Abstract
Background A secure incorporation of the graft in a bone tunnel is a prerequisite for successful anterior cruciate ligament reconstruction. In this cross-sectional pilot study, we studied the healing process with positron emission tomography (PET) scanning.
Patients and methods 8 young patients underwent an anterior cruciate ligament reconstruction with a bonepatellar tendon-bone graft (BTB, n = 4) or a quadruple semitendinosus and gracilis graft (ST/G, n = 4). Regional bone turnover was quantified with an 18F-fluoride PET scan in each patient 1 day, 3 weeks, 7 months, or 22 months after surgery.
Results The highest activity level was found 3 weeks after surgery, but the activity at the femoral fixation points was markedly increased even after 7 months. The bone turnover was almost normalized 22 months after the operation.
Interpretation It would take at least 7 months until an anterior cruciate ligament graft, fixed with an interference screw, is completely incorporated. This finding is important for postoperative rehabilitation. Furthermore, PET is a feasible tool when studying new ways of fixing soft tissue to bone.
Anterior cruciate ligament (ACL) reconstruction is a common procedure; approximately 3,000 ACL reconstructions are performed annually in Sweden.
Following introduction of arthroscopy in the past two decades, the surgical morbidity has decreased. The gold-standard procedure has been replacement of the torn cruciate ligament with a bone-tendon-bone (BTB) autograft from the central part of the patellar tendon, with bone blocks at both ends (Fu and Shulte Citation1996). This method allows secure fixation of the graft with presumed bone-to-bone integration. Because of donor site morbidity with BTB grafts, hamstring tendons as a graft have gained increasing popularity. The tendinous tissue is believed to heel onto bone within the graft tunnel. Both methods have provided similar functional results after 2 years (Beynnon et al. Citation2002a, Ejerhed et al. Citation2003, Feller and Webster Citation2003, Jansson et al. Citation2003). The timing of the healing process of the graft is not well understood, however. There is no consensus regarding the appropriate time after surgery for return to strenuous physical activity. The recommended time duration before return to sport, based on clinical experience, has ranged from 2 to 12 months—but few authors advocate resumption of sport activities before 6 months after surgery (Beynnon et al. Citation2002b).
How long does it take for a BTB graft or a hamstring graft to safely heal and be incorporated within the graft tunnel, producing a rigid fixation? One measure of incorporation might be to estimate local bone turnover in the graft area relative that in to the adjacent bone. Studies on local bone turnover are possible in animal models, but in humans invasive histomorphometric techniques are not generally feasible. Noninvasive functional imaging techniques are therefore attractive as a research tool in the clinical setting. 18F-fluoride positron emission tomography (PET) allows the measurement of regional skeletal kinetics with high spatial resolution compared to older ordinary skeletal scintigraphic methods. Quantative assessment by three-dimensional imaging of skeletal metabolism at specific sites of the skeleton can be obtained. After intravenous injection and diffusion through bone capillaries into the extracellular fluid of bone, the fluoride ion is exchanged with hydroxyl groups in the matrix hydroxyapatite crystal to form fluoroapatite (Frost et al. Citation2003). Fluoride is preferentially deposited at the osteoid bone interfaces, where remodeling and bone turnover is greatest. The rapid uptake of fluoride thus occurs at sites of high osteoblastic activity. The aim of this pilot study was to use 18F-fluoride PET (Schliephake et al. Citation1999, Blake et al. Citation2001, Piert et al. Citation2001) to study the local bone metabolism at the fixation points—and thereby estimate the dynamics of the graft healing process of the proximal tibia and distal femur—up to 2 years after surgery in patients operated for anterior cruciate reconstruction with either BTB or hamstring grafts.
Patients and methods
The study involved 8 patients with anterior cruciate ligament injury who underwent an anterior cruciate ligament reconstruction, 4 with a bone-patellar tendon-bone graft (BTB) and 4 with a quadruple semitendinosus and gracilis graft (ST/G). There were 3 men and 1 woman aged between 26–44 years in the BTB group, and 2 women and 2 men with an age range of 22–27 years in the ST/G group. We used a cross-sectional design: 1 patient from each group (BTB or ST/G) was examined on 1 postoperative occasion after 1 day, 3 weeks, 7 months, or 22 months after surgery. All patients thus underwent 1 PET scan each. This made it possible to approximate bone metabolism differences over time for both surgical techniques.
One surgeon performed all operations with an arthroscopic reconstruction. To further minimize differences between the operation techniques, in all patients we secured the graft with interference screws. The graft fixation used for the ST/G tendons involved soft tissue screws (RCI) pressing the graft against the bone tunnel in the same manner as the bone blocks are pressed against the bone tunnel with interference screws when using BTB grafts.
The BTB graft was harvested from the central part of the patellar tendon with 2.5–3 cm-long bone plugs at each end. The graft was fixed with a 7 × 20-mm titanium interference screw (Cannuflex; Smith & Nephew) on the femoral side and an 8 × 25-mm screw of the same type on the tibial side. The ST/G graft was harvested with a blunt tendon stripper. 22 cm of each tendon was taken and then doubled, thus creating an 11-cm-long quadrupled tendon graft. The graft was fixed with 7 × 25-mm soft tissue titanium screws (Smith & Nephew) at both ends.
All patients underwent the same postoperative management by a standardized rehabilitation protocol. A cryocuff was administrated immediately postoperatively, and kept for at least 12 h. No bracing was used after the operation. Full weight bearing immediately, assisted by crutches, was allowed during the first 2 weeks after surgery. Return to sport activities was allowed 6 months postoperatively.
PET method
PET scanning
We used a GE Scanditronix 4096 scanner (GE Scanditronix, Uppsala, Sweden 1990) and a Siemens/CTI ECAT HR Plus scanner (Sie-mens/CTI, Knoxville, TN 1999). The GE 4096 has a field of view (FOV) of 10 cm and yields 15 consecutive transaxial slices. The HR Plus has a FOV of 15 cm, yielding 63 transaxial slices. Both scanners were cross-calibrated.
Patients were positioned supine with legs in vacuum cushions and the knees centered in the scanner gantry. A 10-min transmission scan with externally rotating 68Ge/Ga-rods was performed to produce a density map used for subsequent attenuation correction. 3 MBq/kg body weight of 18Ffluoride was injected into a forearm vein, with a subsequent saline flush. Emission scanning was performed from 35–50 min after injection.
Image processing
All emission scans were corrected for attenuation, scatter and decay, and reconstructed with filtered back projection. A 4.2-mm Hann filter was used to obtain a final image resolution of 7- and 6-mm in-plane, full-width-half-max-imum (FWHM) for the two scanner types.
In the density map, regions of interest (ROI) were drawn in the location of the femoral and tibial titanium screws. These ROIs were copied to the emission image, where small circular ROIs were drawn to mark the region of bone tissue with the highest tracer uptake directly adjacent to the screw. ROIs were also placed in patella. A large region in the contralateral femur was used as a reference region for normal bone metabolism and a region in the quadriceps muscle was used to assess the concentration of unbound fluoride in fluids.
Bone metabolic rates in the various regions were compared semiquantitatively between patients. The regional tracer concentration measured was normalized to injected dose and patient weight, to produce standardized uptake values (SUVs; i.e. activity in tissue (Bq/mL) divided by the total dose injected (Bq) / body weight (g)). By setting average body density to 1 g/mL, this expression gives a unitless value of the tissue activity in proportion to the average activity per mL of the entire body. In a recent study, a high correlation was found between the SUV obtained by this mode of investigation and the kinetic rate constant of osseous fluoride incorporation (Sörensen et al. Citation2003).
All values are presented as mean (SD).
The study was approved by the Ethics Committee of Uppsala University Hospital.
Results
Fluoride uptake in the contralateral femoral reference region was invariably discrete (1.1 (0.3) SUVs) and 2.6 (1.4) times higher than in soft tissue.
In the area of surgery, the activity was highly elevated and strongly correlated to time after surgery ().
Figure 1. Quantitative 18F-fluoride PET images of 3 patients at 3 weeks, 7 months, and 22 months after BTB surgery. Small circles indicate the location of the titanium screws. The upper row contains transaxial slices through the knee at the level of the femoral screw, and the middle row at the level of the tibial screw. The bottom row contains oblique slices through both screws and the bone tunnel.
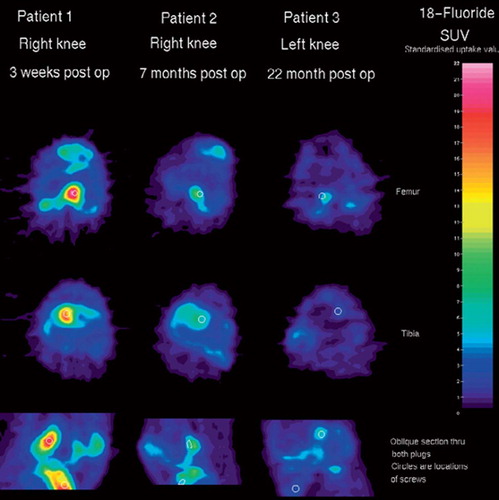
In the area of surgery, the activity was low on the day after surgery, both in the patients with BTB graft and the patients with ST/G graft (). The highest uptakes were in the range of 2–4 times the reference values of the contralateral femur, with no difference observed between BTB and ST/G.
Figure 2. Individual fluoride uptake at the femoral and tibial tunnel areas, and also in the patella region. Values are presented as standardized uptake values (SUV).
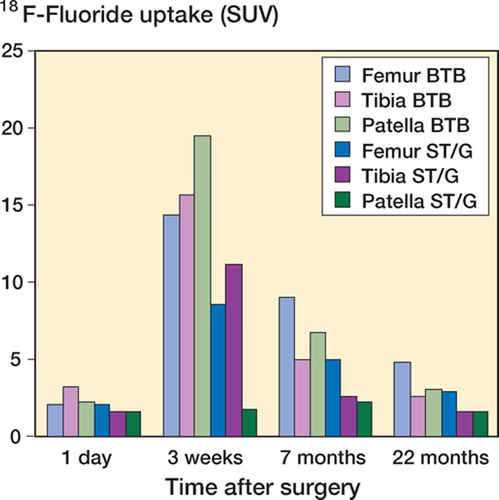
The 2 patients who were examined 3 weeks after surgery had the highest activity levels of our 4 measurement occasions. The activity levels for both were quite similar in the tibia and femur, with SUV values higher than 12. The BTB patient had substantially higher patellar activity.
7 months after surgery, the bone metabolism had decreased in both BTB and ST/G, but there was still an obvious increased activity at the femur fixation points. There was, however, a nearly normal bone turnover at the tibial side.
Even after 22 months, we found a slightly elevated activity at the BTB-femur fixation point. The measurements at the other sites showed an almost normalized bone metabolism.
Discussion
This cross-sectional pilot study indicates that neither BTB nor hamstring grafts are completely integrated with the surrounding bone tissue 7 months after surgery. With our study design, we cannot, however, ascertain whether the persistently increased bone turnover rate at this time is also related to an increased risk of biomechanical graft failure. If this is the case, return to sporting activities should be delayed further in order to reduce the risk of graft failure or elongation. Nowadays, the most common recommendation is a 4–6-month rehabilitation period after surgery before return to sporting activities.
The objective of this pilot study was to investigate changes in bone metabolism at the fixation points in the femur and tibia, using PET scan. The PET scans were performed at 4 different times postoperatively, in 4 patients with BTB graft and 4 with ST/G graft. Since this is the first investigation to use the PET technique to examine local bone turnover in the area of tendon graft healing, we chose a cross-sectional study instead of a longitudinal study design to gain knowledge of the method without high individual radiation exposure. Since all patients were young and healthy, they could be expected to have a similar bone metabolism and turnover, substantiated by the narrow range of activity in the normal femur reported in this study and by others (Brenner et al. Citation2004). The intraindividual variability of fluoride PET measurements in normal limb bone was recently reported to be
0.01 (0.42) SUVs for repeated scans (Brenner et al. Citation2004). These findings indicate that a change in regional fluoride uptake of 1 SUV could be considered significant at the individual level. Accordingly, the rate of bone metabolism in the fixation points of both BTB and ST/G was well above normal values 7 months after surgery.
PET scanning with 18F-fluoride apparently provides an opportunity to quantify regional bone metabolism in a new and more exact way than with conventional bone scintigraphic techniques. After this pilot study, we would advocate a new longitudinal study with repeated PET scans during the period from approximately 3–12 months after surgery.
In conclusion, these results indicate that the complete incorporation of the anterior cruciate ligament graft will take at least 7 months in the femur tunnel, regardless of which graft is used. This study can be used as a reference for new techniques of graft fixation, especially when bioabsorbable fixation devices and/or bone stimulating agents are used locally.
We wish to thank Professor Bengt Långström and the staff of the Uppsala Imanet PET Center for valuable support in this study.
No competing interests declared.
Contributions of authors
JS worked on the study plan, performed PET scanning, data analysis and writing of the manuscript. KM worked on the study plan, and performed data analysis and writing. HS performed data analysis. SS worked on the study plan and examined patient material. HR worked on the study plan, examined patient material, and performed data analysis and writing.
- Beynnon B D, Johnsson R J, Flemming B C, Kannus P, Kaplan M, Samani J, Renström P. Anterior cruciate ligament replacement: Comparison of boane patellar tendonbone grafts with two-strand hamstring graft. J Bone Joint Surg (Am) 2002a; 84(9)1503–13
- Beynnon B D, Johnson R J, Fleming B C. The science of anterior cruciate ligament rehabilitation. Clin Orthop 2002b, 402: 9–20
- Blake G M, Park-Holohan S J, Cook G J, Fogelman I. Quantitative studies of bone with the use of 18F-Fluoride and 99mTc-methylene diphosphonate. Semin Nucl Med. 2001; 31(1)28–49
- Brenner W, Vernon C, Muzi M, Mankoff D A, Link J M, Conrad E U, Eary J F. Comparison of different quantitative approaches to 18F-fluoride PET scans. J Nucl Med 2004; 45(9)1493–500
- Ejerhed L, Kartus J, Sernert N, Kohler K, Karlsson J. Patellar tendon or semitendinosus tendon autografts for anterior cruciate ligament reconstruction? A prospective randomized study with a two-year follow-up. Am J Sports Med 2003; 31: 19–25
- Feller J A, Webster K E. randomized comparison of patellar tendon and hamstring tendon anterior cruciate ligament reconstruction. Am J Sports Med 2003; 31: 564–73
- Frost M L, Cook G J, Blake G M, Marsden P K, Benatar N A, Fogelmann N J. A prospective study of risedronate on regional bone metabolic and blood flow at the lumbar spine measured by 18F-fluoride positron emission tomography. J Bone Miner Res 2003; 18: 2215–22
- Fu F H, Shulte K R. Anterior cruciate ligament surgery 1996, State of the art. Clin Orthop 1996, 325: 19–24
- Jansson K A, Linko E, Sandelin J, Harilainen A. A prospective randomized study of patellar versus hamstring tendon autografts for anterior cruciate ligament reconstruction. Am J Sports Med 2003; 31: 12–8
- Piert M, Zittel T, Becker G, Jahn M, Stahlschmidt A, Maier G, Machulla H J, Bares R. Assessment of porcine bone metabolism by dynamic 18Ffluoride ion PET: Correlation with bone histomorphometry. J Nucl Med. 2001; 42(7)1091–100
- Schliephake H, Berding G, Knapp W H, Sewilam S. Monitoring of graft perfusion and osteoblast activity in revascularised fibula segments using 18F-positron emission tomography. J Orthop Sci 1999; 4(3)216–22
- Sörensen J, Ullmark G, Låström B, Nilsson O. Rapid bone and blood flow formation in impacted morselized allografts: positron emission tomography (PET) studies on allografts in 5 femoral component revisions of total hip arthroplasty. Acta Orthop Scand 2003; 74(6)633–43