
Abstract
This study investigated individuals’ preference for different levels of realism in anatomical 3D scans. Staff and students working with anatomical material at the University of Dundee were asked to look at three versions of a 3D scan of the upper limb as follows: high realism – i.e. minimally altered from the original scan; moderate realism – i.e. a more significantly processed scan; and lower realism – i.e. the most significantly processed scan. Twenty-two participants took part in the study, with the majority preferring the ‘moderate realism’ scan overall, suggesting however that the ‘high realism’ scan would be most preferable for use in relation to anatomy (i.e. cadaver) practical sessions.
Introduction
Digital 3D models have become well established as a means of learning and teaching within anatomy and medical education, most often being viewed as an adjunct to other methods such as lectures and dissection/prosection study (Erolin, Citation2019; Tiznado-Matzner et al., Citation2020; Trelease, Citation2016). These models can take a number of forms but are usually either ‘models’ created from scratch using 3D software, or ‘scans’ of real specimens. There are advantages and disadvantages to each approach, with models tending to have an increased clarity, with brighter colours and more distinct structures, whereas scans may have less clarity but increased realism and possibly increased accuracy.
It is important to clarify at the outset what is meant by the term ‘realism’ in this paper. Realism here refers to how closely the scan resembles the appearance of the real specimen it is based upon. It is distinct from ‘detail’ in that it is possible to have a highly detailed cartoon illustration of anatomy, but this would not be considered realistic, and likewise it is possible to have a blurred photograph of an anatomical specimen, which lacks detail but retains realism. Therefore, each of the scans presented in this study were prepared to a similar level of detail and anatomical accuracy. Rather, it was the level of realism that varied, with the more processed scans becoming brighter in colour, and the distinction between structures becoming more defined. A previous study investigating user preference for detail in anatomical illustrations (Strong & Erolin, Citation2013) found that both professionals and lay persons showed a preference for high-detail (i.e. complex) illustrations. A similar result was found by Haragi et al. (Citation2021), when studying user preference for degrees of detail in cancer information. They found that participants over 40 years old tended to prefer higher detail, with those under 40 years old preferring medium detail. The low detail option was the least preferred amongst all groups, however. It is with this in mind that all three scans were prepared at a reasonably high level of detail.
Studies into user preference for realism in medical illustration are rare but a notable example is that by Scheltema et al. (Citation2018) who explored user preference for varying degrees of ‘naturalism or abstraction from reality’ in clinical (2D) illustrations gathering feedback from both patients and medical professionals. They found that most users preferred the more realistic depictions; however, patients often preferred illustrations depicting a greater amount of information than the medical professionals thought necessary. Unlike the study presented here, Scheltema and Reay’s research linked realism with visually complex images, so it becomes difficult to untangle whether the preference was for the realism of the image, or the larger degree of information contained within, or both.
The concept of realism in art is discussed in the book Understanding comics, by Scott McCloud. McCloud’s ‘Big Triangle’ is used to combine all visual vocabulary (pictures, words, symbols, etc.) into an easily understood map of possibilities (McCloud, Citation1994). All visual outputs can be mapped onto the triangle at varying lengths from its three points of: realism (reality), idealisation (meaning) and abstraction (the picture plane). For example, a photograph of an object would be positioned close to realism, whereas a cartoon would move further away but still be capable of conveying the same essential meaning. This continuum from realistic to cartoon images represents increasing levels of iconic abstraction. When taken to its extreme, the result of this process is written language. Pure abstraction, however, departs from both resemblance and meaning. Taken to its extreme, it leads to the picture plane of pure shape, colour and line.
With an increasing amount of 3D digital models being created, and anatomical specimens being scanned and made available remotely to students, it is important to understand what level of realism is best for a given audience (in this case anatomy and medical students). Should 3D models be created with a higher degree of realism, or should scans of real specimens undergo post-processing to improve their clarity? It could be argued that increased clarity is most important to learning and teaching; however, students also need to be able to identify structures on real cadavers (and later potentially on living bodies during surgery), so too much artificial clarity may not be in their best interests. This study therefore aimed to investigate preferences for different levels of realism in anatomical 3D scans amongst staff and students working with anatomical material at the University of Dundee. Three versions of a 3D scan of the upper limb were presented: high realism – i.e. minimally altered from the original scan; moderate realism – i.e. a more significantly processed scan; and lower realism – i.e. the most significantly processed scan.
Methods
The Centre for Anatomy and Human Identification at the University of Dundee uses the Thiel method of embalming (Eisma et al., Citation2013), this is soft fix method that produces cadavers that are both flexible and retain lifelike colour. Over the academic year of 2021–2022, a number of high-quality dissections were produced on Thiel cadavers including of the head and neck, upper limb and lower limb. All of these were scanned to create online versions for learning and teaching. The scan of the dorsal upper right limb was chosen for this study due to being of the highest quality.
Initial scanning
The scan was created using an Artec Space Spider structured light scanner and the associated software Artec Studio 15. The Space Spider scanner provides a 3D point accuracy of up to 0.05 mm and a 3D resolution of up to 0.1 mm.Footnote1 The dorsal and palmar aspects of the specimen were scanned individually; it was not possible to combine these into a single model due to the movement of structures that occurred when the specimen was rotated. The resulting scan therefore has a flat under surface which was later coloured black so as to blend with the background. Surface scanners are known to struggle with wet and shiny surfaces (Erolin, Citation2019), so the specimen was gently dabbed with paper towels prior to scanning to minimise this issue.
Once scanning was complete, Artec Studio 15 was used to run rough, fine and global registrations of the individual scans before using the ‘auto-alignment’ feature to align them. The aligned scans were then fused using the ‘sharp fusion’ feature with the ‘fill holes’ option set to ‘watertight’. In addition to the geometry, a photographic colour texture map was also produced and was exported at a map size of 4096 × 4096. The texture map was exported along with the .obj mesh as a .jpeg file.
Cleaning scan data (high realism)
The intent for the high realism version of the scan was that it should be as close as possible in appearance to the original specimen. Therefore, only minimal cleaning of the scan data was undertaken. The scan was imported into the 3D modelling software ZBrush (2022.0.5) as an .obj file along with the accompanying texture map. The geometry (i.e. point count) was divided to increase the resolution of the scan before converting the texture map to Polypaint (using the ‘Polypaint from Texture’ feature) in order for it to be further edited along with the geometry. The geometry was only minimally edited by deleting unnecessary data and artefacts using the TrimLasso brush and smoothing out minor artefacts with the Smooth brush. The colour was corrected for harsh shadows and missing data using the Polypaint feature. The flat underside of the scan was painted black so as to later blend with the background when viewed online. Although a new texture map was created from the updated Polypaint, this resulted in a slightly lower quality, so the final model was exported with the Polypaint as vertex colour. Vertex colour applies the RGBA value directly to the vertices of a mesh. When exporting from ZBrush, vertex colour is embedded within the .obj file and can be read by Sketchfab, the online platform used to share the models.
Enhancing scan data (moderate realism)
Further post-processing was undertaken in ZBrush to create the moderate realism version of the scan. Enhancing scans is subtly different to cleaning them, where the intent is to replicate the object being scanned by editing any errors on the mesh. Editing a scan to enhance it is generally done to improve its clarity and/or to highlight certain features. As described above, each version of the scan used in this study is of an approximately similar level of detail, rather it is the degree to which the scan has been processed that differs. With decreased ‘realism’ comes increased ‘clarity’, structures are more clearly defined, there is less ‘noise’ from anatomical debris, and the colours are brighter.
In this case, the scan was enhanced to what the author considered to be a moderate level of clarity/realism. In addition to ‘cleaning’ the data as described above, this involved deleting further areas of ‘messy’ tissue such as small pieces of fat and fascia found adhering to tendons. The smooth brush was used to further smooth out imperfections on the surface and to help clarify structures. The Move brush was used to straighten structures that were slightly bent or in unnatural positions and the Standard brush was used in both its additive and subtractive modes to build structures up and down as required, again to make the structures appear more as they would likely have done in life. Finally, the Damstandard brush was used to create ‘creases’, which were helpful for clarifying the edges of structures.
Once complete, the mesh was retopologised using the Z-Remesher feature, which recreates the surface with a more optimal geometry. As with the high realism version, a texture map was created but the vertex colour was ultimately used both as it appeared to be a slightly higher quality and for consistency between the versions.
It was noted while enhancing this version that Extensor Pollicis Longus and Extensor Digiti Minimi were too short, likely having their ends damaged on the dissection or disappearing from view under fascia. Therefore, the missing elements were remodelled on this version (and carried over to the next).
Further enhancement of scan data (lower realism)
For the final version, the scan was enhanced to what the author considered to be a lower level of realism, but arguably the highest level of clarity. As with the moderate realism version, further post-processing was undertaken in ZBrush, using the same brushes to further normalise and define structures. Surfaces were smoothed further, and the colours simplified. The depiction of fascia over the muscles (which is visible on the high and moderate versions) was removed and replaced with the depiction of more ‘organised’ muscle fibre texture. compares the appearance of the geometry from the high realism scan with that of the lower realism.
Figure 1. A comparison between the geometry of the high realism scan with that of the lower realism.

As with the previous two versions, a texture map was created but the vertex colour was ultimately used both as it appeared to be a slightly higher quality and for consistency between the versions.
Dissemination
The online 3D model sharing platform SketchfabFootnote2 was used to host and distribute the three scans. The Centre for Anatomy and Human Identification at the University of Dundee has a professional Sketchfab account, which allows for models to be uploaded under a ‘private’ setting, meaning that only those with a direct link can view the models, rather than them being publicly available.
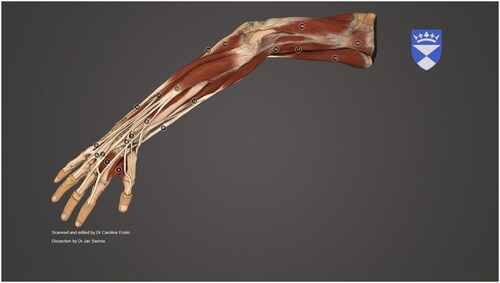
The scans were uploaded to Sketchfab as .obj files with vertex colour embedded. Once uploaded to Sketchfab, various settings were altered within the ‘3D Settings’ window. These included positioning the scans, setting a custom background to include the university logo, applying lighting, and material properties. In addition, annotations were added to label the main structures. Settings and annotations were consistent across all scans. As the scans were based on human material, they were set to private. Screen shots of the final scans as viewed in Sketchfab can be seen in .
Figure 2. A screenshot of the final ‘high realism’ scan as seen in Sketchfab.

Figure 3. A screenshot of the final ‘moderate realism’ scan as seen in Sketchfab.

Figure 4. A screenshot of the final ‘lower realism’ scan as seen in Sketchfab.
Study design
This study investigated individuals’ preference for different levels of realism in anatomical 3D scans. Staff and students working with anatomical material at the Centre for Anatomy and Human Identification, at the University of Dundee were asked to look at three versions of a 3D scan of the upper limb as follows: high realism – i.e. minimally altered from the original scan; moderate realism – i.e. a more significantly processed scan; and lower realism – i.e. the most significantly processed scan.
Ethical approval for this study was granted by the University of Dundee Research Ethics Committee (application/approval number: UOD_SSREC_CAHID_STAFF_2022_007). Staff and students were recruited via email either from the researcher (in the case of staff) or their programme lead (for students). The recruitment emails made it clear that taking part was voluntary and that there would be no disadvantage to not taking part. Students could be from any programme or year of study, as long as they had some experience of working with human anatomical material. As they were not going to be questioned on their anatomical knowledge, the different levels of experience were not considered an issue.
The recruitment email contained a link to an anonymous online survey, created using JISC Online Surveys. The first page of the survey consisted of the participant information sheet and informed consent. The end of the consent page stated that ‘by clicking “next” you are indicating that you have read and understood the Participant Information Sheet and that you agree to take part in this research study’. Page two of the survey consisted of links to the three scans along with brief information on how to best navigate the models (how to rotate, zoom, pan, etc.). Participants were invited to view the scans for as long as they chose and were encouraged to move between the scans to compare them.
Once all of the scans had been viewed the participants were asked to move to page three, ‘about you’, which asked a series of demographic questions as well as if they currently use any 3D anatomy resources. Finally, page four asked for their feedback and preference for anatomical realism, both overall as well as in various situations, such as for revision before and after anatomy practical sessions. This section ended with the opportunity for participants to make any further comments or suggestions.
Results
Testing and feedback took place during October and November of 2022. Twenty-two participants completed the online survey. The survey consisted of a mix of closed Likert style and open/free text questions. The closed questions alternated between positive and negative phrasing to avoid acquiescence bias. Of the 22 participants, 16 identified as female and five as male (with one preferring not to say). Fifteen participants were aged between 18 and 29 years, six between 30 and 39 years, and one 60−69 years. Six were members of staff and 16 were students. Of the students, 12 were studying an undergraduate programme and five postgraduate. When asked if they currently used any 3D anatomy resources 17 participants answered ‘yes’, and five ‘no’. Various resources were cited, with Sketchfab and Primal Picture Anatomy TV getting the most mentions, being named 10 and 11 times, respectively.
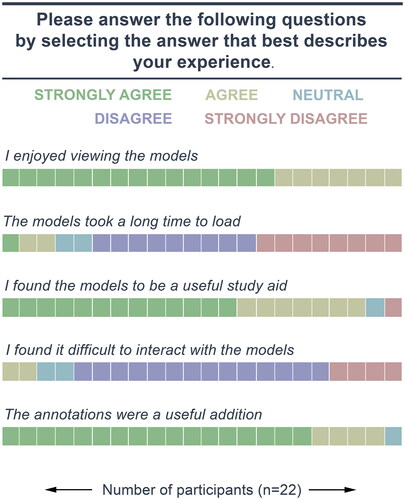
The next page of the survey asked a variety of questions around preference for realism in anatomical scans. The first section asked a series of five closed Likert style questions, starting with ‘I enjoyed viewing the models’ to which all (22) participants either ‘agreed’ or ‘strongly agreed’. Seventeen participants ‘disagreed’ or ‘strongly disagreed’ that loading times were long, with just three answering, ‘strongly agree’, or ‘agree’ and two selecting ‘neither agree nor disagree’. Most (20) participants either ‘agreed’ or ‘strongly agreed’ with the statement ‘I found the models to be a useful study aid’, with one strongly disagreeing, and another selecting ‘neither agree nor disagree’. A majority (18) of participants ‘disagreed’ or ‘strongly disagreed’ with the statement ‘I found it difficult to interact with the models’, with just two ‘agreeing’ and another two selecting ‘neither agree nor disagree’. Finally, 21 participants either ‘agreed’ or ‘strongly agreed’ with the statement ‘the annotations were a useful addition’ with just one selecting ‘neither agree nor disagree’ ().
Figure 5. Results for the first Likert style questions.
The next section asked six single answer style questions, with each having a free text space for participants to further explain their answer. The first of these asked which of the three scans they preferred overall? A majority of participants (12) selected the moderate realism scan with seven choosing high realism and three choosing lower realism (). When asked which scan they thought most useful for preparation in advance of an anatomy (cadaver) practical, a majority (13) chose high realism, with eight selecting moderate realism, and just one selecting lower realism (). When asked which scan they thought most useful for revision after an anatomy (cadaver) practical, a majority (11) chose high realism, while seven selected moderate realism, and a minority (4) lower realism (). When asked which scan they thought was best suited to undergraduate study, a majority (11) chose moderate realism, with seven selecting high realism, and four lower realism (). When asked which scan they thought was best suited to postgraduate study, a majority (14) chose high realism, with four selecting moderate realism, and two lower realism (). It should be noted that for this question, two students did not answer. Finally, when asked whether they considered ‘realism’ or ‘clarity’ to be most important in 3D anatomical scans and models, a majority (15) chose ‘clarity’ with seven selecting ‘reality’ ().
Figure 6. Results for question 7: ‘Which of the three scans did you prefer overall?’, for all responses, then comparing staff and students.

Figure 7. Results for question 8: ‘For preparation in advance of an anatomy (cadaver) practical, which scan do you think is most useful?’, for all responses, then comparing staff and students.
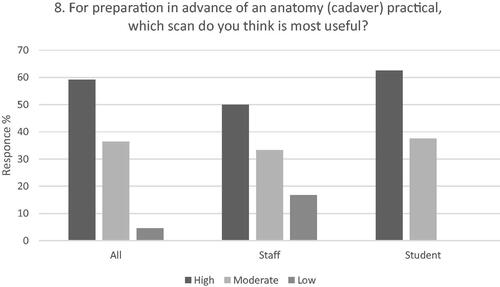
Figure 8. Results for question 9: ‘For revision after an anatomy (cadaver) practical, which scan do you think is most useful?’, for all responses, then comparing staff and students.
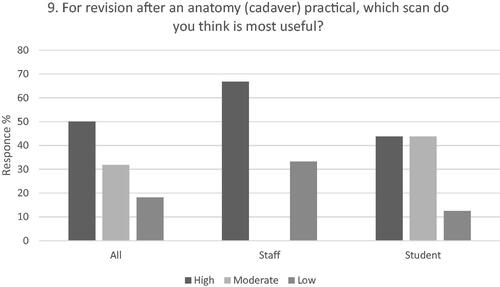
Figure 9. Results for question 10: ‘Which scan do you think is best suited to undergraduate study?’, for all responses, then comparing staff and students.
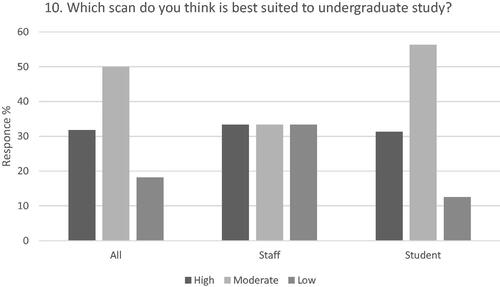
Figure 10. Results for question 11: ‘Which scan do you think is best suited to postgraduate study?’, for all responses, then comparing staff and students.
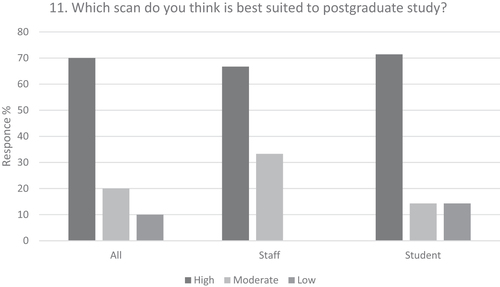
Figure 11. Results for question 12: ‘Which do you think is most important in 3D anatomical scans and models?’, for all responses, then comparing staff and students.
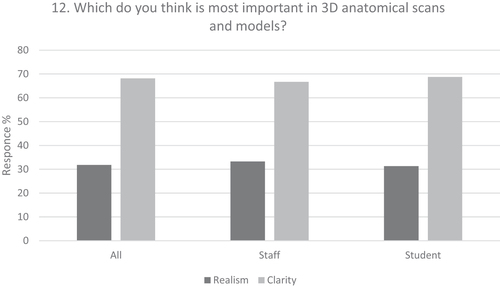
When split into staff and student cohorts, the results are slightly different between each group. Staff responses were split evenly across all three options for overall preference, with students having a preference for moderate realism overall (). Staff preferred the high realism scan for both preparation in advance of an anatomy (cadaver) practical and for revision after an anatomy (cadaver) practical. Students also preferred the high realism scan in advance of an anatomy (cadaver) practical but were equally split between high and moderate realism for revision after an anatomy (cadaver) session ( and ). When asked about their preference for use in undergraduate study, staff were again evenly split between all three options, whereas students favoured the moderate realism scan (). When asked about their preference for use in postgraduate study, both staff and students preferred the high realism scan (). Finally, when asked whether they felt ‘realism’ or ‘clarity’ was most important in 3D anatomical scans, a majority of both staff and students selected ‘clarity’ (). It should be noted that the small participant numbers, especially of staff, means the comparison of these results can only be indicative at best.
Thematic analysis
A thematic analysis was undertaken following the method outlined by Braun and Clarke (Citation2006). Thematic analysis is used to analyse qualitative data such as text from surveys, or transcripts from interviews. It is ideally suited to the analysis of smaller data sets, with 10–50 participants being recommended for participant generated text (Braun & Clarke, Citation2006). The researcher closely examines the data to familiarise themselves with it, before going on to code the text and then identify common themes. Thematic analysis was applied to the open answer questions, consisting of the free text elements of the six questions listed above as well as the final question ‘Any other comments or suggestions?’. To become familiar with the content, all of the comments were read through twice before being manually coded on a PDF exported from JISC surveys. From the codes, initial themes were developed and reviewed before forming the final themes and sub-themes and accompanying thematic map ().
Figure 12. Thematic map showing the final themes and sub-themes.
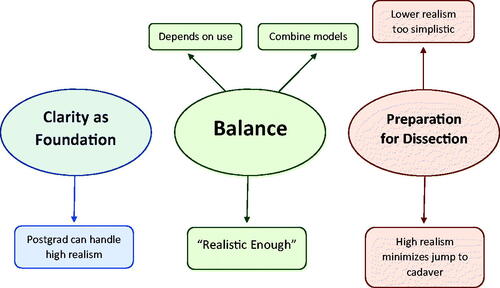
From the feedback comments analysed, three primary themes were evident in the data. These themes were labelled as ‘Clarity as Foundation’, ‘Balance’ and ‘Preparation for Dissection’. Each primary theme also had at least one sub-theme associated with it.
Clarity as Foundation: This theme was defined as including all of the feedback that commented on the need for understanding and clarity to come first, before building up to realism. There was an associated sub-theme of ‘postgraduates can handle high realism’ to encapsulate a number of comments that stated that by postgraduate level the foundation knowledge should already be set and that these students might benefit most from more realistic models.
Examples of feedback comments from this theme include:
Clarity is essential so that those who don’t have a strong foundation of knowledge yet can create that foundation, so that, in later years they can go on to understanding anatomy which lacks clarity, such as in cadavers who maybe haven’t held their shape quite as well or have anatomical anomalies. (Undergraduate student)
I feel like if you are looking at a model and cannot identify structures at all, then you will gain little from it. However you can start with an unrealistic, clear model and then build up to realistic models/scans. (Postgraduate student)
Students with prior anatomical knowledge will be able to cope better with the detail provide in the high realism model and will be able to make direct comparisons between this and real specimens. (Staff)
In this case, if you already have knowledge in anatomy and worked previously with cadavers, working with high realism can be easier and will allow you to concentrate in other aspects of the model like interactions or even recognize the anatomical variations for example. (Postgraduate student)
Examples of feedback comments from this theme include:
It provides the best of both worlds. (realism and clear diagrammatic quality)
I think it’s interesting and useful to combine several resources, both more schematic and more realistic. (Postgraduate student)
This probably depends on the aim of the figures. If they are intended to indicate to the students the realism of the dissection experience, then the high realism model is probably preferable; if they are intended as a learning aid for the anatomy before entry to the DR, then the lower realism model might be preferable. (Staff)
I think a combination of both is the most effective because the high realism one can be hard to understand but the low realism one doesn’t always accurately reflect what you are looking at in a body. The medium one helps to highlight and differentiate structures. (Postgraduate student)
A good balance between a clear division between the different components but wasn’t too cartoon like. Looks real enough to apply in Anatomy cadaver practical. (Undergraduate student)
Examples of feedback comments from this theme include:
I preferred the high realism scan because it made it more like what I will actually be seeing in real life. Because a lot of the time, most anatomy reasources (sic) are similar to the lower realism scan and then when I go into the anatomy lab, it is difficult to identify certain structures and muscles because all I have ever seen is a version which doesn’t really look a lot like real life. (Undergraduate student)
Allows students to see what they expect to see in a practical class. One bit of feedback we often get is that the cadavers don’t look like the textbook they have prepped from……by using a high realism model they can understand what it should actually look like before coming into the practical. (Staff)
The higher realism is truer to real life. I always find when using lower realism photos and 3d models it’s difficult to translate these images to the real structures on a cadaver. (Undergraduate student)
High realism resources make this a much easier jump. (Undergraduate student)
Discussion
Overall, the feedback on the scans was very positive, with all participants either agreeing or strongly agreeing with the statement ‘I enjoyed viewing the models’. Likewise, most (91%) participants either ‘agreed’ or ‘strongly agreed’ with the statement ‘I found the models to be a useful study aid’. Interestingly, one participant selected ‘strongly disagree’ to this statement; however, their other answers suggest this may have been an error, as they ‘strongly agreed’ that they enjoyed viewing the models and made no comments to suggest that they did not also find them useful. It is impossible to be sure, but this could be due to the alternating of positive and negative phrasing done to avoid acquiescence bias.
The overall preference was for the moderate realism scan, with numerous comments suggesting that participants considered this as providing the best balance between reality and clarity. However, results varied depending on the circumstances and target audience, with some responses even suggesting it would be beneficial for students to have access to two or more of scans as they each have different benefits. For preparation in advance of, and revision after, an anatomy (cadaver) practical, the overall preference was for the high realism scan. This indicates that for a majority of participants realism becomes more important once there is any cross over with cadaver study. This is further expanded on in several of the comments, which explain that often anatomy resources (whether 2D or 3D) are too simplistic, thus necessitating a large cognitive leap between the resource and the cadaver. The preference for the high realism scan is slightly stronger in advance of an anatomy practical than it is after, again supporting the notion that students feel under prepared for working with real anatomical material with many of the currently available resources. The responses for revision after an anatomy practical were more varied, and although the overall preference was still for high realism, there was an increase in selections of both the moderate and lower realism scans, indicating that there is more scope for individual preference when it comes to revision. The overall preference for undergraduate study was for the moderate realism scan, which may explain why this was the preferred choice overall. The majority of teaching undertaken at the centre is of undergraduate students, so this is perhaps understandably where the main focus lies. When asked about postgraduate study, the preference was for the high realism scan, with a number of comments stating that by this level, students should be able to better interpret the high realism scan and therefore benefit the most from it. The final quested asked participants to select which they felt was most important between ‘realism’ and ‘clarity’. Interestingly, despite the numerous comments about the importance of realism, the majority of participants chose clarity over realism. This does fit with the overall preference of the moderate realism scan, however, as this has improved clarity over the high realism version. A number of comments went on to clarify that while both are important, clarity is the essential foundation and only once there is basic understanding can further insight and benefit be gained from higher realism.
Limitations and suggestions for future work
Although a useful pilot study with some very insightful feedback comments being provided by the participants, there is certainly scope for research around this topic to be further expanded. While the number of participants (22) was suitable for the type of data analysis carried out, it could certainly be increased to allow for further statistical analysis to be undertaken.
It would also be useful to increase the number of specimens included in such studies, perhaps comparing scans of specimens or regions of varying complexity. It would make sense that increased clarity is more important for particularly complex areas, but this is yet to be investigated. There were also a small number of comments to suggest that the moderate and lower realism scans were too alike, and if undertaking a similar study in the future, these would be more distinct.
Finally, a number of comments indicated that some participants found the majority of existing resources to be too low in terms of realism, and this suggests that there is scope for further investigations around realism not just in terms of 3D models but also 2D illustrations.
Conclusions
The results of this study showed that the overall preference was for the moderate realism scan, with participants finding this to be the best balance between reality and clarity. However, the results also show that the preferred level of realism is not static, rather it varies depending on the target audience and use case. However, one thing that is clear is that the least preferred by far was the low realism scan. This is particularly interesting because the majority of the models found in anatomy apps would likely fall into this category. Although there is no doubt a role for these models to play, there also seems to be an appetite for more realistic models/scans. It is worth mentioning here that there is a difference between scans and models, with scans being created from real specimens and models usually not. The results of this study indicate that best practice is to not edit scans so much that they start to look like generic anatomy models, rather it is preferable to retain at least a moderate degree of realism, with some refining of details potentially useful. As mentioned previously, on occasion it might even be preferable to have more than one version available, with a more edited/clearer scan presented alongside a minimally edited highly realistic version.
Acknowledgements
The author acknowledge Dr Jac Saorsa for her careful and detailed dissection on which the 3D scan is based.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Notes
References
- Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101. doi:10.1191/1478088706qp063oa.
- Eisma, R., Lamb, C., & Soames, R. W. (2013). From formalin to Thiel embalming: What changes? One anatomy department’s experiences. Clinical Anatomy, 26(5), 564–571. doi:10.1002/ca.22222.
- Erolin, C. (2019). Interactive 3D digital models for anatomy and medical education. Advances in Experimental Medicine and Biology, 1138, 1–16. doi:10.1007/978-3-030-14227-8.
- Haragi, M., Hayakawa, M., Watanabe, O., & Takayama, T. (2021). An exploratory study of the efficacy of medical illustration detail for delivering cancer information. Journal of Visual Communication in Medicine, 44(1), 2–11. doi:10.1080/17453054.2020.1834838.
- McCloud, S. (1994). Understanding comics. HarperCollins.
- Scheltema, E., Reay, S., & Piper, G. (2018). Visual representation of medical information: The importance of considering the end-user in the design of medical illustrations. Journal of Visual Communication in Medicine, 41(1), 9–17. doi:10.1080/17453054.2018.1405724.
- Strong, J., & Erolin, C. (2013). Preference for detail in medical illustrations amongst professionals and laypersons. Journal of Visual Communication in Medicine, 36(1–2), 38–43. doi:10.3109/17453054.2013.790793.
- Tiznado-Matzner, G., Bucarey-Arriagada, S., & Pérez, R. L. (2020). Three-dimensional virtual models of 3D-scanned real cadaveric samples used as a complementary educational resource for the study of human anatomy: Undergraduate student’s perception of this new technology. International Journal of Morphology, 38(6), 1686–1692. doi:10.4067/S0717-95022020000601686.
- Trelease, R. B. (2016). From chalkboard, slides, and paper to e-learning: How computing technologies have transformed anatomical sciences education. Anatomical Sciences Education, 9(6), 583–602. doi:10.1002/ase.1620.