Abstract
Background Hip fracture incidence rates are high, and increase with increasing age. Previous studies have predicted a continued increase in both crude and age-standardized rates.
Method We estimated incidence rates, based on a complete and validated register containing verified and individually sequenced hip fractures from 1996–2003, for a population of 500,000 people in Funen County, Denmark.
Results The verified number of the first hip fractures was 6,676, with 520 subsequent fractures. Between 1996 and 2003, the incidence rate of first hip fracture fell by 2.4% per year for males (p = 0.02) and by 1.8% per year for females (p = 0.004). The highest decrease of 3.4% per year (p = 0.02) was seen in 80–84-year-old women.
Interpretation The incidence rate of the first hip fracture has fallen in both sexes. In most age groups, the actual number of fractures has also decreased. The findings emphasize the need for valid projection studies which should include both demographic projections and modeling of the effects of different levels of prevention.
Worldwide, there has been a significant rise in both crude incidence and age-standardized incidence of hip fractures during the second half of the twentieth century (Melton et al. Citation1987). The highest incidence rates have been found in Northern and Western Europe (Hedlund et al. Citation1986, Gullberg et al. Citation1993, Finsen et al. Citation2004). Lifetime risk of hip fracture among postmenopausal women was found to be 14%–23% in Sweden, depending on the underlying life expectancy used (Oden et al. Citation1998), and 17% in Australia (Doherty et al. Citation2001). Based on an estimate of the total number of hip fractures in 1990, the WHO has estimated that there will be 4.5–6.3 million new hip fractures globally in the year 2050 (Gullberg et al. Citation1997).
There is no clear pattern or trend in the level of incidence of hip fractures with time. Some studies have indicated a rise (Frandsen and Kruse Citation1983, Gullberg et al. Citation1993), and others have suggested a decline or steady state (Melton et al. Citation1982, Naessen et al. Citation1989, NHS Scotland Citation2002). One of the main problems could be different numerators(Fielden et al. Citation2001, Stephenson et al. Citation2003).
Validated incidence figures are important for the development of preventive efforts, rehabilitation facilities and new treatments. We estimated the incidence rates of hip fractures in Funen County, Denmark.
Patients and methods
Funen County accounts for 9% of the Danish population, with 169,999 inhabitants who are over 50 years of age (2003). Treatment of hip fractures is done at three orthopedics departments. The current study covered the period 1996 through 2003. We used two sources for identification of patients: 1) the Central Patient Administrative System, which has information on all patient contacts with the hospitals in Funen County since 1975, and 2) the Funen County Hip Fracture Register, which was started on January 1, 1996. Information from the two sources was combined and checked to make sure the cases were appropriate (as explained in greater detail below).
Based on diagnosis and surgical procedure codes, we constructed an electronic extract from the Central Patient Administrative System for all possible hip fracture contacts. The ICD-10 diagnoses used were: S72.0 femoral neck, S72.1 intertro-chanteric, S72.2 subtrochanteric (5 cm below the trochanter minor), T84.1 complications to internal fixation, and T93.1 complications to fracture of lower extremity (WHO 1992). The surgical procedure codes used were: NFJxx, NFBxx, NFCxx, NFGxx, and NFUxx (NOMESCO 2004). This included both primary and secondary admissions: 10,433 records, of which 80% had a diagnosis of hip fracture (S72.0, S72.1, and S72.2).
The Funen County Hip Fracture Register is a dedicated clinical database containing every resident over 50 years of age who has been admitted to any of the three orthopedics departments in the county with a hip fracture. Case ascertainment is done according to a structured identification routine. For the study period, 6,692 incident hip fractures had been registered.
When information from the Central Patient Administrative System and the Funen County Hip Fracture Register was combined, records not present in the hip fracture register or showing inconsistency of information (diagnosis and surgical procedure codes) in the two sources were marked for manual inspection (n = 4,660) of the original case files. This allowed identification of 765 new incident cases for the hip fracture register, whereas the remaining equivocal patient records (n = 3,895) either related to follow-up admissions (n = 2,976) or had inconsistent diagnosis or surgical procedure codes, but had already been included in the original list of 6,692 records.
Apart from checking whether each hospital contact had been primary or follow-up, the sequence of fractures for individual patients from 1975 to 1995 was ascertained by referring again to the Central Patient Administrative System.
The case verification procedure described above for the study period 1996–2003 resulted in three levels of precision in ascertainment of fracture status: “diagnosis of hip fracture” (n = 8,307), “verified hip fracture” (n = 7,457) or “verified first hip fracture” (n = 6,676).
Statistics
Student's t-test was used to test for differences in mean age. Incidence rates were calculated using the mid-year population of Funen County for each year. We used Poisson regression in estimation of overall and age-stratified developments in incidence rate over the study period, with calendar year entered as a continuous variable and evaluation of significance from the calendar year parameter. The statistical software used was Stata version 8.2 (StataCorp, College Station, TX; http://www.stata.com).
Results
From 1996 through 2003, 7,457 hip fractures occurred in Funen County, all of which were verified. In 261 cases, the fracture recorded was a subsequent fracture, with the first fracture occurring before January 1, 1996. These were excluded from the analysis; thus, there were 7,196 hip fractures, of which were 6,676 verified first fractures and 520 were subsequent fractures.
Incidence rates were calculated using “verified first hip fracture”, “verified hip fracture”, and “diagnosis of hip fracture”. Inclusion of unverified diagnoses clearly results in an overestimation of the true incidence rate by up to 20%. However, all rates showed a decline—the decline in the rate of the verified first fracture being steeper than those for verified hip fracture or diagnosis of hip fracture. The rates of verified hip fracture and verified first hip fracture diverged as a consequence of the accumulation of subsequent hip fractures ().
Figure 1. Hip fracture incidence rates per 1,000 inhabitants (mid-year population) from 1996 to 2003 in Funen County, Denmark, with Poisson based 95% CI. Poisson regression line added on all. *Significant decrease. Blue – all records with a diagnosis of hip fracture (n = 8,307). Green – all verified hip fractures (n = 7,457). Red – all verified first hip fractures (n = 6,676). Circles – women, squares – men.
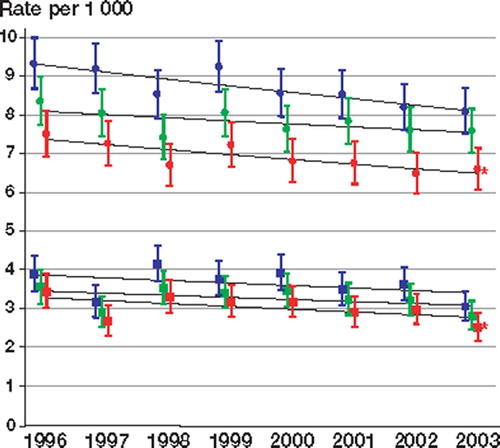
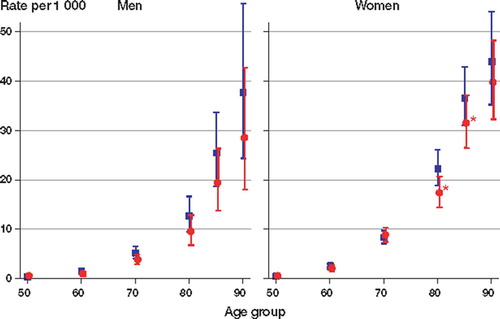
During the period 1996–2003, the incidence rate of the first hip fracture for men decreased by 2.4% per year (p = 0.02) from 3.4 per 1,000 person years (95% CI: 3.0–3.9) to 2.5 (2.2–2.9). For women, the incidence rate of the first hip fracture decreased by 1.8% per year (p = 0.004) from 7.5 (6.9–8.1) to 6.5 (6.1–7.1) (). When stratifying for age, the highest decreases were seen in the incidence rate for 80–84-year-old women of 3.4% per year (p = 0.02) and in 85–89–year-old women of 2.4% per year (p = 0.03) (). A decrease was seen in the actual number of first fractures in almost all agegroups .
Figure 2. The age and sex-specific incidence rate per 1,000 inhabitants (mid-year population) of verified first hip fracture for 1996 (blue) and 2003 (red) in Funen County, Denmark, with Poisson-based 95% CI. *Significant decrease.
The male and female distribution of the population of Funen County, verified first and subsequent hip fracture, for specific age groups, 1996–1999 and 2000–2003
Mean age at the first fracture was 80 years (78 years for men and 81 years for women). 54% of the total number of first fractures were cervical, 40% were trochanteric, and 6% were subtrochanteric. A similar distribution was seen for second fracture.
Men had a shorter interval from the first to the second hip fracture (p = 0.03). The median interval was 265 (0–2,312) days for men and 434 (1–2,498) days for women.
Discussion
In most age groups, the incidence rate of the first hip fracture along with the actual number of first fractures decreased over the period 1996–2003. The level of the verified incidence rates was about 20% lower than rates based on the presence of a hip fracture diagnosis.
The strength of our study is the that the incidence rates have been based on a thoroughly verified, complete, and revised hip fracture register containing every hip fracture in a defined population (one county of Denmark) over the study period of 8 years. Based on the Danish personal ID number, the Funen County Hip Fracture Register enabled complete checking of hip fracture events. The necessity of distinguishing clearly between the first and any subsequent hip fracture became obvious when calculating the incidence rates. The rate of all verified hip fractures clearly showed the effect of the accumulation of subsequent hip fractures over time. As seen in , the decline in the rate of all verified fractures is much less clear (and less significant) than the decline in the incidence rate of the first hip fracture. Whether this decrease indicates a turning point in the history of hip fracture rates will remain unanswered until validated updates from other regions become available.
A reduced incidence rate has also been noted in other studies (Naessen et al. Citation1989, Melton et al. Citation1996), but most previous studies have reported an increase (Frandsen and Kruse Citation1983, Schroder et al. Citation1995, Lauritzen Citation1996, Fielden et al. Citation2001, Stephenson et al. Citation2003). Several studies have indicated an increasing crude incidence rate as well as an increasing age and gender-specific incidence rate (Hedlund et al. Citation1987, Melton et al. Citation1987, Gullberg et al. Citation1993, Gullberg et al. Citation1997, Finsen et al. Citation2004).
Hip fracture incidence numerators vary: Frandsen and Kruse (Citation1983) included all validated hip fractures. Fielden et al. (Citation2001) included all hip fractures based on diagnosis at admission, while Hedlund et al. (Citation1986) included first hospital admissions only and Gullberg et al. (Citation1993) included all hip fractures based on radiological diagnosis. Thus, there is a need for common guidelines should be established.
The causes of the observed decline in the incidence rate of the first hip fracture are unknown. The decline may be due to an improvement in the general health status of the elderly population, as life expectancy has increased in recent years and mortality rates have decreased (Kannisto et al. Citation1994). It may also be a result of a multitude of interventions concerning the elderly such as preventive home visits, exercise, fall prevention, optimized nutrition and medication—which have been implemented more or less systematically in Denmark in recent years.
The exact nature and size of the burden in future remains uncertain, and the declining rates shown here emphasize the need for valid projection studies which should include both demographic projections and modeling of the effects of different levels of prevention.
No competing interests declared.
Related Research Data
- Doherty D A, Sanders K M, Kotowicz M A, Prince R L. Lifetime and five-year age-specific risks of first and subsequent osteoporotic fractures in postmenopausal women. Osteoporos Int 2001; 12: 16–23
- Fielden J, Purdie G, Horne G, Devane P. Hip fracture incidence in New Zealand, revisited. N Z Med J 2001; 114: 154–6
- Finsen V, Johnsen L G, Trano G, Hansen B, Sneve K S. Hip fracture incidence in central Norway: a followup study. Clin Orthop 2004, 419: 173–8
- Frandsen P A, Kruse T. Hip fractures in the county of Funen, Denmark. Implications of demographic aging and changes in incidence rates. Acta Orthop Scand 1983; 54: 681–6
- Gullberg B, Duppe H, Nilsson B, Redlund-Johnell I, Sernbo I, Obrant K, Johnell O. Incidence of hip fractures in Malmo. Bone (14 Suppl 1). Sweden 1993; S23–S29, (1950-1991)
- Gullberg B, Johnell O, Kanis J A. World-wide projections for hip fracture. Osteoporos Int 1997; 7: 407–13
- Hedlund R, Ahlbom A, Lindgren U. Hip fracture incidence in Stockholm 1972-1981. Acta Orthop Scand 1986; 57: 30–4
- Hedlund R, Lindgren U, Ahlbom A. Age and sex-specific incidence of femoral neck and trochanteric fractures. An analysis based on 20,538 fractures in Stockholm County. Clin Orthop. Sweden 1987; 222: 132–9, 1972-1981
- Kannisto V, Lauritsen J, Thatcher A R, Vaupel J W. Reductions in mortality at advanced ages several decades of evidence from 27 countries. Popul Develop Rev 1994; 20: 793–810
- Lauritzen J B. Hip fractures: incidence, risk factors, energy absorption, and prevention. Bone 1996; 18: 65S–75S
- Melton L J, Ilstrup D M, Riggs B L, Beckenbaugh R D. Fifty-year trend in hip fracture incidence. Clin Orthop 1982, 162: 144–9
- Melton L J, O'Fallon W M, Riggs B L. Secular trends in the incidence of hip fractures. Calcif Tissue Int 1987; 41: 57–64
- Melton L J, Atkinson E J, Madhok R. Downturn in hip fracture incidence. Public Health Rep 1996; 111: 146–50
- Naessen T, Parker R, Persson I, Zack M, Adami H O. Time trends in incidence rates of first hip fracture in the Uppsala Health Care Region. Am J Epidemiol. Sweden 1989; 130: 289–99, 1965-1983
- NHS Scotland. Scottish Hip Fracture Audit Report 2002, www.show.scot.nbh.uk/shfa
- Oden A, Dawson A, Dere W, Johnell O, Jonsson B, Kanis J A. Lifetime risk of hip fractures is underestimated. Osteoporos Int 1998; 8: 599–603
- Schroder H M, Andreassen M D, Villadsen I, Sorensen J G, Erlandsen M. Increasing age-specific incidence of hip fractures in a Danish municipality. Dan Med Bull 1995; 42: 109–11
- Stephenson S, Langley J, Campbell J, Gillespie W. Upward trends in the incidence of neck of femur fractures in the elderly. N Z Med J 2003; 116: U665