
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
To reach the most vulnerable individuals in under-resourced countries, health communication interventions increasingly move towards the community level. However, little is known about how health information spreads through local social networks. This paper maps the health information network of a rural trading centre in Uganda. As part of a five-year ethnographic study of sustainable community health resources, ego networks were obtained for 231 village residents in March 2014. Using both ethnographic and social network data, we analyze how the village social network is structured, and how this structure may influence the transmission of health information. Results show a network with low average proximity, with a small number of individuals, notably key administrative officials, much closer connected to many other community members than average. However, because of social partitioning in the village network, a number of people are outside the social clusters in which the top influencers are located.
Introduction
Background
Although public health agencies have long recognised the role of culture in shaping health communication at the community level, the evidence base regarding information flow at the community-level is still small (De Vries & Pool, Citation2017; Kreuter & McClure, Citation2004). Given the large cultural diversity to be covered, we actually know very little about community level dynamics of health information. This is particularly the case in many low-resourced, rural communities, where access to accurate health information is problematic (Campbell & Cornish, Citation2012). At the same time, there is a policy shift towards small-scale, community-based efforts in health communication based on the premise that participatory methods increase involvement. However, in a review of 48 studies of health communication campaigns in poor countries, Sood et al. (Citation2014) cautiously note that ‘it would be premature to presume that these community-based communication campaigns are truly community driven and participatory’ (p82). Without a strong evidence base, it is difficult to evaluate what actually works, and what is mere window dressing for business as usual (De Vries & Pool, Citation2017).
The aim of this paper is to describe how health information is distributed in a rural community. During a two-year anthropological research project on community health resources, ethnographic and social network data were collected detailing community-level social network relationships in a low resourced, rural community in Uganda. We asked how health information diffused through this community network, and which types of people (e.g. chairpersons or community health workers) and/or groups of people are most influenced by this information flow. The study location is Dekabusa, a small trading centre off the main road in Luwero district, about two hours north of Kampala by car.
We turned to social network analysis after we observed how important social groups were for the resilience of local people. Many community members had joined various small groups that supported them in times of urgent need, including funeral, health, agricultural and general saving groups, embedded in a traditional moral context of community work (bulungi bwansi). Many of these local, informal groups served as vehicles for the exchange of health information, underscoring the influence of friendship and family relations in health communication (Musinguzi, Citation2015). In addition, it appeared that these local networks were more influential than external sources of information, a finding supported by other studies (Adams, Citation2007; Matouš et al., Citation2013; Todo et al., Citation2014). External health communicators were often seen as detached, technical messengers who were not interested in staying, and as such did not gain the same influence as local actors. In Dekabusa, even the local community health workers were perceived by many as co-opted by not-to-be-trusted external (medical) networks, partly as a result of exclusionary recruitment practices (Turinawe et al., Citation2015). We believe occured not only because biomedical beliefs clash with local, traditional ways of thinking (de Vries et al., Citation2016), but also because local community members simply put more effort into making sure their message is perceived as credible. In other words, during the course of ethnographic observations, we learned that trusted sources of health information were often more local than external, and typically this meant that credible health information came through informal chatting, rumours, the village chairman, or those community members with some education, able to translate technical knowledge into local vernacular.
Based on these ethnographic observations, and with the intent of finding ways to access this local network for health information campaigns about sanitation, we developed a simple social network measurement instrument to document the potential local health information network. We turned to social network theory to find out how the local social network’s structure influences health information flow. Furthermore, the ethnographic details we had collected on the local social structure allowed us to validate and interpret social network results. It provided unique context to the specific health roles of the most influential actors and interpretation and contextualisation to the findings about power and influence in the village network. We also used the ethnographic knowledge to verify the validity of the mentioned local support groups people attended to in their community.
Health information networks at the community level
Studies on social networks have shown that people’s health is socially interdependent and that health and health care transcends the individual-level (Behrman et al., Citation2002; Kohler et al., Citation2015; Smith & Christakis, Citation2008). Network composition, individual network centrality, and network structure are associated with important health behaviours and health and development outcomes in different contexts across multiple levels of analysis and across distinct network types (Perkins et al., Citation2015). Interestingly, social network studies show similar results despite cultural differences (Adams et al., Citation2006). Smith and Christakis (Citation2008) concluded that generally, dyadic influences such as spousal and other interpersonal connections, in particular peers, as well as super-dyadic effects (where entire networks influence health outcomes), affect the spread of reproductive health behaviour and emotions. Chami et al. (Citation2014) found that in-degree, the number of incoming connections, to some extent a measure of popularity, is a significant predictor of self-reported physical health. Furthermore, they found that heads of households with high betweenness, or a brokerage position in between non- or sparsely connected others, tend to avoid poor health behaviours more than most other people who are not in brokerage positions, and are also more susceptible to social influence for preventative health measures.
However, while these findings articulate the relevance of social networks to health behaviour, fewer studies relate this relevance to health communication, and within these even less to the information dynamics at a local, community level. When studies do describe communal health systems, including informal health workers, they typically pay less attention to information and communication networks (e.g. Sudhinaraset et al., Citation2013). Some exceptions exist. Alverge and colleagues found that in Ethiopian rural areas, decisions on first-ever use of contraceptives were mostly related to individual demographic and socio-economic characteristics, as well as religious group, whereas the contribution of social transmission from either best friends or contraceptive ever-users in proximate households was minimal (Alvergne et al., Citation2011). However, their study tells about a population in the early stages of contraceptive uptake, which means that at the time of adoption most of these women were innovators relative to their friendship networks. Other studies show different patterns. In a longitudinal study on contraceptive use in rural Kenya, Behrman et al. (Citation2002) showed that social networks primarily affected respondents’ contraceptive choices through the provision of information, rather than by exerting social influence. Adams et al. mentioned the size of cognitive support networks – defined as networks that provide preventive and therapeutic suggestions and directives – as one of the main influences on child survival among the Fulbe in Mali (Adams et al., Citation2002). In an urban setting in Tanzania, Mulawa et al. (Citation2016) explained significant clustering of men's HIV-related normative beliefs and behaviours within their naturally occurring peer social networks as caused by denser (more connected) social networks. Additionally, groups with greater transitivity, where someone’s friends are also friends with each other, may also be characterised by more frequent discussions about health behaviours and the consequences of those behaviours (Burt, Citation1987).
Overall, information flow as object of study in social network analyses of health dynamics in rural, vulnerable communities has remained quite scarce. What we do know is that in rural settings, local networks have strong influence on the spread of information. Loutfi et al. investigated social networks of young women to see if recruitment into an HIV programme would work better if women were approached based on their social networks (Loutfi et al., Citation2019). They found that marginalised young women went most often to other women, usually in the same community, and with children if they had children themselves. They also found that rural women were better connected with each other than women in urban areas, although there also were isolated young women in all communities. Similarly, a study of social networks in Malawi by Houston and Hovorka (Citation2007) concluded that in ‘traditional African society’, oral tradition, high degrees of solidarity and mutual support are associated with a stronger influence of family, friends, neighbours, religious leaders, and traditional healers on health-related behaviour, in contrast to generic messages on HIV prevention. Musalia (Citation2005) showed that community wide networks among Kenyan Murang people were not as influential on fertility behaviour as more close knit social networks of family members.
Specific to Uganda, Ssengas, or maternal aunts, are likely to play roles in health communication efforts based on documented historical relationship with young people (Dralega, Citation2008; Muyinda et al., Citation2004). Yet, while such insights are quickly used in health communication campaigns as promising practices (e.g. Ybarra et al., Citation2014) it is not clear what the relative power of Ssengas actually is compared to other social actors in small localities without a broader, social network approach. Writing about other areas in Uganda, Jacobs et al. (Citation2004) reported that health information about STDs – erroneous or not – often comes from parents, teachers and health workers, while Ssengas are not mentioned. Kiapi-Iwa and Hart (Citation2004) identified health workers as the most important category of people providing information on SRHR to young people in Adjumani, northern Uganda. When it comes to common childhood illnesses, Twabeze (Citation2001) pointed out that there is no documentation of credible studies addressing communication for behaviour change in Uganda. Overall, we find no comprehensive description of rural, community level information networks.
Materials and methods
Dekabusa is located in central Uganda’s Luwero district, located approximately 60 kms from Kampala city, along Kampala-Gulu road. A significant majority of the people are native Baganda, and speak Luganda. The district was a centre of the guerrilla war activities between 1981 and 1986 during which the health infrastructure was greatly affected. The rehabilitation efforts that followed saw the establishment of the Ministry in charge of Luwero Triangle, including Luwero county. A host of non-government organisations (NGOs) such as Plan International Uganda, AMREF and Association Francois-Xavier Bagnoud (AFXB) have also implemented programmes in the district aimed at improving the health of communities. Dekabusa has no formal treatment facility assigned to its jurisdiction; residents often have to go further away, to private providers or informal providers. Data from Konde-Lule et al. (Citation2010) suggest that health care services in rural areas are provided mostly by private providers (63%), mostly for ambulatory health care, leaving more serious conditions to public hospital care.
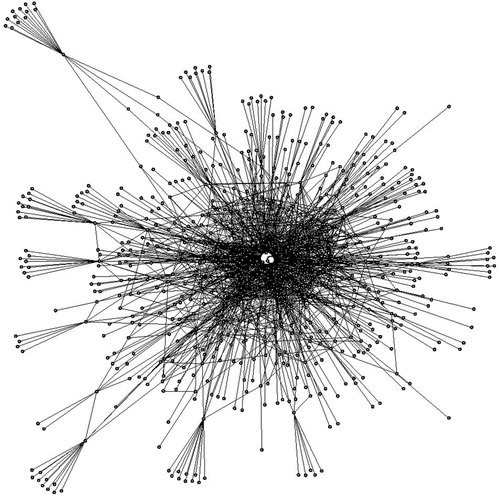
As part of a larger ethnographic project and pilot intervention concerning development of sustainable community health resources in poor resources settings in Uganda (CoHeRe), between 2012 and 2014, three team members lived in Dekabusa Trading Center off the main road in Luwero County, and carried out ethnographic research. They participated in community activities – village meetings, parties, funerals – and held informal and formal interviews and focus group discussions with community members. This ethnographic approach provided the trust needed to have access to the community for a social network analysis survey. In March 2014 the Makerere University study team conducted a social network census in the village of Dekabusa. Ego networks were obtained for 231 adults living in Dekabusa, which composes nearly the entire adult population. The estimated number of missing adults is about 10, maximally 20. Criteria for inclusion were that respondents were 18 years or older, have a residence in Dekabusa, or spend three or more days a week in the village. Although formal population data are lacking, other household surveys conducted as part of this project estimate that around 500 individuals, including children, comprise the entire population. Respondents were asked the main question: ‘to which five people would you go for health information?’ In our approach, we presumed that health communication is generic in its content and mode of diffusion. This may be a simplification, since health communication and its flow through social networks may be fundamentally different based on type of information sought: communicable disease prevention information might flow through one network while pregnancy related information through another. However, because asking directly about health may selectively probe for a certain response, and also because we wanted to know if health networks differed substantially from other types of social networks, respondents were in addition asked in more general terms about their social networks without explicitly mentioning health in order to compare and complement the health answers. These included: with whom they spend the most time, who their friends are, who they would call influential, and finally who had recently helped them. The answers to these questions created five different social networks emerging from the pertaining social contacts of residents in Dekabusa around the time of measurement, of which one network is specifically about health. We only included five contacts for each network because more contacts would not be needed considering our aim of uncovering the most important individuals. Although these important individuals themselves can only list five names, as everybody else, they can be mentioned by many more others as influential. Merluzzi and Burt (Citation2013) investigated this issue systematically and concluded that asking for five names is enough to assess informal power centrality, a measure of influentialness, which makes interviewing a great deal more feasible compared to asking for (many) more names. The consequence of this decision is that the average distance (hops through the network from one person to another) is somewhat overestimated, and in actuality is shorter due to the availability of ties that are not recorded in the data. Note that the social contacts to be listed were not restricted to others living within village boundaries (inclusion criteria) but included outsiders living in any other surrounding village or area but visited the area for three or more days per week. Based on this listing of the different ties by the 231 adult respondents, a network consisting of 715 people in total emerged, shown in shown below.
Figure 1. The overall network obtained by merging the five subnetworks together. The two white dots in the center are the two actors with highest power centrality.
Social network analysis was conducted using UCINET and igraph (an R package). To calculate the distribution of informal power-centrality, we used Bonacich’s well-known measure (Bonacich, Citation1987). Bonacich’ power-centrality measure is a refined way to measure someone’s influentialness because it acknowledges that on top of her direct influence, indicated by indegree, (s)he also has some influence on people one removed, i.e. at distance two. A focal actor’s power, or influentialness, thus not simply depends on how many people ask her for advice, but how many well-connected people ask for advice. How much less indirect contacts contribute to focal actors’ power is indicated by a parameter b < 1/λ, where λ is the largest eigenvalue of the adjacency matrix A (Bonacich, Citation1987). Longer paths than two are truncated, because influence then dilutes to insignificance (Luo et al., Citation2017; Pinheiro et al., Citation2014), and power centrality is defined accordingly as indegree plus weaker influence (b < 1) at distance two,(1)
(1) where AT
is the transpose of the adjacency matrix, 1 the unit vector, and cp a dimension-less measure that makes it possible to compare and rank order individuals’ power (cf. ). To detect clusters, the difference between actual within-cluster densities and expected densities in a randomised counterpart of the network (with the same degree distribution) was maximised, using the ‘Louvain’ algorithm (Blondel et al., Citation2008). Because social groups, or network clusters, form on the basis of lived social life, not according to researchers’ pre-determined categories, we here used all networks rather than one of the subnetworks, including non-residents who may co-determine clusters within Dekabusa.
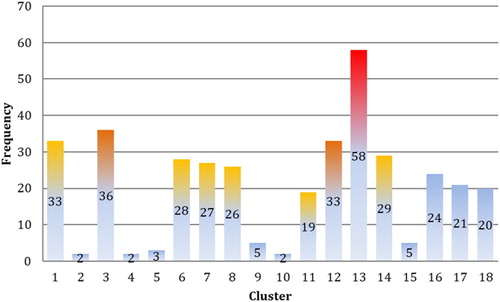
Figure 2. Numbers of respondents in the clusters of the health subnetwork (n = 373). The coloring of the tips of some of the bars reflects the presence of influential members.
Next to the use of the social network analysis, we also asked all respondents in the social network survey to list any local support groups they attended to in their community from which they received a lot of important advice. Groups can be big or small, formal or informal. In this way we received information about 55 self-identified groups, based on information from 140 of the 231 respondents, or 61% of surveyed respondents who self-identified with one or more groups to get important information, including health. The full list is provided in Appendix I. These self-identified groups were not used in the network analysis.
The qualitative data and observations made to contextualise the network analysis have been documented using qualitative analysis software (QSR Nvivo). Preliminary social network findings were discussed with the ethnographic team leading to the identification of the most influential individuals in the village and enabling contextualisation of the social network data using ethnographic information. An advantage of the combined useof these methods is the ability to check the validity and relevance of the social network data.
Results
A sparse, long-distance information network
During fieldwork, many residents at first noted that health information would come from health workers conducting checkups, this interpretation was quickly abandoned when we asked about public health issues, such as vaccination campaigns, sanitation or sexually transmitted diseases. For most residents, such information starts with close, trusted care individuals in the community. These are neighbours, friends, family who provide financial and health care support, and in case of illness spread information around in the village after they learn one of their close relationships is sick. One respondent said:
People talk about it in the community, you will hear them say, in so and so’s home there is measles. And sometimes the head of the home where measles is can come and tell you about it, someone can come and during the conversation you talk about it and they say, hmm, so and so’s child was visited by mukulu. Then you know that it’s measles … when you are there in the garden and meet, you can talk about it …
We evaluated how these ethnographic observations compare to the social network data. shows an overview of the network of 231 people living in Dekabusa plus their social contacts in other villages (in total, n = 715).
Socio-demographic characteristics of the respondents are shown in .
Table 1. Socio-demographic characteristics of the respondents.
The overall network is decomposed into five subnetworks: (1) giving health related information; (2) spending time with; (3) friendship; (4) giving important information; and, (5) providing help. These sub-networks are analysed separately below.
For information to be transmitted relatively fast and reliably, it is important that distances are short, else information gets distorted or lost or arrives late. The average distance can be calculated meaningfully if the network is a component (when everybody is (in)directly connected to everybody else); if it is split up in disconnected components or (sub)communities instead, the distance is by definition infinite, or undefined, and information from one component cannot be received from, or transmitted to, other components of the network. Only the network with all types of ties taken together forms one connected component, with an average distance of 4.61 steps, close to the distance in a randomised version of the network with the same density (0.0039) over a hundred simulations, where it is 4.22 on average. This is rather long, though: most information, with the exception of some spectacular rumours, travels no further than just a few steps. In the health advice network among the 231 adults in Dekabusa, the average distance is even 5.07. When looking at the distance from the eight most influential people (discussed below) to the remainder, however, it turns out that 216 out of 231 people can be reached at a distance of one or two steps. Hence the most central individuals are relatively close to the majority, and could in principle disseminate their health advice rapidly. This explains the paradoxical finding of the long average distance based on the network data and the interpretation that this means a relatively slow spread of information and the contradicting ethnographic observations suggesting a fast spreading of rumours.
Network clusters and self-identified groups
The apparent contradiction may be further resolved when realising that social life always clusters into groups. It is known that within groups, where people identify, and more easily share information, with one another and information flows through multiple channels, transmission tends to be fast and effective (Centola, Citation2010), yet this is less so across groups. It was therefore believed that overall information transmission would be slower in a clustered network than in randomised versions of it, where individuals would be connected to arbitrary others and average distance would be considerably shorter. In actuality such random networks without clusters do not exist, but when created for an experiment, transmission turned out to be slower than in clustered networks with longer average distance (Centola, Citation2010). This experimental finding complements the proximate central actors explanation of relatively fast information transmission in a clustered network with a large average distance, even though not everybody will be reached in actuality. In the health information network in and around Dekabusa, the community detection algorithm found 18 groups (modularity = 0.48). shows the distribution of respondents across the 18 different clusters based on health network data only, not on activities (that the algorithm is unaware of) or self-identification.
Of the five subnetworks constrained to residents of Dekabusa, each has a largest connected component, comprising the majority of inhabitants but leaving some disconnected, although everybody is embedded in, and ultimately connected by, the overall network. shows these numbers.
Table 2. Number of Dekabusa residents in largest component per subnetwork, and remainder number of people.
Next to the social network analysis, we also asked all respondents in the social network survey to list any local support groups they attended to in their community from which they received a lot of important advice. These groups can be big or small, formal or informal. In this way we received information about 55 self-identified groups, based on information from 140 of the 231 respondents, or 61% of surveyed respondents. The full list is provided in Supporting File 1. Analysis of the overlap between these 18 statistical clusters and the self-identified group membership showed that all groups other than the smallest had at least 25% of the members claiming membership to a specific village group, with the highest membership claims in clusters 3 (56%), 10 (50%), 13 (45%), 7 (44%) and 12 (42%).
In actuality, clustering can both increase information transmission, as in Centola’s (Citation2010) experiment, but can also impede it if some groups, for whatever reason, are reluctant to accept certain information from (some) other groups. Moreover, the actual influentialness of the most central individuals also depends on their legitimacy in the different village, gender and age groups. If C wants health advice from B and B from A, this does not imply that in all cases, C wants health advice from A. After all, transitivity is stochastic, not deterministic. To find out more about the groups and residents’ perceptions of the central individuals, the ethnography is important.
Power and influence in the village network
Health information is normally communicated through the typical community structures, with the Local Council (LC) chairman in a prominent position. As an informant told us:
It’s the chairman who came and told me. Some information I get from radio but radio doesn’t give us the news of the village. So for the village it’s usually the LC chairman. In some cases also I may be in a village meeting and they tell you that there is this and that going on please go, or that there is say people checking eyes, go and they check. They tell you the time and say that the doctors will be going to the hospital. So I get to know these things.
Those [VHTs] move around the villages telling people that they have to be clean, provide first aid to the people. For example they are given coartem to give to parents of children who may have malaria. These have played a big role in passing on information to our people.
And the people believe in them. Just like you see how the chairman mobilizes us to participate in research. If another person comes to mobilize them, people may be suspicious and create reasons not to be available. They may for example say that they are going somewhere. So the local leaders and the people share a mutual relationship. We honor them and they honor us.
With respect to Bonacich’ power-centrality measure for all five networks, b = 0.3, with the exception of the important information network where b = 0.4; this parameter says how strongly people at distance two are influenced compared to direct contacts, respectively 0.3 and 0.4 times.
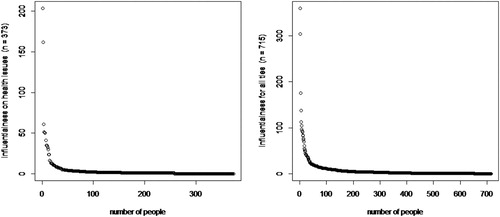
Figure 3. Distributions of power, based on the combined network data (top) and on the health network data (bottom).
Characterisation of the most influential actors
As there is a clustering into groups, those who broker between groups can be important, to be computed by betweenness centrality. Someone with high betweenness centrality stands in between many others who have no access to each other directly, and indirect access only (or mainly) through the broker. Again, this measure is truncated to distance two, which here means the distance from one of broker’s contacts through the broker to another contact (Bruggeman, Citation2016). This truncation is based on research on information transmission by Burt (Citation2010) and Aral and Van Alstyne (Citation2007). In the health network, the two brokers with much higher betweenness than the rest turn out to be also the two most influential people; see for the most influential people and for the entire distribution.
Table 3. The most central people in the health information network, limited to residents of Dekabusa.
Overall, the same two actors are at the top in all five networks. These two people hold unique administrative functions in the village, and their power centrality scores as well as their positions as brokers connecting groups makes them stand out above all the rest. The highest ranked person on the list (2034) has a high administrative position. He is consulted by all community members, young and old, for a range of issues including personal advice. He is generally good natured, loved and trusted. His high score by many concerning health information is somewhat puzzling as he is not seen as a role model in terms of home hygiene. This score is better explained by the observation that generally people make sure not to talk ill of him. The second highest person on the list (2058) also holds a high administrative position and is involved in local saving and burial groups. Her friendliness and leadership capabilities makes that she is indeed regularly approached by many for advice, particularly women and young men. She is a power broker and influential in social groups. She closely associated herself to our research team and the village health workers (VHTs).
The third to sixth in the list have nearly the same power centrality. The third (1019) is a local government official representing the parish at the sub-county leadership council; rich by all standards in the community and influencing many of the decisions of other local leaders. Our ethnographers note that many respect him and value what he says because of his position. The youngest on the short list (1020) is a community health worker. He owns a solar powered battery and a motor bike (bodaboda) which he uses as a taxi sometimes, which makes him crucial for emergency transport needs at night. He is well connected and his father’s home is where infant and child immunisation outreaches are hosted. He is quite sociable and caring and seen as one of the most respected individuals in the community. Moreover, he has also set up a video hall at his home now, which gives him more influence especially among the youths who frequent the video hall to watch local and western movies. The fifth on the list (2050) is a good friend of number two (2058) and is very active with almost everybody in the community. As she has a very friendly and social personality, she is seen as chit chatting with almost everybody. When it comes to health information, it seems that it is actually the sixth on the list (3059) who really has influence, particularly when health is seen to encompass spiritual and social-conflict situations. This elderly lady is a calm, composed woman with a very clean household and is respected by many in the community. She is for many an example of a person who does not have a quarrel with anyone, and therefore becomes a suitable person to mediate when two members of the community conflict on anything. She helps women with marital problems a lot and many couples look to her for advice.
The seventh person on the list (1029) is a retired mason who is highly respected and loved. He is very elderly and many people look to him for advice on almost all issues concerning daily life challenges in marriage and familial relations. He is slightly richer than many needy persons in the community and is seen as generous. He is a community health worker for Dekabusa and a friend of the LC chairman who consults him regularly. The next two in line have power centrality scores of 35, and the rest has so much lower scores than the top of the list that their influence is insignificant. Of these two with score 35, there is one with high brokerage (1021) who owns a local brew bar and is sociable with many people in the community. As she has aged, she is highly respected among men and women of younger age groups. She is a traditional birth attendant, and has helped many women and men with advice concerning management of pregnancy and also good at family counselling. Compared to her female age mates, she is relatively well-off and thus is seen as quite resourceful for needy neighbours and friends. Her local brew bar hosts a loose group of men who meet for a drink after farm work almost on a daily basis.
Although the people presented above are the most influential in the health network as a whole, this type of analysis might overlook the influence actors may have over certain demographic groups, such as age and education. shows the most influential people for elderly, youth, men and for women. Notice that here, influentialness is simply calculated by indegree, leaving out influence beyond direct contacts. The results show that there are no different group leaders for the different age groups and genders. The two most prominent positions are again, and in the same order, taken up by the two top administrators, 2034 and 2058.
Table 4. Centrality (indegree) for different sub-populations.
Finally, we looked at the overlap of the most influential people with cluster membership. From this it turns out that the top two most influential people both belong to the largest cluster (13, highlighted in hot red, see ), with further membership of the next three influential people in clusters 3 and 12 (in darker orange, ), while the rest of the most influential respondents spread over clusters 1,6,7,8, 11 and 14 (in lighter orange, ). As a result, all of the smaller clusters and the somewhat larger clusters 16, 17, and 18 are remote from the influence of the dominant group.
Discussion
The ethnographic data shows that in the largely non-literary community of Dekabusa, health information primarily flows through conversational networks, with at its core dyadic relationships between close, trusted community members. Entry points for external health information are specific information brokers who are trusted individuals. As one respondent said: ‘local people can’t bring me lies’. What is evident is that only few actors have high popularity, proximity, brokerage and power-centrality. This small group of people has a crucial health information role in the community health system. It includes the already mentioned top administrators (one merely powerful and another one also charismatic leader), two district health workers (a Parish representative and a regional community health worker leader), a conflict mediator, a natural helper and carer (and friend of the administrators), and two community health workers with different demographics (one aged and council to the chair, another young with emergency transportation options and a video hall).
The social network analysis further shows a relatively large average distance between actors. Most information, with the exception of some spectacular rumours, travels no further than just a few steps, and intimate or complex information rarely travels further than the single step from source to receiver. Although the two most influential people can reach many people directly, both of them are members of the same subgroup. Cleavages between subgroups may prevent health information to be transmitted from one group to another. Given weak extension services and a missing nearby health centre, a strong reliance on social network-based information spread by a small number of major influencers may leave some people uninformed. An additional complication is that tensions between certain personalities who hold key information and other community members may imply that some people will be excluded. Indeed, one informant noted about the community health worker: ‘But the one they appointed in our area … let me say if he has jealousy and misunderstanding with you, he does not come to you. So at times we do not get to know’.
Community cleavages and a skewed distribution of influentialness are not special for Dekabusa but are characteristic of many communities throughout the world. Based on our findings we therefore recommend that health communication outreach efforts first identify the local ‘team’ of the most influential actors – some of whom most likely have pre-existing links to formal or informal health systems – and support efforts of this group to work together. Because parts of the community beyond a cleavage may remain untouched by this core group, however, additional outreach efforts will have to be made. In other words, a community engagement strategy that only relies on the top influencers is not sufficient, particularly in the case of urgent health information needs, such as during an epidemic outbreak. This confirms observations made by Loutfi et al. (Citation2019) regarding rural populations in under-resourced settings on the need to diversify recruitment strategies.
Conclusion
In this paper we asked how health information diffused through a village community in rural Uganda using a combination of detailed ethnographic and social network data. The study confirms the importance of working with community members who are trusted (Todo et al., Citation2014). Ethnographic information suggests a relatively rapid spread of information, particularly rumours and gossip, but also health information. The latter is confirmed by social network analysis indicating the relatively high influentialness of the two most central players, with administrative roles, complemented by a small group of actors with a supportive role for the transmission of health information. This group of influencers taken together stands at a close distance to most residents. However, asking only the top influencers to distribute external health information means that a number of residents will not receive information in a timely manner, if at all. This is because the social partitioning in the village network leaves a number of people disconnected from the social clusters in which the top influencers are located. The network of relationships shown here, together with the ethnographic detail, are a unique source of data that may be compared with data from other areas to establish a general pattern representative of many similar rural and under-resourced environments.
Ethics
Institutional ethics clearance was received from Makerere University’s Higher Degrees Research and Ethics Committee (IRB00011353), the Uganda National Council for Science and Technology (SS2754) and the University of Amsterdam Institute for Social Science Research Ethical Advisory Board. No social network data including personal identifiers were at any time disclosed to the local community members. Informed consent was used throughout.
Supporting_information_1.docx
Download MS Word (25.7 KB)Acknowledgments
We acknowledge the people of Luwero who graciously provided their time and input during the period of study. We thank Marije de Groot for her general support to the CoHeRe project (https://www.nwo.nl/onderzoek-en-resultaten/onderzoeksprojecten/i/28/6128.html). We are grateful to the anonymous reviewer for valuable comments.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Adams, J. (2007). Religion networks and HIV/AIDS in rural Malawi (Dissertation/Thesis). http://rave.ohiolink.edu/etdc/view?acc_num=osu1179942482
- Adams, A. M., Madhavan, S., & Simon, D. (2006). Measuring social networks cross-culturally. Social Networks, 28(4), 363–376. https://doi.org/10.1016/j.socnet.2005.07.007
- Adams, A. M., Madhavan, S. F., & Simon, D. (2002). Women's social networks and child survival in Mali. Social Science & Medicine, 54(2), 165–178. https://doi.org/10.1016/S0277-9536(01)00017-X
- Alvergne, A., Gibson, M. A., Gurmu, E., Mace, R., & Bentley, R. A. (2011). Social transmission and the spread of modern contraception in rural Ethiopia. PLoS ONE, 6(7), Article e22515. https://doi.org/10.1371/journal.pone.0022515
- Aral, S., & Van Alstyne, M. W. (2007). Network structure and information advantage [Paper presented]. the Proceedings of the Academy of Management Conference, Philadelphia.
- Behrman, J. R., Kohler, H., & Watkins, S. C. (2002). Social networks and changes in contraceptive use over time: Evidence from a longitudinal study in rural Kenya. Demography, 39(4), 713–738. https://doi.org/10.1353/dem.2002.0033
- Blondel, V. D., Guillaume, J.-, Lambiotte, R., & Lefebvre, E. (2008). Fast unfolding of communities in large networks. Journal of Statistical Mechanics: Theory and Experiment, 10(P10008), 1–12. https://doi.org/10.1088/1742-5468/2008/10/P10008
- Bonacich, P. (1987). Power and centrality: A family of measures. American Journal of Sociology, 92(5), 1170–1182. https://doi.org/10.1086/228631
- Bruggeman, J. (2016). The strength of varying tie strength: Comment on Aral and Van Alstyne. American Journal of Sociology, 121(6), 1919–1930. https://doi.org/10.1086/686267
- Burt, R. S. (1987). Social contagion and innovation: Cohesion versus structural equivalence. American Journal of Sociology, 92(6), 1287–1335. https://doi.org/10.1086/228667
- Burt, R. S. (2010). Neighbor networks: Competitive advantage local and personal. Oxford University Press.
- Campbell, C., & Cornish, F. (2012). How can community health programmes build enabling environments for transformative communication? Experiences from India and South Africa. AIDS and Behavior, 16(4), 847–857. https://doi.org/10.1007/s10461-011-9966-2
- Centola, D. (2010). The spread of behavior in an online social network experiment. Science, 329(5996), 1194–1197. https://doi.org/10.1126/science.1185231
- Chami, G. F., Ahnert, S. E., Voors, M. J., & Kontoleon, A. A. (2014). Social network analysis predicts health behaviours and self-reported health in african villages. PLoS ONE [Electronic Resource], 9(7). Article e103500. https://doi.org/10.1371/journal.pone.0103500
- Clauset, A., Shalizi, C. R., & Newman, M. E. J. (2009). Power-law distributions in empirical data. SIAM Review, 512(4), 661–703. https://doi.org/10.1137/070710111
- De Vries, D. H., & Pool, R. (2017). The influence of community health resources on effectiveness and sustainability of community and lay health worker programs in lower-income countries: A systematic review. PLoS ONE, 12, 1. https://doi.org/10.1371/journal.pone.0170217
- de Vries, D. H., Rwemisisi, J. T., Musinguzi, L. K., Benoni, T. E., Muhangi, D., de Groot, M., Kaawa-Mafigiri, D., & Pool, R. (2016). The first mile: Community experience of outbreak control during an Ebola outbreak in Luwero district, Uganda. BMC Public Health, 16(1), 161. https://doi.org/10.1186/s12889-016-2852-0
- Dralega, C. A. (2008). Examining women's customary roles as sex educators through community media in Uganda. Agenda (durban, South Africa), 22(77), 91–99. https://doi.org/10.1080/10130950.2008.9674963
- Houston, V., & Hovorka, A. (2007). HIV/AIDS messages in Malawi and their implications for effective responses. African Journal of AIDS Research, 6(3), 205–214. https://doi.org/10.2989/16085900709490416
- Jacobs, B., Whitworth, J. F., Kambugu, F. F., & Pool, R. (2004). Sexually transmitted disease management in Uganda's private-for-profit formal and informal sector and compliance with treatment. Sexually Transmitted Diseases, 31(11), 650–654. https://doi.org/10.1097/01.olq.0000143087.08185.17
- Kiapi-Iwa, L., & Hart, G. J. (2004). The sexual and reproductive health of young people in Adjumani district, Uganda: Qualitative study of the role of formal, informal and traditional health providers. AIDS Care, 16(3), 339–347. https://doi.org/10.1080/09540120410001665349
- Kohler, H.-P., Watkins, S. C., Behrman, J. R., Anglewicz, P., Kohler, I. V., Thornton, R. L., Mkandawire, J., Honde, H., Hawara, A., Chilima, B., Bandawe, C., Mwapasa, V., Fleming, P., & Kalilani-Phiri, L. (2015). Cohort profile: The Malawi longitudinal study of families and health (MLSFH). International Journal of Epidemiology, 44(2), 394–404. https://doi.org/10.1093/ije/dyu049
- Konde-Lule, J., Gitta, S. N., Lindfors, A., Okuonzi, S., Onama, V. O. N., & Forsberg, B. C. (2010). Private and public health care in rural areas of Uganda. BMC International Health and Human Rights, 10(1), 29. https://doi.org/10.1186/1472-698X-10-29
- Kreuter, M. W., & McClure, S. M. (2004). The role of culture in health communication. Annual Review of Public Health, 25(1), 439–455. https://doi.org/10.1146/annurev.publhealth.25.101802.123000
- Loutfi, D., Andersson, N., Law, S., Salsberg, J., Haggerty, J., Kgakole, L., & Cockcroft, A. (2019). Can social network analysis help to include marginalised young women in structural support programmes in Botswana? A mixed methods study. International Journal for Equity in Health, 18(1), 12. https://doi.org/10.1186/s12939-019-0911-8
- Luo, S., Morone, F., Sarraute, C., Travizano, M., & Makse, H. A. (2017). Inferring personal economic status from social network location. Nature Communications, 8(1), 1–7. https://doi.org/10.1038/s41467-016-0009-6
- Matouš, P., Todo, Y., & Mojo, D. (2013). Roles of extension and ethno-religious networks in acceptance of resource-conserving agriculture among Ethiopian farmers. International Journal of Agricultural Sustainability, 11(4), 301–316. https://doi.org/10.1080/14735903.2012.751701
- Merluzzi, J., & Burt, R. S. (2013). How many names are enough? Identifying network effects with the least set of listed contacts. Social Networks, 35(3), 331–337. https://doi.org/10.1016/j.socnet.2013.03.004
- Mulawa, M., Yamanis, T. J., Hill, L. M., Balvanz, P., Kajula, L. J., & Maman, S. (2016). Evidence of social network influence on multiple HIV risk behaviors and normative beliefs among young Tanzanian men. Social Science & Medicine, 153, 35–43. https://doi.org/10.1016/j.socscimed.2016.02.002
- Musalia, J. M. (2005). Gender, social networks, and contraceptive use in Kenya. Sex Roles: A Journal of Research, 53(11-12), 835–846. https://doi.org/10.1007/s11199-005-8296-0
- Musinguzi, L. K. (2015). The role of social networks in savings groups: Insights from village savings and loan associations in Luwero, Uganda. Development Journal, 51(4), 499–516. bsv050.https://doi.org/10.1093/cdj/bsv050
- Muyinda, H., Nakuya, J., Whitworth, J. A., & Pool, R. (2004). Community sex education among adolescents in rural Uganda: Utilizing indigenous institutions. AIDS Care, 16(1), 69–79. https://doi.org/10.1080/09540120310001633985
- Perkins, J. M., Subramanian, S. V., & Christakis, N. A. (2015). Social networks and health: A systematic review of sociocentric network studies in low- and middle-income countries. Social Science & Medicine, 125, 60–78. https://doi.org/10.1016/j.socscimed.2014.08.019
- Pinheiro, F. L., Santos, M. D., Santos, F. C., & Pacheco, J. M. (2014). Origin of peer influence in social networks. Physical Review Letters, 112(9), Article 098702. https://doi.org/10.1103/PhysRevLett.112.098702
- Smith, K. P., & Christakis, N. A. (2008). Social networks and health. Annual Review of Sociology, 34(1), 405–429. https://doi.org/10.1146/annurev.soc.34.040507.134601
- Sood, S., Shefner-Rogers, C., & Skinner, J. (2014). Health communication campaigns in developing countries. Journal of Creative Communications, 9(1), 67–84. https://doi.org/10.1177/0973258613517440
- Sudhinaraset, M., Ingram, M., Lofthouse, H. K., & Montagu, D. (2013). Correction: What Is the role of informal Healthcare providers in Developing countries? A Systematic review. PLoS ONE, 8(9), https://doi.org/10.1371/annotation/93bc7847-5c4e-4b66-8923-500aa4fa4da5
- Todo, Y., Matous, P., & Mojo, D. (2014). Effects of social network structure on the diffusion and adoption of agricultural technology: Evidence from rural Ethiopia. Ssrn, https://doi.org/10.2139/ssrn.2447208
- Turinawe, E. B., Rwemisisi, J. T., Musinguzi, L. K., de Groot, M., Muhangi, D., de Vries, D. H., Mafigiri, D. K., & Pool, R. (2015). Selection and performance of village health teams (VHTs) in Uganda: Lessons from the natural helper model of health promotion. Human Resources for Health, 13(1), https://doi.org/10.1186/s12960-015-0074-7
- Twabeze, D. (2001). A literature review of care-seeking practices for major childhood illnesses in Uganda. United States Agency for International Development.
- Valente, T. W. (2012). Network interventions. Science, 337(6090), 49–53. https://doi.org/10.1126/science.1217330
- Ybarra, M. L., Bull, S., Prescott, T. L., & Birungi, R. (2014). Acceptability and feasibility of CyberSenga: An Internet-based HIV-prevention program for adolescents in Mbarara, Uganda. AIDS Care, 26(4), 441–447. https://doi.org/10.1080/09540121.2013.841837