
Abstract
Background and purpose — Fast-track protocols have been successfully implemented in many hospitals as they have been shown to result in shorter length of stay (LOS) without compromising results. We evaluated the effect of fast-track implementation on the use of institutional care and results after total hip replacement (THR).
Patients and methods — 3,193 THRs performed in 4 hospitals between 2009–2010 and 2012–2013 were identified from the Finnish Hospital Discharge Register and the Finnish Arthroplasty Register. Hospitals were classified as fast-track (Hospital A) and non-fast-track (Hospitals B, C, and D). We analyzed LOS, length of uninterrupted institutional care (LUIC, including LOS), discharge destination, readmission, revision rate, and mortality in each hospital. We compared these outcomes for THRs performed in Hospital A before and after fast-track implementation and we also compared outcomes, excluding readmission rates, with the corresponding outcomes for the other hospitals.
Results — After fast-track implementation, median LOS in Hospital A diminished from 5 to 2 days (p < 0.001) and (median) LUIC from 6 to 3 (p = 0.001) days. No statistically significant changes occurred in discharge destination. However, the reduction in LOS was combined with an increase in the 42-day readmission rate (3.1% to 8.3%) (p < 0.001). A higher proportion of patients were at home 1 week after THR (p < 0.001) in Hospital A after fast-tracking than before.
Interpretation — The fast-track protocol reduces LUIC but needs careful implementation to maintain good quality of care throughout the treatment process.
Due to the high economic burden on the healthcare system of total hip replacement (THR), efforts to enhance recovery and reduce length of primary hospital stay (LOS) to decrease costs without compromising results are mandatory. During the last decade, LOS in Finnish hospitals has decreased (Mäkelä et al. Citation2011a, Pamilo et al. Citation2013). However, potential to further reduce LOS and increase the discharge rate directly to home remains, especially in lower volume hospitals (Pamilo et al. Citation2013).
The aim of a fast-track protocol is to optimize the whole treatment protocol, leading eventually to shorter LOS with no impairment of treatment quality (Husted Citation2012). Several studies have shown that a fast-track protocol reduces LOS after primary THR, but the overall shortening of LOS even without a fast-track protocol is rarely taken into account (Husted and Holm Citation2006, Husted et al. Citation2010b, Citation2012, den Hartog et al. Citation2013, Glassou et al. Citation2014, Winther et al. Citation2015). Fast-tracking has not been found to be associated with higher readmission, reoperation, mortality, or postoperative hip dislocation rate (den Hartog et al. Citation2013, Glassou et al. Citation2014, Jorgensen et al. Citation2014, Gromov et al. Citation2015). Apart from studies on LOS which included only hospitals discharging 100% of patients home (Husted et al. Citation2010b, Citation2011, Jorgensen et al. Citation2013a), no reports have been published on length of uninterrupted institutional care (LUIC, defined as the combined surgical treatment period (LOS) and any immediately following period of uninterrupted institutional care) after fast-track THR.
By combining the Finnish Arthroplasty Register, Hospital Discharge Register, and benchmarking data from 4 different hospitals, we evaluated the effect of fast-tracking on LOS, LUIC, discharge destination, readmissions, early revisions, and mortality.
Patients and methods
For this study, we selected 4 similar Finnish public central hospitals, all with some teaching responsibilities, from a benchmarking database maintained by the Nordic Healthcare Group (NHG). Implementation of a fast-track protocol started in September 2011 in Hospital A, which soon after that date fulfilled all the fast-track criteria. The other hospitals (Hospitals B, C, and D) did not meet the fast-track criteria to the same extent (). The characteristics of the hospitals, drawn from the benchmarking database, are given in .
Table 1. Criteria for a hospital to be characterized as a fast-track hospital a
Table 2. Characteristics of the 4 benchmark hospitals included in the studyTable Footnotea
A hospital was classified as a fast-track hospital if it had (i) written standardized patient information aiming at fast recovery, (ii) standardized opioid-sparing anesthesia, (iii) no use of drains or urinary catheters, (iv) standardized opioid-sparing pain management, (v) discharge criteria from the post-anesthesia care unit (PACU), (vi) mobilization on the day of surgery and (vii) standardized discharge criteria (fulfillment checked several times per day) (). Fulfillments of the fast-track criteria were evaluated from answers to a written questionnaire sent to each study hospital.
Patient education and information in Hospital A was planned to give the patient all the information needed to enable early discharge. Preoperative education included patient education seminars and an outpatient session with an orthopedic surgeon and a nurse before surgery. Written standardized information was given to all patients. A phone number to be called in case of any questions was included in this written information.
This study is based on the PERFECT hip and knee replacement databases (Mäkelä et al. Citation2011b), which collect data from the Finnish Hospital Discharge Register (FHDR) and the Finnish Arthroplasty Register (FAR), cause of death statistics (Statistics Finland), drug prescription register, and drug reimbursement register (Social Insurance Institution). All public and private hospitals in Finland are obliged to report all surgical procedures to the FHDR. In comparison with the FHDR, the coverage of the FAR for primary hip replacements in the 4 target hospitals during the study period was 88% in Hospital A, 93% in Hospital B, 79% in Hospital C, and 97% in Hospital D (Institute for Health and Wellfare 2017). We evaluated LOS, LUIC, discharge destination, presence at home 1-week post-surgery, readmissions, revisions, and mortality during 2 2-year periods, 1 before (2009–2010) and 1 after (2012–2013) fast-track implementation in Hospital A. Patients were followed up until the end of 2015. The results for Hospital A were also compared with those for the other hospitals (B, C, and D). However, readmission rates were not compared with those of the other hospitals due to variation in the readmission criteria.
LOS was counted as the number of nights in the surgical specialty ward of the hospital from admission to discharge, as recorded in the hospital discharge register. LOS terminated in either discharge home, transfer to another facility, or death. LUIC, defined as the combined surgical treatment period and any immediately following period of uninterrupted institutional care, was calculated in the same manner. Any rehabilitation given in an outpatient setting or at home was not included in LUIC. LUIC ended in either the patient’s death or discharge home. LUIC includes patient transfers to another facility such as an old people’s home or institution run by a social welfare organization. In the analyses, the maximum length of institutional care was limited to 60 days. We considered that if a patient stays in a health care facility for more than 60 days after THR, the reason is not directly related to the operation.
Inclusion criteria
The study population was formed by selecting patients from the FHDR according to the WHO International Classification of Diseases (ICD-10 2010) and applying the following criteria: M16.0/M16.1 for primary osteoarthritis (OA) of the hip or M16.2/M16.3 for developmental dysplasia of the hip (DDH), linked with a code for primary THR during the same treatment period performed over the periods 2009–2010 and 2012–2013. Patients with diagnosed DDH were included in the study owing to the variation in the coding of mild DDH and primary OA. The codes for primary THR were NFB30, NFB40, NFB50, NFB60, NFB62, and NFB99 according to the NOMESCO classification of surgical procedures, Finnish version. The accuracy of the diagnosis of primary OA was double-checked against the relevant data in the FAR. Total hip replacements—not patients—were evaluated when considering the length of the surgical treatment period, the length of institutional care, and unscheduled readmissions.
Exclusion criteria
THRs performed for secondary OA, and revisions were excluded (Appendix 1, see Supplementary data). A diagnosis of secondary hip OA was noted retrospectively from the beginning of 1987. A patient was excluded from the study if a diagnosis of secondary hip OA had been recorded in the Hospital Discharge Register between the beginning of 1987 and the day of the operation. Patients with a diagnosis of congenital hip dislocation (Q65.0–Q65.9) were excluded. Patients listed in the Social Insurance Institution database as eligible for reimbursement for the sequelae of transplantation, uremia requiring dialysis, rheumatoid arthritis, or connective tissue disease were excluded from the study. We also excluded patients who were not Finnish citizens or were residents of the autonomous region of Åland.
Readmission
Readmission was recorded if the patient had been readmitted after discharge to any ward in any hospital in Finland during the first 14 or 42 days from the index operation. A direct transfer to another hospital was not counted as a readmission. Only the first readmissions for any reason after the index operation (also readmissions not directly related to the index THR operation) were included in the study.
Revision
We searched for revision surgery on the same hip after THR using codes NFC00, NFC20, NFC30, NFC40, NFC50, and NFC99. A search for removal of the total prosthesis from the hip was made in the FAR. Patients were followed up until the end of 2015. Only first revisions of the same hip as the primary THR were included.
Discharge home destination rate
Some patients are admitted to hospital from other social and welfare institutions and therefore are unlikely to be discharged home. Thus, only patients who came from home to hospital for their THR were included in the discharge destination analyses. The percentage of patients who were at home 1 week after THR was also analyzed irrespective of the hospital discharge destination.
Statistics
To adjust the dependent variables for confounding factors we used Poisson regression models for LOS and LUIC, and logistic regression models for revisions, readmissions, mortality, home 1 week after THR, and discharge destinations at the individual level. In addition, 95% confidence intervals (CIs) were determined. The patient’s age (under 40 years, over 40 years (divided into 9 5-year incremental groups up to age 85, and over 85 years)), sex, any previous THR, co-morbidities and femoral head size were included in all the adjusted analyses. Co-morbidities were determined using the diagnoses obtained from the Hospital Discharge Register from the beginning of 1987 to the date of surgery. In addition, the Social Insurance Institution database showing eligibility for reimbursement for medication costs and drug prescription was used to adjust for co-morbidity (Appendix 2, see Supplementary data). The illnesses chosen for adjustment were those that could have had an effect on prosthesis survivorship after THR (Jämsen et al. Citation2013), length of hospital stay, or the complications rate.
Differences in median LOS and in median LUIC were tested with the Mann–Whitney U-test (Wilcoxon rank-sum test). Median values for LOS and LUIC were used because of skewed distributions. The results for LOS and LUIC are presented with CIs and p-values. Differences in discharge destination, home 1 week after THR, readmission rates, sex, and age of patients were tested with the chi-square test and the results are presented with CIs and with p-values where appropriate. P-values less than 0.05 were considered statistically significant.
Ethics, funding, and potential conflicts of interest
Permission for the study was obtained from each register and from each study hospital. No ethics permission was required to perform this registry study. KP received a grant from the Finnish Arthroplasty Society to conduct this study. No conflicts of interest declared.
Results
3,193 THRs meeting the inclusion but not exclusion criteria were identified from the FHDR and FAR. Of these, 464 were performed in Hospital A before, and 437 after, implementation of the fast-track protocol. The corresponding volumes in the other hospitals were 265 and 302 in Hospital B, 402 and 424 in Hospital C, and 375 and 524 in Hospital D. No statistically significant age or sex differences were observed before or after implementing the fast-tracking protocol in Hospital A, or between other hospitals.
Hospital
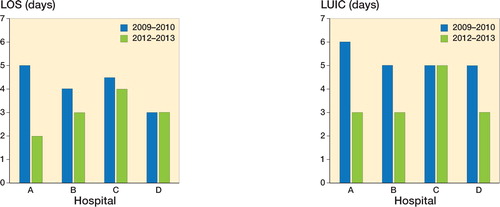
Before implementing fast track, median LOS in Hospital A was 5 (CI 2–8) days: after implementation, it fell to 2 (CI 1–5) days (p = < 0.001) (). After implementing fast track, Hospital A seemed to have the shortest median LOS, but the difference was only significant when compared with Hospital C (p = 0.001). Unlike the other study hospitals, after fast-tracking, Hospital A discharged 10% of the patients home on the first postoperative day. Discharge destination rates to home in Hospital A increased slightly (71% to 77%) but not statistically significantly despite the shortened LOS. Discharge destination rates were similar between hospitals.
Figure 1. a. Median length of stay in days (LOS) in 2 2-year periods for primary total hip arthroplasty in 4 different hospitals. Hospital A was defined as a fast-track hospital after 2011. b. Median lengths of uninterrupted institutional care (LUIC) in 2 2-year periods for primary total hip arthroplasty in four different hospitals. Hospital A was defined as a fast-track hospital after 2011.
Episode
Median LUIC in Hospital A was 6 (3–30) days before implementing fast track and 3 (CI 1–24) days (p = 0.001) after implementation (). After fast-track implementation, Hospital A had a shorter median LUIC than Hospital C. However, LUIC in Hospital A was similar to that in the other hospitals. The percentage of patients at home a week after THR increased from 57% (CI 53–61) before to 75% (CI 72–79) after fast-tracking in Hospital A (p < 0.001), and was higher than in Hospital C (p = 0.001). This percentage was similar between Hospitals A, B, and D.
Quality and complications
In Hospital A, the rate of revision THR (within 1 year after the primary operation) was 1.8% (CI 0.5–3.1) in 2009 and 2010 and 5.5% (CI 4.0–7.1) in 2012 and 2013 (). In the later study period, the increase in revisions in Hospital A was mainly due to revisions of hips operated in 2012: the rate of revision THR was 6.4% (CI 4.2–8.6) in 2012 decreasing to 4.4% (CI 2.3–6.4) 1 year later.
Table 3. Adjusted revision rates and mortality in 1 year in 2-year periods for primary total hip arthroplasty in 4 different hospitalsTable Footnotea
Unscheduled readmissions and mortality
In Hospital A, the 14-day readmission rate was 1.3% (CI 0.2–2.3) before and 2.9% (CI 1.7–4.1) after fast track implementation, and the corresponding 42-day readmission rates were 3.1% (CI 1.3–4.8) and 8.3% (CI 6.3–10). The increase in the 42-day readmission rate in Hospital A was significant (p < 0.001). The reasons for readmission recorded in the hospital discharge register are given in Table 4 (see Supplementary data). Readmissions due to a surgery-related infection increased from 0.2% to 2.1% and mechanical complications from 0.2% to 2.3%.
Mortality within 1 year after THR in Hospital A was 1.1% both before and after fast-track implementation (see ).
Discussion
We found that median LOS and LUIC both decreased after implementing fast-track while the readmission rate increased. The decrease in LOS did not affect the discharge destination rate. However, the proportion of patients at home 1-week post-surgery increased after implementation of the fast-track protocol.
Validity of the data
The level of completeness and accuracy in the FHDR is satisfactory (Sund Citation2012) and coverage of FAR is good (Institute for Health and Welfare Citation2017). The strength of our study is that it included data from all the private and public hospitals in Finland. Thus, all revisions and readmissions were included in the analyses. Only 1 hospital (A) in our study fully implemented the fast-track protocol. Thus, the changes in the studied parameters may in part be explained by other factors, for example decrease in LOS across the board, other changes in process and surgeons’ annual arthroplasty volume.
LOS
Several factors have been reported to be associated with LOS: surgeon volume, hospital volume, time between surgery and mobilization, and process standardization (such as fast-track programs) (Judge et al. Citation2006, Mitsuyasu et al. Citation2006, Bozic et al. Citation2010, Husted et al. Citation2010a, Paterson et al. Citation2010, Styron et al. Citation2011, Pamilo et al. Citation2013). Fast-track methods aim at optimizing the whole treatment protocol, which eventually leads to shorter LOS without compromising quality (Husted Citation2012). However, an annual decline in LOS after THR, even without a fast-track protocol, has been reported (Wolf et al. Citation2012, Pamilo et al. Citation2013). The same observation was also made in the hospitals we studied.
In our study, before fast-track implementation LOS and LUIC were longer in Hospital A than in the other hospitals studied. After fast-track implementation in Hospital A, LOS and LUIC decreased statistically significantly. The LOS value (median 2 days) is in line with those previously reported in fast-track studies. However, the effect on LUIC has not been reported (den Hartog et al. Citation2013, Winther et al. Citation2015). Median LUIC after implementing the fast-track protocol in our study was 3 days. Husted at al. (2012) reported a median LOS, which included transferals to other hospitals, of 4 days in 2009. The other hospitals in our study had implemented some elements of the fast-track protocol (). However, median LOS and LUIC decreased statistically significantly only in Hospital A, which had systematically implemented fast-tracking to its full extent. Further, after fast-track implementation Hospital A showed somewhat shorter LOS, but the difference was only statistically significant when compared with Hospital C.
Discharge destination
Shorter LOS has been coupled with a higher likelihood of discharge to an extended institutional care facility (Paterson et al. Citation2010). 2 earlier fast-track studies reported no change in the proportion of patients discharged to their own homes after introduction of the fast-track protocol, the rate remaining at about 80% (den Hartog et al. Citation2015, Winther et al. Citation2015). Our results accord with these. However, in our study, the proportion of patients at home 1 week after THR increased statistically significantly after fast-tracking was implemented. This is a new finding, as no previous studies have reported on this issue.
Unplanned readmissions
Comparison of readmission rates between studies is difficult. Definitions of readmission vary between studies as also do the diagnoses included. Moreover, some complications may be treated in an outpatient setting in one hospital and during readmission in another. Readmissions to other hospitals have not been included in all previous studies. A recent systematic review found the readmission rate after THR to be 5.6% within 30 days and 7.7% within 90 days (Ramkumar et al. Citation2015). The readmission rate within 90 days after fast-track THR has been reported to be between 8.6% and 11%, with no increase after implementing the protocol (Husted et al. Citation2010b, Citation2016, den Hartog et al. Citation2013, Jorgensen et al. Citation2013b, Glassou et al. Citation2014, Winther et al. Citation2015). However, we found that the readmission rate increased from 3.1% to 8.3% within 42 days after fast-track implementation. This increase was mainly due an increase in infections and mechanical complications, also potentially causing the need for revision.
Revision
The revision rate after fast-track THR has been reported to be between 1.4% and 2.9% within 90 days and 2.9% within 1 year (Husted et al. Citation2008, den Hartog et al. Citation2013, Glassou et al. Citation2014, Winther et al. Citation2015). An earlier study raised the possibility of an association between an elevated infection-related revision risk and the introduction of a fast-track protocol (Amlie et al. Citation2016). In contrast to previous studies (den Hartog et al. Citation2013, Glassou et al. Citation2014), the 1-year revision rate in our study showed a statistically non-significant increase from 1.8% to 5.5% after a fast-track protocol was introduced. We believe that the trend towards a higher revision rate was associated with other factors, rather than fast-track THR per se. For example, simultaneously with fast-track implementation we enhanced operating theater efficiency and introduced the use of a new uncemented implant stem. The learning curve associated with the use of a new implant stem potentially caused complications at the beginning. Enhancing operation theater efficiency can at first induce an unnecessary feeling of hurry, which could also cause complications.
Mortality
An enhanced recovery program has been found to be associated with a significant or nearly significant reduction in 30-day, 90-day, and 2-year mortality after THR and TKR (Malviya et al. Citation2011, Savaridas et al. Citation2013, Khan et al. Citation2014). 90-day mortality with fast-track THR and TKR has been reported to be 0.2%–0.5% (Husted et al. Citation2010b, Malviya et al. Citation2011, Khan et al. Citation2014, Jorgensen et al. Citation2017). In our study, in line with previous research (Savaridas et al. Citation2013), the 1-year mortality rate was 1.1% both before and after implementing fast-tracking.
Summary
After implementing fast-tracking, LOS and LUIC declined substantially without affecting discharge destination. It is possible that a learning curve also exists in process standardization, causing more readmissions and revisions in the early stage after a change of protocol.
Supplementary data
Table 4 and Appendices 1 and 2 are available as supplementary data in the online version of this article, http://dx.doi.org/10.1080/17453674.2017.1370845
KJP, PT, MiP, MaP, VR, and JP wrote the manuscript. PT and MiP performed the data analysis. All contributed to the conception and design of the study, to critical analyses of the data, to interpretation of the findings, and to critical revision of the manuscript.
Acta thanks Sameer Khalid Khan and Per Kjaersgaard-Andersen for help with peer review of this study.
IORT_A_1370845_SUPP.PDF
Download PDF (31.3 KB)Related Research Data
- Amlie E, Lerdal A, Gay CL, Hovik O, Nordsletten L, Dimmen S. A Trend for increased risk of revision surgery due to deep infection following fast-track hip arthroplasty. Adv Orthop 2016; 2016: 7901953.
- Bozic K J, Maselli J, Pekow P S, Lindenauer P K, Vail T P, Auerbach A D. The influence of procedure volumes and standardization of care on quality and efficiency in total joint replacement surgery. J Bone Joint Surg Am 2010; 92 (16): 2643–52.
- Glassou E N, Pedersen A B, Hansen T B. Risk of re-admission, reoperation, and mortality within 90 days of total hip and knee arthroplasty in fast-track departments in Denmark from 2005 to 2011. Acta Orthop 2014; 85 (5): 493–500.
- Gromov K, Troelsen A, Otte K S, Orsnes T, Ladelund S, Husted H. Removal of restrictions following primary THA with posterolateral approach does not increase the risk of early dislocation. Acta Orthop 2015; 86(4): 463–8.
- den Hartog Y M, Mathijssen N M, Vehmeijer S B. Reduced length of hospital stay after the introduction of a rapid recovery protocol for primary THA procedures. Acta Orthop 2013; 84 (5): 444–7.
- den Hartog YM, Mathijssen NMC, Vehmeijer SBW. Total hip arthroplasty in an outpatient setting in 27 selected patients. Acta Orthop 2015; 86 (6): 667–70.
- Husted H. Fast-track hip and knee arthroplasty: Clinical and organizational aspects. Acta Orthop 2012; 83(Suppl346): 1–39.
- Husted H, Holm G. Fast track in total hip and knee arthroplasty: Experiences from Hvidovre University Hospital, Denmark. Injury 2006; 37(Suppl5): S31–S5.
- Husted H, Holm G, Jacobsen S. Predictors of length of stay and patient satisfaction after hip and knee replacement surgery: Fast-track experience in 712 patients. Acta Orthop 2008; 79 (2): 168–73.
- Husted H, Hansen H C, Holm G, Bach-Dal C, Rud K, Andersen K L, et al. What determines length of stay after total hip and knee arthroplasty? A nationwide study in Denmark. Arch Orthop Trauma Surg 2010a; 130 (2): 263–8.
- Husted H, Otte K S, Kristensen B B, Orsnes T, Kehlet H. Readmissions after fast-track hip and knee arthroplasty. Arch Orthop Trauma Surg 2010b; 130 (9): 1185–91.
- Husted H, Lunn T H, Troelsen A, Gaarn-Larsen L, Kristensen B B, Kehlet H. Why still in hospital after fast-track hip and knee arthroplasty? Acta Orthop 2011; 82 (6): 679–84.
- Husted H, Jensen C M, Solgaard S, Kehlet H. Reduced length of stay following hip and knee arthroplasty in Denmark 2000-2009: from research to implementation. Arch Orthop Trauma Surg 2012; 132 (1): 101–4.
- Husted H, Jørgensen C C, Gromov K, Kehlet H, Hip on behalf of the LFC for F, Group KRC. Does BMI influence hospital stay and morbidity after fast-track hip and knee arthroplasty? Acta Orthop 2016; 87 (5): 466–72.
- ICD-10. International statistical classification of diseases and related health problems 10th revision: http://apps.who.int/classifications/icd10/browse/2010/en. Vol. 2012. 2010.
- Institute for Health and Welfare. Finnish Arthroplasty Register: https://www.thl.fi/far//#data/cphd [Internet]. Vol. 2017. 2017. Available from: https://www.thl.fi/far//#data/cphd
- Jämsen E, Peltola M, Eskelinen A, Lehto M U. Comorbid diseases as predictors of survival of primary total hip and knee replacements: A nationwide register-based study of 96,754 operations on patients with primary osteoarthritis. Ann Rheum Dis 2013; 72(12): 1975–82
- Jorgensen C C, Kehlet H, Group LFC for FH and KRC. Fall-related admissions after fast-track total hip and knee arthroplasty: Cause of concern or consequence of success? Clin Interv Aging 2013a; 8: 1569–77.
- Jorgensen C C, Kehlet H, Group LFC for FH and KRC. Role of patient characteristics for fast-track hip and knee arthroplasty. Br J Anaesth 2013b; 110 (6): 972–80.
- Jorgensen C C, Kjaersgaard-Andersen P, Solgaard S, Kehlet H, Group LFC for FH and KRC. Hip dislocations after 2,734 elective unilateral fast-track total hip arthroplasties: Incidence, circumstances and predisposing factors. Arch Orthop Trauma Surg 2014; 134 (11): 1615–22.
- Jorgensen C C, Kehlet H, group LFC for FH and KRC. Time course and reasons for 90-day mortality in fast-track hip and knee arthroplasty. Acta Anaesthesiol Scand 2017; 1(4): 436–44.
- Judge A, Chard J, Learmonth I, Dieppe P. The effects of surgical volumes and training centre status on outcomes following total joint replacement: Analysis of the Hospital Episode Statistics for England. J Public Health (Oxf) 2006; 28 (2): 116–24.
- Khan S K, Malviya A, Muller S D, Carluke I, Partington P F, Emmerson K P, et al. Reduced short-term complications and mortality following enhanced recovery primary hip and knee arthroplasty: Results from 6,000 consecutive procedures. Acta Orthop 2014; 85 (1): 26–31.
- Mäkelä K T, Hakkinen U, Peltola M, Linna M, Kroger H, Remes V. The effect of hospital volume on length of stay, re-admissions, and complications of total hip arthroplasty. Acta Orthop 2011a; 82 (1): 20–6.
- Mäkelä K T, Peltola M, Sund R, Malmivaara A, Hakkinen U, Remes V. Regional and hospital variance in performance of total hip and knee replacements: A national population-based study. Ann Med 2011b; 43(Suppl1): S31–S8.
- Malviya A, Martin K, Harper I, Muller S D, Emmerson K P, Partington P F, et al. Enhanced recovery program for hip and knee replacement reduces death rate. Acta Orthop 2011; 82 (5): 577–81.
- Mitsuyasu S, Hagihara A, Horiguchi H, Nobutomo K. Relationship between total arthroplasty case volume and patient outcome in an acute care payment system in Japan. J Arthroplasty 2006; 21 (5): 656–63.
- Pamilo K J, Peltola M, Mäkelä K, Häkkinen U, Paloneva J, Remes V. Is hospital volume associated with length of stay, re-admissions and reoperations for total hip replacement? A population-based register analysis of 78 hospitals and 54,505 replacements. Arch Orthop Trauma Surg 2013; 133 (12).
- Paterson J M, Williams J I, Kreder H J, Mahomed N N, Gunraj N, Wang X, et al. Provider volumes and early outcomes of primary total joint replacement in Ontario. Can J Surgery/Journal Can Chir 2010; 53 (3): 175–83.
- Ramkumar P N, Chu C T, Harris JD, Athiviraham A, Harrington M A, White D L, et al. Causes and rates of unplanned readmissions after elective primary total joint arthroplasty: A systematic review and meta-analysis. Am J Orthop (Belle Mead NJ) 2015; 44 (9): 397–405.
- Savaridas T, Serrano-Pedraza I, Khan S K, Martin K, Malviya A, Reed M R. Reduced medium-term mortality following primary total hip and knee arthroplasty with an enhanced recovery program: A study of 4,500 consecutive procedures. Acta Orthop 2013; 84 (1): 40–3.
- Styron J F, Koroukian S M, Klika A K, Barsoum W K. Patient vs provider characteristics impacting hospital lengths of stay after total knee or hip arthroplasty. J Arthroplasty 2011; 26 (8): 1412–18.
- Sund R. Quality of the Finnish Hospital Discharge Register: A systematic review. Scand J Public Health 2012; 40 (6): 505–15.
- Winther S B, Foss O A, Wik T S, Davis S P, Engdal M, Jessen V, et al. 1-year follow-up of 920 hip and knee arthroplasty patients after implementing fast-track. Acta Orthop 2015; 86 (1): 78–85.
- Wolf B R, Lu X, Li Y, Callaghan J J, Cram P. Adverse outcomes in hip arthroplasty: Long-term trends. J Bone Joint Surg Am 2012; 94 (14): e103.