
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
Even with a reduced burden of malaria in sub-Saharan Africa (SSA), differences remain in the rate of change among countries and sub-regions. We used data from the Global Burden of Disease Study 2019 to establish the relationship between Development Assistance for Health (DAH) and governance and trends in malaria burden in SSA. The trend was estimated using the Joinpoint regression program and the Institute of Health Metrics and Evaluation’s DAH database, and World Bank Governance Indicators to analyze the DAH and governance respectively from 2000 to 2017 and used two-way fixed effects to establish their association with the trend in the period. The findings showed decreases in SSA’s age-standardised rates for disability-adjusted life years (ASDR) (−47% (95% uncertainty interval (UI) −69% to −14%)), deaths (−38% (95% UI −65% to −3%)), incidence (−35% (95% UI −44% to −25%)), and prevalence (−34% (95% UI −43% to −24%)). Decreases in ASDR were associated with increases in DAH (β −134.18, standard error (SE) 27.26) and governance scores (β −246.19, SE 39.13). The association between reductions in malaria burden and increases in DAH and in governance scores shows the need for accelerated funding of malaria programs and advocacy for better disease governance in malaria-endemic countries.
Abbreviations: APC: Annual percentage change; ASDR: Age-standardised disability-adjusted life-year rate; ASIR: Age-standardised incidence rate; ASIR: Age-standardised incidence rate; ASMR: Age-standardised mortality rate; CSSA: Central sub-Saharan Africa; DAH: Development Assistance for Health; DALYs: Disability-adjusted life years; ESSA: Eastern sub-Saharan Africa; GBD: Global burden of disease; GHDx Global Health Data Exchange; IHME: Institute of Health Metrics and Evaluation; SDGs: Sustainable Development Goals; SSA: Sub-Saharan Africa; SSSA: Southern sub-Saharan Africa; UNSD: United Nations Statistics Division; USD: United States dollars; WGI: World Bank Governance Indicators; WHO: World Health Organization; WSSA: Western sub-Saharan Africa
Introduction
According to the World Health Organization (WHO), malaria is a life-threatening disease caused by parasites that are transmitted to people through the bites of infected female Anopheles mosquitoes (World Health Organization, Citation2022a). The disease is estimated to have caused 234 million cases and 593,000 deaths in 2021 and is endemic in 85 countries (World Health Organization, Citation2022b). Malaria is the sixth leading cause of death in low-income countries, of which the majority are in Africa. In 2020 alone, only 29 of the endemic countries accounted for 96% of malaria cases globally. Unsurprisingly, these too are majorly located in sub-Saharan Africa (SSA), with Nigeria’s leading 29% share being followed by the Democratic Republic of Congo’s 12%, Uganda’s 5%, Mozambique’s 4%, and Angola’s 3.4%, among others (World Health Organization, Citation2021). The African region alone had 215 million cases in 2019 and 386,000 malaria deaths in the region, yet like the global trend, malaria in the SSA region has fallen, with the case incidence rate per 1000 population dropping from 362.8 in 2000 to 225.2 in 2019 and deaths per 1000 dropping from 121.1 in 1990 to 40.3 in 2019. However, the burden remains high to date (World Health Organization, Citation2020). The reduction in burden is attributable to interventions, such as the widespread use of insecticide-treated nets and artemisinin-based combination therapy, along with funding from the Global Fund, Bill and Melinda Gates, and the United States (US) Government, and other contributors to the Development Assistance for Health (DAH) (World Health Organization, Citation2020). The DAH is complemented by funding from endemic countries and the engagement of stakeholders through declarations like the Abuja Declaration in 2000, the adoption of malaria alleviation in the Sustainable Development Goals (SDGs) in 2015, and the recent strategic inclusion of country-specific programs in Global Fund financing strategies (World Health Organization, Citation2010, Citation2020).
In response to the high global burden of malaria, aid from governments, individuals, and foreign interventions has been applied over time, and this has had a direct impact on malaria. In 2020, funding for global malaria interventions was estimated at 3.3 billion dollars, an increase from 3 billion dollars in 2019 (World Health Organization, Citation2021). International sources still contribute the largest portion of malaria funding. For example, over 2.2 billion (69%) of the total funding directed for the control and elimination of malaria was contributed by international funders in 2020, with the US (1.3 billion) leading the funders, followed by the United Kingdom, Germany, and France. Seventy-nine percent of the international funding for malaria was directed to the WHO African Region, focusing on the research and development of malaria treatments and prevention methods and, most notably, the widespread use of insecticide-treated nets, indoor residual spread, and artemisinin-based combination therapy (World Health Organization, Citation2021). Although the burden of malaria has gradually decreased and funding has increased, the sub-regions and countries share individual variations in governance, which play a role in the use of funds, the choice of interventions, and the strictness in adhering to standard procedures. This was evident in a comparative study on Uganda and Rwanda’s malaria eradication strategies, which showed how Rwanda’s good political will and high levels of commitment have contributed to more accelerated reductions in the burden of disease compared to Uganda (Kasim, Citation2019).
Governance is a crucial part of all responses worldwide, and disease alleviation processes usually require ready and willing governments armed with a healthcare system that can respond to these diseases (Palagyi et al., Citation2019). The effect of governance on malaria has not been widely studied, but Hsiao and Emdin (Citation2015) found no significant association between governance and malaria mortality, yet their focus was mainly on the association between mortality and the DAH (Hsiao & Emdin, Citation2015). In contrast, a systematic review by Ohiri et al. (Citation2022) indicated that improved governance could lead to potential disease eradication when the authors focused on how governance could lead to malaria eradication using examples from other epidemics, including smallpox, polio, onchocerciasis, and the global coronavirus pandemic control program (Ohiri et al., Citation2022).
Existing literature findings relating governance and the DAH to health differ, with some establishing that governance and accountability affected disease burden, including that of malaria. The affirmers of the DAH and other foreign aid interventions have established the benefits of the funds, arguing that it supports disease alleviation programs while improving institutions, fighting corruption, and supporting development. The recent focus of the Global Fund is on country- and global-level interventions (Kavanagh & Chen, Citation2019; Rannan-Eliya, Citation2022; Sarpong & Bein, Citation2021). However, some studies reported negative facts about the topic, with Easterly (Citation2009) emphasizing the issue of poor governance being a hindrance to the effectiveness of the high investment by developed nations in development programs, including health (Easterly, Citation2009). The argument was furthered by Moyo (Citation2009), who emphasized how corruption in governments and the non-response of foreign aid providers makes it easier for foreign aid to not deliver on its cause (Moyo, Citation2009).
This article seeks to bridge this gap by reporting the 30-year trend in malaria burden in the region and showing the differences in the burden among sub-regions while adding to the literature available to inform stakeholders about the extent to which malaria is in the SSA region. Our study also seeks to extend the span of literature outlining the impact of DAH and governance on the trends in malaria burden.
Materials and methods
Data source
We used data from the Global Burden of Disease (GBD) study that generated estimates for 286 causes of death, 368 causes of non-fatal burden, and 87 risk factors from 204 countries and territories grouped under seven super-regions and 21 regions from 1990 to 2019 (Sharma et al., Citation2022; Vos et al., Citation2020). Modelling and the estimation of GBD results for malaria have been extensively discussed elsewhere (Murray et al., Citation2014).
We extracted data from the GBD results tool on the Institute for Health Metrics and Evaluation (IHME) website (Global Health Data Exchange- GHDx), covering malaria-related annual disability-adjusted life years (DALYs), deaths, prevalence, and incidence for 46 countries in the SSA region and four sub-regional averages (central, eastern, southern, and western SSA subregions). Among the 46 countries in the SSA, according to the IHME database, four countries were excluded from country-specific data analysis. Djibouti and Lesotho had no malaria cases during the period, while Somalia is not considered part of the WHO African Region Office. South Sudan was also not included because of data validation issues, as the nation was established in 2011. The rest of the countries’ data from 1990 to 2019 were extracted alongside regional averages.
We used data on governance attained from the World Bank Governance Indicators (WGI). The WGI uses six indicators: voice and accountability, political stability and the absence of violence, government effectiveness, the rule of law, regulatory quality, and the control of corruption, based on 30 underlying datasets and multiple data sources. The indicators have an annual scale between −2.5 (lowest) and 2.5 (highest) per country. The individual indicators were used in this study and aggregated per year for every country to establish the governance score. Further details about the WGI are found in papers by Kauffman and colleagues at the World Bank (Kaufmann et al., Citation2009, Citation2011).
Data for DAH directed for malaria were extracted from the IHME DAH database from 1990 to 2019. The database includes estimates based on project databases, financial statements, and correspondence with agencies, among other sources. The database’s methodology and estimation procedures have been extensively discussed by GBD collaborators (Institute for Health Metrics and Evaluation (IHME), Citation2020; Micah et al., Citation2020).
Data from the UNdata website was used to estimate the per capita gross domestic product (GDP) in US dollars. The database made by the United Nations Statistics Division (UNSD) includes time series data from 1970 to date for all member countries of the UN. The data are collected through official submissions made by member states annually through the National Accounts Questionnaire, with supplements from data estimates for any years with incomplete or inconsistent information. To estimate the GDP per capita for the United Republic of Tanzania, we averaged the estimates of the Tanzanian mainland and those of Zanzibar (United Nations Statistics Division, Citation2019). Population estimates were extracted from the United Nations Department of Economic and Social Affairs-Population Dynamics found on the UN World Urbanization Prospects (WUP) website (population.un.org/wup) (United Nations, Citation2018).
Measures
We compared the burden in the four sub-regions of the SSA region, including age-standardised rate changes from 1990 to 2019, and also performed a sub-regional level comparison of the number of malaria-related DALYs, deaths, prevalence, and incidence among different age groups (< 5 years, 5–9 years, 10–24 years, 25–49 years, 50–74 years, and 75 + years). The annual percent change (APC) was defined as where i = baseline year (1990-2018). All rates presented are estimates per 100,000 population at risk. In this study, DALYs = years of life lost + years lived with disability.
The countries included in the study were categorised into similar subregions as the IHME classifications. They were included if they had malaria cases during the study period (1990–2019) and were under the WHO African Region Office. Thus, we classified the remaining 42 countries into four subregions: central SSA (CSSA, six countries), eastern SSA (ESSA, 12 countries), southern SSA (SSSA, five countries), and western SSA (WSSA, 19 countries). In the article, when age-standardised rates are used, they are abbreviated as ASMR for mortality, ASDR for DALYs, ASPR for prevalence, and ASIR for incidence.
Statistical analyses
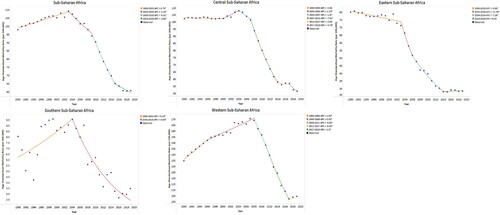
Joinpoint regression was performed for every subregion using the Joinpoint Regression Program (Version 4.9.1.0) developed by the Statistical Research and Applications Branch of the National Cancer Institute (Bethesda, MD, U.S.A.) to establish changes in mortality trends. The program describes changes in data trends by connecting several line segments on a log scale at ‘joinpoints’ (where 0 joinpoints represents a straight line) and tests for model fit with a maximum of five joinpoints. The significance tests use a Monte Carlo permutation method, and the results include an APC in age-standardised rates for each line segment and its corresponding 95% confidence interval (CI). The APC is tested to determine whether a difference exists from a null hypothesis of no change (Dragomirescu et al., Citation2019; Hsiao & Emdin, Citation2015; Park et al., Citation2021; Qiu et al., Citation2009). In our analysis, we focused on regional and subregional trends in the ASMR ().
Figure 1. Joinpoints for the ASMR of Sub-Saharan African and Sub-regions. APC is significantly different from zero at the alpha = 0.05 level.
To study the association between malaria DAH, governance, and the measures of malaria burden, we utilised a two-way fixed effects analysis, capturing country-specific and time-period-specific characteristics that account for the malaria burden in SSA. The following two-way fixed model was used to estimate the association between DAH per capita, governance, population, and malaria DALYs. A similar model was previously used by Hsiao and Emdin (Citation2015).
Where αi is a country-specific fixed effect capturing unobserved, time-invariant country characteristics, malaria_DAH_perCapita is DAH per capita for malaria; governance is the aggregate total of the six world bank governance indicators, and GDP_perCapita and population are control variables. μt is time-period fixed effects and ϵit is the error term. The coefficient of interest is δ, which represents the change in malaria mortality associated with an increase in malaria DAH per capita by one US dollar. The fixed effects model implies that the relationship is estimated using within-country, within-time variations in DAH and governance. The same model was used to assess the effect of individual governance indicators. The dependent variables for the models were malaria DALYs, deaths, prevalence, and incidence in period t, and the independent variables included DAH and governance. Due to missing governance data from 1990 to 2000 and for 2018 and 2019, the fixed effects analysis captured changes over 18 years, that is, from 2000 to 2017. All analyses were carried out using SAS version 9.4.
Results
Trends in SSA and subregions
The DALYs, deaths, incidents, and prevalent case rates all decreased for the SSA region and all its sub-regions. shows that in SSA, the ASDR decreased to 3339.41 (95% UI: 1647.34–5959.92) in 2019, dropping by 47% from 6264.88 (95% UI: 3148.77–10611.33) in 1990. The ASMR decreased by 38% (95% UI: −65% – 3%), the ASIR decreased by 35% (95% UI: −44% – −25%), and the ASPR decreased by 34% (95% UI: −43 – −24%). It is notable that SSSA has had the lowest burden of disease among all subregions since 1990. In 1990, all measures were highest in WSSA, but even with a low percentage change, the age-standardised rates were close to those of CSSA, i.e. in 2019, the ASDR and ASMR were still higher in WSSA than in other regions at 5204.34 (95% UI: 2529.28–9325.86) and 104.53 (95% UI: 47.28–196.51) respectively. However, the ASPR and ASIR were higher in CSSA than in other regions, at 21557.65 (95% UI: 16639.4–27027.89) and 19883.01 (95% UI: 16010.45–27027.89), respectively. In 2019, the ASMR in CSSA, ESSA, and SSSA was all below the SSA regional average, which was about 60.73(27.4–113.49), but was higher in WSSA, where it was 104.53 (95% UI: 47.28–196.51).
Table 1. Changes in the Malaria burden in Sub-Saharan African regions (1990–2019).
The percentage changes among the subregions all indicated reductions but differed significantly. shows the Joinpoint regression analysis for the ASMR. The varied results show that SSA’s burden decreased the most from 2009 to 2015, with a −6.31% APC. However, there have been continuous reductions since 2003. Considerable trends were seen among subregions, although, in contrast to the regional trend, WSSA’s burden continued to increase past 2007, with later significant reductions between 2011 and 2017 with a 6.031% APC. A unique trend was seen in SSSA, where continued increases from 1990 to 2004 were followed by a rapid decline until 2019, with an 8.69% APC.
Notable country-specific trends
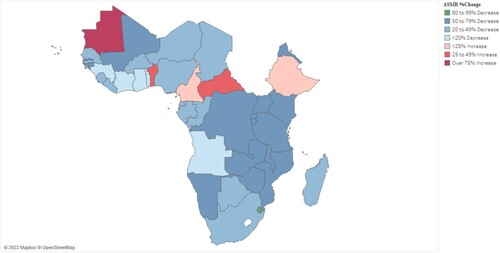
Country-specific differences among subregions were observed, with annual percentage changes ranging from decreases of up to 91% (95% UI: −100% – 11%) in eSwatini to increases surpassing 100% in Mauritania and Cabo Verde, where the ASMR percentage increases were 61060% (95% UI: 0% – 802964%) and 455% (95% UI: −21% – 3712%), respectively. shows that the countries with increases were found in various regions, regardless of the subregional decreases, and Supplementary Table 1 shows country-specific differences in percentage changes, even in similar regions.
Figure 2. Percentage change in age-standardised mortality rates in 42 Sub-Saharan African countries.
Trend by age (the high burden among children under five years)
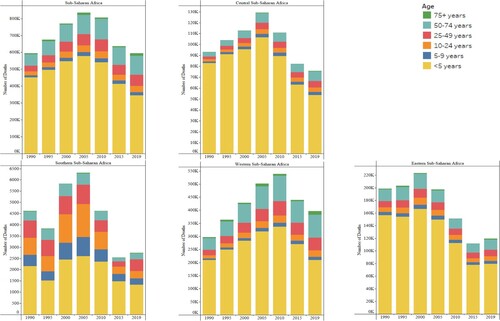
indicates that among all subregions, malaria deaths among children under five have remained high across all subregions, accounting for over 50% of the burden in all regions apart from SSSA. These were followed by a wider age range of 50–74 in all other subregions apart from SSSA. In SSSA, there was a different age composition for malaria deaths, even though the numbers remained lower than those in all other subregions.
Figure 3. Thirty-year distribution of malaria mortality by age in Sub-Saharan Africa.
Effect of DAH and governance on malaria burden
There was an average increase in DAH per capita from 0.13 in 2000 to 2.09 in 2017 for all 42 of the studied countries. The effect of this increase among the countries during the 18 years was analyzed. When controlled for GDP and population, both DAH per capita and aggregate governance showed a negative relationship with all the measures of malaria burden. Notable results include the finding that an increase in per capita DAH by one US dollar was likely to cause a decrease in the ASDR by 134.29 (standard error (SE) = 27.26) and a decrease in the ASMR of 1.84 (p = 0.0002). Improvement in governance, accounted for by an increase in summed governance indicator values by 1, was associated with a subsequent −246.19 (SE = 39.13) change in the ASDR and a decrease in the ASMR of 4.99 (SE = 0.7). Significant, associated decreases in incidence and prevalence rates were seen when the DAH per capita increased ().
Table 2. Country and time-period effects regression analysis of malaria burden measures, DAH, and governance with control variables 2000–2017.
When individual governance indicators were analyzed, like aggregate governance, all the indicators were associated with decreases in the ASDR and ASMR, but apart from voice and accountability, no other indicators were significantly associated with prevalence and incidence. In , model 1 is an unadjusted analysis, and model 2 is an analysis adjusted with controls including the per capita DAH, per capita GDP, and population. Even when adjusted, there was little or no change in the association. Notably, an increase in scores of political stability and the absence of war showed a decrease in DALYs of −695.08 (SE = 105.7, p < 0.0001) when unadjusted, and was close to a −689.05 decrease (SE = 104.0, p < 0.0001) when adjusted.
Table 3. Country and time-period effects regression analysis of malaria burden measures and six governance indicators 2000–2017.
Discussion
This study examined the trend in malaria in 42 countries for 30 years, covering all four sub-regions in SSA. It also established how governance and its six indicators affected changes in the burden, and the findings were consistent with previous studies (Hsiao & Emdin, Citation2015; O’Meara et al., Citation2010). Our findings extend the proof that the burden of malaria in SSA has decreased, and DAH is part of the reason. However, we also identified a new reason, the effect of governance. The burden was found to be lowest in SSSA, with both WSSA and CSSA posting significant reductions in the burden of malaria. But the burden in the two subregions remains bigger than elsewhere in the region (O’Meara et al., Citation2010; World Health Organization, Citation2021). This is consistent with existing literature indicating a lower burden in countries in southern regions and a high burden still existing in Nigeria, Burkina Faso, and Sierra Leone, all of which are in WSSA. Yet CSSA’s Democratic Republic of Congo is one of the world’s highest malaria-burdened countries (World Health Organization, Citation2020).
The downward trend showed variations in regions, but with clear indications of larger drops in all areas from 2004 to 2015, the trend however isn’t isolated as DAH was also low until 2002 and is seen to have taken an upward turn from 2003 (Hsiao & Emdin, Citation2015). This could explain the higher rate of decline. The burden of DALYs and deaths has majorly dropped, but the high age-standardised rates for incidence and prevalence have decreased at a slower rate. While the continued prevalence of P. Falciparum positivity in rural areas associated with poverty was noted by De Beaudrap et al. (Citation2011), it was contested by Froeschl et al. (Citation2018), whose findings indicated great reductions in the positivity rate when areas conducted artemisinin-based combination therapy as the first-line treatment, which has been a common policy in malaria-endemic countries since 2004 (De Beaudrap et al., Citation2011; Froeschl et al., Citation2018). Countries with significant reductions in malaria, like Eswatini, have been hailed by the WHO, noting that the country may be malaria-free by 2025 (World Health Organization Eswatini, Citation2023). The reductions have been linked to widespread indoor residual spraying, mosquito nets, and specifically, in Eswatini’s case, to their telephone reporting system, which has increased surveillance for malaria in the country (Gates, Citation2018).
Despite the reduction, a sizeable portion of the burden of malaria affects children under the age of five. In our analysis, in SSA, only SSSA had less than 50% of the number of deaths accounted for in children under five, a consistent fact, yet it is true that the burden is similarly declining in all regions (World Health Organization, Citation2021). However, we found that the mortality rate among elders over 75 years was also high and increasing, an important finding considering the usual focus on younger populations in the studied countries (Carneiro et al., Citation2010). Thus, more studies aimed at understanding the prevalence of malaria in endemic countries are recommended, as the finding was similar to that of Jenkins et al. (Citation2015) where in endemic areas, even with high transmission and mortality among children, adults were also at high risk.(Jenkins et al., Citation2015).
It is also notable that the distribution of endemic countries was diverse. Thus, our findings reinforce the need to intervene in malaria with the recognition that countries in similar regions could have different malaria burdens. Another finding was that highly endemic countries recorded reductions in the malaria burden over the 30 years of the study. Some countries with a lower burden than the regional average have experienced increases in the burden during the same period, and there has been a common concern regarding increases in all measures of malaria burden since 2015 in some countries (World Health Organization, Citation2020).
To address these variances, understanding the effect of DAH and governance was important, and thus, we carried out an analysis to understand the effect of these two factors on the variance in country-specific trends. Our results are consistent with previous literature. DAH increases were associated with decreases in malaria burden (Hsiao & Emdin, Citation2015). The funds, which are known to contribute over 60% of the malaria intervention expenditures, have direct and indirect effects on the recipient societies. DAH is known to have an effect on reducing the incidence, curbing deaths, financing research and development, and improving livelihoods (Kavanagh & Chen, Citation2019). Much of the DAH is disbursed by both governments and private entities through the global fund, whose role has been critically appraised. Sarpong and Bein (Citation2021) found that among low and middle-income countries, the recipients of global funds have not benefitted similarly with countries who have other sources of income (in their case, oil-producing countries) and, thus, are in a better position to benefit from the global fund (Sarpong & Bein, Citation2021). They cited the fact that funds could be more easily misappropriated in non-oil-producing countries due to shortages in other areas and a lack of adequate structures.
Governance has been noted not only to play a role in ensuring that the received funds are put to use but also to create systems and structures enabling the eradication of disease and financing disease eradication programs in the recipient countries. Easterly (Citation2009) noted that governments usually receive aid for a problem and transfer the money they would have spent on that program to another possible other usually bad cause Thus, aid is usually used to finance causes other than its aim (Easterly, Citation2009). All interventions are led by policies. Therefore, governments without the will to follow WHO guidelines or those at war without the capacity to enact policies are at a high risk of having no set guidelines, which could lead to lower performance in the eradication of malaria. Good governance is also known to attract additional investments and resilience, enabling governments to supplement the DAH with their budgets and increase surveillance, providing a chance to lower the malaria burden (Acht et al., Citation2015).
Our findings emphasize the association between corruption and the lack of accountability and disease burden. The global fund has previously been marred by corruption, in some countries amounting to over 67% of the disbursement (CBS News, Citation2011). These countries, including Zambia, Mali, Uganda, and others, unsurprisingly, still suffer a high burden, yet the embezzled funds usually end up serving the intentions of individuals. In other countries, drugs have been stolen directly from shipments for resale (Bate, Citation2011; Steurs, Citation2019). The global fund has allocated funds according to the burden of disease rather than on the basis of the quality of the governance, yet some countries state that the global fund has enforced strings attached (Radelet, Citation2004; Taylor & Harper, Citation2014). This allocation gives countries with a high burden more allocations, yet some of them continue to mismanage the funds, causing a slower reduction in the burden compared to other countries.
Countries at war and politically unstable are more likely to have dysfunctional health systems. Thus, the finding that political stability contributes to a reduced burden is justified. Our findings indicated that countries like Liberia, with a civil war that started in 1990 and lasted until 1997, and Sierra Leone, from 1991 to 2002 (Fang et al., Citation2020), experienced increases in the ASDR due to malaria during the study period. Liberia’s ASMR increased from 163.95 (95% UI: 63.26-308.55) Connolly and David (Citation2002), also emphasized the high incidence of malaria among displaced populations, a phenomenon proven by the mass of people that flock to borders, the lack of shelter and basic sanitation, and usually being placed in camps surrounded by forests in which mosquitoes can breed. Most of these do not have access to treatment or insecticide-treated nets. They also suggest the provision of antimalarials and bed nets for malaria-endemic regions at war (Connolly & Heymann, Citation2002).
Although this study provides a comprehensive view of malaria trends in SSA and its possible contributing factors, there remain limitations. These include the concerns in earlier studies about the quality of primary data in the GBD study, considering the reporting systems in low-income countries (He et al., Citation2021). Another limitation was that an association between malaria burden indicators and governance and DAH could not be assumed as the sole explanation for the malaria trends (Blanchet et al., Citation2017). The study also investigated malaria trends until 2019 which doesn’t cover years during the coronavirus pandemic. The world malaria report 2021 has reported increases in cases of malaria from 218 million in 2019–234 million cases in 2021in the African region. The report also highlighted a significant increase in deaths from 544,000 in 2019–593,000 in 2021. The report owes these increases to an increase in case incidence rate per 1,000 population which also increased from 225.5 in 2019–229.4 in 2021 due to service disruptions caused by the coronavirus pandemic (World Health Organization, Citation2022b).
Our findings maintain a decline in the burden of malaria in SSA. We also noted differences in subregional burden, specifically, the lower burden of disease in countries in the southern sub-region. However, the rate of burden remains high in other subregions, especially the WSSA. The rate of change in mortality rates was slower in some areas but has increased in some countries. The findings also emphasize the need for DAH increases to enable malaria eradication. However, they also advocate for better governance because if malaria is to be eradicated, there is a need for additional funding to reach projected needs, but the funds will accomplish less if they are not combined with improved governance, including minimising corruption, peace, the absence of war, and more accountability among other improved governance indicators. SSA’s malaria deaths and DALYs were decreased when funding and governance improved, but incidence and prevalence were not dependent on improved governance, indicating that other factors were responsible for the reductions, even though the overall APC in prevalence and incidence was lower than that of DALYs and deaths.
In conclusion, the burden of malaria in SSA has been on a downward trend over the last 30 years. Although some countries registered increases in the period, increases in DAH and improved governance were factors contributing to the decrease. However, they were not significantly associated with the downward trend in prevalence and incidence. We recommend further research to identify other factors that can contribute to further decreasing malaria burden and the effect of the disruptions caused by the coronavirus pandemic on the burden.
Availability of data and materials
The data used in this study are freely available from different websites listed below.
Global Burden of Disease Data at https://vizhub.healthdata.org/gbd-results.
Development Assistance for Health at https://ghdx.healthdata.org/.
World Bank Governance Indicators at https://info.worldbank.org/governance/wgi/Home/Reports.
Population data at population.un.org/wup.
Gross domestic product data at https://data.un.org/.
Supplemental Material
Download MS Word (52.3 KB)Acknowledgements
J.K.S. and Y.H.L. conceptualised and designed the study. Data were acquired by J.K.S.; analyzed by J.K.S., M.C., and E.H.L.; and interpreted by all the authors. J.K.S., M.C., and E.H.L wrote the first draft which was supervised and revised by Y.H.L. The final draft was revised and approved by all the authors. Ethical approval for this type of study is not required by our institute.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Acht, M., Mahmoud, T. O., & Thiele, R. (2015). Corrupt governments do not receive more state-to-state aid: Governance and the delivery of foreign aid through non-state actors. Journal of Development Economics, 114, 20–33. https://doi.org/10.1016/j.jdeveco.2014.11.005
- Bate, R. (2011). Partners in crime: National theft of global fund medicines. Africa Fighting Malaria Briefing Paper.
- Blanchet, K., Nam, S. L., Ramalingam, B., & Pozo-Martin, F. (2017). Governance and capacity to manage resilience of health systems: Towards a new conceptual framework. International Journal of Health Policy and Management, 6(8), 431. https://doi.org/10.15171/ijhpm.2017.36
- Carneiro, I., Roca-Feltrer, A., Griffin, J. T., Smith, L., Tanner, M., Schellenberg, J. A., & Schellenberg, D. (2010). Age-patterns of malaria vary with severity, transmission intensity and seasonality in sub-Saharan Africa: A systematic review and pooled analysis. PLoS One, 5(2), e8988. https://doi.org/10.1371/journal.pone.0008988
- CBS News. (2011). Ap: Fraud plagues global health fund. CBS News. https://www.cbsnews.com/news/ap-fraud-plagues-global-health-fund/.
- Connolly, M. A., & Heymann, D. L. (2002). Deadly comrades: War and infectious diseases. The Lancet, 360, 23–424. https://doi.org/10.1016/S0140-6736(02)11807-1
- De Beaudrap, P., Nabasumba, C., Grandesso, F., Turyakira, E., Schramm, B., Boum, Y., & Etard, J.-F. (2011). Heterogeneous decrease in malaria prevalence in children over a six-year period in south-western Uganda. Malaria Journal, 10(1), 1–9. https://doi.org/10.1186/1475-2875-10-132
- Dragomirescu, I., Llorca, J., Gómez-Acebo, I., & Dierssen-Sotos, T. (2019). A join point regression analysis of trends in mortality due to osteoporosis in Spain. Scientific Reports, 9(1), 1–8. https://doi.org/10.1038/s41598-019-40806-0
- Easterly, W. (2009). Can the west save Africa? Journal of Economic Literature, 47(2), 373–447. https://doi.org/10.1257/jel.47.2.373
- Fang, X., Kothari, S., McLoughlin, C., & Yenice, M. (2020). The economic consequences of conflict in Sub-Saharan Africa.
- Froeschl, G., Saathoff, E., Kroidl, I., Berens-Riha, N., Clowes, P., Maboko, L., & Ntinginya, E. N. (2018). Reduction of malaria prevalence after introduction of artemisinin-combination-therapy in Mbeya Region, Tanzania: Results from a cohort study with 6773 participants. Malaria Journal, 17(1), 1–11. https://doi.org/10.1186/s12936-017-2149-5
- Gates, B. (2018). Could this be the first country in sub-Saharan Africa to defeat malaria? Swaziland’s success fighting malaria can teach the world valuable lessons. Retrieved May 15, 2023 from https://www.gatesnotes.com/Buzz-Kill.
- He, J., Ouyang, F., Qiu, D., Li, L., Li, Y., & Xiao, S. (2021). Time trends and predictions of suicide mortality for people aged 70 years and over from 1990 to 2030 based on the global burden of disease study 2017. Frontiers in Psychiatry, 12. https://doi.org/10.3389/fpsyt.2021.721343
- Hsiao, A. J., & Emdin, C. A. (2015). The association between development assistance for health and malaria, HIV and tuberculosis mortality: A cross-national analysis. Journal of Epidemiology and Global Health, 5(1), 41–48. https://doi.org/10.1016/j.jegh.2014.10.001
- Institute for Health Metrics and Evaluation (IHME). (2020). Development assistance for health database 1990–2019. United States of America.
- Jenkins, R., Omollo, R., Ongecha, M., Sifuna, P., Othieno, C., Ongeri, L., & Ogutu, B. (2015). Prevalence of malaria parasites in adults and its determinants in malaria endemic area of Kisumu County, Kenya. Malaria Journal, 14(1), 1–6. https://doi.org/10.1186/s12936-015-0781-5
- Kasim, H. A. (2019). State effectiveness and political will: The case of malaria control in Uganda and Rwanda. Carleton University.
- Kaufmann, D., Kraay, A., & Mastruzzi, M. (2009). Governance matters VIII: Aggregate and individual governance indicators, 1996–2008. World bank policy research working paper (4978).
- Kaufmann, D., Kraay, A., & Mastruzzi, M. (2011). The worldwide governance indicators: Methodology and analytical issues. Hague Journal on the Rule of Law, 3(2), 220–246. https://doi.org/10.1017/S1876404511200046
- Kavanagh, M. M., & Chen, L. (2019). Governance and health aid from the Global Fund: Effects beyond fighting disease. Annals of Global Health, 85(1), 69. https://doi.org/10.5334/aogh.2505
- Micah, A. E., Su, Y., Bachmeier, S. D., Chapin, A., Cogswell, I. E., Crosby, S. W., & Moitra, M. (2020). Health sector spending and spending on HIV/AIDS, tuberculosis, and malaria, and development assistance for health: Progress towards sustainable development goal. The Lancet, 396(10252), 693–724. https://doi.org/10.1016/S0140-6736(20)30608-5
- Moyo, D. (2009). Why foreign aid is hurting Africa. The Wall Street Journal, 21, 1–2.
- Murray, C. J., Ortblad, K. F., Guinovart, C., Lim, S. S., Wolock, T. M., Roberts, D. A., & Brown, J. C. (2014). Global, regional, and national incidence and mortality for HIV, tuberculosis, and malaria during 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. The Lancet, 384(9947), 1005–1070. https://doi.org/10.1016/S0140-6736(14)60844-8
- Ohiri, K., Aniebo, I., & Akinlade, O. (2022). Rethinking malaria: Governance lessons from other disease programs. PLoS Global Public Health, 2(9), e0000966. https://doi.org/10.1371/journal.pgph.0000966
- O'Meara, W. P., Mangeni, J. N., Steketee, R., & Greenwood, B. (2010). Changes in the burden of malaria in sub-Saharan Africa. The Lancet Infectious Diseases, 10(8), 545–555. https://doi.org/10.1016/S1473-3099(10)70096-7
- Palagyi, A., Marais, B. J., Abimbola, S., Topp, S. M., McBryde, E. S., & Negin, J. (2019). Health system preparedness for emerging infectious diseases: A synthesis of the literature. Global Public Health, 14(12), 1847–1868. https://doi.org/10.1080/17441692.2019.1614645
- Park, H. J., Kim, U. J., Lee, W. k., Park, B., Shin, Y., Lee, S., & Park, H. (2021). Joinpoint regression about injury mortality and hospitalization in Korea. Journal of Korean Medical Science, 37(3), e10–e10. https://doi.org/10.3346/jkms.2022.37.e10
- Qiu, D., Katanoda, K., Marugame, T., & Sobue, T. (2009). A Joinpoint regression analysis of long-term trends in cancer mortality in Japan (1958–2004). International Journal of Cancer, 124(2), 443–448. https://doi.org/10.1002/ijc.23911
- Radelet, S. (2004). The global fund to fight AIDS, tuberculosis and malaria: Progress, potential, and challenges for the future. Center for Global Development.
- Rannan-Eliya, R. P. (2022). Financing malaria. PLoS Global Public Health, 2(6), e0000609.
- Sarpong, S. Y., & Bein, M. A. (2021). Global fund and good governance in sub-Saharan Africa: Accounting for incidence of malaria and quality of life in oil and non-oil producing countries. SN Social Sciences, 1(8), 1–32. https://doi.org/10.1007/s43545-021-00213-7
- Sharma, R., Abbasi-Kangevari, M., Abd-Rabu, R., Abidi, H., Abu-Gharbieh, E., Acuna, J. M., & Meybodi, M. A. (2022). Global, regional, and national burden of colorectal cancer and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019, 627-647. The Lancet Gastroenterology & Hepatology. https://doi.org/10.1016/S2468-1253(22)00044-9
- Steurs, L. (2019). European aid and health system strengthening: An analysis of donor approaches in the DRC, Ethiopia, Uganda, Mozambique and the global fund. Global Health Action, 12(1), 1614371. https://doi.org/10.1080/16549716.2019.1614371
- Taylor, E. M., & Harper, I. (2014). The politics and anti-politics of the global fund experiment: Understanding partnership and bureaucratic expansion in Uganda. Medical Anthropology, 33(3), 206–222. https://doi.org/10.1080/01459740.2013.796941
- United Nations, D. o. E. a. S. A., Population Division. (2018). World urbanization prospects: The 2018 revision, online edition. https://population.un.org/wup/Download/Files/WUP2018-F18-Total_Population_Annual.xls.
- United Nations Statistics Division. (2019). Per capita GDP at current prices US dollars.
- Vos, T., Lim, S. S., Abbafati, C., Abbas, K. M., Abbasi, M., Abbasifard, M., & Abdelalim, A. (2020). Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. The Lancet, 396(10258), 1204–1222. https://doi.org/10.1016/S0140-6736(20)30925-9
- World Health Organization. (2010). The Abuja declaration: Ten years on.
- World Health Organization. (2020). World malaria report 2020: 20 years of global progress and challenges.
- World Health Organization. (2021). World malaria report 2021. (9240040498).
- World Health Organization. (2022a). Malaria fact sheet. Retrieved June 26, 2022 from https://www.who.int/news-room/fact-sheets/detail/.
- World Health Organization. (2022b). World malaria report 2022. Geneva: World Health Organization.
- World Health Organization Eswatini. (2023). WHO 75th anniversary: Eswatini commits to the who agenda of improving health for the people of Eswatini. Retrieved May 16, 2023. https://www.afro.who.int/countries/eswatini/news/who-75th-anniversary-eswatini-commits-who-agenda-improving-health-people-eswatini.