
ABSTRACT
A range of research reports that many gender and sexually diverse people drink alcohol at heavy levels. This study used 24 focus groups to explore shared understandings of alcohol use among gender and sexually diverse people living in New Zealand. An inductive, data-driven thematic analysis was employed to identify explanations for heavy drinking among gender and sexually diverse people. Three key explanations were articulated: alcohol is needed for socialising; drinking helps coping with stress; alcohol and drug treatment services are inadequate. These results demonstrate justifications for heavy drinking in certain contexts. This behaviour runs counter to public health approaches and messages that highlight low-risk levels of drinking or not drinking as desirable. Public health interventions should continue to address alcohol use at a whole population level but should be supplemented by policy and interventions that take into account the sociocultural contexts and structural conditions that encourage drinking among gender and sexually diverse people.
Introduction
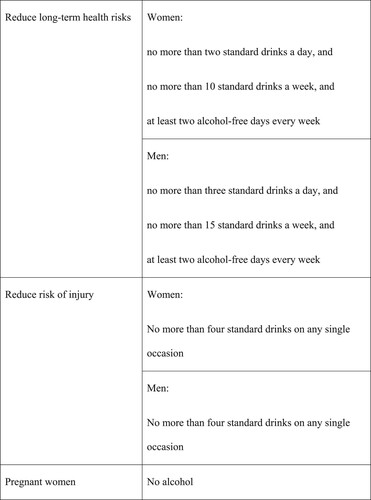
Alcohol use is a significant global public health issue. The dominant understanding is that the harmful effects of alcohol consumption contribute to a variety of health and social harms that are significant at the population level in many countries (Babor et al., Citation2010). However, these harmful effects are not shared equally within populations and some sub-groups that share characteristics experience more harm. Across the broad grouping of gender and sexually diverse people (including, but not limited to, those who identify as lesbian, gay, bisexual, or transgender) the heavy use of alcohol and the health and well-being impacts of its use has been advanced as an area of health disparity when compared with those who are cisgender and heterosexual (Australian Institute of Health and Welfare, Citation2020; Greenwood & Gruskin, Citation2007). While definitions of ‘heavy’ alcohol use vary across jurisdictions and across various studies, we use the term generically to signify alcohol consumption in excess of recommended guidelines designed to keep the health and injury risks from alcohol use low ().
Figure 1. Low-risk alcohol drinking advice – adapted from Te Hiringa Hauora/Health Promotion Agency of New Zealand (Citationn.d.) guidelines.
The global evidence-base relating to alcohol use among gender and sexually diverse people is limited due to the lack of disaggregation of these data by sexuality and the relative absence of research among transgender people. One impact of this is that differences between and within the gender and sexually diverse sub-groups are not always apparent. Nevertheless, a clear theme in the global research is that as a group sexually diverse people have higher rates of alcohol use and alcohol-related problems than are reported among heterosexual people (Australian Institute of Health and Welfare, Citation2020; Bloomfield et al., Citation2011; Bourne et al., Citation2017; Hughes et al., Citation2016; Schuler et al., Citation2020). However, while these broad claims are useful to highlight disparity, some of the differences within the broad grouping of gender and sexually diverse people remain hidden. A recent review of international studies concluded that while high levels of alcohol use are relatively similar among men irrespective of sexuality, higher levels of problematic alcohol use are much more common among sexual minority women than among heterosexual women (The Global Forum on MSM & HIV & OutRight Action International, Citation2017). While there is less comprehensive evidence about transgender people and drinking, some studies from the U.S.A. (Coulter et al., Citation2015) and Canada (Scheim et al., Citation2016) and an international review (Gilbert et al., Citation2018), report high levels of alcohol use including heavy episodic/binge drinking are common.
In contrast to the robust international literature, little is known about drinking among gender and sexually diverse adults in New Zealand. The most recently published data is from a national survey of over 13,000 respondents, which identifies lesbian, gay and bisexual (LGB) people as 2.2 times more likely than non-lesbian, gay and bisexual people to drink hazardously (AUDIT score of 8 or above) (Surace et al., Citation2019). This effect is driven by lesbian and bisexual women, who reported similar drinking patterns to males. No significant difference in hazardous drinking was found between gay/bisexual men and heterosexual men. Such findings are consistent with research from many countries (Boyd et al., Citation2019; Hughes et al., Citation2016). This national survey does not collect gender information beyond a female/male binary so information about gender diverse people is not available.
Data on alcohol use among young gender and sexually diverse people in New Zealand is available from a series of national surveys of secondary school students (within the age range of less than 13 years to 17 years or older) (Lucassen et al., Citation2014). Two key results have been reported. Firstly, among students reporting a sexual attraction to others, an elevated risk of alcohol use was evident for students who reported being same- or both-sex attracted compared with students who reported being opposite-sex attracted. Binge drinking (the consumption of five or more alcoholic drinks within four hours at least once in the last four weeks) was reported by 40.8% of same-sex/both-sex attracted students, compared with 23.1% of opposite-sex attracted students. Secondly, students who identified as transgender were two times more likely to drink alcohol at least weekly than non-transgender students (Clark et al., Citation2014).
In addition to prevalence data, a limited amount of qualitative research has explored the social contexts of drinking among gender and sexually diverse people to more fully understand practices, experiences and cultures of drinking. Drawing on a range of international studies about substance use among men who have sex among men Bourne and Weatherburn (Citation2017) propose three key ways to frame understandings of alcohol use among gender and sexually diverse people. First is the notion that drinking alcohol is normalised amongst gender and sexually diverse people (Condit et al., Citation2011) with bars being perceived as a safe place for meeting others and widely frequented (Lea et al., Citation2013; Schulman & Erickson-Schroth, Citation2017). This provides readily accessible opportunities for ‘risky’ and heavy drinking among gender and sexually diverse people (Bourne & Weatherburn, Citation2017). Secondly, heavy drinking has been identified as a response to the discrimination and marginalisation experienced by sexual and gender minority people. This is further amplified as stressors and mental health issues disproportionately experienced by gender and sexual minority people are also associated with alcohol use (McNair et al., Citation2016). Increased alcohol use has also been found among youth (14–21 years) in the U.S.A. in the process of ‘coming out’ or making their diverse gender and sexual identity known to others (Rosario et al., Citation2004). The third area is drinking alcohol for pleasure. Alcohol is often discussed as having disinhibiting effects and these effects are generally understood to be positive for individuals. For example, alcohol has been used by Black and Latino men who have sex with men in the U.S.A. to increase comfort with their sexuality and sexual desires (Mutchler et al., Citation2014). Also in this vein, gender and sexual diverse people in Scotland are reported to use alcohol and ways of drinking as a means of constructing and portraying a desired identity (Emslie et al., Citation2017a).
These quantitative and qualitative data clearly suggest that public health intervention is warranted to reduce high rates of drinking and minimise harm from alcohol use. While a number of ‘best buy’ policies and actions to counter alcohol-related harm have been developed (Chisholm et al., Citation2018), initiating action to address alcohol use and related harm remains contentious globally and within New Zealand (Casswell & Rehm, Citation2020). Governments and other agencies apply such initiatives variably reflecting local political, social and economic conditions. Typical actions that have been employed have included controlling affordability and access to alcohol through measures such as taxation and trading hours, restricting alcohol marketing, and drink driving legislation (Babor et al., Citation2010). In addition, in a number of jurisdictions, including New Zealand, guidelines have been developed by health promotion agencies to support people to make sensible decisions about drinking alcohol through promoting low-risk drinking (or non-drinking) (Te Hiringa Hauora/Health Promotion Agency of New Zealand, Citationn.d.).
Against this backdrop of varied public health interventions and commitment to reducing harm, data from many countries, including New Zealand, demonstrate alcohol continues to be consumed by gender and sexually diverse people at rates that contribute to individual and community harm. Given this, our study, among a community sample of gender and sexually diverse people, sought to identify shared information and understandings and explanations for heavy drinking within the broad gender and sexually diverse community. These findings are intended to provide information to inform and support appropriate public health and health promotion responses.
Materials and methods
The study setting
New Zealand is an island country in the southwest Pacific comprising five million people. The population is ethnically diverse. While Māori were the original inhabitants, the initial migrants to New Zealand beginning from the 1800s have overwhelmingly been from Britain. However, the range of origin countries has widened significantly over time and includes significant numbers of people from Asian and Pacific countries (Butcher et al., Citation2015). New Zealand has an open economy, characterised by minimal regulation. Consistent with this are concerns to prioritise individual choice and limit government involvement (Lyons & Kersey, Citation2020), which has contributed to the development of a relatively liberal drinking environment (Ball et al., Citation2020; Randerson et al., Citation2018). This has included the lowering of the minimum purchase age for alcohol in 1999 from 20 to 18 years, increased opportunities for mainstream media promotion of alcohol, and ‘relaxed conditions for obtaining a licence to sell alcohol, along with the sale of wine being allowed in supermarkets and grocery outlets’ (Huckle et al., Citation2006, p. 232). New Zealand’s consumption of pure alcohol per person (10.7 L) is similar to Australia (10.6 L), less than the U.K. (11.5 L), and more than the U.S.A. (9.8 L) and Canada (8.9 L) (Health Promotion Agency, Citation2019a).
New Zealand is regarded as relatively accepting of gender and sexually diverse people (Treharne & Adams, Citation2017). Various rights are protected by legislation, and same-sex marriage has been legal since 2013. Nevertheless, health and wellbeing inequities persist for gender and sexually diverse people (Health Promotion Agency, Citation2019b; Pihama et al., Citation2020; Surace et al., Citation2019; Tan et al., Citation2020).
Design
The research was informed by a critical realist position that theorises people’s accounts as constructed, yet at the same time accepts them as descriptions of events and personal experiences that have some basis/meaning in reality (Willig, Citation2013). It provided a way to recognise notions (including events and personal experiences such as drinking practices) exist, but that they can only be known as socially constructed entities. A qualitative design with focus groups and thematic analysis was used. Focus groups provide an environment for open discussion among participants, and are an excellent method for obtaining shared cultural information and understandings (Braun & Clarke, Citation2013).
Recruitment
Recruitment was designed to attract a broad range of gender and sexually diverse participants living in New Zealand. To obtain the views held about drinking among people in this group, anyone 16 years and over, drinker or non-drinker, and who identified as gender and/or sexually diverse was eligible to take part. The focus groups were organised by people linked to at least one gender and sexually diverse community. These people were typically leaders of existing community groups or had strong professional or social networks within these communities. These organisers recruited people to take part in a group they hosted. They used a variety of recruitment strategies appropriate for their situation. These included posts on Facebook pages, notices in newsletters, announcements at meetings; as well as face-to-face, email and telephone contact with people they knew. Participants and the organisers received a small monetary gift for taking part and/or organising a group.
Data collection and analysis
A total of 24 focus groups were held in six cities across New Zealand. Nearly all (92%) of the 131 participants had drunk alcohol in the previous year. In the four weeks prior to the focus groups, around three quarters (77%) had drunk alcohol and two in five had drunk 7+ drinks on at least one occasion in that period (). Additionally, less than half (44%) of the participants had purchased alcohol for themselves or others in a bar or club in these four-weeks.
Table 1. Participant demographics.
Groups ranged in size from two to nine participants (mean size five participants). Most of the groups had a specific focus on a particular gender and sexually diverse grouping (). The majority of the groups were moderated by one of the authors (all of whom identify as sexually diverse). A few groups were moderated by colleagues who were chosen due to their sexually diverse identity, or because their ethnic identity matched that of group members. Moderators, therefore, had some affiliation with participants due to ‘insider’ status because of a shared sexual and/or ethnic identity but were also ‘outsiders’ as academics in a research role. Moderators were careful to not to make assumptions based on their own knowledge during the focus groups and acted as much as possible as naïve questioners guiding discussion.
Table 2. Focus group participant characteristics.
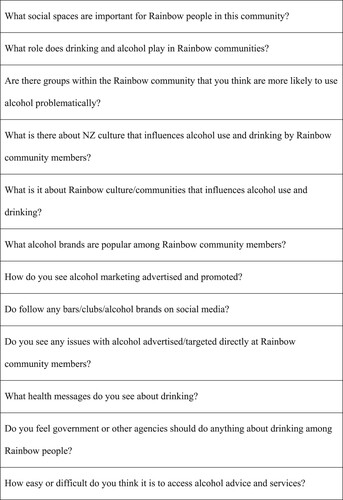
Focus groups ranged in length from 35 minutes to 2 hours (median length 1 hour 14 minutes). A guide for moderators was used to ensure a similar range of topics was covered in the groups (). To identify shared understandings the moderators encouraged discussion and debate in the groups, therefore, not every person answered each question or spoke about every topic raised. All group discussions were recorded and transcribed.
Figure 2. Focus group moderator guide.
Thematic analysis was used to identify patterns of shared meaning across the focus groups (Braun et al., Citation2019). The thematic analytic approach was inductive and data-driven, focusing initially on the semantic content, and then the latent constructs underpinning this content. The analysis was initially led by the first two authors. The process involved them reading the transcripts and coding the entire transcripts within NVivo. These two authors then met and identified and agreed on provisional themes. All authors then reviewed and discussed these themes, before further refinement and development of the themes was undertaken by the first author. The authors brought to the research and analysis processes their ‘affiliation’ to a sexually diverse community, as well as extensive experience of research within these communities. In addition to this, the results of the study were reported back at community meetings which included focus group participants and non-participants. This processes provided further insight and helped refine the researchers’ understandings and analysis. All authors subsequently reviewed and agreed upon the final themes reported and the illustrative quotes selected.
The project was conducted under Massey University research and ethical procedures. In line with this, the research was assessed by peer review to be low risk. Consequently, it was not reviewed by one of the university’s human ethics committees, and the research team (authors of this article) were responsible for the ethical conduct of the research. Full written information about the study (including contact details for alcohol and other support services) was provided to all participants. A written consent form was completed by all participants.
Results
Across the groups, there was considerable debate about what constitutes problem drinking and resistance to always labelling periodic heavy drinking/binge drinking as problematic. This article reports on participants’ accounts of when heavy drinking is considered ‘justified’. Three key explanations for heavy drinking were articulated: alcohol is needed for socialising; drinking helps coping with stress; and alcohol and drug treatment services are inadequate.
Alcohol is needed for socialising
Drinking alcohol was discussed as being at the core of social activities both within society at large, and within specific settings used by gender and sexually diverse people. The predominant view was that alcohol drinking is a norm within the general community and within gender and sexually diverse communities, and to not drink in social settings would be out of place. However, beyond this general view, the increased importance of alcohol in gender and sexually diverse social contexts was raised. Drinking alcohol was regarded as necessary in order to meet other gender and sexually diverse people and making connections was reported as being much more difficult without it. Alcohol used in these ways was portrayed as a social lubricant that provided people with the courage to mix and socialise.
If you’re going to any social situations where groups of people know each other alcohol gives you the courage to go out and talk to, break the ice and talk to people. (Mid-age/older age gay men group)
An additional element for gender and sexually diverse people reported by participants was the difficulty in determining another person’s sexuality or gender before approaching them in social situations. Being ‘under the influence’ of alcohol was described as one way of bolstering confidence to approach others when the outcome was not certain and could, for example, result in physical rebuke.
So you’ve got to have a couple of drinks to kind of pluck up the courage to maybe get knocked back, or punched. (Mixed/social group)
Alcohol use and being drunk (or pretending to be) was also viewed as a mechanism to facilitate social and sexual experimentation and as an easy way to brush-off behaviour if the recipient felt it inappropriate.
I think that excuse, it’s a show, a cover up. It’s like, ‘oh sorry I was drunk I didn’t know what I was doing. It’s the alcohol’. And then the classic, ‘I can’t remember a thing’. (Mid-age/older age gay men group)
Participants’ descriptions of the places where socialising occurred for gender and sexual diverse people reinforced the ongoing role of gay bars and clubs as an important central meeting and socialising places. A few participants noted that in recent years commercial venues had become more accessible to some groups including transgender and takatāpui, who had previously been excluded.
Socialising in the actual gay club environment is a new phenomenon. Because we were actually ostracised from that and a lot of the times a lot of our sisters couldn’t get into places and they were actually kept out of those clubs, couldn’t get in the door. (Māori/Takatāpui group)
For several participants bars and clubs offered a place to be anonymous if required, and one of the few safe public spaces for meeting others and relaxing. Opportunities for safety and anonymity for many participants were much more likely to be in a ‘gay’ bar or club, and much less likely in mainstream bars and clubs.
I still only feel comfortable in gay bars but that’s because I am transgender. If anything happens in the bathroom in a straight bar it’s gonna be a lot worse than anything at a gay bar. (Gender diverse group)
Drinking helps coping with stress
Drinking alcohol was identified as a key way to cope with exclusion, stigma and distress. These stressors were typically viewed as being outside a gender and sexually diverse person’s individual control, although their effects are felt by individuals. For transgender participants, this stress was reported to be more amplified than for lesbian, gay and bisexual people, and for some included being the victim of physical violence.
I think just the sense of isolation, and disapproval from society, potentially from people’s families, communities, accounts for a lot. And while we have witnessed that change for gay people, I just think it [isolation, disapproval etc.] is still very acute for transgender people. (Mixed/social group)
The (heavy) use of alcohol was viewed as a socially accepted way to deal with stressful experiences and issues arising from oppression, exclusion and isolation. It was quite clearly expressed that gender and sexually diverse people experience negative stressors that are not felt by cisgender and heterosexual people. Further, it was noted some gender and sexual people hold expectations of experiencing negative stressors, and use alcohol to cope. Because such expectations are held, it was argued these negative stressors were more likely to be experienced – in other words, a self-fulfilling prophecy. In one group, the notion of gender and sexually diverse people having to ‘come out’ through the public identification of their sexual or gender identities was noted as a particular burden and stress. A participant noted remaining in the ‘closet’ was safe as no public declarations were required. Similarly, drinking to cope with issues was reported as being a safe strategy in that public declarations about identity could be avoided.
The very fact that we have to, or we’re expected to [deal with coming out], adds another burden to us and the closet that’s still a safe place for many, and a bottle is the safe closet. A bottle is another closet. (Mixed/social group)
In several groups, there was discussion of how high rates of mental health issues are experienced by gender and sexually diverse people. When this was discussed a strong relationship between alcohol use and mental health was claimed. This was identified primarily as drinking being used to deal with depression. It was also noted that the impact of this varies across various sub-groupings, with transgender people more likely to be impacted.
I think gay is a lot more okay than all the other the subsets [of gender and sexually diverse people] or whatever. I think as you go down the line, you know, that transgender … is more of a minority group, and they might have a higher depression rate, or higher suicide rate, or whatever. So that affects drinking and drinking is quite prevalent in groups that deal with depression and things like that. (Mixed/social group)
In instances such as this, a direct link between alcohol consumption and distress was noted. Excessive consumption and using alcohol to self-medicate were viewed as understandable and a rational practice as people looked for strategies to cope with life challenges.
It’s like self-medicating. Yeah, I think that’s interesting. It’s interesting because in some ways any kind of self-medication can be a positive thing, because it’s a thing people use for survival. (Gender diverse group)
Several participants cautioned that across the various sub-groups within the gender and sexually diverse communities, experiences of distress are likely to vary and be experienced in different ways. Further, not all people will use alcohol as a way of coping with distress and the drivers for alcohol use may not be gender or sexuality related.
People I know of who’ve struggled with alcohol are really presumed to say it’s because of their sexuality. You know I wouldn’t make that link because that’s not mine to make. If there are, if it is an issue for them, then fine. But I wouldn’t assume that anyone I knew who is gay and has an alcohol problem that those things go hand in hand. (Mixed/social group)
Alcohol and drug services are inadequate
Access to appropriate alcohol and drug services was identified as challenging. Only one service focused on gender and sexually diverse people was identified, meaning many genders and sexually diverse people would need to use mainstream alcohol and drug services. Participants believed they should be treated with dignity when attending mainstream services. Alcohol and drug services with religious (e.g. Salvation Army) or spiritual connections (e.g. Alcoholics Anonymous) were discussed as often being inappropriate, due to many gender and sexually diverse people having had negative previous experiences of faith-based services and churches more broadly.
You’re not gonna go and talk about how you have a drinking problem because you’re first scared of being trans while you’re surrounded by like highly Christians who are not okay with it. It’s like half of why I stopped going to Alcoholics Anonymous. (Mixed/social group)
In addition, existing capacity within mainstream alcohol and drug services was understood by participants to be lacking, with services being difficult to access. Access was discussed as only being readily available for those with the most severe needs.
You have to be really rock bottom and rotten really, your life. Your life has to be completely fucked in several ways. You know, to get into it. The only other way is if you got shitloads of money. (Mid-age/older age gay men group)
Having services staffed by practitioners known to provide culturally competent care was viewed as critical, as their presence would likely signal a service was safe to use. However, it was noted that services like this were rare and difficult to find in New Zealand, meaning mainstream services which may not offer culturally competent services were often the only option.
It’s like, you don’t know they’re safe … any of those organisations out there, like Alcoholics Anonymous and whatever else, if we don’t know that the gay community go to them, we’re not gonna use them. We don’t know if they’re safe. (Mixed/social group)
Participants recognised the diversity across the gender and sexually diverse communities and that some may have unique needs and require specific services and support. Because of the limited capacity of existing services and desire of many people to maintain privacy, there was strong support for the provision of online services.
A lot of people in Rainbow [an alternate term for gender and sexually diverse people] communities might not feel comfortable going to a physical support group or a service … and that anonymous thing too because that’s another big thing for people in queer communities. (School student/youth focused group)
A challenge identified by participants was the need for those planning alcohol health promotion and treatment services to understand the reasons for drinking among gender and sexually diverse people, and to address these rather than focusing on drinking behaviours in isolation. In several groups, heavy drinking of alcohol was not necessarily viewed as an issue or a problem; rather the reasons for drinking were viewed as an issue that needed to be addressed. In many instances these underlying concerns were regarded as complex, relating to the stress caused by the difficulties and negative experiences arising in people’s lives.
I think that the bigger issue is, why are people drinking to excess … and it’s addressing that reason, not looking at someone to blame and then ban that … it’s actually finding the cause where the problem is, not just putting it all on alcohol. (Mid/older age gay male group)
Given these immense challenges in service provision, many people had low expectations of what help might be available and how effective it might be. This was conceptualised quite clearly by participants as a valid reason to justify alcohol use. Alcohol being used to self-medicate was characterised as therapeutic and justified. However, although seen as an entirely reasonable response, the underlying system failures that lead to such practices were seen as unacceptable.
If they’re not able to access the inclusive mental health treatment that they need or aren’t being supported in other ways and their alcohol or drug use or other things are helping them survive, then that’s good on some weird kind of fucked level. It’s better than not, not having that support. So in some ways it’s those things that need to change, like our mental health systems, to reduce those problems. (Mixed/social group)
Discussion
Alcohol is a part of the lives of most gender and sexually diverse people, and for some, the amount and pattern of drinking alcohol is heavier than for cisgender and heterosexual people. Our research has identified justifications advanced by gender and sexually diverse people living in New Zealand that demonstrate support for heavy use of alcohol in certain contexts and as such run counter to public health approaches and messages that highlight low-risk levels of drinking or not drinking as desirable. In these instances, the narrative that heavy drinking is always ‘irresponsible’ was actively challenged. Such findings are useful to inform public health responses.
A novel finding in this research was the layers of complexity involved for gender and sexual minority people when they sought to make connections with others in social settings. Heavy alcohol use to negotiate the complexity within these settings was viewed as essential. In line with international research, bars and other commercial venues selling alcohol were identified as important places for socialising (Croff et al., Citation2017; Emslie et al., Citation2017b), as was the role of peer expectations in encouraging drinking (Longerbeam et al., Citation2007; McKie et al., Citation2020; Morris et al., Citation2020; Robertson & Tustin, Citation2018). Additionally in the New Zealand context, there was recognition that non-alcohol venues and opportunities for socialising are not readily available for gender and sexually diverse people, something that has been reported elsewhere (Adams, McCreanor, et al., Citation2007).
Alcohol use to counter the effects of social stigma, marginalisation and discrimination due to being gender and sexually diverse was justified by participants. The negative mental health impacts resulting from these factors are well documented among gender and sexually diverse people in New Zealand (Fergusson et al., Citation1999, Citation2005; Pihama et al., Citation2020; Tan et al., Citation2020; Treharne et al., Citation2020; Veale et al., Citation2019) and international research evidence has also linked sexual orientation discrimination with problematic drinking of alcohol (Crane et al., Citation2020; Gilbert & Zemore, Citation2016; Slater et al., Citation2017). The participants identified that often external factors rather than the person’s diverse gender or sexual identity were likely to be the underlying cause of heavy drinking. This finding is consistent with the model of minority stress which explains that a variety of external stressors contribute to poorer mental health among gender and sexually diverse people (Meyer, Citation2003). Coping processes of individuals can sometimes mitigate the effects of this, but poor coping processes may also compound the impact of the minority stress. It is also consistent with stigma arising from relationships between stigmatised and non-stigmatised people (interpersonal stigma), and societal-level conditions that impact on the wellbeing of the stigmatised person (structural stigma) (Hatzenbuehler, Citation2016). In such instances, the use of alcohol to self-medicate was identified by participants as a necessary practice employed by many gender and sexually diverse people to cope with varied stressors experienced by them. This local finding is consistent with other research that associates sexual orientation-based discrimination with exceeding recommended weekly drinking limits (Slater et al., Citation2017).
The limited availably of culturally safe alcohol treatment services that were welcoming of gender and sexually diverse people was identified by participants as a key local issue. Several participants recounted their negative personal experiences of accessing these services. Without sufficient and ready access to quality services, using alcohol to self-medicate was supported by participants as an entirely reasonable action among individual drinkers. This finding adds to the local literature that has reported ongoing challenges for gender and sexually diverse people with accessing appropriate health care services (New Zealand Human Rights Commission, Citation2020; Veale et al., Citation2019).
The drinking norms of gender and sexually diverse people in New Zealand need to be viewed within the context of the country’s drinking culture and norms which are shaped by a relatively liberal drinking environment (Ball et al., Citation2020). These results quite clearly suggest that public health and health promotion interventions are required if shifts in drinking cultures among gender and sexually diverse people are to be made to allow opportunities for better relationships with alcohol. Broadly speaking, this means that interventions aimed at the general population should continue, and be extended to focus on key public health priorities including actions such as increasing taxes to reduce affordability, regulating marketing and sponsorship, and strengthening drink driving countermeasures (Health Coalition Aotearoa, Citation2020). These actions from governments and public health agencies have not been as stringent in developing interventions for alcohol as for tobacco use, in part because the alcohol industry has considerable influence in the policy-making process in many countries and globally (Hawkins et al., Citation2018). However, lessons from tobacco control suggest that governments can build and maintain support to implement progressive policy and effective public health measures (Crosbie et al., Citation2018).
Recent evidence suggests that stronger alcohol policy environments may not always contribute to reduced alcohol-related harm for gender and sexually diverse people (Greene et al., Citation2021). It follows that general population initiatives would be usefully supplemented with interventions targeted at gender and sexually-diverse people. Such an approach will recognise the social realities and social identities of gender and sexually diverse people (Phillips et al., Citation2016) and should look to ways of working with, and supporting these communities to identify ways to enhance health and well-being. This research supports actions such as government and other agencies working with gender and sexually diverse communities to develop services that meet the diversity of needs across these communities, and also to provide spaces and venues that are alcohol-free. This may need to include providing funding for organisations so they are not reliant on support from the commercial alcohol sector (Adams, McCreanor, et al., Citation2007). Additionally, work to restrict alcohol companies from targeting gender and sexually diverse communities may be warranted. Given the strong reasons for heavy drinking articulated by participants, which run counter to low-risk drinking advice, new and appropriate ways to communicate this information to gender and sexually diverse communities are required. These should be co-developed with these communities.
Addressing discrimination and exclusion for gender and sexually diverse people is key as they both impact alcohol use. While minority stress theory focuses on the negative impacts of discrimination on individuals, public health and health promotion actions should look upstream to take account of the impacts of social norms and institutions (Riggs & Treharne, Citation2016). This means that responses to address the causes of discrimination experienced by gender and sexually diverse people are required. Initiatives aimed at gender and sexually diverse people must take account of the specific impacts of stigma, discrimination and exclusion and how these contribute to hazardous drinking among gender and sexually diverse people. Mental health and addictions policy and services need to specifically respond to the needs of gender and sexually diverse people.
Public health and health promotion agencies need to authentically include and represent gender and sexually diverse people in mainstream alcohol health promotion campaigns. In addition, agencies need to investigate and develop appropriate alcohol health responses targeted to gender and sexually diverse specific communities. Such responses will need to recognise the social realities and social identities of the groups being targeted (Phillips et al., Citation2016). An example of a successful response is a campaign in Victoria, Australia focusing on alcohol use within lesbian communities (Vic Health, Citation2018). In addition, consideration could be given to minority-stress focused treatments in the community which have been found to be effective in reducing alcohol use (Pachankis et al., Citation2015, Citation2020).
Many improvements are also required within existing alcohol treatment services. While a specialist alcohol and drug service for gender and sexually diverse is available in Auckland (New Zealand’s largest city), its reach and capacity are limited. Realistically, it is most likely mainstream treatment services will be available and used by most individual gender and sexually diverse drinkers seeking help. Additionally, it should be recognised that gender and sexually diverse people will not always seek to link their health and wellbeing issues to these identities and many are more likely to seek help from mainstream health and support services rather than those focused on gender and sexually diverse people (Adams et al., Citation2012). For this reason, building skills in health professionals to act in a culturally responsive way to support all individuals appropriately is necessary (Blakey et al., Citation2019; Saxton et al., Citation2017). Support for health and social service organisations to enable this to happen is crucial. In areas of high demand, gender and sexually-diverse targeted treatment options may be warranted. The absence of culturally appropriate treatment services may potentially result in gender and sexually-diverse people not seeking professional help and over-reliance on self-medication options (Pedersen et al., Citation2020).
Limitations
As with all research, there are limitations with this study. The focus groups were organised by community members and researchers had limited control over who participated. To ensure a wide range of participants, a variety of gender and sexually diverse people were used as organisers. Nonetheless, some gaps were apparent. Lesbian, bisexual, and gender diverse participants were less well represented, as were those living rurally. It is also very unlikely that people not connected with other gender and sexually diverse people or affiliated with a gender and sexually diverse focused community group would have taken part. In addition, it is possible the presence of the organiser in the group may have compromised the full expression of views by some participants.
Conclusion
Government policy interest in health and wellbeing issues for gender and sexually diverse people in New Zealand has been uneven for some time (Adams, Braun, et al., Citation2007). This commissioned research offered an opportunity to investigate and present issues to a government agency for policy consideration. The research results suggest that drinking alcohol, and risky drinking, are influenced by a range of individual, community and societal factors. Heavy drinking among gender and sexually diverse people was conceptualised, in some instances, by participants in a positive way – as a way to counter challenges in life. Despite this, we suggest that action to reduce the impact of these challenges is warranted. This requires the implementation of public health and health promotion interventions that focus on addressing sociocultural contexts and structural conditions that promote drinking by gender and sexually diverse individuals and groups. These interventions should also include those that explore ways to reduce minority stress, and in doing so reduce triggers for heavy drinking by gender and sexually diverse people.
Acknowledgements
The authors offer thanks to the members of various gender and sexually diverse communities who took part in this research and offer special thanks to those who organised the focus groups. We acknowledge colleagues (Dr Teah Carlson, Dr Belinda Borell, Jitesh Prasad, Rommel Coquilla) who assisted with focus group moderation. Dr Asiasiga contributed this project while at Massey University; she is now an independent researcher. The views expressed here are those of the authors and not Te Hiringa Hauora.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Adams, J., Braun, V., & McCreanor, T. (2007). Warning voices in a policy vacuum: Professional accounts of gay men’s health in Aotearoa New Zealand. Social Policy Journal of New Zealand, 30, 199–215.
- Adams, J., Braun, V., & McCreanor, T. (2012). Gay men talking about health: Are sexuality and health interlinked? American Journal of Men’s Health, 6(3), 182–193. https://doi.org/10.1177/1557988311421980
- Adams, J., McCreanor, T., & Braun, V. (2007). Alcohol and gay men: Consumption, promotion and policy responses. In V. Clarke, & E. Peel (Eds.), Out in psychology: Lesbian, gay, bisexual, trans and queer perspectives (pp. 369–390). John Wiley & Sons.
- Australian Institute of Health and Welfare. (2020). National drug strategy household survey 2019.
- Babor, T., Caetano, R., Casswell, S., Edwards, G., Giesbrecht, N., Graham, K., Grube, J., Hill, L., Holder, H., Homel, R., Livingston, M., Osterberg, E., Rehm, J., Room, R., & Rossow, I. (2010). Alcohol: No ordinary commodity. Oxford University Press.
- Ball, J., Edwards, R., Sim, D., Cook, H., & Denny, S. (2020). What explains the decline in adolescent binge-drinking in New Zealand? International Journal of Drug Policy, 84, 102826. https://doi.org/10.1016/j.drugpo.2020.102826
- Blakey, G., & Treharne, A., & J, G. (2019). Overcoming barriers to transgender healthcare education in Aotearoa New Zealand. New Zealand Journal of Educational Studies, 54(2), 357–366. https://doi.org/10.1007/s40841-019-00143-2
- Bloomfield, K., Wicki, M., Wilsnack, S., Hughes, T., & Gmel, G. (2011). International differences in alcohol use according to sexual orientation. Substance Abuse, 32(4), 210–219. https://doi.org/10.1080/08897077.2011.598404
- Bourne, A., Davey, C., Hickson, F., Reid, D., & Weatherburn, P. (2017). Physical health inequalities among gay and bisexual men in England: A large community-based cross-sectional survey. Journal of Public Health, 39(2), 290–296. https://doi.org/10.1093/pubmed/fdw029
- Bourne, A., & Weatherburn, P. (2017). Substance use among men who have sex with men: Patterns, motivations, impacts and intervention development need. Sexually Transmitted Infections, 93(5), 342–346. https://doi.org/10.1136/sextrans-2016-052674
- Boyd, C. J., Veliz, P. T., Stephenson, R., Hughes, T. L., & McCabe, S. E. (2019). Severity of alcohol, tobacco, and drug use disorders among sexual minority individuals and their “not sure” counterparts. LGBT Health, 6(1), 15–22. https://doi.org/10.1089/lgbt.2018.0122
- Braun, V., & Clarke, V. (2013). Successful qualitative research: A practical guide for beginners. SAGE.
- Braun, V., Clarke, V., Terry, G., & Hayfield, N. (2019). Thematic analysis. In P. Liamputtong (Ed.), Handbook of research methods in health and social sciences (pp. 843–860). Springer.
- Butcher, A., Spoonley, P., & Gendall, P. (2015). New Zealanders’ attitudes to Asia and Asian peoples: An exceptional case? Political Science, 67(1), 38–55. https://doi.org/10.1177/0032318715585032
- Casswell, S., & Rehm, J. (2020). Reduction in global alcohol-attributable harm unlikely after setback at WHO Executive Board. The Lancet, 395(10229), 1020–1021. https://doi.org/10.1016/S0140-6736(20)30476-1
- Chisholm, D., Moro, D., Bertram, M., Pretorius, C., Gmel, G., Shield, K., & Jürgen, R. (2018). Are the “best buys” for alcohol control still valid? An update on the comparative cost-effectiveness of alcohol control strategies at the global level. Journal of Studies on Alcohol and Drugs, 79(4), 514–522. https://doi.org/10.15288/jsad.2018.79.514
- Clark, T. C., Lucassen, M. F. G., Bullen, P., Denny, S. J., Fleming, T. M., Robinson, E. M., & Rossen, F. V. (2014). The health and well-being of transgender high school students: Results from the New Zealand Adolescent Health Survey (Youth’12). Journal of Adolescent Health, 55(1), 93–99. https://doi.org/10.1016/j.jadohealth.2013.11.008
- Condit, M., Kitaji, K., Drabble, L., & Trocki, K. (2011). Sexual-minority women and alcohol: Intersections between drinking, relational contexts, stress, and coping. Journal of Gay & Lesbian Social Services, 23(3), 351–375. https://doi.org/10.1080/10538720.2011.588930
- Coulter, R. W. S., Blosnich, J. R., Bukowski, L. A., Herrick, A. L., Siconolfi, D. E., & Stall, R. D. (2015). Differences in alcohol use and alcohol-related problems between transgender- and nontransgender-identified young adults. Drug and Alcohol Dependence, 154, 251–259. https://doi.org/10.1016/j.drugalcdep.2015.07.006
- Crane, P. R., Swaringen, K. S., Foster, A. M., & Talley, A. E. (2020). Alcohol use disorders among sexual and gender minority populations. In E. D. Rothblum (Ed.), The Oxford handbook of sexual and gender minority mental health (pp. 87–111). Oxford University Press.
- Croff, J. M., Hubach, R. D., Currin, J. M., & Frederick, A. F. (2017). Hidden rainbows: Gay bars as safe havens in a socially conservative area since the Pulse Nightclub massacre. Sexuality Research and Social Policy, 14(2), 233–240. https://doi.org/10.1007/s13178-017-0273-1
- Crosbie, E., Thomson, G., Freeman, B., & Bialous, S. (2018). Advancing progressive health policy to reduce NCDs amidst international commercial opposition: Tobacco standardised packaging in Australia. Global Public Health, 13(12), 1753–1766. https://doi.org/10.1080/17441692.2018.1443485
- Emslie, C., Lennox, J., & Ireland, L. (2017a). The role of alcohol in identity construction among LGBT people: A qualitative study. Sociology of Health & Illness, 39(8), 1465–1479. https://doi.org/10.1111/1467-9566.12605
- Emslie, C., Lennox, J., & Ireland, L. (2017b). The social context of LGBT people’s drinking in Scotland. Scottish Health Action on Alcohol Problems and Glasgow Caledonian University.
- Fergusson, D. M., Horwood, L. J., & Beautrais, A. L. (1999). Is sexual orientation related to mental health problems and suicidality in young people. Archives of General Psychiatry, 56(10), 876–880. https://doi.org/10.1001/archpsyc.56.10.876
- Fergusson, D. M., Horwood, L. J., Ridder, E. M., & Beautrais, A. L. (2005). Sexual orientation and mental health in a birth cohort of young adults. Psychological Medicine, 35(7), 971–981. https://doi.org/10.1017/S0033291704004222
- Gilbert, P. A., Pass, L. E., Keuroghlian, A. S., Greenfield, T. K., & Reisner, S. L. (2018). Alcohol research with transgender populations: A systematic review and recommendations to strengthen future studies. Drug and Alcohol Dependence, 186, 138–146. https://doi.org/10.1016/j.drugalcdep.2018.01.016
- Gilbert, P. A., & Zemore, S. E. (2016). Discrimination and drinking: A systematic review of the evidence. Social Science & Medicine, 161, 178–194. https://doi.org/10.1016/j.socscimed.2016.06.009
- The Global Forum on MSM & HIV & OutRight Action International. (2017). Agenda 2030 for LGBTI health and well-being. The Global Forum on MSM & HIV & OutRight Action International.
- Greene, N., Johnson, R. M., German, D., Rosen, J., & Cohen, J. E. (2021). State-level alcohol environments and sexual identity disparities in binge drinking in the behavioral risk factor surveillance system. LGBT Health, 8(3), 190–200. https://doi.org/10.1089/lgbt.2020.0182
- Greenwood, G. L., & Gruskin, E. (2007). LGBT tobacco and health disparities. In I. H. Meyer, & M. Northbridge (Eds.), The health of sexual minorities: Public health perspectives on lesbian, gay, bisexual and transgender populations (pp. 566–583). Springer.
- Hatzenbuehler, M. L. (2016). Structural stigma: Research evidence and implications for psychological science. The American Psychologist, 71(8), 742–751. https://doi.org/10.1037/amp0000068
- Hawkins, B., Holden, C., Eckhardt, J., & Lee, K. (2018). Reassessing policy paradigms: A comparison of the global tobacco and alcohol industries. Global Public Health, 13(1), 1–19. https://doi.org/10.1080/17441692.2016.1161815
- Health Coalition Aotearoa. (2020). Priority prevention policies. Retrieved November 30, 2020 from https://www.healthcoalition.org.nz/health-issues/alcohol/.
- Health Promotion Agency. (2019a). Key facts about drinking in New Zealand: alcohol use in New Zealand. Retrieved April 9, 2021 from https://www.alcohol.org.nz/sites/default/files/documents/Key-facts-about-drinking-in-New-Zealand.PDF.
- Health Promotion Agency. (2019b). Wellbeing and mental health among rainbow New Zealanders: Results from the New Zealand Mental Health Monitor. Retrieved April 8, 2021 from https://www.hpa.org.nz/research-library/research-publications/wellbeing-and-mental-health-among-rainbow-new-zealanders-infographic.
- Huckle, T., Pledger, M., & Casswell, S. (2006). Trends in alcohol-related harms and offences in a liberalized alcohol environment. Addiction, 101(2), 232–240. https://doi.org/10.1111/j.1360-0443.2006.01326.x
- Hughes, T. L., Wilsnack, S. C., & Kantor, L. W. (2016). The influence of gender and sexual orientation on alcohol use and alcohol-related problems: Toward a global perspective. Alcohol Research: Current Reviews, 38(1), 121–132. https://www.arcr.niaaa.nih.gov/arcr381/article14.htm.
- Lea, T., Reynolds, R., & de Wit, J. (2013). Alcohol and club drug use among same-sex attracted young people: Associations with frequenting the lesbian and gay scene and other bars and nightclubs. Substance Use & Misuse, 48(1–2), 129–136. https://doi.org/10.3109/10826084.2012.733904
- Longerbeam, S. D., Inkelas, K. K., Johnson, D. R., & Lee, Z. S. (2007). Lesbian, gay, and bisexual college student experiences: An exploratory study. Journal of College Student Development, 48(2), 215–230. https://doi.org/10.1353/csd.2007.0017
- Lucassen, M. F. G., Clark, T. C., Moselen, E., & Robinson, E. M. (2014). Youth’12 the health and wellbeing of secondary school students in New Zealand: Results for young people attracted to the same sex or both sexes. The University of Auckland.
- Lyons, A., & Kersey, K. (2020). Alcohol and intoxication. In F. Hutton (Ed.), Cultures of intoxication: Key issues and debates (pp. 17–43). Springer. https://doi.org/10.1007/978-3-030-35284-4_2
- McKie, R. M., Skakoon-Sparling, S., Levere, D., Sezlik, S., & Humphreys, T. P. (2020). Is there space for our stories? An examination of North American and Western European gay, bi, and other men who have sex with men’s non-consensual sexual experiences. The Journal of Sex Research, 57(8), 1014–1025. https://doi.org/10.1080/00224499.2020.1767023
- McNair, R., Pennay, A., Hughes, T., Brown, R., Leonard, W., & Lubman, D. I. (2016). A model for lesbian, bisexual and queer-related influences on alcohol consumption and implications for policy and practice. Culture, Health & Sexuality, 18(4), 405–421. https://doi.org/10.1080/13691058.2015.1089602
- Meyer, I. H. (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychological Bulletin, 129(5), 674–697. https://doi.org/10.1037/0033-2909.129.5.674
- Morris, H., Larsen, J., Catterall, E., Moss, A. C., & Dombrowski, S. U. (2020). Peer pressure and alcohol consumption in adults living in the UK: A systematic qualitative review. BMC Public Health, 20(1), 1014. https://doi.org/10.1186/s12889-020-09060-2
- Mutchler, M. G., McDavitt, B., & Gordon, K. K. (2014). “Becoming bold”: Alcohol use and sexual exploration among Black and Latino young men who have sex with men (YMSM). The Journal of Sex Research, 51(6), 696–710. https://doi.org/10.1080/00224499.2013.772086
- New Zealand Human Rights Commission. (2020). Prism: Human rights issues relating to sexual orientation, gender identity and expression, and sex characteristics (SOGIESC) in Aotearoa New Zealand – A report with recommendations. New Zealand Human Rights Commission.
- Pachankis, J. E., Hatzenbuehler, M. L., Rendina, H. J., Safren, S. A., & Parsons, J. T. (2015). LGB-affirmative cognitive-behavioral therapy for young adult gay and bisexual men: A randomized controlled trial of a transdiagnostic minority stress approach. Journal of Consulting and Clinical Psychology, 83(5), 875–889. https://doi.org/10.1037/ccp0000037
- Pachankis, J. E., McConocha, E. M., Clark, K. A., Wang, K., Behari, K., Fetzner, B. K., Brisbin, C. D., Scheer, J. R., & Lehavot, K. (2020). A transdiagnostic minority stress intervention for gender diverse sexual minority women’s depression, anxiety, and unhealthy alcohol use: A randomized controlled trial. Journal of Consulting and Clinical Psychology, 88(7), 613–630. https://doi.org/10.1037/ccp0000508
- Pedersen, A., Haslund-Thomsen, H., Curtis, T., & Grønkjær, M. (2020). Talk to me, not at me: An ethnographic study on health-related help-seeking behavior among socially marginalized Danish men. Qualitative Health Research, 30(4), 598–609. https://doi.org/10.1177/1049732319868966
- Phillips, J. C., Rowsell, D. J., Boomer, J., Kwon, J.-Y., & Currie, L. M. (2016). Personas to guide understanding traditions of gay men living with HIV who smoke. Qualitative Health Research, 26(1), 41–54. https://doi.org/10.1177/1049732315581614
- Pihama, L., Green, A., Mika, C., Roskrudge, M., Simmonds, S., Nopera, T., Skipper, H., & Laurence, R. (2020). Honour project aotearoa. Te Kotahi Research Institute.
- Randerson, S., Casswell, S., & Huckle, T. (2018). Changes in New Zealand’s alcohol environment following implementation of the Sale and Supply of Alcohol Act (2012). New Zealand Medical Journal, 131(1476), 14–23.
- Riggs, D. W., & Treharne, G. J. (2016). Decompensation: A novel approach to accounting for stress arising from the effects of ideology and social norms. Journal of Homosexuality, 64(5), 592–605. https://doi.org/10.1080/00918369.2016.1194116
- Robertson, K., & Tustin, K. (2018). Students who limit their drinking, as recommended by national guidelines, are stigmatized, ostracized, or the subject of peer pressure: Limiting consumption is all but prohibited in a culture of intoxication. Substance Abuse: Research and Treatment, 12. https://doi.org/10.1177/1178221818792414
- Rosario, M., Schrimshaw, E. W., & Hunter, J. (2004). Predictors of substance use over time among gay, lesbian, and bisexual youths: An examination of three hypotheses. Addictive Behaviors, 29(8), 1623–1631. https://doi.org/10.1016/j.addbeh.2004.02.032
- Saxton, P., Newcombe, D., Ahmed, A., Dickson, N., & Hughes, A. (2017). Illicit drug use among New Zealand gay and bisexual men: Prevalence and association with sexual health behaviours. Drug and Alcohol Review, 37(2), 180–187. https://doi.org/10.1111/dar.12536
- Scheim, A. I., Bauer, G. R., & Shokoohi, M. (2016). Heavy episodic drinking among transgender persons: Disparities and predictors. Drug and Alcohol Dependence, 167, 156–162. https://doi.org/10.1016/j.drugalcdep.2016.08.011
- Schuler, M. S., Prince, D. M., Breslau, J., & Collins, R. L. (2020). Substance use disparities at the intersection of sexual identity and race/ethnicity: Results from the 2015–2018 National Survey on Drug Use and Health. LGBT Health, 7(6), 283–291. https://doi.org/10.1089/lgbt.2019.0352
- Schulman, J. K., & Erickson-Schroth, L. (2017). Mental health in sexual minority and transgender women. Psychiatric Clinics of North America, 40(2), 309–319. https://doi.org/10.1016/j.psc.2017.01.011
- Slater, M. E., Godette, D., Huang, B., Ruan, W. J., & Kerridge, B. T. (2017). Sexual orientation-based discrimination, excessive alcohol use, and substance use disorders among sexual minority adults. LGBT Health, 4(5), 337–344. https://doi.org/10.1089/lgbt.2016.0117
- Surace, A., Riordan, B. C., & Winter, T. (2019). Do New Zealand sexual minorities engage in more hazardous drinking than non-sexual minorities? Drug and Alcohol Review, 38(5), 519–522. https://doi.org/10.1111/dar.12940
- Tan, K. K., Ellis, S. J., Schmidt, J. M., Byrne, J. L., & Veale, J. F. (2020). Mental health inequities among transgender people in Aotearoa New Zealand: Findings from the Counting Ourselves Survey. International Journal of Environmental Research and Public Health, 17(8), 2862. https://doi.org/10.3390/ijerph17082862
- Te Hiringa Hauora/Health Promotion Agency of New Zealand. (n.d.). Low-risk alcohol drinking advice. Retrieved January 11, 2021 from https://www.alcohol.org.nz/help-advice/advice-on-alcohol/low-risk-alcohol-drinking-advice.
- Treharne, G. J., & Adams, J. (2017). Critical perspectives on research into sexualities and health in Aotearoa/New Zealand: Thinking outside the boxes. Psychology of Sexualities Review, 8(1), 53–70.
- Treharne, G. J., Riggs, D. W., Ellis, S. J., Flett, J. A. M., & Bartholomaeus, C. (2020). Suicidality, self-harm, and their correlates among transgender and cisgender people living in Aotearoa/New Zealand or Australia. International Journal of Transgender Health, 21(4), 440–454. https://doi.org/10.1080/26895269.2020.1795959
- Veale, J., Byrne, J., Tan, K., Guy, S., Yee, A., Nopera, T., & Bentham, R. (2019). Counting ourselves: The health and wellbeing of trans and non-binary people in Aotearoa New Zealand. University of Waikato.
- Vic Health. (2018). Couldn’t have done that with a hangover: New campaign aims to shift LBQ Drinking culture in Regional Victoria. Retrieved January 11, 2021 from https://www.vichealth.vic.gov.au/media-and-resources/media-releases/new-drinking-culture-campaign.
- Willig, C. (2013). Introducing qualitative research in psychology. Open University Press.

