Abstract
Background The occurrence of club foot (CF) varies between countries and populations, and may be related to endogenous and exogenous factors. We analyzed the occurrence of CF in a whole country over a long period of time (16 years).
Methods Patients born in Denmark with a foot deformity 1978–93 were identified from the National Patient Register and the Register of Inborn Malformations. The records for each patient were studied in the hospital departments to establish the diagnoses and to obtain additional information. Demographic data were obtained from the Danish National Demographical Institute and from the Danish Population Register.
Results The incidence of isolated CF was 1.2/1,000 live births. It increased significantly during the study period, and the incidence of CF and the standardized morbidity ratio for CF were significantly positively correlated to population densities in the counties and the districts. There was no significant increase in the relative proportion of children with CF born to non-Scandina-vian parents during the period.
Interpretation The increasing incidence of isolated CF with higher population density indicates that there may be exogenous factors that are pathogenic.
The regular occurrence of inborn foot deformities has been recognized since ancient times. They appear as isolated foot deformities or as part of syndromes, e.g. multiple arthrogryposis, chromosomal abnormalities, aplasia of fibula, spina bifida etc.
The incidence of club foot (CF) varies between countries, e.g. CF is 4–6 times as common in the Far East than in Europe (Hanify et al. Citation1980, Boo and Ong Citation1990). This has been suggested to be caused to some extent by differences in genetic disposition (Lochmiller et al. Citation1998), and therefore immigration may lead to changes in the incidence over time. At the same time, environmental and other exogenous factors may lead to geographic clustering of inborn foot deformities, e.g. deformities related to medication (Gonzalez et al. Citation1998), occupational exposure (Kristensen et al. Citation1997), altitude (Castilla et al. Citation1999), and socioeconomic inequalities (Vrijheid et al. Citation2000). Thus, it is essential to map the incidences of the different foot deformities to monitor changes over time. Geographic variation in a whole country has not been studied before.
In Denmark, healthcare is public, and all admissions to hospitals are reported to one register (Andersen et al. Citation1999) covering the whole country. In addition, inborn malformations were reported to a national register between 1983 and 1994 (Christensen and Knudsen Citation1998). By identifying patients with inborn foot deformities from the two national registers and examining the hospital records on location, including all clinical information for each person, it was possible to minimize the number of unrecognized cases and erroneous diagnoses. In addition, detailed statistical information about the population is available, making calculations of geographical variations possible.
We analyzed the incidence of CF in Denmark, including geographical variations, over a long period of time, and related it to other inborn malformations in the children.
Subjects and methods
The person and patient registers in Denmark
Everyone living in Denmark (not counting Greenland and the Faeroe Islands) has a personal ID number (birth date (6 digits) and a unique suffix (4 digits)). The number is exclusive to an individual and is not changed during a person's life. All inhabitants are listed in the Danish Population Register (DPR), which includes information about gender, marital status, address, birthplace, present and any previous citizenship, and the personal ID numbers of parents and children.
Since January 1, 1978, all hospitals in Denmark have reported well-defined patient information to the Danish National Patient Register (NPR), including personal ID number, admission period, hospital, department, diagnoses and treatments (according to the WHO classification codes), address of the patient, death, and so on. This register mainly contains information about all diseases diagnosed and treated during admission to a particular hospital in Denmark.
The Danish Register of Inborn Malformations (RIM) was established by the Danish Board of Health in 1983. The aim was to register all inborn malformations in children in Denmark, no matter whether they were diagnosed: during admission to hospital or in an outpatient clinic. All doctors had an obligation to report to this register. The reports contain information about ID number of the child, mother and father, address and employment history of mother and father, the sort of malformation (described in writing), length of pregnancy, birth weight and length, and so on. The malformations were coded by the Danish Board of Health according to an internal coding system and all information was stored electronically. The register was closed at the end of 1994, as it was felt that the occurrence of inborn malformations could be monitored sufficiently by the NPR.
Between 1965 and 1993, the eighth revision of the WHO classification system for diseases was used in Denmark. The 9th revision was never used in Denmark, but the 10th revision—which was basically a new classification system—was introduced January 1, 1994. Thus, the same system for coding diagnoses in the NPR was used during the period 1978–1993.
Methods
Information about children with inborn foot deformities was obtained from the NPR and the RIM. As a new revision of the WHO classification codes was introduced in 1994, the period 1978–1993 was chosen for obtaining information from the NPR. Information from the RIM was obtained for the period 1983–1993. The extent to which inborn foot deformities were coded correctly in the two registers was not known; thus, we studied a broad choice of diagnoses covering inborn foot deformities.
From the NPR, we identified individuals with the following WHO diagnoses: pes equino-varus-adductus (75,400), pes calcaneo-valgus (75,402), pes metatarso-varus (75,401), malformatio congenita extremitas, alia et non specificata (75,599), malformatio congenita ossium et articulorum extremitas inferioris alia (75,579), arthrogryposis multiplex congenita (75,589), malformatio congenita ossium et musculorum, tendinis et fascia alia specificata (75,699), talipes congenitus (75,409), talipes congenitus alius definitus (75,408), aplasia, hypoplasia fibulae (75,533), reductio congenita extremitas inferioris alia definata (75,538), aplasia, hypoplasia tibia (75,534). For the persons identified, the following information was obtained: personal ID number, admission period, hospital and department for the admission(s) with the diagnoses and all following admissions for the patient (irrespective of diagnosis), all diagnoses and treatments (according to the WHO classification codes) for all admissions, address of the patient (district and county), and deaths.
From the RIM, we identified individuals with the following diagnoses (according to the internal coding manual of the Danish Board of Health): pes equinovarus, pes varus, pes metatarsus varus, pes calcaneovalgus, pes calcaneus, pes valgus, hypo-plasia/aplasia fibulae, arthrogryposis multiplex, other malformations of the feet, other malformations of the arms/legs. Information about personal ID number was obtained, and for all these people, information (as described above) was obtained from the NPR.
The personal ID numbers and present and previous citizenships of the parents of the children identified as described above were obtained from the DPR.
We studied the patient records (hospital paper reports, imaging investigations etc.) for each admission. A database was developed in MS-Access by author PKJ, and relevant data (see below) were transferred directly to the database. 5 of the authors registered the data. A coding manual was used after consensus had been established regarding interpretation of more difficult or “unclear” text or data in the journals. In cases of doubtful diagnoses, or mismatch of text, data, and/or diagnosis, the first author (MRK) decided how to deal with that particular case to ensure a high degree of consistency in the coding procedure.
For each patient, information was registered in the database concerning chromosomal abnormalities, multiple malformations (defined as additional malformations except in bones and joints), whether the child was alive or dead at birth, the personal ID number of the mother, and the mother's address at the time of birth.
Based on the information from the hospital records (including the clinicians’ description of the foot), the diagnosis for each patient was established. CF was defined as irreduceable equinus, varus of the hindfoot and adduction of the forefoot and an “empty” heel pad (soft heel because of a high calcaneus). Most patients were seen by several clinicians, and in some cases an unspecific diagnosis of “foot deformity” was made by the first clinician (often a junior doctor) and later corrected by the orthopedic surgeon. In all cases the most specific diagnosis was used in the study, and the authors specifically made sure that the diagnosis was in accordance with the clinical description of the foot.
When radiographs had been taken (which was the case for 470 of the 1,126 feet with isolated CF), the description was studied and they were used to confirm the diagnosis: the TC-angle (the angle between the axis of calcaneus and talus) in lateral and anterior-posterior views were reduced (the sum < 35 degrees).
From the Danish National Demographical Institute, we obtained demographic information for each sex about the number of births in each community and county. Denmark is divided into 15 counties, which are further divided into 276 districts.
For each child, we obtained information about the parents’ birthplace and citizenship from the DPR to establish whether a parent was of Scandinavian or non-Scandinavian origin.
The study protocol was approved by the Danish Board of Health, the Danish Data Register, and the local ethics committee. The patients were not contacted. Each ward was asked for permission to go through the hospital records.
Statistics
We used the Poisson model to investigate the development of the incidence of club foot over time for girls and boys. The dependence of the incidence on time was assumed to be log-linear, i.e. the percentwise change of incidence between 2 consecutive years was assumed to be constant. The model was investigated using a goodness-of-fit statistic for overdispersion.
The Poisson model was also used to investigate whether the incidence of club foot in children born to parents living in densely populated neighborhoods was higher than the incidence in sparsely populated areas. The neighborhoods were split into 4 groups corresponding to the quartiles of the density of the neighborhoods, and the hypothesis of equal incidences across the 4 groups was tested in the Poisson model, including also sex.
The Chi-square-distributed deviance was used as the test criterion, and p-values below 5% were considered significant.
The expected numbers (E) of CF in the 15 counties of Denmark and in areas with different population densities were calculated as the number of births in each region multiplied by the incidences of CF in Denmark (calculated for boys and girls separately and then summed). The standardized morbidity ratio (SMR) for each region was calculated as the observed number of cases (n) divided by the expected number of cases. The 95% confidence limits for SMR were calculated as follows:
lower limit = SMR / exp (1.96/√n) and upper limit = SMR exp (1.96/√n)
Results
6,530 individuals born in Denmark with CF (13,621 admissions) were identified from the NPR and RIM.
The patient files for 12,924 admissions were available (corresponding to 96% of all admissions). 62 subjects were stillbirths. For 96 individuals (representing 1.5% of all), the diagnoses could not be established from the patient files. Excluding these cases and stillbirths, 6,372 patients remained for the study. During the 16-year period, the number of births was 936,525, of which 478,508 were boys and 457,017 were girls. We found 1,126 children with isolated CF (). Of these, 10 were registered in the RIM only and not in the NPR.
Table 1. The total numbers and incidences (n/1000 live Incidence (number of club foot) / 1000 live births births) of inborn club foot in Denmark during 1978–1993 among 936,525 births. Isolated cases were defined as foot deformities in children with no chromosomal abnormalities, syndromes, multiple malformations, multiple arthrogryposis or aplasia of the tibia or fibula. Combined cases were foot deformities in children with one or more of these conditions
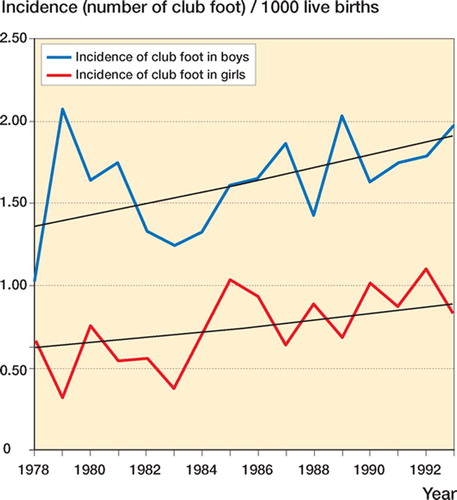
We found no overdispersion in the model allowing for different development of the incidence of club foot over time (p = 0.074). Thus, the log-linear effect of time is reasonable, and the model provides a good description of the data. The percentwise change over time was no different between the two sexes (p = 0.07), i.e. the ratio between boys and girls remained constant over time. The incidence for the boys was 2.190 (CI 1.93–2.49, p < 0.001) times that of girls. The increase of the incidence was 1.024 (CI 1.011–1.04, p < 0.001) per year, or 1.43 over the 15-year period, corresponding to an increase of 43% from 1978 to 1993 ().
Figure 1. The yearly incidence (n/1,000 live births) of isolated club foot (CF) in Denmark 1978–1993 among 936,525 births. The smooth curve is the model-based (estimated) incidence in the model with constant boy-girl ratio. There was a significant increase in incidence during the period for both sexes, and also for boys and girls separately (p < 0.001).
We found a significant difference in the incidence across neighborhoods with different densities (p = 0.005). Comparing with the 25% most sparsely populated areas, the incidence was 1.17, 1.46, and 1.35 times greater for the areas in the relative density range 25%–50%, 50–75% and above 75%.
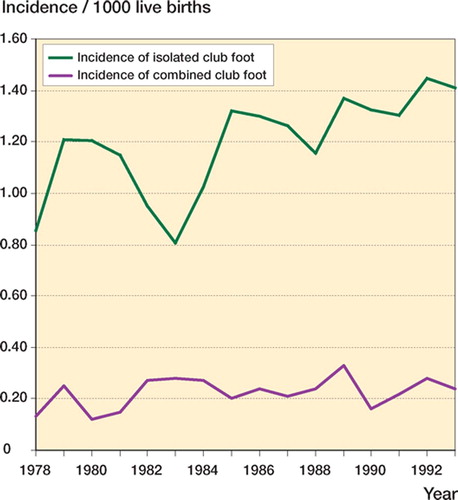
The incidence of CF changed over time (). The changes in the incidence mainly occurred among cases with isolated CF.
Figure 2. The yearly incidence (n/100,000 live births) of club foot (CF) in Denmark 1978–1993 among 936,525 births, divided into cases of isolated CF and cases of CF combined with chromosomal defects, multiple malformations, aplasia of the tibia/fibula, or multiple arthrogryposis.
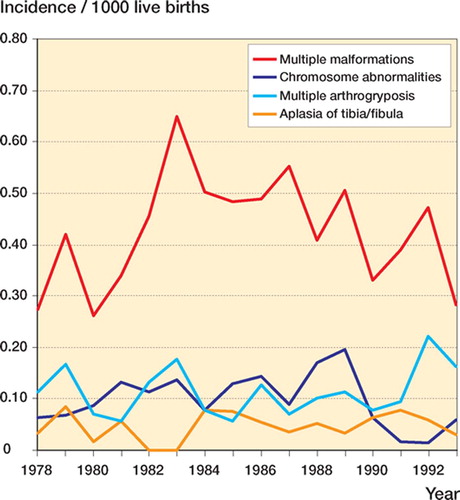
There was no change in the annual incidences of chromosomal abnormalities, multiple malformations, aplasia of the tibia or fibula, or multiple arthrogryposis over time ().
Figure 3. The yearly incidences (n/1,000 live births) among 936,525 births in Denmark 1978–1993 of children with chromosomal abnormalities (dark blue), multiple malformations (red), aplasia of the tibia or fibula (yellow), and multiple arthrogryposis (light blue). There were no significant changes over time.
We found no statistical difference in the standardized morbidity ratio for isolated CF between the 15 counties ().
Table 2. The numbers and (in parentheses) incidences (n/1000 live births) of isolated club foot in each county in Denmark 1978–1993, among 936,525 births. The standard morbidity ratio (SMR) in each county for clubfoot is listed followed by 95% CI
The incidences of isolated and combined CF in the 30 districts of Denmark with the highest population density (more than 500 inhabitants/km2) was 1.35, respective 0.19 per 1,000 live births. The calculated standardized morbidity ratio was significantly increased to 1.12 (CI 1.02–1.23) for isolated CF, and reduced to 0.84 (CI 0.65–1.08) for combined CF in these communities (not significant).
There was a significant increase in population density with increasing incidence of CF in both sexes (p < 0.001) ().
Table 3. The incidences of isolated clubfoot (n/1000 live births) in Denmark 1978–1993 among 936,525 births, related to population density (number of inhabitants/km2 divided into 10 groups). SMR = standard morbidity ratio (observed number/expected number)
Over the whole period we found a small, statistically insignificant increase in the annual percen tage of children with parents (either one or both) of non-Scandinavian origin among the cases of isolated CF.
Discussion
This is the first study to examine the epide miology of CF in a whole country over a long period of time.
The validity of patient registers depends on se veral factors. For severe diseases, particularly if they require admissions to hospital, the registrations are usually quite complete (e. g. 90–94% in Crohn's disease when compared with a register of pathological specimens) (Fonager et al. Citation1997), whereas often less than 50% of the cases are registered for diseases with a less severe course, or chronic diseases that can be treated in outpatient clinics (e.g. 8% of patients with arterial hypertension, relative to a primary healthcare registration) (Allebeck and Lindberg Citation1984). CF is generally regarded as a severe condition that can result in substantial disability if not treated. All children in Denmark are examined after birth by a doctor who is usually not an orthopedic specialist, and who might tend to suspect CF in some cases of metatarsus varus foot or calcaneo-valgus foot (to be on the safe side). So when the registration is filled in, inordinately many cases of CF may be registered, or the doctors may use more unspecific diagnoses. This is why it was necessary in this study to go through all patient files to establish the diagnoses, and to identify persons with a broader spectrum of diagnoses (e.g. “malformatio congenita extremitas, alia et non specificata”). On the other hand, CF will require treatment—traditionally often surgery— and as we identified all individuals born 1978–93 with a diagnosis of an inborn foot deformity at any time during childhood, the risk that a CF was not registered in the NPR at least once must be very small. Between 1983 and 1993, we only identified 10 children with CF in the RIM who had not been registered in the NPR.
The incidence of CF in this study (1.2 per thousand) is a little higher than seen in other studies of European or North American children. In Malmö, Sweden, an overall incidence of 0.93/1,000 was found among all births in the city in the period 1946–1990, but with a slight tendency toward increase (Danielsson Citation1992). In Scotland, different surveys have revealed incidences of 0.64/1,000 (Wynne-Davies et al. Citation1982) and 0.89/1,000 live births (Barker and Macnicol Citation2002), whereas 1.26/1,000 was found in southern England in the 1960s (Wynne-Davies Citation1964). In a study of routine ultrasound examination at 18–23 weeks’ gestation in 103,228 mothers, Bakalis et al. (Citation2002) found 107 cases of fetal CF (an incidence of 1.0/1,000), of which only 51% were isolated deformities. Even though most of the pregnancies with combined deformities terminated in abortion, bringing the proportion of combined CF down to about 20% in live births, the incidence of isolated CF was only 0.53/1,000 (Bakalis et al. Citation2002). In North and South America, incidences of about 1/1,000 have been reported (Castilla et al. Citation1999). So among western countries, there appears to be a 2-fold variation in the reported incidence of CF, with our series at the high end. In India, a CF prevalence of 0.9/1,000 was seen among 50,055 individuals in a population survey (Mittal et al. Citation1993). An up to 5-fold higher incidence has been found in Maori and Polynesian people (Hanify et al. Citation1980, Boo and Ong Citation1990).
There are geographic variations in the incidence of CF, being higher in the Far East (about 4.5/1,000) (Boo and Ong Citation1990) and among the black population of South Africa (about 3.5/1,000) (Pompe van Meerdervoort Citation1976). Genetic disposition has been suggested as an explanation of these differences, but the geographic variation within a country has not been studied before. We found the incidence and risk of CF to be positively related to population density in the counties and in the districts. The cause of this could be endogenous as well as exogenous. Generally, in areas with a high population density, exposure to environmental stress (traffic, pollution, noise) as well as the stress of urban living (including misuse of alcohol, tobacco and drugs) is more intense than in areas of low population density. The number of daily person-to-person contacts is higher, leading to a higher exposure to infections. Exposure of the father to toxic agents in paint or from the printing business has been suspected to increase the risk of CF in the offspring (Olsen Citation1982, Olshan et al. Citation1991), but it has not been possible to reproduce this finding in other studies (Irgens et al. Citation2000). Because of a seasonal variation in the number of children born with CF, it has been suggested that infection with enterovirus may be responsible for some cases of CF (Robertson and Corbett Citation1997), but even though some variation with time has been demonstrated in other studies, the results are not uniform and they are based on quite small numbers (Barker and Macnicol Citation2002). In a large series from South America and Italy, no seasonal variation could be found for CF (Castilla et al. Citation1990). Many other differences between high and low population density areas (e.g. eating habits and type of work) can theoretically be exogenous factors influencing the risk of giving birth to a child with CF. The increase in the population density in Danish cities during the 16-year period, and its consequences for individuals, could be a reason for the increasing incidence of CF. Alderman demonstrated that the odds ratio for CF in boys was 2.6 in mothers who smoked, compared to non-smokers (Alderman et al. Citation1991), and this also supports the possibility that exogenous factors are related to the risk of being born with CF.
CF defined after strict criteria, that exclude soft, fully reduceable club-foot-like feet, were found in isolation in 84% of cases, and found in connection with other malformations in 16% of cases. The risk of having CF is higher in boys than in girls (Wynne-Davies Citation1964, Wynne Davies et al. Citation1982, Alderman et al. Citation1991, Danielsson Citation1992, Lochmiller et al. Citation1998, Bakalis et al. Citation2002, Barker and Macnicol Citation2002). In our series, the incidence of CF in isolation was 2.2 times higher in boys than in girls, but in CF combined with other malformations the ratio was only 1.4. This suggests that CF is a multigenetic disease, partly related to genetic information on the sex chromosomes, and partly to information on other chromosomes and exogenous factors.
The significant increase in incidence of CF during the 16-year period may have been caused by both exogenous and endogenous (genetic) factors. That the increase is mainly seen in isolated CF—and not in CF combined with other malforma-tions—makes it most likely that exogenous factors play an important role. There was a small, insignificant increase in the relative number of pa rents from countries outside Scandinavia during the last years of the study period among the children with CF, but this shift in the genetic pool was not large enough in itself to explain the steady increase in incidence during most of the study period.
This study has been supported by grants from the SAHVA Foundation (the Society for Handicapped and Disabled), the Danish Orthopaedic Society Foundation, and the Vanføre Fund.
No competing interests declared.
Contributions of authors
MK project setup, planning, data collection, data interpretation, presentation in writing, PKJ planning, programming, data manufacturing, IK, HH, JL and BH-C planning, data collection, KL statistics, SBC and SS-H planning and data interpretation.
- Alderman B W, Takahashi E R, LeMier M K. Risk indicators for talipes equinovarus in Washington State, 1987-89. Epidemiology 1991; 2: 289–92
- Allebeck P, Lindberg G. Rheumatic diseases in a health interview survey and in inpatient care. A record linkage study on two registers. Scand J Soc Med 1984; 12: 147–54
- Andersen T F, Madsen M, Jørgensen J, Mellemkjær L, Olsen J H. The Danish National Hospital Register. A valuable source of data for modern health sciences. Dan Med Bull 1999; 46: 263–8
- Bakalis S, Sairam S, Homfray T, Harrington K, Nicolaides K, Thilaganathan B. Outcome of antenatally diagnosed talipes equinovarus in an unselected obstetric population. Ultrasound Obstet Gynecol 2002; 20: 226–9
- Barker S L, Macnicol M F. Seasonal distribution of idiopathic congenital talipes equinovarus in Scotland. J Pediatr Orthop B 2002; 11: 129–33
- Boo N Y, Ong L C. Congenital talipes in Malaysian neonates: incidence, pattern and associated factors. Singapore Med J 1990; 31: 539–42
- Castilla E E, Orioli I M, Lugarinho R, Dutra G P, Lopez-Camelo J S, Campana H E, Spagnolo A, Mastroiacovo P. Monthly and seasonal variations in the frequency of congenital anomalies. Int J Epidemiol 1990; 19: 399–404
- Castilla E E, Lopez-Camelo J S, Campana H E. Altitude as a risk factor for congenital anomalies. Am J Med Genet 1999; 86: 9–14
- Christensen K, Knudsen L B. Registration of congenital malformations in Denmark. Dan Med Bull 1998; 45: 91–4
- Danielsson L G. Incidence of congenital clubfoot in Sweden. 128 cases in 138,000 infants 1946-1990 in Malmo. Acta Orthop Scand 1992; 63: 424–6
- Fonager K, Sørensen H T, Olsen J. Change in incidence of Crohn's disease and ulceratice colitis in Denmark. A study based on the national registry of patients, 1981–92. Int J Epidemiol 1997; 26: 1003–8
- Gonzalez C H, Marques-Dias M J, Kim C A, Sugayama S M. M, da Paz J A, Huson S M, Holmes L B. Congenital abnormalities in Brazilian children associated with misoprostol misuse in first trimester of pregnancy. Lancet 1998; 351: 1624–7
- Hanify J A, Metcalf P, Nobbs C L, Worsley K J. Congenital malformations in the newborn in Northland: 1966-1977. N Z Med J 1980; 92: 245–8
- Irgens Å, Krüger K, Skorve A H, Irgens L M. Birth defects and paternal occupational exposure. Hypotheses tested in a record linkage based dataset. Acta Obstet Gynecol Scand 2000; 79: 465–70
- Kristensen P, Irgens L M, Andersen A, Bye A S, Sundheim L. Birth defects among offspring of Norwegian farmers, 1967-91. Epidemiology 1997; 8: 537–44
- Lochmiller C L, Johnston D, Scott A, Risman M, Hecht J T. Genetic epidemiology study of idiopathic talipes equi novarus. Am J Med Genet 1998; 79: 90–6
- Mittal R L, Sekhon A S, Singh G, Thakral H. The prevalence of congenital orthopaedic anomalities in a rural community. Int Orthop 1993; 17: 11–2
- Olsen J. Risk of exposure to teratogenes amongst laboratory staff and painters. D Med Bull. 1982; 30: 24–8
- Olshan A F, Tschenke K, Baird P A. Paternal occupation and congenital anomalies in offspring. Am J Ind Med 1991; 20: 447–75
- Pompe van Meerdervoort H F. Congenital musculoskeletal malformation in South African blacks: a study of incidence. S Afr Med J 1976; 50: 1853–5
- Robertson W W, Jr, Corbett D. Congenital clubfoot. Month of conception. Clin Orthop 1997, 338: 14–8
- Vrijheid M, Dolk H, Stone D, Abramsky L, Alberman E, Scott J E. S. Socioeconomic inequalities in risk of congenital anomaly. Arch Dis Child 2000; 82: 349–52
- Wynne-Davies R. Family studies and the cause of congenital club foot. Talipes equinovarus, talipes calcaneo-valgus and metatarsus varus. J Bone Joint Surg (Br) 1964; 46: 445–63
- Wynne-Davies R, Littlejohn A, Gormley J. Aetiology and interrelationship of some common skeletal deformities (talipes equinovarus and calcaneovalgus, metatarsus varus, congenital dislocation of the hip and infantile idiopathic scoliosis). J Med Genet 1982; 19: 321–8