Abstract
Background If it would be possible to detect lack of flow and/or the development of ischemia in bone, we might have a way of predicting whether a broken bone will heal. We established microdialysis (MD) and laser Doppler (LD) flow measurement in the human femoral head in order to be able to detect ischemia and measure changes in blood flow.
Material and methods In 9 patients undergoing total hip arthroplasty for primary osteoarthrosis, two MD catheters were inserted into the femoral head through two drill holes after the blood flow had been visualized by LD. Then primary samples were collected with the femoral head in situ; thereafter, the head was removed and samples were collected over the following 4 hours ex vivo. The variables obtained by MD were concentrations of glucose, lactate, pyruvate, and glycerol in extracellular fluid.
Results The results showed development of ischemia with a statistically significant decrease in glucose concentration and elevation of the lactate/pyruvate ratio over time. The LD showed flow with the femoral head in situ and lack of flow when the femoral head was removed.
Interpretation The use of MD was established in the human femoral head. Ischemic levels were detected within 2 h of cessation of blood flow in most patients.
Microdialysis was initially developed more than 25 years ago to study the metabolism in the central nervous system of rats and other experimental animals. More recently, it has been used to study the metabolism in many different tissues such as brain tissue in humans (Skjoth-Rasmussen et al. Citation2004), muscle, and adipose tissue (Rooyackers et al. Citation2004). The use of microdialysis in bone has been limited to measurement of the concentrations of antibiotics (Stolle et al. Citation2003, Citation2004) and of the release of prostaglandin E2 (Thorsen et al. Citation1996). However, measurements of metabolism in bone could very well be of importance. The microdialysis technique is only semiquantitative, which limits its use to temporal changes. Otherwise, the results have to be compared against a reference value.
Laser Doppler has been used for measuring blood flow in human bone, and has shown valid results (El Maraghy et al. Citation1999, Notzli et al. Citation2002, Beck et al. Citation2004). It seems that laser Doppler gives optimum results in areas where the blood supply is limited to a few vessels, e.g. the femoral head (Sugamoto et al. Citation1998) or the proximal humerus (Herzog et al. Citation2002, Hinsley et al. Citation2002). One previous study has evaluated laser Doppler flow in the femoral head (Sugamoto et al. Citation1998).
Adequate perfusion of the femoral head is essential for bone healing. Thus, detection of ischemia in the femoral head or the lack of blood flow measured by laser Doppler could be predictors for the outcome of the treatment of femoral neck fractures.
We investigated whether microdialysis and laser Doppler can demonstrate ischemia and change in blood flow in the femoral head of humans.
Material and methods
Patients who underwent total hip replacement were included into the study. The inclusion criterion was primary osteoarthrosis. Exclusion criteria were rheumatoid arthritis, previous fracture or surgery of the hip, and previous or ongoing treatment with glucocorticosteroids. 10 femoral heads from 10 patients were included. 1 femoral head was excluded because the laser Doppler did not show pulsatile flow. This was due to the drill holes being too close to the cortex. Thus, 4 females and 5 males with a median age of 71 (47–74) years were included into the study. In the first patient, only microdialysis measurements were done due to technical difficulties.
Microdialysis
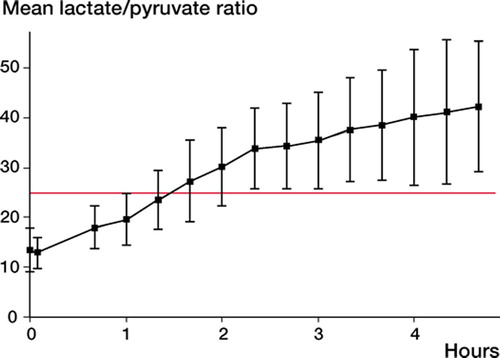
2 microdialysis catheters with a membrane length of 20 mm (CMA 70; CMA, Solna, Sweden), each connected to a CMA 107 pump, were used in each patient. The reason for using a membrane length of 20 mm was to make sure that the catheter would fit within the trabecular part of the femoral head. The microdialysis catheters were perfused with a Ringer NaCl suspension (CMA). The samples were collected with a flow rate of 2 μL/min, in order to make sure that enough dialysate was collected over the relatively short sampling period (5 min). During perfusion, an equilibrium between the perfusion fluid in the catheters and the interstitial fluid is believed to be established. The samples were collected in micro-vials and analyzed for glucose, lactate, pyruvate, and glycerol on a CMA 600 analyzer. The detection ranges for the CMA 600 analyzer are: glucose 0.1–25 mm, lactate 0.2–12 mm, pyruvate 10–1,500 μm, and glycerol 10–1,500 μm (data supplied by the manufacturer). Ischemia was evaluated from the lactate/pyruvate ratio. A ratio above 25 was considered ischemic, as proposed by Ungerstedt and Rostami (Citation2004) based on measurements in brain and muscle tissue.
For most substances, the uptake across the membrane is incomplete. The fraction of the substance collected in the dialysate relative to the concentration in plasma is defined as the relative recovery (RR), and is calculated as: RR = Cdialysate/Cplasma. The relative recovery is calculated using the concentration of glucose in dialysate and plasma. In this study we were not aiming at obtaining a recovery of 100%, since we were interested in the lactate/pyruvate ratio as a predictor of ischemia. We assumed that the recovery of lactate and pyruvate was similar and that recovery was constant throughout the sampling period. We calculated recovery by using plasma glucose and the concentration of glucose in the microdialysis samples, when the femoral head was still in situ.
Laser Doppler
When laser light is introduced into the tissue, approximately 1% of the light is reflected and scattered by moving erythrocytes (Bonner Citation2005). The frequency of the reflected light is broadened and it is possible to calculate the average speed of movement in the tissue. By multiplication by the concentration of erythrocytes (measured by the laser Doppler by absorption), it is possible to calculate the flux—measured in arbitrary perfusion units (AU).
We used a 2-mW laser Doppler (DRT4 laser Doppler blood flow monitor; Moor Instruments, UK). To measure within the bone, two types of needle probes were used: 1) DP4sd, which is a bluntneedle side-delivery probe, and 2) DP3, which is a blunt-needle end-delivery probe; both were from Moor Instruments. Both the side-delivery probe and the end-delivery probe were used on the first 3 patients, but the signal was better with the enddelivery probe and this was used exclusively for the remaining 7 patients. The data presented are from the end-delivery probe. The flow data were recorded using Moorsoft/DRT4 software v. 2.0 for Windows (Moor Instruments).
In order to show blood flow and not interference from Brownian motion (movements of molecules), or the shaking of the investigator's hand, we used pulse synchronic pulsatile flow.
We define pulsatile flow as being when the following requirements have been fulfilled:
A steady DC curve. This gives an indication of the back-scattered laser light intensity. It can be used to check the efficiency of light collection by the laser Doppler probes,
a pattern of waves with a uniform appearance.
pulse synchronous waves,
mean flux >10 AU (Gamse and Saria Citation1987),
change in flux (ΔFlux) of minimum 8 AU (amplitude),
measurement done over 10 sec.
Mean flux and standard deviation, maximum flux, and minimum flux were measured over a period of 10 sec using the statistics function in the DRT4 monitor software. From this, the Δflux was calculated.
Surgery and measurements
All patients were operated via a posterolateral approach with the patient in the lateral decubitus position. Gluteus maximus was divided. The external rotators were cut and kept away by stay sutures. Care was taken not to disturb the medial circumflex artery. The capsule was opened and the femoral neck and head were exposed, leaving the femoral head in situ. Two drill holes (2 mm diameter and 30 mm deep) were made at the osteochondral junction pointing towards the center of the femoral head, in order to ensure that the holes were in the trabecular part of the bone. Flow was measured with the laser Doppler in both holes. Then the two microdialysis catheters were inserted into the drill holes. They were flushed for 3 min with a flow rate of 2.0 μL/min in order to empty the efferent tube. Two sets of samples were collected over 5 min with the flow rate of 2.0 μL/min. We did not have time to let the catheters stabilize for 20–40 min before the first samples were collected, since the measurements were made during a hip replacement. The microdialysis catheters were removed from the drill holes and the holes were marked according to the catheters. Then the hip was dislocated and the femoral head was immediately removed by using an oscillating saw, the catheters were reinserted, and the femoral head was subsequently put into a chamber which was submerged in a water bath kept at 37°C.
With the femoral head in the chamber, the mean temperature was 34.0°C (SD 0.8°C). Over the next 4 h, samples were collected, at intervals of 5 min every 20 min, with a flow rate of 2.0 μL/min. The samples were analyzed for glucose, lactate, pyruvate, and glycerol.
In all but 1 patient, an arterial blood sample was taken at the time when the femoral head was removed to measure plasma glucose.
The study was carried out according to the Helsinki Declaration and the protocol was approved by the local Ethics Committee. The patients gave their informed written consent prior to surgery.
Statistics
Data are presented as mean with standard deviation (SD) in parentheses, except for age where median and range are used.
The 2 samples from the same point in time and from each femoral head were averaged before the data were analyzed. Student's t-test was used on the mean of the first 2 samples and on the mean of the 3 last samples for the lactate/pyruvate ratio. For glucose concentration, Student's t-test was used on the mean of the first 2 samples and on the mean of the 2 samples at times 1 h 40 min and 2 h, because after 2 h the lower detection limit for glucose had been reached.
Results
We demonstrated pulsatile flow in all 8 femoral heads. In patients 4 and 6, only one drill hole gave pulsatile flow (). The relative recovery of the microdialysis was 55% (15%).
Lactate/pyruvate ratio was consistent with ischemia after 2–2.5 h (). In one femoral head, the lactate/pyruvate ratio did not increase above 25, but still had a trend of a rise in lactate/pyruvate ratio, indicating development of ischemia. Lactate/pyruvate ratio increased from 13.2 (3.5) (mean of the 2 first samples, before the femoral neck was cut) to 41.4(12.4) (mean of the 3 last samples, after 3 h) (p < 0.001).
Figure 1. Lactate/pyruvate ratio measured in 9 femoral heads of humans by use of microdialysis. A ratio of above 25 is defined as ischemia.
Laser Doppler measurements performed in the femoral head of humans presented as flux (mean with SD in parentheses) and Δflux which is the amplitude of the curve. Pulsatile flow: see text for definition
The glucose concentration in the samples decreased (p < 0.001) (). After 3 h the concentration was under the detection limit, whereas the concentration of glycerol increased over time after a drop during the first hour.
Figure 2. Mean glucose, glycerol, pyruvate, and lactate concentrations over time measured by microdialysis in 9 femoral heads after removal to a chamber, and in 5 syringes with human blood. The development in the bone shows a decrease in glucose and pyruvate, but an increase in glycerol and lactate. In the syringes, the development shows “wash-out” with a reduction in all substrates except lactate.
Discussion
There are 2 main treatments for dislocated femoral neck fractures: arthroplasty and osteosynthesis. Among the patients having their fracture osteosynthesized, 20–30% will experience failure—resulting in reoperation (Rogmark et al. Citation2002, Keating et al. Citation2006). Preserving the hip seems optimal, as studies have shown that patients with a united femoral neck fracture have a better functional outcome than patients with hemiarthroplasty (Partanen and Jalovaara, Citation2004). In order to distinguish between potential treatments for the individual patient, ischemia might be an important factor (Swiontkowski et al. Citation1993).
We evaluated ischemia by use of microdialysis in the femoral head in humans. The microdialysis technique uses catheters with a semipermeable membrane at the tip. The catheter acts as a small capillary in the tissue, and it is assumed that the perfusion fluid establishes equilibrium with the extracellular fluid as the perfusion fluid moves through the tip of the catheter. By measuring the concentrations of glucose, lactate, and pyruvate in the perfusion fluid, it is possible to asses the metabolic status of the tissue. Production of lactate from pyruvate only happens during anaerobic metabolism. Thus, if the tissue lacks oxygen the level of pyruvate will fall and the level of lactate will increase, leading to a rise in the lactate/pyruvate ratio. In addition, the glucose level will fall when the supply is reduced (low or no blood flow) (Ungerstedt and Rostami Citation2004).
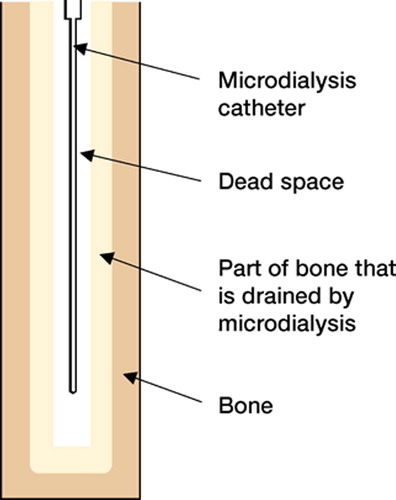
The microdialysis catheter is estimated to drain approximately 100 mg of tissue (Rosdahl et al. Citation1993). In bone, this is estimated to be around 100 mm3, while the drill hole in our study had a volume of approximately 63 mm3 (V = πr2h = π × (1 mm)2 × 20 mm). The catheter has a volume of 6 mm3, which gives a dead space around the catheter of 57 mm3, where there will be exudation of extracellular fluid from the bone ().
Figure 3. Drawing of the catheter used for microdialysis, placed in bone. The light gray area is the part of the bone from which the metabolites diffuse. The area around the catheter is the dead space, from which the metabolites diffuse into the catheter.
It can be argued that the microdialysis measurements will only show what is happening in a small clot of blood in the dead space around the catheter, where a washout phenomenen would be expected. However, we have shown from the results of microdialysis performed on blood collected in a syringe that there is a clear wash-out pattern where all substances decrease in concentration over time except lactate, which remains the same (Pedersen et al. Citation2006). In addition, a high flow rate during microdialysis can also cause wash-out of the substances, when the microdialysis fluid is moving substances away from the tissue. A slow supply of the substance to the tissue will result in a lower concentration with time. When we look at our results, there is no evidence of wash-out since both lactate and glycerol increased over time, whereas the only fall was seen for glucose and its metabolite, pyruvate ().
The microdialysis technique demonstrated a rise in lactate/pyruvate ratio and a decrease in glucose concentration over time, consistent with development of ischemia within 2 h of cessation of blood flow. This was done using a flow rate of 2 μL/min. The flow rate normally used in other tissues such as muscle and brain has been 0.2 μL/min. By using the high flow rate, the recovery will be lower because the time to equilibrate over the membrane is shorter. The reason for using a high flow rate was to collect enough fluid over the relatively short time that the study was done—during insertion of a total hip arthroplasty. Since we are measuring the lactate/pyruvate ratio and not an absolute value, the ratio is not influenced by the flow rate.
We used glucose as a marker to calculate recovery, in order not to introduce another substance into the patient. Recovery was estimated to be 55%, by using the blood glucose concentration as reference value. This seems reasonable, as studies have shown that plasma glucose levels and bone marrow glucose levels are comparable (Ummenhofer et al. Citation1994, Hurren Citation2000). We are aware that the most correct method to calculate recovery is by using an inert tracer, due to the fact that glucose is being used and transformed in the tissue. However, this fact will make our real recovery higher than the one we have calculated. A recovery of 55% has also been found in another study in which muscle glucose was evaluated (Korth et al. Citation2000). The recovery can only be calculated before the osteotomy of the femoral neck, because it is not possible to establish a value to calculate a recovery rate from after the head has been removed. We can only assume that recovery stays the same throughout the experiment.
By using our definitions of pulsatile flow and the laser Doppler signal on the monitor, we were able to distinguish between pulsatile flow and no flow with 100% agreement on duplicate measurements. In our results the mean flux ranged from 6 AU to 112 AU, which has also been reported in other studies (Beck et al. Citation2004). Studies with other equipment have also shown large variations in mean flux values (Sugamoto et al. Citation1998). This variation in flux may be explained by the position of the laser Doppler probe. If it is close to a trabecular vessel or a sinusoid, the flow figure will be higher than if the probe is far from a vessel or a sinusoid.
We have found no other reports showing detection of ischemia development by using microdialysis in bone. The method might be used in a modified setting in treatment of patients with femoral neck fractures.
Contributions of authors
MBP: involved in all aspects of the investigation and completion of the paper. CE and SO: surgery and participation in the conception and writing of the article.
- Beck M, Siebenrock K A, Affolter B, Notzli H, Parvizi J, Ganz R. Increased intraarticular pressure reduces blood flow to the femoral head. Clin Orthop 2004, 424: 149–52
- Bonner R F. Principles of laser-Doppler flowmetry. Laserdoppler blood flowmetry, A P Shepherd, P A Öberg. Kluwer Academic Publishers, Boston 2005
- ElMaraghy A W, Schemitsch E H, Waddell J P. Greater trochanteric blood flow during total hip arthroplasty using a posterior approach. Clin Orthop 1999, 363: 151–7
- Gamse R, Saria A. Antidromic vasodilatation in the rat hindpaw measured by laser Doppler flowmetry: pharmacological modulation. J Auton Nerv Syst 1987; 19: 105–11
- Herzog L, Huber F X, Meeder P J, Muhr G, Buchholz J. Laser doppler flow imaging of open lower leg fractures in an animal experimental model. J Orthop Surg 2002; 10: 114–9, (Hong Kong)
- Hinsley D E, Hobbs C M, Watkins P E. The role of laser Doppler flowmetry in assessing the viability of bone fragments in an open fracture. Injury 2002; 33: 435–8
- Hurren J S. Can blood taken from intraosseous cannulations be used for blood analysis?. Burns 2000; 26: 727–30
- Keating J F, Grant A, Masson M, Scott N W, Forbes J F. Randomized comparison of reduction and fixation, bipolar hemiarthroplasty, and total hip arthroplasty. Treatment of displaced intracapsular hip fractures in healthy older patients. J Bone Joint Surg (Am) 2006; 88: 249–60
- Korth U, Merkel G, Fernandez F F, Jandewerth O, Dogan G, Koch T, van Ackern K, Weichel O, Klein J. Tourniquetinduced changes of energy metabolism in human skeletal muscle monitored by microdialysis. Anesthesiology 2000; 93: 1407–12
- Notzli H P, Siebenrock K A, Hempfing A, Ramseier L E, Ganz R. Perfusion of the femoral head during surgical dislocation of the hip. Monitoring by laser Doppler flowmetry. J Bone Joint Surg (Br) 2002; 84: 300–4
- Partanen J, Jalovaara P. Functional comparison between uncemented Austin-Moore hemiarthroplasty and osteosynthesis with three screws in displaced femoral neck fractures—a matched-pair study of 168 patients. Int Orthop 2004; 28: 28–31
- Pedersen M B, Emmeluth C, Overgaard S. Microdialysis in bone, a method study. 2006, (paper in preperation)
- Rogmark C, Carlsson A, Johnell O, Sernbo I. A prospective randomised trial of internal fixation versus arthroplasty for displaced fractures of the neck of the femur. Functional outcome for 450 patients at two years. J Bone Joint Surg (Br) 2002; 84: 183–8
- Rooyackers O, Thorell A, Nygren J, Ljungqvist O. Microdialysis methods for measuring human metabolism. Curr Opin Clin Nutr Metab Care 2004; 7: 515–21
- Rosdahl H, Ungerstedt U, Jorfeldt L, Henriksson J. Interstitial glucose and lactate balance in human skeletal muscle and adipose tissue studied by microdialysis. J Physiol 1993; 471: 637–57
- Skjoth-Rasmussen J, Schulz M, Kristensen S R, Bjerre P. Delayed neurological deficits detected by an ischemic pattern in the extracellular cerebral metabolites in patients with aneurysmal subarachnoid hemorrhage. J Neurosurg 2004; 100: 8–15
- Stolle L B, Arpi M, Jorgensen P H, Riegels-Nielsen P, Keller J. In situ gentamicin concentrations in cortical bone: an experimental study using microdialysis in bone. Acta Orthop Scand 2003; 74: 611–6
- Stolle L B, Arpi M, Holmberg-Jorgensen P, Riegels-Nielsen P, Keller J. Application of microdialysis to cancellous bone tissue for measurement of gentamicin levels. J Antimicrob Chemother 2004; 54(1)263–5
- Sugamoto K, Ochi T, Takahashi Y, Tamura T, Matsuoka T. Hemodynamic measurement in the femoral head using laser Doppler. Clin Orthop 1998, 353: 138–147
- Swiontkowski M F, Tepic S, Rahn B A, Cordey J, Perren S M. The effect of fracture on femoral head blood flow. Osteonecrosis and revascularization studied in miniature swine. Acta Orthop Scand 1993; 64: 196–202
- Thorsen K, Kristoffersson A O, Lerner U H, Lorentzon R P. In situ microdialysis in bone tissue. Stimulation of prostaglandin E2 release by weight-bearing mechanical loading. J Clin Invest 1996; 98: 2446–9
- Ummenhofer W, Frei F J, Urwyler A, Drewe J. Are laboratory values in bone marrow aspirate predictable for venous blood in paediatric patients?. Resuscitation 1994; 27: 123–8
- Ungerstedt U, Rostami E. Microdialysis in neurointensive care. Curr Pharm Des 2004; 10: 2145–52