
ABSTRACT
Female genital cutting (FGC) and intimate partner violence (IPV) are highly prevalent forms of violence against women, and the UN has encouraged strengthening policy linkages between FGC and IPV programme work (UN Women, Female genital mutilation/cutting and violence against women and girls. Strengthening the policy linkages between different forms of violence. UN Women, 2017a). However few studies have examined the relationship between these behaviours. This study addresses two research gaps identified by the UN; (a) whether women with FGC are more likely to experience physical or sexual IPV, and (b) whether women’s IPV experiences are associated with their support for FGC. Multilevel multivariate logistic regression models were run using Demographic and Health Survey data from 6 sub-Saharan African countries (Burkina Faso, Ethiopia, The Gambia, Ivory Coast, Kenya and Nigeria, n33,170). Our results show no association between FGC and IPV. Women with FGC are not at greater risk of experiencing IPV, and women who experienced IPV in the preceding year are not more likely to support FGC. Further, the importance of individual and community factors differ; IPV experience is influenced by individual factors, whereas FGC support is more influenced by ethnic group characteristics. Although the proposition that FGC and IPV could be tackled collaboratively is attractive for policy makers, these results are important because they indicate that eradication programmes will be more effective when targeted at specific behaviours.
Introduction
Joint eradication programmes which could reduce the prevalence of several forms of violence against women and girls (VAWG) simultaneously are a compelling proposition for policy makers, presenting the possibility of increasing programme efficiency and making greater progress towards achieving the Sustainable Development Goals by 2030 (UN, Citation2016). Likewise, practitioners have long urged policy makers to recognise the overlapping nature of different types of VAWG (physical, sexual and psychological behaviours perpetrated against women both within and outside the home) and to design interventions that target multiple forms of VAWG together rather than in isolation (MIGS, Citation2015; Yount et al., Citation2017). Recently this approach has been extended to include FGC. In 2017 the UN released a policy note saying that ‘both VAWG and FGM/C have some common underlying causes that would greatly benefit from common strategies to eliminate them. This can be done in part through increased coordination and collaboration between different actors working to end VAWG and FGM/C’ (UN Women, Citation2017a).
However, although FGC and IPV are often grouped together as VAWG or harmful cultural practices, there are some fundamental differences in their profiles which challenge the suggestion that they have common underlying causes. FGC is only practiced in specific communities or countries, and can be characterised as a one-off practice, arranged by a girl’s family sometime between birth and marriage, and is typically imbued with cultural significance (Shell-Duncan & Hernlund, Citation2000). By contrast, IPV is found globally, perpetrated in private and often recurrently by a woman’s partner or husband, and a women’s IPV experiences may change over their lifetime (Heise, Citation2011). Although it is commonly suggested that FGC and IPV experiences are associated, their co-occurrence is not well-documented (Barbaro, Citation2017; UN Women, Citation2017a), and this assertion is examined in this paper.
Co-occurrence of different forms of VAWG
Empirical evidence demonstrating the co-occurrence of different forms of psychological, physical and sexual violence towards women, either within the home or in the community, is relatively well-established (e.g. Garcia-Moreno et al., Citation2006; Hayes & Van Baak, Citation2017; Heise, Citation2012). The term ‘polyvictimisation’ describes women and girls’ experiences of multiple forms of violence, either concurrently or sequentially, drawing attention to the augmented impact this has on victims’ trauma symptoms (Yount et al., Citation2017). The co-occurrence of IPV specifically with other forms of VAWG has also been demonstrated, such as IPV and early marriage (Kidman, Citation2017), and IPV and non-partner violence (Abramsky et al., Citation2011; Krebs et al., Citation2011). This gives rise to the as yet unproven prediction that IPV and FGC might also co-occur.
Two main hypotheses have been put forward to suggest why different forms of VAWG may co-occur. At the individual level, psychologists have focused on the phenomenon of revictimisation, whereby individuals who experience adverse childhood experiences are at greater risk of experiencing IPV or other forms of VAWG in adulthood (Barnes et al., Citation2009; Classen et al., Citation2005). The mechanisms underlying revictimisation are not yet understood, but a common explanation relates to the psychological sequelae resulting from childhood abuse, such as alcohol and drug use, post-traumatic stress, and poor risk recognition, which increase the odds of being revictimised as adults (Kennedy, Citation2008).
The alternative hypothesis suggests that VAWG behaviours share the same societal root causes, namely patriarchal values and gender inequality (UN Women, Citation2017a). Women at the intersection of societal systems (such as ethnicity, class, religion, socio-economic status) may face multiple forms of oppression in the form of VAWG (Garcia-Moreno et al., Citation2006; Kelly, Citation1987).
Both theories have been drawn on to predict an association between FGC status and IPV experience. Individual revictimisation has been suggested (Peltzer & Pengpid, Citation2014;Salihu et al., Citation2012), but more commonly it is argued that IPV and FGC are both maintained by societal patriarchal norms intended to control women (Barbaro, Citation2017; Shell-Duncan et al., Citation2011; UN Women, Citation2017a). However patriarchal norms are difficult to prove empirically due to the challenges of capturing suitable data, and the idea of a common root cause for FGC and IPV is challenged by studies which have demonstrated different drivers for these behaviours. FGC is typically motivated by parental concerns about social acceptance and marriageability, with men often stating lower or similar levels of support for FGC than women (Varol et al., Citation2015; Yoder & Wang, Citation2013). By contrast commonly recognised drivers of IPV perpetration relate to men’s individual circumstances, such as witnessing parental violence, alcohol use and involvement in community violence (Fleming et al., Citation2015).
The relationship between FGC and IPV has been examined in four empirical studies to date, all of which used demographic health survey data (DHS), to test whether FGC status is a risk factor for experiencing IPV. A study using Egypt data found women with FGC had higher odds of experiencing IPV, however only 2.9% of the sample did not have FGC (Refaat et al., Citation2001); a study using Ivory Coast data found a positive association between FGC status and sexual IPV, but not other forms of IPV (Peltzer & Pengpid, Citation2014); and a study which used Mali 2006 DHS data found a positive association between FGC and all subtypes of IPV (Salihu et al., Citation2012). However, a subsequent study using Mali 2013 DHS data did not find a positive association (Hayes & Van Baak, Citation2017). Therefore although three of the four studies found a positive association, the results are not definitive. The authors variously attribute these associations to revictimisation (Peltzer & Pengpid, Citation2014; Salihu et al., Citation2012), gender imbalance or intersectionality (Refaat et al., Citation2001).
Few studies have examined the association between women’s endorsement of both practices (i.e. support for the FGC continuation, and agreement with IPV justifications). A positive association has been found in data from Benin, Ethiopia, Eritrea, and Mali, whereas this was not the case in Nigeria, and the evidence from Egypt appears mixed (Afifi, Citation2009; Refaat et al., Citation2001; UNICEF, Citation2005; Yount & Li, Citation2009).
Eradication policy and research gaps identified by UN women
It is unclear whether coordinated elimination strategies targeted at reducing FGC and IPV together would be beneficial, as no joint programmes have been documented and evaluated in the literature to date. However, it has been suggested that programmes which used a social norms change approach to address either FGC or IPV, may have indirectly reduced the other behaviour. In particular, an FGC eradication programme in Senegal reported a decrease in IPV, as well as FGC (Diop, Citation2004). Much weight has been given to this result which has been widely cited and used to promote the use of multiple programme interventions as a means of accelerating FGC and IPV change (Gennari et al., Citation2014; Heise, Citation2011; UN Women, Citation2017a; UNICEF, Citation2008). However, the report in which these results are described is not peer-reviewed and the sample sizes are small (n200 women, n198 men). Therefore, it remains to be established whether FGC and IPV are more effectively tackled together.
The UN Women paper, which advocates strengthening policy linkages between IPV and FGC interventions, recognises two major knowledge gaps in understanding (UN Women, Citation2017b) which are addressed here by testing the following hypotheses; (1) Women with FGC have a higher risk of experiencing IPV, and (2) Experiencing IPV increases women’s support for the continuation of FGC.
Methods
Data and sample
DHS datasets were used for this study. These nationally representative surveys collect data on a range of subjects including socioeconomic profile, reproductive and maternal health, marriage and sexual activity. Additional optional modules on IPV and FGC are also available (www.dhsprogram.com).
In this study global coverage was restricted to sub-Saharan Africa, where FGC is most prevalent. Thirteen recent country surveys which used both the IPV and FGC modules were assessed for suitability. Countries in which FGC prevalence was greater than 90% in all ethnic groups (Sierra Leone, Mali) or less than 10% in all ethnic groups (Uganda, Cameroon, Togo) were excluded. Chad was excluded because there was no overlap between women sampled for both IPV and FGC modules, and Tanzania was excluded because ethnic group information was not collected. The remaining six countries were suitable for analysis; Kenya 2014, Nigeria 2013, Gambia 2013, Ivory Coast 2012, Burkina Faso 2010 and Ethiopia 2008 (n33,689 women). Overall 12.3% of women had experienced physical or sexual IPV in the 12 months preceding the survey, and 59.1% of women had some form of FGC.
The FGC profile is similar in the six countries. The average age at FGC is between 2.5 and 4.7 years in all countries except Kenya where it is 11.2 years. The most common form of FGC is flesh being removed from the genitals, experienced by 81–96% of women with FGC, although slightly less in Nigeria (67%). The DHS uses descriptors of FGC type rather than the WHO classification system. In this sample, 8% of women with FGC were cut with no flesh removed (WHO Type IV), 79% had flesh removed from their genitals (WHO Type I or Type II), and 8% were infibulated (WHO Type III). The remaining 6% did not know or did not answer concerning FGC type.
Data analysis
The same datasets were used to test both hypotheses. Women who were unmarried, and whose FGC status, IPV experience or ethnic group were unknown, were excluded. Respondents from ethnic groups with fewer than 50 women were also excluded. Otherwise all women with available data for the selected variables were used in the analyses (n31,170 for hypothesis 1, n31,067 for hypothesis 2).
Hypothesis 1: Women with FGC have a higher risk of experiencing IPV
The outcome variable was women’s experience of physical and/or sexual IPV during the 12 months preceding the survey. Restricting IPV experience to a specific recent timeframe reduces recall bias and allowed the control variables to be matched temporally as far as possible to the IPV experience. The DHS survey asks respondents about several specific experiences relating to physical IPV (being pushed, shaken, slapped, punched, kicked, dragged, beaten up, choked or attacked with a weapon) and sexual IPV (being forced, physically or in any other way, to have sexual intercourse, or perform sexual acts). Women who reported that they had experienced one or more of these behaviours, either sometimes or often, were coded as having experienced IPV.
FGC status is the key predictor variable of interest. The DHS asks women whether they are circumcised (translated into their local equivalent), and women who had experienced any form of FGC were coded as cut.
The statistical models control for variables which have been shown in previous studies to be associated with the risk of women experiencing IPV (Abramsky et al., Citation2011; Garcia-Moreno et al., Citation2006; Jewkes et al., Citation2017). These variables are household wealth (using the DHS quintiles poorest, poorer, middle, richer, richest), household location (rural or urban), woman’s age, woman’s education (none, primary, and secondary or higher), and marriage type (polygamous or monogamous). The model also controls for whether the husband drinks alcohol as reported by his wife (yes or no), whether the woman was exposed to IPV in childhood (whether her father beat her mother) as both these variables have been shown to be highly predictive of IPV experience (WHO/LSHTM, Citation2010). Age at FGC cannot be controlled for as it is only relevant for women who have been cut.
Two indicators of female empowerment are included in the model as studies have shown that women with more autonomy have a lower risk of experiencing IPV (Benebo et al., Citation2018;Rahman et al., Citation2013). The first indicator is the number (out of five) of controlling behaviours exerted by their husbands (whether their husband; is jealous or angry if she talks to other men, frequently accuses her of being unfaithful, does not permit her to meet female friends, insists on knowing where she is at all times, or tries to limit her contact with family). The second indicator is the number (out of four) of household decisions in which women participate (their own healthcare, large household purchases, what is done with the husband’s earnings, and visits to friends or relatives). Participation was assumed where women responded that they solely or jointly made these decisions.
A community level variable was also included in the multilevel model to control for social acceptance of IPV among men which varies by community, and which is argued may influence IPV perpetration (Benebo et al., Citation2018; Jewkes et al., Citation2017). Male attitudinal data was extracted from the male DHS datafiles for the same countries and ethnic groups. Men are asked whether ‘wife beating’ is justified in five different circumstances; if his wife burns the food, refuses to have sex, goes out without telling him, neglects the children, or argues with him. Responses were used to calculate the average number of statements agreed with by men in each ethnic group.
Hypothesis 2: Experiencing IPV increases women’s support for FGC
The outcome variable of interest is whether women think that FGC should be stopped or continued. Women who were undecided or said they didn’t know were excluded from the analysis (n1,600).
The predictor variable of interest was women’s experience of physical and/or sexual IPV during the preceding 12 months. Variables known to affect women’s FGC support were controlled for in the models. Women’s own FGC status is the strongest predictor of FGC support (Bellemare et al., Citation2015) and additionally, the models controlled for women’s education (categorised as none, primary, and secondary or higher), household wealth (using the DHS quintiles), religion (Muslim, Christian, or None/Other), and age. Possible exposure to anti-FGC media campaigns is controlled for using a composite mass media variable, calculated from women’s responses to their use of television, radio and newspapers. Responses are categorised into no exposure, infrequent exposure (less than weekly) or frequent exposure (daily) (Benebo et al., Citation2018). Additionally, the two indicators of female empowerment described above (experience of controlling behaviours and involvement in household decisions) were included as these have been shown to affect women’s support of FGC (Afifi, Citation2009; Rahlenbeck et al., Citation2010), as well as the number of IPV justifications women agreed with (out of five). A community level variable of FGC prevalence (percentage of women over 15 years in each ethnic group who have experienced FGC) was also included in the multilevel model as this has been shown to influence FGC behaviour (Howard & Gibson, Citation2017).
Statistical analysis
Multivariate logistic regression analyses were used to test both hypotheses. Single level models were run on the six individual datasets, then the data was pooled for multilevel analyses. The DHS data is suited to multilevel modelling due to the hierarchical structure. Here individual women are nested in 73 ethnic groups which are nested in 6 countries. Ethnic group affiliation was used as the secondary level as this has been shown to be an important determinant of individual FGC behaviour and provides an adequate sample size for analysis (Bellemare et al., Citation2015; Shell-Duncan et al., Citation2011; Yoder & Wang, Citation2013).
Multilevel models recognise the clustering of data at different levels. This addresses some of the perils of analysing aggregate data, and allows assessment of the effect of individual and community effects on the outcome variable as well as estimating the extent of variation across communities. It is generally recommended that there should be more than 15 units in each level to avoid standard errors being underestimated (Rasbash et al., Citation2012). With just six countries at level 3, there is a possibility that the country-level random variances and standard errors may be underestimated.
Second and third level variance was calculated to understand the variation between ethnic groups and countries regarding the IPV experience and FGC support (the intercepts in the multilevel logistic regression), and to interpret the importance of the different levels on the outcome. The intra-class correlation (ICC), expressed as a percentage, gives a measure of the variance in the logistic outcome attributable to different levels in the model (Goldstein, Citation2010). The median odds ratio (MOR) expresses the level variance as an odds ratio. High MOR indicate that the contextual effects are more important for understanding the individual probability of experiencing the outcome.
Four multilevel models were run to test hypothesis 1. A null model 1 which showed the variance in IPV experience attributable to the three different levels. Model 2 only included the woman’s FGC status. Model 3 included all control variables but excluded woman’s FGC status. Model 4 included all control variables and the woman’s FGC status. Running separate models allows the effect of FGC status on the variance to be analysed.
Five models were run to test hypothesis 2. Model 1 was a null model. Model 2 only included the woman’s IPV experience. Model 3 included all control variables but excluded IPV experience. Model 4 included all control variables and the woman’s IPV experience. Model 5 additionally included the number of years since anti-FGC legislation was passed as a level 3 contextual variable. FGC was legal in The Gambia and some states of Nigeria at the time these DHS surveys were conducted, whereas it was criminalised over 20 years ago in Burkina Faso and Ivory Coast (World Bank, Citation2018). It is anticipated that stated support for FGC will be lower in countries which have longer-standing anti-FGC legislation (Kovacs, Citation2017).
Results
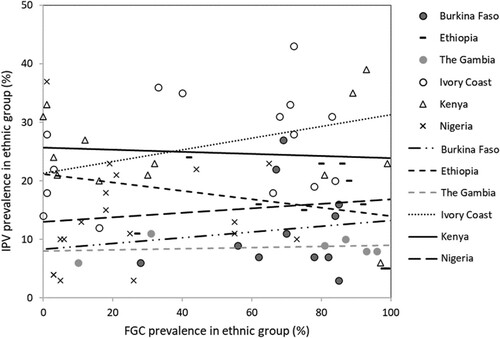
A bivariate Pearson correlation analysis examining the relationship between FGC prevalence and physical and sexual IPV prevalence in the 73 ethnic groups in the six study countries showed no significant correlations at the ethnic group level, either overall (r = −0.031, p = .794 n73), or in any of the study countries (illustrated in , full results in SI Table 1).
Hypothesis 1: Women with FGC have a higher risk of experiencing IPV
Figure 1. Prevalence of IPV and FGC by ethnic group and country.
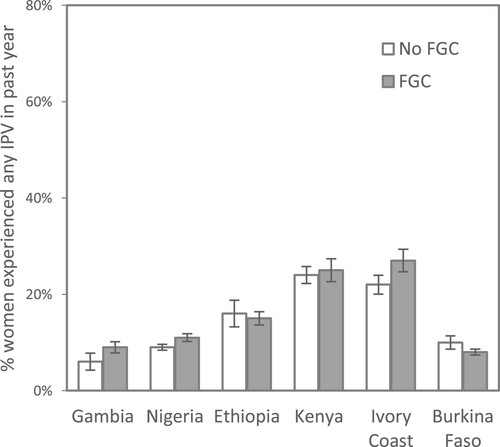
On average a slightly smaller proportion of women with FGC experienced IPV in the preceding year, compared to women without FGC (12.1% compared to 12.7%), illustrated by country in . Descriptive analytics are available in SI Table 2. There is a higher IPV prevalence in Ethiopia, Kenya and Ivory Coast, but there is no common pattern found in these six countries in relation to FGC status. A higher proportion of women with FGC experienced IPV in the Gambia, Nigeria and notably Ivory Coast, whereas in Ethiopia and Burkina Faso a higher proportion of women without FGC experienced IPV, and in Kenya there is no difference by FGC status.
Figure 2. Women’s IPV experience by FGC status (n31,170).
Single level multivariate logistic regression analyses by country tested the effect of FGC status while controlling for confounding factors (SI Table 4). The association between FGC status and IPV experience was only found to be significant and positive in Ivory Coast (OR 1.27, 95%CI 1.01–1.59, p = 0.043). In Ethiopia, Gambia, Kenya and Nigeria the association was positive but not at significant levels, and in Burkina Faso the association was negative, but not at a statistically significant level.
The results of the multilevel multivariate models using pooled data from all six countries () show that FGC status is not associated with IPV experience. The null Model 1 shows that there is little variance between ethnic groups (9.5%) or between countries (5.6%), and that most of the variation in IPV experience is at the individual level (84.9%). Model 2 shows that without any control variables FGC status has a positive and significant association with IPV experience (OR 1.15, 95%CI 1.05–1.27, p = .003), although the inclusion of FGC status has little effect on the overall model or the Level 2 and Level 3 variance.
Table 1. IPV experience: Three level logistic regression models analysing factors associated with women’s IPV experience in past year.
Model 3 controls for variables which have been shown in previous studies to affect women’s risk of experiencing IPV; wealth reduces the risk of IPV but only significantly so in the richest households (OR 0.74, 95%CI 0.63–0.87, p < .000); women whose husbands drink alcohol, and who in polygamous marriages have a significantly higher risk of experiencing IPV (OR 2.10, 95%CI 1.09-1.32, p = .004 and OR 1.20, 95%CI 1.09–1.32, p < .000). Childhood exposure to IPV also increases the odds of experiencing IPV (OR 2.10, 95%CI 1.92–2.30, p < .000), and experience of more spousal controlling behaviours also significantly increases the odds of experiencing IPV (OR 1.70, 95%CI 1.66–1.75, p < .000). The other individual level control variables (household location, woman’s age, woman’s education, and the number of household decisions the woman is involved in) are not significantly associated with IPV experience. Likewise, men’s attitude towards IPV in the ethnic group, included as a level 2 contextual variable, is not significantly associated with IPV experience (OR 1.15, 95%CI 0.93–1.43, p = .200). Together the control variables reduce the level 2 variance from 0.354 to 0.217 (38.5%) and the level 3 variance from 0.215 to 0.082 (63.7%).
Model 4 adds FGC status to the control model, and the results show that the effect of being cut has a positive but small association with IPV experience and is not a statistically significant (OR 1.10, 95%CI 0.99–1.21, p = .067). Adding FGC status has a negligible effect on the level 2 or level 3 variance and does not alter the effect of the control variables in the model. Further analysis shows that no individual control variable included in Model 4 accounts for the relationship between FGC status and IPV experience found in the bivariate Model 2 becoming non-significant in Model 4. Each control variable explains a small portion of the effect.
Hypothesis 2: Experiencing IPV increases women’s support for FGC
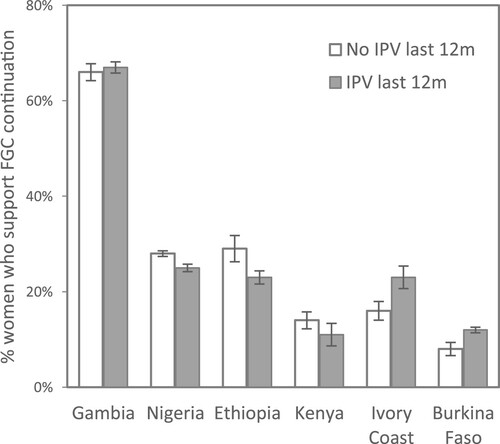
Three quarters of women in the study sample (76.6%) do not support the continuation of FGC. FGC support does not vary greatly by IPV experience; overall FGC support is slightly lower among women who had experienced IPV (21.5% compared to 23.6%), illustrated by country in . Full descriptive statistics are provided in SI Table 3. In The Gambia, where FGC was legal at the time of survey, support for FGC is markedly higher compared to the other five countries. There is no common pattern between IPV experience and FGC; in half the countries more women who experienced IPV support FGC, whereas the opposite is found in the other half.
Figure 3. Women’s support for FGC by IPV experience (n31,067).
The single level logistic regression models by country (SI Table 5) show that IPV experience is significantly associated with supporting FGC in Burkina Faso (OR 1.47, 95%CI 1.14–1.89, p = .003) and Ivory Coast (OR 1.43, 95%CI 1.11-1.86, p = .007). However, the opposite is found in Ethiopia (OR 0.73, 95%CI 0.56-0.94, p = .017) and the Gambia (OR 0.67, 95%CI 0.46–0.99, p = .044) where women who experienced IPV have higher odds of stating that FGC should not be continued. In Nigeria and Kenya, IPV experience is not significantly associated with FGC support.
The multilevel models with pooled data from all six countries () demonstrate that when variables known to affect women’s support of FGC are controlled for, IPV experience is not significantly associated with women’s support for FGC. The null Model 1 shows that a large element of variance in FGC support is at the ethnic group level (42.8%) with 7.8% at the country level, and 49.4% at the individual level. Model 2 shows that IPV experience alone does increase the odds of a woman supporting the continuation of FGC (OR 1.18, 95%CI 1.07–1.31, p = .001). Although this association is statistically significant, the addition of IPV experience in Model 2 makes very little difference to the level 2 or level 3 variance compared to Model 1 (the proportional change in variation is only 0.7% and 14.4%, respectively).
Table 2. Three level logistic regression models analysing factors associated with women’s agreement that FGC should be continued.
Model 3 shows the effect of controlling for variables known to be important predictors of FGC support, most of which have the anticipated effect on women’s support for FGC. A woman’s own FGC status is the strongest predictor of supporting FGC (OR 8.75, 95%CI 7.47–10.25, p < .000), and women who agree with IPV justifications are also more likely to state support for FGC (OR 1.14, 95%CI 1.12–1.16, p < .000). Variables which are shown to reduce the probability of women supporting FGC are greater household wealth (OR 0.60, 95%CI 0.51–0.70, p < .000), older age (OR 0.99, 95%CI 0.98–0.99, p < .000) having either primary or secondary education, being Christian rather than Muslim (OR 0.50, 95%CI 0.44–0.56, p < .000) and having any exposure to mass media (OR 0.79 95%CI 0.71–0.87 p = .000). In this sample, household location, whether the woman has any daughters, and whether the woman is involved in any household decisions, are not significantly associated with a woman’s FGC support. FGC prevalence in the woman’s ethnic group, a level 2 contextual variable, also has a significant effect; the odds of supporting FGC increases significantly as FGC prevalence increases (OR 1.02, 95%CI 1.01–1.02, p < .000). The addition of the control variables reduces the level 2 variance substantially, with a 78.8% PCV, whereas they result in a 154% increase in level 3 variance.
The results of Model 4 show that IPV experience is not significantly associated with FGC support in the full model (OR 1.08, 95%CI 0.97–1.21 p = 0.166), and the addition of IPV experience makes a negligible impact on the level 2 or 3 variance, or on the effect of the control variables. Model 5 includes the number of years since FGC was made illegal as a level 3 contextual variable which has a large impact on the level 3 variance, reducing it by 79.6%. However, its inclusion does not alter the effect size or significance of any of the individual level variables, including IPV experience.
Discussion
In this study, two research gaps concerning the relationship between FGC status or support, and physical and sexual IPV experience, were addressed using multilevel models and data from 6 countries in sub-Saharan Africa (UN Women, Citation2017b). The results do not show an association between the two behaviours.
The first analysis tested whether women with FGC are more likely to experience physical or sexual IPV. The multilevel logistic regression analysis results (, Model 4) do not support this hypothesis. Women with FGC have a slightly higher, but not statistically significant, odds of experiencing IPV and the effect of FGC status on the model variance is negligible. Other factors are of much greater importance in understanding variation in women’s IPV experience, including living in poorer households, their husband’s alcohol use, their exposure to IPV in childhood, being in a polygamous marriage, and experience of controlling behaviours by their husband.
The multilevel model only controls for a small number of potentially confounding variables, and only explains a small proportion of the individual level variance. Numerous other factors which have been demonstrated to affect the incidence of IPV are not included here, for example, their husband/partner’s exposure to childhood violence, involvement in community violence, and gender attitudes (Fleming et al., Citation2015) and their couple dynamics (e.g. extra-marital sexual activity or marital conflict (Jewkes et al., Citation2017)). It is likely that the effect of FGC status on IPV experience would be further reduced if data for these other relevant factors were available.
This result conflicts with previous single country studies which found that women with FGC had significantly higher odds of experiencing some form of IPV, in the Ivory Coast, Mali, and Egypt (Peltzer & Pengpid, Citation2014; Refaat et al., Citation2001; Salihu et al., Citation2012). The same Ivory Coast DHS dataset is represented in this study and the positive association is replicated in the single level logistic regression results (Salihu et al., Citation2012) (SI Table 4). However these results demonstrate the value of multilevel models which avoid incorrect inferences based on ecological fallacies by recognising the clustering of data at different levels (Lawson et al., Citation2015; Pollet et al., Citation2015), and do not support a generalised statement that women with FGC have an increased risk of experiencing IPV.
This null result challenges both the individual (revictimisation) and societal (patriarchal) theoretical bases for anticipating that FGC and IPV may be associated. It is unknown whether FGC in childhood would result in the same psychological sequelae in adulthood (e.g. alcohol use, drug abuse, sexual risk-taking) that are associated with other forms of adverse childhood experiences, and accordingly FGC may not lead to revictimisation or polyvictimisation in the same way. Although a recent study has shown depression and PTSD resulting from FGC (Bendiksen et al., Citation2021), the bulk of studies to date have studied trauma from FGC associated with women’s first sexual or obstetric experiences e.g. (Mulongo et al., Citation2014). And conversely, FGC can be a source of pride for some girls and women, and women with FGC may have higher status in the societies in which FGC is practiced (Shell-Duncan & Hernlund, Citation2000).
The role of the patriarchy in maintaining FGC is also uncertain, and there is counter evidence that questions whether FGC is driven by a desire to control women (Howard & Gibson, Citation2019). Patriarchal explanations for an association between FGC and IPV are also problematic as they do not explain the individual rationale; why would men married to women with FGC might be more likely to be violent towards them, or alternatively, why would men who perpetrate IPV might be more likely to marry a woman with FGC. In fact the opposite prediction could equally be made; that men married to women with FGC (already under patriarchal control and with controlled sexual desire) would have less cause to resort to violence. In contrast to the broad literature on women’s multiple experiences of VAWG, the drivers for ‘poly-perpetration’ by men has been little studied.
The second analysis tested whether women’s IPV experience is associated with their support for FGC continuation. The single level analyses showed that the relationship between IPV experience and women’s stated FGC support varies by country, but the multilevel model with pooled data from all six countries (Table 3, Model 4) showed that the effect of IPV experience is small and not statistically significant. The other variables controlled for in the model, such as the mother’s FGC status and FGC prevalence in the ethnic group, are most strongly significantly associated with FGC support.
This finding challenges the expectation that women who experience IPV will be more likely to support FGC (UN Women, Citation2017b), and likewise that reducing IPV levels would necessarily result in a reduction in FGC. The theoretical basis for this expectation is not explained, but it seems to assume that IPV experience affects women’s autonomy, and that women’s autonomy is related to their FGC support. These assumptions appear to be based on a patriarchal interpretation of FGC, posing men as the proponents of FGC and women as the opposers, anticipating that women who experience IPV will have lowered resistance to oppose FGC. The reverse could be equally possible, whereby women with higher autonomy may support FGC (Shell-Duncan & Hernlund, Citation2000). The intricacies of FGC support and decision-making regarding daughters’ FGC procedures are poorly understood (Kaplan et al., Citation2013). However, the assumption that greater female autonomy would necessarily lead to lower support for FGC needs further evidence and theoretical grounding.
IPV experience and FGC support are associated with different individual and community level factors
Several differences between the drivers of IPV and FGC are revealed here, adding further doubt that these behaviours are explained by common factors. Firstly, community level factors are more important in maintaining FGC support than in determining IPV experience. This is unsurprising given the highly enculturated nature of FGC, and is evident from two aspects of the results. There is much greater variation seen in FGC support (ranging from 0% to 99%), compared to IPV experience which is relatively uniform across ethnic groups (ranging from 0% to 35%) (illustrated in ). Further, the multilevel model results show that the variance between ethnic groups (and to a lesser extent between countries) is much greater in the model examining FGC support ((B 2.460 SE 0.449), 42.8% ICC in the null model) than in the model testing IPV experience ((B 0.354 SE 0.070), 9.5% ICC in the null model).
Community level factors, such as the behaviours and beliefs among members of a woman’s ethnic group are more important determinants of women’s FGC support than their personal IPV experience. The FGC support model (Table 3) included ethnic group FGC prevalence as a level 2 contextual variable which was shown to be positively and significantly associated with women’s support of FGC. The IPV experience model () included men’s IPV justifications in the ethnic group, but the results show that living in an ethnic group in which men agreed with a greater number of IPV justifications did not increase the odds of a woman experiencing IPV. In this model IPV behaviour is better predicted by individual level variables. This finding contrasts with the prevailing view of IPV adopted by the WHO which suggests that social norms concerning IPV acceptability within the community are important determinants of IPV risk (WHO/LSHTM, Citation2010).
Secondly, the results also show that different predictor variables are significantly associated with IPV experience and FGC support. Women’s age and education are not significantly associated with IPV experience, nor is household wealth or household location. Whereas all four of these variables are associated with FGC support. The variables most strongly related to IPV experience are male characteristics; whether the husband has more than one wife, whether he drinks alcohol, whether he exerts controlling behaviours over his wife, and whether the wife’s father beat her mother. By contrast, male factors are largely absent from the FGC support model and the key explanatory variable is the mother’s own FGC status.
Finally, explaining women’s risk of experiencing IPV appears to be more elusive than explaining their FGC support. The small number of control variables included in the FGC support model explain a large amount of the variance (reducing the ethnic group variance by 77% in Model 5 compared to Model 1). By contrast, the variables used in the IPV experience model only reduce the ethnic group variance by 40% from Model 1 to Model 4. This suggests that many further variables are required to fully understand women’s risk of IPV.
Study limitations and further research
The use of cross-sectional data means that a temporal relationship between the variables cannot be established. This temporal relationship is likely to be particularly key for understanding causes and consequences of women’s IPV experience. For example, longitudinal data that captures women’s FGC support or decision regarding their daughters’ FGC procedure before and after any IPV experience would improve understanding of whether IPV experience influences FGC behaviour.
Another limitation relates to the use of secondary datasets as the survey questions are not tailored to these specific research questions. Here all available relevant DHS variables were used, but more nuanced data would be revealing. For example, it would be interesting to know whether men who marry women with FGC have different attitudes about gender equality or IPV acceptability. In relation to women’s support for FGC it would be informative to have a better understanding of how the decision to have FGC performed on any daughters is made, for example, whether there is any evidence that women’s autonomy influences this decision, and if so, in which direction (Kaplan et al., Citation2013). Further the way in which women’s support for FGC is captured by the DHS questionnaires (should FGC be continued or stopped) does not allow for a range of responses reflecting different circumstances, life stages and relationships to the women or girls involved.
Finally, here data from only six out of the possible thirteen countries were suitable for analysis. The results might differ if data from all thirteen countries (or even all 29 countries in which FGC is commonly practiced) met the inclusion criteria for this study.
Conclusion
This paper examines the association between FGC and physical and sexual IPV to address the research gaps identified by the UN Women paper ‘Finding convergence in policy frameworks’ using data from six countries in sub-Saharan Africa (UN Women, Citation2017a). Two models were run, testing firstly whether women who have been cut are more susceptible to physical and sexual IPV, and secondly whether women’s experience of IPV affects their support of FGC. The results do not support either hypothesis, and there is no evidence of an association between FGC and IPV. Additionally, the results reveal differing importance of individual and community level variables which further challenges the suggestion that FGC and IPV share common underlying causes. The distinct enculturated nature of FGC practices may not result in co-occurrence in the same way that has been documented for other forms of VAWG.
The lack of a demonstrable association between FGC and IPV has important implications for policy and programme work, suggesting that there is unlikely to be a knock-on effect from programmes aimed at either behaviour; reducing levels of FGC will not affect IPV prevalence, and vice versa. These results highlight the potential problems that can result from grouping disparate behaviours together, as important differences may be overlooked. Even FGC and IPV include numerous sub-types of behaviours which may be more effectively tackled separately and in a context-specific manner (Berg & Denison, Citation2012; Fulu et al., Citation2013).
The clear difference in profile and risk factors between IPV and FGC challenges the value of implementing common strategies to eliminate them. The results suggest that it will be more effective to create targeted programmes tailored to the specific risk factors involved in either IPV or FGC, taking the local context into account.
Supplemental Material
Download MS Word (64.8 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The datasets used for this study are publicly available at www.dhgprogram.com.
Additional information
Funding
References
- Abramsky, T., Watts, C. H., Garcia-Moreno, C., Devries, K., Kiss, L., Ellsberg, M., Jansen, H. A., & Heise, L.(2011). What factors are associated with recent intimate partner violence? Findings from the WHO multi-country study on women’s health and domestic violence. BMC Public Health, 11(1), 1–17. https://doi.org/10.1186/1471-2458-11-109
- Afifi, M.(2009). Women’s empowerment and the intention to continue the practice of female genital cutting in Egypt. Archives of Iranian Medicine, 12(2), 154–160.
- Barbaro, N.(2017). Violence to control women’s sexuality. In T. K.Shackelford& V. A.Weekes-Shackelford(Eds.), Encyclopaedia of evolutionary psychology(pp. 8407–8412). Springer International.
- Barnes, J. E., Noll, J. G., Putnam, F. W., & Trickett, P. K.(2009). Sexual and physical revictimization among victims of severe childhood sexual abuse. Child Abuse & Neglect, 33(7), 412–420. https://doi.org/10.1016/j.chiabu.2008.09.013
- Bellemare, M. F., Novak, L., & Steinmetz, T. L.(2015). All in the family: Explaining the persistence of female genital cutting in West Africa. Journal of Development Economics, 116, 252–265. https://doi.org/10.1016/j.jdeveco.2015.06.001
- Bendiksen, B., Heir, T., Minteh, F., Ziyada, M. M., Kuye, R. A., & Lien, I. L.(2021). The association between physical complications following female genital cutting and the mental health of 12-year-old gambian girls: A community-based cross-sectional study. Plos one, 16(1), 1–15. https://doi.org/10.1371/journal.pone.0245723
- Benebo, F. O., Schumann, B., & Vaezghasemi, M.(2018). Intimate partner violence against women in Nigeria: A multilevel study investigating the effect of women’s status and community norms. BMC Women’s Health, 18(1), 1–17. https://doi.org/10.1186/s12905-018-0628-7
- Berg, R. C., & Denison, E.(2012). Effectiveness of interventions designed to prevent female genital mutilation/cutting: A systematic review. Studies in Family Planning, 43(2), 135–146. https://doi.org/10.1111/j.1728-4465.2012.00311.x
- Classen, C. C., Palesh, O. G., & Aggarwal, R.(2005). Sexual revictimization: A review of the empirical literature. Trauma Violence & Abuse, 6(2), 103–129. https://doi.org/10.1177/1524838005275087
- Diop, N. J.(2004). The TOSTAN program: Evaluation of community based education program in senegal(FRONTIERS Final Report). Population Council.
- Fleming, P. J., Mccleary-Sills, J., Morton, M., Levtov, R., Heilman, B., & Barker, G.(2015). Risk factors for men’s lifetime perpetration of physical violence against intimate partners: Results from the international men and gender equality survey (IMAGES) in eight countries. PLOS ONE, 10(3), 1–18. https://doi.org/10.1371/journal.pone.0118639
- Fulu, E., Jewkes, R., Roselli, T., Garcia-Moreno, C., & Me, U. N. M. C. S.(2013). Prevalence of and factors associated with male perpetration of intimate partner violence: Findings from the UN multi-country cross-sectional study on Men and violence in Asia and the pacific. The Lancet Global Health, 1(4), E187–E207. https://doi.org/10.1016/S2214-109X(13)70074-3
- Garcia-Moreno, C., Jansen, H. A. F. M., Ellsberg, M., Heise, L., & Watts, C. H.(2006). Prevalence of intimate partner violence: Findings from the WHO multi-country study on women’s health and domestic violence. The Lancet, 368(9543), 1260–1269. https://doi.org/10.1016/S0140-6736(06)69523-8
- Gennari, F., Mccleary-Sills, J., & Hidalgo, N.(2014). Violence against women and girls: Introduction. World Bank.
- Goldstein, H.(2010). Multilevel statistical models. John Wiley & Sons.
- Hayes, B. E., & Van Baak, C.(2017). Risk factors of physical and sexual abuse for women in Mali: Findings from a nationally representative sample. Violence Against Women, 23(11), 1361–1381. https://doi.org/10.1177/1077801216658979
- Heise, L.(2011). What works to prevent partner violence? An evidence overview. Working Paper. STRIVE Research Consortium, London School of Hygiene and Tropical Medicine.
- Heise, L. L.(2012). Determinants of partner violence in low and middle-income countries: Exploring variation in individual and population-level risk[PhD thesis]. London School of Hygiene & Tropical Medicine.
- Howard, J. A., & Gibson, M. A.(2017). Frequency-dependent female genital cutting behaviour confers evolutionary fitness benefits. Nature Ecology & Evolution, 1(3), 1–6. https://doi.org/10.1038/s41559-016-0049
- Howard, J. A., & Gibson, M. A.(2019). Is there a link between paternity concern and female genital cutting in West Africa?Evolution and Human Behavior, 40(1), 1–11. https://doi.org/10.1016/j.evolhumbehav.2018.06.011
- Jewkes, R., Fulu, E., Naved, R. T., Chirwa, E., Dunkle, K., Haardorfer, R., Garcia-Moreno, C., & Vi, U. N. M. S. M.(2017). Women’s and men’s reports of past-year prevalence of intimate partner violence and rape and women’s risk factors for intimate partner violence: A multicountry cross-sectional study in Asia and the pacific. Plos Medicine, 14(9), 1–20. https://doi.org/10.1371/journal.pmed.1002381
- Kaplan, A., Cham, B., Njie, L. A., Seixas, A., Blanco, S., & Utzet, M.(2013). Female genital mutilation/cutting: The secret world of women as seen by men. Obstetrics and Gynecology International, 2013, 643780–643780. https://doi.org/10.1155/2013/643780
- Kelly, L.(1987). The continuum of sexual violence. In H.J, & M.M.(Eds.), Women, violence and social control(pp. 46–60). Palgrave MacMillan.
- Kennedy, A. C.(2008). An ecological approach to examining cumulative violence exposure among urban, African American adolescents. Child and Adolescent Social Work Journal, 25(1), 25–41. https://doi.org/10.1007/s10560-007-0110-0
- Kidman, R.(2017). Child marriage and intimate partner violence: A comparative study of 34 countries. International Journal of Epidemiology, 46(2), 662–675. https://doi.org/10.1093/ije/dyw225
- Kovacs, R. J.(2017). The macro-level drivers of intimate partner violence: New evidence from a multilevel dataset. Global Public Health, 13(7), 1–13. https://doi.org/10.1080/17441692.2017.1317010
- Krebs, C., Breiding, M. J., Browne, A., & Warner, T.(2011). The association between different types of intimate partner violence experienced by women. Journal of Family Violence, 26(6), 487–500. https://doi.org/10.1007/s10896-011-9383-3
- Lawson, D. W., James, S., Ngadaya, E., Ngowi, B., Mfinanga, S. G., & Mulder, M. B.(2015). No evidence that polygynous marriage is a harmful cultural practice in northern Tanzania. Proceedings of the National Academy of Sciences, 112(45), 13827–13832. https://doi.org/10.1073/pnas.1507151112
- MIGS. (2015). Repositioning FGM as a gender and development issue. Mediterranean Institute of Gender Studies (MIGS).
- Mulongo, P., Hollins Martin, C., & Mcandrew, S.(2014). The psychological impact of female genital mutilation/cutting (FGM/C) on girls/women’s mental health: A narrative literature review. Journal of Reproductive and Infant Psychology, 32(5), 469–485. https://doi.org/10.1080/02646838.2014.949641
- Peltzer, K., & Pengpid, S.(2014). Female genital mutilation and intimate partner violence in the Ivory Coast. BMC Women’s Health, 14(1), 1–5. https://doi.org/10.1186/1472-6874-14-13
- Pollet, T. V., Stulp, G., Henzi, S. P., & Barrett, L.(2015). Taking the aggravation out of data aggregation: A conceptual guide to dealing with statistical issues related to the pooling of individual-level observational data. American Journal of Primatology, 77(7), 727–740. https://doi.org/10.1002/ajp.22405
- Rahlenbeck, S., Mekonnen, W., & Melkamu, Y.(2010). Female genital cutting starts to decline among women in Oromia, Ethiopia. Reproductive BioMedicine Online, 20(7), 867–872. https://doi.org/10.1016/j.rbmo.2010.01.009
- Rahman, M., Nakamura, K., Seino, K., & Kizuki, M.(2013). Does gender inequity increase the risk of intimate partner violence among women? Evidence from a national Bangladeshi sample. PLOS ONE, 8(12), 1–12. https://doi.org/10.1371/journal.pone.0082423
- Rasbash, J., Steele, F., Browne, W., & Goldstein, H.(2012). A user’s guide to MLwiN, v2. 26. Centre for Multilevel Modelling. University of Bristol.
- Refaat, A., Dandash, K. F., El Defrawi, M. H., & Eyada, M.(2001). Female genital mutilation and domestic violence among Egyptian women. Journal of Sex & Marital Therapy, 27(5), 593–598. https://doi.org/10.1080/713846819
- Salihu, HM, August, E. M., Salemi, J. L., Weldeselasse, H., Sarro, Y. S., & Alio, A. P.(2012). The association between female genital mutilation and intimate partner violence. BJOG An International Journal of Obstetrics and Gynaecology, 119(13), 1597–1605. https://doi.org/10.1111/j.1471-0528.2012.03481.x
- Shell-Duncan, B., & Hernlund, Y.(2000). Female “circumcision” in Africa: Dimensions of the practice and debates. In B.Shell-Duncan, & Y.Hernlund(Eds.), Female “circumcision” in Africa: Culture, controversy and change(pp. 1–40). Lynne Rienner Publishers ltd.
- Shell-Duncan, B., Wander, K., Hernlund, Y., & Moreau, A.(2011). Dynamics of change in the practice of female genital cutting in Senegambia: Testing predictions of social convention theory. Social Science and Medicine, 73, 1275–1283. https://doi.org/10.1016/j.socscimed.2011.07.022
- UN. (2016). Transforming our world: the 2030 agenda for Sustainable Development A/RES/70/1. United Nations.
- UNICEF. (2005). Female genital mutilation/cutting: A statistical exploration.
- UNICEF. (2008, September). Long term evaluation of the TOSTAN programme in Senegal: Kolda, Thies and Fatick region.
- UN WOMEN. (2017a). Female genital mutilation/cutting and violence against women and girls. Strengthening the policy linkages between different forms of violence.
- UN WOMEN. (2017b). Finding convergence in policy frameworks. A background paper on the policy links between gender, violence against women and girls, and female genital mutilation/cutting.
- Varol, N., Turkmani, S., Black, K., Hall, J., & Dawson, A.(2015). The role of men in abandonment of female genital mutilation: A systematic review. BMC Public Health, 15(1), 1–14.
- WHO/LSHTM. (2010). Preventing intimate partner and sexual violence against women: Taking action and generating evidence. World Health Organisation.
- World Bank. (2018). Protecting women from violence. Retrieved May 1, 2018, from http://wbl.worldbank.org/en/data/exploretopics/protecting-women-from-violence.
- Yoder, S. P., & Wang, S.(2013). Female genital cutting: The interpretation of recent DHS data female genital cutting: The interpretation of recent DHS Data. DHS Comparative Reports No. 33. ICF International.
- Yount, K. M., Krause, K. H., & Miedema, S. S.(2017). Preventing gender-based violence victimization in adolescent girls in lower-income countries: Systematic review of reviews. Social Science & Medicine, 192, 1–13. https://doi.org/10.1016/j.socscimed.2017.08.038
- Yount, K. M., & Li, L.(2009). Women’s “justification” of domestic violence in Egypt. Journal of Marriage and Family, 71(5), 1125–1140. https://doi.org/10.1111/j.1741-3737.2009.00659.x