
ABSTRACT
Orphaned and vulnerable children (OVC) are not only affected by, but also rendered at-risk of, HIV due to overlapping deficits in protective assets, from school to household financial security. Drawing from a protective deficit framework, this study examines correlates of sexual risk – including multiple sexual partnerships, unprotected sex, and age at sexual debut – among OVC aged 13–17 years in Zambia. In May-October 2016, a two-stage stratified random sampling design was used to recruit OVC and their adult caregivers (N = 2,034) in four provinces. OVC-caregiver dyads completed a structured interview addressing household characteristics, protective assets (i.e. finances, schooling, and nutrition), and general health and wellbeing. Associations of factors derived from the multi-component protective deficits framework were examined using multivariable ordered logistic regression, comparing sexually inexperienced OVC to those with a sexual debut and reporting ≥1 sexual behavior(s). A sub-analysis of older (ages 15–17) OVC identified correlates of early (before age 15) and later (at or after age 15) sexual debut using multinomial logistic regression. Among 735 OVC aged 13–17, 14% reported a sexual debut, among whom 14% and 22% reported 2+ past-year partners and non-condom last sex, respectively. Older age (Adjusted Odds Ratio [aOR] = 2.08, 95% Confidence Interval [CI] 1.32–3.27), male sex (aOR = 1.90, CI 1.22–2.96), not having a birth certificate (aOR = 2.05, CI 1.03–4.09), out-of-school status (aOR = 2.63, CI 1.66–4.16), and non-household labor (aOR = 1.84, CI 1.01–3.38) were significantly associated with higher sexual risk. Male sex was the only factor significantly associated with early sexual debut in multivariable analysis. Sexual risk-reduction strategies require age- and sex-specific differentiation and should be prioritized for OVC in financially distressed households.
Introduction
Despite substantial gains in prevention and treatment over the last decade, the HIV epidemic presents unyielding health, financial, and social challenges for households and communities in Zambia. One million Zambians, roughly 12% of the adult population, are living with HIV (Zambia Ministry of Health, Citation2019). While steady increases in antiretroviral therapy (ART) coverage have improved health outcomes and led to noteworthy declines in population HIV incidence (R. R. Hayes et al., Citation2017; R. J. R. J. Hayes et al., Citation2019), an irreversible consequence of the epidemic’s duration and magnitude is sizeable numbers (~600,000) of HIV-orphaned children (National HIV/AIDS/STI/TB Council, Citation2012).
Orphaned and vulnerable children (OVC) are not only affected by, but also rendered at-risk of, HIV and other challenges due to overlapping, mutually reinforcing social and structural forces. Parental death is a traumatic event accompanied by dramatic changes in household structure and a child’s broader care environment, including newly appointed caregivers (Embleton et al., Citation2014; Nyambedha et al., Citation2003). The loss of a parental income source, or unplanned adoption of new dependents, increases financial strain on a household, rendering basic expenses on food, health, and education unaffordable (Kasedde et al., Citation2014; Lee et al., Citation2014; Olanrewaju et al., Citation2015; Rivers et al., Citation2010). Untethered to sources of parental stimulation and psychosocial support in schools and in the household, OVC may experience re-traumatizing neglect and distress that can impair decision-making and drive sexual experimentation to cope with these emotional and material deficits (Cluver et al., Citation2007, Citation2011; Gray et al., Citation2016; Thurman et al., Citation2006; Whetten et al., Citation2011). This subsequently exposes OVC to harms like earlier and non-condom sex, as well as sexual coercion (Gray et al., Citation2016; Operario et al., Citation2011). Deficits in protective assets, therefore, act synergistically in shaping the HIV risk environment for OVC.
While the contribution of instrumental and material scarcity to youth HIV risk is well-established (Dellar et al., Citation2015; Mathur et al., Citation2020; Pascoe et al., Citation2015; Pettifor et al., Citation2018), the mechanisms through which deficits in protective assets shape OVC sexual behavior is less understood, particularly in the Zambian context. A psychometric assessment of Zambian OVC’s HIV risk found prevalent (50%) sexual risk behaviors (Kane et al., Citation2018), but did not identify factors associated with specific sexual outcomes. Other studies of youth sexual behavior in Zambia have similarly reported suboptimal trends in condom use and early sex (Kayeyi et al., Citation2013; Ndongmo et al., Citation2017), but these results may have limited generalizability to OVC.
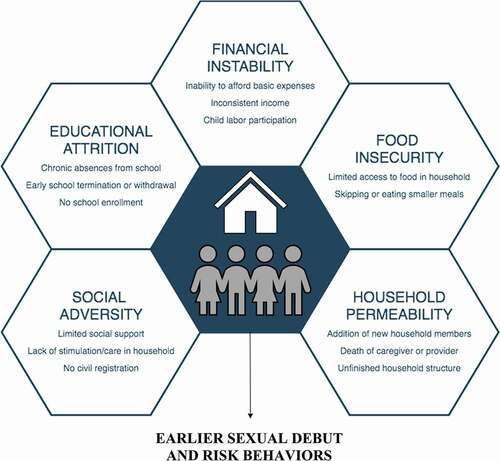
This study examines correlates of sexual risk – including multiple sexual partnerships, unprotected sex, and age at sexual debut – among OVC aged 13–17 years in Zambia. Drawing from a protective deficits framework (see ), which situates child and adolescent sexual behavior at the intersection of overlapping psychosocial and material scarcities, this study identifies and quantifies the contribution of co-occurring, multidimensional factors to OVC sexual behavior. Findings will help elucidate strategies for tailoring and differentiating HIV prevention programming for OVC with distinct HIV vulnerabilities and sexual risk profiles.
Figure 1. Protective deficits framework for sexual behavior among orphaned and vulnerable children
Materials and methods
Study setting and population
Data are derived from a benchmark survey of households supported by the Zambia Family (ZAMFAM) project, funded by the U.S. Agency for International Development (USAID) via the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR). ZAMFAM is a five-year project (2015–2020) implemented in four provinces by two community-based partners: Development Aid from People to People (DAPP) and the Expanded Church Response (ECR) Trust. The project’s primary objective is to strengthen health and resilience of OVC, young people living with HIV, and their caregivers through a multi-sectoral service package, including: 1) combination socioeconomic interventions (e.g. village loans and savings groups), 2) food subsidies, 3) psychosocial support, 4) parenting workshops, and 5) community-based HIV care and treatment support (Mbizvo et al., Citation2018; Project SOAR, Citation2019).
Prior to survey implementation, DAPP and ECR Trust enumerated households receiving ZAMFAM services in project catchment areas. Eligible study participants resided in households supported by the ZAMFAM project and included adults (18+ years) who served as primary caregivers for OVC 17 years or younger. ZAMFAM-eligible OVC, conforming to the Zambian government’s classification, are children younger than 18 living in adverse conditions, including: HIV-positive status, disability, chronic illness, or household environments engendering significant physical or emotional stress threatening healthy development (Mbizvo et al., Citation2018).
Recruitment and sampling
A two-stage stratified random sampling procedure was used to recruit ZAMFAM-beneficiary households in four provinces: 1) Central and Southern (DAPP implementing areas) and 2) Copperbelt and Lusaka (ECR Trust implementing areas). Survey implementation occurred at two distinct time points in each provincial cluster: between May and July 2016 in Central and Southern (approximately one-year after ZAMFAM project introduction) and between September and October 2016 in Copperbelt and Lusaka (immediately following project introduction).
After enumeration of eligible households across 131 wards in the sampling frame, fifty wards were randomly selected proportional to the OVC beneficiary population size. Stratification by residence type ensured a representative sample of urban and rural wards was selected across provincial clusters. Thirty-five households were selected in each ward through systematic random sampling with replacement. Among 2,462 households approached across wards, 2,034 (82%) were enrolled.
OVC aged 0–9 years and 10–17 years, respectively, as well as their primary caregiver were eligible for participation. In accordance with PEPFAR OVC survey guidelines, random selection was used to enroll one OVC in households where more than one OVC per age band was present (Office of the Global AIDS Coordinator, Citation2017). In households with OVC aged 0–9 and 10–17, both OVC were eligible for participation.
Data collection
Caregivers and OVC in each household completed an enumerator-administered, tablet-based questionnaire adapted from the Child, Caregiver and Household Well-being Survey Tools for Orphaned and Vulnerable Children (MEASURE Evaluation, Citation2013). Caregivers answered questions pertaining to household characteristics, finances, schooling, hunger, and their general health and wellbeing. OVC aged 10–17 were interviewed directly (without a response proxy) with an age-appropriate survey instrument.
Measures
The primary outcomes of this study were lifetime and past-year sexual behaviors, obtained via self-report from OVC aged 13–17. A categorical sexual debut variable was constructed from responses to two survey items gauging whether the participant ever had sex and, if so, at what age. The variable compared OVC who report early sexual debut (before age 15), to those who report first sex at or after age 15 (later sexual debut), to those who have never had sex. An ordinal sexual risk variable was also constructed using responses to three questions assessing sexual debut, multiple (two or more) sexual partners in the past year, and condom use at last sex. The variable was coded as follows: 0 – not sexually experienced (‘low/no risk’); 1 – sexually experienced but reports neither multiple past-year partners nor unprotected last sex (‘some risk’); and 2 – sexually experienced and reports multiple past-year partners and/or unprotected last sex (‘higher risk’).
Selection of explanatory variables was guided by the protective deficits framework for HIV risk (see ). Operationalization procedures for explanatory covariates derived from the study’s guiding theoretical framework are described in . Socio-demographic covariates included age, sex, residence type, and province.
Table 1. Operationalization of dichotomous explanatory variables included in analysis, by corresponding domain in the protective deficits framework
Analysis
Data were managed and analyzed in Stata 15.1 (StataCorp®, College Station, TX). Descriptive sample statistics were calculated and compared across sex using design-based Pearson’s chi-square tests of association. Multivariable ordered logistic regression modeled associations of demographic and protective deficit factors with ordinal sexual risk. Covariates were introduced into multivariable analysis in stepwise fashion, including only those that were significantly (p < 0.05) associated with the outcome in bivariate analysis. A post-estimation Brant test was performed to verify the specified model supporting the proportional odds assumption of ordered logistic regression (Brant, Citation1990). Subgroup analyses were subsequently implemented to compare effect estimates in models stratified by sex (see Supplementary ).
A sub-analysis restricted to older OVC (ages 15–17) was conducted to identify factors associated with age at first sex. Multinomial logistic regression compared associations of the aforementioned covariates with OVC reporting early (before age 15) and later (at or after age 15) sexual debut, respectively, with sexually inexperienced OVC served as the universal reference group in analysis. Only covariates significantly (p < 0.05) associated with either early or later sexual debut in bivariate analysis were introduced into multivariable analysis.
Variance Inflation Factor (VIF) scores were inspected for multicollinearity and, when indicated, guided removal of covariates from the multivariable models until acceptable thresholds of covariate saturation (mean VIF < 5) were achieved (Craney & Surles, Citation2002). Linearized standard errors produced robust estimates sensitive to hierarchical clustering and stratification (by urban and rural residence) as well as the probability of selection and non-response.
Ethics
The Population Council Institutional Review Board (New York, NY, USA) and ERES Converge (Lusaka, Zambia) reviewed and approved the current study. The National Health Research Authority (Lusaka, Zambia), under the Zambian Ministry of Health, and the Ministry of Community Development and Social Services (Lusaka, Zambia) administratively approved the study. Caregivers provided written informed consent prior to survey administration. Assent and caregiver written consent was obtained for all participants aged 10–17.
Results
Among 2,034 households enrolled, 742 (36.5%) had an eligible OVC aged 13–17. Seven had incomplete or missing responses to sexual behavior items and were excluded from analysis. presents sex-stratified descriptive statistics of the analytic sample (N = 735). The mean age was 14.7 years (Std. Dev: 1.3). Age and sex were evenly distributed in the sample. A significantly higher proportion of male OVC were older (15–17 years) than female OVC (59.7% vs. 47.0%, p < 0.001). Most OVC resided in urban/mixed wards (68.3%), and the largest proportion were sampled from Central Province (38.5%).
Table 2. Descriptive statistics (%) of orphaned and vulnerable children aged 13–17 years in Zambia Family project catchment areas, by sex (N = 735)
One hundred OVC (13.6%) reported ever having sex, a majority of whom reported their first sex occurred before age 15 (68.0%). Among sexually debuted OVC, 14.0% reported multiple past-year sex partners, and 21.0% denied using condoms during their most recent sexual encounter. displays sexual behaviors among sexually experienced OVC by sex and residence. Male OVC were more likely to report early sexual debut (73.5% vs. 56.3%, p = 0.074) and multiple past-year sex partners (17.6% vs. 6.3%, p = 0.148), while female OVC reported unprotected last sex with greater frequency (25.0% vs. 19.1%, p = 0.485). OVC in rural settings were more likely to report early sexual debut (78.4% vs. 61.9%, p = 0.057), unprotected last sex (35.1% vs. 12.7%, p = 0.008), and multiple past-year sex partners (27.0% vs. 6.3%, p = 0.007).
Figure 2. Proportion of sexually debuted orphaned and vulnerable children aged 13–17 who report sexual risk behaviors (early sexual debut [before age 15], unprotected last sex, and multiple past-year sex partners), by sex and residence (N = 100)
![Figure 2. Proportion of sexually debuted orphaned and vulnerable children aged 13–17 who report sexual risk behaviors (early sexual debut [before age 15], unprotected last sex, and multiple past-year sex partners), by sex and residence (N = 100)](/cms/asset/48ddd1f0-e3f2-46b5-a341-3ef482acff6a/rvch_a_1975858_f0002_oc.jpg)
OVC reported overlapping deficits in protective assets (see ). Most did not have birth certificates (79.6%) and had caregivers who met their child’s needs worse than other households (63.7%). One-fourth (24.8%) had caregivers who were too sick to participate in daily activities in the previous month. A majority of OVC never discussed sex (86.0%) or HIV/AIDS (85.9%) with a caregiver. Male OVC were significantly more likely than female OVC to have never discussed sex with their caregiver (91.0% vs. 81.0%, p < 0.001).
Approximately one-fifth (17.7%) of OVC were out-of-school. Among those who had ever attended school, 17.0% had withdrawn. Half of school-enrolled OVC (49.1%) had missed at least three days of school in the past week, a significantly larger proportion of whom were female (52.9% vs. 45.1%, p = 0.036), and 15.1% did not progress in school in the previous academic year. Half of OVC lived in households where caregivers struggled to afford basic expenses, including those for food (55.1%). Most caregivers reported being less financially secure compared to their neighbors (64.2%), a significantly higher proportion of whom were guardians to female OVC (68.5% vs. 59.9%, p = 0.012). As a potential consequence of this economic instability, nearly one-fifth (21.0%) of OVC reported engagement in income-generating activities outside the household, with over twice as many males reporting labor participation (28.9% vs. 13.0%, p < 0.001).
Over three-fourths of caregivers (76.1%) had no food in their homes at least once in the previous month. OVC reported eating a smaller meal than desired (65.6%), skipping a meal (62.3%), and going to bed hungry (51.0%) at least weekly in the past month with alarming frequency. One-fourth (25.0%) spent an entire day and evening without eating at least weekly in the past month. In terms of household permeability, fewer but noteworthy proportions of OVC lived in households where a death occurred (19.9%) or new members were added (27.1%) in the past year. Insufficient shelter protection was observed in 11.6% of households, a significantly larger proportion of which housed male OVC (14.7% vs. 8.4%, p = 0.008).
Heightened sexual risk
presents unadjusted and adjusted proportional odds ratios (OR) from ordered logistic regression, modeling associations between tiered sexual risk and explanatory covariates. An aOR for a three-level (ordinal) sexual risk is a pooled estimate of: 1) the odds of sexual debut plus multiple past-year partners and/or unprotected last sex compared to no sexual debut (‘higher risk’ + ‘some risk’ vs. ‘low/no risk’) with 2) the odds of sexual debut and multiple past-year partners and/or unprotected last sex compared to sexual debut without other risks and no sexual debut (‘higher risk’ vs. ‘some risk’ + ‘low/no risk’). The pooled regression coefficient (i.e. proportional odds ratio) can, therefore, be interpreted as an odds estimate corresponding to heightened, or greater degrees of, sexual risk.
Table 3. Unadjusted and adjusted proportional odds ratios (pOR) of sexual risk behaviors (0 – no sexual debut, 1 – sexual debut only, 2 – sexual debut and unprotected last sex and/or multiple past-year sex partners) derived from ordered logistic regression, by demographic and protective deficit factors, among orphaned and vulnerable children (N = 735)
In multivariable analysis, OVC who were 15–17 years (vs. 13–14: Adjusted OR [aOR] = 2.08, 95% Confidence Interval [CI] 1.32–3.27), were male (aOR = 1.90, CI 1.22–2.96), did not have a birth certificate (aOR = 2.05, CI 1.03–4.09), currently out-of-school (aOR = 2.63, CI: 1.66–4.16), and engaged in income-generating activities (aOR = 1.81, CI 1.01–3.38) had significantly higher odds with elevated sexual risk. While OVC who withdrew from school (OR = 3.50, CI 2.28–5.36) and did not progress in school in the previous academic year (OR = 2.07, CI 1.16–3.70) had higher odds of elevated sexual risk in bivariate analysis, these covariates were excluded from multivariable analysis due to multicollinearity.
Sex-stratified models produced similar results for male and female OVC (see Supplementary ). However, significant associations of not having birth certificate and engaging in income-generating activities, respectively, with ordinal sexual risk observed in the pooled model were attenuated in females.
Early and later sexual debut
To identify correlates of early and later sexual debut among older OVC (n = 392), multinomial logistic regression produced unadjusted and adjusted relative risk ratios (RRR) comparing OVC with early and later sexual debut, respectively, to those without sexual debut (see ). Relative to OVC without sexual debut, OVC with later sexual debut were significantly more likely to be out-of-school (Adjusted RRR [aRRR] = 2.89, CI 1.25–6.67), engage in income-generating activities (aRRR = 2.44, CI 1.00–5.95), and have caregivers who could not afford food expenses (aRRR = 3.32, CI 1.28–8.60).
Table 4. Unadjusted and adjusted relative risk ratios (RRR) of early (before age 15) and later (at or after age 15) sexual debut derived from multinomial logistic regression, by demographic and protective deficit factors, among older (ages 15–17) orphaned and vulnerable children (N = 392)
Relative to OVC without sexual debut, unadjusted significant correlates of early sexual debut included: male sex (RRR = 3.25, CI: 1.59–6.66), not having a birth certificate (RRR = 3.72, CI 1.06–13.09), being currently out-of-school (RRR = 2.17, CI 1.04–4.53), and engaging in income-generating activities (RRR = 2.83, CI 1.41–5.70). In the presence of other covariates, however, only male sex remained significantly associated with early sexual debut (aRRR = 2.72, CI: 1.23–6.04). School attrition was independently associated with later (RRR = 3.18, CI 1.48–6.85) and early (RRR = 2.31, CI 1.12–4.83) sexual debut, respectively, but this covariate was ultimately dropped from the multivariable model due to multicollinearity.
Discussion
Despite the UNAIDS global call for leaving no one behind in the multi-national efforts towards HIV prevention, treatment and care, including attainment of the 95–95-95 targets for testing, treatment and viral suppression through treatment adherence, much less research efforts have looked at factors that attenuate risk or confer protection among OVC. Drawing from a theoretical framework, this large study of Zambian OVC situates sexual debut and risk behaviors in a constellation of social, educational, and financial deficits. These emerged as significant drivers of sexual behaviors and risk among Zambian OVC. Children growing without birth certificates have limited access to schooling and other social services, and their health care can be compromised without knowledge of their actual age. In the present study, not having a birth certificate, out-of-school status, and engaging in income-generating activities were significantly associated with increased sexual risk (early sexual debut, multiple past-year sexual partners, and unprotected last sex) in ordered logistic regression. Out-of-school status, but engaging in income-generating activities, and caregiver inability to afford food expenses were, likewise, significant correlates of later sexual debut. Only male sex emerged as a significant correlate of early sexual debut among older OVC, suggesting that associations between age at first sex and protective deficits were predominantly driven by OVC with later sexual debut. This is unsurprising, given that the majority of sexually experienced OVC reported their first sex before age 15.
Findings highlight the contribution of social adversity, educational attrition, and financial insecurity to HIV sexual risks in OVC. A qualitative study in Kenya identified food insecurity, school attrition, poor housing, and labor participation as mechanisms through which poverty influences sexual experimentation and risk-taking among orphaned and non-orphaned youth alike (Juma, Alaii, Bartholomew, Askew, Van Den Born et al., Citation2013a). A parallel quantitative study found caregiver social support and discussing sex with caregivers buffered sexual risks in Kenyan youth (Juma, Alaii, Bartholomew, Askew, Van den Borne et al., Citation2013b). The contribution of food insecurity and household wealth to OVC sexual behavior and risks, including transactional sex and sexual coercion, have similarly been documented in Malawi and South Africa (Cluver et al., Citation2011; Littrell et al., Citation2011). While previously identified associations of food security, and instrumental support from caregivers with lower sexual risk were not found in this study, these results build on existing evidence linking educational and financial deficits to sexual behavior among OVC.
Not having a birth certificate surfaced as a dimension of social adversity associated with elevated sexual risk. As a conduit to vital social and health services, civil registration is a well-documented determinant of future social and economic wellbeing (Crea et al., Citation2015; Phillips et al., Citation2015). Civil registration is also cardinal in protection against early marriages among female adolescents (The International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b) et al., Citation2013). In this study context, the absence of a birth certificate could reflect extreme household poverty or indicate a change in the OVC’s caregiving environment (e.g. as a result of orphanhood or financially motivated adoption). As a potential driver of access to social and financial assets, which are protective against sexual risks, civil registration should remain a programming priority for OVC, especially for those who are out-of-school or lack access to public services.
Male and rural-dwelling OVC reported more sexual risks than their female and urban-dwelling counterparts, respectively. Except for unprotected sex, male OVC reported early sexual debut and multiple partnerships with greater frequency than females, while sexual behaviors were consistently and significantly more prevalent among OVC in rural settings. Findings around sex and community differences in age at first sex and other sexual behaviors among youth in sub-Saharan Africa are highly variable. While some studies report more prevalent and earlier sexual behavior among women and in urban settings (Cluver et al., Citation2011; Gregson et al., Citation2005; Robertson et al., Citation2010), others observe these outcomes more frequently in men and rural communities (Juma, Alaii, Bartholomew, Askew, Van den Borne et al., Citation2013b; Puffer et al., Citation2011). Sex differences in sexual behavior could be an artifact of social desirability, with males overreporting their sexual behavior and females underreporting theirs. Without discounting the potential contribution of response biases to observed sex-specific patterns in sexual behavior, prioritizing and differentiating sexual risk-reduction strategies, including social asset building and behavior change communication, to adolescent boys and rural OVC, respectively, could reduce harms associated with earlier sex and risky sexual behavior.
This study illuminated key protective deficits associated with sexual behavior and risks among Zambian OVC; these findings, nonetheless, should be reviewed with several limitations in mind. First, as a cross-sectional study, temporal and causal relationships cannot be inferred from results. Second, self-reported measures, particularly for sensitive topics like sexual behavior, are susceptible to response biases. Third, the available measures of sexual behavior are crude indicators of sexual risk and do not capture all dimensions of sexual risk, including coercive encounters and transactional sex. Fourth, given the small proportion of OVC reporting sexual debut, sexual behaviors were aggregated analytically to achieve sufficient statistical power to detect meaningful associations. Fifth, while the ZAMFAM project supports households meeting predetermined vulnerability criteria, orphanhood status was not ascertained in the survey; its association with OVC sexual behavior, therefore, could not be assessed. Further interrogation of factors associated with independent sexual risks, including multiple partnerships and unprotected sex, is warranted. Lastly, while the sampling strategy facilitated representative selection of ZAMFAM-beneficiary households, results cannot be generalized to the broader OVC population in Zambia or other settings.
This study found that odds of sexual risk were highest among older, male, and rural-dwelling OVC. Likewise, OVC who lack birth certificates, are out-of-school, and engage in income-generating activities were more likely to have experienced their sexual debut and report other sexual risks, including multiple partners and unprotected sex. Recommended modifications to ZAMFAM service-delivery include differentiated sexual risk-reduction strategies for male and rural-dwelling OVC; prioritizing support to households experiencing financial distress (e.g. food insecurity, child labor participation, school attrition); and increasing civil registration. Given the infrequency with which OVC discussed sex and HIV/AIDS with their caregivers, leveraging existing programmatic infrastructure (i.e. ZAMFAM trained counselors) to initiate dialogue on these sensitive matters between OVC and their caregivers is a viable, low-cost risk-reduction strategy.
Author contributions
NK and MTM conceptualized and secured funding for the study. MC and LP oversaw study implementation, including data collection and data management. JGR led data analysis, with support from MC, LP, and ESN. JGR prepared the first draft of the manuscript. All authors contributed to and approved the final manuscript.
Abbreviations
ARTAntiretroviral therapy
DAPP Development Aid from People to People
ECR Expanded Church Response
OVC Orphaned and vulnerable children
PEPFAR U.S. President’s Emergency Plan for AIDS Relief
USAID U.S. Agency for International Development
ZAMFAM Zambia Family project
Supplemental Material
Download MS Word (21.2 KB)Acknowledgments
We express gratitude to all survey participants for their time and candor. We thank ZAMFAM implementing partners, DAPP and ECR Trust, for their support of this research. We thank the community-based organizations, community health volunteers, and Community Welfare Assistance Committees for their support with household enumeration and recruitment. We want to acknowledge the Ministry of Health and Ministry of Community Development and Social Services for administratively approving the study and availing staff to support study activities in numerous districts. We are grateful to the study Technical Advisory Group, comprised of representatives from the above government Ministries, UN agencies, University Teaching Hospital, health professional bodies, USAID, and civil society representatives who provided technical and scientific advice throughout the course of study implementation. We acknowledge the efforts of enumerators and their supervisors, specifically Saziso Mulenga and Bwalya Mushiki, in supporting survey implementation. Lastly, we thank Paul Hewett, Jean Digitale, Francis Onyango, Scott Geibel, Ellen Weiss, and Waimar Tun for their technical guidance and editorial input.
Data availability
Data presented for this study are available from the corresponding author (MTM) upon reasonable request.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Supplementary material
Supplemental data for this article can be accessed here.
Additional information
Funding
References
- Brant, R. (1990). Assessing proportionality in the proportional odds model for ordinal logistic regression. Biometrics, 46(4), 1171–1178. https://doi.org/https://doi.org/10.2307/2532457
- Cluver, L., Gardner, F., & Operario, D. (2007). Psychological distress amongst AIDS-orphaned children in urban South Africa. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 48(8), 755–763. https://doi.org/https://doi.org/10.1111/j.1469-7610.2007.01757.x
- Cluver, L., Orkin, M., Boyes, M., Gardner, F., & Meinck, F. (2011). Transactional sex amongst AIDS-orphaned and AIDS-affected adolescents predicted by abuse and extreme poverty. JAIDS Journal of Acquired Immune Deficiency Syndromes, 58(3), 336–343. https://doi.org/https://doi.org/10.1097/QAI.0b013e31822f0d82
- Craney, T. A., & Surles, J. G. (2002). Model-dependent variance inflation factor cutoff values. Quality Engineering, 14(3), 391–403. https://doi.org/https://doi.org/10.1081/QEN-120001878
- Crea, T. M., Reynolds, A. D., Sinha, A., Eaton, J. W., Robertson, L. A., Mushati, P., Dumba, L., Mavise, G., Makoni, J. C., Schumacher, C. M., Nyamukapa, C. A., & Gregson, S. (2015). Effects of cash transfers on children’s health and social protection in Sub-Saharan Africa: Differences in outcomes based on orphan status and household assets. BMC Public Health, 15(1), 511. https://doi.org/https://doi.org/10.1186/s12889-015-1857-4
- Dellar, R. C., Dlamini, S., & Karim, Q. A. (2015). Adolescent girls and young women: Key populations for HIV epidemic control. Journal of the International AIDS Society, 18(2), 1. https://doi.org/https://doi.org/10.7448/IAS.18.2.19408
- Embleton, L., Ayuku, D., Kamanda, A., Atwoli, L., Ayaya, S., Vreeman, R., Nyandiko, W., Gisore, P., Koech, J., & Braitstein, P. (2014). Models of care for orphaned and separated children and upholding children’s rights: Cross-sectional evidence from western Kenya. BMC International Health and Human Rights, 14(1), 9. https://doi.org/https://doi.org/10.1186/1472-698X-14-9
- Gray, C. L., Whetten, K., Messer, L. C., Whetten, R. A., Ostermann, J., O’Donnell, K., Thielman, N. M., & Pence, B. W. (2016). Potentially traumatic experiences and sexual health among orphaned and separated adolescents in five low- and middle-income countries. AIDS Care, 28(7), 857–865. https://doi.org/https://doi.org/10.1080/09540121.2016.1147013
- Gregson, S., Nyamukapa, C. A., Garnett, G. P., Wambe, M., Lewis, J. J. C., Mason, P. R., Chandiwana, S. K., & Anderson, R. M. (2005). HIV infection and reproductive health in teenage women orphaned and made vulnerable by AIDS in Zimbabwe. AIDS Care, 17(7), 785–794. https://doi.org/https://doi.org/10.1080/09540120500258029
- Hayes, R., Floyd, S., Schaap, A., Shanaube, K., Bock, P., Sabapathy, K., Griffith, S., Donnell, D., Piwowar-Manning, E., El-Sadr, W., Beyers, N., Ayles, H., Fidler, S., & Low, N., & HPTN 071 (PopART) Study Team. (2017). A universal testing and treatment intervention to improve HIV control: One-year results from intervention communities in Zambia in the HPTN 071 (PopART) cluster-randomised trial. PLoS Medicine, 14(5), e1002292. https://doi.org/https://doi.org/10.1371/journal.pmed.1002292
- Hayes, R. J., Donnell, D., Floyd, S., Mandla, N., Bwalya, J., Sabapathy, K., Yang, B., Phiri, M., Schaap, A., Eshleman, S. H., Piwowar-Manning, E., Kosloff, B., James, A., Skalland, T., Wilson, E., Emel, L., Macleod, D., Dunbar, R., Simwinga, M., Bond, V., … Fidler, S. (2019). Impact of a universal testing and treatment intervention on HIV incidence in Zambia and South Africa: Results of the HPTN 071 (PopART) community-randomized trial. The New England Journal of Medicine, 381(3), 207–218. https://doi.org/https://doi.org/10.1056/NEJMoa1814556
- Juma, M., Alaii, J., Bartholomew, L. K., Askew, I., & Van Den Born, B. (2013a). Understanding orphan and non-orphan adolescents’ sexual risks in the context of poverty: A qualitative study in Nyanza Province, Kenya. BMC International Health and Human Rights, 13(1), 32. https://doi.org/https://doi.org/10.1186/1472-698X-13-32
- Juma, M., Alaii, J., Bartholomew, L. K., Askew, I., & Van den Borne, B. (2013b). Risky sexual behavior among orphan and non-orphan adolescents in Nyanza Province, Western Kenya. AIDS and Behavior, 17(3), 951–960. https://doi.org/https://doi.org/10.1007/s10461-012-0336-5
- Kane, J. C., Bolton, P., Murray, S. M., Bass, J. K., Lakin, D., Whetten, K., van Wyk, S. S., & Murray, L. K. (2018). Psychometric evaluation of HIV risk behavior assessments using Audio Computer Assisted Self-Interviewing (ACASI) among orphans and vulnerable children in Zambia. AIDS Care, 30(2), 160–167. https://doi.org/https://doi.org/10.1080/09540121.2017.1384787
- Kasedde, S., Doyle, A. M., Seeley, J. A., & Ross, D. A. (2014). They are not always a burden: Older people and child fostering in Uganda during the HIV epidemic. Social Science & Medicine (1982), 113(100), 161–168. https://doi.org/https://doi.org/10.1016/j.socscimed.2014.05.002
- Kayeyi, N., Fylkesnes, K., Wiium, N., Sandøy, I. F., & Graham, S. M. (2013). Decline in sexual risk behaviours among young people in Zambia (2000–2009): Do neighbourhood contextual effects play a role? PLoS ONE, 8(5), 5. https://doi.org/https://doi.org/10.1371/journal.pone.0064881
- Lee, V. C., Muriithi, P., Gilbert-Nandra, U., Kim, A. A., Schmitz, M. E., Odek, J., Mokaya, R., & Galbraith, J. S. (2014). Orphans and vulnerable children in Kenya: Results from a nationally representative population-based survey. JAIDS Journal of Acquired Immune Deficiency Syndromes, 66(Suppl 1), S89–S97. https://doi.org/https://doi.org/10.1097/QAI.0000000000000117
- Littrell, M., Boris, N. W., Brown, L., Hill, M., & Macintyre, K. (2011). The influence of orphan care and other household shocks on health status over time: A longitudinal study of children’s caregivers in rural Malawi. AIDS Care, 23(12), 1551–1561. https://doi.org/https://doi.org/10.1080/09540121.2011.582079
- Mathur, S., Pilgrim, N., Patel, S. K., Okal, J., Mwapasa, V., Chipeta, E., Musheke, M., Mahapatra, B., & Pulerwitz, J. (2020). HIV vulnerability among adolescent girls and young women: A multi-country latent class analysis approach. International Journal of Public Health, 65(4), 399–411. https://doi.org/https://doi.org/10.1007/s00038-020-01350-1
- Mbizvo, M., Hewett, P. C., Kayeyi, N., Phiri, L., Mulenga, S. N., Mushiki, B., Chibuye, M., & Digitale, J. (2018). Benchmark assessment of orphaned and vulnerable children in areas of the Zambia family (ZAMFAM) project. Washington, D.C.: Population Council. http://www.projsoar.org/wp-content/uploads/2018/02/Zambia_ZAMFAMBnchmrk_full.pdf
- MEASURE Evaluation. (2013). Child, caregiver & household well-being survey tools for orphans & vulnerable children programs: protocol template. MEASURE Evaluation. http://45.79.212.156/system/files/resource/files/Child%2C%20Caregiver%20and%20Household%20Well-being%20Survey%20Tools%20for%20OVC%20Programs%20-%20Protocol%20Template.pdf
- National HIV/AIDS/STI/TB Council. (2012). Zambia country report: Monitoring the declaration of commitment on HIV and AIDS and the universal access. http://www.unaids.org/sites/default/files/country/documents/ZMB_narrative_report_2015.pdf
- Ndongmo, T. N., Ndongmo, C. B., & Michelo, C. (2017). Sexual and reproductive health knowledge and behavior among adolescents living with HIV in Zambia: A case study. The Pan African Medical Journal, 26, 71. https://doi.org/https://doi.org/10.11604/pamj.2017.26.71.11312
- Nyambedha, E. O., Wandibba, S., & Aagaard-Hansen, J. (2003). Changing patterns of orphan care due to the HIV epidemic in western Kenya. Social Science & Medicine (1982), 57(2), 301–311. https://doi.org/https://doi.org/10.1016/S0277-9536(02)00359-3
- Office of the Global AIDS Coordinator. (2017). PEPFAR monitoring, evaluation, and reporting [MER 2.0] indicator reference guide. U.S. President’s Emergency Plan for AIDS Relief. https://www.pepfar.gov/documents/organization/263233.pdf
- Olanrewaju, A. D., Jeffery, C., Crossland, N., Valadez, J. J., & Van Wouwe, J. (2015). Access to education for orphans and vulnerable children in Uganda: A multi-district, cross-sectional study using lot quality assurance sampling from 2011 to 2013. PloS One, 10(7), e0132905. https://doi.org/https://doi.org/10.1371/journal.pone.0132905
- Operario, D., Underhill, K., Chuong, C., & Cluver, L. (2011). HIV infection and sexual risk behaviour among youth who have experienced orphanhood: Systematic review and meta-analysis. Journal of the International AIDS Society, 14(1), 25. https://doi.org/https://doi.org/10.1186/1758-2652-14-25
- Pascoe, S. J. S., Langhaug, L. F., Mavhu, W., Hargreaves, J., Jaffar, S., Hayes, R., Cowan, F. M., & Wilkinson, R. J. (2015). Poverty, food insufficiency and hiv infection and sexual behaviour among young rural Zimbabwean women. PLoS ONE, 10(1), 1. https://doi.org/https://doi.org/10.1371/journal.pone.0115290
- Pettifor, A., Stoner, M., Pike, C., & Bekker, L.-G. (2018). Adolescent lives matter: Preventing HIV in adolescents. Current Opinion in HIV and AIDS, 13(3), 265–273. https://doi.org/https://doi.org/10.1097/COH.0000000000000453
- Phillips, D. E., AbouZahr, C., Lopez, A. D., Mikkelsen, L., de Savigny, D., Lozano, R., Wilmoth, J., & Setel, P. W. (2015). Are well functioning civil registration and vital statistics systems associated with better health outcomes? The Lancet, 386(10001), 1386–1394. https://doi.org/https://doi.org/10.1016/S0140-6736(15)60172-6
- Project SOAR. (2019). Health and socioeconomic well-being of young people living with HIV one year after implementation of the ZAMFAM Project. Project SOAR. http://www.projsoar.org/wp-content/uploads/2019/04/ZAMFAM_Cohort_R2_ResBrief.pdf
- Puffer, E. S., Meade, C. S., Drabkin, A. S., Broverman, S. A., Ogwang-Odhiambo, R. A., & Sikkema, K. J. (2011). Individual- and family-level psychosocial correlates of HIV risk behavior among youth in rural Kenya. AIDS and Behavior, 15(6), 1264–1274. https://doi.org/https://doi.org/10.1007/s10461-010-9823-8
- Rivers, J., Mason, J. B., Rose, D. D., Eisele, T. P., Gillespie, S., Mahy, M., & Monasch, R. (2010). The impact of orphanhood on food security in the high-HIV context of Blantyre, Malawi. Food and Nutrition Bulletin, 31(3 Suppl), S264–271. https://doi.org/https://doi.org/10.1177/15648265100313S305
- Robertson, L., Gregson, S., & Garnett, G. P. (2010). Sexual risk among orphaned adolescents: Is country-level HIV prevalence an important factor? AIDS Care, 22(8), 927–938. https://doi.org/https://doi.org/10.1080/09540121003758622
- The International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b), Associates for Community and Population Research (ACPR), & Plan International Bangladesh. (2013). Child Marriage in Bangladesh: Findings from a National Survey, 2013. Plan International Bangladesh. https://plan-international.org/publications/child-marriage-bangladesh-findings-national-survey#:~:text=Bangladesh%20has%20one%20of%20the,before%20the%20age%20of%2018.&text=This%20survey%20by%20Plan%20International,with%20levels%20of%20child%20marriage
- Thurman, T. R., Brown, L., Richter, L., Maharaj, P., & Magnani, R. (2006). Sexual risk behavior among South African adolescents: Is orphan status a factor? AIDS and Behavior, 10(6), 627–635. https://doi.org/https://doi.org/10.1007/s10461-006-9104-8
- Whetten, K., Ostermann, J., Whetten, R., O’Donnell, K., & Thielman, N., & Positive Outcomes for Orphans Research Team. (2011). More than the loss of a parent: Potentially traumatic events among orphaned and abandoned children. Journal of Traumatic Stress, 24(2), 174–182. https://doi.org/https://doi.org/10.1002/jts.20625
- Zambia Ministry of Health. (2019). Zambia population-based HIV impact assessment (ZAMPHIA) 2016: Final report. Zambia Ministry of Health. https://phia.icap.columbia.edu/wp-content/uploads/2019/03/ZAMPHIA-Final-Report__2.26.19.pdf
