ABSTRACT
This systematic review assessed outcome evidence of financial education and plural interventions aimed at reducing HIV vulnerability for youth, orphans and vulnerable children in low and middle-income countries. Relevant evidence reviews found both positive and mixed evidence that HIV prevention may be addressed through economic strengthening activities such as financial education for youth. There was some evidence related to the potential for plural interventions that include sexual and reproductive health education but limited quality evidence that focused on HIV vulnerable youth in low-and-middle income countries. To address this gap, the team systematically reviewed the scope and strength of impact evidence of financial education and plural interventions for HIV-vulnerable youth and OVC in LMIC, with a focus on outcome analysis. Of 5,216 records, 16 moderate to higher quality studies representing 10 interventions were identified, mostly focusing on HIV-vulnerable girls in Sub-Saharan Africa. More than half of the interventions were plural and included access to finance and counseling or social supports. Most used an experimental design. The strongest odds ratio effects were found to be on HIV-related outcomes by plural interventions. Observed improvements included increased HIV related knowledge, attitudes, reduced sexual risk-taking behavior and improved self-efficacy. While positive effects were also observed related to increased savings and improved attitudes toward saving, generally interventions showed mixed effects on financial and economic outcomes. This review supports emerging evidence that plural interventions are associated with positive health and economic outcomes for vulnerable youth and children in LMIC. Even so, as a body of evidence, it is not clear which components are effective at producing favorable outcomes. Quality evidence is needed in more settings separating out economic, health and self-efficacy components to better understand pathways and effects on outcomes. Segmentation will enhance our understanding of asset, capability and self-efficacy theories for greater impact.
Introduction
Global commitments to reverse the HIV epidemic will only be achieved if strategies focus on children and youth (United Nations).Footnote1 HIV is the leading cause of youth mortality in Africa, and the second cause of death among young people worldwide (UNAIDS, Citation2015; WHO, Citation2014). Young girls are particularly vulnerable (Fleischman & Peck, Citation2015), accounting for 20% of the new HIV infections globally in 2015, despite accounting for just 11% of the adult population (UNAIDS, Citation2016, p. 8). As of 2014, 13.3 million children were orphaned and made vulnerable (OVC)Footnote2 by AIDS globally of an estimated 140 million orphaned to all causes (UNICEF, Citation2016).
There is positive evidence linking economic interventions and HIV reduction. Kim, Pronyk, Barnett, and Watts (Citation2008, p. 61) found that economic interventions have more potential to address structural issues such as poverty and gender norms that influence the health context as compared to more conventional health strategies. Orton et al. (Citation2016) found that membership in larger, established microfinance groups showed some improvements in maternal and infant mortality, better sexual health and, in some cases, lower levels of interpersonal violence. Pronyk et al. (Citation2008) found the combination of financial education and microfinance effective at reducing HIV risk behavior in young women in rural South Africa. Cui, Lee, Thirumurthy, Muessig, and Tucker (Citation2013) found potential utility in microenterprise development to reduce HIV risk, particularly for sex workers with limited effects for non-sex workers. Asset theory holds that economic and financial supports reduce economic vulnerability and increase overall resources which may lead to other positive personal and social outcomes (Kennedy, Fonner, O’Reilly, & Sweat, Citation2014; Witte et al., Citation2015).
However, other evidence suggests that increased economic strengthening does not necessarily translate to improved health and HIV prevention. Kennedy et al. (Citation2014, p. 13) found positive effects on HIV prevention through condom use and reducing sexual partners in a minority of studies. There was ‘inconclusive evidence that microfinance and vocational skills interventions were effective at changing HIV-related sexual risk behaviors,’ noting the inadequate statistical power in some studies. One study even showed increased risk of harassment. Dworkin and Blankenship (Citation2009) found microfinance to show mixed results in offering young women independence from male partners. However, there was more positive evidence where skills taught in microfinance included assertiveness and challenging gender norms. ICRW (Citation2010) cautioned that economic strategies do not necessarily empower girls and women given social, economic and legal constraints that are structural in nature. This study also identified that economic activities may increase incentives for girls to leave school which may expose them to different kinds of risks. Students reported positive impacts on self-confidence but found financial education less applicable when they lived in poverty (Shephard et al., Citation2017).
There is growing recognition that in HIV-prevention, economic vulnerability is best addressed alongside other vulnerabilities through multiple interventions such as health education, counseling, safe spaces, training in negotiating ability and well-being (De Guzman, Citation2001; Dworkin & Blankenship, Citation2009; Kim et al., Citation2008; Plourde, Fischer, Cunningham, Brady, & McCarraher, Citation2016; UNAIDS & The African Union, Citation2015). The confidence and ‘self-efficacy’ to act on knowledge is a complex mix of personal and societal norms and conditions (Bandura, Citation1977, Citation1994). The ability to reach economic goals may also be associated with increased self-efficacy to avoid unprotected sex that some housing and income-generating arrangements entail (Jennings, Ssewamala, & Nabunya, Citation2016, p. 279). International Center for Research on Women [ICRW] (Citation2010) found that social supports and mentoring improved outcomes in their review of eight economic and plural interventions for HIV-vulnerable girls and young women. Economic stress was linked with low decision-making power for girls which can lead to early school dropouts, early marriage and gender-based violence including trafficking.
There is emerging but scant evidence related to financial education interventions for HIV vulnerable youth (Kim et al., Citation2008), particularly in the Global South. Plural interventions usually have economic, health and self-efficacy components. However, too few studies separate these components to understand their particular effects on HIV outcomes (Child and Youth Finance International [CYFI], Citation2012; YouthPower, Citation2017). Further, few impact studies have adequate sample sizes (Kim et al., Citation2008); long-term effects (Kalamar, Bayer, & Hindin, Citation2016; YouthPower, Citation2017); reliability and validity related to data contamination, attrition and statistical power (Kalamar et al., Citation2016).
This evidence review addresses these gaps by focusing on high-quality evidence for financial education and plural interventions for HIV vulnerable youth and OVC in low- and middle-income countries (LMIC) as World Bank defined.Footnote3 The review examined intervention components to analyze outcome pathways for reducing HIV vulnerability in youth and children.
Materials and methods
Search strategy and identification
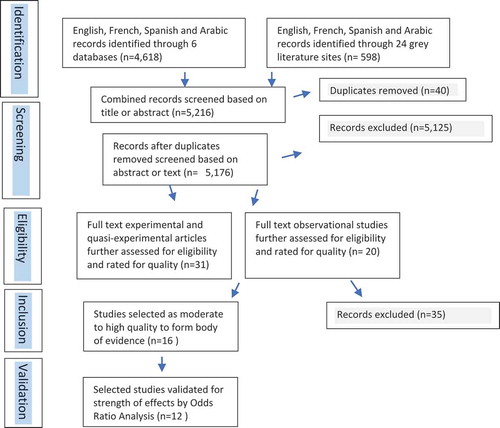
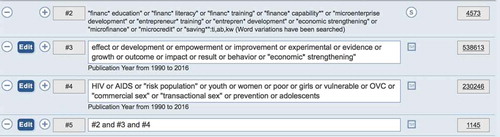
A diverse teamFootnote4 searched 6 bibliographic mainly health-related databasesFootnote5 and 24 grey literature sitesFootnote6 for relevant studies in English, French, Spanish and Arabic published between 1990 and 2016.Footnote7 See . Key search words included: financ* education; finance* literacy; economic strengthening; HIV; AIDs; vulnerable; children; youth; OVC. [See Appendix 1].
Figure 1. Review process.
Screening for eligibility
Two reviewers screened the titles and abstracts for relevant studies focused on financial education for vulnerable youth or OVC in LMIC with or without financial services.Footnote8 Plural interventions that combined financial with health, sexual and reproductive education with other social supports were also included. Relevant outcomes included: financial behavior change; financial attitude change; change in use of or access to a financial product or service; change in expenditures related to health; change in treatment, prevention or other behaviors related to HIV; change in financial situation; change in economic situation; other unanticipated changes in outcomes. Experimental and quasi-experimental research methods were considered where data were gathered at baseline and at least six months after the end of the intervention. Mixed methods studies were considered provided they demonstrated validity in terms of randomization, appropriate sampling and controls and minimization of bias errors and attrition. Single-group pre-post test design or single-subject design studies were excluded.
Two independent reviewers screened records based on the title, and where unclear, abstract and main text. After duplicates were removed, 51 studies were selected for quality assessment.Footnote9
Inclusion
Three independent reviewers screened full text articles and critically rated the quality of evidence based on clarity of outcomes, cogency, internal and external validity, reliability (DFID, Citation2014), target population relevance including gender awareness and appropriateness of pedagogy including safe spaces and learner-centered approaches. High-quality interventions had a clear method for randomization, control and could account for, or at least render explicit, potential risks in selection bias, estimation, spill-over or contamination effects. See Appendix 2 for the rating tool. From the 51 studies, 16 studies evaluating 10 interventions rated moderate to higher quality and were selected to form the body of evidence ().
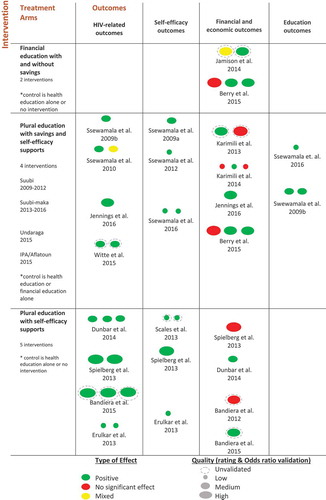
Figure 2. Evidence map.
Data analysis and validation
The Context Mechanisms Outcomes (CMO) approach (van der Knaap, Leeuw, Bogaerts, & Nijssen, Citation2008) was used to map the evidence in terms of multiple pathways to see which programs work.Footnote10 Context (C) examined the conditions of setting and target population issues such as gender, education setting. The mechanisms (M) analyzed and clustered the treatment arms to examine individual components of interventions. Outcomes (O) analyzed outcome direction (positive, no effect, mixed) and type (HIV-related; self-efficacy; financial and economic; education). See and Appendix 3 for the detailed chart of evidence.
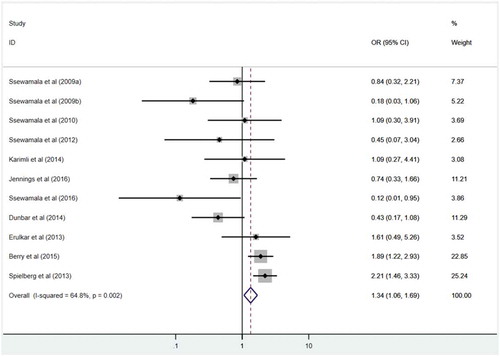
The body of evidence was then validated using odds ratio analysis (Appendix 4). This analysis illustrated the relative effect or weight of these measures based on confidence levels and sample sizes. Only 12 studies had comparable enough variables and treatment conditions to be validated and only data from the baseline and the end-line were used.
Results
This section reports the findings of two financial and nine plural education intervention arms emphasizing the outcome effects of individual treatment arms. See the evidence map (see ) for the three different types of treatment arms and the corresponding outcome pathways. Each oval represents an individual outcome. One intervention (Berry, Karlan, & Pradhan, Citation2015) is included in both financial and plural education. See Appendix 3 for the detailed evidence table including Odds ratio analysis and confidence intervals.
Financial education treatment arms
Two interventions focused on financial education for vulnerable youth (with and without savings) with mixed results on financial and economic outcomes. A study in Uganda combined financial education with savings in one treatment arm and savings-only in the other (Jamison, Karlan, & Zinman, Citation2014). The combined treatment group improved financial literacy after 9 months where the savings-only group did not. These results might indicate that financial education plays a role in effective use of financial services. However, there was little evidence that savings account access and financial education complement one another.
An intervention in Ghana compared financial education and savings with plural education (combined with personal awareness and child rights education) and savings (Berry et al., Citation2015). Both led to a positive effect on savings after 9 months mainly due to a change in location (from home to school) rather than an increase in savings. Children were also more likely to work than have leisure with financial education, but no negative effect was shown on either child labor or school attendance. These studies some inconclusive evidence for the role of financial education in improving financial literacy and savings. The quality of these studies was high though the Ugandan study was unvalidated by the odds ratio analysis because the study used Ordinary least squares analysis and did not use comparable variables.
Plural education with plural supports
Four plural (financial and health education) interventions offered self-efficacy supports and savings services with six positive effects on HIV outcomes and four positive effects on self-efficacy. In three of the interventions, plural education led to positive outcomes compared with either health education or financial education alone. Effects on financial and economic outcomes were more mixed with five positive outcome effects and four with no effect.
The earlier intervention in Ghana showed that the plural education had the same positive effects on savings behavior (Berry et al., Citation2015). An intervention with female street-based sex workers in Mongolia provided financial education and matched savings only in the treatment which showed fewer paying sexual partners and zero unprotected sexual contacts after six months (Witte et al., Citation2015).
The Suubi project targeted HIV-orphaned and out-of-school youth in Uganda. Financial education was offered through their primary schools along with sexual and reproductive health education, matched savings, counseling on life skills, school supplies and peer mentoring. After 10 months, treatment groups showed positive effects on self-rated health and sexual risk-taking behavior as well as improved attitudes toward academic performance and education aspirations (Ssewamala, Han, & Neilands, Citation2009a; Ssewamala & Ismayilova, Citation2009b). Later studies showed improved attitudes toward sexual risk for males but not females. Positive effects were also found on youth self-rated mental health (Ssewamala et al., Citation2009a) and depression (Ssewamala, Neilands, Waldfogel, & Ismayilova, Citation2012).
In terms of economic outcomes, Ssewamala et al. (Citation2010) found no difference in the amount that males and females saved. The value placed on savings and confidence in the ability to save decreased after the matched incentives stopped indicating that these initial attitude improvements may not last. There were no changes in savings attitudes or financial literacy and a few significant effects on risk preferences and spending.
The Suubi-Maka project followed a similar intervention but extended the treatment groups over 12 and 24 months to include parents to examine family effects on outcomes, which were mixed. While the treatment group reported increased likelihood of the family having saved money (Karimli, Ssewamala, & Neilands, Citation2014) and an increase in self-reported youth savings (Karimili, Citation2013), later studies showed no significant effect on the reported amounts saved (Jennings et al., Citation2016; Karimli et al., Citation2014) and no significant effect on the use of formal financial institutions (Karimli et al., Citation2014). Savings attitudes were also found to be weakened by the number of children in the family and significantly affected by family relations, family finance, caregivers’ gender, adolescent’s gender and educational aspirations (Karimili, Citation2013). This study seems to indicate that household conditions may affect individual outcomes for youth. HIV preventative attitudes improved as well as attitudes toward family saving, purchases and vocational training (Jennings et al., Citation2016).
As the evidence map shows, the quality of the evidence for plural education and supports was mixed. Two studies were not validated. Two of the SUUBI studies rated quite low in terms of quality because of the sample size and reliability issues. Eight of 10 studies related to the SUUBI programs.
Plural education with self-efficacy supports
Five plural interventions offered financial and sexual reproductive health education with self-efficacy supports and showed positive effects on HIV and self-efficacy-related outcomes. All were implemented through groups or clubs often with peer or trusted adult counseling and personal development supports. Unfortunately, these components were not isolated for analysis of effects on outcomes.
One intervention focused on female youth orphans in Zimbabwe. Financial and health education, vocational training and micro-grants were offered to treatment participants where the control arm was a plural intervention. Positive outcomes included lower risk of transactional sex, higher likelihood of condom use, fewer unintended pregnancies reported, reduced food insecurity and an improved economic situation compared to the baseline (Dunbar et al., Citation2014).
One intervention took place in community clubs in rural Uganda with adolescent girls, the majority of whom were in school. They mixed financial education with sexual and reproductive health education and negotiation skills. There was significant improvement in HIV and pregnancy-related knowledge, behaviors after 4 years. Sex against their will dropped 26%; early marriage and cohabitation fell by 58%; teen pregnancy fell by 26% (Bandiera et al., Citation2015). In terms of financial or economic outcomes, results were mixed. An earlier study showed no increased likelihood that treatment participants would engage in income-generating activities (Bandiera et al., Citation2012) but a later study showed an increased likelihood mainly driven by increased participation in self-employment (Bandiera et al., Citation2015).
An intervention in Ethiopia targeted out-of-school girls and youth in slum areas. Supports included HIV awareness training, counseling and testing, self-esteem, gender and power, basic literacy and financial education. The control arm had no intervention. This intervention showed positive effects on HIV related outcomes after 30 months. Girls in the treatment site were twice as likely to score highly on HIV knowledge questions, know where to obtain voluntary counseling and testing and also more likely to want to be tested. In terms of self-efficacy, girls in the treatment site were more than twice likely to report social support (Erulkar, Ferede, Girma, & Ambelu, Citation2013).
Another intervention aimed to build internal and external assets in vulnerable girls and youth in Bangladesh. Three treatment arms were offered: one health education and school supports; one plural adding financial education and one a cooking oil supplement for delayed marriage. The first showed a significant increase in constructive use of time while the plural intervention showed the largest increase in positive values. External assets overall showed the most significant increases across the treatments. The addition of cooking oil showed a smaller gain in assets (Scales et al., Citation2013). Unfortunately, the study did not examine health outcomes.
The last plural intervention was implemented in India where adolescent females participated with other women in self-help groups. While this intervention did not offer savings services, the self-help groups rotate savings and loans. The treatment groups were provided an array of supports including learning games, health education focused on sanitation, body and HIV protection as well as financial education and negotiating power. The treatment groups showed significant gains in HIV knowledge including awareness that condoms prevent HIV and sexually transmitted infections. They also reported self-efficacy for HIV prevention and confirmed use of clean needles. There were positive savings outcomes as well where the girls reported significantly higher motivation to save money and to be more likely to have a plan to save after one year (Spielberg et al., Citation2013).
The quality of the evidence for plural education with self-efficacy supports is mixed. Two studies were not validated. In addition, the evidence in three of the studies was weakened by the sample size andconfidence intervals.
Discussion
A number of lessons can be learned from the selected studies on the mix of financial and plural education and supports that led to positive health and economic outcomes for vulnerable youth and children. Both financial and plural education interventions showed at least one positive outcome, mostly in Sub-Saharan Africa where HIV is most prevalent.
The two financial education interventions showed mixed results, with positive effects on spending, risk preferences and savings behavior (Berry et al., Citation2015) and mixed results on financial literacy and the role that savings plays (Jamison et al., Citation2014). Three interventions that separated financial education from health education in treatment showed the potential value-added of financial education for HIV and self-efficacy related outcomes (Dunbar et al., Citation2014; Scales et al., Citation2013; Witte et al., Citation2015). There is some evidence in support of asset theory; that is, linking financial education to asset-building and financial literacy for vulnerable youth, but outcome pathways are inconclusive.
Four plural education interventions, with savings and self-efficacy supports, showed more positive outcomes than financial and health education approaches on their own. Observed improvements included increased HIV related knowledge, attitudes, reduced sexual risk-taking behavior and improved self-efficacy. While positive effects were also observed related to increased savings and improved attitudes toward saving, the relationship between the economic and health components was less clear. Self-efficacy supports such as counseling, mentoring, negotiation and self-esteem training also were present with positive outcomes but not isolated in analysis. Studies did not increase understanding of the relationship between positive HIV and self-efficacy outcomes. Five plural interventions that did not offer finance still showed positive effects on HIV and self-efficacy related outcomes warranting more research to understand the value-added of financial services in the mix.
In terms of context and target population, disaggregated impact evidence is thin. There is some evidence that household level conditions and outcomes can affect child and youth outcomes positively. Individual studies found differences in outcomes by marital status, gendered savings attitudes, sexual risk taking and type of orphan. Conditional factors such as the setting of the education, whether community or school, if a trusted adult offered counseling were not analyzed.
Conclusion
This systematic review supports the emerging evidence that plural approaches (financial education combined with sexual and reproductive health education and self-efficacy supports) may reduce HIV vulnerabilities in vulnerable children and youth in LMIC. The team came from health, finance, academe and HIV organizing so was able to provide a grounded analysis of the outcome evidence and components. Nevertheless, the evidence is scant and quality mixed. The strength of these findings is limited by the few studies available, largely self-reported from limited settings and all secondary, not raw data. Furthermore, length, number of waves and quality of the studies made comparisons and clustering of pathways difficult. Studies used varied outcome variables and treatment formats.
While positive effects have been shown across a number of studies, it is often not clear which components are effective at producing favorable outcomes. For health and economic practitioners and evaluators, much greater attention needs to be paid to disaggregating program components. In particular, it would be helpful to disaggregate the target group (by age, gender, type of orphan), program components (whether school or community setting, separation of education components from self-efficacy supports), and examine individual vs family conditions for positive outcomes.
There are policy and theoretical implications too. Asset theory pathways linking economic strengthening to reduced vulnerabilities are not as clear as may be commonly assumed for vulnerable children and youth. Self-efficacy, both as a condition and as a set of outcomes, seems important but details are unclear. Literature and emerging evidence support that negotiating power and the ability to retain assets are linked to personal and structural elements such as gendered social norms. In other words, self-efficacy is more complex than personal well-being. More research is needed on the role of plural education, self-efficacy supports and conditional factors in these pathways.
Correction Statement
This article has been republished with minor changes. These changes do not impact the academic content of the article.
Acknowledgments
This systematic review was produced for FHI 360 by Sisters Ink., a global consulting and peer coaching group of self-employed women working on issues of women’s economic empowerment. The review team included Nanci Lee (editor), Dr. Sabrina Beeler Stücklin, Dr. Patricia López Rodríguez, Meryem Faris and Ida Mukaka.
The team is grateful for detailed review and inputs from Jessica Bachay, David Myhre and Michael Ferguson of the ASPIRES Project, FHI 360.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
Notes
1. Children and youth are defined as those between 0-24 years by UN and UNICEF definitions (http://www.un.org/esa/socdev/documents/youth/fact-sheets/youth-definition.pdf, https://www.unicef.org/crc/files/Guiding_Principles.pdf, retrieved on 15 November 2017).
2. OVC, as defined by PEPFAR (U.S. President’s Emergency Plan for AIDS Relief), are children aged 0-17 years who have lost a parent to HIV/AIDS, who are otherwise directly affected by the disease, or who live in areas of high HIV prevalence and may be vulnerable to the disease or its socioeconomic effect (PEPFAR, Citation2012).
3. As of 1 July 2016, low-income economies are defined as those with a GNI per capita, calculated using the World Bank Atlas method, of $1,025 or less in 2015; lower middle-income economies are those with a GNI per capita between $1,026 and $4,035.
4. Two academics, one practitioner in the health sector, one practitioner in the finance sector, one HIV organizer.
5. Web of Science, Cochrane Library, EconLit, Popline, PubMed, Economia y negocios.
6. Aflatoun, Global Partnership for Financial Inclusion and Alliance for Financial Inclusion (AFI), 3ie, MEDA, MasterCard Foundation, United Nations Capital Development Foundation-YouthStart, World Health Organization, Microfinance Opportunities, Women’s World Banking, International Labor Organisation, Freedom from Hunger, Save the children – Youthsave, FHI360, Population Council, Microsave, Child and Youth Finance International, International Gateway for Financial Education (OECD), Google Scholar, UNDP, World Bank, Sultan Qabus University of Oman, Jordanian Public University Library, King Faysal University-Saudi.
7. The team searched back to 1990 due to limited studies that met criteria.
8. Two programs included adults. The Indian program focused on self-help groups that included adolescent girls with their mothers but did not target them. Another program focused on sex workers at least 18 years old. Sixteen of the studies focused on girls or women vulnerable to HIV, gender-based violence including early marriage, trafficking.
9. Reasons for exclusion were: no use of controls, high-income country, evidence of selection bias, outcomes focused only on teachers rather than students; qualitative studies with no controls or other rigor issues such as obvious or reported issues with selection bias, contamination or spillover risks; evaluation too soon after end of program, vocational entrepreneurship training without clear financial education; protocol or base-line assessments; too little information on which to analyze study.
10. CMO is a realist inquiry that attempts to understand why a particular program or policy works sometimes and not others. In contrast to a results chain, this approach explores multiple pathways (van der Knaap et al., Citation2008). van der Knaap et al. (Citation2008) discuss a systematic review process which combines Campbell standards of systematic review with the CMO principle as a basis for aggregation.
1 Each parameter of quality was associated with three key questions which were rated either weak (1), moderate (2), strong (3) or not enough information (NA). The total possible score was 36 or less if elements were missing such as curriculum to assess pedagogical rigor. The score was then turned into a % out of 100.
References
- Bandiera, O., Buehren, N., Burgess, R., Goldstein, M., Gulesci, S., Rasul, I., & Sulaiman, M. (2012). Empowering adolescent girls: Evidence from a randomized control trial in Uganda. Washington, DC: World Bank.
- Bandiera, O., Buehren, N., Burgess, R., Goldstein, M., Gulesci, S., Rasul, I., & Sulaimany, M. (2015). Women’s empowerment in action: Evidence from a randomized control trial in Africa. Washington, DC: World Bank.
- Bandura, A. (1977). Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review, 84(2), 191–215.
- Bandura, A. (1994). Self-efficacy. In V. S. Ramachaudran (Ed..), Encyclopedia of human behavior ((Reprinted in H. Friedman [Ed.], (1998). Encyclopedia of mental health. San Diego: Academic Press). https://www.uky.edu/~eushe2/Bandura/Bandura1994EHB.pdf, Vol. 4, pp. 71–81). New York: Academic Press.
- Berry, J., Karlan, D., & Pradhan, M. (2015). The impact of financial education for youth in Ghana. Amsterdam, The Netherlands: Tinbergen Institute.
- Child and Youth Finance International [CYFI]. (2012). Children and youth as economic citizens:Review of research on financial capability, financial inclusion, and financial education (Research Working Group Report). Amsterdam, The Netherlands: CYFI.
- Cui, R. R., Lee, R., Thirumurthy, H., Muessig, K. E., & Tucker, J. D. (2013). Microenterprise development interventions for sexual risk reduction: A systematic review. AIDS and Behavior, 17(9), 2864–2877.
- De Guzman, A. (2001). Reducing social vulnerability to HIV/AIDS: Models of care and their impact in resource-poor settings. AIDS Care, 13(5), 663–675.
- Department for International Development [DFID]. (2014). Assessing the strength of evidence. London, UK: DFID.
- Dunbar, M. S., Dufour, M. S. K., Lambdin, B., Mudekunye-Mahaka, I., Nhamo, D., & Padian, N. S. (2014). The SHAZ! project: Results from a pilot randomized trial of a structural intervention to prevent HIV among adolescent women in Zimbabwe. PLoS One, 9(11), e113621.
- Dworkin, S. L., & Blankenship, K. (2009). Microfinance and HIV/AIDS prevention: Assessing its promise and limitations. AIDS and Behavior, 13(3), 462–469.
- Erulkar, A., Ferede, A., Girma, W., & Ambelu, W. (2013). Evaluation of “Biruh Tesfa” (Bright Future) program for vulnerable girls in Ethiopia. Vulnerable Children and Youth Studies, 8(2), 182–192.
- Fleischman, J., & Peck, K. (2015). Addressing HIV risk in adolescent girls and young women. Washington, DC: Center for Strategic and International Studies.
- International Center for Research on Women [ICRW]. (2010). What role can economic empowerment strategies play in reducing HIV risk and vulnerability among girls and young women? Washington, DC: International Center for Research on Women.
- Jamison, J. C., Karlan, D., & Zinman, J. (2014). Financial education and access to savings accounts: Complements or substitutes? Evidence from Ugandan youth clubs (National Bureau of Economic Research Working Paper No. 20135, JEL No. D12,D91,O12). Cambridge, MA: National Bureau of Economic Research.
- Jennings, L., Ssewamala, F. M., & Nabunya, P. (2016). Effect of savings-led economic empowerment on HIV preventive practices among orphaned adolescents in rural Uganda: Results from the Suubi-Maka randomized experiment. AIDS Care, 28(3), 273–282.
- Kalamar, A. M., Bayer, A. M., & Hindin, M. J. (2016). Interventions to prevent sexually transmitted infections, including HIV, among young people in low- and middle-income countries: A systematic review of the published and gray literature. Journal of Adolescent Health, 59(3), S22–S31.
- Karimili, L. (2013). Financial asset accumulation by poor adolescents participating in child savings accounts in low resource communities in Uganda. New York, NY: Columbia University.
- Karimli, L., Ssewamala, F. M., & Neilands, T. B. (2014). Poor families striving to save in matched children‘s savings accounts: Findings from a randomized experimental design in Uganda. Social Service Review, 88(4), 658–694.
- Kennedy, C. E., Fonner, V. A., O‘Reilly, K. R., & Sweat, M. D. (2014). A systematic review of income generation interventions, including microfinance and vocational skills training, for HIV prevention. AIDS Care, 26(6), 659–673.
- Kim, J., Pronyk, P., Barnett, T., & Watts, C. (2008). Exploring the role of economic empowerment in HIV prevention. South Africa: SEF. Retrieved from http://www.sef.co.za/
- Orton, L., Pennington, A., Nayak, S., Sowden, A., White, M., & Whitehead, M. (2016). Group-based microfinance for collective empowerment: A systematic review of health impacts. Bulletin of the World Health Organization, 94(9), 694–704.
- Plourde, K. F., Fischer, S., Cunningham, J., Brady, K., & McCarraher, D. R. (2016). Improving the paradigm of approaches to adolescent sexual and reproductive health. Reproductive Health, 13(1), 72.
- President’s Emergency Plan for AIDS Relief [PEPFAR]. 2012. Guidance for orphans and vulnerable children programming. Washington, DC: U.S. President’s Emergency Plan for AIDS Relief. Retrieved from http://www.pepfar.gov/documents/organization/195702.pdf
- Pronyk, P. M., Kim, J. C., Abramsky, T., Phetla, G., Hargreaves, J. R., Morison, L. A., … Porter, J. D. (2008). A combined microfinance and training intervention can reduce HIV risk behaviour in young female participants. Aids, 22(13), 1659–1665.
- Scales, P. C., Benson, P. L., Dershem, L., Fraher, K., Makonnen, R., Nazneen, S., … Titus, S. (2013). Building developmental assets to empower adolescent girls in rural Bangladesh: Evaluation of project kishoree kontha. Journal of Research on Adolescence, 23(1), 171–184.
- Shephard, D.D., & Contreras, J. Meuris, J., te Kaat, A., Bailey, S., Custers, A., Spencer, N. (2017). Beyond Financial Literacy: The Psychological Dimensions of Financial Capability. Think Forward Initiative. Retrieved from https://8b109582833d5c2e19d5-b8e01d380645fda9dfa9d12a21c5e59a.ssl.cf3.rackcdn.com/downloads/Beyond-financial-literacy_The-psychological-dimensions-of-financial-capability_Technical-report.pdf
- Spielberg, F., Crookston, B. T., Chanani, S., Kim, J., Kline, S., & Gray, B. L. (2013). Leveraging microfinance to impact HIV and financial behaviors among adolescents and their mothers in West Bengal: A cluster randomized trial. International Journal of Adolescent Medicine and Health, 25(2), 157–166.
- Ssewamala, F. M., Han, C. K., & Neilands, T. B. (2009). Asset ownership and health and mental health functioning among AIDS-orphaned adolescents: Findings from a randomized clinical trial in rural Uganda. Social Science & Medicine, 69(2), 191–198.
- Ssewamala, F. M., & Ismayilova, L. (2009). Integrating children‘s savings accounts in the care and support of orphaned adolescents in rural Uganda. Social Service Review, 83(3), 453–472.
- Ssewamala, F. M., Ismayilova, L., McKay, M., Sperber, E., Bannon, W., Jr., & Alicea, S. (2010). Gender and the effects of an economic empowerment program on attitudes toward sexual risk-taking among AIDS-orphaned adolescent youth in Uganda. Journal of Adolescent Health, 46(4), 372–378.
- Ssewamala, F. M., Neilands, T. B., Waldfogel, J., & Ismayilova, L. (2012). The impact of a comprehensive microfinance intervention on depression levels of AIDS-orphaned children in Uganda. Journal of Adolescent Health, 50(4), 346–352.
- UNAIDS. (2015). Update: Active involvement of young people is key to ending the AIDS epidemic by 2030. Geneva, Switzerland: Author.
- UNAIDS. (2016). Global Aids Update 2016. Geneva, Switzerland: Author.
- UNAIDS & The African Union. (2015). Empowerment young women and adolescent girls: Fast-tracking the end of the aids epidemic in Africa. Geneva, Switzerland: UNAIDS and the African Union.
- UNICEF. (2016). State of the world’s children. New York, NY: Author.
- van der Knaap, L. M., Leeuw, F. L., Bogaerts, S., & Nijssen, L. T. J. (2008). Combining campbell standards and the realist evaluation approach: The best of two worlds? American Journal of Evaluation, 29(1), 48–57.
- Witte, S. S., Aira, T., Tsai, L. C., Riedel, M., Offringa, R., Chang, M., … Ssewamala, F. (2015). Efficacy of a savings-led microfinance intervention to reduce sexual risk for HIV among women engaged in sex work: A randomized clinical trial. American Journal of Public Health, 105(3), e95–e102.
- World Health Organization [WHO]. (2014). Health for the world’s adolescents: A second chance in the second decade. Geneva: World Health Organization.
- YouthPower. (2017). A systematic review of positive youth development programs in low-and middle-income countries. Washington, DC: Author.
Appendix 1:
Search terms
Web of Science
“financial education”; financ* literacy; (“financ* education” OR “financ* literacy” OR “financ* training” OR “financ* capabilities” OR “product awareness training” OR (“consumer protection” AND micro*) OR “microenterprise develop*” OR “entrepren* training “ OR “entrepren* development” OR “economic strengthening”) AND ((influenc* OR effect OR develop* OR empower* OR improv* OR test* OR *experiment* OR evidenc* OR grow* OR matter* OR outcome OR impact OR result* OR health OR financ* behaviour OR HIV OR AIDS OR economic* strengthening OR behaviour OR power) OR (HIV OR AIDS OR (HIV AND (diagnosis OR “risk population” OR youth OR gender OR prevention)) OR OVC OR (“sex workers”) OR “commercial sex” OR “transactional sex”)
Cochrane Library
EconLit
“financ* education” OR “financ* training” OR “financ* literacy” OR “financ* capabilit*” OR “entrepr* develop*” OR “economic strengthening” AND influence or impact or effect or affect or develop or enhance or promote OR grow* OR empower* OR improv* OR test* OR experiment* OR evidence OR matter OR outcome OR result* OR health OR “financ* behavior” OR power OR empower*
Popline
“financial literacy” OR “financial training” OR “financial education” OR “financial capability” OR “financial capabilities” OR “financial behavior” OR “financial behaviour” OR “economic strengthening
PubMed
“financial education”[All Fields] OR “financial literacy”[All Fields] OR (inancial[All Fields] AND (“education”[Subheading] OR “education”[All Fields] OR “training”[All Fields] OR “education”[MeSH Terms] OR “training”[All Fields])) OR “micro finance” OR microfinance OR “micro credit” OR microcredit OR microcredit
Economia y Negocios
Educación Financiera AND evaluación de impacto OR PSP OR pruebas controladas por aleatoriedad OR pruebas controladas por aleatoriedad por grupos OR regresión discontinua OR Educación Financiera Educación AND pobre Educación Financiera AND remota OR Financiera OR Educación Financiera AND niños AND en la parte más baja de la desigualdad OR Educación Financiera AND población vulnerable OR Educación Financiera AND jóvenes R en los últimos deciles de la distribución Entrenamiento financiero AND America Latina AND Sida, VIH población infectada AND América Latina
Grey Literature (English)
“financial education” OR “financial literacy” OR “financial capability” OR “economic strengthening”
OR “microfinance” OR “microenterprise” AND “youth” OR “children” OR “HIV youth” OR “AIDS”
Grey Literature (Spanish)\
Financial Education AND Latin America OR Argentina OR Bolivia OR
Brazil OR Chile OR Colombia OR Costa Rica OR Cuba OR Ecuador OR El Salvador OR
Guatemala OR Haití OR Honduras OR Jamaica OR México OR Nicaragua OR
Panamá OR Paraguay OR Perú OR República Dominicana OR Trinidad y Tobago OR
Uruguay OR Venezuela Educación Financiera AND America Latina
Educación Financiera AND evaluación de impacto OR PSP OR pruebas controladas por aleatoriedad OR pruebas controladas por aleatoriedad por grupos OR regresión discontinua OR Educación Financiera Educación AND pobre Educación Financiera AND remota OR Financiera OR Educación Financiera AND niños AND en la parte más baja de la desigualdad OR Educación Financiera AND población vulnerable OR Educación Financiera AND jóvenes R en los últimos deciles de la distribución Entrenamiento financiero AND America Latina AND Sida, VIH población infectada AND América Latina
Grey Literature (Arabic)
Financial Education : التربية المالية
Financial Literacy: محو الأمية المالية
Financial Capability: كفاءة مالية
Children أطفال
HIV Youth
شباب نقص المناعة
Youth شباب
“تربية مالية” OR “محو الأمية المالية” OR “كفاءة مالية” AND "شباب” OR "أطفال” OR “شباب نقص المناعة"
شباب مصاب بداء نقص المناعة
Youth having HIV/AIDS
Appendix 2:
Quality Rating Tool for Eligible Studies
Each study was scored on a scale from zero to 100, with narrative assessment to back the scoring. The following is a description of the elements of quality that were assessed:Footnote1
Conceptual rigor examined the clarity and coherence of the theory of change, clear measurement of changes in outcomes and evidence of behavioral outcomes including how they were measured.
Methodological rigor used Department for International Development, UK (DFID)’s Quality of Evidence Framework (2014) to assess key principles of high quality research.
Internal validity. Appropriateness of methodology to research questions. Minimization of risk and bias errors including incomplete data, sampling and controls. These include selection bias, randomization errors, problems of endogeneity.
External validity. Generalizability. Can results from one setting apply to another? This should be asked of all research projects for which there are multiple countries. Also considered are coherence and comparability questions.
Reliability. Appropriateness of methodology to what is being assessed. For example, Randomized Control Trials (RCTs) are best to address causal, observable phenomenon. Also, methods and instruments that will ensure consistent results across tools, contexts etc.
Cogency. High quality studies will provide a clear logical thread that runs through the entire paper. High quality studies will guide the reader and avoid making claims in their conclusions that are not clearly backed up by the data and findings. They also identify limitations of the work and alternative interpretations of analysis.The review team included questions related to how well the methodology matched the research questions and how robust the impact methodology was in terms of rendering limitations explicit. Because methodological rigor is so foundational to a high-quality study, the review team gave this area an extra weighting by a factor of five. This weighting was tested across the assessments. As intended, high rating in areas of pedagogical rigor and relevance did not falsely distort the rigor of the overall program. If methodological rigor was a serious problem, overall the financial education program and its impact evaluation would fall below a score of 60 out of 100.
(3) Relevance examined demonstration of tailoring to the audience, analysis of the target group in the context and clear gender awareness built into design.
(4) Pedagogical rigor examined the extent to which curriculum was learner-centered and tailored to vulnerable children and youth, including safe and accessible outreach or delivery mechanisms.
The following rating tool was used to assess the quality of the impact evaluations.
Quality Rating Tool for Financial Education Interventions
Financial Education Intervention (Country):
Corresponding Study (Authors, year):
Reviewer:
Appendix 3:
Evidence table
Financial education intervention impact studies and outcome effects on vulnerable youth and OVC.
Appendix 4:
Odds Ratio Analysis