
ABSTRACT
Health challenges of communities are often assessed using biomedical or individual risk-based frameworks which are often inadequate for understanding their full extent. We use observations from the global South to demonstrate the usefulness of structural assessment to evaluate a public health problem and spur action. Following newspaper reports of excessive deaths in the marginalised indigenous or Adivasi community of the Pando people in Northern Chhattisgarh in central India, we were asked by the state government’s public health authorities to identify root causes of these deaths. In this rapidly evolving situation, we used a combination of public health, social medicine, and structural vulnerability frameworks to conduct biomedical investigation, social inquiry, and structural assessment. After biomedical investigations, we identified scrub typhus, a neglected tropical disease, as the most likely cause for some of the deaths which was unrecognised by the treating physicians. In the social inquiry, the community members identified the lack of Adivasi status certificates, education, and jobs as the three major social factors leading to these deaths. During the structural assessment of these deaths, we inductively identified the following ten structures– political, administrative, legal, economic, social, cultural, material, technical, biological, and environmental. We recommended improving the diagnosis and treatment of scrub typhus, making the hospitals more friendly for Adivasi people, and tracking the health status of the Adivasi communities as some of the measures. We suggest that a combination of biomedical, social,and structural assessments can be used to comprehensively evaluate a complex public health problem to spur action..
Violence is built into the structure and shows up as unequal power and consequently as unequal life chances. (Johan Galtung (Galtung, Citation1969))
Introduction
A nine-year-old boy in a family of six fell sick in a remote village in northern Chhattisgarh in India. He belonged to the Pando community – a largely forest-dwelling indigenous group, hereafter referred as Adivasi group, living across central India. The child had fevers and was not feeling well. He soon died in the village. The villagers found that the father had a high fever when he performed his last rites. They pooled money to get him to the divisional-level secondary care hospital 100 km away. His second son, 12 years of age, accompanied him. In the hospital, the second son got sick with fever, became unresponsive, and died in the hospital after two days. The father died a day later. In four days, half of the family was dead. The cause of the deaths remained unclear (Mishra, Citation2021).
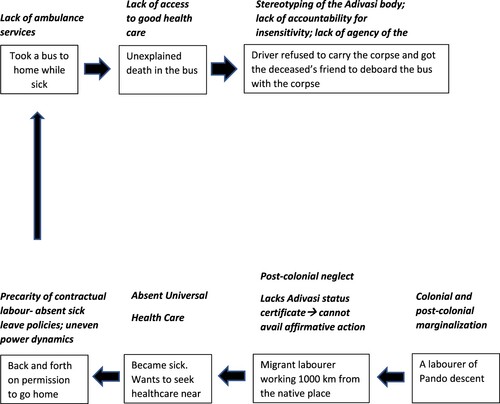
A 28-year-old Pando labourer took ill working on a construction site in another state more than 1000 km away from his home. He requested his supervisor to let him go to his native place. After some effort, he got permission to travel back home. With a friend in tow, he took a bus to his village. He died on the bus. The bus driver did not wish to carry a corpse in his vehicle and made the friend get down with the dead body. The cause of death and of the insensitivity meted out to the Pando remained unclear.
These and a string of deaths in the Pando community in northern Chhattisgarh caused an uproar in the local media (Dutta, Citation2021a; Mishra, Citation2021; Reporter, Citation2021b, Citation2021c). In response, the state government’s health department requested our team of clinicians and public health professionals to evaluate root causes of these deaths. A biomedical approach suggested scrub typhus as the likely cause of some of these deaths which was unrecognised by the treating physicians. In addition to biomedical investigation for disease control and prevention, we conducted social inquiry as well as identified structural aspects underlying these deaths.
The limitations of the use of a purely biomedical approach to investigate health problems have now been flagged for more than two decades, particularly for patients from marginalised communities (Swazo, Citation2005). African American and Hispanic patients were historically caricatured as careless and blamed for their ailments (Metzl & Roberts, Citation2014). In the United States (US), a discourse began on the need for ‘cultural competency’ among clinicians. Cultural competency aimed at informing clinicians and policymakers about culture and its effects on health and healthcare-seeking (Gregg & Saha, Citation2006). The emergence of the concept of cultural competency was a significant development as it emerged during an era when medical care in the US was not acknowledging the importance of culture in the decisions by patients regarding treatment (National Juneteenth Medical Commission). Beyond ethnic minorities, are a multitude of patient populations that face marginalisation. There were calls to incorporate information on marginalised groups that differ by age, gender, and migratory status into the cultural competency framework (Sorensen et al., Citation2017). It was also proposed that cultural competency should address institutional challenges of bullying, harassment, abuse and discrimination and promote a safe and inclusive work culture and study environment (Sorensen et al., Citation2017). In addition, in the last few decades, there has been an improvement in accepting the role of biases and stigma in patient care.
However, Metzl and Hansen suggested a shift in thinking away from cultural competency (Metzl & Hansen, Citation2014). They argued that the assumption that culturally sensitive clinicians will reduce patients’ overall stigma and improve health outcomes is no longer valid in the changing political environment. They brought attention to deeper structures that pose barriers to patient care. Reflecting on the US’ current situation, they provide some examples of these structural problems. For instance, low-income African Americans are unable to comply with doctors’ orders to take their medications with food, not because they have cultural mistrust of the medical establishment but because they live in food deserts with no access to grocery stores. Similarly, Central American immigrants at risk for Type-II diabetes refuse to exercise, not because they are unaware of the benefits of weight reduction but because their neighbourhoods have no gyms, sidewalks, or parks (Metzl & Roberts, Citation2014). These examples take the focus away from individual patient or clinician or the individual risk-based approach to broader structures in which the doctor-patient dyad operates. Scholars in public health, social science, and critical race studies have located stigma outside individuals’ attitudes in the actions of institutions, markets, and healthcare delivery systems (Bonilla-Silva, Citation1997; Hatzenbuehler & Link, Citation2014). There are disparate attempts to highlight these broader structures. For example, students in global health at Harvard learn to think about ‘sickness’, diagnosis, and treatment in relation to food and medication distribution networks (Farmer et al., Citation2006). Moreover, sociologists learn to observe the interplay of social structures and ‘neighbourhood effects’ (Sampson, Citation2012). Borrowing on these structural approaches to inequalities and stigma in healthcare, Metzl and Hansen proposed a concept of ‘structural competency’ in medical education. They proposed training medical students in five core competencies – recognising the structures that shape clinical interactions; developing an extra-clinical language of structure; rearticulating ‘cultural’ formulations in structural terms; observing and imagining structural interventions; and developing structural humility (Metzl & Hansen, Citation2014). Structural competency builds on the concept of social determinants of health – the conditions in which people are born, grow, live, work and age (World Health Organization, Citation2010). Structural competency helps the learner engage with upstream causes of immediately observed downstream factors or helps to engage with the ‘causes of causes’ (Braveman & Gottlieb, Citation2014) and helps health practitioners to engage with patients in a positive and more empathetic way (Neff et al., Citation2020).
Harvey et al. extended the structural competency framework to teaching global health (Harvey et al., Citation2022). Global health is affected by various structures such as the global political economy, systems for international finance, trade agreements and the operations of global corporations (Archer et al., Citation2011; Buyum et al., Citation2020; Oni et al., Citation2019). Recent calls to decolonise global health raise concerns about the inadequacy of existing global health equity frameworks in countering structural oppression or taking notice of laws, policies and norms structurally shaping health (Buyum et al., Citation2020). Along the lines of Metzl and Hansen, Harvey and colleagues suggest five core structural competencies in global health. These include – describing the role of social structures in producing and maintaining health inequities globally; identifying the ways that structural inequalities are naturalised within the field of global health; discussing the impact of structures on the practice of global health; recognising structural interventions for addressing global health inequities; and applying the concept of structural humility in the context of global health (Harvey et al., Citation2022). The structural competency framework can thus be broadened to inform health problems beyond the clinic and help develop solutions.
We applied the lens of ‘structures’ in addition to using biomedical and social inquiry to evaluate the root causes of excess deaths reported among the Pando people, a vulnerable indigenous group in the Northern Chhattisgarh region of India, to find gaps and spur action.
Material and methods
Broader context
The social medicine and public health professionals among the authors (CM, YK and YJ) based out of a not-for-profit organisation Sangwari were asked by the provincial health authority of state government of Chhattisgarh state in India to evaluate the root causes of excess deaths reported among the members of Pando indigenous community by newspapers. The public health department of the state of Chhattisgarh runs health facilities in the state which include district hospitals at district headquarters, community health centres at block headquarters, primary health centres and health and wellness centres catering to smaller population clusters. These facilities are expected to provide tertiary, secondary and primary health care free of cost to people. The department also has a group of village-based health volunteers or community health workers (CHWs) who are village women selected by the village council. They are supposed to mobilise communities to seek care from public health facilities for various programmes such as those related to maternal and child health, immunisation and tuberculosis. They also provide medicines for selected ailments to the patients from their village (see supplementary material for more details).
Sangwari works to improve healthcare of people, especially the marginalised people in the Surguja district in northern Chhattisgarh. It has a team of public health and social medicine professionals, social workers, nurses and pharmacists with 5–25 years of experience in the field. It provides healthcare services through outreach clinics in hard-to-reach areas in Surguja district and has a community health programme covering a population of 50,000 in this district where its community health programme team provides village-based healthcare. Sangwari works with other community-based organisations to highlight health issues faced by marginalised communities. It also works with the public health department to improve healthcare in the Surguja province comprising of five districts (Surguja, Surajpur, Balrampur, Korea and Jashpur) by way to training of healthcare professionals, providing inputs on gaps in healthcare services and advocacy. Close to half of the population of Surguja province is Adivasi.
People from Adivasi communities are referred to as ‘Scheduled Tribes’ in the administrative parlance as these communities are enlisted in a Government of India's schedule (Xaxa et al., Citation2014). The terms Adivasi or indigenous people are politically contested as such a recognition might give them additional rights (Xaxa, Citation1999). They constitute 8.6% population of India and are a heterogeneous group of people with varying cultures, customs and languages distributed in more than 700 distinct groups with a population close to 104 million. Some of these communities are considered by the state government of Chhattisgarh as ‘special backward tribes’ (Chhattisgarh, Citation2022). They largely live in and around forests. The Government of India provides benefits to Adivasi people through affirmative action, such as reservations in jobs, fee waivers, scholarships for education, and stricter punishments for atrocities committed against them. Getting ‘Adivasi status’ or a ‘Adivasi caste certificate’ ensures access to these constitutional benefits. However, even after 70 years of independence, they remain marginalised and have poor socioeconomic status. Their health indicators remain poor compared to other non-Adivasi communities (Bang et al., Citation2018). Traditionally, they were hunter-gatherers and shifting cultivators migrating from one area to another. They were dependent on the forest for their livelihood but were deprived of this way of self-sustenance through various Forest Acts during the British colonial period when the state acquired sweeping control over forests in India and the rights of forest dwellers to collect forest produce, graze cattle or reclaim forest land for cultivation were restricted (Xaxa et al., Citation2014). The colonial era, British rulers exploited forests to generate revenue. Several of these colonial-era practices were continued post-independence, thus depriving Adivasi people of their rights until the recent Scheduled Tribes And Other Traditional Forest Dwellers (Recognition Of Forest Rights) Act, 2006 passed by the parliament of India whereby an attempt is made to correct the historical injustice (Xaxa et al., Citation2014). Although the act was passed in 2006, it is still not fully implemented in many Adivasi regions of India. Since the forested lands inhabited by Adivasi people are also rich in mineral resources and water, they are often the locations for large-scale ‘development’ projects such as mines and dams, which displace Adivasi people from their habitat. This historical context sets the background of our evaluation.
Pando people are one of the Adivasi communities residing in the state of Chhattisgarh in central India. In this state, they predominantly live in the three northern districts of Balrampur, Surajpur and Surguja (see figure 1a and 1b in the supplementary online material for more details). Their population is estimated to be around 40,000 in India. They live in forested and hilly areas and depend on minor forest produce and subsistence farming for their livelihood. Some people migrate temporarily during non-farming seasons to earn a livelihood. Very few have proper jobs. They are being considered for the status of ‘special backward tribes’ by the state government of Chhattisgarh, which imply that they remain underdeveloped and the government will give them additional benefits under the affirmative action policies such as preference in jobs in government institutions, financial incentives for housing and agriculture and educational scholarships.
Geographical setting
Our evaluation took place in the state of Chhattisgarh, which is in the central-eastern part of India. Close to one-third population of the state is Adivasi, predominantly residing in the northern and southern forested parts of the state. Agriculture is the major occupation in the state. The deaths among Pando community were mostly reported from Balrampur and Surguja districts of northern part of Chhattisgarh and hence our inquiry was conducted in these two districts (see supplementary figure 1a and b in the online material for more details). This region has remained underdeveloped, and healthcare facilities are not well developed due to poverty, lack of trained healthcare personnel, and weak healthcare infrastructure. Healthcare is provided predominantly by the Chhattisgarh government’s health service (see supplementary online material for more detailed information on the health services provided by the government) coupled with a few private practitioners.
Information gathering
As we were asked to evaluate the root causes of the deaths among Pando people in a dynamically evolving situation by the public health department, we acted in an ethical imperative and provided support to the public health department. We could not use a formal research method that was planned a priori at the desk but drew upon three broad frameworks – social medicine, public health and structural vulnerability.
While our mandate was to investigate root causes of a high number of deaths in the Pando community, no specific objectives were provided to us by the state government’s public health department. We set the following objectives before the evaluation
estimate the absolute number of deaths in these communities and know if there has been an increase in deaths in the recent months
understand the medical cause of deaths and identify any treatable or preventable cause/s
document the response of the health system
document the health status of these communities
understand the perception of health practitioners and the community regarding potential causes of these deaths and the challenges they face
identify underlying structures that led to these deaths
recommend actions based on the above evaluation to improve the health of Pando people and reduce premature deaths.
We used a multi-layered approach for this inquiry. First, we used a biomedical investigation to identify if there are any preventable medical causes of deaths. Second, we conducted a social inquiry to identify social factors leading to excess deaths and third, we conducted a structural analysis of these deaths to identify gaps in a systematic manner. We then drafted our recommendations regarding potential solutions as the fourth step.
We relied on qualitative information obtained through discussions with community members and leaders and public health professionals as well as observations made by the authors in field and health facility visits and the quantitative information provided to us by the public health department. The information was collected by three authors who are public health professionals and social medicine practitioners (CM, YK, YJ) with 5–20 years of experience in providing healthcare in Adivasi areas and conducting public health research. We invited two additional members – a community leader from the Pando community (UP), a senior rural development practitioner who also belongs to another Adivasi community and the director of a community-based organisation with more than 20 years of experience on health, food, and forest rights for Adivasi people (GP) to join the evaluation process and another public health academic to help with structural analysis (MK). UP, who is a community leader from the Pando community helped to organise some of the meeting with the community members. We are cognizant of the fact that authors other than UP and GP are not Adivasis.
Stakeholder meetings
We first identified the key stakeholders. These included families of three recently deceased patients, Pando patients admitted in the wards of block and district-level hospitals in the Balrampur district and the divisional medical college at Ambikapur in Surguja district, community members, CHWs working in and around villages where one of these patients lived, medical officers working in one primary health centre (Ramchandrapur), three block-level hospitals (Ramanujganj, Wadruffnagar, Rajpur) and the district hospital in the Balrampur district, public health officials in these three blocks and at the district levels as well as medical superintendent and dean of the divisional medical college and the joint director of the public health system in the division. We (CM, YK) conducted one meetings with a total of 14 women CHWs. Also, we (CM, YK, YJ) met more than 15 Pando patients who were admitted in various public health facilities at the time of our evaluation and interviewed 12 health healthcare authorities in the public health system and informally interacted with more than 20 allied health professionals like, nurses and pharmacists in these facilities.
We visited the houses of deceased patients (CM, YK, YJ) and understood the circumstances around the death of these patients and their perceptions about the healthcare received by the patients and challenges they faced. Discussions with the CHWs focused on challenges faced by Pando community members in seeking healthcare, their healthcare-seeking behaviour and perceptions of the community members regarding the care provided in the public health facilities. Discussions with medical officers and allied health professionals focused on the type of ailments that they see among the patients from Pando community, their perceptions about reported deaths among Pando community members and challenges they face while treating these patients and facilities available for diagnosis and treatment of patients. Discussions with the public health professionals and authorities focused on common public health problems among Pando community members, their perceptions on reported deaths in this community, steps taken by them to prevent further deaths and the challenges they face.
One of the Pando community leaders and an author of this paper (UP) organised a community meeting. Invitation was sent by him to Pando people from over 10 villages. Close to 150 Pando community members attended the meeting and around one-third of the participants in this meeting were women. In this meeting, we asked the attendees regarding their perceptions of the deaths, including the causes of these deaths. It was ensured by the authors (CM, UP, YK) that women were given an equal opportunity to speak in these meeting. To mitigate power dynamics operating as the CM and YK are doctors and are considered more powerful in the community, which may create a fear among participants to speak up about injustice done to them, these authors explained to the community members that there job was to convey to the health authorities the challenges faced by the Pando community and so they should speak up freely. UP, who is a community leader from the Pando community further facilitated these discussions.
Authors CM, YK and YJ took detailed notes during these meetings and listed down their observations from the visits to medical facilities with particular attention to the gaps in medical care provided at these facilities.
Quantitative health data
We also systematically analysed anonymised data provided by the health authorities at the two districts’ medical facilities and the public health system. Following data sets were used: (a) narrative reports of 47 deaths from the Pando community between April and October 2021 in the Balrampur district; (b) details of eleven deaths from Pando community that occurred in the District Hospital, Ambikapur between July and September 2021; (c) reports from nine patients at the District Hospital (Ambikapur), admitted to the facility for a febrile illness with multi-system involvement in November 2021. This information was used to identify potential causes of death and the frequency of these causes, clinical characterisation of patient’s symptoms and analysis of laboratory findings.
Structural analysis
Three authors (CM, YK, YJ) made field notes throughout the evaluation. Extensive discussions were conducted among the authors (CM, YK, YJ, MK, UP and GP). Finally, being cognizant of the structural framework, we iteratively identified structural factors in the deaths using the field notes for critical reflection. Stonington et al define ‘social structure’ as durable patterned arrangement – from language barriers and social hierarchies to policies, economic systems, and other institutions (such as judicial systems, and educational systems) – that produce and maintain social inequalities and health disparities, often along the lines of social categories such as race, class, gender, and sexuality (Stonington et al., Citation2018). Thus, these structures are the determinants of social determinants themselves. A structural analysis tries to identify structures underlying health-related behaviour of an individual or a community that determines what happens to an individual’s or community’s health. We did this by first collating the information collected from biomedical investigations, including the gaps in the healthcare system and a social inquiry. We deliberated them among ourselves to identify the structures underlying these deaths. This involved an inductive process whereby these structures were not apriorily defined but were allowed to emerge from the field observations and discussions among the authors (Patton, Citation1990). We then identified structural determinants for each of these structures, structural vulnerability and violence. The recommended actions for the purpose of our report were attempts to address the structural factors leading to poor health among Pando community. The discussions with community members helped us further identify critical structural factors.
Results
Biomedical investigations
Based on the narrations of the CHWs and the treating physicians in the Balrampur district, fever of unknown origin accounted for 23% of all deaths in the Balrampur district. While among Pando patients admitted at the District Hospital Ambikapur, close to three forth (8/11) died due to this cause. The presence of deaths due to acute undifferentiated fever with multiorgan dysfunction which is a common feature of scrub typhus and recent reports of scrub typhus emerging as an important cause of acute febrile illness in central India made us suspect scrub typhus as a potential underlying cause on some of the deaths due to fever of unknown origin (Vikram et al., Citation2019). As a preliminary exercise, we recommended the treating doctors to send the serum samples of a selected group of patients with fever and multiorgan involvement who were admitted in the district hospitals at Ambikapur and Balrampur at the time of our evaluation to a national facility where serological testing for scrub typhus by ELISA (IgM) was available. Four out of nine patients admitted to the District Hospital, Ambikapur and Balrampur had elevated IgM against scrub typhus. These were the district hospitals where maximum deaths occurred. These findings hinted at scrub typhus as a potential cause of the deaths due to fever of unknown origin. None of the patients who died due to the febrile illness had received doxycycline or azithromycin, which are effective treatments for scrub typhus. No laboratory tests were available to diagnose scrub typhus in any of the healthcare facilities in the entire division with a population of four million. There was little to no awareness of the disease among healthcare workers and administrators at all levels, including specialist doctors. It was possible that there was an outbreak of scrub typhus in this region, but the public health system was unable to detect it due to a lack of local epidemic investigation capacity.
At the health systems level, there was a shortage of staff, laboratory services and inadequate documentation of patient’s course in the hospital. This was largely seen as something for which action could be taken up at the state level. The inability to provide a reasonable quality of healthcare to people from Adivasi communities was acknowledged as an overall weakness of the health system. Most healthcare providers could not provide specific reasons for this weakness. There were no members from the Pando community working at the district hospital in the district where maximum deaths were reported. There was no representation of the community in the Patient Welfare Committees.
While the information on deaths from the Pando community was provided to us, whether they represented all the deaths from this community could not be confirmed. In India, a majority of deaths occur at home and are not medically certified. Also, some are not notified to the health or civic authorities in the district. Therefore, we could not estimate death rates or the causes of death for all deaths at the community level as both need information on all deaths in the community as well as the total population. This was one of the examples of ‘health data poverty’ for this marginalised community (Ibrahim et al., Citation2021).
The health system started responding to the situation by enumerating the number of patients admitted daily from the Pando and other vulnerable Adivasi communities. Arrangements were made to provide free food to patients and all their accompanying relatives from these communities. Transport arrangements were made to ferry patients to the public hospitals and back to their villages. Senior officers in the public health system supervised the arrangements. The public health system conducted village health camps to screen patients for symptoms of any illness and these patients were brought to the community health centres or the district hospital. However, a public health officer admitted that ‘these (measures) can not be sustained for long’.
Social inquiry
We interacted with members from Pando community to understand the community’s perspective towards health and healthcare services, changes with time and their view about the social causes of excess deaths. These interactions took place during the field visits to villages of the deceased patients and a meeting of community members and leaders in two villages.
The community members across the meetings conveyed three reasons for excess deaths – the lack of Adivasi status certificates, education, and jobs. Many members of the community found it hard to get this certificate due to technical issues such as lack of records indicating their settlement in an area from their erstwhile status as migrants, misspelling of their names in available documents needed for this purpose, intermarrying people from another community (Parhaiya) which is considered Adivasi in the neighbouring state (Jharkhand) but not considered as Adivasis in the state of Chhattisgarh due to administrative rules and so forth. ‘As we do not have caste (Adivasi status) certificate, we are marginalised’, said one community leader. They highlighted that due to a lack of the certificate, the students from the Pando community could not avail government scholarships to pursue higher education. This, in turn, hampered their upward social mobility. Similarly, employment opportunities are limited for them as they cannot avail the benefits of the government’s affirmative action policies. The lack of jobs for the community’s youth has made senior community members sceptical about the value of education. The elders’ opinion was that ‘if the youth cannot get a job after school education, then there is no point going for it. Instead, the youth should work on farms’. Lack of a documented Adivasi status also makes them vulnerable to exploitation and oppression by members of other castes in their villages. They reported instances where their lands were grabbed by members of other social groups which have more political clout. There were instances of them being beaten up by the members of other social groups on suspicion of theft. The perpetrators were not handed stricter punishments – a provision available to scheduled castes or Adivasis (scheduled tribes) – as the affected Pando people did not have an Adivasi status certificate needed to enforce what is called the Scheduled Caste and Scheduled Tribe (Prevention of Atrocities) Act (passed in 1989). Due to this perpetual violence and the government's inability to protect them, there was a lack of trust in the government system, including health services.
In addition to the above challenges, some families faced a risk of hunger. One young community member remarked ‘food ration (provided by the government’s welfare scheme) is not enough when we have more people at home’. Access to safe water in the form of tap water and/or handpumps was not available in some villages. One community member stated ‘we do not have good drinking water. We do not have taps or handpumps and drink water from wells. Because of this we have more health problems’. The community members alleged that handpumps meant for hamlets where Pando community members lived were installed in hamlets where people from other social groups lived. One member remarked – ‘handpumps given to our para (hamlet) have been diverted to other paras (where people from other social groups lived)’. In one of the Pando villages, we witnessed many toilets and houses built through government schemes dilapidated due to poor construction materials. Women shared a disappointment with the lack of good roads in their hamlets. One lady remarked – ‘as we do not have access to roads, ambulance does not come near our house’. The lack of roads creates difficulty in transporting pregnant ladies at the time of delivery and other sick patients. The community tried to address this issue by themselves – ‘our para (hamlet) did not have good access road. We built one by ourselves’. This was an indication of structural neglect of the Pando people.
We met the CHWs in the public health system who work in the blocks of Balrampur district where many Pando people live. There were very few CHWs from the Pando community. They reported that some healthcare services in the public health system have improved over the years. An important observation shared by many CHWs was the expectations from the community members that CHWs should help them navigate the health system when they seek care at public health facilities. The CHWs stated that patients feel their presence is reassuring in an unfamiliar hospital setting. Currently, CHWs only accompany pregnant mothers for delivery.
Structural analysis of deaths
We reflected and deliberated on our observations, field notes and the gathered data to identify upstream structural factors or understand the ‘structural pathogenesis’ for the reported excess deaths among the Pando community members.
We started with the widely reported death of the migrant Pando in the bus, discussed in the introduction. Through discussions, it was obvious that several structural factors were responsible for these deaths, as shown in .
Figure 1. Structural factors underlying an untimely death of a young labourer from the Pando community.
We then conducted a structural analysis of deaths at the community level. We have summarised the identified structures, components of structural vulnerability and manifest structural violence in . We used this analysis to systematically identify actions that need to be taken to address the structural factors to mitigate preventable deaths among Pando people.
Table 1. Structures identified while evaluating causes of excess deaths among Pando people along with their determinants, vulnerabilities and violence and proposed solutions.
We found that the structural inequalities related to the provision of healthcare to Pando people were either unrecognised or deliberately neglected. They were thus normalised at three levels – the bureaucracy, the health system, and the community. In the bureaucracy, the Pandos faced difficulty obtaining Adivasi status or caste certificate depriving them of affirmative action policies. The bureaucracy was caught in the maze of rules and regulations for designating an individual as an Adivasi community member. In the health system, Pandos were stereotyped as regressive and were blamed for excessive death and therefore no need was felt to give them a special status and protect their health. For example, the healthcare workers at all levels of public health services blamed these deaths on poor or delayed healthcare seeking and low level of awareness among the Pando people. They also conveyed a stereotypical notion about the community. As one of the functionaries in the public health system remarked, ‘these people drink water from ponds and eat stale food. So obviously they are going to have illnesses’. This stereotype consisted of the Pando people being unclean, not interested in education, employment or engagement with the government health system and perpetually intoxicated due to alcohol. They believed any support to them was not going to improve their health. They also believed that the issue of excess deaths is not accurate. Reporting these deaths in the newspapers was considered a political ploy by the Pando people as expressed by a physician working in the public health system ‘the issue of excess deaths is not real. Pando people are dying due to causes which are not very different from those of other rural people. They are not Adivasi. It is a political ploy to get themselves the Adivasi status (which will get then the benefits of the affirmative action)’.
In the society, Pando community members faced oppression, extraction, and violence and other communities were not bothered to understand the difficulties faced by them.
Actions taken
We presented the report of the evaluation (see supplementary online material) to the health minister as well as health authorities of the state of Chhattisgarh. To improve the healthcare delivery to Pando people we recommended various steps, including generation of data on causes of death among Pando people to make informed decisions, strengthening diagnostic facilities for scrub typhus, use of doxycycline or azithromycin among patients with fever of unknown origin. A prominent and aspirational recommendation was for creation of Adivasi-friendly healthcare facilities. We recommended six steps to make a health facility Adivasi-friendly ensuring that – (1) there is no need for out-of-pocket expenditure; (2) there is arrangement for food for patients and all accompanying family members and arrangement for referral and transportation of patients; (3) a help desk staffed by a member from the Adivasi community and a patient navigator to help patients navigate the hospital; (4) individuals from Adivasi community are recruited in the hospital as staff members including in patient welfare committees; (5) community engagement/outreach by the hospital staff to understand the culture and customs of the community and to build a bond; and (6) sensitisation of the hospital’s staff to the historical inequalities faced by the people from Adivasi communities and a need for understanding their side of the story. We also flagged structural reasons behind excess deaths and recommended streamlining the procedures to provide Adivasi status certificate and creating educational and employment opportunities for people from the Pando community.
After our evaluation, the Government Medical College at Ambikapur procured and started conducting serological tests for scrub typhus and has planned a regional conference on this topic to sensitise healthcare providers about this neglected yet prevalent cause of death in the vulnerable population.
In addition to providing recommendations to the government, we have started collaborating with the Pando community to help them highlight this problem at the national level. We helped the Pando community members draft and submit a petition to the Ministry of Tribal Affairs of the Government of India regarding their grievances related to the Adivasi status certificate. In order to make health care more accessible, we have trained about 150 volunteers from nearly 60 villages where Pando people lived to identify common ailments like diarrhoea and fevers, provide community-based treatment of these conditions and make appropriate referrals.
Discussion
Our inquiry into excess deaths among Pando people found various structural problems, continued structural violence and vulnerability in this community. In the high-income country settings, structural competency is emerging as a new way to sensitise and train doctors and public health personnel to identify upstream causes and go beyond the pure biomedical explanations of disease. Examples from the global south, especially India, have been limited, though. As a group of health practitioners interested in the health of the people from Adivasi communities, we went a step beyond and used this broad approach to evaluate root causes of excessive deaths in an Adivasi community in central India. We have conducted a structural analysis of a public health problem. We iteratively evolved a structural framework to understand gaps and spur action to improve the health and socioeconomic condition of the Pando people. The analysis helped us think beyond determinants like malnutrition and poverty and identify bureaucratic, environmental, material, technical and other upstream factors leading to deaths among the Pando community members.
People from Adivasi communities are more likely to die than non-Adivasi people in India (Mishra et al., Citation2020) and have a lifespan shorter by at least five years (Vyas et al., Citation2022). Previous inquiries into deaths of people from Adivasi communities have identified poverty, malnutritional and barriers to accessing healthcare as potential concerns (Sri et al., Citation2012). After multiple committees appointed by the Government of India, reports, and efforts by stakeholders, the improvement in the health of Adivasis has been painfully slow. The approach to improving the health of the communities has largely been through medical interventions such as providing safe delivery services, vaccinations, and facilities for early diagnosis and treatment of malaria or treatment of diarrhoea with oral rehydration solutions. However, delivery of these services into areas inhabited by Adivasis has been slow and there has been a lack of cultural sensitivity (George et al., Citation2020; Sundararajan et al., Citation2013). Social determinants of health are increasingly being recognised as important factors in maintaining health disparities and there are calls to act on them (World Health Organization, Citation2010). For example, there is some success in India in reducing poverty over last several decades (Datt et al., Citation2016). However, the disparity in income has increased and Adivasis continue to be among the most poor and marginalised (Mohanty, Citation2020). They are often the victims of projects meant to bring money for the exchequer of the state government, e.g. mining. While the population of Adivasis in India is 8.6%, 40–50% of people who are displaced by ‘development’ projects such as mines and dams are Adivasi people (Singh Negi & Ganguly, Citation2011). This displacement is not by their choice. We observed that people from other communities often blamed Pando people for not making right choices related to health. However, can Pando people make free choices? Their choices, ‘are limited by racism, sexism, political violence and grinding poverty’ as Farmer has remarked (Farmer, Citation1996).
While the Government of India has tried to create a mechanism for protecting the rights of the Adivasis and help in their socioeconomic development, through efforts such as creation of a separate ministry of tribal affairs, the efforts have not borne enough success. This ministry can only give money to other ministries to implement projects for people from Adivasi communities and often has no control over the implementation. The money allocated for the development of Adivasis is often diverted for infrastructure projects not directly meant for these people (Nayak, Citation2022). Also, as Adivasis are divided into more than 700 groups, their individual population in an electoral district is small, politicians are often not interested in wooing them and working for their development. The plight of the Adivasis is often paid some attention to when there are excess deaths reported in the media, thus they are recognised only in death. Political parties fight over newspaper reports of excess deaths with the opposition parties building pressure on the ruling party (Dutta, Citation2021b) and the ruling party denying it (Reporter, Citation2021a, Citation2021c). Some knee-jerk efforts are taken to assuage public sentiments but then the matter is largely forgotten. The insensitivity of the healthcare functionaries, lack of the ability to understand their issues when availing health care facilities related to limited economic resources, lack of food security at home, lack of caregiver support in the hospital and at home and dealing with an alien atmosphere in a medical facility like a district hospitals and medical college leads to aversion to public health facilities among Adivasi people.
Communicating with the community as manifest structural humility also helped us go beyond the short-sighted identification of factors like disruption of care due to COVID-19 duties as the sole factor. Similar excessive deaths have been previously reported among the Pando community members and highlight the importance of examining structural issues at play (Drolia, Citation2017). It brought to light the challenges faced by the community in accessing quality healthcare which becomes invisible as existing structures normalise them. For instance, a highly biased assessment of deaths among Adivasis stated on record that ‘there is a tendency among the tribals to believe in quack and exorcism without taking medical advice, neglecting eating habits, excessive consumption of alcohol and not following medical advice’ (Reporter, Citation2021c). However, there is no talk about the public health care set up which is inaccessible, of poor quality, unaffordable, alien and unwelcoming. A recent news report on death in a Pando woman said the woman did not take medicines as advised (Reporter, Citation2021b). However, it did not talk about the availability of medicines or what prevented her from appropriate health access. In one of the deaths reported in the newspaper, Pando people pooled money to get the patients to the hospital (Mishra, Citation2021). Our focus on structures helped us identify and articulate why this stereotyping is wrong.
We used three broad frameworks for our inquiry. The public health framework focuses on the prevention and control of diseases and deaths, the social medicine one on social factors that determine health and illness, and the structural vulnerability one on structural forces (e.g. class, race, policies and laws) which contribute to inequities in health rather individual’s behaviour being the sole factor responsible. Based on these frameworks, we used a combination of biomedical investigation, social inquiry and structural analysis to get a broader understanding into the deaths among Pando people to understand the ‘causes of causes’. This layered approach helped us identify potential solutions which are not restricted to the medical domain. For example, social inquiry helped us understand lack of representation of Pando community members in the public health system and the need for Adivasi-friendly hospital and its components. The structural analysis, in addition, helped us see inherent biases and stereotyping of Pando people, which was common among public health professionals and a need to sensitise health professionals to historical injustice done to Adivasi people. Thus, in our opinion, these three frameworks worked complementarily to bring out a more comprehensive pathogenesis of deaths among Pando people.
There were several limitations to our observations. This was not a prospectively planned study due to the nature of rapidly evolving circumstances. We relied only on the data provided to us by the provincial health department which was inadequate and incomplete. Thus, we had to make certain assumptions. Data provided with respect to deaths among Pando community members were not assigned any cause of death. A preliminary inquiry told us that several deaths were due to fever. However, we could not conclusively establish scrub typhus among those who died. Data from other government departments were not available as our investigation was mandated only by the provincial health department. As a result, issues related to social determinants highlighted in our paper are based on anecdotal experience shared by community members and larger national-level surveys done which highlight poor status of these determinants in general for Adivasi communities. Local data to highlight these points were not available.
Several factors needed greater and deeper inquiry – for example, the issue of lack of Adivasi caste certificates, forest, and land rights among marginalised Adivasi groups. We believe these issues need further research by subject experts. We have applied the approach of structures to an emergent rapidly evolving situation where the time we had to evaluate causes of death was limited. The evaluation was conducted by a group of health professionals experienced in providing health care to indigenous people but would have been further enriched by involving sociologists, anthropologists, political scientists, historians, adding theoretical richness to the paper and helping in a deeper understanding of the deeper structures determining health of the Pando people. The lens of our evaluation is predominantly going to be that of social medicine and public health given the background of majority of the authors in these fields. However, we have tried to balance this approach by including authors (UP, GP) whose area of work is that of social justice. Although all the non-Adivasi authors have provided healthcare in Adivasi areas, having more or all the investigators from the Adivasi community would have been ideal as the non-Adivasi authors would lack a lived experience of social discrimination faced by the Adivasi community members. Furthermore, we could identify ten structures during our evaluation of causes of excess deaths among Pando community members and there is a possibility that we could have missed additional structures. Also, while we conducted a structural analysis of deaths looking at factors beyond the healthcare system, the recommendations we could give were mainly related to the healthcare domain.
To our knowledge, this is the first attempt to use a structural analysis approach to understand and address a problem in one of the most marginalised indigenous communities in India. The non-agentic view of structural competency is in contrast with the individual risk-based approach, which is mainstreamed in public health investigation. In addition, we involved community members and two community leaders working for community's development to help with the structural assessment of deaths among Pando people thus reducing the risk of missing some aspects while using a purely clinical or public health approach. This is a strength of this paper. Such an approach to identifying structural factors underlying a public health problem can potentially help in developing long-term solutions. Our work can provide a case study for structural competency training in both the global south and north.
Acknowledgements
We are thankful to Pando community members who actively participated in the discussions, members of the public health department of districts of Balrampur and Surguja in the state of Chhattisgarh, who provided the necessary information.
Data availability statement
Not applicable.
References
- Archer, N., Moschovis, P. P., Le, P. V., & Farmer, P. (2011). Perspective: Post earthquake Haiti renews the call for global health training in medical education. Academic Medicine, 86(7), 889–891. https://doi.org/10.1097/ACM.0b013e31821b3e14
- Bang, A., Jhalani, M., Angami, N., Beck, H., Jain, Y., Kujur, J., Mavalankar, D., Ram, F., Singh, N., Sudarshan, H., Sundararaman, T., & Kumar, S. (2018). Report of the Expert Committee on Tribal Health. G. O. I. Ministry of Health & Family Welfare. https://nhm.gov.in/New Updates 2018/NHM Components/Health System Stregthening/tribal health/Tribal-Health-Report.pdf
- Bonilla-Silva, E. (1997). Rethinking racism: Toward a structural interpretation. American Sociological Review, 62, 465–480. https://doi.org/10.2307/2657316
- Bourgois, P., Holmes, S. M., Sue, K., & Quesada, J. (2017). Structural vulnerability: Operationalising the concept to address health disparities in clinical care. Academic Medicine, 92(3), 299–307. https://doi.org/10.1097/ACM.0000000000001294
- Braveman, P., & Gottlieb, L. (2014). The social determinants of health: It’s time to consider the causes of the causes. Public Health Reports, 129(1_suppl2), 19–31. https://doi.org/10.1177/00333549141291S206
- Buyum, A. M., Kenney, C., Koris, A., Mkumba, L., & Raveendran, Y. (2020). Decolonising global health: If not now, when? BMJ Global Health, 5(8), e003394. https://doi.org/10.1136/bmjgh-2020-003394
- Chhattisgarh Government. (2022). Special backward tribes of Chhattisgarh. Retrieved May 4 from http://cgtrti.gov.in/PVTG.html#:~:text=%22%20Birhor%20%22,were%20male%20and%201578%20female
- Datt, G., Martin, R., & Murgai, R. (2016).Growth, urbanization, and poverty reduction in India. (Policy Research Working Paper; No. 7568). W. Bank. https://openknowledge.worldbank.org/handle/10986/23896
- Drolia, R. (2017). National Commission for ST to probe deaths of 29 Pando tribes in Chhattisgarh. The Times of India . https://timesofindia.indiatimes.com/city/raipur/national-commission-for-st-to-probe-deaths-of-29-pando-tribals-inchhattisgarh/ articleshow/60955755.cms.
- Dutta, A. (2021a, October 13). Malnutrition deaths of Pando people highlight systemic failure. The Hindu. Retrieved March 22 from https://www.thehindu.com/news/national/other-states/malnutrition-deaths-of-pando-people-highlight-systemic-failure/article36976025.ece
- Dutta, A. (2021b). Malnutrition deaths of Pando people highlight systemic failure. The Hindu. https://www.thehindu.com/news/national/other-states/malnutrition-deaths-of-pando-people-highlight-systemic-failure/article36976025.ece
- Farmer, P. (1996). On suffering and structural violence: A view from below. Daedalus, 125(1), 261–283. http://www.istor.org/stable/20027362
- Farmer, P. E., Nizeye, B., Stulac, S., & Keshavjee, S. (2006). Structural violence and clinical medicine. PLoS Medicine, 5(10), 1686–1691. https://doi.org/10.1371/iournal.pmed.0030449
- Galtung, J. (1969). Violence, peace, and peace research. Journal of Peace Research, 6(3), 167–191. https://doi.org/10.1177/002234336900600301
- George, M. S., Davey, R., Mohanty, I., & Upton, P. (2020). ‘Everything is provided free, but they are still hesitant to access healthcare services’: Why does the indigenous community in Attapadi, Kerala continue to experience poor access to healthcare? International Journal for Equity in Health, 19(1), 1–15. https://doi.org/10.1186/s12939-020-01216-1
- Gregg, J., & Saha, S. (2006). Losing culture on the way to competence: The use and misuse of culture in medical education. Academic Medicine, 81(6), 542–547. https://doi.org/10.1097/01.ACM.0000225218.15207.30
- Harvey, M., Neff, J., Knight, K. R., Mukherjee, J. S., Shamasunder, S., Le, P. V., Tittle, R., Jain, Y., Carrasco, H., Bernal-Serrano, D., Goronga, T., & Holmes, S. M. (2022). Structural competency and global health education. Global Public Health, 17(3), 341–362. https://doi.org/10.1080/17441692.2020.1864751
- Hatzenbuehler, M. L., & Link, B. G. (2014). Introduction to the special issue on structural stigma and health. Social Science & Medicine, 103, 1–6. https://doi.org/10.1016/j.socscimed.2013.12.017.
- Ibrahim, H., Liu, X., Zariffa, N., Morris, A. D., & Denniston, A. K. (2021). Health data poverty: An assailable barrier to equitable digital health care. The Lancet Digital Health, 3(4), e260–e265. https://doi.org/10.1016/S2589-7500(20)30317-4
- Metzl, J. M., & Hansen, H. (2014). Structural competency: Theorising a new medical engagement withstigma and inequality. Social Science and Medicine, 103, 126–133. https://doi.org/10.1016/i.socscimed.2013.06.032
- Miller, S. (2019). Social institutions. https://plato.stanford.edu/archives/sum2019/entries/social-institutions/
- Mishra, R. (2021, August 18). 3 members of Pando tribe die due to multiple organ failure in Chhattisgarh. Hindustan Times. Retrieved March 22 from https://www.hindustantimes.com/cities/others/3-members-of-pando-tribe-die-due-to-multiple-organ-failure-in-chhattisgarh-101629289541003.html
- Mishra, U. S., Rinju, R., & Panda, B. K. (2020). Gauging class and caste differences in mortality: The Indian experience. Journal of Death and Dying, 86(1), 4–20. https://doi.org/10.1177/0030222820959970
- Mohanty, A. (2020, September 8). Pro-poor schemes in plenty, but no end to tribal community struggles. Down to Earth. Retrieved April 19 from https://www.downtoearth.org.in/blog/governance/pro-poor-schemes-in-plenty-but-no-end-to-tribal-community-struggles-73273
- National Juneteenth Medical Commission. http://www.amaapology.com/
- Nayak, V. (2022, April 24). The fate of SC/STfunds is a secret even to the sarkar! Deccan Herald. Retrieved April 26 from https://www.deccanherald.com/opinion/the-fate-of-sc/st-funds-is-a-secret-even-to-the-sarkar-1103397.html
- Neff, J., Holmes, S. M., Knight, K. R., Strong, S., Thompson-Lastad, A., McGuinness, C., Duncan, L., Saxena, N., Harvey, M. J., Langford, A., Carey-Simms, K. L., Minahan, S. N., Satterwhite, S., Ruppel, C., Lee, S., Walkover, L., De Avila, J., Lewis, B., Matthews, J., & Nelson, N. (2020). Structural competency: Curriculum for medical students, residents, and interprofessional teams on the structural factors that produce health disparities. MedEdPORTAL: The Journal of Teaching and Learning Resources, 16, 10888–10888. https://doi.org/10.15766/mep2374-8265.10888
- Oni, T., Yudkin, J. S., Fonn, S., Adongo, P., Kaseje, M., Ajuwon, A., Doyal, L., & London, L. (2019). Global public health starts at home: Upstream approaches to global health training. The Lancet Global Health, 7(3), e301–e302. https://doi.org/10.1016/S2214-109X(18)30558-8
- Patton, M. Q. (1990). Qualitative evaluation and research methods. Sage. 536 p
- Reporter. (2021a, September 22). BJP alleges Pandos neglected, Baghel denies. VisionMP. http://www.visionmp.com/regional-mp-cg/bip-alleges-pandos-neglected-baghel-denies/
- Reporter. (2021b, September 17). C’garh govt denies malnutrition death. The Pioneer. https://www.dailypioneer.com/2021/state-editions/c—garh-govt-denies—malnutrition-death.html.
- Reporter. (2021c, September 23). Death of 20 Pando tribals due to diseases. The Pioneer. https://www.dailypioneer.com/2021/state-editions/death-of-20-pando-tribals-due-to-diseases.html.
- Sampson, R. J. (2012). Moving and the neighborhood glass ceiling. Science, 337(6101), 1464–1465. https://doi.org/10.1126/science.1227881
- Singh Negi, N., & Ganguly, S. (2011). Development projects vs. internally displaced populations in India: A literature based appraisal.
- Sorensen, J., Norredam, M., Dogra, N., Essink-Bot, M.-L., Suurmond, J., & Krasnik, A. (2017). Enhancing cultural competence in medical education. International Journal of Medical Education, 8, 28–30. https://doi.org/10.5116/ijme.587a.0333
- Sri, B. S., Sarojini, N., & Khanna, R. (2012). An investigation of maternal deaths following public protests in a tribal district of Madhya Pradesh, Central India. Reproductive Health Matters, 20(39), 11–20. https://doi.org/10.1016/S0968-8080(12)39599-2
- Stonington, S., Homes, S., Hansen, H., Greene, J., Wailoo, K., Malina, D., Morissey, S., Farmer, P., & Marmot, M. (2018). Case studies in social medicine—Attending to structural forces in clinical practice. New England Journal of Medicine, 379(20), 1958–1961. https://doi.org/10.1056/NEJMms1814262
- Sundararajan, R., Kalkonde, Y., Gokhale, C., Greenough, P. G., & Bang, A. (2013). Barriers to malaria control among marginalised tribal communities: A qualitative study. PLoS One, 8(12), e81966. https://doi.org/10.1371/journal.pone.0081966
- Swazo, N. K. (2005). Research integrity and rights of indigenous peoples: Appropriating Foucault’s critique of knowledge/power. Studies in History and Philosophy of Science Part C: Studies in History and Philosophy of Biological and Biomedical Sciences, 36(3), 568–584. https://doi.org/10.1016/i.shpsc.2005.07.006
- Vikram, K., Agarwala, P., Bhargava, A., Jain, Y., Jagzape, T., & Wasnik, P. (2019). Scrub typhus and leptospirosis in rural and urban settings of central India: A preliminary evaluation. Tropical Doctor, 50(2), 111–115. https://doi.org/10.1177/0049475519889712
- Vyas, S., Hathi, P., & Gupta, A. (2022). Social disadvantage, economic inequality, and life expectancy in nine Indian states. Proceedings of the National Academy of Sciences, 779(10), e2109226119. https://doi.org/10.1073/pnas.2109226119
- World Health Organization. (2010). A conceptual framework for action on the social determinants of health. World Health Organization. https://apps.who.int/iris/handle/10665/44489
- Xaxa, V. (1999). Tribes as indigenous people of India. Economic & Political Weekly, 34(51). https://www.epw.in/journal/1999/51/special-articles/tribes-indigenous-people-india.html.
- Xaxa, V., Ramanathan, U., Bara, J., Misra, K. K., Bang, A., Basant, S., & Panda, H. (2014). Report of the high-level committee on socioeconomic, health and educational status of tribal communities of India. http://archive.indianstatistics.org/misc/xaxacommittee.pdf
