
ABSTRACT
Prevention capacity of local health organisations is associated with the performance and outcomes in public health. In Colombia, where cardiovascular disease is the leading cause of morbidity and mortality, there is limited knowledge about the capacity of local health departments to prevent this condition. Efforts are needed to address problems, potential solutions and expected outcomes regarding cardiovascular disease. In this study, a conceptual model for cardiovascular disease prevention capacity in Colombian local health departments was developed, a questionnaire based on this model was validated, the overall cardiovascular disease prevention capacity in a subsample of these organisations was measured, and the association between cardiovascular disease prevention capacity and political, population, and organisational factors was examined. Once the acceptable performance of the questionnaire was verified, variability in cardiovascular prevention capacity was found among a subsample of local health departments. Furthermore, this study provides primary evidence regarding the association between the size of local health departments and overall cardiovascular disease prevention capacity in Colombia. Future studies should focus on measuring this capacity on a larger scale and developing, implementing, and evaluating interventions aimed at strengthening cardiovascular prevention capacity in Colombian local jurisdictions.
Introduction
Cardiovascular disease (CVD) is the leading cause of morbidity and mortality in Colombia (Dirección de Epidemiología y Demografía. Ministerio de Salud y Protección Social, Citation2021; Instituto Nacional de Salud, Citation2013). From 2005 to 2011 the age-adjusted mortality rates for CVD decreased from 166.42 to 146.16 deaths per 100,000 inhabitants. After a short stabilisation between 2011 and 2013, it increased until 2018 reaching 152.42 deaths for 100,000 inhabitants. For 2019, the mortality rate of CVD was 132.22 per 100,000 inhabitants. In that year, it represented 31.03% (75,826) of total deaths and 18.1% years of potential life lost (YPLL) (Dirección de Epidemiología y Demografía. Ministerio de Salud y Protección Social, Citation2021).
Although in Colombia the mortality for CVD is mainly concentrated in the most urbanised and economically developed areas of the country (Dirección de Epidemiología y Demografía. Ministerio de Salud y Protección Social, Citation2021), geographic, social and economic disparities in the main risk factors, morbidity and mortality for CVD have been reported (Camacho et al., Citation2016; Lucumi et al., Citation2017; Meisel et al., Citation2020; Pérez-Flórez & Achcar, Citation2021; Universidad Nacional de Colombia et al., Citation2017). For instance, in children and adults, the prevalence of excess body weight in two different peripheral departments (known as provinces in other countries) was almost 15 percentage points higher than the national estimation that was 24.40% in children 5–12 years old and 56,00% in adults 18–64 years old (Universidad Nacional de Colombia et al., Citation2017). Disparities between departments have also been reported for hypertension (García-Peña et al., Citation2022; Lucumi et al., Citation2017), being an estimated prevalence of 24.00% (95% CI: 19.00–29.00%) (Zurique-Sánchez et al., Citation2019). This epidemiological evidence suggests that CVD is and will continue to be one of the most challenging public health problems in Colombia, and there is room for improvement in the prevention of this condition in the country as a whole and in its administrative divisions.
To achieve higher standards of CVD prevention in Colombia, more attention needs to be given to the role of local jurisdictions, since this is the context where people are exposed to conditions that increase or protect against CVD at the population level (Homer et al., Citation2008; Lucumi et al., Citation2016). Among contextual conditions, the health system is an important intermediate determinant of health and CVD (Hanusaik et al., Citation2007; Solar & Irwin, Citation2010). The critical role played by local health organisations in promoting health and preventing diseases has been emphasised since the 1970s mainly in high-income countries (HIC) (Erwin et al., Citation2011, Citation2012; Ransom et al., Citation2012; Schenck et al., Citation2015). Local health departments (LHD) are expected to have the knowledge of the population they serve and a close relationship with other agencies and organisations involved in addressing health issues at the local level. However, in countries like Colombia, the contribution of LHD to CVD prevention could vary between organisations because the social, political and economic heterogeneity of administrative divisions, the differences in the living conditions experienced by their populations, and the way LHD respond to prevention challenges.
Colombia is a decentralised unitary republic divided administratively into 32 departments and 1102 and municipalities (12 of them are districts). Although public health in Colombia involves numerous public and private stakeholders at different levels of the political division, the major providers are governments. Under this structure, LHD located in each administrative division are instrumental parts of the health system. They serve populations ranging from 8,000,000 to 1000 inhabitants and most of them rely on a significant proportion of funding from the national government. Although the functions of LHD vary according to competencies based on the type of administrative division and the categories in which the Colombian General Accounting Office (GAO) classifies these divisions each year, LHD are territorial health authorities, have resources and competencies for doing CVD prevention that effectively contributes to reducing the burden of this chronic condition, and participate in a variety of policy activities for improving healthy environments and are responsible of diverse health promotion and disease prevention interventions. Besides, Colombian LHD play a central role in providing population-based services, including to analyse and monitor health status, investigate health hazards, educate people about public health issues, mobilise community partnerships, build intersectoral alliances, and enforce laws and regulations.
Many factors explain the gap between the effective prevention of CVD and the improvement of outcomes at the local level. Among these factors, prevention capacity (Flaspohler et al., Citation2008), a construct with an elusive definition (Meyer et al., Citation2012), has been highlighted. Despite the lack of consensus regarding the definition of prevention capacity, it relates to motivations, knowledge, skills and resources that allow carrying out stated objectives. Likewise, prevention capacity is a multidimensional and multilevel construct (Flaspohler et al., Citation2008; Goodman et al., Citation1998). Regarding the first, it needs to be measured and modified through various dimensions and mechanisms. And, it is multilevel because it is observed at the individual, organisational, community and system levels (Flaspohler et al., Citation2008; Goodman et al., Citation1998; Mays & Smith, Citation2011). All these characteristics make it difficult to develop a satisfactory and unified analytical approach and unique tools to measure capacity in a variety of contexts. However, previous literature has noted that assessing the capacity of local health organisations is a first step in efforts to improve it (LaFond et al., Citation2002).
Prevention capacity is a prerequisite for achieving appropriate performance in public health and for effectively preventing diseases, especially in contexts with a high and unequal prevalence of health problems (Homer et al., Citation2008; Meyer et al., Citation2012). Also, capacity contributes to the health assessment in each jurisdiction and the planning, development, implementation, monitoring and evaluation of public health interventions (Meyer et al., Citation2012). Qualitative and quantitative evidence from HIC suggests that the prevention capacity of local health organisations is associated with performance and different health outcomes (Ransom et al., Citation2012; Schenck et al., Citation2015), including CVD and other chronic conditions (Erwin et al., Citation2011; Hanusaik et al., Citation2015; Mays & Smith, Citation2011; Riley et al., Citation2003). For example, research on resources, one dimension of capacity widely studied, has found that increased staffing was significantly associated with decreases in CVD mortality (Erwin et al., Citation2011). Similarly, increases in public health spending were associated with statistically significant reductions in the same outcome (Mays & Smith, Citation2011).
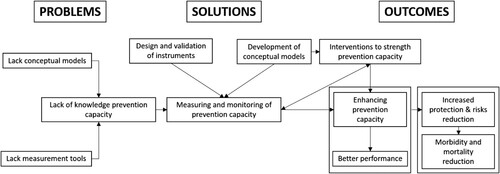
As depicted in , in Colombia, the knowledge on the capacity of LHD for the prevention of CVD is almost absent, and are needed efforts to address problems, potential solutions and expected outcomes regarding this capacity. This lack of knowledge includes data about different domains or dimensions of capacity, such as staffing, infrastructure, or leadership of LHD. To expand knowledge in this field outside of HIC, this study was aimed at: (1) developing a conceptual model for CVD prevention capacity in Colombian LHD, (2) validating a questionnaire built on this model, (3) measuring the dimensions and overall CVD prevention capacity in a sample of LHD and (4) examining the association between CVD prevention capacity and political, population, and organisational factors.
Figure 1. Problems, potential solutions and expected outcomes regarding the cardiovascular disease prevention capacity in Colombia.
Methods
The three phases of this study were carried out between June 2017 and June 2021. In the first phase, we developed the conceptual model that informed the design of a CVD prevention capacity questionnaire. In the second phase, we validated this questionnaire. In the final phase, we applied this questionnaire to a nonrandomised subsample of Colombian LHD to measure their CVD prevention capacity and examine associated factors. This study was part of a project reviewed and approved by the Universidad de los Andes’ IRB in 2016 (Act 676 and Act 680).
Development of the conceptual model and questionnaire
We conducted a narrative review using PubMed, Google Scholar and grey literature to identify published papers or documents proposing conceptual models for prevention capacity in public health and specific constructs used for the conceptualisation, measurement and intervention of CVD or for developing prevention capacity of chronic diseases in health organisations. For this search we used terms such as chronic disease; prevention; cardiovascular disease; capacity; performance, conceptual framework, conceptual model. We identified 20 papers and grey documents that matched with the aim of this review. From these documents we extracted dimensions or dimensions and, where possible, their definitions.
In addition, we searched for questionnaires developed in the United States, Australia and Canada for measuring prevention capacity at the local level. These countries were chosen because of their recognised experience in this field. Through an iterative process, the research team selected and adapted a definition for each dimension of prevention capacity that would be suitable for the Colombian context. After several rounds among the research team, a final version of the questionnaire in Spanish was developed.
Validation of the questionnaire
For face validity, we convened a multidisciplinary meeting with ten experts from academia and public health organisations working at the national or local level in the prevention of CVD. We asked them to read the questions and evaluate if they: (1) contributed to covering the definition of their corresponding dimension, (2) served their intended purpose and (3) had clear wording. We also asked experts to identify any problem of the questionnaire from a theoretical or measurement perspective. We took note of all experts’ comments for further review and adjusted the final version of the questionnaire accordingly.
For the construct, content and criterion validation of the questionnaire, we used a convenience sampling strategy based on two criteria to select 30 administrative units. Firstly, we chose Bogotá, the country’s capital city, where the research team was located, and where most prevention capacity was expected. We also selected administrative units located primarily in the vicinity of Bogotá. Secondly, we aimed to include administrative units from different GAO categories. These categories are based primarily on the fiscal resources of the administrative units and secondarily on their population size. Using this classification, our sample included three departments and Bogotá. Additionally, we selected 26 municipalities distributed as follows: (a) three municipalities from the 1st GAO category, including two that were department capitals, which, along with the special GAO category, grouped together the municipalities with the highest fiscal resources; (b) two municipalities from each GAO categories from the 2nd to the 4th, for a total of six; (c) five municipalities from the 5th GAO category; and (d) twelve municipalities, including a department capital, from the 6th GAO category. This last category comprises those municipalities with the lowest fiscal resources and covers 89% of Colombian local jurisdictions.
Directors of LHD or the person with direct responsibility for the prevention of CVD in each jurisdiction (e.g. public health coordinator or leader of the non-communicable prevention team) were invited to participate in the study by email or phone, as they were supposed to have the authority and knowledge to answer the entire questionnaire. One member of the research team visited in person each of the 30 health departments to get the participants’ signature of the informed consent form and administer the questionnaire. In some municipalities, mainly in those ranked in the 6th GAO category, we found that the role of the health departments was played by planning or social services office, or these were transferred to the local hospital. Regardless of this circumstance, in each case, we interviewed the person or team that was considered more knowledgeable about the prevention of CVD in the jurisdiction. In all cases, we completed only a questionnaire for each jurisdiction, and discrepancies in the answers among participants were solved during the interviews. In the very few occasions discrepancies persisted, we used the information from the source more directly involved in the prevention of CVD in the municipality.
We conducted statistical analysis that included factor and reliability analysis and assessment of convergent and divergent validity. The factor analysis aimed to reduce the dimensionality of the data to identify homogenous groups of variables that explain the biggest proportion in the multidimensional space. Additionally, this analysis allowed us to establish the correspondence between the theoretical and the empirical multidimensionality (Burga, Citation2006; Lloret-Segura et al., Citation2014). We used principal component analysis, to examine whether eigenvalues were higher than 1, and we retained factors that explained at least 40% of the variance. For the reliability analysis, we calculated Cronbach alpha for each of the factors we extracted in the previous step. This analysis also helped to estimate the magnitude of the association between items. We considered good reliability with Cronbach’s alpha > 0.6.
For construct validity, we conducted both convergent and a divergent analysis. The goal of the convergent validity was to assess whether the items had good correlation with the scores of the subdimension they belonged. Conversely, divergent validity sought to assess if the items were not correlated or had a negative correlation with the scores of the subdimensions to which they did not belong. For these analyses, we estimated Pearson’s correlation coefficients. Coefficients equal or higher than 0.4 were expected in the convergent analysis, whereas lower values were expected in the divergent one (Perrot et al., Citation2018). Finally, due to the lack of a gold standard, for the criterion validity, we followed the procedure of a previous study and estimated the correlation between the total score questionnaire and the score obtained for each dimension (Dunet & Butterfoss, Citation2005).
Measurement of the overall CVD capacity and its associated factors
After validating of the questionnaire, to measure CVD prevention capacity, we purposively selected a new sample of municipalities. These municipalities were chosen from two Colombian departments, one in the West and other in the Mideast. These departments exhibited heterogeneity in terms of some social and economic characteristics of their municipalities. Based on the economic resources available for the project, we planned to collect information from all municipalities in one department (n = 42) and 50% of the 123 municipalities in the other (n = 62).
Using the information provided by the non-communicable diseases team in each department, we created a dataset containing information about the officials responsible for CVD prevention in the selected municipalities. This dataset was utilised by trained interviewers from an external survey company to contact each official to schedule an appointment for administering the questionnaire, either by phone or through a digital platform.
Overall CVD prevention was calculated as the mean of the scores obtained for each municipality using the 88 items that remained after validation. Similarly, the scores of each dimension and subdimension were calculated using the items that remained after validation.
Based on the conceptual and empirical literature that identified explanatory indicators of capacity and performance of LHD (Bhandari et al., Citation2010; Erwin, Citation2008; Schenck et al., Citation2015), as well as the small sample size available for measuring the overall CVD capacity of this study, we selected one indicator from each structural factor of the conceptual model to estimate its association with overall CVD prevention capacity. The political indicator was the financial resources allocated to public health in each municipality in 2020 (divided into three quantiles of the most recent fiscal year before the survey, taken from the report Colombian municipalities must provide to the GAO). For population factors, we chose the population size in 2021 (logarithmic transformation of the information obtained from the National Department of Statistics). Finally, for organisational factors we included the self-reported number LHD employees in 2021. The allocation of resources to public health was categorised into three quantiles because to address its skewness and reduce uncertainty. For the same reasons, we applied a logarithmic transformation to population size.
Before running univariate and multivariate generalised estimation equation (GEE) models, we obtained descriptive statistics for overall CVD prevention capacity, its dimensions, and subdimensions. We employed GEE models to address potential correlations among observational units, which violate independence assumptions made by traditional regression procedures. This violation is particularly relevant to estimates of the variability of estimates. In this regard, the GEE approach does not require distributional assumptions (Hubbard et al., Citation2010). After running univariable models, in the first multivariable models we included the selected variable for each structural factor one at a time and adjusted for the category of the municipality (1–6), department (West or Mideast) and percentage of urban population in each municipality. Then, we ran a full model in which we included structural and adjustment variables simultaneously. We examined collinearity without finding statistical evidence of it. Given the conceptualisation and specific information provided by the three structural indicators included in the GEE models, as well as its metric, we considered a composite score would not be a useful and understandable measure for this analysis.
We conducted all analyses in Stata 17.0.
Results
Conceptual model and questionnaire
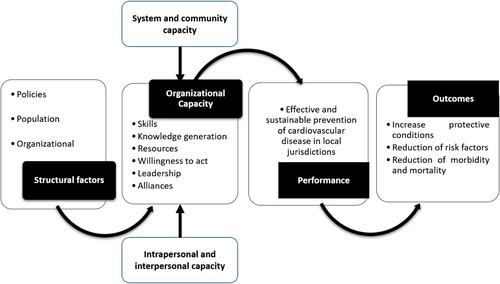
depicts the conceptual model for CVD prevention capacity at Colombian local level. This model suggests that there are three main determinants that influence this capacity, which, in turn is measured through six dimensions that shape the performance of LHD for achieving mid- and long-term behavioural, morbidity and mortality outcomes.
Figure 2. Conceptual model of the cardiovascular disease prevention capacity in Colombian local health departments.
The questionnaire comprised two sections. The first section asked about the political (e.g. GAO category, resources allocated to public health in the jurisdiction) and population-based determinants (e.g. population size, density) of the jurisdiction where the LHD was located, as well as internal characteristics of each organisation (e.g. size of the LHD's current workforce; size of its budget). The goal of this section was to provide information that took into account the organisation's external and internal context. To obtain information about the political and population-based determinants, we relied on routine data provided by the Colombian National Department of Statistics, the National Department of Planning, and the GAO. The information about the LHD’s internal context was self-reported by the participants. We did not apply validation procedures to this section because it was not intended as a scale.
The second section of the questionnaire focused on the assessment of the CVD prevention capacity. During the face validity process, experts did not suggest changes to modify the number of dimensions and items in the questionnaire but offered inputs about wording. There were no suggestions to add dimensions. Thus, this version of the questionnaire comprised 24 subdimensions and 103 items needed to measure the six dimensions depicted in the conceptual model. Items were measured using seven-point Likert scale, where 1 was ‘very bad’, ‘strongly disagree,’ or ‘absolutely inappropriate’ and 7 was ‘very good’, ‘strongly agree,’ or ‘absolutely appropriate’. This scale was used for all items, except for six in the subdimension of human resources, which asked about the educational level of the LHD’s staff.
Construct, content and criterion validity
These results were obtained through the application of the questionnaire in the 30 administrative units selected for the second phase of the study. We obtained 32 factorial solutions from the principal component. Eighteen factors did not fulfil the criteria for their retention, Cronbach’s α > 0.6 and eigenvalues ≥1. This left us with 19 subdimensions and 88 items (). The other factors were excluded from the final version of the questionnaire.
Table 1. Cronbach’s α of the final subdimensions of the organisational cardiovascular disease prevention capacity in Colombian local levels.
Regarding convergent validity, the correlations within the same subdimension were positive and statistically significant with coefficients ranging between 0.40 and 0.97 (results not shown). For the divergent validity, we obtained correlations ranging between −0.25 and 0.70, except for a higher correlation between the subdimension that asked about the actions for addressing psychosocial and behavioural factors and the one related to actions for addressing biological risks for CVD.
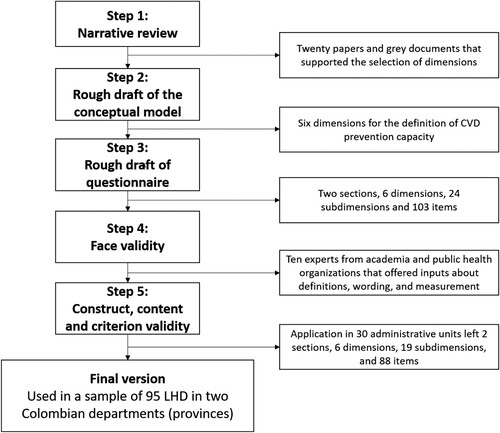
In terms of criterion validity, we found that the correlations between the total score and four dimensions were higher than 0.69. The exceptions were willing to act (0.46) and alliances (0.55). All correlations were statistically significant (p < 0.005). The five steps for the development of the questionnaire are summarised in the flow diagram in .
Figure 3. Flow diagram for the development of the quesstionaire for assess the organisational prevention capacity of cardiovascular disease in Colombian local health departments.
Overall CVD prevention capacity and its associated factors
We were able to get the information from the LHD of 95 municipalities in both departments, 40 in the West and 55 in the Mideast, resulting in a response rate of 91.3%. The population in these municipalities ranged from 325,477 to 1117 inhabitants in 2021. There were no missing values for the information collected from the 95 LHD. The mean of the overall CVD capacity prevention for the 95 municipalities was 5.10 (West = 5.14, Mideast = 5.06; p = 0.61). This score ranged from 3.38 to 6.20 (). shows the distribution in the overall score of the CVD capacity prevention for the municipalities in each department. also describes the mean and range for the dimensions and subdimensions of the LHD in each department. T-tests were performed to compare means across dimension and sub-dimensions. All tests were smaller than the pre-established threshold of 0.05. These results show that in both departments, willingness to act is the dimension with higher score, while the lowest scores were for resources, alliances and leadership; however, the order varies in each department.
Figure 4. Overall score of CVD prevention capacity in 95 municipalities of two Colombian departments.
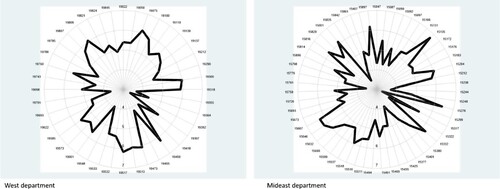
Table 2. Descriptive statistics of the overall, dimensions and subdimension of cardiovascular capacity prevention in two Colombian departments, 2021*.
In the multivariate GEE models (models a and b in ), we did find a statistically significant association between the overall CVD capacity prevention and the number of the employees in the LHD. No statistically significant association was found for either the resources allocated public in each municipality, or the population size of the municipality served for each LHD.
Table 3. Univariable and multivariable GEE models for the association between overall CVD prevention capacity with political, population and organisational factors.
Although we ran different models, including one with the three structural variables as continuous, we kept the model presented in because after comparing these models, we found that the results did not change and the deviance of the model in which resources was a categorical variable was slightly lower than in the model in which the three variables were run as continuous. The deviance of the retained model was 53.02.
Discussion
This study aimed to develop a conceptual model, validate a questionnaire and measure the CVD prevention capacity in LHD of Colombian municipalities, which are the basic administrative and political units of this country. Below, we discuss the main findings and limitations of this study.
In this study, we developed a conceptual model to guide the study of CVD prevention capacity based on the Colombian context. In HIC, conceptual models have been developed to assess the organisational capacity of local health organisations for preventing diseases (Meyer et al., Citation2012), specifically chronic conditions such as CVD (Hanusaik et al., Citation2007; Riley et al., Citation2003). Given the lack of consensus about the dimensions used for conceptualising and measuring a multidimensional and multilevel construct such as capacity, a challenge of this study was to select dimensions that match political, social, economic and public health aspects of Colombia. In response to this challenge, our conceptual model () sought to critically synthesise the evidence through six dimensions to cover this construct in accordance with the organisation and regulation of the Colombian public health system.
The proposed conceptual model suggests that policy, population and organisational factors shape the CVD prevention capacity at local Colombian levels. These three factors are important because they highlight that, from a socio ecological perspective, the functioning of LHDs is not isolated from proximal and distal factors, which play a key role in explaining how this organisations achieve their goals (Hanusaik et al., Citation2007; Meyer et al., Citation2012; Riley et al., Citation2003).
As public health service and system research has been characterised by poor reports of validity and reliability testing of new instruments (Harris et al., Citation2012), particularly a lack of validated quantitative measures of organisational capacity, this study makes a relevant contribution to this field in a country where these types of studies are not usually conducted. Transparency in this reporting is important to show how decisions about instruments were made and the rationale behind them. To contribute to addressing these barriers, our instrument adds to other efforts to measure general organisational capacity or specifically for preventing chronic diseases at local level. These other instruments have used quantitative or qualitative approaches (Bagley & Lin, Citation2009; Hanusaik et al., Citation2007).
This study found a heterogenous distribution of the score of CVD prevention capacity among the municipalities within each department (). This finding suggests that not all assessed LHD are in the same position to fulfil the competencies that have been assigned by the Colombian laws and regulations for the prevention of CVD. As described in the literature, this variability may be problematic because it is considered a contributing factor to the weak public health infrastructure (Erwin, Citation2008). Given CVD is a growing public health problem in Colombia, people living in municipalities with LHD with lesser capacity may be exposed to both weaker preventive interventions and more vulnerabilities.
Beyond the heterogenous distribution of the overall CVD prevention capacity found in this study, it also provides evidence of the dissimilar results in terms of the dimensions and subdimensions used to measure this capacity. While the results suggest that the selected LHD in both departments have a high willingness to act for the prevention of CVD, they face challenges in terms of resources, alliances and leadership. Regarding this former dimension, professional development policies, had the lowest scores among all 19 subdimension measured in both departments. Future research should assess if similar results are found in a larger sample of these organisations, or they vary among Colombian departments. However, this finding could show the low priority given in Colombia to interventions focused on educating the public health workforce by enhancing their competences in delivering services for the prevention of CVD. Thus, it stresses the importance of implementing evidence-based interventions that focused on enhancing specific dimensions and subdimensions in the sampled LHD.
To advance in the understanding of the structural factors associated with the CVD prevention capacity, in this study we selected three factors that have been associated in the literature in the field with the capacity and performance of LHD (Bhandari et al., Citation2010; Erwin, Citation2008; Schenck et al., Citation2015). Although the effect of financial resources allocated to public health and the population size were in the expected direction, these associations were not statistically significant. While the lack of statistical power may have restricted the finding of associations among these two variables and CVD prevention capacity, in adjusted models we found a low but statistically significant coefficient for the association between the dependent variable and the number of employees of the LHD. Regarding this association, two aspects are important to highlight. First, it may suggest that more proximal factors may play a stronger role in explaining the CVD prevention capacity in this sample, as having enough staff directly contributes to fulfil the functions of the LHD. Second, previous research has found that increases in staffing were significantly associated with decreases in cardiovascular mortality. This association may be consequence of more population-based preventive activities developed for a larger staff (Erwin et al., Citation2011). Thus, further studies in Colombia should examine the impact of staffing on different CVD outcomes in addition to provide evidence of staff turnover and profiles.
This study has four main limitations. First, like other studies in public health service and system research, we conducted a cross sectional study and used a non-probabilistic and small sample (Harris et al., Citation2012). Although these conditions prevent generalising the findings, one of our goals was to examine the psychometric features of the questionnaire by using a heterogonous sample and appropriate statistical approaches. Beyond the validation of the questionnaire, the small sample we used for measuring CVD prevention capacity restricted the inclusion of variables for other relevant information collected in the 95 municipalities. The cross-sectional approach of our study is problematic because it does not recognise the dynamic nature of the prevention capacity (Harris et al., Citation2012). Further studies aimed at assessing the CVD prevention capacity in Colombia using the validated questionnaire should have larger samples of LHDs and a longitudinal approach. Second, due to the lack of a gold standard questionnaire, we could not conduct a more formal assessment of criterion validity. To overcome this limitation, however, we used the approach suggested in the literature and applied in a similar validation study of instrument for a risk factor for chronic diseases (Dunet & Butterfoss, Citation2005). Third, like other studies in the field, our study is based on self-completion of a survey. However, this approach allows for a deeper understanding of the dimensions asked in the questionnaire because is the people working in the LHD who are more knowledgeable of the conditions and context for the prevention of CVD in their jurisdictions. Finally, we recognise that capacity prevention is an elusive construct, which may restrict our instrument, like others, from capturing all dimensions needed for measuring this construct comprehensively. However, the analytical approach and results of this study provide some confidence about the psychometric properties of our questionnaire and that it captures the essential aspects of the CVD prevention capacity in a language that made sense to experts of the face validity and respondents in LHD. A qualitative approach, as further step in our research agenda, should play an instrumental role in having a more comprehensive assessment of CVD prevention capacity in Colombian LHD.
Futures studies should address these limitations and advance knowledge in several directions. First, additional research is needed to examine the hypothesised relationship highlighted in the conceptual model between capacity and performance. For this research, it is necessary to have appropriate and available measures of performance of Colombian LHD. Second, it is necessary to assess if capacity prevention is associated with CVD outcomes and its risk factors. Although there are challenges to attribute health outcomes to LHD capacity, approaches used in previous research may contribute to generate in Colombia this type of evidence (Erwin et al., Citation2011; Mays & Smith, Citation2011; Schenck et al., Citation2015). Finally, once theory-based interventions have been designed or adapted and implemented, studies in this field in Colombia must tackle the lack of knowledge about effectiveness of programmes to increase CVD capacity and reduce risk factors and outcomes.
To our knowledge, this is the first study in Latin American aimed at validating a theory-based questionnaire and measuring CVD prevention capacity in LHD. In sum, the results of this study suggest that the questionnaire had a good performance in the different validation test we used, and it provides enough evidence of the usefulness of this instrument for assessing the CVD prevention capacity in Colombia. Without means for measuring this capacity in each specific context, it will be difficult to advance in enhancing LHD performance and reaching better prevention outcomes. In this regard, findings from the assessment of capacity at the local level could support the design of more specific capacity-building interventions, as well as provide valuable input for strategic planning in each LHD. Additionally, this study offers primary evidence of the relevance of the size of LHD.
Acknowledgments
This study was funded by the Vice President for Research Office and the School of Government of the Universidad de los Andes. We would like to acknowledge the valuable contribution of the public health staff in all jurisdictions involved in this study.
Disclosure Statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The datasets generated and analysed during the current study are available from the corresponding author upon reasonable request.
Additional information
Funding
References
- Bagley, P., & Lin, V. (2009). The development and pilot testing of a rapid assessment tool to improve local public health system capacity in Australia. BMC Public Health, 9(1), 413. https://doi.org/10.1186/1471-2458-9-413
- Bhandari, M. W., Scutchfield, F. D., Charnigo, R., Riddell, M. C., & Mays, G. P. (2010). New data, same story? Revisiting studies on the relationship of local public health systems characteristics to public health performance. Journal of Public Health Management and Practice, 16(2), 110–117. https://doi.org/10.1097/PHH.0b013e3181c6b525
- Burga, A. (2006). La unidimensionalidad de un instrumento de medición: Perspectiva factorial. Revista de Psicologia, 24(1), 53–80.
- Camacho, P. A., Gomez-Arbelaez, D., Molina, D. I., Sanchez, G., Arcos, E., Narvaez, C., Garcia, H., Perez, M., Hernandez, E. A., Duran, M., Cure, C., Sotomayor, A., Rico, A., David, T. M., Cohen, D. D., Rangarajan, S., Yusuf, S., & Lopez-Jaramillo, P. (2016). Social disparities explain differences in hypertension prevalence, detection and control in Colombia. Journal of Hypertension, 34(12), 2344–2352. https://doi.org/10.1097/HJH.0000000000001115
- Dirección de Epidemiología y Demografía. Ministerio de Salud y Protección Social. (2021). Análisis de Situación de Salud (ASIS). Colombia, 2021. Ministerio de Salud y Protección Social.
- Dunet, D. O., & Butterfoss, F. D. (2005). State plan index: A tool for assessing the quality of state public health plans. Preventing Chronic Disease, 2(2), A15.
- Erwin, P. C. (2008). The performance of local health departments: A review of the literature. Journal of Public Health Management and Practice, 14(2), E9–E18. https://doi.org/10.1097/01.PHH.0000311903.34067.89
- Erwin, P. C., Greene, S. B., Mays, G. P., Ricketts, T. C., & Davis, M. V. (2011). The association of changes in local health department resources with changes in state-level health outcomes. American Journal of Public Health, 101(4), 609–615. https://doi.org/10.2105/AJPH.2009.177451
- Erwin, P. C., Mays, G. P., & Riley, W. J. (2012). Resources that may matter: The impact of local health department expenditures on health status. Public Health Reports, 127(1), 89–95. https://doi.org/10.1177/003335491212700110
- Flaspohler, P., Duffy, J., Wandersman, A., Stillman, L., & Maras, M. A. (2008). Unpacking prevention capacity: An intersection of research-to-practice models and community-centered models. American Journal of Community Psychology, 41(3-4), 182–196. https://doi.org/10.1007/s10464-008-9162-3
- García-Peña, Á. A., Ospina, D., Rico, J., Fernández-Ávila, D. G., Muñoz-Velandia, Ó, & Suárez-Obando, F. (2022). Prevalencia de hipertensión arterial en Colombia según información del Sistema Integral de Información de la Protección Social (SISPRO). Revista Colombiana de Cardiología, 29(1), 29–35https://doi.org/10.24875/rccar.m22000114.
- Goodman, R. M., Speers, M. A., McLeroy, K., Fawcett, S., Kegler, M., Parker, E., Smith, S. R., Sterling, T. D., & Wallerstein, N. (1998). Identifying and defining the dimensions of community capacity to provide a basis for measurement. Health Education & Behavior, 25(3), 258–278. https://doi.org/10.1177/109019819802500303
- Hanusaik, N., O'Loughlin, J. L., Kishchuk, N., Eyles, J., Robinson, K., & Cameron, R. (2007). Building the backbone for organisational research in public health systems: Development of measures of oganisational capacity for chronic disease prevention. Journal of Epidemiology and Community Health, 61(8), 742–749. https://doi.org/10.1136/jech.2006.054049
- Hanusaik, N., Sabiston, C. M., Kishchuk, N., Maximova, K., & O'Loughlin, J. (2015). Association between organizational capacity and involvement in chronic disease prevention programming among Canadian public health organizations. Health Education Research, 30(2), 206–222. https://doi.org/10.1093/her/cyu062
- Harris, J. K., Beatty, K. E., Barbero, C., Howard, A. F., Cheskin, R. A., Shapiro, R. M. I. I., & Mays, G. P. (2012). Methods in public health services and systems research: A systematic review. American Journal of Preventive Medicine, 42(5 Suppl 1), S42–S57. https://doi.org/10.1016/j.amepre.2012.01.028
- Homer, J., Milstein, B., Wile, K., Pratibhu, P., Farris, R., & Orenstein, D. (2008). Modeling the local dynamics of cardiovascular health: Risk factors, context, and capacity. Preventing Chronic Disease, 5(2), A63.
- Hubbard, A. E., Ahern, J., Fleischer, N. L., Van der Laan, M., Lippman, S. A., Jewell, N., Bruckner, T., & Satariano, W. A. (2010). To GEE or not to GEE: comparing population average and mixed models for estimating the associations between neighborhood risk factors and health. Epidemiology, 21(4), 467–474. https://doi.org/10.1097/EDE.0b013e3181caeb90
- Instituto Nacional de Salud. (2013). Enfermedad Cardiovascular. Principal Causa de Muerte en Colombia. Instituto Nacional de Salud. Retrieved Junio 30, 2021 from https://www.ins.gov.co/Direcciones/ONS/Boletines/boletin_web_ONS/boletin1.html#:~:text = En%20Colombia%20la%20enfermedad%20cardiovascular,nuna%20tendencia%20hacia%20el%20descenso.
- LaFond, A. K., Brown, L., & Macintyre, K. (2002). Mapping capacity in the health sector: A conceptual framework. The International Journal of Health Planning and Management, 17(1), 3–22. https://doi.org/10.1002/hpm.649
- Lloret-Segura, S., Traver, A., & Hernandez-Baeza, A. (2014). El Análisis factorial exploratorio de los ítems: una guía práctica, revisada y actualizada. Anales de Psicología, 30(3), 23–26. https://doi.org/10.6018/analesps.30.3.199361
- Lucumi, D. I., Schulz, A. J., & Israel, B. A. (2016). Local actors’ frames of the role of living conditions in shaping hypertension risk and disparities in a Colombian Municipality. Journal of Urban Health, 93(2), 345–363. https://doi.org/10.1007/s11524-016-0039-8
- Lucumi, D. I., Schulz, A. J., Roux, A. V. D., & Grogan-Kaylor, A. (2017). Income inequality and high blood pressure in Colombia: A multilevel analysis. Cadernos of Saúde Publica, 33(11), e00172316. https://doi.org/10.1590/0102-311(00172316
- Mays, G. P., & Smith, S. A. (2011). Evidence links increases in public health spending to declines in preventable deaths. Health Affairs, 30(8), 1585–1593. https://doi.org/10.1377/hlthaff.2011.0196
- Meisel, J. D., Ramirez, A. M., Esguerra, V., Montes, F., Stankov, I., Sarmiento, O. L., & Valdivia, J. A. (2020). Using a system dynamics model to study the obesity transition by socioeconomic status in Colombia at the country, regional and department levels. BMJ Open, 10(6), e036534. https://doi.org/10.1136/bmjopen-2019-036534
- Meyer, A. M., Davis, M., & Mays, G. P. (2012). Defining organizational capacity for public health services and systems research. Journal of Public Health Management and Practice, 18(6), 535–544. https://doi.org/10.1097/PHH.0b013e31825ce928
- Pérez-Flórez, M., & Achcar, J. A. (2021). Desigualdades socioeconómicas en la mortalidad por enfermedades cardiovasculares: Región Pacifico de Colombia, 2002-2015. Ciência & Saúde Coletiva, 26(suppl 3), 5201–5214. https://doi.org/10.1590/1413-812320212611.3.02562020
- Perrot, B., Bataille, E., & Hardouin, J.-B. (2018). Validscale: A command to validate measurement scales. The Stata Journal, 18(1), 29–50. https://doi.org/10.1177/1536867X1801800104
- Ransom, J., Schaff, K., & Kan, L. (2012). Is there an association between local health department organizational and administrative factors and childhood immunization coverage rates? Journal of Health and Human Services Administration, 34(4), 418–455.
- Riley, B. L., Taylor, S. M., & Elliott, S. J. (2003). Organizational capacity and implementation change: A comparative case study of heart health promotion in Ontario public health agencies. Health Education Research, 18(6), 754–769. https://doi.org/10.1093/her/cyf051
- Schenck, A. P., Meyer, A. M., Kuo, T. M., & Cilenti, D. (2015). Building the evidence for decision-making: The relationship between local public health capacity and community mortality. American Journal of Public Health, 105(Suppl 2), S211–S216. https://doi.org/10.2105/AJPH.2014.302500
- Solar, O., & Irwin, A. (2010). A conceptual framework for action on the social determinants of health. Social determinants of dealth discussion paper 2. World Health Organization.
- Universidad Nacional de Colombia, Instituto Nacional de Salud, & Instituto Colombiano de Bienestar Familiar. (2017). Encuesta Nacional de la Situación Nutricional en Colombia 2015. Ministerio de Salud y Protección Social.
- Zurique-Sánchez, M. S., Zurique-Sánchez, C. P., Camacho-López, P. A., Sánchez-Sanabria, M., & Hernández-Hernández, S. C. (2019). Prevalence of arterial hypertension in Colombia. Systematic review and meta-analysis. Acta Medica Colombiana, 44(4), 20–33. https://doi.org/10.36104/amc.2019.1293