Abstract
Background Arthroscopic subacromial decompression (ASD) for shoulder impingement has gained popularity. We evaluated the result of this common procedure prospectively, from a patient perspective.
Method We used the Disability of the Arm, Shoulder and Hand questionnaire (DASH) and the Visual Analogue Scale (VAS) to evaluate 50 patients with a mean age of 49 (27–72) years. All patients had undergone 6 months of failed nonoperative treatment prior to surgery. Exclusion criteria were total rotator cuff rupture, shoulder instability, clinically verified acromioclavicular joint osteoarthritis, calcifying tendonitis or neurological symptoms. All the decompressions were done by experienced shoulder arthroscopists.
Results A significant improvement in both the median DASH score and the VAS had occurred 6 months after surgery.
Interpretation ASD for impingement in properly selected patients performed by experienced surgeons gives a high degree of patient satisfaction 6 months after surgery. ▪
The most common alternatives for surgical treatment of shoulder impingement are open decompression and ASD. No difference in long-term outcome has been found between the two methods (Lindh and Norlin Citation1993, Husby et al. Citation2003).
The Constant-Murley score is often used to measure the outcome of shoulder surgery (Anderson et al. Citation1999, Patel et al. Citation1999, Dom et al. Citation2003). It has questions that measure daily activities (ADL) and others that measure the strength and range of motion (Constant and Murley Citation1987). The value of this score is questionable, because it uses objective values that are useful to surgeons but does not take account of the patient's satisfaction regarding health and function. Several authors have emphasized the importance of measuring the patient's own experience of disability using self-reported questionnaires. These consist of different scales that measure specific health considerations such as physical function and pain (Atroshi et al. Citation2000, Michener et al. Citation2000). The DASH questionnaire is a region-specific instrument that is reliable and valid in patients with elbow and shoulder disorders (Hudak et al. Citation1996, Turchin et al. Citation1998, McConnel et al. Citation1999).
Using the Swedish version of the DASH questionnaire, we have prospectively measured the satisfaction of subacromial impingement patients who were treated with ASD.
Patients and methods
67 consecutive patients who had undergone ASD for clinically verified impingement syndrome (Neer grade II) (Neer and Welsh Citation1977) at Ängelholm Hospital, Sweden, in 2002 and 2003 were studied prospectively. ASD was chosen as a routine instead of open surgery because of its diagnostic advantages and shorter rehabilitation period (Lindh and Norlin Citation1993). To be included in the study, the patients had to have had subacromial pain for more than 6 months which did not improve by nonoperative treatment.This comprised a training program supervised by an experienced physiotherapist. Most patients received at least one subacromial injection of corticosteroid as part of this regime. Exclusion criteria included: total rotator cuff rupture, instability, clinically verified acromioclavicular joint osteoarthritis, calcifying tendonitis, neurological symptoms, or not being able to read and understand Swedish. As part of the preoperative evaluation, all patients received a subacromial injection of local anesthesia to assess whether the pain emanated from the subacromial structures. Radiographs of the humeroscapular and acromioclavicular joints were taken in all patients. Co-planing, or removal of osteophytes under the lateral end of the clavicle and medial acromion, was done as part of the ASD in patients with asymtomatic acromioclavicular joints. 5 patients who were included preoperatively were excluded at surgery because of instability in the glenohumeral joint, repair of the rotator cuff, or resection of the lateral end of clavicle.
The research leader (MB) was informed as soon as any patient was scheduled for ASD due to impingement syndrome. The patients were then asked by telephone if they wanted to participate in the study. All patients were given the information that it was optional to participate in the study, and that every statement and result would be anonymous. To prevent bias, the research leader never met the patients. 1 week before and 6 months after surgery, the patients received an envelope with two self-assessment questionnaires (the Swedish version of the DASH questionnaire and the VAS) and a return envelope (Hudak et al. Citation1996, Atroshi et al. Citation2000). If any questionnaire was not returned, the patient was reminded twice. 10 patients who did not respond at all, and 2 patients who left more than 4 of the 30 questions unanswered were excluded from the study. 50 patients completed the questionnaire (31 men). Mean age was 49 (27–72) years.
The DASH self-assessment questionnaire () is designed to assess symptoms and functional status in patients with musculoskeletal conditions of the upper extremity, the main emphasis being physical function (Turchin et al. Citation1998, McConnel et al. Citation1999, Atroshi et al. Citation2000). Each item has 5 choices of response, ranging from “no difficulty or no symptom” to “unable to perform activity or very severe symptom”, and is scored on a 1- to 5-point rating scale. The DASH questionnaire also includes 2 optional 4-item scales about occupational function and additional questions about leisure activities (e.g. the ability to perform sports and/or to play a musical instrument) (). The DASH score was used to evaluate whether gender and/or sick leave were prognostic factors for the result of the operation. Pain was measured using the visual analogue scale (VAS).
Table 1. The items in the Disabilities of the Arm, Shoulder and Hand (DASH) symptom scale
Table 2. The items in the DASH symptom scale regarding work and leisure activity
The ASD was performed with the arthroscope in the posterior port. The coracoacromial ligament was released (Ellman Citation1988). All 4 surgeons were experienced shoulder arthroscopists to eliminate the learning curve. Patients had met a physiothera-pist on the day of surgery, and were given a standard rehabilitation protocol starting with active assisted range of motion at day 1. As the pain decreased, this progressed with strengthening exercises of the rotator cuff and shoulder muscles.
Statistics
We used non-parametric statistical methods because of the small number of samples. The Wilcoxon signed-rank test was used to compare the results of related groups. The Mann-Whitney U test was then used to compare unrelated groups. Probabilities of less than 0.05 were considered significant.
Results
The median DASH overall score improved by 24 points after surgery (median 42 (9–87) before surgery and 18 (0–78) after surgery; p < 0.001, Wilcoxon signed-rank test) ().A mean improvement in DASH score of 19 points has been suggested to be “much better” (Gummesson et al. Citation2003).A 10-point difference in DASH score may be considered to be the minimal amount of change of any importance, and this improvement was observed in 38 patients. 2/19 women and 6/31 men showed no improvement after surgery.
Figure 1. Box plots of overall DASH score, work score and leisure (sport/music) score before surgery (blue box) and after surgery (green box).ap < 0.001.
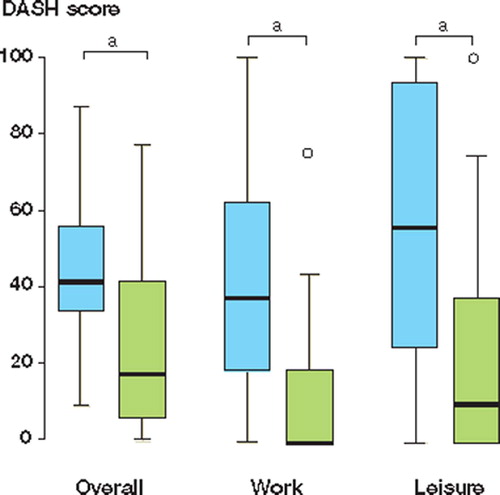
The DASH work score was studied in 25 patients and improved after surgery (median 44 (0–100)) before surgery compared with 0 (0–75) after surgery; p < 0.001, Wilcoxon signed-rank test). The DASH sport/music score was studied in 18 patients and improved after surgery (median 56 (0–100) before surgery compared with 10 (0–75) after surgery; p < 0.001, Wilcoxon signed-rank test) ().
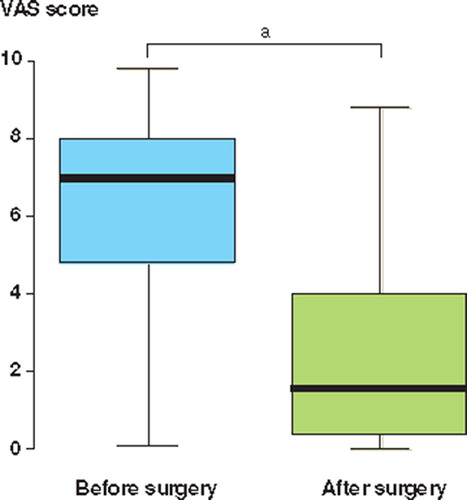
There was no sex-related difference in the absolute change in DASH (women: median 22 (–8 to 43); men: 21 (–27 to 49); p = 0.4, Mann Whitney U test). There was no difference in the absolute change in DASH between those who had sick leave before surgery (median 19 (–28 to 49) and those who had not (median 23 (–16 to 48); p = 0.5, Mann-Whitney U test). There was a significant improvement in the VAS score after surgery (median 1 (0–9) compared with median 7 (0–10) before surgery; p < 0.001, Wilcoxon signed-rank test) ().
Figure 2. Box plots of VAS score before surgery and after.ap < 0.001.
Discussion
Shoulder impingement is a common disorder and when nonoperative treatment has failed, ASD has proven useful. We have evaluated this common procedure from the point of view of the patient. The region-specific self-assessment instrument DASH, which is applicable to a large variety of disorders of the upper extremity, has shown effectiveness of treatment and has even detected mild disability. A review of disease-specific instruments that evaluate disorders of the arm has shown that only the Carpal Tunnel Instrument had higher sensitivity than the DASH questionnaire (Gummesson et al. Citation2003). Most of the questions were useful in detecting the symptoms of shoulder impingement in the current study ().The DASH questionnaire is of good quality in comparison with other shoulder assessment scales, such as the American Shoulder and Elbow Surgeons’(ASES) Shoulder Index, the Simple Shoulder Test (SST), and the DASH in combination with more function-orientated scales such as the Constant-Murley score (Skutek et al. Citation2000). The interpretation of DASH can be influenced by patient age: a recent study has shown that scores are higher in older patients (Hunsaker et al. Citation2002). The mean age in our study appears to be similar to those in other rotator cuff disease studies (Ellman Citation1988, Dom et al. Citation2003).
To our knowledge, the result of ASD for shoulder impingement has only been evaluated prospectively once before using a DASH questionnaire; the score increased by (median) 11 points (Gummesson et al. Citation2003). This is less than half of the improvement seen in our patients. The reason for this may be that we applied a stricter patient selection and excluded patients who were found to have other causes of shoulder pain or who had concomitant surgery other than ASD.Furthermore, the number of our patients was double that in Gummesson et al. (Citation2003), and with less selection bias. Gummesson et al. (Citation2003) had a mean follow-up period of 12 (6–21) months. Even so, there was no further improvement after 6 months in their study. We are well aware that the patient's progress may continue until 1 year after surgery; however, we found improvement in both DASH and VAS with 6 months of follow-up. A longer follow-up period would probably not have changed the conclusion of our study and, to our knowledge, there is no evidence in the literature of inferior results with a longer follow-up period. Gummesson et al. (Citation2003) used only DASH questions about ADL. We included parts of the DASH questionnaire that evaluate work and leisure activities, and found significant improvement in these scores. Pain is the main complaint in shoulder impingement patients and it reduces the patient's quality of life. We have found a remarkable improvement in the VAS score after ASD.
Female sex and work absence have been reported to be prognostic factors. Women have been reported to be more troubled by the musculoskeletal symptoms (especially in the neck and shoulder regions) than men (Henriksson et al. Citation1996). We did not find any difference between men and women regarding change in DASH score. One of the best independent prognostic factors in patients with rotator tendinosis was restricted prescription of sick leave (Brox et al. Citation1996, Citation1999). We found no significant change between those who were on sick leave compared and those who were not.
We conclude that ASD for impingement, performed by experienced shoulder surgeons after appropriate patient selection, gives high patient satisfaction 6 months after surgery.
We thank Skåne Council Primary Care Research for financial support.
No competing interests declared.
Author contributions
MB participated in the design and conduction of the study, data collection and drafted the manuscript. KL participated in the design of the study, analysis of the result and in editing the manuscript. YH participated in the design and editing of the manuscript. AN participated in the design and conduction of the study and editing of the manuscript. FA-Z was actively involved in the analysis of the results and the editing of the manuscript.
Related Research Data
- Anderson N H, Sojbjerg J O, Johannsen H V, Sneppen O. Selftraining versus physiotherapist-supervised rehabilitation of the shoulder in patients treated with arthroscopic subacromial decompression: a clinical randomized study. J Shoulder Elbow Surg, 1999; 8(2)99–101
- Atroshi I, Gummesson C, Andersson B, Dahlgren E, Johansson A. The disabilities of the arm shoulder and hand (DASH) outcome. Acta Orthop Scand 2000; 71(6)613–8
- Brox J I, Brevik J I, Ljunggren A E, Staff P H. Influence of anthropometric and psychological variables pain and disability on isometric endurance of shoulder abduction in patients with rotator tendinosis of the shoulder. Scand J Rehabil Med 1996; 28(4)193–200
- Brox J I, Gjengedahl E, Uppheim G, Böhmer A S, Brevik J I, Ljunggren A E. Arthroscopic surgery versus supervised exercises in patients with rotatorcuff disease (stage II impingement syndrome): a prospective, randomized, controlled study in 125 patients with a 2-year follow up. J Shoulder Elbow Surg 1999; 8(2)102–11
- Constant C R, Murley A H G. A clinical method of func-tional assessment of the shoulder. Clin Orthop 1987, 241 160–4
- Dom K, Van Glabbeck F, Van Riet R P, Verborgt R P, Wuyts F L. Arthroscopic subacromial decompression for advanced (staged II) impingement syndrome: a study of 52 patients with five years follow-up. Acta Orthop Belg 2003; 69(1)13–7
- Ellman H. Arthroscopic subacromial decompression. Arthroscopic surgery, J S Parisien. McGraw-Hill, New York 1988; 243–8
- Gummesson C, Atroshi I, Ekdahl C. The Disabilities of the arm, shoulder and hand (DASH) outcome questionnaire: longitudinal construct validity and measuring selfrated health change after surgery. BMC Musculoskelet Disord 2003; 4: 11
- Henriksson K G, Böckman E, Henriksson C, de Laval J H. Chronic regional muscular pain in women with precise manipulation work. Scand J Rheumatol 1996; 25: 213–23
- Hudak P L, Amadio P C, Bombardier C. Development of an upper extremity outcome measure. The DASH (disabilities of the arm,shoulder and hand). Am J Ind Med 1996; 29: 602–8
- Hunsaker F G, Cioffy D A, Amadio P C, Wright J G, Cauglin B. The American academy of orthopaedic surgeons outcomes instruments: normative values from the general population. J Bone Joint Surg (Am) 2002; 84: 208–15
- Husby T, Haugstvedt J R, Brandt M, Hom I, Steen H. Open versus arthroscopic subacromial decompression. A prospective randomized study of 34 patients followed for 8 years. Acta Orthop Scand 2003; 74(4)408–14
- Lindh M, Norlin R. Arthroscopic subacromial decompression versus open acromioplasty. A two-year follow-up study. Clin Orthop 1993, 290: 174–6
- McConnel S, Beaton D E, Bombardier C. Disabilities of the arm, shoulder and hand: The DASH outcome measure user's manual. First edition. Toronto, Ontario 1999
- Michener L A, Legging B G. A review of selfreport-scales for the assessment of functional limitation and disability of the shoulder. J Hand Ther 2000; 14: 68–76
- Neer C S, Welsh R P. The shoulder in sports. Orthop Clin North Am 1977; 85: 83–91
- Patel V R, Singh D, Calvert P T, Bayley J I. Athroscopic subacromial decompression: results and factors affecting outcome. J Shoulder Elbow Surg 1999; 8(3)231–7
- Skutek M, Fremerey R W, Zeichen J, Bosch U. Outcome analysis following open rotator cuff repair. Early effectiveness validated using four different shoulder assessment scales. Arch Orthop Trauma Surg 2000; 120(7–8)432–6
- Turchin D C, Beaton D E, Richards R R. Validity of observer-based aggregate scoringsystems as descriptors of elbow pain, function and disability. J Bone Joint Surg (Am) 1998; 80: 154–62