
ABSTRACT
Early motherhood can negatively impact health, educational, and socio-economic outcomes for adolescent mothers and their children. Supporting adolescent mothers’ educational attainment, and timely return to school, may be key to interrupting intergenerational cycles of adversity. Yet, there remains a paucity of evidence on the factors that are associated with mothers’ postpartum return to school and the mediators of this process, particularly across sub-Saharan Africa where adolescent pregnancy rates remain high . This paper is based on interviews with 1,046 adolescent mothers from South Africa. Mothers who had returned to school after birth showed lower poverty, fewer repeated grades preceding the pregnancy, continued schooling during pregnancy, higher daycare/crèche use, more family childcare support, and lower engagement in exclusive breastfeeding within six months postpartum. Mediation analyses showed that lower poverty was directly associated with school return and via two indirect pathways: continued schooling during pregnancy and using daycare/crèche services. This study demonstrates that lacking childcare constitutes a major hurdle to mothers’ school return which needs to be addressed in addition to socioeconomic and individual-level barriers. Policy makers and practitioners should consider supporting young mothers with combination interventions which include services supporting school retention during pregnancy and access to, and financial supplements for, daycare.
Introduction
Adolescent fertility remains high in many regions of the world, with particularly elevated rates across Africa where about one-fifth of adolescent girls become pregnant under the age of 19 (Kassa et al., Citation2018; Mori et al., Citation2017; United Nations, Citation2020). Early pregnancies can have major health consequences for adolescent girls (Ganchimeg et al., Citation2014), and childbirth complications remain the leading cause of death among girls between 15–19 years globally (Neal et al., Citation2012). Across sub-Saharan Africa, adolescent pregnancies occur against the backdrop of the highest global maternal mortality rates (World Health Organisation, Citation2019), high levels of HIV (UNAIDS, Citation2020), violence (Poser & Ritchie, Citation2019), deprivation (Poser & Ortiz-Ospina, Citation2019), low service access (Magadi et al., Citation2007; Mekonnen et al., Citation2019), and limited support mechanisms (Toska et al., Citation2020) – these conditions pose significant obstacles for adolescent mothers and their children to achieve good health and social outcomes.
A common concern related to adolescent pregnancy is impaired school outcomes of the young mother and, intergenerationally, even of her children. Education is a well-established social determinant of health, and supporting adolescent mothers’ continued schooling might provide opportunities to strengthen their long-term health and wellbeing (Feinstein et al., Citation2006; Freudenberg & Ruglis, Citation2007; Viner et al., Citation2012). Indeed, a recent US-based study with 301 adolescent mothers indicates that higher levels of completed education in the years after birth are associated with better self-reported health at age 50 (Maslowsky et al., Citation2021). Studies also suggest that education might work as a ‘social vaccine’ in HIV endemic environments, showing that length and completion of secondary education reduces the risk for HIV infection, especially for girls (De Neve et al., Citation2015; Pettifor et al., Citation2008; Stoner et al., Citation2017). Particularly maternal education is also strongly linked to the use of health services (Forshaw et al., Citation2017; Simkhada et al., Citation2008), child health and life expectancy (Huebender, Citation2019; Mensch et al., Citation2019), and might mediate the negative relationship between the mothers’ age and children’s IQ later in life (Barlow et al., Citation2011; Khatun et al., Citation2017; Mollborn & Dennis, Citation2012). Despite the importance of effectively promoting adolescent mothers’ return to school, evaluated programmes to date – all from the US – show largely small effects (Harding et al., Citation2020; SmithBattle et al., Citation2017; Steinka-Fry et al., Citation2013), and there remains a lack of support for adolescent mothers within sub-Saharan Africa (Callahan et al., Citation2017; Groves et al., Citation2018; Toska et al., Citation2020).
In South Africa, about 20% of female school-going adolescents report having ever been pregnant (Jonas et al., Citation2016) and recent estimates show that approximately 125,000 adolescent girls give birth annually (Maquina, Citation2015). Supporting these girls to return to school after childbirth is critical, especially because prolonged absence can increase the risk of a permanent school dropout (Ardington et al., Citation2015; Panday et al., Citation2009). Like many countries across the African Union, which increasingly aim to provide an enabling policy-environment (Martinez & Odhiambo, Citation2018), the South African Department of Education established a national policy that supports young mothers’ school return (South African Department of Education, Citation2007). However, evidence shows that only between 30% (Grant & Hallman, Citation2008) and 50% (Groves et al., Citation2021; Marteleto et al., Citation2006) of young mothers do manage to continue their education, highlighting a continued need to better understand barriers to school re-enrolment.
Whilst most research on adolescent mothers’ schooling in South Africa investigates the effect of pregnancy on early school dropouts (Ardington et al., Citation2015; Grant & Hallman, Citation2008; Kruger et al., Citation2009; Madhavan & Thomas, Citation2005; Marteleto et al., Citation2008; Stoner et al., Citation2019; Timaeus & Moultrie, Citation2015), finding that pregnancy increases the odds of school dropout both during pregnancy and in the postpartum period, there is sparse quantitative evidence on the factors that enable or limit girls to return to school after birth. Exceptions include two studies, both relying on data collected prior to 2010. Grant and Hallman (Citation2008), utilizing a cross-sectional sample of female adolescents from two districts in KwaZulu Natal, found that greater odds of school return were associated with good school performance prior to pregnancy, co-residency with a female household member younger than 60 years, fewer years since birth, and adolescent mothers’ higher age at the time of the interview (Grant & Hallman, Citation2008). In addition, Timaeus and Moultrie (Citation2015) used longitudinal data drawn from South Africa’s National Income Dynamics Study and showed that living in a higher-income household, higher education of the adolescent mother’s caretaker, and rural residency prior to the pregnancy was associated with higher odds of postpartum return to school. These studies made important contributions to the evidence base but provide limited insights into the support that adolescent mothers require to navigate the dual-challenge of parenting whilst attending school. A recent mixed-methods study with 90 young mothers from Umlazi township in KwaZulu-Natal corroborates the importance of instrumental support, showing associations between the return to school and family assistance with the re-enrolment process, provision of childcare from the family or support to organize external childcare, and financial support (Groves et al., Citation2021). These results align with a small pool of research from Zambia (Zuilkowski et al., Citation2019), Kenya (Birungi et al., Citation2015; Lwanga Walgwe et al., Citation2016; Kruger et al., Citation2009; Ngabaza and Shefer, Citation2013; Ntambo and Malvin, Citation2017), and Mozambique (Salvi, Citation2019), indicating that lacking financial means and the need for childcare are the main barriers to school return for young mothers. Yet, no study to date has been able to quantitatively explore the relationship between financial and childcare obstacles, nor interrogate different pathways towards girls’ school return. For instance, it remains unclear if the relationship between poverty and not returning to school is partly mediated by the inability to cover the cost for daycare services. Whilst multiple studies to date suggest a correlation between school return and family childcare provisions, no study has been able to assess and compare the role of other sources of childcare, such as community-based daycare centres, on adolescent mothers’ school return. It is also possible that adolescent mothers’ return to school is hindered by additional factors which have not yet been empirically examined, such as compliance with recommendations that advices exclusive breastfeeding for six months after birth (World Health Organisation, Citation2021) or certain birth complications which have shown to be elevated in this group (Kassa et al., Citation2017). An improved understanding of these variables and their associations with young mothers’ school return is needed, however, to develop support mechanisms that effectively lead to girls’ re-enrolment after birth.
The current study
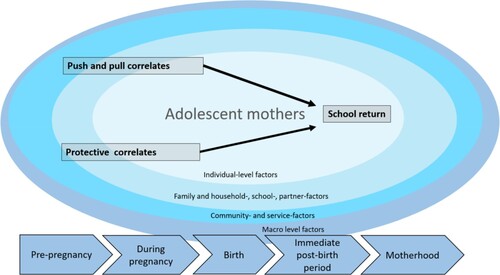
Building on previous evidence, the present study aimed to investigate further pre-and post-pregnancy variables hypothesized to affect the return to school. illustrates the conceptual model to understand school return, building on work by Singh and Mukherjee (Citation2018). The framework posits that the postpartum return to school is influenced by longer-term educational trajectories in addition to influences from multiple interacting individual, family, household, school, and community factors. Aligned with Singh and Mukherjee (Citation2018), all assessed variables included in the analyses (see below), can be categorized into 1) Push and pull correlates which are hypothesized to make a school return less likely (i.e. being the primary caregiver of the child, exclusive breastfeeding, any birth complications, and grade delay preceding the pregnancy) and 2) protective correlates which are variables which were hypothesized to show higher associations with school return (i.e. continued schooling during pregnancy, government child support grant receipt, maintenance payments, lower household poverty, living with a caregiver, household size, familial childcare support, and daycare/crèche use). also reflects that schooling at each point in time was hypothesized to be influenced by schooling at prior stages, leading us to explore not only pre-pregnancy schooling, but also schooling during pregnancy as a correlate for postpartum school enrolment.
Figure 1. Conceptual framework for studying school return after birth, based on Singh and Mukherjee (Citation2018).
Overall, the present research aimed to better understand what is needed to counteract young mothers’ risk for a permanent school dropout by focusing on two overarching objectives (1) Identify which factors are associated with adolescent mothers’ postpartum return to school. Aligned with our conceptual framework and gaps within this area of research, we specifically intended to disentangle the role of childcare provided by the family and community-based childcare, respectively. (2) Assess the mechanisms through which socioeconomic determinants affect the return to school.
Method
Participants and procedures
Data for this study was collected as part of the HEY BABY (Helping Empower Youth Brought up in Adversity with their Babies and Young Children) cohort study of adolescent mothers and their children living in the Eastern Cape province of South Africa (N = 1,046). Adolescent mothers (aged 10–24) residing in urban, peri-urban, and rural locations were recruited between 2017 and 2019. Six parallel sampling strategies were utilized, including recruitment from health facilities (n = 73), secondary schools (n = 43), maternity obstetric units (n = 9), service provider referrals, door-to-door community recruitment and referrals from adolescent mothers themselves. All participating girls and young women had their first pregnancy before the age of 20. Our inclusion criteria therefore align with the World Health Organization definition of ‘adolescence’ (World Health Organization, Citation2016) and describes an adolescent pregnancy as the occurrence of a pregnancy at the age of 19 or below. The period of time since the woman gave birth varied among participants; some mothers completed the interviews a few months postpartum whilst several years had passed for others. Informed consent was sought from adolescents who were above the age of 18 and assent was provided by underage participants in addition to consent from their adult caregiver. All consent forms and questionnaires were available in English and isiXhosa.
Ethical clearance was provided by the Universities of Oxford (R48876/RE001; R48876/RE002) and Cape Town (HREC REF: 226/2017), and by the provincial government departments of Health, Basic Education, and Social Development. Participants were interviewed in private spaces in and around their own home, but they were given the option to conduct the interview in a local restaurant if the privacy in the home was compromised.
Assisted by trained interviewers, adolescents completed two complementary questionnaires, each taking about 60 minutes. The items in the questionnaire predominantly concerned the participants’ lives at the time of the interview (e.g. household poverty, rural/urban residency, living with a caregiver, daycare/crèche use), but a small number of retrospective questions aimed to capture past events (e.g. medical problems during birth, grade delay preceding the pregnancy, the return to school). Confidentiality was maintained throughout the study except where participants requested help or were at risk of significant harm. In this study, 25 referrals were made to health or counselling services with follow-up support. There were no monetary incentives, but all participants received a certificate, refreshments, and a participant pack containing useful items (e.g. washcloth and soap).
Measures
School return after birth was assessed by one item (0: no return to school; 1: return to school).
Individual-level factors: The adolescent mother was considered the primary caregiver of her infant/child if she was the main caretaker (0: no; 1: yes). Exclusive breastfeeding captured feeding in the first six months postpartum (0: no; 1: yes). Birth problems captured the experience of any of the following: The child was the wrong way around, the child was admitted to neonatal intensive care, excessive bleeding during pregnancy, being sick after birth (0: no; 1: yes). Grade-delay preceding the pregnancy was assessed by comparing the grade participants were enrolled in at the beginning of their pregnancy against the appropriate grade for the individual’s age as determined by the South African Schools Act of 1996. Calculations followed the approach taken in comparable studies from South Africa where the correct age norm per grade follows Grade 1 + 6 = age 7; Grade 9 + 6 = age 15; Grade 12 + 6 = age 18 (e.g. Herrero Romero et al., Citation2021). Adolescents who were enrolled in the age-appropriate grade or above were classed as not delayed (0: not delayed; 1: delayed; 2: not enrolled in school). Continued schooling during pregnancy was assessed (0: discontinued schooling; 1: continued schooling). Access to government child support grant receipt (0: no; 1: yes). Relationship with child’s father was assessed by one item enquiring if the adolescent has a continued relationship with the father of her child (0: no; 1: yes, always/mostly). Maintenance payment receipt from the child’s father was assessed (0: no; 1: yes).
Family- and household-level factors: Household poverty was assessed by measuring access to the top eight socially-perceived necessities for children in South Africa i.e. clothes to keep warm in the winter or soap to wash (Barnes & Wright, Citation2012). Items were summed to create a poverty index (range 0-8) with lower numbers reflecting higher levels of poverty. Co-residency with the caregiver enquired whether adolescent mothers lived with their parents, grandparents or another caregiver (0: no; 1: yes). Family childcare support reflects the level of help with childcare tasks (i.e. washing, playing, care-taking, buying necessities) provided by the young mother’s own caregiver or other family members in the past two weeks (0: no help; 1: help with most tasks; 2: help with all tasks).
Community- and service-level factors: Daycare/Crèche use was assessed by one item (0: no; 1: yes).
Potential covariates included the place of residency (0: urban; 1: rural), household size, the participant’s age, participant’s age at the pregnancy with their oldest child, and the age of the infant/child (i.e. the child of the adolescent mother).
Statistical analyses
Participants were eligible for inclusion in the analysis if they had not already finished school at the onset of the pregnancy or throughout pregnancy (49 participants were excluded based on this criteria). Additional 15 participants were excluded from the analyses because they had not received all relevant questions on schooling, 14 participants were excluded because they were older than 19 during their pregnancy. Lastly, 31 participants were excluded because it was not possible to determine whether or not they were grade-delayed at the time of pregnancy. Prior to the analyses, the dataset was checked for inconsistencies. 26 participants indicated inconsistent information for the outcome variable (i.e. the return to school). These cases were re-coded as missing. Little’s test (Little, Citation1988) was used to check whether these variables were missing completely at random, which was the case (χ2 (4) = 4.74, p = 0.31), thus they were safely excluded from the analyses.
All analyses were completed in Stata 15.1. and Mplus 7. First, descriptive statistics for all outcomes, associated factors, and socioeconomic background variables were calculated for the whole sample as well as disaggregated by return-status. Second, models of risk and protective factors were built empirically in two steps. In step 1, school return was logistically regressed onto each hypothesized correlate, controlling for socioeconomic factors (mothers’ age at the pregnancy with their oldest child, urban/rural location, and infant/child age). Analyses were corrected for multiple comparisons using Bonferroni correction. Subsequently, variables that were statistically significant in step 1 (i.e. Bonferroni-corrected p-value < .003) were included in a hierarchical logistic regression (Cohen et al., Citation2003). Variables were entered into the model as follows to assess the contribution of each conceptual set that follows a temporal sequence: (i) Demographic covariates; (ii) Household poverty; (iii) Pre-pregnancy school progression; (iv) Schooling during pregnancy; (v) Postnatal factors (exclusive breastfeeding, living with a caregiver, family childcare support and daycare/crèche use). Each regression controlled for mothers’ age at the pregnancy with their oldest child, urban/rural location, and infant/child age. Finally, mediation analyses were conducted to test whether household poverty operated in ‘risk pathways’ towards the return to school. Direct and indirect effects of the tested mediation model were assessed using MPlus 7, using the robust weighted least square (WLSMV) estimator for categorical outcomes. Analyses were conducted using the bootstrapping procedure with 5,000 bootstrapped samples. The fit of the hypothesized parallel mediation model compared to alternative models was evaluated using the DIFFTEST option which tests for χ2 differences in nested models. The model fit was assessed using the root mean square error of approximation (RMSEA), the comparative fit index (CFI), the Tucker-Lewis index (TLI), and weighted root mean square residual (WRMR). By convention, a CFI value >0.95 indicates good fit and >0.90 adequate fit. For RMSEA a value of 0.05 indicates good model fit, and for WRMR a value close to 1 indicates good model fit (Brown, Citation2015; Distefano et al., Citation2018).
Results
The analyses were based on 911 adolescent mothers in the sample. As shown in , out of the 911 participants, 634 returned to school after birth whereas 277 did not return. The mean age of study participants was 18.1 years (SD 1.77). Most adolescent mothers still lived with a parent or an adult caregiver (91.6%) and seven participants were married (0.8%). Mothers’ mean age at the pregnancy of their oldest child was 16.48 years (SD 1.52), 80 mothers (8.8%) had more than one child, and most mothers in our sample were the primary caregiver of their infant/child (94.1%). Over half of the mothers were classed as grade-delayed preceding the pregnancy (58.1%) and 73.9% had continued schooling throughout their pregnancy. About 80% of mothers received financial support in form of a government child grant, but only 4.7% of adolescent mothers received maintenance payments from the father of their child. Just over a quarter of children attended daycare/crèche services (27.6%). Approximately half of all participants were still in a relationship with the father of the child (50.1%). shows independent multiple logistic regressions which were run to determine which factors were significantly related to school return, controlling for the mothers’ age at the pregnancy with their first-born child, urban/rural residency, and the child’s age at the time of the interview ().
Table 1. Descriptive statistics for the sample of adolescent mothers from the Eastern Cape, South Africa (n = 911).
Table 2. Independent associations between hypothesized correlates and postpartum school return.
Associations between hypothesized correlates and postpartum school return
Results from the hierarchical logistic regression analyses are shown in . Model 1 included only relevant socioeconomic and demographic variables; Model 2 added household factors; Model 3 captured school progression preceding the pregnancy; Model 4 added pregnancy variables, and the final Model 5 added variables on postpartum practices and support. The final model showed that returning to school after birth was associated with lower household poverty (OR 1.18, 95% CI [1.09, 1.28]), less grade delay preceding the pregnancy (OR 0.51, 95% CI [0.33–0.79]), continued schooling during pregnancy (OR 7.04, 95% CI [4.77, 10.40]), the use of daycare/crèche services (OR 4.15 95% CI [2.37, 7.27]) and family childcare support (OR 2.33 95% CI [1.47, 3.69]), and not exclusively breastfeeding in the first six months after birth (OR 0.50 95% CI [0.33, 0.76]).
Table 3. Associations between hypothesized correlates and postpartum school return.
Mediation pathways from economic hardship to school return
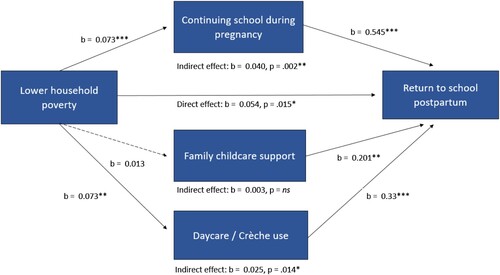
Mediation analyses were conducted to evaluate whether household poverty affects the postpartum return to school directly or via mediating pathways (). Lower household poverty was directly associated with the return to school postpartum. Lower poverty was also moderately associated with continued schooling during pregnancy (b = 0.07) which, in turn, was associated with returning to school (b = 0.54). At the same time, lower poverty was associated with more use of daycare/crèche services (b = 0.07) which, in turn, was associated with school return (b = 0.33). Whilst the path between household poverty and family childcare support was not significant, the childcare support received from the family was associated with return to school (b = 0.20).
Figure 2. Tested mediation pathways towards postpartum school return. The coefficients are based on 5,000 bootstrapped samples. Mediation analyses controlled for all variables in the final model of school return (), n = 805. Dotted lines indicate hypothesised pathways that were non-significant. *p< .05. **p< .01. ***p< .001.
Discussion
As education is a modifiable social determinant of health, supporting adolescent mothers’ continued schooling might provide opportunities to strengthen their health and well-being. This paper set out to investigate the impact of hypothesized correlates on postpartum school return among adolescent mothers. Almost 70% of young mothers in our sample had returned to school after birth, even in a highly deprived area of South Africa, where almost no educational support services are available. Given that approximately 50% of non-returned mothers in this sample had children younger than one year, further girls might return to school as their children get older. A recent study from Zambia suggests that knowledge of school policies could protect adolescent mothers against being forced out of school as a result of the pregnancy (Zuilkowski et al., Citation2019). It is possible that the return rates in our study are elevated compared to older samples from South Africa (e.g. Grant & Hallman, Citation2008; Groves et al., Citation2021; Marteleto et al., Citation2008) because adolescent mothers are increasingly aware of their right to education, which could equip them with the confidence to insist on staying in school despite being asked to leave (Ngabaza & Shefer, Citation2013).
The present results echo prior findings from sub-Saharan Africa, indicating that poverty and unmet childcare needs are major contributors to adolescent mothers’ school return (Madhavan & Thomas, Citation2005). Previous quantitative studies from South Africa showed mixed results for the association between poverty and the return to school, indicating that higher poverty lowers the odds of a school return (Timaeus & Moultrie, Citation2015) or no effect (Grant & Hallman, Citation2008). In South Africa, socioeconomic status is highly correlated with attending poor quality schools (Spaull, Citation2013) which, in turn, is associated with slower school progression (Branson et al., Citation2014). Our findings might point to a particular vulnerable group of young mothers affected by a compounded disadvantage of poverty and deficits in cumulative learning for whom a pregnancy might act as a catalyst for a permanent school dropout (Branson et al., Citation2014). At the same time, girls’ inability to cover school-related costs after the birth of their child has emerged in numerous qualitative studies (Bhana & Nkani, Citation2016; Morrell et al., Citation2012; Ngabaza & Shefer, Citation2013). Even though our findings showed no associations between the return to school and mothers’ receipt of financial support in form of the child support grant and child maintenance, future research should further explore the impact of other sources of support, such as government childcare subsidies (e.g. childcare vouchers, see Schochet & Johnson, Citation2019) to increase adolescent mothers’ return to school in South Africa. Whilst our analyses showed that lower levels of poverty clearly contributed to continued schooling throughout pregnancy and the use of daycare/crèche services (the mediators in our analyses), their relatively weak association suggests that financial support alone may not be sufficient to address the identified risk pathways. Future studies should investigate the range of additional factors that influence schooling during pregnancy and the use of childcare services so that interventions can better target the breadth of challenges mothers face in addition to financial deprivation. For instance, it remains unclear if daycare and crèche services are merely unavailable in some communities or if specific obstacles and objections prevent adolescent mothers to take up these services even when they are within reach. An exploration of these barriers and concerns could build support structures that best address adolescent mothers’ needs and help them succeed.
Results from the mediation analyses suggest two distinct routes towards postpartum school return among adolescent mothers (i) a pre-birth pathway where discontinued schooling throughout pregnancy drives lower return-rates; and (ii) a post-birth pathway where the use of daycare/crèche services drives greater return-rates. These findings support a framework of multiple pathways towards early school dropout (Dupéré et al., Citation2015) and suggest that supporting adolescent mothers’ education may require a combination of interventions addressing both their pre-birth and post-birth challenges. With the exception of one promising pilot intervention (Shazi et al., Citation2018), no known evaluated programmes exist to improve school outcomes in South Africa’s adolescent mothers (Toska et al., Citation2020). In light of the present findings, which showed that school continuation during pregnancy affects the return to school, extending school-based programmes to target retention during pregnancy may be required to further increase postpartum return-rates. For instance, school-based antenatal care has been shown to improve attendance and enrolment during pregnancy in high-income countries, even though the effects did not persist after birth (Barnet et al., Citation2004). One study from South Africa proposed that existing school-based services might be well placed to identify girls at risk for school discontinuation during pregnancy (Jochim et al., Citation2021), but future research should explore which additional services could interrupt pathways of risk to early school discontinuation.
The present findings also point to the importance of childcare access for adolescent mothers’ return to school. This finding is not surprising given results from high-income countries showing that childcare access is associated with nine times the odds of school return after birth (Assini-Meytin et al., Citation2018). Whilst our results corroborate numerous studies from South Africa which have pointed to the pivotal role of family networks to support girls’ schooling through childcare (Bhana & Nkani, Citation2016; Chigona & Chetty, Citation2008; Hatch & Posel, Citation2018; Russel, Citation2003), the use of formal daycare facilities showed a much stronger association with school return.
Prior research suggest that adolescents mothers’ caregivers and families do not necessarily provide a reliable source of childcare, potentially because their capacity is limited by their own employment (Bhana & Nkani, Citation2016; Chigona & Chetty, Citation2008). Below half of all children in South Africa use daycare services, but adolescent mothers’ uptake might be disproportionally reduced by high-cost, inconvenient locations, or operating hours that are incompatible with schooling (De Henau et al., Citation2019; Devercelli & Beaton-Day, Citation2020). For instance, adolescent mothers’ might need childcare outside the regular opening hours in the months leading up to the final examinations when school lessons often extend into the evening hours. These difficulties might be amplified for mothers from rural areas with limited transport options or those who undertake long commutes to school. Concerted efforts to provide adolescent mothers with childcare to support continued education appear scarce across sub-Saharan Africa, even though they might be essential to support the educational advances of adolescent mothers (Kassebaum et al., Citation2017; Kennedy, Citation2017) and circumvent perpetuating gendered cycles of poverty (Samman & Lombardi, Citation2019). Exceptions have emerged from Gabon, Zambia, Tanzania, Kenya, and Ethiopia where childcare centres have been built close to schools and NGO initiatives support temporary residence, education, and vocational training for adolescent mothers and their children (Kabanze, Citation2019; Martinez & Odhiambo, Citation2018; Mulinya, Citation2021; Ochiel, Citation2017; The Hunger Project, Citation2019). However, there is a need to address the current lack of accessible documentation and evaluation of these programmes which is necessary to understand their reach and effectiveness to create sustainable solutions.
Of note is that mothers’ exclusive breastfeeding in the first six months after birth was associated with reduced odds of school return. The causal direction of this relationship is unclear and, given the low rates of exclusive breastfeeding among adolescent mothers in South Africa, it is possible that mothers who decided not to return to school end up breastfeeding the child exclusively (Zweigenthal et al., Citation2019). We have previously shown that most ‘returned’ mothers continued school relatively early after birth (Jochim et al., Citation2020), which may indicate a difficulty of navigating schooling whilst adhering to the recommendations to breastfeed the child for six months postpartum (South African Department of Health, Citation2013; Zweigenthal et al., Citation2019). Future work is needed to address how educational policies can be compatible with infant feeding policies (Zweigenthal et al., Citation2019) to simultaneously protect adolescent mother’s educational rights and maximize healthy child development.
The present study has several limitations. First, this study did not assess successful school completion and it is possible that mothers discontinued schooling after an initial return. It is also important not to conflate school enrolment with attendance (Ardington et al., Citation2015), which could have been impaired even for mothers who managed to return to school. As the new policy on the Prevention and Management of Learner Pregnancy in Schools comes into effect (Department of Basic Education, Citation2021), it is important for future research to assess both matriculation and attendance rates among adolescent mothers in South Africa. Second, the variables pertaining to pregnancy and birth experiences were assessed retrospectively and may be subject to recall bias. However, for 50% of mothers less than a year had passed since birth, which could reduce the risk for biased reports (Stull et al., Citation2009).
Third, the cross-sectional nature of the data precludes establishing a clear temporal sequence. To mitigate this, the questionnaire was designed to establish some temporality through items requiring recall of past events (Shahar & Shahar, Citation2013). Whilst some covariates were assessed with reference to the time of the interview (e.g. household poverty, living with a caregiver, grant access, breastfeeding, and available childcare) and could have changed since the participant returned to school, the resulting biases are likely minimal. Specifically, for 50% of mothers about 12 months had passed since their pregnancy (85% within the past 36 months), reducing the likelihood that substantial changes have occurred in this short period of time. Also, the mediation model in this study has been developed bearing in mind plausible causal pathways that preclude reverse causality, which is one crucial aspect of causality in structural modelling (Cohen et al., Citation2003).
Fourth, the study would have benefitted from additional factors that may affect the return to school, including parental education and different types of social support that mothers’ received (i.e. financial, practical, or emotional). Fifth, it is possible that the rates of schooling may be inflated by socially desirable responding, including over-reporting of continued schooling during pregnancy and school return. Sixth, the generalizability of our findings beyond the Eastern Cape requires additional research with samples from other South African provinces.
The study also has multiple strengths. The results are based on the largest sample of adolescent mothers in South Africa and participants were not exclusively recruited within clinical settings. Rather, the study deployed multiple parallel recruitment channels to strengthen the recruitment of a representative community-based sample of mothers engaged and not engaged in services. In addition, this is the first study which tests multiple pathways towards school return and provides evidence that supports the testing of feasible combination interventions.
Conclusion
Enabling girls’ postpartum education is important to ensure good outcomes for adolescent mothers and their children. To date, not all adolescent mothers are benefitting from the policy advances across sub-Saharan Africa which aim to protect their right to education (Martinez & Odhiambo, Citation2018). However, policies that protect adolescent mothers and speak to their needs are clearly an essential step to facilitate re-enrolment following childbirth. South Africa’s 2021 policy advances demonstrate a continued will to improve policies for adolescent mothers and a commitment to protect their right to education (Department of Basic Education, Citation2021). Our results do not only underscore the potential need to better support girls affected by poverty and deficits in cumulative learning, but also suggest that young mothers in South Africa require improved access to affordable childcare options to continue their education. Moreover, an increase in scientific engagement and systematic documentation of the effectiveness of programmes that are already available to support adolescent mothers will foster a system that can successfully support the pre-birth and post-birth challenges to continued education of this vulnerable population.
Acknowledgements
The authors are grateful to the young mothers and their families, the data collection team, and partner organizations who supported the research process. We are also grateful to Maria-Therese Fries, William Rudgard, Yulia Shenderovich, and Lakshmi Neelakantan for valuable discussions and comments on the manuscript.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Ardington, C., Menendez, A., & Mutevedzi, T. (2015). Early childbearing, human capital attainment, and mortality risk: Evidence from a longitudinal Demographic surveillance area in rural KwaZulu-natal, South Africa. Economic Development and Cultural Change, 63(2), 281–317. https://doi.org/10.1086/678983
- Assini-Meytin, L. C., Mitchell, S. J., & Lewin, A. (2018). Support relationships and teen mothers’ school retention at one-year postpartum. Journal of Community Psychology, 46(6), 734–746. https://doi.org/10.1002/jcop.21969
- Barlow, J., Smailagic, N., Bennett, C., Huband, N., Jones, H., & Coren, E. (2011). Individual and group based parenting programmes for improving psychosocial outcomes for teenage parents and their children. Cochrane Database of Systematic Reviews, 3, CD002964, 1–79. https://doi.org/10.1002/14651858.CD002964.pub2
- Barnes, H., & Wright, G. (2012). Defining child poverty in South Africa using the socially perceived necessities approach. In A. Minujn, & S. Nandy (Eds.), Global child poverty well-being: Measurements, concepts, policy and action (pp. 135–154). The Policy Press.
- Barnet, B., Arroyo, C., Devoe, M., & Duggan, A. K. (2004). Reduced school dropout rates among adolescent mothers receiving school-based prenatal care. Archives of Pediatrics & Adolescent Medicine, 158(3), 262–268. https://doi.org/10.1001/archpedi.158.3.262
- Bhana, D., & Nkani, N. (2016). ‘What can I do, the child is already here?’ caregivers, gender, poverty and the contradiction of care in supporting teenage mothers at school. South African Review of Sociology, 47(2), 3–18. https://doi.org/10.1080/21528586.2015.1132082
- Birungi, H., Undie, C.-C., MacKenzie, I., Katahoire, A., Obare, F., & Machawira, P. (2015). Education sector response to early and unintended pregnancy: A review of country experiences in sub-Saharan Africa. Population Council. https://knowledgecommons.popcouncil.org/cgi/viewcontent.cgi?article=1261&context=departments_sbsr-rh
- Branson, N., Hofmeyr, C., & Lam, D. (2014). Progress through school and the determinants of school dropout in South Africa. Development Southern Africa, 31(1), 106–126. https://doi.org/10.1080/0376835X.2013.853610
- Brown, T. A. (2015). Confirmatory factor analysis for applied research (2nd ed.). Guilford Press.
- Callahan, T., Modi, S., Swanson, J., Ng’eno, B., & Broyles, L. N. (2017). Pregnant adolescents living with HIV: What we know, what we need to know, where we need to go. Journal of the International AIDS Society, 20(1), 21858, 1–4. https://doi.org/10.7448/IAS.20.1.21858
- Chigona, A., & Chetty, R. (2008). Teen mothers and schooling: Lacunae and challenges. South African Journal of Education, 28(2), 261–281. https://doi.org/10.15700/saje.v28n2a174
- Cohen, J., Cohen, P., West, S. G., & Aiken, L. S. (2003). Applied multiple regression/correlation analysis for the behavioural sciences (3rd ed.). Lawrence Erlbaum Associates Publishers.
- De Henau, J., Budlender, W. D., Filgueira, F., Ilkkaraçan, I., Kim, K., & Mantero, R. (2019). Investing in free universal childcare in South Africa, Turkey and Uruguay. UN Women. https://www.unwomen.org/en/digital-library/publications/2019/07/discussion-paper-investing-in-free-universal-childcare-in-south-africa-turkey-and-uruguay#view
- De Neve, J. W., Fink, G., Subramanian, S. V., Moyo, S., & Bor, J. (2015). Length of secondary schooling and risk of HIV infection in Botswana: Evidence from a natural experiment. The Lancet Global Health, 3(8), E470–E477. https://doi.org/10.1016/S2214-109X(15)00087-X
- Devercelli, A. E., & Beaton-Day, F. (2020). Better jobs and brighter futures: Investing in childcare to build human capital. World Bank. http://hdl.handle.net/10986/35062
- Distefano, C., Liu, J., Jiang, N., & Shi, D. (2018). Examination of the weighted root mean square residual: Evidence for trustworthiness? Structural Equation Modeling: A Multidisciplinary Journal, 25(3), 453–466. https://doi.org/10.1080/10705511.2017.1390394
- Dupéré, V., Leventhal, T., Dion, E., Crosnoe, R., Archambault, I., & Janosz, M. (2015). Stressors and turning points in high school and dropout. Review of Educational Research, 85(4), 591–629. https://doi.org/10.3102/0034654314559845
- Feinstein, L., Sabates, R., Anderson, T. M., Sorhaindo, A., & Hammond, C. (2006). What are the effects of education on health. In measuring the effects of education on health and civic engagement. Proceedings of the Copenhagen Symposium. https://www.oecd.org/education/innovation-education/37437718.pdf.
- Forshaw, J., Gerver, S. M., Gill, M., Cooper, E., Manikam, L., & Ward, H. (2017). The global effect of maternal education on complete childhood vaccination: A systematic review and meta-analysis. BMC Infectious Diseases, 17(1), 801, 1–16. https://doi.org/10.1186/s12879-017-2890-y
- Freudenberg, N., & Ruglis, J. (2007). Reframing school dropout as a public health issue. Preventing Chronic Disease, 4(4), A107, 1–11. PMID: 17875251. https://pubmed.ncbi.nlm.nih.gov/17875251/
- Ganchimeg, T., Ota, E., Morisaki, N., Laopaiboon, M., Lumbiganon, P., Zhang, J., Yamdamsuren, B., Temmerman, M., Tunçalp Ö., S. L., Vogel, J. P., Souza, J. P., & Mori, R. (2014). Pregnancy and childbirth outcomes among adolescent mothers: A World Health Organization multicountry study. BJOG: An International Journal of Obstetrics & Gynaecology, 121(Suppl), 40–48. https://doi.org/10.1111/1471-0528.12630
- Grant, M. J., & Hallman, K. K. (2008). Pregnancy-related school dropout and prior school performance in KwaZulu-natal, South Africa. Studies in Family Planning, 39(4), 369–382. https://doi.org/10.1111/j.1728-4465.2008.00181.x
- Groves, A. K., Gebrekristos, L. T., McNaughton Reyes, L., Moddley, D., Raziano, V., & Maman, S. (2021). A mixed-methods study of resilience and return to school among adolescent mothers in South Africa. Global Public Health, 1–14. https://doi.org/10.1080/17441692.2021.1970208
- Groves, A. K., Maman, S., Stankard, P. H., Gebrekristos, L. T., Amon, J. J., & Moodley, D. (2018). Addressing the unique needs of adolescent mothers in the fight againstHIV. Journal of the International AIDS Society, 21(6), e25155, 1–3. https://doi.org/10.1002/jia2.25155
- Harding, J. F., Knab, J., Zief, S., Kelly, K., & McCallum, D. (2020). A systematic review of programs to promote aspects of teen parents’ self-sufficiency: Supporting educational outcomes and healthy birth spacing. Maternal and Child Health Journal, 24(S2), 84–104. https://doi.org/10.1007/s10995-019-02854-w
- Hatch, M., & Posel, D. (2018). Who cares for children? A quantitative study of childcare in South Africa. Development Southern Africa, 35(2), 267–282. https://doi.org/10.1080/0376835X.2018.1452716
- Herrero Romero, R., Hall, J., Cluver, L., Meinck, F., & Hinde, E. (2021). How does exposure to violence affect school delay and academic motivation for adolescents living in socioeconomically disadvantaged communities in South Africa? Journal of Interpersonal Violence, 36, NP3661–NP3694. https://doi.org/10.1177/0886260518779597
- Huebender, M. (2019). Life expectancy and parental education. Social Science & Medicine, 232, 351–365. https://doi.org/10.1016/j.socscimed.2019.04.034
- Jochim, J., Cluver, L., D., & Meinck, F. (2021). Learner pregnancy in South Africa's Eastern Cape: The factors affecting adolescent girls’ school withdrawal during pregnancy. International Journal of Educational Development, 87, 102484, 1–10. https://doi.org/10.1016/j.ijedudev.2021.102484
- Jochim, J., Groves, A. K., & Cluver, L. D. (2020). When do adolescent mothers return to school? Timing across rural and urban South Africa. South African Medical Journal, 110(9), 850–854. https://doi.org/10.7196/SAMJ.2020.v110i9.14664
- Jonas, K., Crutzen, R., Van Den Borne, B., Sewpaul, R., & Reddy, P. (2016). Teenage pregnancy rates and associations with other health risk behaviours: A three-wave cross-sectional study among South African school-going adolescents. Reproductive Health, 13(1), 1–14. https://doi.org/10.1186/s12978-016-0170-8
- Kabanze, B. (2019). A key ingredient for helping young mothers succeed. https://globalfundforchildren.org/story/a-key-ingredient-for-helping-young-mothers-succeed/
- Kassa, G. M., Arowojolu, A. O., Odukogbe, A. A., & Yalew, A. W. (2018). Prevalence and determinants of adolescent pregnancy in Africa: A systematic review and meta-analysis. Reproductive Health, 15(195), 1–17. https://doi.org/10.1186/s12978-018-0640-2
- Kassebaum, N., Kyu, H. H., Zoeckler, L., Olsen, H. E., Thomas, K., Pinho, C., … Vos, T. (2017). Child and adolescent health from 1990 to 2015, JAMA Pediatrics 171 study. JAMA Pediatrics, 171(6), 573–592. https://doi.org/10.1001/jamapediatrics.2017.0250
- Kennedy, D. (2017). Jamaica’s policy for the school reintegration of school-age mothers: How are we doing and where do we need to go? Center for Universal Education at Brookings. https://www.brookings.edu/wp-content/uploads/2017/11/dasmine-kennedy_final_20171101_web.pdf
- Khatun, M., Mamun, A. A., Scott, J., William, G. M., Clavarino, A., & Najman, J. M. (2017). Do children born to teenage parents have lower adult intelligence? A prospective birth cohort study. Plos One, 12(3), E0167395, 1–15. https://doi.org/10.1371/journal.pone.0167395.
- Kruger, D., Berthelon, M. E., & Navia, R. (2009). Adolescent motherhood and secondary schooling in Chile (IZA Discussion Papers No. 4552). Institute for Labor Economics: Bonn. https://www.iza.org/publications/dp/4552/adolescent-motherhood-and-secondary-schooling-in-chile.
- Little, Roderick J. A. (1988). A test of missing completely at random for multivariate data with missing values. Journal of the American Statistical Association, 83(404), 1198–1202. http://doi.org/10.1080/01621459.1988.10478722
- Lwanga Walgwe, E., Termini LaChance, N., Birungi, H., & Undie, C. (2016). Kenya: Helping adolescent mothers remain in school through strengthened implementation of school re-entry policies. Population Council. https://knowledgecommons.popcouncil.org/cgi/viewcontent.cgi?article=1242&context=departments_sbsr-rh
- Madhavan, S., & Thomas, K. J. A. (2005). Childbearing and schooling: New evidence from South Africa. Comparative Education Review, 49(4), 452–467. https://doi.org/10.1086/432770
- Magadi, M. A., Agwanda, A. O., & Obare, F. O. (2007). A comparative analysis of the use of maternal health services between teenagers and older mothers in sub-Saharan Africa: Evidence from Demographic and health surveys (DHS). Social Science & Medicine, 64(6), 1311–1325. https://doi.org/10.1016/j.socscimed.2006.11.004
- Maquina. (2015). Concern as more than 120 000 schoolgirls fall pregnant. https://www.unescwa.org/sites/www.unescwa.org/files/un_resolutions/a_res_69_315_e.pdf
- Marteleto, L., Lam, D., & Ranchhod, V. (2006). Schooling and early childbearing in urban South Africa. Institute for Social Research, Population Studies Center. http://www.psc.isr.umich.edu/pubs/pdf/rr06-610.pdf
- Marteleto, L. J., Lam, D., & Ranchhod, V. (2008). Sexual behavior, pregnancy, and schooling among young people in urban South Africa. Studies in Family Planning, 39(4), 351–368. https://doi.org/10.1111/j.1728-4465.2008.00180.x
- Martinez, E., & Odhiambo, A. (2018). Leave no girl behind in Africa: Discrimination in education against pregnant girls and adolescent mothers. Human Rights Watch. https://www.hrw.org/sites/default/files/report_pdf/au0618_insert_webspreads.pdf
- Maslowsky, J., Hendrick, C. E., & Stritzel, H. (2021). Mechanisms linking teenage mothers’ educational attainment with self-reported health at age 50. BMC Women's Health, 21(1), 1–9.https://doi.org/10.1186/s12905-020-01150-y
- Mekonnen, T., Dune, T., & Perz, J. (2019). Maternal health service utilisation of adolescent women in sub-Saharan Africa: A systematic scoping review. BMC Pregnancy and Childbirth, 19(1), 1–16. https://doi.org/10.1186/s12884-019-2501-6
- Mensch, B. S., Chuang, E. K., Melnikas, A. J., & Psaki, S. R. (2019). Evidence for causal links between education and maternal and child health: Systematic review. Tropical Medicine & International Health, 24(5), 504–522. https://doi.org/10.1111/tmi.13218
- Mollborn, S., & Dennis, J. A. (2012). Ready or not: Predicting high and low school readiness among teen parent’s children. Child Indicators Research, 5(2), 253–279. https://doi.org/10.1007/s12187-011-9126-2
- Mori, A. T., Kampata, L., Musonda, P., Johansson, K. A., Robberstad, B., & Sandøy, I. (2017). Cost-benefit and extended cost-effectiveness analysis of a comprehensive adolescent pregnancy prevention program in Zambia: Study protocol for a cluster randomized controlled trial. Trials, 18(1), 1–10. https://doi.org/10.1186/s13063-017-2350-4
- Morrell, R., Bhana, D., & Shefer, T. (2012). Books and babies: Pregnancy and young parents in schools. HSRC Press.
- Mulinya, B. (2021). Kenyan private school opens for teen mothers and babies. https://www.voanews.com/africa/kenyan-private-school-opens-teen-mothers-babies
- Neal, S., Matthews, Z., Frost, M., Fogstad, H., Camacho, A. V., & Laski, L. (2012). Childbearing in adolescents aged 12-15 years in low resource countries: A neglected issue. New estimates from demographic and household surveys in 42 countries. Acta Obstetricia et Gynecologica Scandinavica 91 countries. Acta Obstetricia et Gynecologica Scandinavica, 91(9), 1114–1118. https://doi.org/10.1111/j.1600-0412.2012.01467.x
- Ngabaza, S., & Shefer, T. (2013). Policy commitments vs. Lived realities of young pregnant women and mothers in school, western cape, South Africa. Reproductive Health Matters, 21(41), 106–113. https://doi.org/10.1016/S0968-8080(13)41683-X
- Ntambo, A., & Malvin, K. (2017). The impact of re-entry policy on girls who fall pregnant and re-admitted back to school in selected schools in mpongwe district. International Journal of Multidisciplinary Research and Development, 4(6), 66–74. http://www.allsubjectjournal.com/download/3112/4-5-51-764.pdf.
- Ochiel, H. (2016). Kenya tackles poverty by sending teen mothers back to school. https://www.reuters.com/article/us-kenya-education-teenmothers-idUSKCN0W602A
- Panday, S., Makiwane, M., Ranchod, C., & Letsoalo, T. (2009). Teenage pregnancy in South Africa - with a specific focus on school-going learners. South AfricaN Department of Education, 1–84. https://repository.hsrc.ac.za/handle/20.500.11910/4711
- Pettifor, A. E., Levandowski, B. A., MacPhail, C., Padian, N. S., Cohen, M. S., & Rees, H. V. (2008). Keep them in school: The importance of education as a protective factor against HIV infection among young South African women. International Journal of Epidemiology, 37(6), 1266–1273. https://doi.org/10.1093/ije/dyn131
- Poser, M., & Ortiz-Ospina, E. (2019, December). Global extreme poverty. https://ourworldindata.org/extreme-poverty<otherinfo>#citation<
- Poser, M., & Ritchie, H. (2019, December). Homicides. https://ourworldindata.org/homicides#citation.
- Russel, M. (2003). Understanding black households: The problem. Social Dynamics, 29(2), 5–47. https://doi.org/10.1080/02533950308628674
- Salvi, F. (2019). Teenage pregnancy and education in the Global south - The case of Mozambique. Routledge.
- Samman, E., & Lombardi, J. (2019). Childcare and working families: New opportunities or missing link? An evidence brief. Unicef. https://www.unicef.org/documents/childcare-and-working-families-new-opportunity-or-missing-link.
- Schochet, O. N., & Johnson, A. D. (2019). The impact of child care subsidies on mothers’ education outcomes. Journal of Family and Economic Issues, 40(3), 367–389. https://doi.org/10.1007/s10834-019-09628-0
- Shahar, E., & Shahar, D. J. (2013). Causal diagrams and the cross-sectional study. Clinical Epidemiology, 5(1), 57–65. https://doi.org/10.2147/CLEP.S42843
- Shazi, Z., Groves, A. K., Bruns, L., Gebrekristos, L. T., Moletsane, R., Maman, S., & Moodley, D. (October, 2018). Describing the feasibility and acceptability of an intervention designed to increase adolescent mothers return to school postpartum. International Workshop on HIV and Adolescence.
- Simkhada, B., Teijlingen, E. R., Porter, M., & Simkhada, P. (2008). Factors affecting the utilization of antenatal care in developing countries: Systematic review of the literature. Journal of Advanced Nursing, 61(3), 244–260. https://doi.org/10.1111/j.1365-2648.2007.04532.x. PMID: 18197860.
- Singh and Mukherjee. (2018). Push out, pull Out, or opting Out? Reasons cited by adolescents for discontinuing education in four low- and middle-income countries. In J. E. Lansford, & P. Banati (Eds.), Handbook of adolescent development research and its impact on global policy (pp. 1–482). Oxford University Press. https://doi.org/10.1093/oso/9780190847128.003.0012
- SmithBattle, L., Loman, D. G., Chantamit-o-pas, C., & Schneider, J. K. (2017). An umbrella review of meta-analyses of interventions to improve maternal outcomes for teen mothers. Journal of Adolescence, 59, 97–111. https://doi.org/10.1016/j.adolescence.2017.05.022
- South African Department of Basic Education. (2021). Policy on the prevention and management of learner pregnancy in schools. South African Government. https://www.gov.za/documents/national-policy-act-policy-prevention-and-management-learner-pregnancy-schools-3-dec-2021.
- South African Department of Education. (2007). Measures for the prevention and management of learner pregnancy. South African Government. https://www.gov.za/sites/default/files/gcis_document/201409/learnerpregnancy0.pdf.
- South African Department of Health. (2013). Infant and young child feeding policy. South African Government. https://www.gov.za/sites/default/files/gcis_document/201409/infantfeed.pdf.
- Spaull, N. (2013). Poverty & privilege: Primary school inequality in South Africa. International Journal of Educational Development, 33(5), 436–447. https://doi.org/10.1016/j.ijedudev.2012.09.009
- Steinka-Fry, K. T., Wilson, S. J., & Tanner-Smith, E. E. (2013). Effects of school dropout prevention programs for pregnant and parenting adolescents: A meta-analytic review. Journal of the Society for Social Work and Research, 4(4), 373–389. https://doi.org/10.5243/jsswr.2013.23
- Stoner, M. C. D., Pettifor, A., Edwards, J. K., Aiello, A. E., Halpern, C. T., Julien, A., Selin, A., Twine, R., Hughest, J. P., Wang, J., Agyei, Y., Gomez-Olive, F. X., Wagner, R. G., MacPhail, C., & Kahn, K. (2017). The effect of school attendance and school dropout on incident HIV and HSV-2 among young women in rural South Africa enrolled in HPTN 068. Aids (london, England), 31(15), 2127–2134. https://doi.org/10.1097/QAD.0000000000001584
- Stoner, M. C. D., Rucinski, K. B., Edwards, J. K., Selin, A., Hughes, J. P., Wang, J., Agyei, Y., Gomez-Olive, F. X., MacPhail, C., Kahn, K., & Pettifor, A. (2019). The relationship between school dropout and pregnancy among adolescent girls and young women in South Africa: A HPTN 068 analysis. Health Education & Behavior, 46(4), 559–568. https://doi.org/10.1177/1090198119831755
- Stull, D. E., Kline Leidy, N., Parasuraman, B., & Chassany, O. (2009). Optimal recall periods for patient-reported outcomes: Challenges and potential solutions. Current Medical Research and Opinion, 25(4), 929–942. https://doi.org/10.1185/03007990902774765
- The Hunger Project. (2019). Teenage mother Bizuhaye goes back to school in Ethiopia. https://www.thehungerproject.org.uk/teenage-mother-bizuhaye-goes-back-to-school-in-ethiopia/.
- Timaeus, I. M., & Moultrie, T. A. (2015). Teenage childbearing and educational attainment in South Africa. Studies In Family Planning, 46(2), 143–160. https://doi.org/10.1111/j.1728-4465.2015.00021.x
- Toska, E., Laurenzi, C. A., Roberts, K. J., Cluver, L. D., & Sherr, L. (2020). Adolescent mothers affected by HIV and their children: A scoping review of evidence and experiences from sub-Saharan Africa. Global Public Health, 15(11), 1655–1673. https://doi.org/10.1080/17441692.2020.1775867
- UNAIDS. (2020). Unaids data 2020. https://www.unaids.org/en/resources/documents/2020/unaids-data.
- United Nations. (2020). World Fertility 2019 - Early and later childbearing among adolescent women. https://www.un.org/en/development/desa/population/publications/pdf/fertility/World_Fertility_2019.pdf.
- Viner, R. M., Ozer, E. M., Denny, S., Marmot, M., Resnick, M., Fatusi, A., & Currie, C. (2012). Adolescence and the social determinants of health. The Lancet, 379(9826), 1641–1652. https://doi.org/10.1016/S0140-6736(12)60149-4
- World Health Organisation. (2021). Breastfeeding recommendations. https://www.who.int/health-topics/breastfeeding#tab=tab_2.
- World Health Organization. (2016). Global Health Estimates 2015: Deaths by cause, age, sex, by country and by region, 2000-2015.
- World Health Organization. (2019). Trends in maternal mortality 2000 to 2017: Estimates by WHO, Unicef, UNFPA, World Bank Group and the United Nations Population Division. https://www.unfpa.org/sites/default/files/pub-pdf/Maternal_mortality_report.pdf.
- Zuilkowski, S. S., Henning, M., Zulu, J., & Matafwali, B. (2019). Zambia’s school re-entry policy for adolescent mothers: Examining impacts beyond re-enrollment. International Journal of Educational Development, 64, 1–7. https://doi.org/10.1016/j.ijedudev.2018.11.001
- Zweigenthal, V., Strebel, A., & Hunter-Adams, J. (2019). Adolescent girls’ perceptions of breastfeeding in two low-income periurban communities in South Africa. Health Care for Women International, 40(7–9), 995–1011. https://doi.org/10.1080/07399332.2018.1549043