Function after hindquarter amputation is poor. When the complete P2, P3 and sometimes also P1 area is resected, the pelvic ring is interrupted, and the ischial tubercle is missing. This can cause problems in sitting and in fitting the exoprosthesis. We describe a method whereby the ipsilateral femur or tibia is harvested after amputation and used as an allograft for reconstruction of the pelvic ring. We report our experience with 3 patients, 2 of whom were alive 1 and 4 years postoperatively. Sitting stability was excellent, and both used their prosthesis without problems.We believe that in selected cases with a large defect in the hemipelvis after resection, this method may improve function and quality of life.
Surgical technique
The patient is positioned semi-prone and the Southern approach is used (Enneking and Dunham Citation1978). After the amputation, the femur or tibia is harvested from the amputated limb. The autograft is stripped from all soft tissue and shaped to fit in the hemipelvectomy defect. The graft is placed with the condyle (femoral or tibial) distally in the pelvis, so that the condyle can serve as a replacement for the ischial tubercle. Good bony contact is aimed at, to facilitate healing. Depending on the remaining pelvic bone, a “side to side” connection can be made to the sacrum and pubis (). If part of the ilium remains, a sleeve can be made in the end of the graft, with which it can be fixed to the ilium (). The graft is clamped in place and fixed with minimal ostheosynthesis, e.g. 2 cancellous screws, just enough for initial stability. Before wound closure, the stability of the implant fixation should be tested. Postoperatively, a bandage is applied for 5 days to prevent edema. After this period, mobilization can be started. If wound healing is uneventful, an exoprosthesis can be fitted. Weight bearing can be resumed from about 2–3 months postoperatively.
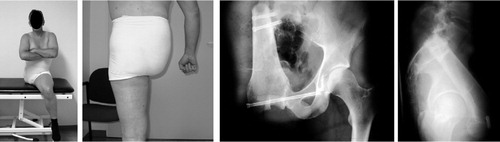
Figure 1. The 62-year-old man, 1 year after operation.

Figure 2. Postoperative status of the 35-year-old man, showing good stability on sitting, good stability on standing, with normal buttock contour, and good positioning and incorporation of the graft.
Cases
The method was used for 3 patients after resection of a large malignant pelvic tumor. One of the patients died of metastatic disease 16 months after the operation. The other 2 were seen at the clinic. In the first (a 62-year-old man), a secondary (post radiation) osteosarcoma was diagnosed, arising from the left ilium, involving the acetabulum. A hindquarter amputation was done, taking the complete ischium, and most of the ilium and ipsilateral pubic bone. The pelvic ring was reconstructed using the ipsilateral proximal tibia. 1 year after the operation, he was able to sit on a chair without support. He used the exoprosthesis without any major problem, could walk with 1 crutch, and even ride his bicycle. Radiographs showed partial incorporation of the graft in what remained of the pelvis ().
The second patient (a 35-year-old man) was diagnosed with a high-grade primary osteosarcoma of the ilium and acetabulum, extending to the sacroiliac joint and ischium. There was no sign of metastatic disease.
After preoperative chemotherapy, hindquarter amputation was done, in which the complete hemipelvis was removed. The pelvic ring was reconstructed with a graft from the distal femur from the amputated leg. The patient was reviewed 4 years after the operation. He was able to sit without support on a normal chair. With his prosthesis, he could walk without walking aids which was strenuous, but with two crutches he could walk up to 4 km in one stretch. The buttock contour was almost normal. On radiographs, the autograft appeared completely incorporated in the remaining pelvic bone ().
Discussion
To our knowledge, no publications have yet addressed the issue of sitting stability and orthesis-fitting after external hemipelvectomy. The method we describe is cheap and is not time consuming. A simple osteosynthesis was sufficient. Incorporation of the graft in the remaining pelvis was successful. Sitting stability was excellent, the newly formed ‘ischial tubercle’apparently serving its purpose. There is no need for extended rib support of the prosthesis. Of course, one would always have to check preoperatively that the graft does not carry bony metastasis. We believe that this method could improve function and quality of life in selected cases where hindquarter amputation would other-wise result in a large defect.
- Enneking W F, Dunham W K. Resection and reconstruction for primary neoplasms involving the innominate bone. J Bone Joint Surg (Am) 1978; 60: 731–46