Abstract
Background Idiopathic clubfoot is one of the most common congenital orthopedic problems. Nationwide studies of the incidence are scarce. We performed a prospective multicenter study in order to assess the cumulative incidence in Sweden over 2 consecutive years.
Patients and methods 44 clinics identified as treating clubfoot reported new cases prospectively. The medical records of 280 children with clubfoot born during 1995– 1996 were collected and analyzed with special reference to gender, regional distribution and seasonal variation.
Results The average cumulative incidence of clubfoot during the study period was 1.4/103 (95% CI 1.2– 1.6). Three-quarters of the cases were boys. In half of the cases both feet were affected. There was significant regional heterogeneity, but no seasonal variation in occurrence of clubfoot.
Interpretation The cumulative incidence was higher than in earlier Scandinavian studies. Gender distribution and laterality were similar to those in previous reports. We found significant regional differences in incidence, but the cause of this observation must be investigated in greater depth.
Idiopathic clubfoot is a common congenital orthopedic problem of unknown but complex etiology, and with a reported cumulative incidence of 0.64–6.8 per 1,000 live births (Ching et al. Citation1969, Cartlidge Citation1984). In several previous studies performed in different regions of Scandinavia (Nilsonne Citation1927, Thomasen Citation1941, Severin Citation1956, Reimann Citation1967, Somppi Citation1984, Danielsson Citation1992) the reported cumulative incidence of congenital clubfoot was stable (). During the observed period 1913–1990, the various authors revealed similar figures of between 0.8/103 to 1.0/103. There has, however, been no national study in Sweden to confirm these estimates, except for the one by Severin (Citation1956). Furthermore, nationwide surveys and regional comparisons regarding the cumulative incidence of idiopathic clubfoot have been associated with complicating factors such as variations in diagnostic criteria and the registration methods used (Chesney et al. Citation1999). Such conceivable inaccuracies caused the Swedish Registry of Congenital Malformations to exclude clubfoot as a registry diagnosis during the period 1982–1999.
Table 1. Cumulative incidence estimates of congenital clubfoot in previous Scandinavian studies
In an attempt to improve the accuracy of the registered diagnosis with coherent diagnostic criteria, we performed a prospective, nationwide multicenter study in collaboration with the Swedish Pediatric Orthopaedic Society with the main aim of assessing the cumulative incidence of congenital clubfoot in Sweden over 2 consecutive years.
Patients and methods
In 1994, all public Orthopedic Departments in Sweden (n 65) were approached and 44 clinics reported that they treated newly diagnosed cases of congenital club foot. At each of these hospitals, we recruited a contact person to be responsible for the local registration during the recruitment period. To our knowledge, no private hospitals in Sweden were treating clubfoot during the study period.
Children with the ICD-9 code of congenital clubfoot (754F) were included. The sampling period started on January 1, 1995 and ended on December 31, 1996. For this period, we requested the medical records of 292 children who had been identified and reported in a preliminary way as new cases of cub foot. All the records that were available were scrutinized and children with positional clubfeet (n 3) and cases with additional neurological findings (n 3) were excluded, together with 6 preliminarily reported cases that could not be identified later on or which had missing records. Thus, 280 children were finally included in the present study.
Statistics
To compare the annual number of newborn children with congenital clubfoot with the total number of live births during 1995 and 1996, we used official reports concerning native data from the Swedish Board of Statistics (SCB). The cumulative incidence was calculated as the ratio between the number of children with clubfoot born during 1995–96 and the number of native births during the same period. For the estimated incidence, the 95% confidence intervals (CIs) were thus calculated, both for the total number of cases and for the subgroups year and sex. Abortive cases and stillbirths were not included in the population at risk and therefore, theoretically, the term prevalence proportion would be the most appropriate disease measure (Rothman Citation2002). However, we prefer to use the term cumulative incidence to avoid confusion when comparing the results of this study with those from earlier reports, which have generally used incidence (meaning cumulative incidence and not rate) as a description of clubfoot occurrence.
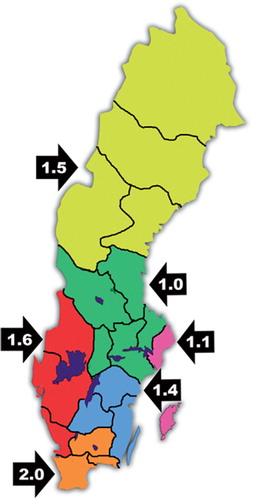
To assess the geographical distribution of clubfoot deformities, the country was divided into 6 regions commonly used by Health Service Authorities for administrative purposes (). The chi-square test was used for grouped data and a pvalue of < 0.05 was considered significant.
Figure 1. Cumulative incidence of idiopathic clubfoot during 1995–96 in 6 regions of Sweden. See Table 5 and text.
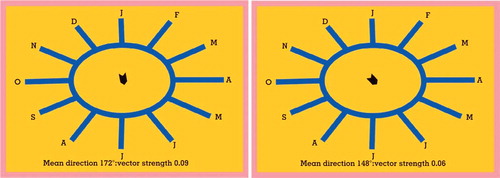
We also assessed seasonal variation by describing the monthly distribution of clubfoot deformities around the year (monthly cumulative incidence). We used a circular scale starting with January at 0° and the following months at 30° increments (Fischer Citation1993, Robertson and Corbett Citation1997) (). The angle 0° (range 345–15) represents January and the scale ends up with December at a mean angle of 330° (range 315–345). The average vector represents mean birth month for the children. We estimated one vector for children born with congenital clubfoot and another vector for all other children born in Sweden during the same period. The advantages and methodology of analyzing circular data have been thoroughly described by Zar (Citation1999). We used the Rayleigh z-test (Fischer Citation1993) to test whether there was a uniform distribution of seasonal cumulative incidence for the children with clubfoot and for all other live births, respectively. To test whether the two distributions of month of birth (mean vector) were equal between the clubfoot group and other newborn children, the nonparametric Watson's test was used (Zar Citation1999).
Figure 2. Monthly distribution of births in Sweden during 1995–96 for A. Congenital clubfoot (n 280) mean vector corresponding to July. B. Native births (n 198,719) mean vector corresponding to June.
Results
The cumulative incidence of idiopathic clubfoot in each of the 2 years studied was similar, at 1.5% and 1.3%, (p for difference = 0.2) (). The average cumulative incidence was 1.4% (95% CI 1.2–1.6). As commonly found, the majority (72%) of cases were boys. We found bilateral clubfeet in 46% of the cases. We also analyzed whether the distribution of patients with left or right side affected or bilateral clubfoot was similar for boys and girls. No gender-related side difference could be detected (p = 0.7) and the proportion of bilateral clubfeet was similar in boys (47%) and girls (41%) (p = 0.3; ).
Table 2. Number of children with idiopathic clubfoot in relation to number of native births
Table 3. Distribution according to gender, side and bilateral occurrence of clubfoot
Most clinics (82%) had up to 5 cases per year, while 8 larger clinics (18%) treated 43% of the children with a range of 8–13 children per year.
When the cumulative incidence in different regions was determined, a statistically significant heterogeneity was found (p = 0.007) (). In comparison, the lowest cumulative incidence was 1.0/103 (95% CI 0.7–1.4) in one region as compared to 2.0/103 (95% CI 1.5–2.6) in the region with highest cumulative incidence (, ).
Table 4. Cumulative incidence of idiopathic clubfoot during 1995 and 1996 in 6 regions of Sweden
The seasonal variation in children with clubfoot peaked at 172°, corresponding to birth in July (). The strength of this mean vector was, however, weak (r = 0.09). The distribution by month might in this case be uniform and the hypothesis of uniform distribution could not be rejected (p < 0.05). This means that for the children with clubfoot, there was no predominance of any month regarding birth. The angle of the mean vector for all live births was 148° (r = 0.06), corresponding to June. This is probably not a uniform distribution, i.e. the null hypothesis can be rejected (p < 0.001). Even so, there was no significant difference in distribution of birth month between clubfoot children and all other live births (p < 0.5).
Discussion
We found a higher cumulative incidence of congenital clubfoot during the 2 years of the study than has been found in previous studies from Scandinavia (). Does this mean that our sampling method is more accurate than in previous studies, or that the cumulative incidence is increasing—or both? It is difficult to provide a definite answer. We do, however, agree with Severin (Citation1956) that the derived cumulative incidence is an underestimation of the true estimate. There are always a number of cases missing. Thus, our study is most likely not an exception, but a confident estimation of cases overlooked is difficult to make. The clubfoot diagnosis is easily set at birth, and since practically all children in Sweden are born in hospital, we can conclude that there are merely no nondiagnosed cases.
The cause of missing data is therefore probably more often failure to properly record and report the diagnosis. In this respect, there may be several additional reasons for different cumulative incidence figures in our study and in earlier Scandinavian studies. Firstly, there is always the critical issue of how to define the population when assessing the cumulative incidence. All the previous studies in Scandinavia, except the one by Severin (Citation1956), took place in only part of the respective country. Secondly, especially in retrospective studies, there is uncertainty as to how cases were collected in relation to the defined population. Since the collection of cases in our study was prospective, we believe that we have achieved a good level of accuracy in the figures presented. Thirdly, by collecting medical records rather than using plain registry data, it was possible to exclude nonidiopathic cases, for instance those associated with syndromes or positional clubfeet. Since there was no central registration in Sweden of children with this diagnosis during the study period, the only way to obtain accurate data was to maintain continuous contact with all orthopedics departments in Sweden treating clubfeet. Nonetheless, we did observe a tendency of a decrease in the number of cases reported during the second year, which might reflect the general difficulty in continuous registration work.
One critical issue is, of course, whether the true cumulative incidence of congenital clubfoot in Sweden is increasing or not. A study from southern Sweden for the period 1946–90 (Danielsson Citation1992) concluded that there was an increase in the cumulative incidence during the late part of the period, from approximately 0.6/103 up to 1/103 at the end of the study. The authors suggested that the increase could be explained by immigration from non-Nordic countries. The estimated cumulative incidence for the Nordic part of Europe has generally been demonstrated to be lower than for other European regions (Cartlidge Citation1984, Somppi Citation1984, Danielsson Citation1992). A further increase in cumulative incidence might therefore be due to a continuous ethnic dilution of the Swedish population. Several extrinsic factors have also been analyzed (Barker and Macnicol Citation2002), such as a higher prevalence of maternal smoking during pregnancy over the past decades (Honein et al. Citation2000, Skelly et al. Citation2002), with a possible association with the regional difference in clubfoot cumulative incidence seen in our study (http://www.sos.se/fulltext/125/2004-125-4/2004-125-4.pdf, ). The highest incidence of maternal smoking is found in southern Sweden, the region that also has the highest proportion of clubfoot deformity. The higher proportion of immigrants in southern Sweden might also explain the regional differences in cumulative incidence of clubfoot (Franzén Citation2005).
Theories related to gestation giving increased intrauterine compression have been both recognized and rejected (Somppi Citation1984), and at present there seems to be convincing evidence that intrauterine compression is not a major risk factor (Barker and Macnicol Citation2002).
Several authors have suggested a seasonal variation in cumulative incidence of clubfoot, with a peak birth rate during December to March (Pryor et al. Citation1991), July (Lochmiller et al. Citation1998), or March–April (Barker and Macnicol Citation2002), and peak month of conception in October (Robertson and Corbett Citation1997). We could not confirm the observations of these authors. Others (Wynne-Davies Citation1964, Carney and Coburn Citation2005) have found no seasonality, which is in line with our observations. The study group (n 330) in the work of Robertson and Corbett (Citation1997) was collected during the years 1956–1994, and the control group was collected from 1989 through 1993, which raises the question of whether the environmental exposure was the same during these overlapping time periods (Barker and Macnicol Citation2002).
We could not find any gender difference regarding uni- or bilateral distribution, an issue that has attracted little attention in the literature. Our results are in accordance with the findings of Severin (Citation1956).
To summarize, we found a somewhat higher cumulative incidence of congenital clubfoot in Sweden compared to earlier reports, although the sex ratio and laterality distribution is in accordance with previous reports. Regional differences were significant, but we could not detect any seasonal variation.
Financial support was received from the Center for Research and Development, Uppsala University and the County Council of Gävleborg, Sweden.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent was obtained.
Contributions of authors
HW: collection of data, statistical analysis and manuscript writing. LH: Contributed in general discussion concerning incidence research and giving views on the manuscript. KM: contributed in the analysis and interpretation of the data and in writing the manuscript.
- Barker S L, Macnicol M F. Seasonal distribution of idiopathic congenital talipes equinovarus in Scotland. J Pediatr Orthop B 2002; 11: 129–33
- Carney B T, Coburn T R. Demographics of Idiopathic Clubfoot: Is there a seasonal variation?. J Pediatr Orthop 2005; 25: 351–52
- Cartlidge I J. Observations on the epidemiology of clubfoot in Polynesian and Caucasian populations. J Med Genet 1984; 21: 290–2
- Chesney D, Barker S, Miedzybrodzka Z, Haites N, Maffulli N. Epidemiology and genetic theories in the etiology of congenital talipes equinovarus. Bull Hosp Jt Dis 1999; 58(1)59–64
- Ching G H, Chung C S, Nemecheck R W. Genetic and epidemiological studies of clubfoot in Hawaii: ascertainment an incidence. Am J Hum Genet 1969; 21: 566–80
- Danielson L G. Incidence of congenital clubfoot in Sweden. Acta Orthop Scand 1992; 63: 424–6
- Fischer N I. Statistical analysis of circular data. Cambridge Univ Press. 1993; 70–1
- Franzén M. Unpublished data. 2005, SCB
- http://www.sos.se/fulltext/125/2004-125-4/2004-125-4.pdf.
- Honein M A, Paulozzi L J, Moore C A. Family history, maternal smoking, and clubfoot: an indication of a geneenvironment interaction. Am J Epidemiol 2000; 152: 658–65
- Lochmiller C L, Johnston D, Scott A, Risman M, Hecht J T. Genetic epidemiology study of idiopathic talipes equinovarus. Am J Med Genet 1998; 79: 90–6
- Nilsonne H. Eine statistische Studie über den kongenitalen Klumpfuss. Z Orthop Chir 1927; 48: 219–28
- Pryor G A, Villar R N, Ronen A, Scott P M. Seasonal variation in the incidence of congenital talipes equinovarus. J Bone Joint Surg (Br) 1991; 73(4)632–4
- Reimann I. Congenital idiopathic clubfoot, Munksgaard. Copenhagen, 1967
- Robertson W W, Jr, Corbett D. Congenital clubfoot, month of conception. Clin Orthop 1997, 338: 14–8
- Rothman K J. Epidemiology. Oxford University Press, New York 2002, chapter 3
- Severin E. Frekvensen av luxatio coxae congenita och pes equino varus congenitus i Sverige. Nord Med 1956; 55: 221–3
- Skelly A C, Holt V L, Mosca V C, Alderman B W. Talipes equinovarus and maternal smoking: A population-base case-control study in Washington State. Teratology 2002; 66: 91–100
- Somppi E Clubfoot. Review of the literature and an analysis of a series of 135 treated clubfeet. Acta Orthop Scand 1984, (Suppl 209)
- Thomasen E. Der Angeborne Klumpfuss. Über die Mechanik der Deformität und ihre primäre Behandlung. Acta Orthop Scand 1941; 12: 33–100
- Wynne-Davies R. Family studies and the cause of congenital club foot. J Bone Joint Surg (Br) 1964; 46: 445–76
- Zar J H. Biostatistical analysis. 4th. Prentice Hall, , N.J 1999, (Ed. Upper Saddle River), ch 26–7