
ABSTRACT
Transfers between health facilities for postpartum women living with HIV are associated with disengagement from care. In South Africa, women must transfer from integrated antenatal/HIV care to general HIV services post-delivery. Thereafter, women transfer frequently e.g. due to geographic mobility. To explore barriers to transfer, we conducted in-depth interviews >2 years post-delivery in 28 participants in a trial comparing postpartum HIV care at primary health care (PHC) antiretroviral therapy (ART) facilities versus a differentiated service delivery model, the adherence clubs, which are the predominant model implemented in South Africa. Data were thematically analysed using inductive and deductive approaches. Women lacked information including where they could transfer to and transfer processes. Continuity mechanisms were affected when women transferred silently i.e. without informing facilities or obtaining referral letters. Silent transfers often occurred due to poor relationships with healthcare workers and were managed inconsistently. Fear of disclosure to family and community stigma led to transfers from local PHC ART facilities to facilities further away affecting accessibility. Mobility and the postpartum period presented unique challenges requiring specific attention. Information regarding long-term care options and transfer processes, ongoing counselling regarding disclosure and social support, and increased health system flexibility are required.
Introduction
The number of women on antiretroviral therapy (ART) in South Africa has increased substantially in recent years (Joint United Nations Programme on HIV/AIDS, Citation2022). However, there are concerns regarding disengagement from care postpartum (Haas et al., Citation2016; Knettel et al., Citation2018; Phillips et al., Citation2014). Disengagement is associated with HIV disease progression, virological failure, ART drug resistance and HIV transmission including vertical transmission during breastfeeding (Cohen et al., Citation2016; Davis et al., Citation2016; Frost et al., Citation2002; Johnson et al., Citation2017; Skarbinski et al., Citation2015; Zhao et al., Citation2018). Understanding the reasons for disengagement and developing ways to improve engagement in care in postpartum women living with HIV (WLHIV) are thus vital.
Transfer of care between health care facilities is a step in the continuum of care at which people living with HIV (PLHIV) including pregnant and postpartum women are at risk of disengagement (Bengtson et al., Citation2021; Odayar et al., Citation2022a, Citation2022b; Phillips et al., Citation2018). Transfer processes are potentially complicated, involving multiple facilities and actors. They are further complicated by the fact that they can be official or silent: official transfers are known to the health system, while silent transfers occur when patients transfer without informing the original facility or obtaining a referral letter (Geng et al., Citation2011; Wilkinson et al., Citation2015). In settings where HIV care has been integrated into antenatal care (ANC) including South Africa and other sub-Saharan African countries, pregnant women on ART prior to pregnancy must transfer from general primary health care (PHC) ART facilities to integrated ANC and prevention of mother-to-child transmission of HIV services (Phillips et al., Citation2015; Phillips et al., Citation2021). WLHIV who are not on ART prior to pregnancy are initiated as part of ANC. Postpartum, WLHIV must transfer to general PHC ART facilities; however, a substantial proportion do not link to HIV care (Phillips et al., Citation2018). Among those who do link, additional transfers between PHC ART facilities occur frequently for reasons including mobility and stigma and have been associated with viraemia (Clouse et al., Citation2017; Phillips et al., Citation2018).
Further, transfers from routine care to differentiated service delivery (DSD) models may also be associated with disengagement. DSDs aim to simplify care and provide services based on patient needs. In South Africa, adherence clubs (ACs) are the predominant model: pre-packaged ART is provided to stable patients by community health workers (CHWs) at ART facilities or community venues and postpartum women attending ACs have had good outcomes (Myer et al., Citation2017, Citation2022). However, 15% of both general adults and postpartum women transferred from general PHC ART facilities to ACs do not attend their first AC visit (Myer et al., Citation2017, Citation2022; Odayar et al., Citation2022b).
Reasons for disengagement and viraemia among PLHIV who transfer are unclear. Qualitative studies suggest that current transfer services do not meet patient needs; general adult patients in South Africa who disengaged from care described the transfer process as confusing and complicated and noted difficulties accessing care without specific documentation (Bisnauth et al., Citation2021; Miller et al., Citation2010). Pregnant women in Malawi also described difficulties accessing care when transferring without the correct paperwork (Bengtson et al., Citation2020) but data are limited in postpartum women and a better understanding of barriers to successful transfer is required to improve outcomes in this population. We used qualitative evidence to explore the experiences of transfer and possible barriers to transfer among postpartum women on ART.
Materials and methods
Study setting
This study is part of the Postpartum Adherence Clubs for Antiretroviral Therapy (PACART) study, which was a randomised controlled trial of differentiated care for postpartum ART delivery (NCT03200054) in Cape Town, South Africa (Myer et al., Citation2022; Odayar et al., Citation2019). In this trial, postpartum women on ART were randomised to referral to the ACs (intervention) or a PHC ART facility (standard of care) for ongoing HIV care. In the trial, DSD referral was associated with reduced viraemia through 24 months postpartum compared to referral to PHC ART facilities (Myer et al., Citation2022). The study was conducted at a large public sector PHC facility serving a peri-urban community of approximately 350,000 with high levels of unemployment (Myer et al., Citation2015). Antenatal HIV prevalence in the district was estimated at 22% in 2019 (Woldesenbet et al., Citation2021). The facility includes a midwife obstetric unit (MOU) which provides antenatal, obstetric, and postnatal care, with integrated HIV care. The facility also includes a PHC ART facility separate from the MOU but on the same premises which provides HIV care to the general adult population. The ART facility has an associated AC which operates off-site (Grimsrud et al., Citation2015).
Participants and description of postpartum care
In this setting, postpartum women on ART are referred directly from the MOU to a general adult PHC ART facility. ACs are the predominantly implemented differentiated care model and, as part of routine care, all general adult patients attending the PHC ART facility who are on ART for at least six months and are clinically stable are potentially eligible for referral to the ACs. Women who are referred from the MOU to the PHC ART facility are eligible for referral to the ACs once they meet the relevant criteria. However, postpartum women are not referred directly from the MOU to the ACs and specific clubs for postpartum women are not widely available. In this trial, participants who met the eligibility criteria were randomised to be referred to either the PHC ART facility (the control arm) or the ACs (intervention arm) directly from the MOU.
Women attending the MOU post-delivery were screened for participation in the parent trial and were enrolled if they were ≥18 years, < 10 weeks postpartum and had started ART in pregnancy. Additional criteria were based on eligibility criteria for referral to the ACs which require an HIV viral load (VL) < 400 copies/mL and no comorbidities (Grimsrud et al., Citation2016).
Screening and enrolment for the PACART trial took place from January 2016 to December 2017. Women randomised to the PHC ART facility arm were referred to PHC ART facilities in the local community, including the ART facility at the site of the MOU. Per routine care, the choice of PHC ART facility was based on proximity to the woman's residence and personal preference (Phillips et al., Citation2015). These women received a referral letter, and a two-month supply of ART and were told to visit their selected PHC ART facility within two months. Women randomised to the AC arm were referred to the AC associated with the PHC ART facility at the same site as the MOU. They were accompanied to the AC office, which is at the ART facility, by a CHW with their file and referral letter. At the AC office they were provided with a card with their first visit date and were given directions to the venue.
PHC ART facility visits are 1–2 monthly and include consultation by nurses or doctors (Grimsrud et al., Citation2016). The ACs operate from a community hall approximately one kilometre from the PHC ART facility. ACs are run by CHWs and comprise 25–30 patients who meet for 1-2 h every two months, except for the end-of-year Christmas and summer holiday period in South Africa when patients obtain a four-month supply of pre-packaged ART. AC participants who miss their first visit, are more than one week late for any other visit, or require clinical consultation are referred to the PHC ART facility. For the primary trial, women randomised to the AC or PHC ART facility arms could be transferred to other facilities or models of care as they would be in routine care.
Sampling
Women enrolled in the parent trial were followed through 24 months postpartum with follow-up visits concluding in January 2020. After their 24-month postpartum study visit, women were purposively sampled for qualitative semi-structured in-depth interviews (IDIs). Sampling was purposive to facilitate the enrolment of equal numbers of participants randomised to the AC and PHC ART facility arms. Participants were contacted telephonically, informed about the interviews and invited to participate. If interested, a date was arranged for them to visit the research site for an IDI.
Data collection
In 2019, IDIs were conducted by a trained and experienced female research assistant who was from the same community as the participants. Interviews were conducted in isiXhosa or English based on participant choice. A semi-structured interview guide was developed in English and translated into isiXhosa. The interview guide included the following topic areas: the experience of transfers from the MOU to the AC or PHC ART facility, the experience of subsequent transfers among patients attending the ACs or PHC ART facilities, transfer processes, and reasons for transferring when applicable. Participants were also asked about geographic mobility in the postpartum period and how they accessed care while travelling. Interviews were conducted in private rooms at the research site and were audio-recorded. Interviews were translated into English if conducted in isiXhosa, and transcribed by a staff member who was not involved in the interviews. Transcriptions and translations were reviewed by the interviewer to ensure accuracy.
Ethics approvals
All participants provided separate written informed consent for participation in IDIs. The study was reviewed and approved by the University of Cape Town Human Research Ethics Committee.
Analysis
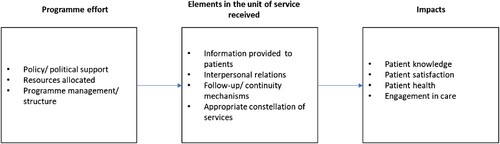
A conceptual framework to assess the quality of family planning services was adopted and adapted to guide these analyses as it maps how programme effort affects the elements of the service received which, in turn, affect programme impacts (Bruce, Citation1990). The aim of this analysis was to identify areas for improvement of transfer services and the quality of care framework has previously been used to identify how care can be improved (Brown et al., Citation1995). To identify barriers to successful transfer and identify places for intervention and/or improvement, we focussed on the elements in the unit of service received. To align the framework with participant responses in relation to transfer, we adapted the elements provided to include the following: information provided to patients, interpersonal and social relations, follow-up/continuity mechanisms and provision of an appropriate constellation of services () (Bruce, Citation1990).
Figure 1. Framework assessing the quality of the transfer service experience adapted from Bruce's framework assessing quality of family planning services (Bruce, Citation1990).
Data were analysed using thematic analysis in an iterative process. Interview transcripts were read for familiarisation, possible codes were identified, and these were discussed by the study team. Thereafter the transcripts were coded manually. Coding was both inductive, with codes informed by the adopted conceptual framework and deductive, with additional codes allowed to emerge from the data. Once coding was complete the text was organised to explore possible themes and emerging patterns with reference to the framework. In addition to the identification of themes, the analysis enabled comparison between initial transfers-out from the MOU and subsequent transfers, and between participants attending ACs and PHC ART facilities. To ensure rigour, the analysis process and identified themes were discussed at regular meetings with the study team to review and compare interpretations.
Results
IDIs were conducted with 28 women between July and September 2019, of whom 14 had been randomised to the AC arm and 14 to the PHC ART facility arm. At the time of the IDI, the median age was 30.6 years and the median duration postpartum was 26.4 months (). Among the 14 women randomised to the ACs, three had transferred to a PHC ART facility and one to an MOU by the time of their interview. Of the 14 randomised to the PHC ART facilities, five had transferred to a different PHC ART facility and four to an AC.
Table 1. Characteristics at time of in-depth interview.
The main themes were informed by the adapted quality of care framework and related to (1) information given to patients regarding facilities to which they could transfer and what to expect at those facilities, (2) interpersonal and social relationships including with HCWs, family and community members, (3) follow-up/continuity mechanisms including referral letters and (4) appropriateness of the constellation of services provided, where we identified mobility and the postpartum period as requiring specific attention.
Information provided to participants
Individuals may require transfer for numerous reasons, yet a few participants who attended the ACs throughout the postpartum period were unaware that they could transfer to another facility. When asked whether she had considered requesting a transfer one participant responded:
I would not have been able to start at a new [health facility] because they don't have my information. I would have stayed here. I would have stayed here because they have my information.
Numerous participants who knew that they could transfer did not know enough about the facilities to which they could transfer to make an informed choice. This applied to the initial transfer-out from the MOU and subsequent transfers. A participant in the PHC ART facility arm was unsure of which facilities she could transfer to from the MOU.
I chose to go to [the facility on the same premises as the MOU] because I wasn't familiar with the [other] places.
If there was a club in [the area closer to home], because sometimes I don't have money to travel, at least I could walk to [the area closer to home]. I don't know [if there is an AC closer], it was my first time hearing about the club here, so I don't know if there's one [there].
Yes, no one prepared me [provided her with information to make a choice]. I used to attend the [chosen PHC ART facility] a long time ago, besides now for my ART care, I used to go there for family planning … I knew that I would be taking my child [there], that's why I chose it.
I thought at [the PHC ART facility], I was going to … it's just going to enter there, produce your referral letter and then you get your medication and then you go. I didn't know that … you have to wait for your folder and stuff, see the nurses and stuff like that, and then go again to the pharmacy.
Several participants at the ACs described a lack of information regarding the process of transfer from the AC to the associated PHC ART facility. After more than a year attending the AC, a participant missed a visit and was transferred to the associated PHC ART facility.
… they [AC] told me to go back to [the PHC ART facility] to look for my folder. I felt like I wasn't being given important information like ‘When you leave [the club], you can go there and ask for so and so, and they will give you all of the information’. I thought that they would maybe call [the PHC ART facility] and tell them to expect a certain patient. … I didn't come to [the PHC ART facility] because I didn't know what I would say [there], this upset me … if they had told us where to go, I would ask the security because they are the first person you see, I would have asked them ‘Where in the [facility] is this side?’ … but I had no other information, so I decided to go to [a different PHC ART facility].
The lack of information thus covered numerous aspects including where to transfer, transfer processes and care delivery at the new facility, and occurred especially when transferring from the MOU to the PHC ART facility and when transferring out of the ACs.
Interpersonal and social relationships
Interpersonal problems leading to transfer included conflict with partners and family as well as relationships with HCWs. In addition, perceived stigma from community members contributed to the decision to transfer.
Conflict with partners/family
Conflict with partners or family that led to a breakdown in personal relationships resulted in women changing their living circumstances and having to change health facilities as illustrated below:
[My mother] is in the rural areas. She said I should come back [to stay with her]. I am waiting for the child, the girl, to finish writing exams. I have already asked for a transfer letter, the nurse said when I return in November, they will give me one.
Transfer due to perceived stigma
Many who had not disclosed to family and friends did not want to attend PHC ART facilities in their communities due to the risk of disclosure if seen there by people they knew. This seemed less of a concern for those in the AC arm. A participant in the PHC ART facility arm who had not disclosed to her husband transferred to a facility further away when she saw people she knew at her first visit and was still attending the facility to which she transferred two years later despite problems with transport.
When I started at the [PHC ART facility that] is close to my home … I would see familiar faces and think that one day when she is out of pills, she will come to my home and ask for our thing [pills]. She might find my husband at home and ask that he tells his wife to borrow her our things [pills]. When I entered [the PHC ART facility] one asked, ‘You too?’ and I said I was there for my cousin. When I went in to see the doctor, I asked for a transfer letter to [a PHC ART facility further from her home]. Sometimes, when I have no taxi fare, I think maybe I should go to that nearest [PHC ART facility]. But I ask myself if I am ready for it to be known before I say it. The day I disclose is the day I attend the [PHC ART facility] nearby.
This thing of going to [the PHC ART facility further away] is an inconvenience because sometimes I don't have money for transportation … Sometimes I have to borrow money to go for my [PHC ART facility] visit. Sometimes the person I borrow money from asks questions, like why I am attending a [PHC ART facility] that is far … I think that woman had mentioned that if I want to get my treatment there [a facility close to home], I could do so. I think [the facility closer to home mentioned by the other woman] is alright … I am familiar with [it] because I used to take the older child there.
In contrast to the PHC ART facility where there was a risk of being seen and talked about by community members, those attending the AC described it as a space free of stigma.
What I saw is that everyone [at the AC] is open … They talk about our treatment, with no problem. It is unlike [at the PHC ART facility], where you see someone from your area and they gossip … Yes, there are people I know in the club, but they are older. No one minds your business there. It is unlike in the community.
Negative interactions with HCWs
Several participants experienced negative interactions with HCWs leading to transfers. A participant attending the AC for more than two years missed an appointment and expressed fear of attending the AC thereafter.
Then I made a mistake in May this year and I was already pregnant; I did not go to [the AC] and I was afraid to go back again … Then I thought I should wait until my antenatal date at the [PHC facility], I will the get pills from there … That is how I defaulted, I did not take the pills well since then.
Another participant, who had been attending the PHC ART facility, was off treatment for a week at the time of her IDI. She had travelled and had timed her return to pick up her treatment without missing a dose. However, she had forgotten her treatment card at her travel destination and did not attend the facility. When asked why, she explained:
I don't want to go back there. Also, you can also see the way you are treated … The treatment [at the facility], you could ask a question, ‘Ask someone else, I don't understand your question’ they will say, they will tell you to ask in the room you will be going to … So, that is why I am running away from there.
Follow-up/continuity mechanisms
In routine care, continuity mechanisms differ for ACs and PHC ART facilities. Patients transferring between PHC ART facilities are given transfer letters. Participants transferred to the ACs are accompanied to the AC office by a CHW with their file and referral letter to facilitate continuity; no problems emerged regarding transfers to ACs. However, difficulties arose for participants transferring out of the ACs, leading to silent transfers i.e. transfers without referral letters. When participants are no longer eligible for AC attendance, e.g. those who have missed their first appointment, they are transferred to the PHC ART facility (Odayar et al., Citation2022b), usually with verbal instructions on where to go. As noted in the section on information provided to patients above, participants at ACs generally obtained limited information about PHC ART facility access. This led one participant who was transferred from the ACs to the PHC ART facility to silently transfer to a different PHC ART facility.
So, I thought to just come to [different facility]. When I got [there] I told them that I am a lady who lives [in the area], I am HIV positive, I used to get my pills at [the AC] but I missed my date, so at [the AC] they told me to go back to the [PHC ART facility] … but they didn't give me any directions about what to say when I got there; I thought instead of not taking pills at all, I thought it would be better to come to the nearest place to me. She asked me if I wouldn't miss my date when I go to this [PHC ART facility], I told her that I would try my best not to miss it because it doesn't happen often and I don't like to miss my date. She said okay, then called another lady who works there who checked me and tested me first, we went to another room where she opened a new folder for me and she gave me pills for two months.
At [the hospital] they gave you pills … So, I think I had pills for about one to two months after being discharged [from the hospital]. I actually went to [the new facility] while I still had pills where they told me I need to get a transfer from where I was getting my pills before, so I asked [a counsellor at the MOU] to make a transfer letter as though I had just been discharged from here.
Patients transferring between PHC ART facilities are given a referral letter and a date to visit the facility on their own. One participant transferred to the PHC ART facility from the MOU reported challenges because despite having a transfer letter from the MOU she was told she also needed to fetch her file from the MOU. She described navigating this experience.
… I had to wake up like early with a month-old baby, and come and sit for long hours, and then you sit for longer hours, and then you don't get the service. They tell you that ‘oh we don't have your stuff’, you have to go and fetch your own folders yourself. … So, it's like they were a bit rough ‘We don't have your folder, so how are we supposed to know what to give you? Go and fetch your folder, you know, we don't do the work for you’ and blah blah blah. I wanted to go back home, but I also wanted the medication. I just came to [the MOU] and then [the HCW at the MOU] gave me the folder. I gave [the staff at the PHC ART facility] the folder and they had to give me another date, and I had wasted transport money. They told me, ‘we can't help you now, you have to come another time.’ I felt like not coming back.
I didn't know that I should ask for a letter. I just travelled there. When I got there, I saw that the pills are almost finished. I went to the well-baby [PHC facility] and I asked what I should do. I told them I am breastfeeding, and I am on treatment. That man said … they can't give me pills but … he will do me a favour and give me one bottle and asked that I make sure that my documents have been sent by the end of the week. I asked a friend I trust to go to the MOU and ask for [a counsellor] who also worked there. They gave her that letter and she faxed it. It didn't take long. She got it immediately.
Patients who miss appointments at health facilities or the ACs should be traced telephonically or through home visits as per policy (South African National Department of Health, 2016). However, none of the women interviewed who disengaged or silently transferred described being traced.
Overall, many patients transferred silently, especially those transferring from the ACs to PHC ART facilities. Receiving facilities managed participants who transferred silently differently, and many participants described challenges and needing to find creative ways to access documentation to obtain care.
Appropriate constellation of services
Mobility
South African ART guidelines state that patients should be counselled to inform HCWs of their travel plans so that they can be given extra treatment and/or a transfer letter to a facility at their destination (South African National Department of Health, 2016). Many participants were aware of this, stating that they informed their facilities when travelling and ensured that they had enough medication for the trip. Most travelled over the end-of-year summer holiday period in South Africa when they routinely receive 3–4 months of treatment. However, a few participants were unsure of what to do when travelling (see last participant above). A participant who had to travel at short notice to look after ill family members was unsure when she would return and discussed her lack of clarity.
As I came here, I wanted to ask a question; because I am getting my treatment from the club. I am not sure how am I supposed to do this … . My mother-in-law has been calling me saying she is not well … So, there was a possibility that I would have left this weekend, but I couldn't just go, I decided that I will wait for [tomorrow]. So, I want to ask from the sister at that club on how I am supposed to do because I have to go to [another province]. I don't think it will be easy to come back soon, when I go in December, I know that I will look at my next date and easily come back. As I have to go now because someone is sick, I don't know, I have become weak.
I have never been. I usually go to home of the father of my eldest child, in [a different province]. The people that side speak [a language she does not speak], so I have not been to those [PHC ART facilities]. I don't even know how they are … In [her home town to which she also sometimes travels] the [PHC ART facilities] are far, they are in town. The [PHC ART facility] in the village often runs out of medication. I rarely go there. I go and come back without going there.
It is hard [to get your pills in the rural area] because you must travel and if you don't have a transfer [letter], you will not get them … It is far. You must take a taxi. [When I travelled] the pills were not enough. I asked [my husband] to collect my pills [at the AC] and give them to my uncle. My uncle is on the road a lot [bus driver]. I collected them from my uncle.
It is not far, its very close. But I wouldn't go because there is only this one in town so everyone I know will be there. So, I don't like to meet with them, I would rather ask for enough pills here. Otherwise I might default.
Care of postpartum/pregnant women
The experiences of a few women suggested that care was not always suited to the circumstances of postpartum women. Participants who do not attend their first AC visit are transferred to the associated PHC ART facility. As mentioned above under 'follow-up/continuity mechanisms', one mother missed her first AC appointment because her newborn was hospitalised but the reason for the missed visit was not considered by HCWs.
I missed the club because I was at the hospital … When I went back to the club, they sent me to [the PHC ART facility], when I got there and was trying to explain to the Sister who I think handles these things said; ‘Do you not have our phone numbers? You should have called us; I’m not getting involved with this’. I tried to explain that the phone number was on my card, which was at home. She just told me to go to reception and ask for a date to come here, mind you my child was still hospitalised, I had asked to come here for my treatment. When I explained this to her, she told me to get in the queue like everyone, I did, but I received a call telling me my child's condition was getting worse and I should get back there urgently. I was also exclusively breastfeeding so I had to go back, I went to tell her this and ask for a new date, she sent me to ask for a date a reception; I got there and same story, so I decided to find another way to get my pills because the care I received here was not good.
Discussion
Using an adapted quality-of-care framework to examine the experiences of transfer among postpartum women on ART, we identified numerous barriers to successful and sustainable transfer. Differences between transfers from the MOU post-delivery versus transfers that occurred once in long-term care were revealed, as well as differences between transfers involving ACs and PHC ART facilities. We are thus able to suggest interventions based on when transfers occur, and the types of facilities involved.
Barriers to transfer included participants at the ACs not knowing that they had the choice to transfer. This could lead women to continue at facilities that are inconvenient for them or where they are unhappy and contribute to disengagement. Women transferring from the MOU to the PHC ART facilities were ill-informed regarding facilities to which they could transfer and the changes in care delivery they would experience. Participants attending the ACs did not understand the process of transfer back to the PHC ART facility. A framework (Yehia et al., Citation2013) to understand the effects of transfer on health behaviours emphasised the importance of preparing PLHIV who transfer for the changes in care delivery they will experience, and this should be applied to postpartum women.
Relationships with HCWs, the community and family all contributed to the occurrence of transfer. Research has shown that negative interactions and fear-based relationships with HCWs lead to disengagement, including through fear of reprimand when rules are not adhered to (Fuente-Soro et al., Citation2019). In this analysis, we show that transfer is involved in this relationship, with women who have had negative interactions with HCWs silently transferring to access care. Silent transfers have been associated with gaps in care and viraemia (Hickey et al., Citation2016; Sikazwe et al., Citation2019) and many participants who silently transferred in this analysis experienced treatment interruptions. Furthermore, PHC ART facilities managed silent transfers differently with some patients sent away or given short-term treatment and required to obtain a referral letter. PLHIV in South Africa who silently transfer have described having to restart treatment or being unable to access care (Bisnauth et al., Citation2021; Miller et al., Citation2010). Guidelines state that patients without treatment should not be refused care regardless of whether they have referral letters, but do not provide specific guidance on management and this should be addressed (South African National Department of Health, Citation2020). The risk of inadvertent disclosure if seen by people they know led women to transfer, as has been previously described among pregnant women in Malawi (Bengtson et al., Citation2020). Here, patients who transferred from the MOU to PHC ART facilities subsequently transferred to PHC ART facilities further away early in the postpartum period, sometimes leading to transport difficulties. Some women were still attending these facilities at 24 months postpartum despite these difficulties. In contrast, women attending the ACs did not mention community stigma as a cause of transfer, with many finding the AC environment supportive. Relationships with partners, including the occurrence of abuse, also led to transfers. HCWs should ask about reasons for transfer and other stressors that participants may be experiencing to identify those in need of additional support.
Women who were geographically mobile experienced numerous different barriers to transfer. Some were unaware of the transfer processes. Numerous participants mentioned barriers to transfer at their travel destinations and preferred to take sufficient treatment with them for the duration of the trip. Similar to all women, access to care at travel destinations for mobile women was affected by lack of documentation and fear of stigma. Unforeseen circumstances and having to travel at short notice may affect access to care for mobile women and the health care system should be understanding of this.
To improve outcomes in postpartum women who transfer, women should be provided with information regarding long-term care options, particularly those being transferred from the MOU to general ART care and those attending ACs. Women should be prepared for what to expect at receiving facilities, particularly those transferring from the MOU to PHC ART facilities, and transfer processes should be explained, especially when being transferred from ACs to PHC ART facilities. Considering the long-term effects of stigma on health behaviours, women may require ongoing counselling, before and after transfer, particularly around disclosure and social support, and especially those attending PHC ART facilities. In addition, the health care system needs to respond with flexibility e.g. to transfers due to mobility that occur at short notice and needs to be understanding of people's circumstances including postpartum women. Silent transfers should be prevented if possible, including by improving relationships between HCWs and patients. Research to inform management of silent transfers when they occur is required.
This study provides insight into a population at high risk of disengagement through 24 months postpartum and provides practical suggestions for improved care delivery. Further, as far as we are aware, this is one of the first studies evaluating transfers to and from DSD models. However, the analysis has limitations, including that participants were enrolled in a research study, and this may have affected health behaviour. In addition, the study was based at one MOU and AC service and results may not be generalisable to other settings.
We described the experiences of transfer among postpartum women on ART and identified numerous barriers to successful transfer. Women were not provided with sufficient information regarding the transfer, particularly those transferring out from the MOU and the ACs. In numerous examples, poor relationships with HCWs contributed to the occurrence of silent transfers which affect continuity of care. A lack of flexibility regarding patients’ circumstances including for geographically mobile and postpartum women also affected health care access. Information regarding long-term care options and transfer processes, ongoing counselling regarding disclosure and social support, and increased health system flexibility are required.
Acknowledgements
The authors are grateful to all those who participated in the study.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Bengtson, A. M., Espinosa Dice, A. L., Kirwa, K., Cornell, M., Colvin, C. J., & Lurie, M. N. (2021). Patient transfers and their impact on gaps in clinical care: Differences by gender in a large cohort of adults living with HIV on antiretroviral therapy in South Africa. AIDS and Behavior, 25(10), 3337–3346. https://doi.org/10.1007/s10461-021-03191-2
- Bengtson, A. M., Go, V., Kumwenda, W., Lurie, M., Kutengule, A., Owino, M., & Hosseinipour, M. (2020). “A way of escaping”: a qualitative study exploring reasons for clinic transferring and its impact on engagement in care among women in option B+. AIDS Care, 32(1), 72–75. https://doi.org/10.1080/09540121.2019.1614521
- Bisnauth, M. A., Davies, N., Monareng, S., Buthelezi, F., Struthers, H., McIntyre, J., & Rees, K. (2021). Why do patients interrupt and return to antiretroviral therapy? Retention in HIV care from the patient’s perspective in Johannesburg, South Africa. PLoS One, 16(9), e0256540. https://doi.org/10.1371/journal.pone.0256540
- Brown, L., Tyane, M., Bertrand, J., Lauro, D., Abououakil, M., & deMaria, L. (1995). Quality of care in family planning services in Morocco. Studies in Family Planning, 26(3), 154–168. https://doi.org/10.2307/2137834
- Bruce, J. (1990). Fundamental elements of the quality of care: A simple framework. Studies in Family Planning, 21(2), 61–91. https://doi.org/10.2307/1966669
- Clouse, K., Vermund, S. H., Maskew, M., Lurie, M. N., MacLeod, W., Malete, G., Carmona, S., Sherman, G., & Fox, M. P. (2017). Mobility and clinic switching among postpartum women considered lost to HIV care in South Africa. Journal of Acquired Immune Deficiency Syndromes, 74(4), 383–389. https://doi.org/10.1097/QAI.0000000000001284
- Cohen, M., Chen, Y., & McCauley, M. (2016). Antiretroviral therapy for the prevention of HIV-1 transmission. New England Journal of Medicine, 375(9), 830–839. https://doi.org/10.1056/NEJMoa1600693
- Davis, N. L., Miller, W. C., Hudgens, M. G., Chasela, C. S., Sichali, D., Kayira, D., Nelson, J. A. E., Fiscus, S. A., Tegha, G., Kamwendo, D. D., Rigdon, J., Stringer, J. S. A., Juliano, J. J., Ellington, S. R., Kourtis, A. P., Jamieson, D. J., & Van Der Horst, C. (2016). Maternal and breast milk viral load: Impacts of adherence on peri-partum HIV infections averted - the BAN study. Journal of Acquired Immune Deficiency Syndrome, 73(5), 572–580. https://doi.org/10.1097/QAI.0000000000001145 0000000000001145.
- Frost, S. D. W., Martinez-Picado, J., Ruiz, L., Clotet, B., & Leigh Brown, A. J. (2002). Viral dynamics during structured treatment interruptions of chronic human immunodeficiency virus type 1 infection. Journal of Virology, 76(3), 968–979. https://doi.org/10.1128/JVI.76.3.968-979.2002
- Fuente-Soro, L., Iniesta, C., López-Varela, E., Cuna, M., Guilaze, R., Maixenchs, M., Bernardo, E. L., Augusto, O., Gonzalez, R., Couto, A., Munguambe, K., & Naniche, D. (2019). Tipping the balance towards long-term retention in the HIV care cascade: A mixed methods study in southern Mozambique. PLoS One, 14(9), e0222028. https://doi.org/10.1371/journal.pone.0222028
- Geng, E. H., Glidden, D. V., Bwana, M. B., Musinguzi, N., Emenyonu, N., Muyindike, W., Christopoulos, K. A., Neilands, T. B., Yiannoutsos, C. T., Deeks, S. G., Bangsberg, D. R., & Martin, J. N. (2011). Retention in care and connection to care among HIV-infected patients on antiretroviral therapy in Africa: Estimation via a sampling-based approach. PLoS One, 6(7), e21797. https://doi.org/10.1371/journal.pone.0021797
- Grimsrud, A., Lesosky, M., Kalombo, C., Bekker, L., & Myer, L. (2016). Community-Based adherence clubs for the management of stable antiretroviral therapy patients in Cape Town, South Africa: A cohort study. Journal of Acquired Immune Deficiency Syndromes, 71(1), 16–23. https://doi.org/10.1097/QAI.0000000000000863
- Grimsrud, A., Sharp, J., Kalombo, C., Bekker, L. G., & Myer, L. (2015). Implementation of community-based adherence clubs for stable antiretroviral therapy patients in Cape Town, South Africa. Journal of the International AIDS Society, 18(1), 19984. https://doi.org/10.7448/IAS.18.1.19984
- Haas, A. D., Tenthani, L., Msukwa, M. T., Tal, K., Jahn, A., Gadabu, O. J., Spoerri, A., Chimbwandira, F., van Oosterhout, J. J., & Keiser, O. (2016). Retention in care during the first 3 years of antiretroviral therapy for women in Malawi’s option B+ programme: An observational cohort study. The Lancet HIV, 3(4), e175–e182. https://doi.org/10.1016/S2352-3018(16)00008-4
- Hickey, M. D., Omollo, D., Salmen, C. R., Mattah, B., Blat, C., Ouma, G. B., Fiorella, K. J., Njoroge, B., Gandhi, M., Bukusi, E. A., Cohen, C. R., & Geng, E. H. (2016). Movement between facilities for HIV care among a mobile population in Kenya: Transfer, loss to follow-up, and reengagement. AIDS Care - Psychological and Socio-Medical Aspects of AIDS/HIV, 28(11), 1386–1393. https://doi.org/10.1080/09540121.2016.1179253
- Johnson, L. F., May, M. T., Dorrington, R. E., Cornell, M., Boulle, A., Egger, M., & Davies, M. A. (2017). Estimating the impact of antiretroviral treatment on adult mortality trends in South Africa: A mathematical modelling study. PLOS Medicine, 14(12), e1002468. https://doi.org/10.1371/journal.pmed.1002468
- Joint United Nations Programme on HIV/AIDS. (2022). UNAIDS Data 2022.
- Knettel, B. A., Cichowitz, C., Ngocho, J. S., Knippler, E. T., Chumba, L. N., Mmbaga, B. T., & Watt, M. H. (2018). Retention in HIV care during pregnancy and the postpartum period in the option B+ Era: Systematic review and meta-analysis of studies in Africa. Journal of Acquired Immune Deficiency Syndromes, 77(5), 427–438. https://doi.org/10.1097/QAI.0000000000001616
- Miller, C. M., Ketlhapile, M., Rybasack-Smith, H., & Rosen, S. (2010). Why are antiretroviral treatment patients lost to follow-up? A qualitative study from South Africa. Tropical Medicine & International Health, 15(Suppl1), 48–54. https://doi.org/10.1111/j.1365-3156.2010.02514.x
- Myer, L., Iyun, V., Zerbe, A., Phillips, T. K., Brittain, K., Mukonda, E., Allerton, J., Kalombo, C. D., Nofemela, A., & Abrams, E. J. (2017). Differentiated models of care for postpartum women on antiretroviral therapy in Cape Town, South Africa: A cohort study. Journal of the International AIDS Society, 20(Suppl 4), 32–40. https://doi.org/10.7448/IAS.20.5.21636
- Myer, L., Odayar, J., Malaba, T. R., Allerton, J., Kabanda, S., Hu, N. C., Kalombo, C., Hsiao, N. Y., Jacobs, S., Nofemela, A., & Lesosky, M. (2022). Improved virologic outcomes in postpartum women living with HIV referred to differentiated models of care. Aids (london, England), 36(15), 2203–2211. https://doi.org/10.1097/QAD.0000000000003385
- Myer, L., Phillips, T., Manuelli, V., McIntyre, J., Bekker, L. G., & Abrams, E. J. (2015). Evolution of antiretroviral therapy services for HIV-infected pregnant women in Cape Town, South Africa. Journal of Acquired Immune Deficiency Syndromes, 69(2), e57–e65. https://doi.org/10.1097/QAI.0000000000000584
- Odayar, J., Chi, B. H., Phillips, T. K., Mukonda, E., Hsiao, N. Y., Lesosky, M., & Myer, L. (2022a). Transfer of patients on antiretroviral therapy attending primary health care services in South Africa. Journal of Acquired Immune Deficiency Syndromes, 90(3), 309–315. https://doi.org/10.1097/QAI.0000000000002950
- Odayar, J., Malaba, T. R., Allerton, J., Kabanda, S., Huang, D., Kalombo, C., Lesosky, M., & Myer, L. (2022b). Virologic outcomes after early referral of stable HIV-positive adults initiating ART to community-based adherence clubs in Cape Town, South Africa: A randomised controlled trial. PLoS One, 17(11), e0277018. https://doi.org/10.1371/journal.pone.0277018
- Odayar, J., Malaba, T. R., Allerton, J., Lesosky, M., & Myer, L. (2019). Delivery of antiretroviral therapy to HIV-infected women during the postpartum period: The postpartum adherence clubs for antiretroviral therapy (PACART) trial. Contemporary Clinical Trials Communications, 16, 100442. https://doi.org/10.1016/j.conctc.2019.100442
- Phillips, T., Mcnairy, M. L., Zerbe, A., Myer, L., & Abrams, E. J. (2015). Postpartum transfer of care Among HIV-infected women initiating antiretroviral therapy during pregnancy. Journal of Acquired Immune Deficiency Syndromes, 70(3), e102–e109. https://doi.org/10.1097/QAI.0000000000000771
- Phillips, T., Thebus, E., Bekker, L.-G., McIntyre, J., Abrams, E. J., & Myer, L. (2014). Disengagement of HIV-positive pregnant and postpartum women from antiretroviral therapy services: A cohort study. Journal of the International AIDS Society, 17(1), 19242. https://doi.org/10.7448/IAS.17.1.19242
- Phillips, T. K., Clouse, K., Zerbe, A., Orrell, C., Abrams, E. J., & Myer, L. (2018). Linkage to care, mobility and retention of HIV-positive postpartum women in antiretroviral therapy services in South Africa. Journal of the International AIDS Society, 21(Suppl4), e25114. https://doi.org/10.1002/jia2.25114
- Phillips, T. K., Olsen, H., Teasdale, C. A., Geller, A., Tsoeu, M., Buono, N., Kayira, D., Ngeno, B., Modi, S., & Abrams, E. J. (2021). Uninterrupted HIV treatment for women: Policies and practices for care transitions during pregnancy and breastfeeding in côte d’Ivoire, Lesotho and Malawi. PLoS One, 16(12), e0260530. https://doi.org/10.1371/journal.pone.0260530
- Sikazwe, I., Eshun-Wilson, I., Sikombe, K., Czaicki, N., Somwe, P., Mody, A., Simbeza, S., Glidden, D. V., Chizema, E., Mulenga, L. B., Padian, N., Duncombe, C. J., Bolton-Moore, C., Beres, L. K., Holmes, C. B., & Geng, E. (2019). Retention and viral suppression in a cohort of HIV patients on antiretroviral therapy in Zambia: Regionally representative estimates using a multistage-sampling-based approach. Plos Medicine, 16(5), e1002811. https://doi.org/10.1371/journal.pmed.1002811
- Skarbinski, J., Rosenberg, E., Paz-Bailey, G., Hall, H. I., Rose, C. E., Viall, A. H., Fagan, J. L., Lansky, A., & Mermin Jonathan, H. (2015). Human immunodeficiency virus transmission at each step of the care continuum in the United States. JAMA Internal Medicine, 175(4), 588–596. https://doi.org/10.1001/jamainternmed.2014.8180
- South African National Department of Health. (2016). Adherence Guidelines for HIV, TB and NCDs.
- South African National Department of Health. (2020). Referral Policy for South African Health Services and Referral Implementation Guidelines.
- Wilkinson, L. S., Skordis-Worrall, J., Ajose, O., & Ford, N. (2015). Self-transfer and mortality amongst adults lost to follow-up in ART programmes in low- and middle-income countries: Systematic review and meta-analysis. Tropical Medicine and International Health, 20(3), 365–379. https://doi.org/10.1111/tmi.12434
- Woldesenbet, S.A., Lombard, C., Manda, S., Kufa, T., Ayalew, K., Cheyip, M., & Puren, A. (2021). The 2019 National Antenatal Sentinel HIV Survey, South Africa, National Department of Health.
- Yehia, B. R., Kangovi, S., & Frank, I. (2013). Patients in transition: Avoiding detours on the road to HIV treatment success. Aids (london, England), 27(10), 1529–1533. https://doi.org/10.1097/QAD.0b013e328360104e
- Zhao, Y., Wu, Z., McGoogan, J. M., Shi, C. X., Li, A., Dou, Z., Ma, Y., Qin, Q., Brookmeyer, R., Detels, R., & Montaner, J. S. G. (2018). Immediate antiretroviral therapy decreases mortality among patients with high CD4 counts in China: A nationwide, retrospective cohort study. Clinical Infectious Diseases, 66(5), 727–734. https://doi.org/10.1093/cid/cix878
