
ABSTRACT
A growing number of studies highlight high levels of misdiagnosis in the scale-up of HIV rapid testing programmes, which often remain invisible to individual testers. Drawing on interviews with HIV testers and observations in four health facilities in Zimbabwe, we show that testers navigated the translation of the standardised, dis-embodied norms of laboratory-based testing into the body work of point-of-care testing through ritualisation of laboratory-practices in their daily clinical work. Yet, this was interrupted through the challenging work conditions the testers face. They ritualised careful procedures, forcing themselves to focus even if queues were long, and making quality assurance procedures part of their daily routine. They actively tried to reduce their workloads and double-checked and discussed unexpected results, especially when a test result did not match their evaluation of clients’ circumstances or clinical status. This helped not only to increase confidence in the authenticity of their diagnosis, but also to share responsibility for potential errors. Existing approaches to tackle the problem of misdiagnosis through quality assurance (QA) procedures mainly focus on adjusting individual testers’ performance and ensuring that basic testing resources were present, thus falling short of creating a work environment that is conducive to high quality testing.
Introduction and background
Rapid tests for HIV provide quick, easy and convenient testing at the point of care, and have therefore helped drastically in expanding access to life-saving antiretroviral treatment and HIV prevention for millions of people. The latest generation of rapid HIV tests offer high sensitivity and validity and can be easily administered, even in low-tech environments and hot climates. Yet, compared to laboratory-based testing technologies, they remain crude, designed to scale up access to HIV programmes, rather than increase the accuracy of HIV surveillance data. Indeed, a growing number of studies (Gregson et al., Citation2021; Klarkowski et al., Citation2009; Kufa et al., Citation2017; Matemo et al., Citation2009; Young et al., Citation2013) highlight high levels of misdiagnosis in the scale-up of HIV rapid testing programmes. A systematic review of 64 studies investigating rapid HIV test misdiagnosis in low-income settings concluded that an average of 0.4% and 3.1% of adults being tested receive a false negative or false positive test result respectively (Johnson et al., Citation2017). Our own study on levels of misdiagnosis in rapid HIV testing in Zimbabwe found a 0.1% rate of false-positive, and a 10% rate of false-negative diagnoses (Gregson et al., Citation2021). Considering the large number of people who get tested using rapid HIV tests each year, even small percentages translate into a significant number of people being misdiagnosed. Of course, all diagnostic tests harbour a margin of error; yet, such cases of HIV misdiagnosis have severe consequences for the affected clients. False-negative clients may unknowingly transmit the virus to others and experience a potentially life-threatening delay in treatment initiation. False-positive clients may suffer from stigmatisation and discrimination, and, in the era of test-and-treat programmes, may be put on lifelong treatment, which can cause serious side effects and pose high costs to the health system.
While rapid HIV tests are highly accurate under laboratory conditions, their use in the field is affected by workplace pressures and challenging material conditions. At the point of care, values and norms that characterise laboratory practices must be integrated into the body work performed by HIV testers. This process is guided by a different set of values and inevitably introduces a ‘messiness’ brought about by the interaction with clients’ bodies and lives into the standardised procedures required by the testing script. The clinicians and primary counsellors who perform rapid HIV testing generally lack opportunities to authenticate their test results, thus rendering cases of misdiagnosis largely invisible (Skovdal et al., Citation2022). In the face of such uncertainty, this paper asks how point-of-care testers make sense of the conflicting demands posed by laboratory-based scripts and values in the context of their clinical work. It argues that their effort to perform careful work to mitigate misclassifications is unsustainable, as it relies entirely on their care ethics in the absence of supportive structures.
The lab and the clinic: Integrating laboratory principles into the practices of body work
As HIV mostly becomes visible through testing, HIV rapid testers at the point of care (POC) cannot know for certain if they have issued the correct result. POC testers do not have access to data from laboratory tests to authenticate their diagnoses, nor do they work in a highly controlled environment like the laboratory. In fact, these are two entirely different work contexts, each defined by significantly different – and at times opposing – values, norms and practices. Laboratory work is based on principles of objectivity and standardisation; it values the emotional detachment brought about by physical distance between laboratory technician and client as important conditions to eliminate bias from the testing procedure. The clinic, on the other hand, is an environment where high-quality work is based on values of care and compassion, physical proximity and detailed knowledge about the individual.
HIV testers working at the point of care engage in body work in the strictest sense (Twigg et al., Citation2011); their work requires close bodily co-presence and emotional attunement to their clients’ needs. This contrasts sharply with the basic values underpinning laboratory work, and yet, the quality of POC testers’ work is measured by how closely it mirrors procedures imbued in laboratory testing. They are trained to administer rapid HIV tests by strictly following the test kits’ standard operating procedures and the national testing algorithm (which together make up the ‘testing script’), adopting techniques of checking and cross-checking that are designed to eliminate bias, and conducting quality control processes to ensure that test kits function correctly. While the administration of the test is embedded in a framework of pre- and post-test counselling, the training the testers receive highlights the need to ‘zoom in’ while administering the actual test. This process requires testers to focus entirely on the relevant body parts, substances and procedures to ensure objective and accurate testing: the fingertip to be cleaned and pricked; the drop of blood to be collected and applied to the test kit; the amount of buffer fluid to be used; recording the time, client number and contact details in the file, while waiting for exactly the prescribed time before reading the test results. While good rapport needs to be built to deliver effective pre-and post-test counselling, the testing script requires a sense of detachment from the client during the process of testing that may not be disturbed until the results can be safely recorded. The testers therefore need to straddle both proximity and detachment from their clients in the course of HIV testing. In the absence of feedback loops that compare and authenticate the results which HIV rapid testers interpret and issue to their clients, testers must separate the messiness of human interaction from the standardised, detached procedure of administering the test in a way that enables them to feel confident that they are issuing the correct results. Ritualising the regimes of standardisation seen in the laboratory, by following the testing script, cross-checking and comparing results, and conducting test kit quality controls, was regarded as the most important strategy to avoid misdiagnosis.
Objectives
This essential conundrum formed the focus of our research, which explored how clinic staff experience and engage with rapid HIV tests, focusing on how specific clinic settings and conditions give rise to different experiences and a divergence away from the national testing algorithm and standard operating procedures (SOPs) that specify how to use rapid HIV test kits. This study was part of a larger mixed-methods study (the ‘misclassification study’) implemented by the Manicaland Centre for Public Health Research that investigated the scale, sources and consequences of misclassification errors in rapid HIV testing in Zimbabwe (see Skovdal et al., Citation2020 for further details). Approvals for the study were granted by the ethical review boards of the Medical Research Council of Zimbabwe (MRCZ/A/1865) and Imperial College London (15IC2797).
Methods
Setting
The qualitative study was conducted in May 2018 in 14 health facilities spread across six districts (Chipinge, Gutu, Buhera, Harare, Mudzi and Rushinga) in Zimbabwe. The health facilities were purposefully sampled out of the 10 sites with the lowest and highest misdiagnosis rates, respectively, as identified in the national HIV surveillance survey. We selected eight district hospitals and six local clinics, including a mix of government-, church- and city council-run facilities. Twenty-two testers from low-performing sites and six testers from high-performing sites (in terms of misdiagnosis rates) were interviewed.
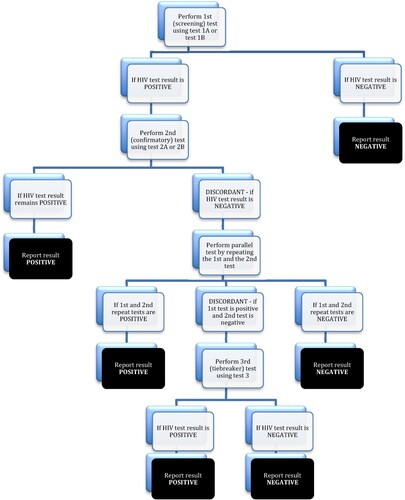
depicts the national HIV testing algorithm at the time of the start of the misclassification study in 2017 and in use during our research. The testing strategy specifies that a positive HIV test must be confirmed with a second rapid HIV test of a different type. If the second test is in agreement with the first positive test result, the result is recorded as positive. However, if the first and second tests are in disagreement, the tests must be repeated in parallel. Only if the test results should remain discordant, will a third ‘tie-breaker’ test be done (see Skovdal et al., Citation2020 for further details).
Figure 1. HIV testing algorithm used in routine healthcare services in Zimbabwe in 2017 and during our study in 2018–2019.
At the time of the study, quality assurance procedures included ensuring that test kits were stored correctly and used by trained testers according to the SOPs; checking expiry date and packaging of the test kit; running controls of known negative and known positive samples every morning and when opening a new pack of test kits; and ensuring accurate documentation. Additionally, some sites also carried out external quality assurance (EQA) procedures, which initially included site-based proficiency testing (PT), and from late 2017 individual-based PT with Corrective Action support visits for poorly performing testers.
Data collection procedures
In each health facility, we recruited two or three rapid HIV testers and conducted in total 28 semi-structured interviews with 17 HIV primary counsellors, 10 nurses and 1 laboratory technician. Twenty of our respondents were female, eight were male. They ranged in age from 28 to 58 years, though the majority were in their late 30s and 40s. Seven interviewees had been working at the current facility for less than five years, another seven from six to nine years, eleven from 10 to 15 years and three for over 15 years.
Interviews were conducted by four experienced local field researchers, guided by a topic guide, recorded, translated, and transcribed into English. We also carried out 24 day-long observational visits in four health facilities (one high-performing and three low-performing sites). The observations were carried out by five researchers, steered by an observation guide focusing on HIV testing practices. All observations started with a tour of the facilities, with particular emphasis on the testing rooms, the pharmacy and the drug storage rooms, followed by a week of observing different HIV testers’ work days and testing practices across the range of departments available in each facility. Data from the observations was captured in field notes and compiled into observation reports.
Interview transcripts and observation reports were imported into NVivo 12 for thematic coding and analysis. Inductive and in-depth coding of 10 randomly selected transcripts was done to develop a coding framework, which was applied to the remaining data. Ongoing data analysis and emerging themes were discussed amongst the authors. This led to a further layer of thematic organising, focusing on testers’ strategies to avoid misdiagnosis and find confidence in their results. In this paper we report on 14 basic themes, selected because they detail the ritualisation of careful procedure, strategies for coping with resource limitations and high workloads, the embodied knowledge testers draw upon to increase confidence in their test results, and testers’ thoughts on quality assurance. We clustered the basic themes into these four organising themes (see ), which form the structure of our presentation of the results.
Table 1. Thematic network of emerging findings.
Findings
Rituals of care – ‘You have to be careful’
Testers recognised the need to care for their clients and for themselves, highlighting their passion for their work and their concern about doing right by their clients. Many claimed that they worried deeply about issuing wrong results and were acutely aware of the serious consequences such a misdiagnosis could have for their client’s life. At the same time, they had fully embraced the idea that rapid tests were failsafe if used correctly. In most interviewees’ views, human error was therefore a major source of misdiagnosis, and the idiom of ‘carelessness’, and the high stakes involved, were often invoked when speaking about misdiagnosis. When asked about newly introduced quality assurance procedures, such as spot checks, or extra blood samples being sent to the laboratory for extra testing, a primary care counsellor at a low-performing site explained:
I think that it’s good because it helps staff members to be accountable for everything they do considering that they are working with people’s lives. It also helps because cases where I am making mistakes, I get corrected on time and improve. It makes it easy to keep track of the test kits to make sure they are functional.
I thought it was a good thing because it helps ensuring that I am confident with what I am doing when I test and issue results. Also because pictures were being taken, it showed that testing was done correctly. There was no room for shortcuts. This was also ensured even way after the survey; it became impossible for people to do anything outside the correct procedure of conducting these tests (authors’ emphasis).
I think there should be quality testing done. Take time and then make sure that you record every client’s name on the card, paper or on the test kit, so that you give the correct result to the correct client. (Primary care counsellor in low-performing site)
Those who are doing the rapid HIV testing, they should take their time, they don’t need to rush even if we are having a lot of people who need the service … I think it’s good to deal with quality than quantity. (Primary care counsellor in high-performing site)
As the tester you are supposed to take your time when testing and put your mind at ease, because you are supposed to be an open minded person, because there are cases where you will be having your own problems and your mind is somewhere else. So for that particular time that you are doing your job, your mind should be there on the job, so that you will be able to read your results at the right time without getting stressed up. And also on the process of agreeing to allow the second person who tests to come in; I see it as helpful because people will be receiving their correct results, because if two people do it there won’t be any mistake. (Primary care counsellor in very low-performing site)
I would definitely say [rapid HIV testing] has made the work easier, especially with regards to service delivery. So, for example, if one received HIV testing here at the hospital and received the same at the clinic, it should be uniform. The SOPs really make life easier in terms of uniformity and this has made our lives easier because it puts us in a position where we are able to give out accurate results because this is a tested procedure. (Registered nurse at low-performing site)
There is need to have enough staff so as to make sure that testers do not work under so much pressure and be prone to making errors. HIV is a very sensitive topic and giving someone the wrong result may cause a lot of damage, in some cases people may even commit suicide. So it is very important to make sure errors are minimised. The testers themselves also need to be reminded over and over again to use enough sample required by the kit in order to read the correct result. It is also important to always remind testers to make sure they wait for the required time to read the results; there is no need to rush when people’s lives are on the line. (Primary care counsellor in a low-performing site)
You should be very organized and your mind must also be fresh (laughs) so that you don’t get mixed up in a lot of things before starting your work for the day. If your mind is really occupied, maybe yesterday you were too emotional, or you have your own social problems, or you are experiencing marital problems; it is better to tell your superiors that you are not feeling well today, because your job is a very emotionally straining job which may make you cause a lot of mistakes. (Primary care counsellor in a high-performing site)
To take shortcuts is to care: Strategies for coping with resource limitations and high workloads
Most of the testers we interviewed worked in high-stress environments characterised by severely limited resources. Test kit stock-outs were reported in almost all the sites, which meant that testers were forced to deviate from the testing algorithm, or use test kits they were not familiar with. This posed an ethical dilemma that made them deeply concerned about the quality of their diagnoses:
[…] if they can only fix this challenge of shortages of the kits, because there is no quality at all. […] what do we do? Do we let them go until we get the kits, or should we just do as we have been doing now, to give them the results and initiate them on treatment? We don’t know, but that is what we are doing. We are not using the algorithm but we are initiating the clients on treatment. We look at the total number of clients that are testing positive and think that what good it would do if I just test them and send them away? Where can we refer them to? (Primary care counsellor in high-performing site)
Individual sites and individual testers also deviated from the national testing algorithm in other ways. For example, while Zimbabwe had shifted from serial HIV testing to parallel HIV testing, not every facility we visited was actually doing parallel HIV testing yet. Some health facilities sent clients whose test results were discordant (e.g. who tested HIV positive with a screening test, while the second, confirmatory test showed a negative result) home and told them to come back after a week for another test, other facilities used a tie-breaker test, such as Insti, in such a scenario. As we discuss in more detail elsewhere (Skovdal et al., Citation2020), testers also tended to have clear preferences for particular test kits, and some testers said that they were so uncomfortable using some of the prescribed test kits in the national testing algorithm that they did not administer them. Instead, they performed confirmatory tests with the same type of test that was used for the initial diagnosis, or merely initiated ARV treatment without running a confirmatory test. Many of our respondents said that they were particularly worried about using the tie-breaker test and had never administered it, nor been trained in its use. If a colleague who knew how to administer the tie-breaker was available, they would be called to help, but often this was not possible.
In addition to test kit stock-outs and uncertainty, most testers also complained about high workloads and time and performance pressures, fully aware of the dangers these posed. Long queues outside the testing room, together with frequent disruptions by staff and clients, made it difficult to stick to the testing script. Our observations showed that while a calm and focused disposition was widely regarded as the best protection from misdiagnosis, work conditions in the clinic often made this near impossible, especially at peak times. Some HIV counsellors reported that they test about 50 clients a day and frequently miss their tea or lunch breaks; others reported being redeployed elsewhere at short notice. We also observed numerous occasions where other health workers interrupted sessions, thereby disturbing the flow of the counselling and testing session. In the face of such pressures, some HIV testers spoke of their worry about having to issue HIV positive results, demonstrating clear desirability bias. They pointed out that post-test counselling may take a long time, especially when a positive result comes out for couples or certain individuals, and thus further added to their time pressures.
Testers attempted to alleviate such pressures by actively trying to reduce their workloads through sharing tasks, and streamlining testing and recording procedures. Working together, double-checking, and discussing unexpected results with each other helped not only to increase confidence in the authenticity of their diagnosis, but also to share responsibility for potential errors.
How successful such strategies are is hard to establish. We observed at some health facilities that pregnant mothers were attended to by four health workers in the same room, with counselling, testing, examination and data collation being done simultaneously. We also observed testers drawing blood from several clients and batch-testing them at the same time. The HIV counsellors and nurses were aware of the dangers of task sharing and batch-testing and emphasised that under less stressful work conditions, one-to-one testing was safest:
If a patient is given a wrong test result, the reason may be because the patient has been delayed to be given their results, or maybe the tester may say that they are going for lunch, or maybe you are testing as two testers and then the patient asks for their result. In such cases, the one who didn’t assist the patient may end up taking the wrong test results and giving them to the patient, and since the patient won’t be patient enough to wait for after lunch to get their results that becomes a problem. But if you are working as one tester and testing one patient at a time, I don’t think you will do such a mistake, because you will be the one who has marked the kits, and knowing that for each patient who comes you are dealing with them one-on-one, haa such mistakes won’t happen. (Primary care nurse in a high-performing site)
Embodied knowledge
While following the script was emphasised by all testers as the most important way to avoid misdiagnoses, our observations showed that testers also frequently used embodied knowledge – or at least their syndromic familiarity with HIV (Palmer et al., Citation2020) – to evaluate the likelihood that a test result was trustworthy. Testers were aware that this practice went against the principles they had learned in their training, where the need for an unbiased, ‘open mind’ was emphasised. The following exchange highlights this:
‘Alright, can you tell me more about when you may feel unsure about the rapid HIV tests?’
‘No, umm, it is not advised to do visual testing, so sometimes you … as people … we come to a point where we judge, but as counsellors it’s one of our principles that we don’t judge, so when a client comes in showing all the signs that maybe this person is getting to the AIDS stage, then you get to test that patient and it comes out negative then as health workers we get to deal with such. Yeah … ’ (Primary care counsellor in a high-performing site)
Yeah, I have confidence [in my test results], but due to the fact that we talked of the specificity and sensitivity, sometimes when[…] a client is recently infected, we are still having challenges on … in our case picking up that, but otherwise I am confident. (Primary care counsellor in a high-performing site)
‘Yes, sometimes there are problems in interpreting results and we always make sure that we ask for a second opinion in such cases.’
‘Are there specific conditions that give rise to the problem of interpreting results and what are those?’
‘I think it has more to do with the anti-bodies. It differs with clients depending on how long someone has been living with the virus and how it has affected them, as well as the length of this.’ (Registered general nurse in a low-performing site)
There are those girls that go into bars. They sleep with the men that do this offloading job in big trucks. Some of these men are clever, for they insist on being tested together with these girls first, before engaging in any sexual activities with them. […] When such clients come for testing, we cannot afford not to test them, because that would be putting them at risk. (Registered general nurse in a high-performing site)
Such instances of diagnostic reflex, where the tester evaluated not only the test result on the diagnostic device, but also the client’s physical appearance, moral and social standing, or life circumstances, were also evident when clients came in to test as a couple and received discordant results, i.e. one partner tested negative, while the other tested positive. These cases always raised suspicion. Here, testers drew on their own cultural knowledge of how unlikely it would be that a couple in an established relationship would consistently abstain from sex or use protection. Such discordant results were also issued with a sense of apprehension in the testers, because they knew that a long and difficult post-test counselling session lay ahead of them: not only did they have to convey a life-changing diagnosis to a client; they also frequently found themselves in the middle of a relationship dispute, and tempers could be running high. In these circumstances, testers therefore often asked for second opinions and paid extra attention to authenticating their results through confirmatory tests.
Making misdiagnosis visible: Testers’ thoughts on changes to the current testing and quality assurance process
While the practices we have presented so far help testers feel confident about their test results, they do not necessarily decrease the rate of actual misdiagnoses, or make such cases visible to the testers. A number of approaches to tackle this problem have been suggested. Existing external quality assurance procedures (EQA), for example, have introduced feedback loops for point-of-care testers through proficiency testing: randomly selected samples of tests are sent off for laboratory re-testing and cases of misdiagnosis trigger follow-up visits, additional training and subsequent performance monitoring. These are costly measures, however, and coverage so far is low.
Additional EQA procedures could also have significant impact on testers’ work practices. EQA results could easily turn into surveillance mechanisms, through the creation of key performance indicators and sanctions for those who fail to meet targets. Testers were aware of such dangers, as a registered nurse in a low-performing site highlighted, drawing on laboratory science language:
Emphasis should be placed on using the SOPs at all times. When SOPs are followed to the dot, chances of errors are very slim, because problems arise when people try to cut corners. The other thing has to do with understanding and respecting the pace of each other as testers. When it comes to issues of HIV testing, there is no need for hurrying someone or telling them they are supposed to push certain numbers, because at the end of the day, 15 minutes is 15 minutes, and that has to be respected at all times. Once one works under pressure whereby they are expected to produce certain numbers at all costs, it opens the testing process up for contamination [author’s emphasis].
What I have discovered and what I wish for to happen is that when we give support and supervision […] where the RDTs are offered […], people go there in a rush and the shumbavision (supervisor who is scary and constantly nagging) that I was talking of; people will end up fearing the supervisor saying that he is one of the people who only want to see our mistakes. They don’t know that those mistakes, we want them, together with the good administration, we want it, but well, it is something very difficult, so what I could say is that we should give ourselves time if we say that we are going for supervision and support.
Okay, my issue is, we have done so many surveys and at the end of the day absolutely nothing changes. No resources are mobilised or anything of that sort, so then we begin to wonder what the point of all these surveys and researches is. We raised these issues I have spoken about over and over again and nothing has been done till this day. Yet we have a clear policy … we have a clear algorithm … a clear direction to take for HTS services and we raise these issues, but here we are, voicing out the same things, but is there even no point to it? Will it help with anything?
Discussion
Quality assurance at the point of care
Certainly, the careful procedures our research participants highlighted are important strategies to ensure quality testing. Yet, some of the other practices we found – such as tinkering with the algorithm, task sharing, batch testing, or using diagnostic reflexes – may in fact increase the likelihood of diagnostic errors or introduce bias into the testing process. Rather than providing a set of recommendations for point-of-care testing quality enhancement, our aim has been to contextualise testers’ work and highlight their strategies for feeling more confident in their practice.
Our results illustrate that rapid HIV testers in Zimbabwe have very few opportunities to develop certainty, or question the authenticity of diagnoses beyond their compliance with, or deviance from, the testing script and a few experiential proxies. This presents an ethical issue that lies at the heart of much ongoing debate about who and what is to blame for issuing wrong test results and how to ensure quality assurance at the point of care.
So far, the main approach has been the implementation of EQAs, particularly in the form of proficiency testing (PT). At first, PT was site-based and often performed by the same tester every time, thus missing the majority of testers. From late 2017, individual-based PT was introduced, which more than doubled the number of participating testers, but coverage remains limited. Currently, there are plans to transition from the reactive approach of PT towards implementing a more proactive, WHO/PEPfAR-supported Rapid Testing-Continual Quality Improvement (RT-CQI) approach, which includes the Stepwise Process for Improving Rapid HIV Testing (SPI-RT) checklist for site certification, and certification of individual testers.
The co-authors also discussed the potential for up-scaling the smartphone-based application for verifying results, which we had piloted in the misclassification study. Such approaches would mimic some of the standardised procedures that characterise laboratory testing, adding another pair of eyes to cross-check results and increasing the distance between client and tester. The smartphone application would also provide a new ‘gold standard’ to compare results against – a standard that is not based on a ‘better’ or ‘more accurate’ test, but on calculating the ‘best’ and ‘most likely’ diagnosis based on combining all available information about the initial test.
However, there is no evidence that the standardised software-based interpretation of results would indeed create a new kind of gold standard: before such technology is scaled up, thorough studies would need to establish that software-based interpretation of results is more accurate than that carried out by the testers. One concern is that while clinical observations and clients’ circumstances may lead to diagnostic bias in testers’ practice, they can also help authenticate results: experience in working with clients may be seen as a valuable resource (Cartwright, Citation2000), rather than only a hurdle to objectivity in testing, and our findings support this argument.
Digital standardisation procedures could threaten to shift accountability for the correct interpretation of the test result to the application and even further dis-embody medical knowledge (Nettleton et al., Citation2008). How telemonitoring technologies may shift responsibilities ‘for spotting trouble’ has also been noted by Pols (Citation2012, p. 67). This may lead to testers disengaging from the process, thus not assuming full responsibility for the results they give out, and to a further erosion of their confidence in their own skills.
EQAs and digital solutions are also not easily implemented on a large scale, and will likely raise a number of problems of their own. Firstly, they require significant added investment and administrative labour: in the case of EQAs, more laboratory tests need to be carried out, reports created and passed on to line managers who will then need to discuss them with individual testers. Costs would be even higher in the case of switching to a digital monitoring system that relies on functioning appliances and a high-speed internet connection. This raises questions around feasibility in a context that is already resource-strapped.
Standardisation in body work
Whilst making misdiagnoses visible is key to changing rapid HIV testing practices and circumventing future misdiagnoses, steady streams of ‘data’ revealing diagnostic errors may undermine testers’ trust in the test kits, the testing script, as well as their own testing practices. This will disrupt their confidence and the sense-making activities key to managing uncertainty (Weick, Citation1979), and raise all sorts of ethical questions: many rapid HIV testers talked about their passion for their work, citing their desire to help people, giving them clarity about their HIV status – what happens if they find out that they may be wrong quite frequently? Testers were very aware of the devastating consequences of misdiagnosis, but also highlighted how the constraints of a high-pressure, resource-limited work environment was to blame in large part for errors they might make. Many spoke of their efforts to do their best, while frequently being forced to diverge from the script and deliver care that they considered sub-standard.
Moreover, we point to the additional challenges posed by the need to integrate a set of norms and values derived from laboratory science into the nature of the bodywork which POC testers perform. Situated on the lower ranks of the care hierarchy, POC testers tend to be on low and often precarious salaries. By the nature of their work, they regularly come into contact with highly stigmatised persons and substances that are often regarded as physically and morally contaminated and polluting. Yet, as testers they are required to embody the purity of the testing script, administering HIV rapid tests unencumbered by the messiness and polluting nature of the subject and its substances. This constant need to straddle conflicting practices and norms of proximity and detachment in their daily practice makes POC testers particularly vulnerable when a culprit for high levels of misdiagnosis is sought.
Under these circumstances, to introduce feedback loops that resemble key performance indicators would merely put additional pressure (practically and emotionally) on the testers rather than solve the underlying problem, and indeed could be counter-productive: almost all research participants emphasised the importance of carrying out their work calmly, unrushed and with great care. In this context, additional support, relief from high workloads, and a continuous supply of test kits that facilitates their ability to stick to the script may be a more promising strategy than increasing the pressure by adding technological ‘fixes’ to structural problems (Oelschlaeger, Citation1979).
Making misdiagnoses visible is likely to contribute to new systems and workflows that look to optimise accuracy and eliminate uncertainty by further mirroring and embodying some of the regimes of standardisation seen in laboratory settings. Some commentators argue that point-of-care testing challenges many conventional approaches to laboratory testing and express concerns about how these are often implemented with limited guidance, poor regulatory control, and difficulties in ongoing monitoring and quality control (Stevens et al., Citation2014). Plebani (Citation2009) argues that the steps of point-of-care testing require the same level of management as laboratory testing to prevent errors, but notes that they are further complicated by environmental and user-related factors, something we have discussed in detail elsewhere (Skovdal et al., Citation2020). Our work in Zimbabwe suggests that many POC testers work in constant crisis mode (Skovdal et al., Citation2020). Several other studies from resource-limited settings have reported on misclassification errors resulting from HIV tester burn out and work-related stress (Louis et al., Citation2013; Shanks et al., Citation2013). Efforts to further standardise and regulate point-of-care testing by training and certifying staff, and putting in place EQA mechanisms must be accompanied with structural investments, shifting the locus of change away from POC testers to health system factors. As Martineau (Citation2020) points out: ‘In contrast to dominant health policy narratives which cast surveillance unproblematically as a key component of health system ‘resilience’, attending to the performativity of public health surveillance reveals its potential role in producing and reproducing precarity.’
Limitations
Our observations are constrained by some methodological limitations. Firstly, our cross-sectional design and rapid ethnographic approach only captured the experiences and (performative) practices of our participants at particular moments in time. Secondly, the design made social desirability bias possible. We cannot rule out that some participants chose to act or represent themselves in a particularly positive way either to protect their own reputation, or that of their organisation. A more in-depth and longitudinal ethnographic approach would be useful for future studies, particularly as the EQA programme in Zimbabwe expands. Finally, the generalizability of our findings is limited, as it focused on the perspectives and experiences of HIV testers in their particular clinical contexts. Future research could include the perspectives of policy makers and health facility administrators in a variety of settings.
Conclusions
Our findings caution against simple user error explanations for misdiagnosis in the absence of a broader recognition of structural determinants, and stresses the need to adequately resource HIV rapid testing programmes to circumvent misclassifications, thus shifting the locus of change away from point-of-care testers to broader health system factors, which provide the context in which testers can or cannot operate in adherence to the testing script.
The above-mentioned Stepwise Process does not go far enough in this respect, still focusing mainly on standardising individual testing practices and site-based preparedness. Rather than ever-increasing performance monitoring, a quality improvement framework needs to include building a work environment that facilitates trust, cooperation and a calm, careful disposition in order to achieve high quality testing. What this means in a particular setting must be based on a thorough understanding of local work dynamics and testers’ experiences and perspectives. Precarious employment contracts, working towards key performance indicators, and constant struggles with resource limitations provide the context in which errors become likely. They will need to be tackled if we are serious about improving point-of-care-testing quality.
Acknowledgements
The authors would like to thank all the participants who contributed their time and effort to the study. The authors would also like to thank Melinda Moyo, Rangararirai Nyamwanza and Constance Makumbe for their fieldwork and research assistance. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Bill and Melinda Gates Foundation.
Disclosure statement
SG declares shareholdings in pharmaceutical companies [GSK and AstraZeneca]; all other authors have no conflicts of interest to declare.
Data availability statement
Data cannot be shared publicly because of ethical restrictions. These restrictions are in place because the qualitative data contain potentially identifying or sensitive information, and because we do not have consent from the participants to share their transcripts with the wider public. Under these conditions, the Medical Research Council of Zimbabwe have imposed restrictions on the public sharing of data. Data is however available from the Biomedical Research and Training Institute (contact via http://www.manicalandhivproject.org/manicaland-data) for researchers who meet the criteria for access to confidential data.
Additional information
Funding
References
- Cartwright, L. (2000). Reach out and heal someone: Telemedicine and the globalization of health care. Health, 4(3), 347–377. https://doi.org/10.1177/136345930000400306
- Gregson, S., Moorhouse, L., Dadirai, T., Sheppard, H., Mayini, J., Beckmann, N., Skovdal, M., Dzangare, J., Moyo, B., Maswera, R., Pinsky, B. A., Mharakurwa, S., Francis, I., Mugurungi, O., & Nyamukapa, C. (2021). Comprehensive investigation of sources of misclassification errors in routine HIV testing in Zimbabwe. Journal of the International AIDS Society, 24(4), e25700. https://doi.org/10.1002/jia2.25700
- Johnson, C. C., Fonner, V., Sands, A., Ford, N., Obermeyer, C. M., Tsui, S., Wong, V., & Baggaley, R. (2017). To err is human, to correct is public health: A systematic review examining poor quality testing and misdiagnosis of HIV status. Journal of the International AIDS Society, 20 (Suppl 6), 21755. https://doi.org/10.7448/IAS.20.7.21755
- Klarkowski, D. B., Wazome, J. M., Lokuge, K. M., Shanks, L., Mills, C. F., & O'Brien, D. P. (2009). The evaluation of a rapid in situ HIV confirmation test in a programme with a high failure rate of the WHO HIV two-test diagnostic algorithm. PLoS One, 4(2), e4351. https://doi.org/10.1371/journal.pone.0004351
- Kufa, T., Kharsany, A. B., Cawood, C., Khanyile, D., Lewis, L., Grobler, A., Chipeta, Z., Bere, A., Glenshaw, M., & Puren, A. (2017). Misdiagnosis of HIV infection during a South African community-based survey: Implications for rapid HIV testing. Journal of the International AIDS Society, 20 (Suppl 6), 21753. https://doi.org/10.7448/IAS.20.7.21753
- Louis, F. J., Anselme, R., Ndongmo, C., Buteau, J., Boncy, J., Dahourou, G., Vertefeuille, J., Marston, B., & Balajee, S. A. (2013). Evaluation of an external quality assessment program for HIV testing in Haiti, 2006–2011. American Journal of Clinical Pathology, 140(6), 867–871. https://doi.org/10.1309/AJCPYWX49IZSQKFS
- Martineau, F. (2020, March 26). Shadow lives of surveillance: Technologies of control and the management of disease and health crisis [Paper presentation]. RAI Research in Progress series. London School of Hygiene and Tropical Medicine, London, UK.
- Matemo, D., Kinuthia, J., John, F., Chung, M., Farquhar, C., John-Stewart, G., & Kiarie, J. (2009). Indeterminate rapid HIV-1 test results among antenatal and postnatal mothers. International Journal of STD & AIDS, 20(11), 790–792. https://doi.org/10.1258/ijsa.2008.008427
- Nettleton, S., Burrows, R., & Watt, I. (2008). Regulating medical bodies? The consequences of the ‘modernisation’ of the NHS and the disembodiment of clinical knowledge. Sociology of Health and Illness, 30(3), 333–348. https://doi.org/10.1111/j.1467-9566.2007.01057.x
- Oelschlaeger, M. (1979). The myth of the technological fix. Southwestern Journal of Philosophy, 10(1), 43–53. https://doi.org/10.5840/swjphil19791014
- Palmer, J. J., Jones, C., Surur, E. I., & Kelly, A. H. (2020). Understanding the role of the diagnostic ‘reflex’ in the elimination of human African trypanosomiasis. Tropical Medicine and Infectious Disease, 5(2), 52. doi:https://doi.org/10.3390/tropicalmed5020052
- Plebani, M. (2009). Does POCT reduce the risk of error in laboratory testing? Clinica Chimica Acta, 404(1), 59–64. doi:https://doi.org/10.1016/j.cca.2009.03.014
- Pols, J. (2012). Care at a distance: On the closeness of technology. Amsterdam University Press.
- Shanks, L., Klarkowski, D., & O'Brien, D. P. (2013). False positive HIV diagnoses in resource limited settings: Operational lessons learned for HIV programmes. PloS one, 8(3), e59906. https://doi.org/10.1371/journal.pone.0059906
- Skovdal, M., Beckmann, N., Maswera, R., Nyamukapa, C., & Gregson, S. (2020). Uncertainty, work conditions and testing biases: Potential pathways to misdiagnosis in point-of-care rapid HIV testing in Zimbabwe. PLoS ONE, 15(8), e0237239. https://doi.org/10.1371/journal.pone.0237239
- Skovdal, M., Beckmann, N., Maswera, R., Nyamukapa, C., & Gregson, S. (2022). The (in)visibility of misdiagnosis in point-of-care HIV testing in Zimbabwe. Medical Anthropology, 42(4), 404–417. https://doi.org/10.1080/01459740.2022.2054715
- Stevens, W., Gous, N., Ford, N., & Scott, L. E. (2014). Feasibility of HIV point-of-care tests for resource-limited settings: Challenges and solutions. BMC Medicine, 12(1), 173. https://doi.org/10.1186/s12916-014-0173-7
- Twigg, J., Wolkowitz, C., Cohen, R. L., & Nettleton, S. (2011). Conceptualising body work in health and social care. Sociology of Health and Illness, 33(2), 171–188. https://doi.org/10.1111/j.1467-9566.2010.01323.x
- Weick, K. (1979). The social psychology of organizing. McGraw-Hill.
- Young, P. W., Mahomed, M., Horth, R. Z., Shiraishi, R. W., & Jani, I. V. (2013). Routine data from prevention of mother-to-child transmission (PMTCT) HIV testing not yet ready for HIV surveillance in Mozambique: A retrospective analysis of matched test results. BMC Infectious Diseases, 13(1), 96. https://doi.org/10.1186/1471-2334-13-96
