
ABSTRACT
Globally, there have been calls for an integrated zoonotic disease surveillance system. This study aimed to assess human and animal health surveillance systems to identify opportunities for One Health surveillance platform in Tanzania. A desk review of policies, acts and strategies addressing disease surveillance that support inter-sectoral collaboration was conducted. A semi-structured questionnaire was administered to key informants from the two sectors. Databases with potential relevance for surveillance were assessed. One Health-focused policies, acts, strategic plans and guidelines emphasising inter-sectoral collaboration strengthening were in place. Stable systems for collecting surveillance data with trained staff to implement surveillance activities at all levels in both sectors were available. While the human surveillance system was a mix of paper-based and web-based, the animal health system was mainly paper-based. The laboratory information system existed in both sectors, though not integrated with the epidemiological surveillance systems. Both the animal and human surveillance systems had low sensitivity to alert outbreaks. The findings indicate that individual, organisational, and infrastructure opportunities that support the integration of surveillance systems from multiple sectors exist. Challenges related to data sharing and quality need to be addressed for the effective implementation of the platform.
ACRONYMS
| CVL | = | Central Veterinary Laboratory |
| DHIS-2 | = | District Health Information Software 2 |
| DVS | = | Directorate of Veterinary Services |
| GoT-HOMIS | = | Government of Tanzania-Hospital Management Information System |
| HMIS | = | Health Management Information Systems |
| IDSR | = | Integrated Disease Surveillance and Response |
| IHR | = | International Health Regulations |
| JEE | = | Joint External EvaluationLMIS – Laboratory Management Information System |
| TVLA | = | Tanzania Veterinary Laboratory Agency |
Introduction
Disease surveillance is an ongoing systematic collection, analysis and interpretation of data, which leads to actions being taken to prevent and control diseases (Groseclose & Buckeridge, Citation2017). In both human and animal health sectors, disease surveillance systems aim to predict, observe, and minimise the impacts caused by outbreaks and consolidate knowledge about factors that contribute to such situations. Disease surveillance is, therefore, an essential component of public and animal health programmes (Berkelman et al., Citation1994) and is made up of three major components: monitoring of the progress of on-going interventions for disease reduction/elimination; early detection of signals for disease outbreaks to initiate prompt response and control measures; and provision of data for decision-making including planning (Berkelman et al., Citation1994; Fasina et al., Citation2021; Groseclose & Buckeridge, Citation2017; John et al., Citation1998). These components must perform adequately for a functional and effective disease surveillance system.
About two-thirds of all infectious diseases and three-quarters of emerging infectious diseases originate from pathogens infecting animals (Taylor et al., Citation2001; Woolhouse & Gowtage-Sequeria, Citation2005). Africa is one of the epicentres of most human emerging infectious diseases with epidemic risk and probably has the highest burden of infectious diseases of both humans and animals, yet with limited capacity for risk management (Kluberg et al., Citation2016). Emerging infectious diseases commonly occur in humans at the animal-environment interface (involving pathogens that evolve or spill over from domestic animals and wildlife) are likely to be driven by multiple factors. These include human demographic and anthropogenic factors, globalisation (human, animal and animal products movements), technological advancement and ecological factors (Church, Citation2004; Sabin et al., Citation2020; Woolhouse & Gowtage-Sequeria, Citation2005; Yale et al., Citation2013). Thus, the prevention and control of zoonotic disease outbreaks require strengthening surveillance systems based on a One Health approach (Hassell et al., Citation2017; Morand & Lajaunie, Citation2021; Plowright et al., Citation2021; Sabin et al., Citation2020).
As part of an effective global response to diseases transmitted between animals and humans, there have been calls for integrated surveillance of zoonotic diseases in human and animal populations (Morens & Fauci, Citation2013). Nonetheless, only a few examples of successful programmes and practices to strengthen preparedness and response capacities for infectious disease mitigation and control that use a one health approach have been described (Buregyeya et al., Citation2020; Drewe et al., Citation2012; Kitua et al., Citation2019; Machalaba et al., Citation2018; Mghamba et al., Citation2017). The operationalisation of the One Health approach in addressing infectious diseases is still unclear for various local health systems (Johnson et al., Citation2018; Nyatanyi et al., Citation2017; Yasobant et al., Citation2021). Some studies have identified critical factors that influence the operationalisation of integrated disease surveillance programmmes. They include micro-level factors at the individual level, meso-level factors at the organisational level, macro-level factors at the system level, and external factors outside of the system (George et al., Citation2020; Peyre et al., Citation2017; Yasobant et al., Citation2021). In Tanzania, like in many other countries in Sub-Saharan Africa, the Health Management Information Systems (HMIS), is currently the primary source of integrated disease surveillance and response data. HMIS consist of routinely collecting epidemiological data from health care facilities with a weak link to the community (Mremi et al., Citation2021). Both human and animal surveillance systems in Tanzania face several challenges in the accessibility and utilisation of the data generated. Sentinel surveillance and research outputs are rarely incorporated or consolidated in the health information system of the sectoral ministries and are not used in the planning and implementation of disease surveillance in the country (George et al., Citation2021; MoHSW, Citation2015).
To adopt the One Health approach in controlling and preventing infectious diseases, Tanzania has developed and introduced the Guidelines for Surveillance of Prioritized Zoonotic Diseases for Human and Animal Health (URT, Citation2018). This was likely to be an impetus to enhance an integrated multi-sectoral approach in disease surveillance, early warning and timely response to infectious disease epidemics. However, the strategy does not explicitly address the need and implementation framework to harvest/access multiple sources of health and health-related information systems; and three years online, there is no platform that integrates surveillance data for zoonoses in the country. This study aimed to assess the human and animal health surveillance systems in Tanzania to identify opportunities for multi-sectoral data integration that could foster the development and implementation of the One Health surveillance platform.
Methods
Study setting and design
Tanzania is a country of about 945,000 km2, with a population of 60 million people (URT, Citation2013) and a life expectancy at birth of 64 years (MoHCDGEC, Citation2019). In Tanzania, health services are provided by both public and non-public health facilities; by 2020, there were a total of 8,458 health facilities comprising of 369 hospitals, 926 health centres and 7,163 dispensaries. The distribution of health facilities in 2020 indicates that dispensaries constitute 84.7% of all health facilities, of which government owns 73.5% of the health facilities. There is a dispensary in almost every village and a health centre in each ward. The human health sector has about 95,827 health workers, of which 45.7% are in urban and 54.3% in rural areas. The ratio of physicians/clinicians per 10,000 is 1.03, while that of nurses is 4.1 per 10,000 (URT, Citation2021). However, the distribution of these core health professionals and ratios varies by region.
Tanzania has the third largest livestock population in Africa, comprising 25 million cattle, 16.7 million goats, 8 million sheep, 2.4 million pigs, and 36 million chickens (FAO, Citation2021). The animal health system is currently saved by different types of registered veterinary facilities (1,707) that operates as veterinary hospital (1), veterinary centres (1,667), veterinary clinics (21), veterinary ambulatory services (12), veterinary quarantine services (6), veterinary practice companies (15) and veterinary laboratory centres (12). There are currently 1,021 registered veterinarians and 4,118 veterinary paraprofessionals in Tanzania, in both public and private sectors (Frumence et al., Citation2021). These facilities are widely distributed in the country.
Desk review
A desk review of policies, acts and strategies addressing infectious disease surveillance, supporting data integration and inter-sectoral collaboration was conducted. The objective was to conduct a review and synthesis of existing national policies, strategies and regulatory frameworks related to pandemic preparedness and response in both animal and health to better understand the extent to which they address and one health surveillance. The document review was guided by a review matrix that clearly indicates the key information/thematic areas of focus for the review. The review adopted the Joint External Evaluation (JEE) tool and thematic areas; namely prevent, detect, respond, international health regulations (IHR) related hazards and point of entry (WHO, Citation2018). The inclusion criteria of the selected documents were based on the description of the JEE thematic areas and whether or not the document comprehensively addressed the IHR (Citation2005). In addition, the individual ministries’ websites were accessed to collect the most up-to-date surveillance information/portal available in the public domain.
Assessment of the surveillance systems
A semi-structured questionnaire was administered to 23 key informants from the ministries responsible for human and animal health to gain an insight into the existence and operationalisation of the surveillance systems. Information sought included key components and characteristics, performance based on the system's attributes, their perception and responsiveness on integration features in One Health, and challenges and opportunities in the existing systems in the aspect of the development of a One Health surveillance platform. Databases with potential relevance for human and animal health were identified and examined to understand the types of data and variables gathered at each level and systems attributes.
Surveillance system attributes were measured in terms of timeliness and completeness, simplicity; flexibility; stability, sensitivity and representativeness and usefulness and acceptability. Timeliness reflects the speed between steps in the surveillance system (i.e. time between the onset of a health-related event and the reporting time). Completeness refers to the proportion of health facilities that submitted reports to the higher level irrespective of the time of submission. Simplicity refers to both its structure and ease of operation. Flexibility is the ability of the systems to adapt with changing in information, time, technologies or resources. Stability is the ability to collect, manage, and provide data properly without failure. Sensitivity refers to the ability to detect outbreaks, including the ability to monitor changes in the number of cases over time. Representativeness refers to the ability of the system to describe the occurrence and distribution of all reported cases accurately in terms of time, place and person. Usefulness refers to the relevance of the system to surveillance stakeholders. Acceptability is the willingness of surveillance stakeholders to implement the system as expressed by their active participation in case detection and reporting. The primary surveillance system identified from each sector was further assessed to get a deeper insight into the system used and disease surveillance functions performed at various levels.
Data Management and analysis
Data from questionnaires were coded manually in a Microsoft™ Excel 2019 spreadsheet and cleaned on immediate mistakes. Significant qualitative findings were narrated and summarised based on key thematic areas of the surveillance system. Responses from the key informants were recorded, reviewed and manually coded in Microsoft™ Word. Information gathered from the surveillance systems assessment was presented using flowchart diagrams, separate for health and animal sector, summarising the overall architecture, the processes and flow of generating disease surveillance data. Collectively, the information from all approaches was synthesised to identify opportunities and challenges for developing a One Health surveillance platform. Envision the proposed platform within the healthcare system architecture, the opportunities and gaps were constructed within the system blocks to realise operational feasibility at micro, meso and macro levels. The impact of each block on the surveillance components, i.e. outbreak detection, generation data for decisions and monitoring progress of intervention was indicated using a colour-code system. A thematic illustration was created to summarise key findings.
Ethical considerations
This study received ethical approval from the Tanzania Medical Research Coordinating Committee of the National Institute for Medical Research (Ref. NIMR/HQ/R.8c/Vol 1/1168). Before the interviews and questionnaire administration, researchers obtained participants’ written informed consent.
Results
Policy, acts, strategies and guidelines
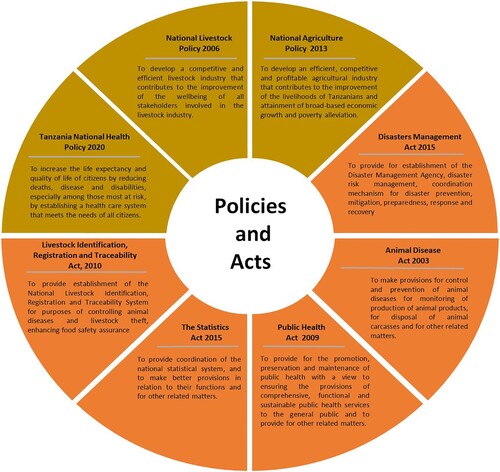
Three national policies were included in the review. These were the National Livestock Policy 2006, National Agriculture Policy 2013 and National Health Policy 2020. The Animal Disease Act 2003, the Public Health Act 2009, the Livestock Identification, Registration & Traceability Act 2010, the Statistics Act Citation2015 and Disaster Management Act 2015 were also reviewed. The livestock policy aims at enhancing development in the livestock industry to increase rural and national income, improve food security and environmental conservation. It targets to increase well-being of all stakeholders involved in the livestock industry. The Agriculture Policy aims include fighting land degradation, favouring organic agriculture and the production of biofuel crop production for increased use as a renewable energy, and more broadly to take adequate measures to improve adaptation to climate change effects. It highlights different challenges facing the agricultural sector and states the policy options and institutional framework selected to address them. The National Health Policy aims to improve the health and well-being of the citizens and encourage the health system to address the health needs of the citizens ().
Figure 1. Policies and acts that support surveillance data integration and sharing in Tanzania.
The guidelines reviewed were the National Integrated Diseases Surveillance and Response Guidelines 2020 and the Guidelines for Surveillance of Prioritized Zoonotic Diseases for Human and Animal Health in the United Republic of Tanzania, 2015-2020. The national strategies/strategic plans reviewed were: The Health Sector Strategic Plan V, 2021-2026; Tanzania National eHealth Strategy 2012-2018; National Animal Health Surveillance Strategy 2019-2023; The National One Health Strategic Plan 2015-2020; The National Action Plan for Health Security 2017-2021; and the All-Hazards Public Health Emergency Response Plan; and Tanzania Digital Health Strategy 2019–2024 ().
Figure 2. Strategic plans that support surveillance data integration and sharing in Tanzania.

The Tanzania National Livestock Policy 2006, National Agriculture Policy 2013, National Health Policy 2017, and the Health Sector Strategic Plan V emphasise the need to strengthen inter-ministerial cooperation (through a multi-sectoral approach) to address health security and emergencies at national, regional and district levels. The National Agriculture Policy 2013 addresses issues in line with infectious disease detection and monitoring, including disease surveillance. The Tanzania National Health Policy emphasises strengthening inter-ministerial cooperation to address health security and emergencies at all levels. The Statistics Act 2015 provides for the national statistical system's coordination and makes better provisions concerning their functions and other related matters.
The Animal Health Surveillance Strategy, 2019-2023, covers essential surveillance issues, laboratory systems and the need to share data between veterinary epidemiology and laboratories and other ministries in case of zoonoses. Generally, this strategy's implementation aims at harnessing a surveillance system to foster early disease detection and prompt response to animal and public health events in Tanzania. The National One Health Strategic Plan 2015–2020 aims to create and maintain active collaboration between the sectors to prevent and control zoonoses to ensure timely preparedness and consistent and coordinated response in a zoonotic event. Following this, a One Health coordination desk was established in the Prime Minister’s Office in February 2018 to address emerging health challenges at the animal-environment-human interface. The National eHealth Strategy describes Tanzania’s long-term vision for eHealth, with an ultimate objective to facilitate information sharing and communication. These include integration and interoperability of health information systems to support more efficient access to needed data and information for policy development and delivery of health care. The Tanzania Digital Health Strategy 2019–2024 aims to harmonise the national health information systems, which are essential for improving access to quality data through seamless and secure information exchange across the health sector and other sectors.
Although the National Integrated Disease Surveillance and Response (IDSR) guidelines do not explicitly address inter-sectoral coordination, they emphasise adopting the One Health approach. The guidelines emphasise that animal and human health workers and other relevant partners should be engaged at various levels as information sources for IDSR to facilitate sharing and joint rapid response activities further. On the other hand, the Guidelines for Surveillance of Prioritized Zoonotic Diseases for Human and Animal Health in the United Republic of Tanzania 2018 provide direction for effective integrated surveillance and response to priority zoonoses in Tanzania. In order of its priority, these diseases are rabies, anthrax, Rift Valley fever, zoonotic avian influenza, human African trypanosomiasis and brucellosis. The Guidelines cover vital aspects crucial for effective surveillance and monitoring and evaluation, including community-based surveillance, sharing of data among sectors, and disseminating information and response.
A total of 23 key informants participated in the interviews and they were from the human sector (9), animal sector (8), National Bureau of Statistics (1) and Prime Minister’s Disaster Management Division (3). The positions of the key informants (hereinafter referred to as respondents) were epidemiologists (8), the data manager (5), information and communication technology (7) and statistician (3). The majority (91%, n = 23) of the key informants were above 30 years of age, 87% were males, and 92% had attained at least a degree level of education. All respondents had worked in their current positions for more than three years. All accepted that it was their responsibility to ensure that surveillance data were collected in the operating information systems and appreciated the role of existing information systems in strengthening disease surveillance.
Surveillance systems
In human health, the HMIS, Government of Tanzania-Hospital Management Information System (GoT-HOMIS), and Laboratory Management Information System (LMIS) were primary sources of disease surveillance data. However, the HMIS was the sole source of indicator-based surveillance data (IDSR). In addition, specific disease control programmes were operating their own parallel surveillance systems. The Animal Health Surveillance Systems, Tanzania Livestock Identification and Traceability System, and Laboratory Information Management System were the major animal disease surveillance sources.
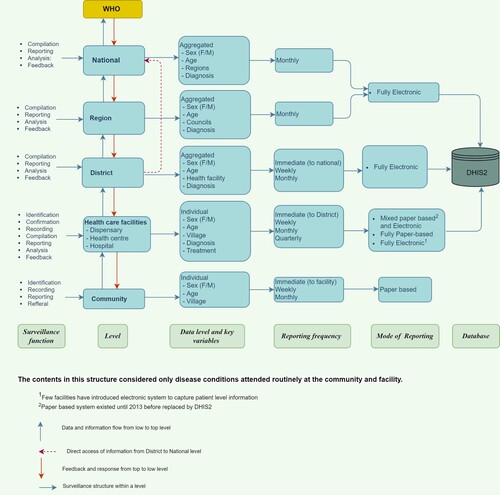
In the human health sector, reporting procedures start at the health facility level, where data are recorded in the specific out-patient and in-patient registers upon provision of care. Key data variables collected includes demographic, provisional/confirmed diagnosis and treatment. Patient data are aggregated using tally sheets and reported to the district health office through weekly or monthly summary report forms. Each facility submits summary forms to the district level, where all data are entered into the District Health Information Software (DHIS-2). The aggregated data are made accessible to the district, regional and national levels for further compilation, analysis, reporting and feedback. Then, the Ministry of Health submits surveillance data on notifiable diseases to the World Health Organization ().
Figure 3. Human health surveillance structure and information flow in Tanzania.
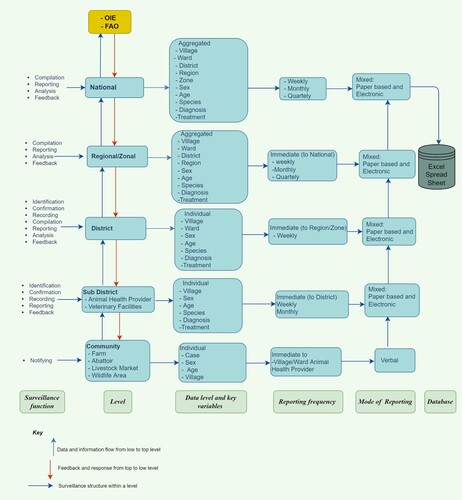
In the animal health sector, the initial reporting starts at the community level, where a farmer notifies the animal health provider about a sick animal. Other sites where a primary recording of the case is done include veterinary practice facilities, zoo-sanitary border ports, checkpoints, slaughter facilities, livestock markets, district livestock offices and zonal veterinary investigation centres (ZVICs). The animal health provider identifies, diagnoses and treats the reported case, records it in the animal disease surveillance field report form and submits it to the District Veterinary Officer (DVO). At the district level, submitted reports are compiled and sent to the ZVIC, where reports are validated and compiled. Then the reports are forwarded to the Directorate of Veterinary Services (DVS) at the ministry level. The DVS office submits notifiable diseases to the regional and international bodies, including the World Organization for Animal Health (). Institutions such as Tanzania Wildlife Research Institute, Tanzania National Parks Authority, Sokoine University of Agriculture, and private veterinary service providers submit reports on disease incidence directly to the DVS.
Figure 4. Animal health surveillance structure information flow in Tanzania.
Surveillance system attributes
Timeliness and completeness: With human health surveillance, the overall reporting rates of health facilities were established to be satisfying irrespective of some reporting gaps in some districts. Analysis of the monthly reporting completeness rates showed a significant increase from 74.5% in 2018–92.6% in 2020, while during the same period, timeliness rates increased from 57.0% to 76.9%. For the animal health surveillance systems, the reporting and completeness rates in 2020 were 70% and 65%, respectively. Data accuracy was reported to be of similar levels, 62% and 65% for the human and animal surveillance systems, respectively. Missing values and incomplete data sets were common in both human and animal surveillance systems, and this was associated with the inadequate human resource at all levels.
Simplicity: Both data management, including collection, reporting and analysis in the human surveillance system, were reported to be simple. The evidence of the systems simplicity stability was complemented by increased data collection completeness and timeliness over the years. The animal health surveillance system was rated as complex in its operation. Data collection, compilation and reporting, was manual at the community, the animal health provider and district levels. The reports from the animal health providers were usually submitted to the districts office and then compiled at a zonal level before being submitted to the national level (Ministry). This mode of reporting caused delays and breakdowns that may lead to data loss. Inadequate resource allocation to facilitate reporting was common.
Flexibility: The human health surveillance system was described as flexible and could accommodate new variables. For instance, the weekly reporting format could be used for new health events not listed among the national priority diseases. Because the reporting format had room for ‘other variables’, which means one may include any other health events that occur during the reporting period. The system was also flexible in the sense that it could be integrated with other information systems. On the other hand, the animal health surveillance system was inflexible and characterised by different versions of the reporting forms.
Stability: Human health surveillance was part of the existing HMIS and the government fully cover the operating resources for the system. Whether due to maintenance, upgrading, or any technical fault, the system downtime does not affect the surveillance procedures and activities. On the other hand, transfer breakdown between levels made the animal health surveillance system unstable. Moreover, the animal health surveillance system being manual was not integrated with other systems.
Sensitivity and representativeness: Human health surveillance system was reported to have low sensitivity and could not provide outbreak alerts. Similarly to the animal health surveillance system, and is manually operated and paper-based, complicated this further. In terms of representativeness, both the human and animal health surveillance systems covered the whole country geographically, hence representing the entire human and animal populations, respectively.
Usefulness and acceptability: The human health surveillance system was found to be very useful in determining the magnitude of morbidity and mortality. It was also described as convenient, acceptable, and useful in monitoring disease incidence and assessing the effectiveness of priority disease control programmes. It could also be used to identify high priority areas for each disease under surveillance for easy resource allocation and intervention. Though the animal surveillance system was described as partially acceptable, data generated was considered useful in informing the national authorities of the magnitude of animal diseases in the country. The system was used for diseases control and tracing of animal movements.
Laboratory Management Information systems
The Laboratory Management Information System (LMIS) was described as operating at the district, regional, zonal, and national hospitals in the human health sector. A laboratory information system software has been installed and works at the National Health Laboratory, Muhimbili National Hospital and three zonal referral hospitals (Bugando Medical Centre, Kilimanjaro Christian Medical Centre and Mbeya Zonal Referral Hospital). The system operates independently at the national laboratory and on each zonal hospital with a separate server installed in each site. In contrast, an open laboratory data repository has been installed at National Data Centre. At the regional level, a different information system software has been installed and operates in 23 hospitals. At the district level, laboratory data are collected through an electronic health records system, GoT-HOMIS, which operates in most public health centres and district hospitals. All the existing laboratory information systems operate in isolation separately at each level. There is no integration of the laboratory data at any health system level or with any other health information system within the human health sector.
Tanzania Veterinary Laboratory Agency (TVLA) is in charge of the LMIS in the animal health sector, with 12 centres spread across the country. The Tanzania Vaccine Institute, the Central Veterinary Laboratory (CVL), the Centre for Infectious Diseases and Biotechnology, and a zonal network of regional laboratories located in Arusha, Dodoma, Iringa, Mtwara, Mwanza, Tabora, and Rukwa. An LMIS software has been installed in all the TVLA centres. Using the assigned unique identifier, this system records samples from the point of collection. The test results are then shared with the customer; and in the case of a notifiable disease, the results are submitted to the Ministry via the DVS. The system has allowed for faster turn-around times of samples, automation and data quality control. The major limitation of the system is that the server is hosted outside the country, which makes it challenging to customise.
Opportunities and challenges
Opportunities: Several opportunities were identified in both sectors for the realisation of the development of an integrated One Health surveillance platform (). These included the understanding role of surveillance, stakeholders, and key players, understanding the purpose and importance of surveillance systems, appreciating one health concept, positive perception of the need to integrate, and willingness to be involved. Others were the availability of policies, legislations, strategies and guidelines that support integration, common vision and purpose towards one health and a political will. The establishment of a national One Health desk within the Prime Minister's office was described as one key strength towards an integrated zoonotic disease surveillance platform. Moreover, already a list of priority zoonoses has been identified.
Figure 5. Opportunities, challenges and level of effect towards establishing One Health platform.
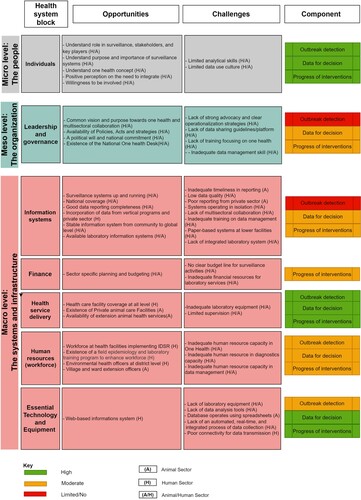
The existence of surveillance systems up and running with national coverage, improved data reporting and completeness, stable health surveillance structure information flows to the global level was also identified as a strength. The availability of laboratory information systems in both sectors and the presence of an operating web-based DHIS2 in the human health sector were identified as critical opportunities towards the development of the One Health Disease Surveillance platform. Availability of sector-specific planning and budgeting, intensive health care facilities coverage up to village level in human health, as well as the existence of animal veterinary facilities and laboratories in most districts and the availability of animal health providers at the community level, were identified as opportunities that support systems and infrastructure towards the realisation of the One Health platform.
Challenges: In both sectors, challenges were described at the individual, organisational, system, and infrastructure levels. Both sectors were represented with limited analytical skills and limited data-use culture at the individual level. At the organisation level, lack of strong advocacy and clear operationalisation strategies, lack of guidelines/platform for data sharing and lack of training focusing on One Health and limited supervision were declared in both sectors. In terms of systems and infrastructure level the challenges that were faced by both sectors were included low data quality, systems operating in isolation, lack of multisectoral collaboration, inadequate training on data management, paper-based systems at lower facilities, fragmentation and use of different tools and lack of integrated laboratory system within the existing surveillance systems. Although the private sector plays a central role in animal health services, private veterinary facilities rarely submit disease incidence reports to the ward or district/national levels as required. Inadequate human resources (in both number and appropriate qualifications) in surveillance, laboratory and data management; unclear indication on a budget line for surveillance activities and laboratory services were also identified by most of the respondents as among the most critical barriers to surveillance programmes. Similarly, gaps described by both sectors in essential technology and equipment included: lack of an automated, real-time, and integrated process of data collection and a shortage of equipment/tools for data analysis. In the human sector, poor connectivity for data transmission was reported as one of the major barriers to the use of technology.
Discussion
The national agriculture, livestock and human health policies emphasise the need to strengthen inter-ministerial cooperation to address health security and emergencies at national and sub-national levels. In addition, the Disaster Management Act (URT, Citation2015a) provides the mandate to coordinate, work with and monitor inter-ministerial and multisectoral entities. The Statistics Act 2015 (URT, Citation2015b) provides the coordination of the national information system. The Health Sector Strategic Plan emphasises the need for a stronger health information system that supports data exchange and interoperability that allows the sharing and use of data from two or more systems to improve its use at all health system levels (URT, Citation2021). The finding of this study indicates that the necessary policy and legal instruments to support and implement an integrated multi-sectoral surveillance data platform are available. However, even though the National One Health Strategic Plan 2015–2020 has identified six priority diseases (URT, Citation2018), sharing of the surveillance data is not formally practised in Tanzania.
The findings indicate that there are several surveillance systems and/programmes in both sectors that operate in isolation. The IDSR has been adopted as a national strategy for disease surveillance in the human sector since the early 2000s (Rumisha et al., Citation2007). There has been substantial success in incorporating vertical programmes, and some data are currently available, captured and accessible through the DHIS2. A previous assessment of the animal health information system in Tanzania reported that the absence of disease information that accurately reflects the health status of the source population and an inefficient information management system are the major challenges (Kivaria & Kapaga, Citation2002).
The LMIS in both animal and human health operate as stand-alone systems, and the generated data are not captured for surveillance purposes. Historically, many surveillance systems/programmes have evolved from different objectives, needs and different organisations (Houe et al., Citation2019). Despite the fact that Tanzania has a National Bureau of Statistics, established to play the role of a coordinating agency (URT, Citation2015b), integration of statistics from different sectors has rarely been a coordinated process but rather represents various initiatives taken by different sectors (Mboera et al., Citation2017).
However, data are rarely used to their full potential despite growing storage and computing capacities in Tanzania. The key informants’ opinion is that mechanisms need to be established to harmonise the information within and between sectors. Most of the respondents identified a lack of a platform for data sharing as a barrier to One Health implementation. However, currently, interoperability of datasets between human and animal sectors is faced by the challenge that animal health surveillance is mainly manual. Some respondents noted that human resource capacity is limited in both human and animal health sectors. A previous study has reported inadequate human and financial resources, lack of incentives and supervision, and lack of standard operating procedures on data management as the main challenges affecting Tanzania's health information system performance (Mboera, Rumisha et al., Citation2021a). Tanzania has established a functioning and institutionalised multi-sectoral coordinating mechanism with a sound institutional structure and capacity to prevent, detect early and respond to health events under the Prime Minister’s Office (Kitua et al., Citation2019). This office could appropriately be used to coordinate and operate an integrated disease surveillance platform.
While in the human health sector, the reporting procedures start at the health facility, for both public and private institutions. In the animal health sector, initial reporting begins at the community level. Like our study, other studies in Tanzania have indicated that most animal health surveillance data are from farmers, slaughter facilities, and livestock markets (George et al., Citation2021; Kivaria & Kapaga, Citation2002). However, the data sources are characterised by variation in terms of data frequency and accuracy. Unlike in the human health sector, there is an absence of web-based animal health surveillance and reporting at the district level, which may hinder the timely incorporation of these data in the proposed integrated platform. Inadequate information sharing has also been reported to be lacking between ministries responsible for animal health, local government authority, and other stakeholders (Mboera, Sindato et al., Citation2021b). A recent study by Fasina et al. (Citation2021) also found that information sharing, communication and collaborations among the various sectors of One Health to be very poor.
Although some of the human health facility level diagnoses are backed by laboratory findings, the national laboratory information systems operate in isolation at each level. There is no data integration at national, regional or district levels or with any other health information system within the health sector. The low capacity of some laboratories, which impairs early diagnosis of suspected diseases and laboratory and surveillance data not being linked in electronic reporting systems, were also pointed out as important challenges in disease surveillance. In the animal health sector, TVLA is responsible for the operation of the LMIS, which communicates with its centres across the country. Despite this, there is an inadequate laboratory confirmation system across the two sectors. A recent study reported that the laboratory confirmation system in animal health was not effectively functioning due to insufficient laboratory facilities, inadequate capacity of the centres, lack of essential equipment for sample collection, inadequate financial resources (URT, Citation2020) as well as the affordability of farmers to pay for the laboratory fees. The study noted that laboratory facilities were mainly accessible by the livestock keepers in the urban areas, particularly those in regions where the zonal offices are stationed. It is important to have the national laboratory and national public health institutions closely connected to address this challenge to enable prompt identification of outbreaks.
Though disease surveillance is intended to produce outputs for decision making, the strength is mainly sector-specific. The findings of this study and others indicate the inadequate capacity in data management and knowledge sharing between sectors and stakeholders (Mboera, Rumisha et al., Citation2021a; Rumisha et al., Citation2020). For surveillance to be relevant and encourage wider use of data, it must be transformed into information and knowledge to address the needs of all key stakeholders (Hernández-Jover et al., Citation2021). All these need to be addressed to strengthen the surveillance systems in the country. The Ministry of Health and partners have currently developed a system to manage data exchange among hospitals and across digital data systems (Nsaghurwe et al., Citation2021). The approach could be used to address surveillance data sharing between animal, human and environmental health sectors.
The complexity of many challenges in animal and human health and related issues requires that all these data are integrated to a greater extent than is currently been done. This is likely to improve effectiveness in surveillance and control of infectious diseases, including risk assessment and early warning of epidemics. Integration does not necessarily mean that data from different sources are directly merged, but merely that the information from various sources is accessed and used in a coordinated manner to address complex questions or challenges from animal and human public health sectors (Houe et al., Citation2019). There are several examples that integration of surveillance information across sectors is beneficial in terms of identifying emerging health issues (Brownstein et al., Citation2004) as well as in understanding risk factors and transmission mechanisms (Guernier et al., Citation2018) and controlling health events (Rahaman et al., Citation2019). The findings of this study are envisaged to be used to assess how combinations and integration of databases could improve existing evidence to support decisions in human and animal health policies. Integration of animal and human surveillance data at national and sub-national levels is likely to provide important epidemiological surveillance data of the identified priority diseases and their risk management. Such integration is expected to enhance the timeliness as the animal population may serve as an early warning for the likelihood of the presence of disease in the human population (Falzon et al., Citation2019). Intersectoral collaborations between multiple sectors are likely to be cost-effective (Halliday et al., Citation2012; Stärk et al., Citation2015; Wendt et al., Citation2015).
Conclusion
The findings from this study indicate that individual, organisational and system, and infrastructure opportunities that support the integration of disease surveillance systems and data from multiple sectors exist in Tanzania, hence encouraging the development and implementation of the One Health integrated surveillance platform. Challenges such as surveillance information systems, databases, skilled workforce, linking laboratory data with the epidemiological surveillance systems and governance need to be addressed at all levels. The existing systems have significant and positive strength on generating data for decision-making and necessary information to monitor impact of interventions, however, weakly on detecting outbreaks. This study evidently suggests that Tanzania is well-positioned to establish a One Health integrated platform to facilitate mining and joint analysis of surveillance data of priority zoonotic diseases to identify epidemic risks earlier for prompt and efficient responses and efficient decisions.
Supplemental Material
Download MS Word (65.5 KB)Acknowledgements
The authors thank the Management of the Ministry of Health, Community Development, Gender, Elderly and Children and the Ministry of Livestock and Fisheries for their support during the engagement of the Key Informants. Prof. Gabriel Shirima is thanked for his critical review of the early draft of the manuscript. IRM carried out data collection and analysis. A first draft of the manuscript was prepared by IRM, expanded by SIK, CS, SFR, and LEGM, then further revised by IRM, SFR, and LEGM. All authors approved the final version of the manuscript.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The datasets generated for this study are available on request to the corresponding author.
Additional information
Funding
References
- Berkelman, R. L., Bryan, R. T., Osterholm, M. T., LeDuc, J. W., & Hughes, T. M. (1994). Infectious disease surveillance: A crumbling foundation. Science, 264(5157), 368–370. https://doi.org/10.1126/science.8153621
- Brownstein, J. S., Holford, T. R., & Fish, D. (2004). Enhancing West Nile Virus surveillance, United States. Emerging Infectious Diseases, 10(6), 1129–1133. https://doi.org/10.3201/eid1006.030457
- Buregyeya, E., Atusingwize, E., Nsamba, P., Musoke, D., Naigaga, I., Kabasa, J. D., Amuguni, H., & Bazeyo, W. (2020). Operationalizing the One Health approach in Uganda: Challenges and opportunities. Journal of Epidemiology & Global Health, 10(4), 250–257. https://doi.org/10.2991/jegh.k.200825.001
- Church, D. L. (2004). Major factors affecting the emergence and re-emergence of infectious diseases. Clinics in Laboratory Medicine, 24(3), 559–586. https://doi.org/10.1016/j.cll.2004.05.008
- Drewe, J., Hoinville, L. J., & Cook, A. J. C. (2012). Evaluation of animal and public health surveillance systems: A systematic review. Epidemiology and Infection, 140(4), 575–590. https://doi.org/10.1017/S0950268811002160
- Falzon, L. C., Alumasa, L., Amanya, F., Kang’ethe, E., Kariuki, S., Momanyi, K., Kang'ethe, E., Muinde, P., Murungi, M. K., Njoroge, S. M., Ogendo, A., Ogola, J., Rushton, J., Woolhouse, M. E. J., & Fèvre, E. M. (2019). One Health in action: Operational aspects of an integrated surveillance system for zoonoses in Western Kenya. Frontiers in Veterinary Sciences, 6, 252. https://doi.org/10.3389/fvets.2019.00252.
- FAO. (2021). Tanzania at a glance. Food and Agriculture Organization of the United Nations. http://www.fao.org.
- Fasina, F. O., Fasanmi, O. G., Makonnen, Y. J., Bebay, C., Bett, B., & Roesel, K. (2021). The One Health Landscape in Sub-Saharan African countries. One Health, 13, 100325. https://doi.org/10.1016/j.onehlt.2021.100325
- Frumence, G., Mboera, L. E. G., Sindato, C., Katale, B. Z., Kimera, S., Metta, E., Durrance-Bagale, A., Jung, A.-S., Mshana, S. E., Clark, T. G., Rweyemamu, M., Legido-Quigley, H., & Matee, M. I. N. (2021). The Governance and Implementation of the National Action Plan on Antimicrobial Resistance in Tanzania: A Qualitative Study. Antibiotics (Basel, Switzerland), 10(3), 273. https://doi.org/10.3390/antibiotics10030273
- George, J., Häsler, B., Komba, E., Sindato, C., Rweyemamu, M., & Mlangwa, J. (2021). Towards an integrated animal health surveillance system in Tanzania: Making better use of existing and potential data sources for early warning surveillance. BMC Veterinary Research, 17(1), 109. https://doi.org/10.1186/s12917-021-02789-x
- George, J., Häsler, B., Mremi, I., Sindato, C., Mboera, L., Rweyemamu, M., & Mlangwa, J. (2020). A systematic review on integration mechanisms in human and animal health surveillance systems with a view to addressing global health security threats. One Health Outlook, 2(1), 11. https://doi.org/10.1186/s42522-020-00017-4.
- Groseclose, S. L., & Buckeridge, D. L. (2017). Public health surveillance systems: Recent advances in their use and evaluation. Annual Review of Public Health, 38(1), 57–79. https://doi.org/10.1146/annurev-publhealth-031816-044348
- Guernier, V., Goarant, C., Benschop, J., & Lau, C. L. (2018). A systematic review of human and animal leptospirosis in the Pacific Islands reveals pathogen and reservoir diversity. PLoS Neglected Tropical Diseases, 12(5), e0006503. https://doi.org/10.1371/journal.pntd.0006503
- Halliday, J., Daborn, C., Auty, H., Mtema, Z., Lembo, T., Bronsvoort, B. M., Handel, I., Knobel, D., Hampson, K., & Cleaveland, S. (2012). Bringing together emerging and endemic zoonoses surveillance: Shared challenges and a common solution. Philosophical Transactions of the Royal Society. London B Biological Sciences, 367(1604), 2872–2880. https://doi.org/10.1098/rstb.2011.036211
- Hassell, J. M., Begon, M., Ward, M. J., & Fèvre, E. M. (2017). Urbanization and disease emergence: Dynamics at the wildlife-livestock-human interface. Trends in Ecology & Evolution, 32(1), 55–67. https://doi.org/10.1016/j.tree.2016.09.012
- Hernández-Jover, M., Phiri, B. J., Stringer, L., & Martínez Avilés, M. (2021). Editorial: Developments in Animal Health Surveillance. Frontiers in Veterinary Sciences, 7, 637364. https://doi.org/10.3389/fvets.2020.637364
- Houe, H., Nielsen, S. S., Nielsen, L. R., Ethelberg, S., & Mølbak, K. (2019). Opportunities for improved disease surveillance and control by use of integrated data on animal and human health. Frontiers in Veterinary Sciences, 6, 301. https://doi.org/10.3389/fvets.2019.00301
- IHR. (2005). International health regulations (2005)—2nd ed. WHO Regional Office for the Western Pacific. http://iris.wpro.who.int/handle/10665.1/10927
- John, T. J., Samuel, R., Balray, V., & John, R. (1998). Disease surveillance at district level: A mode for developing countries. Lancet (London, England), 352(9121), 58–61. https://doi.org/10.1016/s0140-6736(97)10494-9
- Johnson, I., Hansen, A., & Bi, P. (2018). The challenges of implementing an integrated One Health surveillance system in Australia. Zoonoses and Public Health, 65(1), e229–e236. https://doi.org/10.1111/zph.12433
- Kitua, A. Y., Scribner, S., Rasmuson, M., Kambarage, D., Mghamba, J., Mwakapeje, E. R., Chinyuka, H., Bernard, J., Zimmerman, K., Duale, S., & Mutonga, D. (2019). Building a functional national One Health platform: The case of Tanzania. One Health Outlook, 1(1), 3. https://doi.org/10.1186/s42522-019-0003-0
- Kivaria, F. M., & Kapaga, A. M. (2002). Review of current problems and shortcomings in the Tanzanian animal health information system with suggestions on improvement. Onderstepoort Journal of Veterinary Research, 69(4), 305–314. https://repository.up.ac.za/handle/2263/18497
- Kluberg, S. A., Mekaru, S. R., McIver, D. J., Madoff, L. C., Crawley, A. W., Smolinski, M. S., & Brownstein, J. S. (2016). Global capacity for emerging infectious disease detection, 1996–2014. Emerging Infectious Diseases, 22(10), E1–E6. https://doi.org/10.3201/eid2210.151956
- Machalaba, C. C., Salerno, R. H., Barton Behravesh, C., Benigno, S., Berthe, F. C. J., Chungong, S., Duale, S., Echalar, R., Karesh, W. B., Ormel, H. J., Pelican, K., Rahman, M., Rasmuson, M., Scribner, S., Stratton, J., Suryantoro, L., & Wannous, C. (2018). Institutionalizing one health: From assessment to action. Health Security, 16(S1), S37–S43. https://doi.org/10.1089/hs.2018.0064.
- Mboera, L. E. G., Rumisha, S. F., Mbata, D., Mremi, I. R., Lyimo, E. P., & Joachim, C. (2021a). Data utilization and factors influencing the performance of the health management information system in Tanzania. BMC Health Services Research, 21(1), 498. https://doi.org/10.1186/s12913-021-06559-1.
- Mboera, L. E. G., Rumisha, S. F., Sindato, C., Karimuribo, E. D., & Simba, D. (2017). A 3Ms national surveillance platform to detect and respond effectively to public health events in Tanzania. Policy Brief No. NIMR/EPD/010/2017. National Institute for Medical Research, Tanzania.
- Mboera, L. E. G., Sindato, C., Mremi, I. R., Rumisha, S. F., George, J., Ngolongolo, R., Misinzo, G., Karimuribo, E. D., Rweyemamu, M. M., Haider, N., Hamid, M. A., & Kock, R. (2021b). Socio-ecological systems analysis and health system readiness in responding to dengue epidemics in Ilala and Kinondoni districts, Tanzania. Frontiers in Tropical Diseases, 2, 738758. https://doi.org/10.3389/fitd.2021.738758
- Mghamba, J. M., Talisuna, A. O., Suryantoro, L., Saguti, G. E., Muita, M., Bakari, M., Rusibamayila, N., Ally, M., Bernard, J., Banda, R., Mapunda, M., Eidex, R., Sreedharan, R., Sliter, K., Nikkari, S., Saikat, S., Lolong, G. P. M., Verboom, P., Yahaya, A. A., … Fall, I. S. (2017). Developing a multisectoral National Action Plan for Health Security (NAPHS) to implement the International Health Regulations (IHR 2005) in Tanzania. BMJ Global Health, 3(2), e000600. https://doi.org/10.1136/bmjgh-2017-000600
- MoHCDGEC. (2019). Analytical Report to Inform the Tanzania Health Sector Strategic Plan IV, 2015/2016–2019/2020. Ministry of Health, Community Development, Gender, Elderly and Children, United Republic of Tanzania, September 2019.
- MoHSW. (2015). Health Sector Strategic Plan IV. Ministry of Health and Social Welfare, United Republic of Tanzania.
- Morand, S., & Lajaunie, C. (2021). Outbreaks of vector-borne and zoonotic diseases are associated with changes in forest cover and oil palm expansion at global scale. Frontiers in Veterinary Sciences, 8, 661063. https://doi.org/10.3389/fvets.2021.661063
- Morens, D. M., & Fauci, A. S. (2013). Emerging infectious diseases: Threats to human health and global stability. PLoS Pathogens, 9(7), e1003467. https://doi.org/10.1371/journal.ppat.1003467
- Mremi, I. R., George, J., Rumisha, S. F., Sindato, C., Kimera, S. I., & Mboera, L. E. G. (2021). Twenty years of integrated disease surveillance and response in Sub-Saharan Africa: Challenges and opportunities for effective management of infectious disease epidemics. One Health Outlook, 3(1), 22. https://doi.org/10.1186/s42522-021-00052-9
- Nsaghurwe, A., Dwivedi, V., Ndesanjo, W., Bamsi, H., Busiga, M., Nyella, E., Massawe, J. V., Smith, D., Onyejekwe, K., Metzger, J., & Taylor, P. (2021). One country's journey to interoperability: Tanzania's experience developing and implementing a national health information exchange. BMC Medical Informatics and Decision Making, 21(1), 139. https://doi.org/10.1186/s12911-021-01499-6
- Nyatanyi, T., Wilkes, M., McDermott, H., Nzietchueng, S., Gafarasi, I., Mudakikwa, A., et al. (2017). Implementing One Health as an integrated approach to health in Rwanda. BMJ Global Health, 2(1), e000121. https://doi.org/10.1136/bmjgh-2016-000121
- Peyre, M., Pham, H. T. T., Calva, C., Kchulz, K., Delabouglise, A., Goutard, F., Roger, F., & Antoine-Moussiaux, N. (2017). Animal health surveillance constraints in North and South: same-same but different? Proceedings of the 3rd International Conference on Animal Health Surveillance, Rotorua, New Zealand, pp. 105–107.
- Plowright, R. K., Reaser, J. K., Locke, H., Woodley, S. J., Patz, J. A., Becker, D. J., Oppler, G., Hudson, P. J., & Tabor, G. M. (2021). Land use-induced spillover: A call to action to safeguard environmental, animal and human health. Lancet Planetary Health, 5(4), e237–e245. https://doi.org/10.1016/S2542-5196(21)00031-0
- Rahaman, R., Milazzo, A., Marshall, H., & Bi, P. (2019). Is a one health approach utilized for Q fever control? A comprehensive literature review. International Journal of Environmental Research and Public Health, 16(5), 730. https://doi.org/10.3390/ijerph16050730
- Rumisha, S. F., Lyimo, E. P., Mremi, I. R., Tungu, P. K., Mwingira, V. S., Mbata, D., Malekia, S. E., Joachim, C., & Mboera, L. E. G. (2020). Data quality of the routine health management information system at the primary healthcare facility and district levels in Tanzania. BMC Medical Informatics and Decision Making, 20(1), 340. https://doi.org/10.1186/s12911-020-01366-w
- Rumisha, S. F., Mboera, L. E. G., Senkoro, S. F., Gueye, D., & Mmbuji, P. L. (2007). Monitoring and evaluation of integrated disease surveillance and response in selected districts in Tanzania. Tanzania Health Research Bulletin, 9(1), 1–11. https://doi.org/10.4314/thrb.v9i1.14285
- Sabin, N. S., Calliope, A. S., Simpson, S. V., Arima, H., Ito, H., Nishimura, T., & Yamamoto, T. (2020). Implications of human activities for (re)emerging infectious diseases, including COVID-19. Journal of Physiological Anthropology, 39(1), 29. https://doi.org/10.1186/s40101-020-00239-5
- Stärk, K. D. C., Kuribreña, M. A., Dauphin, G., Vokaty, S., Ward, M. P., Wieland, B., & Lindberg, A. (2015). One Health Surveillance—more than a buzz word? Preventive Veterinary Medicine, 120(1), 124–130. https://doi.org/10.1016/j.prevetmed.2015.01.01910
- Taylor, L. H., Latham, S. M., & Woolhouse, M. E. J. (2001). Risk factors for human disease emergence. Philosophical Transactions of the Royal Society. London B Biological Sciences, 356(1411), 983–989. http://www.ncbi.nlm.nih.gov/pubmed/11516376. https://doi.org/10.1098/rstb.2001.0888
- URT. (2013). Population and Housing Census 2012. The United Republic of Tanzania, Dar es Salaam, 2013.
- URT. (2015a). The Disaster Management Act, 2015. The United Republic of Tanzania.
- URT. (2015b). The Statistics Act, 2015. The United Republic of Tanzania.
- URT. (2018). Guidelines for Surveillance of Prioritized Zoonotic Diseases of Human and Animal Health in the United Republic of Tanzania, 2018. Prime Minister’s Office, Dar es Salaam, Tanzania.
- URT. (2020). The National Integrated Disease Surveillance and Response (IDSR) Guidelines, Third Edition, 2020. Ministry of Health, Community Development, Gender, Elderly and Children. Third Edition, 2020.
- URT. (2021). Health Sector Strategic Plan July 2021-June 2026 (HSSP V): Leaving No-one Behind. Ministry of Health, Community Development, Gender, Elderly and Children. The United Republic of Tanzania, Dar es Salaam, Tanzania.
- Wendt, A., Kreienbrock, L., & Campe, A. (2015). Zoonotic Disease surveillance— inventory of systems integrating human and animal disease information. Zoonoses and Public Health, 62(1), 61–74. https://doi.org/10.1111/zph.1212012
- WHO. (2018). Joint External Evaluation Tool. Second Edition, January 2018. The World Health Organization.
- Woolhouse, M. E. J., & Gowtage-Sequeria, S. (2005). Host range and emerging and re-emerging pathogens. Emerging Infectious Diseases, 11(12), 1842–1847. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3367654/pdf/05-0997.pdf 2. https://doi.org/10.3201/eid1112.050997
- Yale, G., Bhanurekha, V., & Ganesan, P. I. (2013). Anthropogenic factors responsible for emerging and re-emerging infectious diseases. Current Science, 105(7), 940–946.
- Yasobant, S., Bruchhausen, W., Saxena, D., & Falkenberg, T. (2021). Systemic factors for enhancing intersectoral collaboration for the operationalization of One Health: A case study in India. Health Research Policy Systems, 19(1), 75. https://doi.org/10.1186/s12961-021-00727-9