Abstract
Background Substantial bone loss and bone defects increase the amount of allografting required in hip revision surgery. Thus, the use of a synthetic material to limit the amount of allograft tissue required for impaction grafting is desirable. We evaluated the potential of hydroxyapatite (HA) mixtures to provide initial mechanical stability to a polished tapered femoral stem.
Material and methods We determined the initial stability of a polished tapered femoral stem after reconstructing a cavitary femoral bone defect by impaction bone grafting with cement in Sawbones composite femurs. Three types of graft material were tested for their ability to improve initial rotational stability. The graft materials investigated were pure allograft, a mixture of 50% allograft and 50% hydroxyapatite (HA), and pure HA.
Results We found a statistically significant difference between the three groups as regards torsional micromotion and failure load.
Interpretation Our findings suggest that reconstruction of femoral bone defects with pure HA or a mixture of allograft and HA provides adequate initial stability for femoral revision arthroplasty using impaction grafting.
The objective of impaction bone grafting in the hip is to achieve stability of an implant with the use of compacted, morselized bone graft and subsequently to allow the restoration of living bone stock by bone ingrowth. Many authors have reported good clinical results with restoration of the proximal femoral bone defect (Gie et al. Citation1993, Linder Citation2000, Halliday et al. Citation2003). However, the issue of subsidence of the stem and other complications after femoral impaction grafting has attracted considerable attention (Eldridge et al. Citation1997, Ornstein et al. Citation2000, Blom et al. Citation2002). The complications depend on many factors, including surgical techniques and the physical nature of the graft. It is clear that clinical success requires the attainment of satisfactory mechanical stability of the cemented implant within the packed bone graft preparation, a procedure that is technically demanding.
Reconstruction of this bone loss with tight packing of morselized cancellous bone graft combined with a cemented stem is a standard technique in revision surgery of the hip. However, due to the limited availability of human bone globally and the associated risks of infection and antigenicity of using allogeneic bone, alternatives are being considered as bone graft substitutes (Tomford et al. Citation1981, Bolder et al. Citation2002). Hydroxyapatite (HA) has been suggested as a bone graft substitute for a wide range of applications. This material has a proven osteocompatibility and can act as an osteoconductive material (Kuhne et al. Citation1994, Tsuruga et al. Citation1997).
Forces on the femoral head during stair climbing and rising from a chair cause high torsional loads, which can cause critical micromotion and play an important role in prothesis loosening. Thus, in evaluating femoral prothesis fixation, it is important to measure fixation not only against axial load but also against torsional load (Crowninshield et al. Citation1978, Mjoberg et al. Citation1984).
This study was designed to evaluate the effect of femoral component fixation with impaction grafting by comparing three types of graft material. Micromotions of the implants were measured at the proximal part of the stem under conditions of torsional loading. The hypothesis tested in this study was that pure HA or a mixture of allograft and HA would exhibit a greater degree of relative micromotion than allograft alone in the reconstruction of femoral bone defects.
Material and methods
Implantations were performed using standard impaction bone grafting techniques, and by the same surgeon in order to minimize variability in implantation conditions. All samples were packed into the graft tightly until no further impaction was possible and the phantom could only be moved with extreme difficulty. The bone cement (Osteobond, Zimmer, Warsaw, IN) was vacuum-mixed (Quickvac Mixing System, Zimmer, Warsaw, IN) and injected with a cement gun. The collarless and polished femoral stems (CPT size 1, Zimmer) were implanted into Sawbones composite femurs (Pacific Research Laboratories, Vashon Island, WA) instead of preserved or fresh-frozen bones. These composite bones contain a cortical and spongiform layer, and are specially made for experimental studies using a fiberglass-reinforced epoxy composite with a urethane foam core, and have physical characteristics similar to those of living bone. Since the primary objective of this study was to reveal the differences between implant materials, the composite bones were preferable to cadaver bones because they could provide the same bone geometry for all test specimens. A cavitary defect like a Paprosky type 1 defect was made by curetting the spongiosa of the proximal femur completely.
We tested three kinds of graft materials: 1) pure allograft, 2) a mixture of 50% allograft and 50% HA, and 3) pure HA. The fresh-frozen bone allograft was harvested from human femoral heads that had been donated with the patient's consent. The cancellous allograft was prepared from the femoral heads morselized to 3–5-mm chips using a Tracer Bone Mill machine (Tracer Designs Inc, Santa Paula, CA). The excess fat was removed by washing the allograft with a saline solution. Apaceram HA granules (Asahi Optical, Tokyo, Japan), measuring approximately 2–4 mm, 1–2 mm, 0.6–1 mm, and 0.3–0.6 mm were mixed in a ratio of 1: 1: 1: 1. We tested 3 specimens in each group.
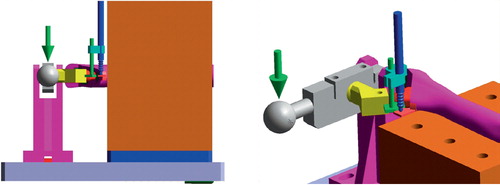
Measurements of relative micromovement between implant and bone were performed using a linearly variable differential transducer (LVDT) (AS-1012; Onosokki, Yokohama, Japan). The LVDT was fixed to the most medial aspect of the medial collar with cyanoacrylate. It was positioned so that the longitudinal access of the transducer was aligned in tangent with the most medial surface of the implant. A metal plate measuring 1 × 1.57 cm was attached to the medial edge of the implant so that it did not engage the bone, or interfere with micromotion (). The LVDT, load, and torque cell outputs were recorded on a digital chart recorder and monitored in real time. From the LVDT data, we determined rotational micromotion and rotational subsidence (Sugiyama et al. Citation1989). Rotational micromotion was defined as the amount of rotational motion between the implant and the bone that was due to the applied torque. Rotational subsidence was the amount of unrecovered micromotion at the completion of each torque application cycle. Total motion was the sum of these two quantities. Torque was applied to the specimen in internal rotation at 0.1 Hz by a ramp waveform. The peak of the ramp was maintained for 5 sec. The first torque cycle was at 4.9 Nm, and subsequent cycles were performed in 2.5 Nm increments until failure occurred. Failure was defined as fracture of the bone, or total motion exceeding 3 mm. The method used in this measurement was a modification of the method described by Whiteside (Sugiyama et al. Citation1989, Otani et al. Citation1993). The data were evaluated for each group and analyzed by the Kruskal-Wallis test. A confidence level of 95% (p < 0.05) was set as a measure of significance.
Figure 1. The LVDTs were fixed to the most medial aspect of the medial calcar and the most medial surface of the implant (left). The upper part of the holder is removed. Rotational load was applied to the specimen in internal rotation (arrow;right).
Results
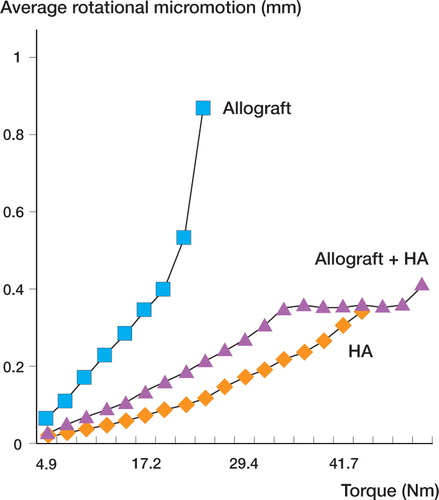
The torsional micromotion increased with an increase in applied torque in all graft types. A significant difference between the three groups was found for the torsional micromotion (p = 0.03). The pure allograft group had a greater mean micromotion than either the pure HA group or the mixture (of allograft and HA) group at a low torque level. In addition, the torque in the pure allograft group just before failure was much lower than in the pure HA group and the mixture group ().
Figure 2. Average rotational micromotion for each group at each torque level. The torque in the pure allograft just before failure was much lower than that in the pure HA group and the group receiving a mixture of allograft and HA.
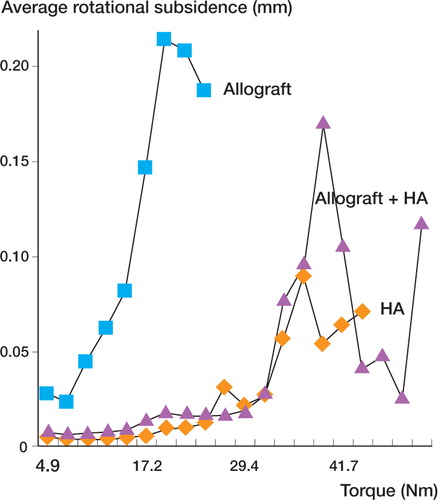
Mean rotational subsidence over the entire torque range for the pure allograft group was greater than for the pure HA group or the mixture group at each torque group. However, all groups showed the same tendency of gradual increase in subsidence with increasing torque levels. The pure HA group and the mixture group had little subsidence at low torque levels (under 30 Nm), but at high torque levels they also showed increasing subsidence with increasing loads (). When total permanent rotational displacement values were compared, there was a significant difference between the three groups (p < 0.001).
Figure 3. Average rotational subsidence for each group at each torque level. The rotational subsidence in the pure allograft group just before failure was larger than that in the pure HA group and the group receiving a mixture of allograft and HA.
The mean failure load was 24 (SD 8.0) Nm for the group grafted with pure allograft, 40 (SD 12) Nm for the group grafted with pure HA, and 45 (SD 13) Nm for the group grafted with a mixture of allograft and HA. A significant difference between the three groups was found. The failure load differed between the groups (p = 0.01).
Discussion
Most surgeons employing impaction grafting use fresh-frozen allograft from femoral heads harvested at primary arthroplasty. Optimum qualities of allograft for use with impaction grafting have not yet been established (Brewster et al. Citation1999), and practice varies among surgeons regarding the extent of removal of cartilage, the size and shape of the morselized fragments, the proportion of cancellous and cortical bone, and the extent to which fat and bone marrow are removed. Procedures intended to ensure the supply of safe allograft for clinical use are well established. As the demand for allografting is likely to increase, it is important that appropriate safeguards are taken to ensure that the safety of both donor and recipient is not compromised. This is especially true regarding impaction grafting cases with severe proximal bone loss, as the amount of bone graft needed may require the use of allograft from multiple donors. Thus, the use of a synthetic material with sufficient mechanical and biological properties to limit the amount of allograft tissue required for impaction grafting is desirable.
Torsional loads may play an important role in loosening of the femoral component of total hip replacements (Mjoberg et al. Citation1984, Sugiyama et al. Citation1989). We have previously shown that implant instability and the resulting changes in prosthetic strain can contribute directly to macrophage activation and osteolysis (Fujishiro et al. Citation2004). In impaction grafting of bone defects after revision hip arthroplasty, the graft behaves as an unstable aggregate. We designed our study to determine whether HA granules are mechanically suitable as a bone graft extender and whether they can provide sufficient structural stability for revision arthroplasty with impaction grafting to withstand the high loads applied to the proximal femur.
We found that adding HA granules to the morselized allograft bone chips as a bone graft extender significantly increased the sample's resistance to rotational micromotion and subsidence in comparison with pure allograft. This suggests that HA mixtures can potentially provide higher initial mechanical stability than pure allograft when used clinically. However, there were no significant differences in micromotion and subsidence tests between pure HA and the mixture of 50% allograft and 50% HA in torsional load tests. We suggest that mechanically, some quantity of allograft bone ‘additive’ may enhance cohesion and adhesion of the otherwise loose mix that is crucial for surgical handling. Adding the HA graft extender would also reduce bone graft variability. Since graft variability is perceived to be the reason for different results achieved in impaction grafting at hip revision (Verdonschot et al. Citation2001), adding HA granules with controllable properties might improve the success rate by providing a more mechanically consistent graft material.
Other authors have also shown improved mechanical properties of allograft after adding synthetic materials. For example, Blom et al. (Citation2002) demonstrated that a porous tricalcium phosphate-hydroxyapatite ceramic exhibits greater mechanical stability and reproducibility than pure allograft. Thus, they concluded that the ceramic tested provided adequate initial stability for use as a bone graft extender in impaction grafting of the femur. Bolder et al. (Citation2003) demonstrated that the initial stability of cemented acetabular cups after reconstructing a combined defect can be augumented by mixing human bone grafts with TCP/HA particles using the impaction grafting technique. Oonishi et al. (Citation1997) presented satisfying mid-term clinical results after acetabular defect reconstruction with impacted HA particles, and showed that one advantage of using HA granules for the management of massive bone deficiency is that a decrease in volume does not occur if the granules are of adequate size and are packed densely and firmly.
Our data suggest that rotational stability is improved with impaction bone grafting using HA particles, but there are still problems. We did not apply an axial load and therefore could only assess the initial rotational stability of the composite in this study. Thus, we cannot conclusively demonstrate that the physiological relevance of the load causes mechanical loosening of the femoral component, because the clinical implications of our results are limited by the in vitro nature of our study. In addition, it is not possible to know the exact mechanical strain force loaded on the femoral component in vivo. Moreover, there are potential problems in using these graft materials in hip surgery, including the poor osteoinductive properties of HA alone, and the different biomechanical characteristics of the HA particles in comparison with human bone grafts. Further work is needed to attempt to answer these questions and thus allow the implementation of meaningfully controlled protocols.
We found that rigid fixation of the femoral component could be achieved with reasonable reliability when impaction bone grafting was performed with HA. From this biomechanical point of view, pure HA or a mixture of HA and allograft are attractive alternatives for morselized bone grafts when using the bone impaction grafting technique in the reconstruction of cavitary defects of the femur.
The authors gratefully acknowledge the assistance of Zimmer Inc. and Asahi Optical Co., Ltd.; however, the authors did not receive payment or other benefits.
- Blom A W, Grimm B, Miles A W, Cunningham J L, Lear-month I D. Subsidence in impaction grafting: the effect of adding a ceramic bone graft extender to bone. Proc Inst Mech Eng [H] 2002; 216(4)265–70
- Bolder S B, Verdonschot N, Schreurs B W, Buma P. Acetabular defect reconstruction with impacted morsellized bone grafts or TCP/HA particles. A study on the mechanical stability of cemented cups in an artificial acetabulum model. Biomaterials 2002; 23(3)659–66
- Bolder S B, Verdonschot N, Schreurs B W, Buma P. The initial stability of cemented acetabular cups can be augmented by mixing morsellized bone grafts with tricalciumphosphate/hydroxyapatite particles in bone impaction grafting. J Arthroplasty 2003; 18(8)1056–63
- Brewster N T, Gillespie W J, Howie C R, Madabhushi S P, Usmani A S, Fairbairn D R. Mechanical considerations in impaction bone grafting. J Bone Joint Surg (Br) 1999; 81(1)118–24
- Crowninshield R D, Johnston R C, Andrews J G, Brand R A. A biomechanical investigation of the human hip. J Biomech 1978; 11(1-2)75–85
- Eldridge J D, Smith E J, Hubble M J, Whitehouse S L, Lear-month I D. Massive early subsidence following femoral impaction grafting. J Arthroplasty 1997; 12(5)535–40
- Fujishiro T, Nishikawa T, Shibanuma N, Akisue T, Takikawa S, Yamamoto T, Yoshiya S, Kurosaka M. Effect of cyclic mechanical stretch and titanium particles on prostaglandin E2 production by human macrophages in vitro. J Biomed Mater Res 2004; 68A(3)531–6
- Gie G A, Linder L, Ling R S, Simon J P, Slooff T J, Timperley A J. Impacted cancellous allografts and cement for revision total hip arthroplasty. J Bone Joint Surg (Br) 1993; 75(1)14–21
- Halliday B R, English H W, Timperley A J, Gie G A, Ling R S. Femoral impaction grafting with cement in revision total hip replacement. Evolution of the technique and results. J Bone Joint Surg (Br) 2003; 85(6)809–17
- Kuhne J H, Bartl R, Frisch B, Hammer C, Jansson V, Zimmer M. Bone formation in coralline hydroxyapatite. Effects of pore size studied in rabbits. Acta Orthop Scand 1994; 65(3)246–52
- Linder L. Cancellous impaction grafting in the human femur: histological and radiographic observations in 6 autopsy femurs and 8 biopsies. Acta Orthop Scand 2000; 71(6)543–52
- Mjoberg B, Hansson L I, Selvik G. Instability of total hip prostheses at rotational stress. A roentgen stereophotogrammetric study. Acta Orthop Scand 1984; 55(5)504–6
- Oonishi H, Iwaki Y, Kin N, Kushitani S, Murata N, Wakitani S, Imoto K. Hydroxyapatite in revision of total hip replacements with massive acetabular defects: 4- to 10-year clinical results. J Bone Joint Surg (Br) 1997; 79(1)87–92
- Ornstein E, Franzen H, Johnsson R, Sundberg M. Radiostereometric analysis in hip revision surgery-optimal time for index examination. 6 patients revised with impacted allografts and cement followed weekly for 6 weeks. Acta Orthop Scand 2000; 71(4)360–4
- Otani T, Whiteside L A, White S E, McCarthy D S. Effects of femoral component material properties on cementless fixation in total hip arthroplasty. A comparison study between carbon composite, titanium alloy, and stainless steel. J Arthroplasty 1993; 8(1)67–74
- Sugiyama H, Whiteside L A, Kaiser A D. Examination of rotational fixation of the femoral component in total hip arthroplasty. A mechanical study of micromovement and acoustic emission. Clin Orthop 1989, 249: 122–8
- Tomford W W, Starkweather R J, Goldman M H. A study of the clinical incidence of infection in the use of banked allograft bone. J Bone Joint Surg (Am) 1981; 63(2)244–8
- Tsuruga E, Takita H, Itoh H, Wakisaka Y, Kuboki Y. Pore size of porous hydroxyapatite as the cell-substratum controls BMP-induced osteogenesis. J Biochem (Tokyo) 1997; 121(2)317–24
- Verdonschot N, van Hal C T, Schreurs B W, Buma P, Huiskes R, Slooff T J. Time-dependent mechanical properties of HA/TCP particles in relation to morsellized bone grafts for use in impaction grafting. J Biomed Mater Res 2001; 58(5)599–604