambete et al., Citation2008; Uplekar, Pathania, & Raviglione, Citation2001) and to be treated with non-standardised drug regimens (Udwadia, Pinto, & Uplekar, Citation2010). In response, the RNTCP's second phase policy document explicitly called for engagement with non-governmental organisations (NGOs) and PPs. Consequently, within the wider transition towards models of public–private partnerships (PPP) in the health sector (Uplekar, Citation2003), the late 1990s and first half of the new decade saw numerous attempts to involve PPs in the RNTCP (Ambe et al., Citation2005; Arora, Sarin, & Lonnroth, Citation2003). Under the public–private mix for DOTS (PPM-DOTS) initiative, PPs were encouraged to engage with the RNTCP in a variety of ways – from referring patients to the public sector for diagnosis to being trained to work as Directly Observed Treatment (DOT) providers for TB patients registered for treatment under the programme.
While the experiences of involving PPs in TB care in India were pioneering (Arora et al., Citation2003; Murthy, Frieden, Yazdani, & Hreshikesh, Citation2001), they rested on contested assumptions about the feasibility and sustainability of working relationships between the public and the private medical sectors (Dewan et al., Citation2006). The private medical sector in India is vast, pluralistic and idiosyncratic in practice. The colonial legacy of public health policy in India has meant that indigenous traditions have been neglected, resulting in marked hierarchies within the health system. The attempt to synchronise other medical traditions under AYUSHFootnote1 has had limited success, not least because it has not adequately addressed the asymmetrical power relations among different medical traditions (Bhardwaj, Citation2010).
High levels of mistrust and suspicion exist between the public and private sectors (De Costa, Johansson, & Diwan, Citation2008; Uplekar et al., Citation2001; Uplekar, Citation2003; Vyas, Small, & DeRiemer, Citation2003): public sector staff commonly perceives PPs as irrational, profit-oriented and non-compliant to TB management guidelines. In turn, private sector practitioners question the fundamental tenets of the DOTS strategy, for example, the effectiveness of intermittent treatment, the use of sputum examination for TB management and the practical implementation of the strategy (Harper, Citation2009; Vyas et al., Citation2003). Limited understanding of each other's functioning has meant that ‘partnerships’ generally amounted to one-sided arrangements whereby the public sector took on the lead role of recruiting, educating and monitoring PPs adherence to the RNTCP without adequate consideration of PPs' interests (Lonnroth et al., Citation2004). Not surprisingly, a review of the evidence suggested that the endeavour was time and resource intensive, with commitment from both sides flagging (Mahendradhata, Lambert, Boelaert, & Van der Stuyft, Citation2007). Formal suggestions to strengthen the participation of PPs included referral slips, tighter maintenance of records, as well as the introduction of intermediary agents to improve communication, build trust and facilitate more effective collaboration (Ambe et al., Citation2005; Lonnroth et al., Citation2004; Pradhan et al., Citation2011; Rangan et al., Citation2004).
Although initiatives like the PPM-DOTS have been in place for more than two decades, little empirical attention has been paid to the social relations among diverse actors tasked with implementing the often complex formal arrangements envisaged under such partnerships. In this paper, we describe the working roles and relationships that underpin PPM-DOTS in western India. Notably, we highlight the role of frontline health workers – the TB health visitors (TB HVs) – in mediating local terms of ‘partnership’ in a highly pluralistic and hierarchical health system.
The backdrop for this paper is PPM-DOTS in the RNTCP in Sundernagar (pseudonym), a highly industrialised township in the State of Maharashtra covering an area of 171 km2. It represents an unusual example of an initiative that was sustained for over a decade exclusively with resources from the programme (Pradhan et al., Citation2011). One of the reasons for its relative longevity was the programme's optimal use of human resources. Under the PPM-DOTS model initiated by the programme officer in Sundernagar, the local programme trained and enlisted PPs to refer their TB patients to the RNTCP for DOTS, or to serve as DOT providers themselves in an attempt to improve coverage of DOTS in areas with scant public health sector facilities. In the initial years, the PPM-DOTS was monitored by medical officers (MOs) and para-medical supervisors. Periodic assessment of the PPM-DOTS initiative showed encouraging results in terms of promoting earlier referrals of patients who sought treatment from PPs involved in the PPM-DOTS as opposed to those not involved in the initiative. As the number of participating PPs increased, and referrals from the enlisted PPs became more erratic and less reliable, the need for additional capacity for monitoring was recognised (Pradhan et al., Citation2011). To this purpose, the City TB Officer (CTO) in Sundernagar decided to enlist TB HVs,Footnote2 contractual field staff normally responsible for outreach activities, to recruit PPs for the programme and monitor those who became affiliated with the programme.
The extended role for TB HVs and the relationships they develop with patients, PPs, programme staff and supervisors form the subject of our analysis in this paper: as active but hidden links in the PPM-DOTS, the TB HVs offer a unique lens for understanding how ‘partnerships’ are negotiated and sustained by actors in local health systems contexts. This emphasis on social relations, and more broadly, the socio-political contexts in which health systems are embedded, is core to an anthropological approach to medical systems (Baer, Singer, & Susser, Citation2003), but remains a fairly recent perspective in the global health systems literature (Atkinson, Citation2002; Bloom & Standing, Citation2008; Freedman, Citation2005; Gilson, Citation2003; Gilson et al., Citation2011). Empirical work on social relations in health systems has tended to focus narrowly on patient–provider relations, and remains relatively unexplored in low- and middle-income settings (Ozawa & Sripad, Citation2013; Rowe & Calnan, Citation2006). We aim to contribute to addressing these gaps by embedding our analysis of TB HVs' working relationships and their understandings of accountability both within the clinical governance structures of the RNTCP as well as the broader organisational culture of the Indian health system within which it operates.
Methodology
Context of study
The CTO of Sundernagar approached an academic NGO based in Pune to collaborate on an operations research study exploring the factors that motivated PPs' involvement in the PPM-DOTS and to test the feasibility of different interventions to strengthen the PPM. Two of the authors (Vinita Datye and Anagha Pradhan) were employees of the NGO at the time and had lead roles in conducting the research and interventions in this project. In addition to the formal data collection conducted as part of the research, Datye and Pradhan were in regular and close contact with the Sundernagar programme staff over the course of two years. The frequent opportunities to observe interactions with various stakeholders in the intervention enhanced researchers' understanding of how the PPM-DOTS was implemented on the ground.
Data collection
Together with three research assistants, Datye and Pradhan were involved in a series of studies that examined the perspectives of different actors within the PPM-DOTS. Prior to the operations research study, a census conducted by the programme listed 767 PPs in Sundernagar, including PPs practicing Western biomedicine (allopathy) as well as three of the alternative medical traditions that make up the Indian health system (Ayurveda, Homeopathy and Unani). A survey conducted with 497 of these PPsFootnote3 examined PPs' referral practices as well as enablers and barriers to their participation in the PPM-DOTS. This sample included 164 PP-DOT providers in the programme catchment area. Less than one-fifth of the PPs were practising allopaths (14%) while more than half were ayurvedic practitioners (57%). Findings indicated that although a majority (87%) of the PPs referred to the RNTCP, only a quarter of these received feedback regarding the diagnosis of the patients. The PPs suggested that better communication and feedback from the programme would be important for sustaining the initiative. In order to obtain a more in-depth understanding of referrals, communication and working relations of the PPM-DOTS in Sundernagar, semi-structured interviews were conducted with patients and with PPs to document the experiences of providing and receiving DOT at a PP-DOT centre. Datye and Pradhan also conducted in-depth interviews with three acting programme officers – the CTO and the two MOs – as well as with the former CTO who had initiated the PPM-DOTS in Sundernagar.
In reviewing these sources of data, the TB HVs emerged as crucial intermediaries in the facilitation of PPM-DOTS. Consequently, the researchers conducted in-depth interviews with eight of the 11 TB HVs working with the programme at the timeFootnote4 about their role in the expansion of the PPM-DOTS, field challenges and suggestions to overcome these challenges. Interviews were conducted in pairs, after obtaining written consent from interviewees. All interviews were conducted in Marathi or English with the help of semi-structured interview guides. This paper draws primarily on the interviews conducted with TB HVs, but also makes reference to two of the interviews with programme officers and interviews with PPs.
Data analysis
The in-depth interviews with TB HVs and programme officers were tape recorded, transcribed and translated where necessary. They were read through several times by the authors. As a first step, the interviews were manually coded around important themes explored during the interviews (role in the expansion of the PPM-DOTS, field challenges and suggestions to overcome these challenges). Further codes, for example, around the scope, nature and consequences of particular roles for working relationships, were inductively derived and discussed among the researchers to refine a preliminary code list. The interview data were managed using the qualitative data management package – Atlas Ti (AtlasTi 4.2, 1997–2003 The Scientific Software Development Berlin). Frequencies of the coded data excerpts helped to further revise the code list, for example, by combining some codes that were too narrow, and breaking down others that were too broad. Three of the four authors including Datye and Pradhan were involved in developing codes and the process of coding. The coded data were entered into matrices relating to the four domains of relationships set out by the framework () in order to examine trends as well as tensions in the ways these relationships were articulated and experienced.
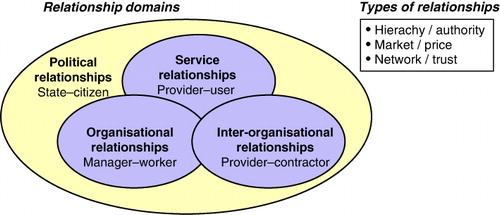
Note: Original diagram from Newman (Citation1998).
Conceptual framework
Although their formal visibility is low, the TB HVs are not just part of the ‘organisational machinery’ of the RNTCP but rather ‘reflective, responsive human beings embedded in networks of social relations’ (Blaauw, Gilson, Penn-Kekana, & Schneider, Citation2003, p. 23). An important strand of recent work on social relations in health systems has centred on the notion of trust as a crucial element underpinning collaboration among health systems actors to achieve health outcomes. While the literature emphasises both inter-personal as well as institutional relations of trust (Gilson, Citation2003; Rowe & Calnan, Citation2006), most empirical work has focused on patient–provider relationships without adequate consideration of the broader context of workforce relationships within which these take place. A recent review of health systems trust measures confirms that most focus on relationships among doctors, nurses and patients rather than examining organisational interactions at the health system and societal level (Ozawa & Sripad, Citation2013). In order to map the web of social relations that sustain the Sundernagar PPM-DOTS, we drew on Newman's categorisation of public sector relationships in the health system (Newman, Citation1998; ). These include: service relationships, i.e. frontline interactions between health care workers and patients; organisational relationships, i.e. interactions between managers and workers, between colleagues or between different categories of health workers; inter-organisational relationships, i.e. relationships with external organisations such as suppliers, PPs and NGOs; and finally political relationships, referring to the broader context of relationships between governments and citizens. The framework highlights the interconnectedness of domains, and specifically of the crucial role of social relationships within the health system.
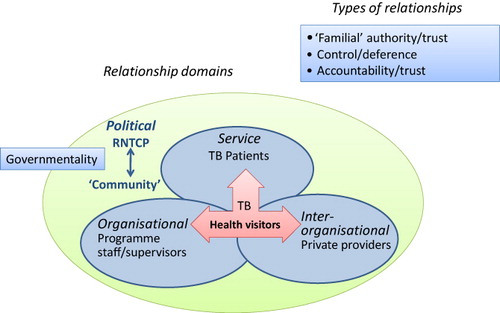
We suggest that the Sundernagar PPM-DOTS represents a micro-system that embodies the full range of these domains. In their interactions with patients, PPs, programme staff and supervisors, TB HVs are at the intersection of the service, organisational and inter-organisational relationships as described by Newman. The working relationships that TB HVs form and sustain as part of their extended role in the PPM-DOTS involve complex negotiations of social and professional hierarchy, regulatory frameworks and personalised moral imperatives in TB care. While these relationships are framed by an overarching political discourse about the accountability of the RNTCP to patient-citizens, they are also undoubtedly shaped by the organisational culture of the Indian health system, which in turn reflects wider normative societal values (Gilson, Citation2003). In line with these considerations, we adapted Newman's framework to structure our analysis in this paper ().
Note: Adapted from Newman (Citation1998).
Results
Profile of TB HVs
The eight TB HVs varied widely in their qualifications and years of experience (). Most of the TB HVs had received practical training related to their tasks ranging from patient counselling to administrative duties such as monitoring of treatment cards and boxes kept at the private clinics. This training was provided both formally as well as informally through observations, field visits with TB supervisors and other TB HVs.
Table 1. Profile of TB HVs.
Service relationships: TB HVs and patients
Our RNTCP is the only programme where we care for patients. We go after the patients. None of the other programmes are like this […]Apart from the TB control society, nobody goes to people's houses to give tablets, nobody goes to patients' homes to invite them – ‘ please come for treatment ’. [Ganesh, male TB HV with one and a half years of experience; for all quotes words spoken in English have been underlined, quotes within quotes are italicised]
Once we are [at the DOT centre] we have only this to do – see the cards, check the box, see if the card and the box match, is the patient due for follow-up? Is the patient on DOT? [i.e. regular in his medication-taking] If not then retrieve immediately. [Prashant, three years of experience]
If we go to a home, then the neighbours gather around immediately. Then we say that we are friends or relatives. That is how the patient also understands these people [TB HVs] have come from the hospital…or even if we go without [advance] notice, we do not identify ourselves [by saying] that we have come from the hospital. When we go inside the home, there are no outsiders. It is only then that we tell them that we have come from [name] hospital. [Shubha, five years of experience]
We told the patient: ‘If you don't take your medicines we will bring the police to your house!’ At that time we took [name of TB HV] there and pretended that he was a policeman. He said: ‘Why aren't you taking your tablets? Come to the police station.’ He put such pressure on the patient. After that he [patient] said: ‘Okay sir, I will take the tablets’. First we took him to the centre and gave him the tablets. Then we told him that [name of TB HV] was not a policeman: ‘We just pretended he was one for your own good’. [Rajesh, five years of experience]
Patients' deference to the authority of the TB HV is tempered with faith. Interventions with patients are often far-reaching and often described in moral terms. Krishna's story about Shankar, a Category I sputum positive patient, indicates the importance of building relationships across family ties and formal contacts with the health system:
When he [Shankar] found out that he had TB and told his wife, she informed her natal family and they immediately came to take her away. They said: ‘No, we won't let her stay here with you!’ He came to me and said: ‘Sir, it is like this. My wife is saying she wants to go back to her native place and now what do I do? If my wife goes away who will feed me? […]So please give me these medicines at my native place […]I said to him: ‘If you go to your native place, will you have the facility for these medicines, investigations? What if something happens? […]I will come to your house or you bring your family here, let us explain to them. Let's see if they listen’. He brought his family, his in-laws. I explained to them and clarified whatever doubts they had. But even after I had explained, they were not satisfied. Then the next day I asked them to come to the TU [TB Unit]. They came, we spoke with madam [referring to Medical Officer in charge] […]When their doubts were clarified [Shankar's] wife stayed and he was completely cured. [Krishna, five years of experience]
The patient [who has to be re-treated] is nervous at that point. [He says] ‘I did not get cured after taking so many tablets, I am going to die now’ …, that is generally the patient's attitude at this point. […]we counsel the patient. […]He is only 50% convinced. But he believes us, trusts us. He has six months experience[…]‘Let's do the [sputum] culture’. We tell him. ‘It did not get cured but now you [also] have an injection [Streptomycin]. That might give relief’. After two, three weeks his weight increases, appetite increases and because of that he is convinced and then his self-confidence increases. He says: ‘I will be cured’ and he gets cured. [Prashant, three years of experience]
I repeatedly reassured him, he took his medicines diligently and I cured him. On the day his final x-ray was taken – madam [Medical Officer] took a look at the x ray and told him ‘you are cured’ … the elderly man fell at my feet. I was overwhelmed … in this life I may or may not do anything else but I earned this satisfaction … I got the satisfaction that I saved a life.
Inter-organisational relationships: TB HVs and PPs
In addition to outreach work with patients, TB HVs in Sundernagar interact with PPs on a regular basis. However, these interactions are inherently unequal, and TB HVs struggle to gain respect as credible programme authorities. Whereas the TB HVs’ relationship with patients is based in paternalism, allowing them to undertake actions ‘for the patient's good’, their relationship with PPs is ambivalent, as they are put in the awkward position of exercising control over individuals they would normally be subservient towards.
Establishing rapport involves lengthy negotiation of hierarchy, knowledge and status. TB HVs have to overcome tainted attitudes towards the public sector. Tales of gaining respect from PPs describe rituals of submission: being forced to wait long hours outside PPs' clinics, told to come back numerous times, and occasionally having to endure disrespect from ‘foul mouths’. Initial attempts to recruit PPs are also not always welcome. Ganesh recalls:
One doctor hassled me so much, right until the end […] There would be one or two patients in that sir's clinic in one to two hours. [But] still he would dilly-dally. When I went in the evening, he would say: ‘Don't come at this time, it is time to light the lamps.Footnote6 Come in the morning’. If I went in the morning, he would say: ‘Now, see here you are again…’ just like that [dismissively]…One would get a feeling of being even below the level of a ward boy.
Krishna suggests that it is not only disagreement on treatment but professional complicity that limits the involvement of allopathic PPs:
They hesitate … to get involved because they are either attached to some physician or they have relations [a relationship] with some hospital. If they come across a patient with Koch's [TB], generally what they do is, they send him to a physician. Initially they get his x-ray, all investigations done from outside [private] and then later if the patient cannot afford, only then they refer to our [public] health system.
TB HVs struggle to establish a distinct professional identity for themselves. For some PPs, TB HVs' affiliation with the programme provides them with legitimate credentials, as expressed by Vivek: ‘In some places we tell the receptionists or sisters [nurses]: “I am from RNTCP. This is my card. I want to speak to sir in this context.”’ Yet in interviews with PPs participating in the programme, confusion as to the underlying occupational motive of the TB HVs was manifest: TB HVs were variously referred to as ‘TB person’, ‘social worker’, ‘multi-purpose worker’, ‘nurse’, ‘doctor’ and even ‘WHO consultant’. Other PPs perceived the TB HV as a ‘public sector employee who is doing his job and who keeps coming back’ (Prashant). While mistakenly identified as such, TB HVs do not share the benefits of public sector employees. Krishna notes that although public sector DOT providers are meant to look after patients ‘properly’, they rarely go to the ‘field’ to follow up patients on DOT:
They are permanent [employees of the municipal corporation] no one can do anything to them […]Here, the municipal corporation is a local self-government…everyone's father or brother is a local politician.Footnote10 If the [senior programme] officer says anything, there would be a phone call from the top [inquiring]: “why did you scold him?”
Some doctors never did the markings, we used to do them. Next week when we visited, we would do that, so that there was nothing pending. We regularly remind them but still there isn't as much change as should have been.
Despite the inherent imbalance in the relationship between TB HVs and PPs, Prashant suggests that sustained interaction with PPs promotes a more positive attitude towards the public sector among PPs:
When they get involved in the programme, when we interact with them, and they come for a meeting, they see our work, our record keeping etc. Then they are astonished […] They say: ‘I never thought that your programme would be like this or that there would be so much transparency. But now I see that it is so.’ After that they change.
Organisational relationships: TB HV and supervisory structures
The programme is accountable for the outcome of every patient treated. This is done using standard recording and reporting system, and the technique of ‘cohort analysis’. The cure rate and other key indicators are monitored at every level of the health system, and if any area is not meeting expectations, supervision is intensified. The RNTCP shifts the responsibility for cure from the patient to the health system. [Central TB Division, Directorate General of Health Services, Citation2010]
Supervision of TB HVs is rigorous as they represent the ‘face of the programme’ (current CTO) and are in daily contact with patients, with PPs and with the public sector DOT centres. Reporting systems are complex, involving interactions with multiple levels of supervisors. Work in the field is monitored through a field log of visits to PPs and patients and duplicate cards maintained for patients receiving DOT from DOT provider PPs. These records are reviewed by the MO TUs in the presence of the senior treatment supervisors (STS) in daily meetings where:
the routine work that we do…is presented […] all that we did yesterday and how we did it, the problems we had yesterday, how many interrupted patients there were or what other problems there were – we bring all this to their notice’. (Krishna)
Instead of talking to us they [STSs] talk directly to the MO TU. They should talk to us first. For example, there was a patient problem. We had paid a home visit…the patient's relatives were out for work during the day. When he [STS] went there he met the relatives. The relatives say that no one had come to the house to speak to them. So he [STS] directly informed the MO TU or CTO [without speaking to us]. [Rajesh, five years of experience]
While TB HVs' ability to convince patients to get back on treatment, or to persuade PPs to work with the programme are based in their familiarity with patients and PPs, too much familiarity is considered undesirable by senior officers, possibly compromising monitoring relationships. In addition to supervisory visits and disciplinary memos, a more serious measure to keep TB HVs in check is to reshuffle administrative areas handled by each TB HV. Intended to avoid complacency resulting from working in a particular area over an extended period of time, the transfer of staff causes upheaval in the work routines of TB HVs and the relationships they have built up with patients and PPs. Rajesh bitterly comments:
There was no need for the transfers and it feels like it was made to trouble someone. It results in […] tension, mental stress. […]They say the detection rate, cure rate was good. Then what was the reason for the transfers?
It is a one-way system with health workers. It is not that all improvements should be through the health workers…the officers are at fault as well. But they are officers. We cannot tell them directly to their faces. And they also are not ready [to take the criticism]. […]Because of this, whatever they say, we have to nod ‘yes’ in front of them … It should not be like this. We [also] have expectations from them.
Discussion
The health system is not simply a mechanical structure to deliver technical interventions the way a post office delivers a letter. Rather, health systems are core social institutions. They function at the interface between people and the structures of power that shape their broader society. [Freedman, Citation2005, p. 20]
As the research came to an end, the initiative had been in place for nearly 10 years, with TB HVs actively involved since three years. When asked about the role of TB HVs in the PPM, the senior programme officers had very different views. The former CTO said rather dismissively that TB HVs were ‘only like postmen, keeping the boxes and conveying the messages from the doctor, sending the report […] A TB HV is not a technical person so cannot make any impact on [treatment] outcomes as such’. In contrast, the current CTO enthusiastically described the TB HV as ‘the grass root workers in this partnership’, reminding us that ‘this partnership depends on the TB HVs working well with the doctors’.
While the former CTO focused on technical treatment outcomes as the ultimate aim of the PPM, the current CTO valued the implications of creating good social relationships – ‘working well with the doctors’ – for soldering the PPM-DOTS. These perceptions do not necessarily conflict. However, a focus on the former may obscure important mechanisms through which low-level, frontline health workers like TB HVs contribute to partnerships in the health system.
Our study focused on a small initiative undertaken by a local programme, one that appears to be a deviant case in terms of its sustainability. The experiences of the eight TB HV represented here are highly individual and subjective, and may not be generalisable for the universe of frontline health workers involved in TB control. However, we drew on the TB HVs accounts of their working lives and practices here not so much to comment on their viability as effective agents in the PPM-DOTS, but rather to highlight the critical importance of social and power relations in facilitating (or hindering) health systems' goals of partnership and integration.
Adapting Newman's (Citation1998) framework of public sector relationships in the health system, we suggest that the relationships described among the diverse actors engaged in the PPM-DOTS are structured not only by the programme's practices of clinical governance, but also by social hierarchies that permeate the broader context of medical pluralism in India. As in many other countries, the reality of pluralistic practice in India is not represented by distinct, independent health care traditions, but rather by more ‘porous’ boundaries where ‘many types of providers operate and markets for almost all medical goods and services have emerged in a largely unregulated way’ (Bloom & Standing, Citation2008, p. 2069). In this context, partnerships such as that represented by PPM-DOTS are not just institutional arrangements but rather, sets of interactions among a broad range of actors who have different sources of legitimacy, power and willingness to contribute towards a shared goal. Changes to systems of governance – as are subtly introduced through the intervention of TB HVs in the PPM-DOTS – ‘invariably affect the distribution of power between various actors, they determine the systems and structures through which accountability is supposed to operate, and they reflect different levels of trust’ (Rowe & Calnan Citation2006, p. 379).
Convinced that DOTS is an appropriate way of demonstrating ‘care’ for TB patients, TB HVs assume a sense of civic duty in protecting the ‘greater good’ as public health workers. At the same time, they actively intervene in patients' lives based on their familial proximity and derive satisfaction in knowing they have contributed towards the ‘cure’ of individual patients. This is experienced by health worker cadres positioned between programmes and individual medical practitioners across diverse settings. Justice's (Citation1983) seminal study on the role of the peon in Nepal's health system points to the paradox of the ‘invisible’ government clerk who assumes critical health care tasks for patients who cannot access the system. Brownlie and Howson (Citation2006) describe health visitors participating in immunisation programmes in the UK, who respond to ‘centralized information’ in conflicting ways, both ‘delivering the “normalizing judgments” essential to governmentality’ (p. 439) and establishing relationships with clients that enable the provision of valuable information. In the Indian setting, ‘conflicting accountabilities’ have been described for doctors struggling to balance the requirements of DOTS with the needs of patients and their relatives (Fochsen et al., Citation2009). In our study, TB HVs' relationships with patients are framed not only through RNTCP directives, but through a prevailing culture of paternalism that assumes patients – especially if less educated, younger or female – have limited awareness or agency in health-related decision-making (Datye et al., Citation2006; Fochsen, Deshpande, & Thorson, Citation2006; Kielmann et al., Citation2005).
In relationships with PPs, TB HVs oscillate between towing and breaking rank to fulfil both programme directives and practitioners' professional interests. Building working relations with PPs entail rites of passage that are shaped by the context of pluralistic practice, in which different medical traditions compete for patients and reputation (Khare, Citation1996; Kielmann et al., Citation2005; Nichter, Citation2002). The TB HVs are able to gain a certain complicity with PPs through shared knowledge of patients and liminal status as health providers. Both TB HVs and PPs experience patients' life circumstances at first hand, expressing the need to adapt DOTS to meet the needs of vulnerable patients (Khan, Walley, Witter, Shah, & Javeed, Citation2005). Ironically, in the public health literature, these views and practices represent ‘conflicting perceptions’ – barriers to PPM-DOTS and the target orientation of the RNTCP (De Costa et al., Citation2008; Vyas et al., Citation2003).
Yet the relationship between TB HVs and PPs is precarious, as the TB HVs have to show up PPs' ‘bending the rules’ for individual patients as well as their lapses in reporting duties. Relationships with supervisors are inherently tense as a result of the need to meet targets, which serve to ‘align managerial and clinical rationalities’ (Flynn, Citation2002, p. 164). In a quasi-Kafkaesque division of labour, programme supervisors monitor TB HVs, who monitor the PP-DOT providers, who monitor the patients. As described elsewhere (Brownlie & Howson, Citation2006; George, Citation2009; Harrison & Dowswell, Citation2002; Murphy, Citation2003), this mechanism of ‘bureaucratic compliance’ (George, Citation2009) appears to confer an important role for health workers in a hierarchical, multi-layered ‘field’ context but ‘restricts their capacity to exercise any real professional judgement in an expanded public health role’ (Brownlie & Howson, Citation2006, p. 441).
Successful integration of PPM-DOTS into the public health system has remained elusive (Mahendradhata et al., Citation2007), in part because efforts to implement ‘partnerships’ often fail to take account of working relations among significant actors on the ground (Birungi et al., Citation2001). Previous work on PPM-DOTS in India has noted the importance of communication and ‘interaction at the individual level’ to build trust between programme staff and PPs who are unequal ‘partners’ (Ambe et al., Citation2005). Trust is more generally seen as an effective and ethical way of ‘framing’ health systems relationships (Gilson Citation2003), yet trust is strongly shaped by cultural norms that govern the form and content of relationships across gender, age, occupation and other relevant social divisions. Professional and social identity are closely allied; health workers who are ‘respected for their skills and access to resources […] are expected to use these important relations of social reciprocity’ (Kyaddondo & Whyte, Citation2003, p. 330). However, the role of frontline health workers like TB HVs in soldering key health systems relationships remains undervalued (Justice, Citation1983; Manongi, Marchant, & Bygbyerg, Citation2006; Mathauer & Imhoff, Citation2006).
Conclusion
As multi-drug resistant TB emerges as a major threat in India, both community-based frontline health workers as well as the private sector have become the focus of renewed efforts to revive PPM-DOTS for management and control of TB. Our insights from Sundernagar suggest the need for public sector staff to increase efforts to build and sustain relationships with the private sector in order to enable viable ‘partnerships’ that can contribute to improving outcomes for TB patients. As hidden links in the PPM-DOTS chain, TB HVs need formal acknowledgement, supportive supervision and the opportunity to acquire new skills. If officially recognised and respected as ‘partners’, TB HVs might take on more active roles in identifying commonly recurring problems, initiating change processes and evaluating improvements in the programme (Béhague, Kanhonou, Filippi, Lègonou, & Ronsman, Citation2008; Dieleman, Gerretsen, & Jan van der Wilt, Citation2009).This is especially relevant given their proximity and close attention to the multiple layers and forms of accountability in the PPM-DOTS. As George (Citation2009) argues, the external accountability of public health programmes ‘cannot be realised in the absence of internal accountability between health administrators and workers’ (p. 209). In order for accountability mechanisms to effectively mediate relationships between the different and inherently unequal sets of actors involved in PPM, they need perhaps to change the ‘terms of engagement’ and ‘transform them in legitimising ways’ (George, Citation2003, p. 11).
While generic recommendations for improving accountability need to be translated into dynamic processes that closely follow the logic of local practices and actors (George, Citation2003), it is worth taking note of the limiting parameters of context specificity: ‘partnerships’ such as that represented by the Sundernagar PPM-DOTS are both enabled and constrained by the wider cultures of pluralism, social hierarchy and paternalism that pervade working relationships in the Indian health system. In this environment, TB HVs' daily adjustments of professional and personal ethic constitute balancing acts in the divide between public and private health goals.
Acknowledgements
Although unable to acknowledge their names for confidentiality reasons, we are very grateful to the former Municipal Commissioner, former Medical Director and both the former and current CTOs of Sundernagar for granting us permission to carry out the project, for their insights on PPM-DOTS and their support throughout the study. Many thanks to the eight TB HVs for sharing their views and working life experiences with us – it is their dedication to the PPM-DOTS that inspired us to write this paper. Ruth Fitzgerald and Anuj Kapilashrami provided pertinent comments on an earlier version of this paper. We also acknowledge the support of Professor R.K. Mutatkar, former President of MAAS, and our colleagues at MAAS-CHRD.
Funding
The study was funded through the Department for International Development, UK (TB Knowledge Programme and the Communicable Diseases RPC – TARGETS [grant number HD205] and the Municipal Corporation of the town we have called Sundernagar.
Additional information
Funding
Notes
1. The Department of Indian Systems of Medicine and Homeopathy (ISM&H) was created in March 1995 and re-named as the Department of Ayurveda, Yoga & Naturopathy, Unnani, Siddha and Homeopathy (AYUSH) in November 2003 with a view to providing focused attention to the development of Education & Research in Ayurveda, Yoga & Naturopathy, Unnani, Siddha and Homeopathy systems.
2. Under the RNTCP, one TB HV serves a population of 100,000.
3. General practitioners, general physicians or chest physicians were included in the study while a total of 92 specialists namely surgeons, dermatologists and dentists who rarely saw TB patients were excluded. Out of the 675 PPs found eligible for the survey, pre-test interviews were conducted with 46 PPs, 6 paediatricians were excluded as they did not see any adult patients, 41 PPs refused to participate, 16 PPs were unavailable, 45 PPs had closed their clinics since the census and 17 PPs could not be located. Out of the 504 PPs surveyed, seven interviews were discarded due to poor quality.
4. One TB HV refused the interview and two were excluded as they were newly recruited and lacked experience.
5. Module for multi-purpose workers and other DOT providers, June 2005.
6. Lamps are traditionally lit at dusk, considered an auspicious period for business and prosperity. Businessmen discourage those seeking alms at this time, since ‘giving’ at this hour symbolises giving away wealth from the establishment.
7. MBBS stands for ‘Bachelor of Medicine, Bachelor of Surgery’. In India, it is the first qualifying degree for a physician trained in biomedicine.
8. BHMS stands for Bachelor of Homeopathic Medicine and Surgery, BAMS refers to Bachelor of Ayurvedic Medicine and Surgery. Ayurveda is an indigenous tradition, while homeopathy is an ‘imported’ tradition, however, both are included within the five medical traditions contributing to the national health system.
9. Of the total PPs surveyed (n = 497), 88% were non-allopaths. The overwhelming majority of the PP-DOT providers (n = 150/164) were non-allopaths.
10. This is figuratively taken to imply the use of political clout to forgo accountability.
References
- Ambe, G., Lönnroth, K., Dholakia, Y., Copreaux, J., Zignol, M., Borremans, N., & Uplekar, M. (2005). Every provider counts: Effect of a comprehensive public–private mix approach for TB control in a large metropolitan area in India. International Journal of Tuberculosis and Lung Diseases, 9, 562–568. Retrieved from http://www.ingentaconnect.com/content/iuatld/ijtld/2005/00000009/00000005/art00017
- Arora, V. K., Sarin, R., & Lonnroth, K. (2003). Feasibility and effectiveness of a public–private mix project for improved TB control in Delhi, India. International Journal of Tuberculosis and Lung Diseases, 7, 1131–1138. Retrieved from http://www.ingentaconnect.com/content/iuatld/ijtld/2003/00000007/00000012/art00004
- Atkinson, S. (2002). Political cultures, health systems and health policy. Social Science & Medicine, 55(1), 113–124. doi:10.1016/S0277-9536(01)00213-1
- Baer, H. A., Singer, M., & Susser, I. (2003). Medical anthropology and the world system (2nd ed.). Westport, CT: Praeger Publishers.
- Béhague, D. P., Kanhonou, L. G., Filippi, V., Lègonou, S., & Ronsman, C. (2008). Pierre Bourdieu and transformative agency: A study of how patients in Benin negotiate blame and accountability in the context of severe obstetric events. Sociology of Health and Illness, 30, 489–510. doi:10.1111/j.1467-9566.2007.01070.x
- Bhardwaj, R. (2010). Medical pluralism in India—The interface of complementary and alternative therapies with allopathy. In A. Mishra (Ed.), Health illness and medicine: Ethnographic readings (pp. 30–60). New Delhi: Orient Blackswan.
- Birungi, H., Mugisha, F., Nsabagasani, X., Okuonzi, S., & Jeppsoon, A. (2001). The policy on private–public mix in the Ugandan health sector: Catching up with reality. Health Policy and Planning, 16(Suppl 2), 80–87. doi:10.1093/heapol/16.suppl_2.80
- Blaauw, D., Gilson, L., Penn-Kekana, L., & Schneider, H. (2003). Organisational relationships and the ‘software’ of health sector reform. Background Paper, Disease Control Priorities Project (DCPP) Capacity Strengthening and Management Reform. Johannesburg: Centre for Health Policy, University of the Witwatersrand School of Public Health. Retrieved from http://www.dcp2.org/file/38/wp23.pdf
- Bloom, G., & Standing, H. (2008). Future health systems: Why future? Why now? Social Science & Medicine, 66, 2067–2075. doi:10.1016/j.socscimed.2008.01.032
- Brownlie, J., & Howson, A. (2006).‘Between the demands of truth and government’: Health practitioners, trust and immunisation work. Social Science & Medicine, 62, 433–443. doi:10.1016/j.socscimed.2005.05.033
- Central TB Division, Directorate General of Health Services. (2010). About the RNTCP. Retrieved from http://www.tbcindia.org/RNTCP.asp
- Datye, V., Kielmann, K., Sheikh, K., Deshmukh, D., Deshpande, S., Porter, J., & Rangan, S. (2006). Private practitioners' communications with patients around HIV testing in Pune, India. Health Policy and Planning, 21, 343–352. doi:10.1093/heapol/czl021
- De Costa, A., Johansson, E., & Diwan, V. K. (2008). Barriers of mistrust: Public and private health sectors' perceptions of each other in Madhya Pradesh, India. Qualitative Health Research, 18, 756–766. doi:10.1177/1049732308318504
- Dewan, P. K., Lal, S. S., Lonnroth, K., Wares, F., Uplekar, M., Sahu, S., & Chauhan, L. S. (2006). Improving tuberculosis control through public–private collaboration in India: Literature review. British Medical Journal, 332, 574–578. doi:10.1136/bmj.38738.473252.7C
- Dieleman, M., Gerretsen, B., & Jan van der Wilt, G. (2009). Human resource management interventions to improve health workers' performance in low and middle income countries: Area list review. Health Research Policy and Systems, 7, 7. doi:10.1186/1478-4505-7-7
- Flynn, R. (2002). Clinical governance and governmentality. Health, Risk, & Society, 4, 155–173. doi:10.1080/13698570220137042
- Fochsen, G., Deshpande, K., & Thorsen, A. (2006). Power imbalance and consumerism in the doctor–patient relationship: Health care providers' experiences of patient encounters in a rural district in India. Qualitative Health Research, 16, 1236–1251. doi:10.1177/1049732306293776
- Fochsen, G., Deshpande, K., Ringsberg, K., & Thorson, A. (2009). Conflicting accountabilities: Doctor's dilemma in TB control in rural India. Health Policy, 89, 160–167. doi:10.1016/j.healthpol.2008.05.013
- Freedman, L. P. (2005). Achieving the MDGs: Health systems as core social institutions. Development, 48(1), 19–24. doi:10.1057/palgrave.development.1100107
- George, A. (2003). Accountability in health services: Transforming relationships and contexts. Working Paper Series 13(1), Harvard Centre for Population and Development, Harvard School of Public Health.
- George, A. (2009). ‘By papers and pens, you can only do so much’: Views about accountability and human resource management from Indian government health administrators and workers. International Journal of Health Planning and Management, 24, 205–224. doi:10.1002/hpm.986
- Gilson, L. (2003). Trust and the development of health care as a social institution. Social Science & Medicine, 56, 1453–1468. doi:10.1016/S0277-9536(02)00142-9
- Gilson, L., Hanson, K., Sheikh, K., Agyepong, I. A., Ssengooba, F., & Bennett, S. (2011). Building the field of health policy and systems research: Social science matters. PLoS Medicine, 8, e1001079. doi:10.1371/journal.pmed.1001079
- Harper, I. (2009). National tuberculosis control programmes of Nepal and India: Are they using the correct treatment regimens? Journal of Health Studies, 2(1–3), 51–67. Retrieved from http://www.jhs.co.in/articles/showArticle.aspx?aid=47
- Harrison, S., & Dowswell, G. (2002). Autonomy and bureaucratic accountability in primary care: What English general practitioners say. Sociology of Health and Illness, 24, 208–226. doi:10.1111/1467-9566.00291
- Justice, J. (1983). The invisible worker: The role of the peon in Nepal's health service. Social Science & Medicine, 17, 967–970. doi:10.1016/0277-9536(83)90223-X
- Kelkar-Khambete, A., Kielmann, K., Pawar, S., Porter, J., Inamdar, V., Datye, A., & Rangan, S. (2008). India's tuberculosis control program: Looking beyond detection and cure. International Journal of Tuberculosis and Lung Diseases, 12(1), 87–92. Retrieved from http://www.ingentaconnect.com/content/iuatld/ijtld/2008/00000012/00000001/art00017
- Kielmann, K., Deshmukh, D., Deshpande, S., Datye, V., Porter, J., & Rangan, S. (2005). Managing uncertainty around HIV/AIDS in an urban setting: Private medical providers and their patients in Pune, India. Social Science and Medicine, 61, 1540–1550. doi:10.1016/j.socscimed.2005.02.008
- Khan, M. A., Walley, J. D., Witter, S. N., Shah, S. K., & Javeed, S. (2005). Tuberculosis patient adherence to direct observation: Results of a social study in Pakistan. Health Policy and Planning, 20, 354–365. doi:10.1093/heapol/czi047
- Khare, R. S. (1996). Dava, Daktar, and Dua: Anthropology of practiced medicine in India. Social Science & Medicine, 43, 837–848. doi:10.1016/0277-9536(96)00128-1
- Kyaddondo, D., & Whyte, S. R. (2003).Working in a decentralized system: A threat to health workers' respect and survival in Uganda. International Journal of Health Planning and Management, 18, 329–342. doi:10.1002/hpm.730
- Lonnroth, K., Uplekar, M., Arora, V. K., Juvekar, S., Lan, N. T. N., Mwaniki, D., & Pathania, V. (2004). Public–private mix for DOTS implementation—What makes it work? Bulletin of the World Health Organisation, 82, 580–586. Retrieved from http://www.who.int/bulletin/volumes/82/8/580arabic.pdf?ua=1
- Mahendradhata, Y., Lambert, M.-L., Boelaert, M., & Van der Stuyft, P. (2007). Engaging the private sector for tuberculosis control: Much advocacy on a meager evidence basis. Tropical Medicine and International Health, 12, 315–316. doi:10.1111/j.1365-3156.2007.01816.x
- Manongi, R. N., Marchant, T. C., & Bygbyerg, I. C. (2006). Improving motivation among primary health care workers in Tanzania: A health worker perspective. Human Resources for Health, 4(6). doi:10.1186/1478-4491-4-6
- Mathauer, I., & Imhoff, I. (2006). Health worker motivation in Africa: The role of non-financial incentives and human resource management tools. Human Resources for Health, 4(24). doi:10.1186/1478-4491-4-24
- Murphy, E. (2003). Expertise and forms of knowledge in the government of families. Sociological Review, 51, 433–462. doi:10.1111/j.1467-954X.2003.00430.x
- Murthy, K. J., Frieden, T. R., Yazdani, A., & Hreshikesh, P. (2001). Public–private partnership in tuberculosis control: Experience in Hyderabad, India. International Journal of Tuberculosis and Lung Disease, 5, 354–359. Retrieved from http://www.ingentaconnect.com/content/iuatld/ijtld/2001/00000005/00000004/art00010
- Newman, J. (1998).The dynamics of trust. In A. Coulson (Ed.), Trust and contracts: Relationships in local government, health and public services (pp. 35–51). Bristol: Polity Press.
- Nichter, M. (2002). The social relations of therapy management. In M. Nichter & M. Lock (Eds.), New horizons in medical anthropology: Essays in honour of Charles Leslie (pp. 81–110). London and New York: Routledge.
- Ozawa, S., & Sripad, P. (2013). How do you measure trust in the health system? A systematic review of the literature. Social Science and Medicine, 19(91), 10–14. doi:10.1016/j.socscimed.2013.05.005
- Pradhan, A., Datye, V., Karina, K., Khilare, K., Datye, A., Inamdar, V., … Rangan, S. (2011). Sustaining PPM-DOTS: The case of Pimpri-Chinchwad, Maharashtra, India. Indian Journal of Tuberculosis, 58(1), 18–28. Retrieved from http://medind.nic.in/ibr/t11/i1/ibrt11i1p18.pdf
- Rangan, S. G., Juvekar, S. K., Rasalpurkar, S. B., Morankar, S. N., Joshi, A. N., & Porter, J. D. H. (2004). Tuberculosis control in rural India: Lessons from public–private collaboration. International Journal of Tuberculosis and Lung Diseases, 8, 552–559. Retrieved from http://www.ingentaconnect.com/content/iuatld/ijtld/2004/00000008/00000005/art00008
- Revised National TB Control Programme India. (2001). Involvement of non-governmental organizations in the revised national tuberculosis control programme. Delhi: Central TB Division, Directorate General of Health Services, Ministry of Health and Family Welfare, Government of India.
- Revised National TB Control Programme India. (2008). Revised scheme for NGOs and private providers. New Delhi: Central TB Division, Directorate General of Health Services, Ministry of Family Health and Welfare, Government of India.
- Rowe, R., & Calnan, M. (2006). Trust relations in health care: Developing a theoretical framework for the “new” NHS. Journal of Health Organization and Management, 20, 376–396. doi:10.1108/14777260610701777
- Udwadia, Z. F., Pinto, L. M., & Uplekar, M. W. (2010). Tuberculosis management by private practitioners in Mumbai, India: Has anything changed in two decades? PLoS ONE, 5(8), e12023. doi:10.1371/journal.pone.0012023
- Uplekar, M. (2003). Involving private health care providers in delivery of TB care: Global strategy. Tuberculosis, 83, 156–164. doi:10.1016/S1472-9792(02)00073-2
- Uplekar, M., Pathania, V., & Raviglione, M. (2001). Private practitioners and public health: Weak links in tuberculosis control. The Lancet, 358, 912–916. doi:10.1016/S0140-6736(01)06076-7
- Vyas, R. M., Small, P. M., & DeRiemer, K. (2003). The private–public divide: Impact of conflicting perceptions between the private and public health care sectors in India. International Journal of Tuberculosis and Lung Diseases, 7, 543–549. Retrieved from http://www.ingentaconnect.com/content/iuatld/ijtld/2003/00000007/00000006/art00008
