Abstract
Background Giant cell tumor of bone (GCT) is a bone-destroying tumor that sometimes recurs locally after treatment. A recent study showed increased levels of serum total acid phosphatase (TACP).
Methods We assessed TACP in the serum of 26 patients with primary GCT, and in 5 of them who developed a local recurrence.
Results We found a correlation between TACP level in serum and tumor size. TACP levels that were elevated preoperatively in patients with GCT became normalized after surgery, but increased in 3 of the 5 patients with local recurrence.
Interpretation TACP could be used as a tumor marker for monitoring response to treatment of GCT.
Giant cell tumor of bone (GCT) is a bone-destroying tumor which occurs most often in the third or fourth decade of life. Local recurrence after treatment is not uncommon, but metastatic disease is rare. Histologically, GCT consists of a large number of osteoclast-like multinucleated giant cells which secrete one subtype of acid phosphatases (ACP): tartrate-resistant acid phosphatase (TRAP) (Bull et al. Citation2002). One clinical report indicated that serum TRAP may be useful for the differential diagnosis of GCT (Yoshikawa et al. Citation1992). A recent study showed that some patients with GCT have high levels of total serum acid phosphatase (TACP) (Goto et al. Citation2001), which can be measured routinely in hospital clinical laboratories. This finding prompted us to examine the clinical significance of serum TACP in GCT, because measurement of serum TRAP has not yet been incorporated into routine clinical laboratories (Bull et al. Citation2002).
Patients and methods
Between 1995 and 2002, 26 adult patients with GCT were treated in our hospital (mean age 36 (16–66) years). 6 patients were treated with curettage and cementation, 10 had curettage followed by bone grafting, and the remaining 10 had endoprosthetic reconstruction because of pathological fractures. The patients were followed for an average of 4 (0.2–8) years. Serum TACP was measured with an automatic serum examination apparatus (Clinical Analyzer 7170; Hitachi High Technologies, Tokyo, Japan) at the time of the patient's first visit to our hospital, and periodically postoperatively in conjunction with radiological imaging. Normal TACP levels at our hospital are 3.5–13.1 U/L. We also measured prostate-specific antigen (PSA) in 4 male patients older than 50 (51–62) years to exclude prostate cancer, which is often associated with elevated levels ACP of prostatic origin. All had normal PSA values. Three-dimensional tumor size was determined on CT scans taken at the time of diagnosis. The association between serum TACP level and tumor size was investigated by correlation analysis. The difference between pre- and postoperative value was analyzed using the unpaired t-test.
Results
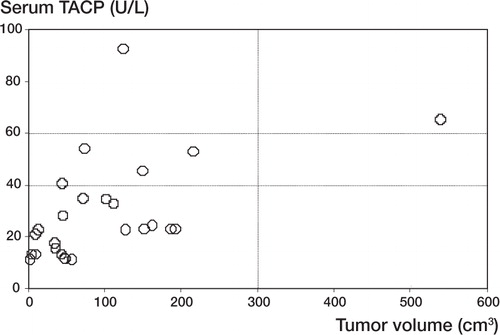
Preoperative serum TACP levels were high in 19 of the 26 patients. There was a significant positive correlation between serum TACP level and tumor size (r = 0.52; p = 0.007) (). The high serum TACP levels seen preoperatively decreased to normal levels immediately after tumor removal in 18 of 19 patients. In the 7 GCT patients with a normal TACP level preoperatively, it remained normal postoperatively. The difference between pre- and postoperative values was statistically significant (preoperative mean value 28 U/L; postoperative mean value 13 U/L; p < 0.001).
Figure 1. Correlation between serum TACP level and volume of tumor in 26 patients with GCT. There was a significant positive correlation (r = 0.52; p = 0.007).
5 patients, all with normalized TACP levels post-operatively, had local recurrence, and 3 of these developed re-elevated TACP levels ().
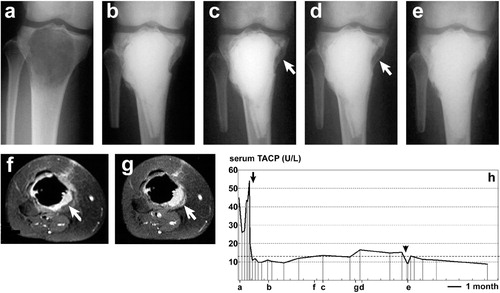
Figure 2. Changes in serum TACP level (panel h) and radiographic images (panels a to g) from one of the GCT patients with local recurrence (a 16-year-old woman). Radiographs of the right tibia with anteroposterior view (a to e) and axial magnetic resonance images of gadolinium-enhanced with fat saturation (TR 400/TE 13) (f, g) were obtained during the pre- and postoperative course. The lower-case letters corresponding to panels a–g represent the time course of examinations shown in the x-axis of the graph (panel h). A continuous decline in TACP level was observed after the first curettage followed by grafting of autologous bone and tricalcium phosphate (black arrow). Re-elevated TACP level accompanying local recurrence was observed and confirmed by radiological imaging (white arrows in panels f, c, g and d). Re-operation with curettage and tricalcium phosphate graft resulted in a reduction of the level to within normal range (black arrow-head).
3 of the 5 patients with local recurrence had a high serum TACP level at recurrence ().
Discussion
There are 5 acid phosphatase (ACP) isoenzymes in humans: lysosomal ACP (LAP), prostatic ACP (PAP), erythrocytic ACP (EAP), macrophage ACP (MAP), and tartrate-resistant ACP (TRAP) (Bull et al. Citation2002). PAP has been used extensively as a serum marker for cancer of the prostate (Henneberry et al. Citation1979), LAP deficiency is an autosomal recessive disorder affecting metabolism (Nadler and Egan Citation1970), and TRAP plays an important role in bone resorption (Lam et al. Citation1984). In bone tumors, since TRAP has been found to be expressed in the multinucleated giant cells in GCT by immunohistochemistry (Clohisy et al. Citation1993), serum TRAP may represent a tumor marker of GCT (Yoshikawa et al. Citation1992). Currently, however, immunoassays for detection of osteoclast-derived TRAP in serum are still under development because of wide differences in methodological protocols and in standard values between research groups (Bull et al. Citation2002).
A recent study indicated high serum TACP in 5 of 9 cases of GCT (Goto et al. Citation2001), and all of these 5 cases showed normal values postoperatively. We found that serum TACP level in GCT patients correlates with tumor size (). The high preoperative TACP values in GCT patients became normalized after surgery, but reappeared in 3 of 5 patients with local recurrence (). We included only adult GCT patients, as children and adolescents have higher serum TACP values because of higher bone turnover (Chen et al. Citation1979).
Our findings indicate that serum TACP measurements may be useful in routine follow-up of patients treated for GCT.
No competing interests declared.
Related Research Data
- Bull H, Murray P G, Thomas D, Fraser A M, Nelson P N. Acid phosphatases. Mol Pathol 2002; 55: 65–72
- Chen J, Yam L T, Janckila A J, Li C-Y, Lam W K W. Significance of ‘high’ acid phosphatase activity in the serum of normal children. Clin Chem 1979; 25: 719–22
- Clohisy D R, Vorlicky L, Oegema T R, Jr, Snover D, Thompson R C, Jr. Histochemical and immunohistochemical characterization of cells constituting the giant cell tumor of bone. Clin Orthop 1993; 287: 259–65
- Goto T, Iijima T, Kawano H, Yamamoto A, Arai M, Matsuda K, Yokokura S. Serum acid phosphatase as a tumour arker in giant cell tumour of bone. Arch Orthop Trauma Surg 2001; 121: 411–3
- Henneberry M O, Engel G, Grayhack J T. Acid phosphatase. Urol Clin North Am 1979; 6: 629–41
- Lam K-W, Dannaher C, Letchford S, Eastlund T, Li C-Y, Yam L T. Tartrate-resistant acid phosphatase in serum of cancer patients. Clin Chem 1984; 30: 457–9
- Nadler H L, Egan T J. Deficiency of lysosomal acid phosphatase. A new familial metabolic disorder. N Engl J Med 1970; 282: 302–7
- Yoshikawa H, Uchida A, Kudawara I, Ono K. Serum tartrate-resistant acid phosphatase as a tumor marker in giant cell tumor of bone. Calcif Tissue Int 1992; 50: 43