Abstract
Background Distraction osteogenesis can be used for the treatment of osteomyelitis and nonunion, conditions thought to benefit from increased blood flow in the bone tissue of the distracted limb. We have questioned whether such an increase occurs, and investigated the spatial distribution of bone blood flow after distraction osteogenesis.
Methods The tibiae of 8 rabbits were lengthened 10 mm by a standard midtibial distraction osteogenesis procedure. 2 weeks into the consolidation phase, the bone and soft tissue blood flow of the distracted and the contralateral extremity were measured using radioactive microspheres.
Results The absolute bone blood flow of the distracted tibia was 4% lower than that of the non-distracted side, representing a 41% decrease in the proximal metaphysis, a smaller decrease in the proximal epiphysis, distal metaphysis and distal epiphysis, and an increase in the diaphysis.
Interpretation Mid-tibial distraction osteogenesis redistributed the bone blood flow of the distracted tibia, but absolute tibial blood flow did not increase. Our results do not confirm previous research in this field.
Ilizarov (Citation1989) introduced the idea that distraction osteogenesis increases blood flow in bone tissue of the distracted limb, which could assist treatment of osteomyelitis, pseudarthroses, and critical limb ischemia (Aronson Citation1997). Evidence of such an increase, however, remains weak. Proxy-parameters for blood flow such as Tc-scintigraphy, angiograms, morphological changes in blood vessels, capillary counting, and vascular casting have indicated increases in bone blood flow (Ilizarov Citation1989, Aronson Citation1994, Shevtsov et al. Citation1995, Gil-Albarova et al. Citation1997, DeCoster et al. Citation1999, Rowe et al. Citation1999, Choi et al. Citation2000). These parameters may correlate well with the actual bone blood flow under ideal conditions, but not necessarily under conditions of inflammation and new bone formation. We there-fore questioned whether distraction osteogenesis causes the bone blood flow of the distracted limb to rise, and investigated the spatial distribution of bone blood flow after distraction osteogenesis. We used radioactive microspheres, the gold standard for in vivo blood flow measurements, to assess blood flow in the rabbit hindlimb 2 weeks into the consolidation period of a standard mid-tibial distraction protocol (Nakamura et al. Citation1995, Mizumoto et al. Citation1996, Li et al. 1999).
Methods
Animals
8 New Zealand White rabbits, weighing 3.2–4.7 kg and 6–7 months old, were kept in separate cages, fed a standard diet and allowed to roam freely. The study was approved by the Danish Committee on Animal Experimentation.
Surgery and distraction
A unilateral external fixator (Orthofix M100) with 4 fixation pins was mounted on the right tibia, which was then osteotomized between pin 2 and 3 below the tibiofibular junction with an oscillating saw under saline irrigation. After a 5-day latency period, the right tibia was elongated 1 mm each day with 2 daily increments for 10 days, followed by a 14-day consolidation period. The contralateral nonoperated leg served as control.
The rabbits served as control group in a larger experiment (Eckardt et al. Citation2003), and therefore had a miniosmotic pump implanted in a subcutaneous pouch on the thigh. The pump was connected to the osteotomy site via a subcutaneous polyethylene catheter, delivering 2 mL of 0.1% bovine serum albumin in phosphate buffered saline for 2 weeks at a rate of 0.0001 mL/min. Periosteum, soft tissues and skin were sutured over the osteotomy and catheter.
Blood flow measurement
The requirements and assumptions for using microspheres to accurately measure bone blood flow have been described and reviewed in detail (Hales Citation1974, Brookes and Revell Citation1998). Our experiments followed these guidelines closely without divergence. Briefly, 3 × 106 Strontium-85 labeled 15-μm microspheres, suspended in 10% dextran and 0.01% Tween-20 (New England Nuclear, Boston, MA) were mixed for 5 min by vigorous mixing on a whirlimixer and then injected into the left ventricle of the heart through a catheter (PE 60) via the left common carotid artery which was exposed and ligated. The catheter was positioned under fluoroscopic control. Another catheter (PE 60) was advanced 2–3 cm cranially through the left common carotid artery and placed with its tip below the circle of Willis and connected to a reversed Terumo syringe pump that acted as the reference organ. The correct positioning of the reference catheter following this procedure had been confirmed after killing in pilot studies. Mean arterial blood pressure, heart rate, rectal temperature and blood saturation were monitored to document cardiovascular stability. The microspheres were injected over 30 sec, reference blood samples were withdrawn over 2 min at a rate of 2 mL/min, and the animals were killed with an overdose of barbiturate. The bones were cleaned from attached soft tissue, the distracted tibia was cut on each side of the regenerate and each part was cut into an epiphyseal, metaphyseal and diaphyseal region. Femora were cut into a proximal metaphyseal, diaphyseal and distal metaphyseal region, while tali and calcanei were left whole and metatarsals and digits discarded. Biopsies were sampled from the patellar tendon, the anterior tibial muscle at the level of the osteotomy, and the Achilles tendon. After symmetric sampling from the contralateral side, all samples were distributed into preweighed counting vials and counted in a gamma counter (Packard Cobra 5000; GMI, Inc., Clearwater; MA). Reference blood was collected in similar counting tubes and counted. Counts in each channel were corrected for background radiation.
Counting procedure and determination of regional blood flow
Blood flow in a region was calculated from SR × CREG/CREF, where SR denotes sampling rate, CREF the activity of the reference sample, and CREG the activity of the region. Regional blood flow (RBF) was standardized to 100 mg of tissue.
Statistics
Normality of data was ensured, region by region, by probability plots, and homogeneity of variance was ensured by Bartlett’s test. Symmetrical regions were compared by paired t-test. Retrospective power analyses were performed when the differences between means were not significant, in order to estimate the risk of a type 2 error (β). In order to calculate β, the minimal relevant difference (the effect size) was set at 30%, and the significance level (α) was set at 0.05. Blood flow on the distracted side minus non-distracted side are presented with 95% confidence interval (CI) of the difference in order to highlight non-significant results and facilitate comparisons with the minimal relevant difference.
Results
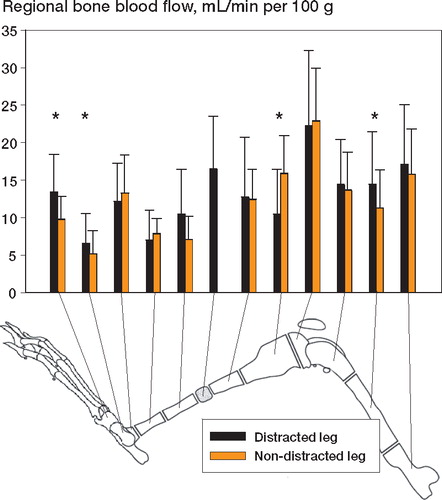
The regional blood flow (RBF) of the distracted tibia was 13.1 mL/min per 100 g, which is 0.6 mL/min per 100 g (95% CI: -3.7–2.5 mL/min per 100 g) or 4% lower than that of the non-distracted tibia (p = 0.6, β= 0.2).This non-significant decrease represented a spatial distribution of the RBF as illustrated in the Figure, which compares the RBF for predefined regions of the distracted leg with those of the non-distracted leg. The blood flow of the proximal tibia metaphysis on the distracted side was 41% lower than the blood flow of the non-distracted side (p = 0.03), and the blood flow of the distal tibia diaphysis was 30% higher than that of the non-distracted side (p = 0.05). Non-significant reductions were found in both proximal and distal epiphyses, and distal metaphysis. The calcaneus and talus blood flows rose on the distracted side also (p = 0.006 and p = 0.01, respectively).
Spatial distribution of regional bone blood flow in rabbit leg after 10 days of mid-tibial callus distraction followed by 14 days of consolidation.Blood flow (with 95% confidence interval) for distracted and non-distracted contralateral leg are shown.The single bar represents the newly formed bone regenerate.Asterisks indicate regions where the difference between sides was significant (p < 0.05). N = 8.
The the absolute bone blood flow of the entire distracted lower extremity increased 0.3 mL/min (95% CI: -0.5–1.0 mL/min), which was an 8% non-significant increase (p = 0.4, β= 0.15). The distracted tibia was 10% heavier than the non-dis-tracted tibia on average (p = 0.02) and the weights of the femora were almost equal. The blood flow of anterior tibial muscle biopsies measured at the level of the osteotomy rose by 30% on the dis-tracted side (p = 0.2) (Table). Patellar tendon blood flow decreased by 54% (p = 0.3) and Achilles tendon blood flow decreased by 40% (p = 0.2) on the distracted side.
Discussion
The process of distraction osteogenesis is thought to provide an angiogenic stimulus to the distracted extremity, resulting in increased blood flow in the bone of the elongated side which lasts several months after distraction (Ilizarov Citation1989, Citation1990, Aronson Citation1994). We have now challenged this dogma, which was introduced by Ilizarov, by reporting that a standard distraction protocol applied to a rabbit model of mid-tibial callus distraction redistributed the blood flow of the distracted limb without affecting the overall blood flow two weeks into the consolidation period. The risk of a type 2 error by concluding that blood flow in the distracted and non-distracted tibiae was equal, calculated by retrospective power analysis, is 20%. Large reductions in blood flow were seen in the juxtaarticular regions of the distracted tibia, whereas the blood flow in the tibial shaft and in the foot increased. This result is surprising and conflicts with previous research in this field.
In previous studies, the angiogenic effects of distraction have been assessed by capillary density in the surrounding soft tissues (Shevtsov et al. Citation1995, Rowe et al. Citation1999), vascular casting of the regenerate (Choi et al. Citation2000), histological changes in bone and soft tissues (Ilizarov Citation1989), arteriography (Mosheiff et al. Citation1996, DeCoster et al. Citation1999), and Doppler analysis of tibial and femoral arterial flows (Gil-Albarova et al. Citation1997). These studies give evidence of increased blood flow in the soft tissues of the distracted extremity, but no evidence of increased bone blood flow. In an excellent experiment, Aronson (Citation1994) used Tc-99 clearance to estimate bone blood flow during and after metaphyseal callus distraction in a canine model. At a time point corresponding to our measurements, he found a 2–3-fold increased blood flow at the distraction site and in bone distal to the osteotomy. Inter-species differences, different age of laboratory animals, and the different features of metaphyseal and diaphyseal distraction may explain the conflicts between our results and the results of Aronson. However, results obtained with Tc-99 scintigraphy should be interpreted with care, because the bone uptake of Tc-99 m increases several times more than the blood flow during the healing of a fracture (Hansen Citation1999), and the soft tissue blood flow may interfere with the Tc-estimation of bone blood flow. In contrast, the microsphere method is the gold standard for precise bone blood flow measurements, and it has achieved high validity for paired comparisons (Brookes and Revell Citation1998). High-quality bone blood flow data in the setting of distraction osteo-genesis has not been reported previously.
The Ilizarov method has been used in the treatment of osteomyelitis and pseudarthrosis—diseases believed to benefit from the increased blood flow distal to the distraction site. Our study indicates that other explanations should also be explored, and that such exploration may give some insight into new treatment modalities for pseudarthrosis and osteomyelitis.
The following are offered as possible explanations for the redistribution phenomenon. The rabbit tibia diaphysis is supplied by two nutrient arteries and at least one of them is injured when periosteum and the soft tissue envelope are lifted off the diaphyseal bone to expose it before osteotomy. Experimental ligation of one nutrient artery resulted in marrow ischemia and an increased cortical flow through a newly developed periosteal network (Brookes and Revell Citation1998). Undisturbed marrow blood flow is about 3 times greater than cortical blood flow (Triffitt and Gregg Citation1990), and thus the flow shift after our operation could reduce metaphyseal RBF and increase diaphyseal RBF. Contractures, pain and osteoporosis are obstacles and problems often encountered during callus distraction (Paley Citation1990). Joint space narrowing, subchondral sclerosis and cysts, resembling changes observed in arthrotic knees, can be seen in distracted limbs (Nakamura et al. Citation1995), as can growth retardation due to premature closure of the growth plate on the distracted side (Lee et al. Citation1993). These phenomena are often explained by increased mechanical loading on the joint and juxtaarticular regions due to contractures after rapid distraction. The reduced juxtaarticular bone blood flow may be rooted in this pathophysiology of the juxtaarticular bone and soft tissues. Alternatively, the reduced RBF may be an important contributor to these events. Stress shielding and disuse of the elongated limb also contributed to the changes observed, although the rabbits ambulated freely without limping.
Distraction of the soft tissue mantle surrounding the regenerate has been reported to result in increased soft tissue capillary density (Anderson et al. Citation1991), proliferation of soft tissue capillaries (Ilizarov Citation1989), increased blood flow in the femoral artery (Gil-Albarova et al. Citation1997), and increased muscle blood flow, as observed in our study. Bone blood flow, and cortical bone blood flow in particular, depends heavily on surrounding soft tissue blood flow due to the vascular anatomy of long bones, and bone blood flow will therefore correlate well with soft tissue blood flow. This correlation may explain the fact that bone blood flow rose in central regions with ample soft tissue coverage, whereas juxtaarticular regions that are covered by tendons and ligaments had a reduced bone blood.
A few methodological considerations regarding bone blood flow measurements should be mentioned. A sufficient number of microspheres must be trapped in each sample to minimize stochastic variations; in practice 150 spheres per sample will give a variation below 10% (Li et al. Citation1989), a requirement fulfilled for bone samples but not for the soft tissue samples in our study. Microsphere injection must not disturb systemic hemodynamics; injection of 2 × 106 microspheres blocks less than 1% of the vascular bed (Davis et al. Citation1990, Brookes and Revell Citation1998), and the quantity of 3 × 106 microspheres we injected is therefore unlikely to have affected hemodynamics. Reference samples must be extracted from an artery in parallel with the bones. Since the Circle of Willis is complete in rabbits, blood passes from the right carotid artery through the Circle of Willis and retrograde into the ligated left carotid artery where we placed our reference sampling catheter (Davis et al. Citation1990). The reference organ contributes to the overall large variation in absolute bone blood flow values, and comparison of operated and nonoperated leg is therefore preferred in order to eliminate the variation of the reference organ. In “Blood Supply of Bone”, Brookes discussed the microsphere method in detail and suggested that the best strategy for determining hemodynamic effects of orthopedic procedures is always to compare the operated limb with its contralateral control (Brookes and Revell Citation1998). The statistics of the Figure are based on paired comparisons and thus offer an unbiased estimation of bone blood flow distribution.
Comparison of bone blood flow recordings from different studies is problematic due to differences in dissection protocols. However, Triffit measured diaphyseal marrow blood flow of the nonoperated leg in rabbits to be 9.08 mL/min per 100 g (standard error (SE): 2.23 mL/min per 100 g, n = 12) and Keller found a diaphyseal blood flow of 3.3 mL/min per 100 g (SE: 0.5 mL/min per 100 g, n = 10) (Triffit and Gregg Citation1990, Keller Citation1991). We recorded a diaphyseal blood flow of 10.2 mL/min per 100 g (SE: 1.5 mL/min per 100 g, n = 8); thus, our results do not diverge from previous studies with respect to magnitude and variation of bone blood flow.
Our study may have weaknesses. The results originate from the control group of an experiment in which a miniosmotic pump implanted into the thigh delivered 2 mL phosphate-buffered saline to the osteotomy gap for 2 weeks at a rate more than 10,000 lower than the absolute tibial blood flow. Saline delivery ceased 2 weeks prior to blood flow measurements, and we therefore believe that this minimal procedure is unlikely to have invalidated our data. Clinically, metaphyseal rather than diaphyseal distraction is often used, which may limit the clinical significance of our results.
In summary, we found that a standard mid-tibial distraction procedure redistributed tibial blood flow, thus reducing the metaphyseal and epiphyseal blood flow and increasing the diaphyseal blood flow, while total tibial blood flow was unchanged. Our results conflict with previous research and they challenge the dogma of increased bone blood flow during limb lengthening.
These experiments were supported by grants from Nordjyllands Amts Research Fund, the Novo Nordisk Fund for Growth and Regeneration, the Obelske Family Fund, the Ib Henriksen Fund, the Stinna and Martinus Sørensen Fund, and the Peder Kristian Tøfting and Dagmar Tøfting Fund.
No competing interests declared.
- Anderson G I, Richards R, R, Paitich B, McKee M, Schemitsch E H. Soft-tissue blood flow after segmental osteotomy of the canine tibia. Ann Plast Surg 1991; 27(1)49–55
- Aronson J. Temporal and spatial increases in blood flow during distraction osteogenesis. Clin Orthop 1994, 301: 124–31
- Aronson J. Limb-lengthening, skeletal reconstruction, and bone transport with the Ilizarov method. J Bone Joint Surg Am 1997; 79(8)1243–58
- Brookes M, Revell W J. Blood supply of bone. 2 ed. Springer-Verlag, New York 1998
- Choi I H, Ahn J H, Chung C Y, Cho T J. Vascular proliferation and blood supply during distraction osteogenesis: a scanning electron microscopic observation. J Orthop Res 2000; 18(5)698–705
- Davis T R, Holloway I, Pooley J. The effect of anaesthesia on the bone blood flow of the rabbit. J Orthop Res 1990; 8(4)479–84
- DeCoster T A, Simpson A H, Wood M, Li G, Kenwright J. Biologic model of bone transport distraction osteogenesis and vascular response. J Orthop Res 1999; 17(2)238–45
- Eckardt H, Bundgaard K G, Christensen K S, Lind M, Hansen E S, Hvid I. Effects of locally applied vascular endothelial growth factor (VEGF) and VEGF-inhibitor to the rabbit tibia during distraction osteogenesis. J Orthop Res 2003; 21(2)335–40
- Gil-Albarova J, Melgosa M, Gil-Albarova O, Canadell J. Soft tissue behavior during limb lengthening: an experimental study in lambs. J Pediatr Orthop B 1997; 6(4)266–73
- Hales J R S. Radioactive microsphere techniques for studies of the circulation. Clin Exp Pharmacol Physiol Suppl 1974; 1: 31–46
- Hansen E S. Tc-disphosphonate uptake and bone hemodynamics. Thesis 1999
- Ilizarov G A. The tension-stress effect on the genesis and growth of tissues: Part II. The influence of the rate and frequency of distraction. Clin Orthop 1989, 239: 263–85
- Ilizarov G A. Clinical application of the tension-stress effect for limb lengthening. Clin Orthop 1990, 250: 8–26
- Keller J. Early hemodynamic response to tibial osteotomy in rabbits: Influence of Indomethacin and Prostaglandin. J Orthop Res 1991; 9(4)539–44
- Lee D Y, Chung C Y, Choi I H. Longitudinal growth of the rabbit tibia after callotasis. J Bone Joint Surg (Br) 1993; 75(6)898–903
- Li G, Bronk J T, Kelly P J. Canine bone blood flow estimated with microspheres. J Orthop Res 1989; 7(1)61–7
- Li G, Simpson A H, Kenwright J, Triffitt J T. Effect of lengthening rate on angiogenesis during distraction osteogenesis. J Orthop Res 1999; 17(3)362–7
- Mizumoto Y, Mizuta H, Nakamura E, Takagi K. Distraction frequency and the gastrocnemius muscle in tibial lengthening. Studies in rabbits. Acta Orthop Scand 1996; 67(6)562–5
- Mosheiff R, Cordey J, Rahn B A, Perren S M, Stein H. The vascular supply to bone in distraction osteoneogenesis: an experimental study. J Bone Joint Surg (Br) 1996; 78(3)497–8
- Nakamura E, Mizuta H, Takagi K. Knee cartilage injury after tibial lengthening. Radiographic and histological studies in rabbits after 3–6 months. Acta Orthop Scand 1995; 66(4)313–6
- Paley D. Problems, obstacles, and complications of limb lengthening by the Ilizarov technique. Clin Orthop 1990, 250: 81–104
- Rowe N M, Mehrara B J, Luchs J S, Dudziak M E, Steinbrech D S, Illei P B, [all names]. Angiogenesis during mandibular distraction osteogenesis. Ann Plast Surg 1999; 42(5)470–5
- Shevtsov V I, Asonova S N, Yerofeyev S A. Morphological characteristics of angiogenesis in the myofascial tissues of a limb elongated by the Ilizarov method. Bull Hosp Jt Dis 1995; 54(2)76–84
- Triffitt P D, Gregg P J. Measurement of blood flow to the tibial diaphysis using 11-microns radioactive micro-spheres. A comparative study in the adult rabbit. J Orthop Res 1990; 8(5)642–5