
ABSTRACT
The global rollout of Antiretroviral Treatment (ART) has revealed an urgent need to understand the medicines-taking practices of HIV-positive adolescents. In the last decade, the literature on the social determinants of health has broadened the evidence-base on ART adherence. Interdisciplinary studies have expanded conceptions of medicines-taking beyond clinical or health systems frameworks, recognising the importance of socio-structural conditions and of patients’ beliefs and experiences. Participatory research techniques which foreground the perspectives of adolescents provide greater insights still into their adherence. This article explores the use of participatory methods within a broader study on the social determinants of ART adherence among HIV-positive adolescents in South Africa. We describe how participatory methods were incorporated into this study (n = 1,059 in the quantitative baseline). We focus on an exercise, ‘Yummy or crummy?’, that explored the multisensory dimensions of medicines-taking, including their colour, smell, shape, and delivery mechanism. We describe two principal findings: first, adolescents’ preference for greater understanding of the chemical workings of medicines, manifested in their preferences for colour, taste and shape of medicines; and second, the vital relationship between sensory preferences and the social imperatives of discretion and confidentiality regarding HIV-status.
Antiretroviral (ART) adherence among youth
The global rollout of ART is among the largest public health interventions in history. By 2016, approximately 17 million people had been initiated onto treatment, with annual AIDS-related deaths decreasing by 43% since 2003 (UNAIDS, Citation2016). The rollout has led to astonishing improvements in global public health, but it has also highlighted the challenges of sustaining access and adherence to treatment, including in contexts that lack comprehensive healthcare. Non-adherence to medical regimens is common across populations and disease types (DiMatteo, Citation2004), revealing common discrepancies in how medicines are prescribed, and how they are taken. Even within well-resourced health contexts, retention in clinical care and ART adherence varies widely (Shubber et al., Citation2016). Continuing high rates of non-adherence demonstrate that vast numbers of people with HIV struggle to comply with their ART regimens.
This is particularly apparent among HIV-positive adolescents (aged 10–19), for whom HIV-related morbidity and mortality remain persistently high. Since 2000, deaths from AIDS declined in every age group except for adolescents, among whom AIDS mortality more than doubled (UNAIDS, Citation2013; UNICEF, Citation2016). Adolescents and young adults have higher rates of viral failure compared to all other age groups, and this is associated with higher rates of non-adherence to ART (Agwu & Fairlie, Citation2013; Fox et al., Citation2017; Maskew et al., Citation2016; Sohn & Hazra, Citation2013). While research on the ART rollout offers a vast corpus of knowledge on medicines-taking, studies on adherence in the global south, particularly among children and adolescents, remain comparably sparse (Ferrand et al., Citation2009; Lall, Lim, Khairuddin, & Kamarulzama, Citation2015; Mofenson & Cotton, Citation2013). Moreover, existing research on adolescent ART adherence has, in large part, been clinically-based (Hudelson & Cluver, Citation2015; Ridgeway et al., Citation2018).
The lack of empirical, extra-clinical data on adherence to ART among adolescents is partly the result of the daunting operational and ethical challenges of working with young research participants outside healthcare facilities (Bekker, Slack, Lee, Shah, & Kapogiannis, Citation2014; Mitchell & Sommer, Citation2016). To honour ethical commitments regarding consent and confidentiality, permissions for participation in research must be sought in ways that are meaningful and resonant for youth. Among research participants who are younger than the age of legal consent, additional permissions must be obtained from adult caregivers (Pope, Citation2007). Maintaining participant confidentiality may be especially difficult in locations that lack privacy, and in which others present are concerned or curious about what participants may confide. In addition, state laws may require researchers to report ‘high-risk’ participants to health and social services, breaking confidentiality through the process of referral.
Cognisant of these ethical cautions, there is a pressing need for research on the health behaviours of HIV-positive adolescents in lower- and middle-income countries, conducted both within and beyond clinical contexts. This includes within homes, schools, workplaces, and leisure spaces, in which adolescents are not identified solely or principally as ‘patients’. Understanding how to support adolescent adherence to ART and retention in care is particularly critical. Here, socio-structural factors – including access to sanitation, adequate food and water, psychosocial support and orphan-status – blend with adolescents’ ideas about medicines in determining adherence.
Numerous studies have demonstrated the confluence of clinical, health systems and socio-economic factors, operating at familial and individual levels, in influencing ART adherence among youth (Ammon, Mason, & Corkery, Citation2018; Heestermans, Browne, Aitken, Vervoort, & Klipstein-Grobusch, Citation2016; Nyogea et al., Citation2015). A focus on the social determinants of ART adherence in particular allows researchers to investigate the wider circumstances surrounding medicines-taking, reconstituting pill-taking from being an isolated, individual act, to a dynamic process involving many actors, and responsive to their ideas and experiences. From biomedical and technological perspectives, pill burden and palatability are widely recognised as key to ART adherence (Nachega et al., Citation2014; Shubber et al., Citation2016). Yet research on other experiential components of adolescent ART adherence, such as the colour, smell, and shape of medicines, remains rare. By integrating qualitative and quantitative research methods, and by foregrounding the perspectives of adolescents through participatory methods, a more diverse and comprehensive understanding of adolescents’ medicines-taking emerges.
There is a growing recognition of the value of interdisciplinary research in public health. This is part of a wider ‘epistemic transformation’ (Adams, Citation2013), in which novel sources of data, and their creative combination, are expanding the evidence-base in health research. One result, including from the literature on randomised controlled trials, is to acknowledge the limits of any single research approach, and to advocate methodological multiplicity (Padian, McLoy, Balkus, & Wasserheit, Citation2010). This is examined briefly below, in relation to two key theoretical and methodological bases for this article: the social determinants of ART adherence among adolescents; and the use of participatory research approaches to investigate these.
The social determinants of health
In the last decade, the World Health Organisation (WHO) has broadened the conceptual scope of its research to include a focus on the social determinants of health: the contextual, socio-structural, and systemic conditions that undergird the health of individuals and populations, and which are the basis of persistent inequalities in global health outcomes (WHO, Citation2008). The social determinants of health operate within and across multiple levels of organisation and action. They are imbricated within global and national political economies, and are responsive to shifting dynamics of governance and power (Blas et al., Citation2011; Solar & Irwin, Citation2010). As a conceptual framework, the social determinants of health combine socio-economic and health systems approaches, synthesising methods from the humanities and social sciences with those of economics, epidemiology and public health.
Exploring the utility of social determinants of health as a conceptual framework in South Africa, researchers have argued that a small number of social determinants, in potent combination, are responsible for the majority of pre-mature mortality. These include poor housing, inadequate water and sanitation, sub-optimal food, high levels of alcohol and substance abuse, low levels of social cohesion, and inadequate health-system responses (Scott, Schaay, Schneider, & Sanders, Citation2017). Thus, vast, heterogeneous phenomena in public health may be parsed through this framework and lent concision, without the loss of contextual specificity. Attention to the significance of location and context are foremost in analyses of the social determinants of health, including within a wide corpus of HIV social science in South Africa (Hodes & Morrell, Citation2018). Within of this study, a focus on the social determinants of health allows for a more expansive engagement with the experiences of medicines-taking among adolescents.
Participatory research
Research and programming drawing on the social determinants of health as a conceptual framework emphasises the value of multisectoral collaborations and participatory approaches (Blas et al., Citation2011; Khan & Ajmal, Citation2011). In recent decades, participatory research methods have gained utility in psychology, anthropology and gender studies. More recently still, and as a part of wider epistemic evolution mentioned above, these methods are being applied to health research (Colvin, Citation2015; Skovdal & Cornish, Citation2016). For the last five decades at least, various terms and definitions have been applied to participatory research (Ibid, 100). In this article, we understand participatory research broadly as a collection of methods and actions in which local perspectives form the basis of research (Ibid), and in which innovative adaptations of conventional research tools may generate new, participant-centred findings (Cornwall & Jewkes, Citation1995).
In a special edition of Global Public Health, Mitchell and Sommer (Citation2016) describe the potential of participatory visual methodologies for ‘eliciting evidence’ in public health research. Their phrasing encompasses the evocative and collaborative potential of participatory methods. While their focus is on visual methodologies, their recognition of the value of participant-generated data aligns with the methods reported here. Mitchell and Sommer also acknowledge the ethical and practical challenges of participatory research, and raise the spectre of potential tokenization of participants (discussed below).
The empirical value of participatory research is contested (Cornwall & Jewkes, Citation1995). With multiple forms of data, including drawings, role-playing sessions and other activities typically construed as ‘games’, what modes of analysis should be applied, and how may findings be construed as robust or representative? One rejoinder to its empirical limits is the potential for participatory methods to encompass longer-term perspectives, lengthening the duration of analysis beyond single ‘snapshots’, and leveraging the methodological strengths of multi-wave quantitative studies, as well as immersive, longer-term ethnographic work (Goldenberg, Finneran, Andes, & Stephenson, Citation2016). Another is the prospective value of research activities that are co-conceived, thematised and analysed by a study or intervention’s ‘target population’.
HIV-programming is regularly accused of neglecting the needs and preferences of HIV-positive youth. Participatory methods are valuable not only for eliciting the perspectives of marginalised populations, such as children and adolescents. In fact, approaching participatory research as another means of data extraction risks reifying research hierarchies in which the directives of researchers are paramount, and in which participants must serve as data points and subjects, rather than collaborators in tools design and analysis. Participatory methods may enhance the accessibility of research, build rapport with participants, and ameliorate power differentials through creative and collaborative strategies (Bray, Gooskens, Kahn, Moses, & Seekings, Citation2010). Based on the findings from the Mzantsi Wakho study – a mixed-method longitudinal cohort in South Africa – and with a focus on participatory methods, this article explores youth preferences for the multisensory components of medicines-taking.
Mzantsi Wakho: Study context and design
The Mzantsi Wakho study is located in the Eastern Cape province of South Africa, with an antenatal HIV prevalence of 29.1% (95% CI 27.3–30.9) (Department of Health, Citation2012) and high HIV and TB burdens (Department of Health, Citation2017a). Through partnerships between healthcare workers and community-based organisations, ART programmes were initiated in the late 1990s and early 2000s (Hofmeyr, Georgiou, & Baker, Citation2009). But, it was not until 2005, after a national civil society campaign and a court-ruling mandating the government to provide public access, that the provincial roll-out began in earnest. It is within this context – of high HIV prevalence and the delayed public provision of ART – that this study is based. South Africa now has the world’s largest ART programme, with an estimated 3.74 million people initiated onto ART by the end of 2016 (Department of Health, Citation2017b), but the historic lack of age disaggregation within national datasets makes it difficult to estimate the numbers of adolescents who have initiated ART. Extant research on clinical cohorts indicates that ART coverage and health outcomes are significantly poorer among HIV-positive adolescents than among adults (Maskew et al., Citation2016).
Permissions for the study were provided by the Universities of Cape Town and Oxford, the Eastern Cape Department of Health, and individual health facilities. In design, data collection, and dissemination phases, researchers consulted the Mzantsi Wakho Teen Advisory Group (TAG) for feedback on the relevance and accessibility of research questions and tools (Hodes et al., Citation2018). Participants and caregivers provided written informed consent for interviews, observations, and access to clinical records. Participant confidentiality was maintained except in cases of reported or witnessed abuse, in which referrals were made to health and social services.
The study was initiated in 2013, with six months of ethnographic research preceding the design and piloting of the first wave of the quantitative survey. Rather than using adult authorities, such as caregivers or healthcare workers, as ‘proxy informants’, in this formative phase we engaged 23 adolescents (11 boys and 12 girls) in ethnographic and participatory research. Over five subsequent years, qualitative investigators conducted over two thousand hours of direct observations and interviews in healthcare facilities, specifically within paediatric ART, family planning, and trauma units. The bulk of primary research with adolescents and their families was located within their homes and leisure spaces. Interviews, focus groups and observations provided insights into adolescents’ experiences of healthcare and medicines-taking. Research assistants experienced in conducting research with children and adolescents affected by HIV facilitated research activities, including through translations in translations in Afrikaans, English and isiXhosa. Participant observations, and informal conversations, were often guided by young people themselves, with discussions taking place while walking around neighbourhoods, spending time with friends, or seated in clinic waiting rooms.
Within the first six months of qualitative work, researchers noted that participants struggled to recollect or explain non-adherence to ART. Inconsistencies in ‘dose recall’, at times within a single interview, revealed participants’ confusion in defining and recounting adherence. This emphasised the importance of designing research tools that allowed adolescents to conceptualise their own medicines-taking practices, and of working in multiple sites – both clinical and extra-clinical. Within health facilities, researchers noted that participants strived to present as ideal patients (Vale, Hodes, Cluver, & Thabeng, Citation2017). In waiting rooms, talk of HIV or ART was thwarted by the fear of unintended HIV disclosure and its stigmatising consequences. Outside facilities, in leisure spaces and homes, discrepancies between reported and actual medicines-taking emerged. Adolescents spoke more freely about the difficulties they encountered in adhering to their medicines. They shared suspicions about the side-effects of ART, and fears that long-term compliance might have a negative effect on their physical health and social lives.
These findings informed the design and adaptation of the baseline quantitative survey, conducted with n = 1,059 HIV-positive adolescents in 2014–2015. They shaped the construction of metrics used for ART adherence, based on a triangulation of methods (three temporal markers of self-report, and biomarker data), and the survey’s mapping of the socio-ecological determinants of health using numerous measures and constructs (Cluver, Hodes, Sherr, et al., Citation2015; Cluver, Hodes, Toska, et al., Citation2015; Toska et al., Citation2016). The survey aimed to provide robust measures of adherence, cognisant of the descriptive difficulties that participants confronting in recalling and relaying medicines-taking. Analysis based on the quantitative baseline demonstrated high rates of non-adherence (Cluver et al., Citation2016), and positive associations between ART adherence and social support mechanisms (Toska et al., Citation2016). During the second and third waves of quantitative data collection, from 2015 to the present, qualitative research has continued to explore the conceptual and experiential challenges of adherence for HIV-positive adolescents.
Developing the ‘Yummy or crummy?’ participatory research tool
Between December 2013 and January 2016, Mzantsi Wakho researchers and young participants explored a range of participatory methods to capture and convey the experiences of ART adherence. Within a series of focus groups and workshops, we used visual, mapping methods, such as bodymapping, ‘dream-clinic’ designs and ‘river-of-life’ drawings, together with more performative approaches, including role-playing exercises such as the ‘dream clinic consultation’, and the convening of ‘youth parliaments’ (Hodes et al., Citation2018). These exercises were co-facilitated by researchers and participants, each receiving training through a facilitator guide developed by investigators and participants within the study.
Participatory approaches present a litany of practical and ethical challenges, including regarding informed consent, the ownership and reproduction of research materials (Vindrola- Padros, Martins, Coyne, Bryan, & Gibson, Citation2016), and the potential for tokenization of youth participants. We sought to address these challenges in multiple ways, ensuring that all participants consented to each exercise. At the beginning of an exercise, participants were given options of other games or activities should they not wish to participate, with no negative consequences. When participatory exercises produced materials, such as drawings or letters, participants were encouraged to keep these if they wished, again, with no negative consequences. Facilitators explained that materials created could be used by researchers in their publications, and shared with wider audiences such as policy-makers, but that these would be anonymised to protect participants’ identities.
Findings from participatory exercises were co-produced by researchers and participants within the sessions themselves, through the materials that were created (including written notes), and through individual and collective discussions in which participants recounted key themes and results. Findings were shared immediately, in group or individual conversations, or within subsequent engagements between participants and researchers (such as home or clinic visits). Findings were disseminated to broader audiences as well, with a focus on local-level health and social service providers working directly with youth. Findings from three participatory exercises in particular, ‘dream clinics’, ‘clinic report-cards’ and ‘dream consultations’, informed the drafting procedures and the content of South Africa’s National and Adolescent Youth Health Policy (Department of Health, Citation2017b).
Aware of the transactional nature of research, in which researchers benefit from the data gathered from participants, while the value of research for participants remains indeterminate, we sought means of building skills and advancing research capacity among participants, following their own suggestions sought through interviews preceding workshops, and during sessions themselves. These included skills-building, such as sessions on CV-writing, or educational exercises, such as a guide to healthy eating. Another principal objective of these research engagements was merely enjoyment: to ensure a safe and warm environment in which youth could be active and creative, and have fun.
Within the early phases of the study, having established that participants struggled to verbalise adherence practices and to define these within a framework of dose-recall, we sought to provide adolescents with a new means of describing these challenges. In 2013, we piloted a participatory exercise, the ‘Smarties game’, in which participants compared taking their ART with a familiar activity: eating sweets. In the course of in-depth interviews about medicines-taking (n = 27, 7 male and 20 female), participants were invited to eat sweets widely available in local shops, and which resembled commonly-prescribed pain medicines. They compared the experiences of eating these sweets with taking ART, describing similarities and differences. Researchers recorded participants’ responses in home-languages (Afrikaans, English and isiXhosa), coded these thematically, and cross-checked their findings with adolescents through subsequent interviews and observations.
Key findings from this exercise were the significance of pill burden and palatability: well-researched experiential components of ART adherence. Participants contrasted the pleasant taste of sweets with the bitterness of their medicines, and the ease of eating sweets with the difficulties of swallowing tablets (Hodes et al., Citation2017). In describing associations with defaulting, participants highlighted the size and shape of their medicines, in addition to their taste and number. For instance, Lulama (female, 18) stated: ‘taking the pills is hard work. I get lazy to take them. They are big and they stick in my throat’ (qualitative interview, 14 February 2013). The exercise suggested that various experiential components of medicines-taking, including the colour, size and shape of tablets, influenced participants’ impressions. It also revealed the role of socio-structural determinants, such as access to sanitation (potable water) in determining adherence. Due to the size of their pills, numerous participants explained that they had to be close to a water source while taking them, or had to have ample drinking water at the ready to prevent choking. One participant explained that she needed to take her pills ‘slowly, because they are hard to swallow’ (Sihle [age 16], qualitative interview, 1 February 2014).
Based on formative findings regarding the utility of participatory methods, including from the ‘Smarties game’, the study piloted additional methods. From November 2015 to January 2016, we designed a participatory research tool to explore the multisensory experiential components of medicines-taking, including sight, sound, smell, taste and touch. Facilitators, engaged participants in their language of choice.
Named ‘Yummy or crummy?: You are the Mzantsi Wakho Masterchef’, the exercise aimed to broaden the scope for the description of adolescents’ experiences and preferences for medicines through incorporating visual and performative components, providing participants with new ways of capturing and relating the multisensory experiences of medicines-taking. The exercise was piloted with a group of adolescents and young adults (n = 16, male 7, female 9) as part of a TAG weekend workshop in January 2016. TAG was established within the Young Carers study in 2012, and participants played an advisory role in the Mzantsi Wakho study, taking part in annual workshops (Hodes et al., Citation2018).
The game was led by a facilitator with nearly two decades of experience in research and advocacy with adolescents and youth. Twelve additional facilitators – one apportioned to each of the game stations – were trained using the facilitation guidelines developed for use in the study. The game was introduced and described by the lead facilitator, with an example of the taste station role-played among facilitators. Adolescents were divided into groups of three or four. Each team visited every game station for around ten minutes. Two roaming facilitators took notes of the exercise, shared in written form with the lead facilitator. Once all participants had been to all stations, the group was brought together for a discussion, with participants sharing their responses so the exercise.
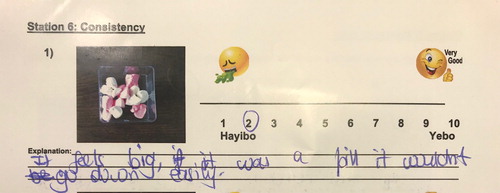
Through its multiple modes of engagement and assessment – written, discursive and performative – ‘Yummy or crummy?’ spanned a range of participatory techniques. We drew on the novel rubric developed by Skovdal and Cornish, identifying categories of participatory methods (Citation2016, p. 102). We combined ‘linkages and relationship tools’ (seeking connections between factors promoting or obstructing health), ‘experiential tools’ (foregrounding participants’ own perspectives), and ‘prioritization and quantification tools’ (utilising ranking and scoring to relay these perspectives) (Ibid). The exercise took the form of a game in which participants role-played as chefs, evaluating their preferences for ten experiential components of medicines-taking: smell, colour, size, shape, clarity, effervescence, consistency, coating, packaging, and delivery method. The game provided stations for each of these components. At each of the ten stations, participants were invited by facilitators to evaluate and document their preferences in two ways: (1) through direct description, captured as oral narratives, and (2) through a form designed collaboratively with study investigators and researchers ().
Figure 1. The front cover of the ‘Yummy or Crummy’ form.
The form aimed to engage participants and to encourage a diversity of responses. It combined an array of techniques for assessing medicines-preferences among young patients (Smith, Sammons, & Conroy, Citation2013), with emoticons from social media applications. These modes of assessment were labelled A-D. A. provided a scale for somatic responses to medicines ranging from disgust (a vomiting face) to delight (a smiley face gesturing ‘thumbs up’); B. made use of a linear scale (numbered one to ten, from least to most preferable); C. employed a rating of ‘Hayibo’ or ‘Yebo’ (translated as ‘No ways!’, or ‘sure thing’ from isiXhosa – the first language of all of the participants); and D. provided a space for discursive explanations.
The exercise used various modes of measurement, from structured, numerical forms of critical ranking (a scale for prioritisation and ‘explanation box’), to casual, interpersonal interactions, and discourses from social media (including slang expressions and emoticons). Emerging research explores the representativity and reliability of using emoticons in adolescent health research, including within the Mzantsi Wakho study (Carty, Hodes, Cluver, & Bhardwaj, Citation2017) ().
Figure 2. Modes of measurement in the form used to capture participants’ preferences in the ‘Yummy or crummy’ exercise (28 February 2016).
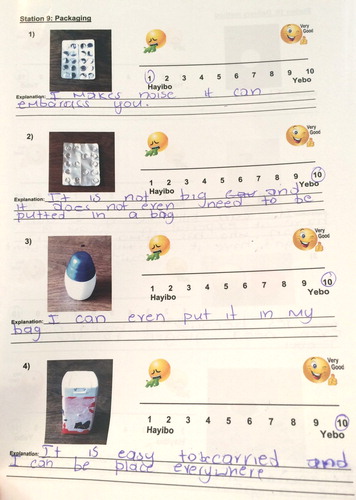
Where possible, ensuring that participants would be protected against potential harm, real medicines were included in the game. These included the stations for smell, size and shape, packaging, and delivery method. For other stations, including for colour, effervescence, clarity, consistency, taste and coating, edible analogues were used. For the smell station, five options were included: neutral (odourless), mint, vanilla, citrus and peach. Within the station on packaging (), participants were given four options: (1) plastic and foil blister pack, (2) foil blister pack, (3) plastic pill container (7 cm high, oval-shaped, screw-lid), and (4) plastic pill container (10 cm high, rectangle shaped, pop up lid).
Figure 3. Yummy or crummy packaging options: 1. Plastic blister pack; 2. Foil blister pack; 3. Conical container with screw-lid; 4. Square container with catch-pop lid.
The content of forms was transcribed, translated, and coded, with key themes identified by both participants and researchers, through one-on-one conversations with participants (noted in research memos), and through the collective appraisal of the exercise that followed its practical component. Participants’ preferences for the smell, taste, colour, consistency, and coating differed widely, foregrounding the significance of individual interpellation in medicines-taking. However, similarities also emerged. These resonated with findings from quantitative and qualitative datasets of the Mzantsi Wakho study, including the enduring effects of HIV-related stigma, and the impacts of various socio-structural determinants on adherence to ART (Cluver et al., Citation2016, Citation2018; Toska et al., Citation2016; Toska, Cluver, Hodes, & Kidia, Citation2015).
Findings
‘Yummy of Crummy?’ demonstrated the importance that adolescent participants ascribed to the ‘knowability’ of medicines: understanding their purposes and effects for those taking them, as well as those who might witness this. Participants expressed strong desires to understand more about their medicines, and sought explicit markers of quality control as an assurance of therapeutic benefit. The illness and treatment histories of these participants provide crucial context for this finding. Many had initiated ART while severely immune-suppressed and ill with opportunistic infections. The disclosure of their HIV-status, by a nurse or family member, was often accompanied by new understandings about the illness and death of their parents and siblings. Within the quantitative sample, an estimated 75% of adolescents were perinatally infected, and 59% had lost one or both parents (Cluver et al., Citation2018).
Within qualitative interviews, many participants recounted the ambiguous experience of ART initiation. On the one hand, this had led to their diagnosis, management and survival as patients with HIV, as well as to their enrolment in health and social support programmes. On the other, initiating ART was also bound up in fearful memories, including diagnosis with a chronic, potentially fatal illness, together with extended hospitalisation and painful recovery. Taking ART came with the continual risk of being ‘outed’ as HIV-positive. This was compounded by the perceived shame of having an HIV-positive (and often deceased) parent, for which daily doses of ART served as an aching reminder (Vale & Thabeng, Citation2016).
Interviews conducted with participants in the broader Mzantsi Wakho study, between January 2013 and March 2018, provided deeper insights into these experiences. Dineo (female, 17), explained that she was ‘infected by my mum from her breast when she was breastfeeding me’. In 2008, struggling to breathe, Dineo had been admitted to hospital. She spent the next eighteen months there, during which she was treated for TB and initiated onto ART. Her memories of that time were vague, but she recalled the colour of her TB medicines (green) and of the HIV test (white). Colours were among the sole descriptors used by Dineo in recounting her stay in hospital. In response to images of green medicines, Mandla (male, 22) wrote: ‘AHHH!! Just reminds me of TB pills and with the bad taste’. For others, green was an agreeable colour for pills due to its familiarity; its association with medicines previously taken. Keke (female, 22) explained: ‘Green is a colour that has been introduced other than white, so it is okay to get green some time’.
The colour of medicines was associated not just with other illnesses, but also with therapeutic efficacy. The strongest collective preference for pill colour was white, due to its familiarity as the colour of a myriad medicines in common use. Kelly (female, 21) explained: ‘I prefer it because … it is the normal colour for most of the pills’. For Keke (female 22) if a pill was not white, it was not ‘promising’. She explained: ‘Because white has always been the colour for pills/medication you get, any other colour would be strange.’ Ruby (female, 21), favoured white for similar reasons, describing it as ‘trustworthy … the most known [for] medicine’ ().
Figure 4. Yummy or Crummy participants at the ‘colour’ station, in which they discussed, described and evaluated their preferences for pill colour.
But while white as a pill colour was favoured by some due to its familiarity, it was disdained by others for its illness associations, with a white tablet disclosing the presence of a medical condition requiring treatment. For instance, Sam (male, 23) remarked that white was ‘too obvious … Some people don’t feel comfortable to drink pills in public’. The positive and negative impressions associated with colours revealed participants’ desires to know and trust their own treatments, while ensuring against inadvertent disclosure of illness to others.
This tension, between the desire for ‘knowability’ and discretion, was also relayed through participants’ preferences for smell. The smell station evoked a wide range of comparisons, foregrounding the power of association and memory. Five smell options – neutral, mint, vanilla, citrus and peach – were included within this station. These smells elicited diverse reactions, testifying to the variety of products at play within experiential repertoires of maintaining and restoring health. The various components of the smell station reminded participants of medicines for diarrhoea, chest infections and fevers, as well as humdrum household toiletries: toothpaste, pimple cream and hair conditioner. Numerous participants favoured odourlessness in medicines, associating a lack of smell with therapeutic benefit. Vuyo (male, 22), for instance, awarded a high ranking to a neutral smell because, simply: ‘it smells like medicine’. He gave a similarly high ranking to mint, which reminded him of toothpaste, signifying a product that was safe to ingest; a ‘medicine that is edible’.
Many participants expressed fears about pharmaceutical adulteration and counterfeit medicines. These surfaced within the stations on ‘size and shape’ (options: scored or unscored tablet) and ‘clarity’ (options: cloudy or clear liquid). Scored and numbered tablets conveyed to participants that medicines were being tested and evaluated, subject to standards of quality control. Ruby, for instance, preferred scored tablets because ‘it shows that it’s original … It shows the main thing of potency’. She regarded scored medicines as stronger and safer. Similarly, numerous participants described their preferences for ‘clear’ rather than ‘cloudy’ liquid suspensions. A dread of pollution and poisoning were evident in Sandy’s (female, 16) desire for a clear, rather than cloudy, liquid. She described the cloudy liquid as ‘like dirt water. I would not feel good. I would think that the person was trying to kill me’. The Mzantsi Wakho study has investigated associations between high rates of violence and non-adherence among participants, finding that violence victimisation at home, school and clinic were strongly associated with non-adherence (Cluver et al., Citation2018).
Hoping to protect themselves from harm, participants preferred clear medicines. Nelly (female, 16) attributed this preference to her need to ‘see if something is inside’. Vuyo concurred: ‘I’ll take the clear one, because it gives you a clear vision of what’s inside’. MJ (male, 17) recounted: ‘I would choose the clear one because, as the medicine, people would not be fooled’. Participants were anxious about the perceived threat of pharmaceutical adulteration, and its toxic or hazardous effects. Through diagnosis with an incurable illness, and initiation onto chronic medicines, participants worried that they were rendered reliable on medicines whose manufacture and regulation were determined by external factors, beyond their control, and whose continued provision and quality seemed uncertain.
Participants’ fears about being seen in possession of medicines stemmed from the stigma associated with being sick, and in particular with being HIV-positive. While ‘Yummy or crummy?’ did not focus specifically on HIV or on ART, qualitative interviews emphasised participants’ anxieties about being known as HIV-positive, through the public provision of medicines at a clinic, or through being seen in possession of ART. Participants feared that HIV disclosure – whether advertent or accidental – would bring shame. Many worried that public knowledge of their HIV-status would brand them as ‘weak’, physically compromised, and chemically reliant, exposing them as ‘damaged’ or ‘spoiled’. In clinic observations, participants avoided tasks that could potentially disclose their HIV-status to others, including carrying patient folders with identifying markers, (such as stickers or coloured forms used in ART stationery). The threat of disclosure was perceived to extend beyond health facilities, to the public transport that participants used to get to and from facilities, and to their schools, homes and leisure spaces. Participants regulated their behaviours closely to protect themselves from involuntarily disclosing their HIV-status, including through concealing their ART. They left their medicines at home rather than taking them out into public, or concealed them in scraps of toilet paper hidden in underwear.
For Keke, being in possession of a pill blister pack was a ‘give-away’, revealing private information about her health status. She described this as ‘like you disclose yourself … It simply shows that you are the medication person’. MJ echoed Keke’s fears. He disdained a plastic pill container as packaging because ‘[P]eople can see that you are sick, especially those you didn’t want to tell them’. Ruby explained her low scores for blister packaging by saying that ‘People will see that you eating medications, and it is so embarrassing to take in front of everyone’.
The crackling sound made by pill packaging invoked anxiety due to its potential exposure of illness. Ruby described how ‘I will be … ashamed of myself, coz it’s noisy and uncontrollable’. Sandy (female, 16 years) conveyed her dislike of the plastic and foil blister pack in similar terms: ‘It makes noise and it can embarrass you’. For a number of participants, then, fear of HIV-related stigma was a multisensory experience, in which even the sounds associated with medicine-taking could be a source of possible disgrace. Participants had strong preferences for packaging that could pass as multi-purpose. For instance, Ruby favoured a blank plastic container because ‘It’s much safer for carrying in public, people will think maybe its sweets or something, they won’t notice if it’s pills’.
The ability to transport medicines with convenience and tact influenced preferences for packaging, but also raised doubts about confidentiality. While blister packs were scored highly for their lightness and portability, they could also compromise privacy. As Amelia (female, 22) explained: ‘It’s easy to slip in your pocket, but it is giving people that look of questioning: “Why is he/she taking the medication?”’ Amelia wanted a smaller and more discreet plastic container which was ‘easy to open and carry in my bag’. For her, a larger container would be cumbersome, taking up ‘a lot of space’. It also risked rousing public suspicions, causing ‘people to wonder and look with questioning eyes’.
While some participants favoured blister packs as a form of packaging, they also described these as flimsier than plastic containers, with the risk that contents could be misplaced. MJ recounted: ‘I cannot carry this one because pills can easily pop out at any time, and you will be left with nothing … All your pills will fall down’. Lost pills threatened unintentional illness disclosure, and saddled participants with the burden of returning to a healthcare facility for replacements. School and work attendance meant that many adolescents and young adults were unable to visit healthcare facilities themselves, relying on family members to fill their prescriptions on their behalf. Scheduled clinic visits, requiring transport money, were already a strain on many household budgets. Unscheduled visits to replace lost pills posed a further drain on finances, meaning that money for essential items such as food and fuel would need to be re-apportioned. In addition to the material and opportunity costs of further clinic visits, stock-outs meant that essential medicines, including for TB and HIV, might be difficult or impossible to replace in time to avoid treatment interruptions (Hodes, Price, Bungane, Toska, & Cluver, Citation2017).
Conclusion
There is a lack of research on the experiential dimensions of ART adherence among children and adolescents. Further studies must seek to answer questions at the cross-sections of clinical, public health and social science research, providing novel solutions to the challenge of chronic adherence. This research indicates that social determinants of health are powerfully associated with adherence, and that the experiential and affective dimensions of medicines-taking are instrumental in adolescents’ adherence. This research aims to challenge univocal approaches to studies on ART adherence and medicines-taking among adolescents. Shifting focus from monochromatic accounts of pill-burden and palatability, it approaches adherence as vividly multisensory. Through participatory techniques that engage adolescents and young adults with HIV, it foregrounds their ideas and experiences of the many facets of ART adherence.
Research on the social implications of ART adherence has focused on the benefits of adherence in restoring health. Among the youth in this study, ART-adherence meant health and survival, with strong associations between positive health outcomes and adherence. However, taking ART was also overlaid with fears of HIV-status exposure, and the concomitant shame this would bring to individuals and their families. Doubts about the reliability and safety of medicines conveyed anxieties about continued access to good quality drugs, and worries about the harmful effects of counterfeit medicines.
Our findings suggests that – for the youth in this study – the public provision of ART in South Africa has not resulted in the social reconfiguration of HIV, from a heavily stigmatised, dread disease, to a manageable and ‘normal’ chronic condition. While the ART rollout has begun to reverse AIDS-related morbidity and mortality, impressions of HIV as a terminal illness persist – informing perceptions about the efficacy and safety of its treatment. For many youth in this study, being HIV-positive remained strongly associated with a sense of contamination, with far-reaching impacts on health behaviours, particularly ART adherence. Participants feared that pill-taking exposed them to public censure and humiliation, revealing that living with HIV remains a marker of derogation. Moreover, their fears about the potential hazards of taking medicines – including the threat of perceived threat of pharmaceutical adulteration, necessitates urgent attention in the form of improved treatment literacy and adherence counselling. Because many active ingredients are insoluble, and require a suspension (cloudy) formulation, participants’ apprehensions of cloudy medicines could impact negatively on their use of certain pharmaceuticals.
Within the ‘Yummy or Crummy?’ exercise, participants’ preferences for medicines were not based on a single, sensory or experiential factor. Rather, they were made up of a composite of physical, social and emotional experiences, of both health and disease. Past experiences of illness, perceived stigma, as well as ideas and aspirations for therapeutic benefit, informed adolescents’ preferences for medicines across an array of sensory dimensions. In order to improve the health outcomes of HIV-positive youth, interventions must support and promote ART adherence, including through practical engagement with the multisensory components of medicines-taking. Participatory research, piloted and adapted with creativity and caution, may expand the evidence-base on ART adherence, focusing research and programming on the immediate and explicit needs of HIV-positive youth.
Data available
Data are not publicly available due to the ethical necessity of maintaining participant confidentiality.
Acknowledgments
The Mzantsi Wakho study was supported by the Nuffield Foundation under Grant CPF/41513, the International AIDS Society through an award of the Collaborative Initiative for Paediatric HIV Education and Research (CIPHER) (155-Hod); Evidence for HIV Prevention in Southern Africa (MM/EHPSA/UCT/05150014); Johnson and Johnson, and the John Fell Fund (103/757). Additional support for LC was provided by the European Research Council (ERC) under the European Union’s Seventh Framework Programme (FP7/2007–2013)/ERC grant agreement n8313421, and the Leverhulme Trust (PLP-2014-095). The project received ESRC Impact Acceleration Account Support. Authors thank participants and their families, and acknowledge the crucial support of the Mzantsi Wakho research team: Nontuthuzelo Bungane, Lizzy Button, Marisa Casale, Eda He, Alex Heusel, Sarah Hoeksma, Zukolwethu Jantjies, Chunyiswa Kama, Beauty Kamile, Bulelani Kinana, Vuyiseka Luke, Blessings Madondo, Kanya Makabane, Babalwa Makwenkwe, Thembani Mampangashe, Zoliswa Marikeni, Amanda Mbiko, Sally Medley, Phumla Mngese, Sibulele Mngese, Philiswa Mjo, Sindiswa Mona, Mavis Mpumlwana, Siyavuya Mqalo, Sinazo Mwellie, Phumla Myoyo, Unathi Ngesi, Sabatha Ngozi, Phumla Nobatye, Nisso Nurova, Marija Pantelic, Thandokazi Ramncwana, Julia Rosenfeld, Bongiwe Saliwe, Izidora Skracic, Janina Steinert, Babalwa Taleni and Mildred Thabeng. For their insights into participatory research, we thank Rachel Bray, Inge Corles, Caroline Kuo, Marija Pantelic and Morten Skovdal. For their fortitude in co-facilitating the exercises described here, we thank Lesley Gittings and Samantha Malunga. We are grateful to two anonymous reviewers who commented on previous drafts of this article.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Adams, V. (2013). Evidence-based global public health: Subjects, profits, erasures. In J. Biehl & A. Petryna (Eds.), When people come first: Critical studies in global health (pp. 54–90). Princeton: Princeton University Press.
- Agwu, A. L., & Fairlie, L. (2013). Antiretroviral treatment, management challenges and outcomes in perinatally HIV-infected adolescents. Journal of the International AIDS Society, 16(1), 18579. doi: 10.7448/IAS.16.1.18579
- Ammon, R., Mason, S., & Corkery, J. M. (2018). Factors impacting antiretorviral therapy adherence among human immunodeficiency virus-positive adolescents in Sub-saharan Africa: A systematic review. Public Health, 157(April), 20–31. doi: 10.1016/j.puhe.2017.12.010
- Bekker, L. G., Slack, C., Lee, S., Shah, S., & Kapogiannis, B. (2014). Ethical issues in adolescent HIV research in resource-limited countries. Journal of Acquired Immune Deficiency Syndromes, 65(1), S24–S28. doi: 10.1097/QAI.0000000000000036
- Blas, E., Sommerfeld, J., & Sivasankara Kurup, A. (2011). Introduction and methods of work. In E. Blas, J. Sommerfeld, & A. Sivasankara Kurup (Eds.), Social determinants approaches to public health: From concept to practice (pp. 1–8). Geneva: WHO.
- Bray, R., Gooskens, I., Kahn, L., Moses, S., & Seekings, J. (Eds.). (2010). Growing up in the new South Africa: Childhood and adolescents in post-Apartheid Cape Town. Cape Town: HSRC Press.
- Carty, R., Hodes, R., Cluver, L., & Bhardwaj, S. (2017). Symptom or sentiment?: Considerations for mHealth interventions designed for HIV+ adolescents. Proceedings of the 2017 International Conference on Digital Health, 227–228. (London, Association for Computing Machinery).
- Cluver, L., Hodes, R., Sherr, L., Orkin, M., Meinck, F., Ken, P., … Vicari, M. (2015). Social protection: Potential for improving outcomes among adolescents. Journal of the International AIDS Society, 18(6), S1–S7.
- Cluver, L., Hodes, R., Toska, E., Kidia, K. K., Orkin, F. M., Sherr, L., & Meinck, F. (2015). HIV is like a tsotsi. ARVs are your guns: Associations between HIV-disclosure and adherence to antiretroviral treatment among adolescents in South Africa. AIDS, 29(1), S57–S65. doi: 10.1097/QAD.0000000000000695
- Cluver, L., Meinck, F., Toska, E., Orkin, F. M., Hodes, R., & Sherr, L. (2018). Violence exposure and adolescent antiretroviral non-adherence in South Africa. AIDS, 32(8), 975–983.
- Cluver, L., Toska, E., Orkin, M., Meinck, F., Hodes, R., Yakubovich, A., & Sherr, L. (2016). Achieving equity in HIV-treatment outcomes: Can social protection improve adolescent ART-adherence in South Africa? AIDS Care, 28(2), 73–82. doi: 10.1080/09540121.2016.1179008
- Colvin, C. J. (2015). Anthropologies in and of evidence making in global health research and policy. Medical Anthropology, 34(2), 99–105. doi: 10.1080/01459740.2014.963196
- Cornwall, A., & Jewkes, R. (1995). What is participatory research? Social Sciences and Medicine, 41(12), 1667–1676. doi: 10.1016/0277-9536(95)00127-S
- Department of Health, South Africa. (2012). The 2011 national antenatal sentinel HIV and syphilis prevalence survey in South Africa. Pretoria: National Department of Health.
- Department of Health, South Africa. (2017a). Let our actions count: South Africa’s national strategic plan on HIV, TB and STI’s 2017–2022.
- Department of Health, South Africa. (2017b). National adolescent and youth health policy. Pretoria: National Department of Health.
- DiMatteo, M. R. (2004). Social support and patient adherence to medical treatment: A meta-analysis. Health Psychology, 23(2), 207–218. doi: 10.1037/0278-6133.23.2.207
- Ferrand, R. A., Corbett, E. L., Wood, R., Hargrove, J., Ndhlovu, C. E., Cowan, F. M., … Williams, B. G. (2009). AIDS among older children and adolescents in Southern Africa: Projecting the time course and magnitude of the epidemic. AIDS, 23(15), 2039–2046. doi: 10.1097/QAD.0b013e32833016ce
- Fox, M. P., Maskew, M., Brennan, A. T., Evans, D., Onoya, D., Malete, G., … Sanne, I. (2017). Cohort profile: The right to care clinical HIV cohort, South Africa. BMJ Open, 7(6), e015620. doi: 10.1136/bmjopen-2016-015620
- Goldenberg, T., Finneran, C., Andes, K. L., & Stephenson, R. (2016). Using participant-empowered visual relationship timelines in a qualitative study of sexual behavior. Global Public Health, 11(5–6), 699–718. doi: 10.1080/17441692.2016.1170869
- Heestermans, T., Browne, J. L., Aitken, S. C., Vervoort, S. C., & Klipstein-Grobusch, K. (2016). Determinants of adherence to antiretroviral therapy among HIV-positive adults in Sub-saharan Africa: A systematic review. BMJ Global Health, 1(4), e000125. doi: 10.1136/bmjgh-2016-000125
- Hodes, R., Doubt, J., Toska, E., Vale, B., Zungu, N., & Cluver, L. (2018). The stuff that dreams are made of: HIV-positive adolescents’ aspirations for development. Journal of the International AIDS Society, 21(S1), E25057. doi: 10.1002/jia2.25057
- Hodes, R., Dowse, R., Cluver, L., Vale, B., Toska, E., Gittings, L., & Ashorn, M. (June 2017). Yummy or crummy? Pill burden, palatability and ART adherence among adolescents. Oral presentation at the Southern African AIDS Conference, Durban, South Africa.
- Hodes, R., & Morrell, R. (2018). Incursions from the epicentre: Southern theory, social science, and the global HIV research domain. African Journal of AIDS Research, 17(1), 22–31. doi: 10.2989/16085906.2017.1377267
- Hodes, R., Price, I., Bungane, N., Toska, E., & Cluver, L. (2017). How frontline healthcare workers respond to stock-outs of essential medicines in the Eastern Cape. South African Medical Journal, 107(9), 738–740. doi: 10.7196/SAMJ.2017.v107i9.12476
- Hofmeyr, G., Georgiou, T., & Baker, C. (2009). The Keiskamma AIDS treatment programme: Evaluation of a community-based antiretroviral programme in a rural setting. Southern African Journal of HIV Medicine, 10(1), 38–41.
- Hudelson, C., & Cluver, L. (2015). Factors associated with adherence to antiretroviral therapy among adolescents living with HIV/AIDS in low- and middle-income countries: A systematic review. AIDS Care, 27, 805–816. doi: 10.1080/09540121.2015.1011073
- Khan, K. S., & Ajmal, A. (2011). Women’s empowerment and its challenges: Review of a multi-partner national project to reduce malnutrition in rural girls in Pakistan. In E. Blas, J. Sommerfeld, & A. Sivasankara Kurup (Eds.), Social determinants approaches to public health: From concept to practice (pp. 118–127). Geneva: WHO.
- Lall, P., Lim, S. H., Khairuddin, N., & Kamarulzama, A. (2015). Review: An urgent need for research on factors impacting adherence to and retention in care among HIV-positive youth and adolescents from key populations. Journal of the International AIDS Society, 18(2S1), 19393.
- Maskew, M., Fox, M. P., Evans, D., Govindasamy, D., Jamieson, L., Malete, G., … Technau, K. (2016). Insights into adherence among a cohort of adolescents aged 12–20 years in South Africa: Reported barriers to antiretroviral treatment. AIDS Research and Treatment, 2016, 1–12. doi: 10.1155/2016/4161738
- Mitchell, C. M., & Sommer, M. (2016). Participatory visual methodologies in global public health. Global Public Health, 11(5–6), 521–527. doi: 10.1080/17441692.2016.1170184
- Mofenson, L., & Cotton, M. (2013). The challenges of success: Adolescents with perinatal HIV infection. Journal of the International AIDS Society, 16(1860), 1–3.
- Nachega, J. B., Parienti, J. J., Uthman, O. A., Gross, R., Dowdy, D. W., Sax, P. E., … Giordano, T. P. (2014). Lower pill burden and once-daily antiretroviral treatment regimens for HIV infection: A meta-analysis of randomized controlled trials. Clinical Infectious Diseases, 58(9), 1297–1307. doi: 10.1093/cid/ciu046
- Nyogea, D., Mtenga, S., Henning, L., Franzeck, F. C., Glass, T. R., Letang, E., … Geubbels, E. (2015). Determinants of antiretroviral adherence among HIV-positive children and teenagers in rural Tanzania: A mixed methods study. BMC Infectious Diseases, 15, 280901. doi: 10.1186/s12879-015-0753-y
- Padian, N. S., McLoy, S. I., Balkus, J. E., & Wasserheit, J. N. (2010). Weighing the gold in the gold standard: Challenges in HIV prevention research. AIDS, 24(5), 621–635. doi: 10.1097/QAD.0b013e328337798a
- Pope, A. (2007). HIV prevention research and minors. South African Law Journal, 124, 165–187.
- Ridgeway, K., Dulli, L. S., Murray, K. R., Silverstein, H., Dal Santo, L., Olsen, P., … Paraskevis, D. (2018). Interventions to improve antiretroviral therapy adherence among adolescents in low- and middle-income countries: A systematic review of the literature. PLoS ONE, 13(1), e0189770. doi: 10.1371/journal.pone.0189770
- Scott, V., Schaay, N., Schneider, H., & Sanders, D. (2017). Addressing social determinants of health in South Africa: The journey continues. In A. Padarath & P. Barron (Eds.), South African health review 2017 (pp. 77–88). Durban: Health Systems Trust.
- Shubber, Z., Mills, E. J., Nachega, J. B., Vreeman, R., Freitas, M., Bock, P., … Weiser, S. D. (2016). Patient-reported barriers to adherence to antiretroviral therapy: A systematic review and meta-analysis. PLOS Medicine, 13, e1002183. doi: 10.1371/journal.pmed.1002183
- Skovdal, M., & Cornish, F. (2016). Chapter 5: Participatory data collection methods. In Qualitative research for development: A guide for practitioners (pp. 99–130). Warwickshire: Practical Action.
- Smith, C. M., Sammons, H. M., & Conroy, S. (2013). A prospective study to assess the palatability of analgesic medicines in children. Journal of Advanced Nursing, 69(3), 655–663. doi: 10.1111/j.1365-2648.2012.06050.x
- Sohn, A., & Hazra, R. (2013). The changing epidemiology of the global paediatric HIV epidemic: Keeping track of perinatally HIV-infected adolescents. Journal of the International AIDS Society, 16(1), 18555. doi: 10.7448/IAS.16.1.18555
- Solar, O., & Irwin, A. (2010). A conceptual framework for action on the social determinants of health. Social Determinants of Health Discussion Paper 2 (Policy and Practice). Geneva: WHO.
- Toska, E., Cluver, L., Boyes, M., Isaacsohn, M., Hodes, R., & Sherr, L. (2016). School, supervision and adolescent-sensitive clinic care: Combination social protection and reduced unprotected sex among HIV-positive adolescents in South Africa. AIDS and Behavior, 21(9), 1–14.
- Toska, E., Cluver, L., Hodes, R., & Kidia, K. (2015). Sex and secrecy: How HIV-status disclosure affects safe sex among HIV-positive adolescents. AIDS Care, 27(1), 47–58. doi: 10.1080/09540121.2015.1071775
- UNAIDS. (2013). Report on the global AIDS epidemic. Geneva: UNAIDS.
- UNAIDS. (2016). Global AIDS update. Geneva: UNAIDS.
- UNICEF. (2016). For every child end AIDS, seventh stocktaking report. Geneva: UNICEF.
- Vale, B., Hodes, R., Cluver, L., & Thabeng, M. (2017). Bureaucracies of blood and belonging: Documents, HIV-positive youth and the state in South Africa. Development and Change, 48(6), 1287–1309. doi: 10.1111/dech.12341
- Vale, B., & Thabeng, M. (2016). Redeeming lost mothers: Adolescent antiretroviral treatment and the making of home in South Africa. Medical Anthropology, 35(6), 489–502. doi: 10.1080/01459740.2016.1145218
- Vindrola- Padros, C., Martins, A., Coyne, I., Bryan, G., & Gibson, F. (2016). From informed consent to dissemination: Using participatory visual methods with young people with long-term conditions at different stages of research. Global Public Health, 11(5–6), 636–650. doi: 10.1080/17441692.2016.1165718
- World Health Organisation, Commission on Social Determinants of Health. (2008). Closing the gap in a generation: Health equity through action on the social determinants of health. Geneva: WHO Press.
