
Abstract
Kinesio taping (KT) is a commonly used intervention in sports and, recently, KT has become popular among athletes competing in sport climbing and bouldering events. However, evidence on the effect of KT on grip strength and endurance is still controversial. Therefore, the purpose of this study was to evaluate immediate effects of KT on muscular strength and endurance of the finger flexor muscles in sport climbers. Twenty recreationally-trained active sport climbers (10 men, 10 women) aged 28.5 ± 10.6 years performed one familiarisation trial and subsequently, in a randomised crossover design, two test trials either with (TAPE) or without (CONTROL) KT over the finger flexor muscles. Test trials consisted of three performance measurements (hand grip strength and endurance, finger hang, and lap climbing) at intervals of 48 h in a randomised order. We observed no significant differences in the parameters of hand grip peak force, fatigue index, finger hang time, lap climbing distance and time, or maximum blood lactate values after lap climbing between the TAPE and CONTROL trials (p > 0.05). The participants’ climbing ability was significantly correlated with the intra-individual performance changes between the TAPE and CONTROL conditions for the fatigue index (r = −0.598, p = 0.005), but not in any of the other performance-related parameters. Therefore, KT over the finger flexor muscles neither enhanced hand grip strength and endurance nor the sport climbing performance parameters of finger hang, lap climbing distance and time, and maximum blood lactate values after lap climbing.
Highlights
Muscular strength- and endurance-enhancing effects of kinesio taping on sport climbing performance has not been investigated so far.
Kinesio taping had no immediate effects on sport climbing performance and did not diminish the effect of muscle fatigue.
Introduction
In the 1970s, kinesio taping (KT) was developed by the Japanese chiropractor Kenzo Kase. Kinesio tape is an elastic, cotton fabric tape with elastic properties similar to the skin that may be stretched up to 160% of its original length (Kase, Wallis, & Kase, Citation2013). Initially, KT was used mostly for treatment of injury, pain reduction, and joint stabilisation (Williams, Whatman, Hume, & Sheerin, Citation2012). Within the last few decades, KT received increased public attention and has also gained popularity among sport professionals for its assumed role in injury prevention and performance enhancement (Williams et al., Citation2012). To date, the proposed therapeutic objectives of KT include pain inhibition, proprioceptive and muscle facilitation, improvement of blood and lymph circulation, reduction of muscle fatigue, and delayed onset of muscle soreness (Basset, Lingman, & Ellis, Citation2010; Csapo & Alegre, Citation2015; Kase et al., Citation2013). In addition, according to Kenzo Kase, the application of the elastic tape leads to tension in the skin, which induces greater motor unit recruitment and subsequent muscle function and muscle strength by facilitating the contraction of inactive motor units (Kase et al., Citation2013). However, evidence of KT’s effects on muscle strength and endurance remains controversial (Vered, Oved, Zilberg, & Kalichman, Citation2016; Zhang et al., Citation2016). Some studies proposed the effectiveness of KT on muscle strength (Lumbroso, Ziv, Vered, & Kalichman, Citation2014; Vered et al., Citation2016), rate of force development (Magalhães et al., Citation2016; Yeung et al., Citation2015), and sprint cycling performance (Trecroci, Formenti, Rossi, Esposito, & Alberti, Citation2017). However, several studies have not supported the beneficial effects of KT on muscular performance parameters (Cai, Au, An, & Cheung, Citation2016; Lee, Jung, Ok, & Lee, Citation2017; Strutzenberger, Moore, Griffiths, Schwameder, & Irwin, Citation2016). In addition, a recent meta-analysis showed that KT to facilitate muscular contraction has no or only negligible effect on muscle strength (Csapo & Alegre, Citation2015). However, few data are available on the effect of KT on muscle endurance parameters as well as muscle fatigue during repetitive exercise bouts or prolonged dynamic movements (Zhang et al., Citation2016). The few studies existing on this topic suggest positive effects of KT on reducing muscle fatigue (Álvarez-Álvarez, José, Rodríguez-Fernández, Güeita-Rodríguez, & Waller, Citation2014; Lee et al., Citation2017; Zhang et al., Citation2016). Hence, there is still uncertainty concerning the beneficial effects of KT in improving muscular strength and endurance.
However, KT is gaining popularity in elite athletes competing at international events such as the Summer Olympics in Bejing (2008), London (2012), and Rio de Janeiro (2016) (Csapo & Alegre, Citation2015). KT applications have also become popular among athletes competing in sport climbing and bouldering events. Athletes have worn these tapes mainly over the shoulder joint and forearm, such as the Korean athlete Jongwon Chon at the Bouldering IFSC series 2018 and the Serbian athlete Staša Gejo at the IFSC Climbing World Championships Innsbruck in 2018. In particular, KT over the wrist flexor muscles may lead to performance enhancement in sport climbing and bouldering performance because climbing performance is mainly dependent on finger flexor strength and endurance (España-Romero et al., Citation2009; Vigouroux, Goislard de Monsabert, & Berton, Citation2015; Watts, Martin, & Durtschi, Citation1993). Climbing is characterised by an acyclic movement pattern that requires intermittent isometric contractions of the forearms separated by dynamic whole-body movements (Baláš et al., Citation2016). Therefore, despite other factors such as coordination and technique, as well as anthropometric, physiological, mental, and tactical parameters, intermittent finger flexor muscle endurance is a key element of sport-climbing performance (Fryer et al., Citation2015; Michailov, Citation2014). Climbing performance and failure in competitive climbing tasks are often related to muscle soreness and fatigue of the finger flexor muscles (Philippe, Wegst, Müller, Raschner, & Burtscher, Citation2012; Watts et al., Citation1993).
Research on KT over the finger flexor muscles and its influence on muscle strength and endurance parameters remain controversial and show no relation to a specific sport. Several studies lend support to the postulated strength-enhancing effect of KT and report augmented handgrip strength after KT over forearm muscles compared with baseline measurements or a control and placebo group (Kim & Kim, Citation2016; Kouhzad Mohammadi et al., Citation2014; Lemos, Pereira, Protássio, Lucas, & Matheus, Citation2015). However, there are other studies that have shown that KT is an ineffective method to enhance grip strength (Chang, Chou, Lin, Lin, & Wang, Citation2010; Zhang et al., Citation2016). Zhang et al. (Citation2016) further concluded that KT over the wrist flexors and extensors may not be able to enhance muscle strength, but could have a positive effect in preventing muscle fatigue in muscle endurance performance tasks in tennis players.
Since there is evidence that KT over the finger flexor muscles may reduce muscle fatigue during repeated and prolonged grip strength tasks, the main aim of our study was to examine the immediate effects of KT over the finger flexors on sport climbing performance. We hypothesised that KT over the finger flexor muscles would lead to an increase in muscle endurance and sport climbing performance related parameters.
Materials and methods
Experimental design
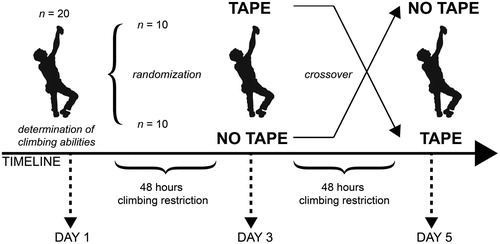
The experimental protocol was completed in three visits separated by at least 48 h (). On the first visit, each participant was informed of the purpose, benefits, and risks associated with the study and underwent a familiarisation trial for the test procedures. On the following two visits, the participants completed the test trials in a crossover design either with kinesio tape (TAPE) or without tape (CONTROL) application. To reduce the interference of uncontrolled variables, all participants were asked to maintain their normal dietary habits and habitual lifestyle before and during the experimental period. Participants were instructed not to exercise during the 48 h before the test trials. We also asked them to avoid alcohol and caffeine ingestion during the experimental period. Furthermore, the evaluation took place at approximately the same time of day for each participant to minimise the effects of diurnal variations on the measured variables. All tests were performed at an indoor climbing wall. Before beginning the assessments, participants completed a standardised 10-minute warm-up, including a general activation of the cardiovascular system, coordination, and light dynamic stretching.
Figure 1. Experimental design.
Within the familiarisation trial, an adjustable Jamar® Plus+ (Patterson Medical/Sammons Preston, Illinois, USA) digital hand dynamometer was used to record handgrip maximum voluntary contraction (MVC) (Ozimek, Staszkiewicz, Rokowski, & Stanula, Citation2016). The participants were seated without leaning with an elbow flexion of 90°, a slight shoulder abduction of about 15°, and the forearms in a neutral supination/pronation position (Trampisch, Franke, Jedamzik, Hinrichs, & Platen, Citation2012). The subjects were asked to grip the handle of the dynamometer with maximum effort for 3 s with a one-minute rest break between the three trials. Maximum force (Fmax) values were recorded for the right and the left hand, and subsequently, the mean value was determined to provide an average handgrip score for both hands (Kim & Kim, Citation2016). To determine the onsight climbing performance, the subjects were first asked for their most difficult ascent by top rope or red point style rated on the UIAA (Union Internationale des Associations d’Alpinisme) scale. Participants then had to climb a predefined route at the self-reported level of difficulty in top rope style. If this route was accomplished without falling, the degree increased in the next route until no better attempt was possible. If the predefined route was not accomplished, the degree decreased accordingly in the next attempt. Between the attempts, a break of 20 min was given. The best attempt was rated as onsight climbing performance within this study. The UIAA scale for free climbing difficulty currently extends from I to XII (Draper et al., Citation2015). To analyze climbers’ abilities statistically (), the UIAA climbing scale was converted to the metric IRCRA (International Rock Climbing Research Association) scale according to recommendations for the statistical analysis of sport-climbing grades (Draper et al., Citation2015). The following two visits (TAPE, CONTROL) included three different measurements (hand grip endurance, finger hang, lap climbing) after the completion of the standardised 10-minute warm-up. Between the measurements, the subject took a ten-minute break, which had to be spent resting.
Table I. Anthropometric, climbing ability, and grip strength of male (n = 10) and female (n = 10) participants.
Participants
A total of 20 (10 male, 10 female) recreationally- and moderately-trained climbers volunteered to participate in this study. The mean (± SD) age was 28.5 ± 10.6 y, with a mean height of 173.2 ± 9.8 cm, mean body mass of 64.0 ± 8.2 kg, and a mean BMI of 21.3 ± 1.5 kg/m². Participants showed climbing abilities between IRCRA 13 and 20 (16.5 ± 1.9), and a maximum grip force of 380.2 ± 79.0 N. Sex-specific characteristics are shown in . All 20 volunteers satisfied the inclusion and exclusion criteria of this study. Inclusion criteria included a top rope onsight climbing ability of at least UIAA grade VII- (IRCRA 13), climbing experience of at least three years, sport climbing as their predominant discipline by self-report, and an average training load of at least two days per week with three hours per session within the last three months. All participants underwent a medical screening before entering the study. Participants had to be in good health without any pre-existing cardiac or pulmonary conditions. Exclusion criteria included acute muscular injuries or restrictions, as well as acute infections, alcohol consumption during the test period, and chronic medication intake. All participants provided written informed consent prior to participation and all procedures were approved by the ethical committee of the German Sport University Cologne in accordance with the Declaration of Helsinki.
Taping technique
The taping technique performed for the TAPE test trial aimed to influence muscle function by activating the finger flexors muscles. Kinesio tapes were applied on the finger flexor muscles of both hands consistent with the guidelines for kinesio taping of the forearm suggested and used in former studies (Chang et al., Citation2010; Kase et al., Citation2013; Zhang et al., Citation2016). All taping was completed by the same investigator, who was trained and experienced in working with kinesio tape applications. Before applying the tape, the skin of the participants was shaved and cleaned with alcohol. Standard 2-in (5 cm) blue kinesio tape (PINOTAPE® pro Therapy blue, PINO GmbH, Hamburg, Germany) was used for all tape applications and the length of tape was measured from 2 cm to the medial epicondyle of the humerus to the wrist joint line for each participant. Subsequently, the strip was cut down the middle to produce two tails (“Y-strip”) and the Y-strip was applied on the common finger flexor muscle from its insertion to origin with 75–100% tape tension to the actively pre-stretched muscle to achieve a toning effect (Bökelberger & Lehner, Citation2015). Pre-stretching of the finger flexor muscles was achieved by full finger extension, a hyperextended wrist, full elbow extension, and full forearm supination. The first tail of the Y-strip was then applied along the medial edge of the forearm over ulnar finger flexors to the medial epicondyle and the second tail on the middle of the forearm along the radial finger flexors to the medial epicondyle.
Hand grip strength and endurance
For the measurement of finger flexor strength and endurance, maximum handgrip and hand grip endurance measurements were carried out first during the test trials. To assess maximum handgrip strength and hand grip endurance, every three seconds an audible signal was given, which signalled the subject to change between maximal effort and relaxation. Each participant completed 10 MVC trials. MVC had to be built up from zero to maximum effort within three seconds and was followed by a 3-s rest for each trial. Participants were asked to grip the handle of the dynamometer as hard as possible and were verbally encouraged throughout the test. We determined the variables peak force (Fmax), lowest force (Fmin), and fatigue index (FI) over the 10 MVC trials. Fmax and Fmin were defined as highest and lowest force, respectively, achieved within the 10 MVC trials, and FI was calculated as FI (%) = [(Fmax – Fmin) / Fmax] x 100. The variables FI and Fmax were used for further statistical analyses. To eliminate a potential hand dominance, right- and left-hand values were averaged for FI and Fmax, and both variables were defined as non-specific muscle endurance parameter dominance (Baláš, Pecha, Martin, & Cochrane, Citation2012; Watts, Citation2003).
Finger hang
The second measurement of the test trials was the climbing-specific finger hang. To assess the participants’ muscle endurance (resistance to fatigue) of the finger flexors, climbers held onto a 4-cm ledge with straight arms (Ozimek et al., Citation2016). The hold on the ledge was carried out with four fingers using an open grip, whereas the thumb was not included to the grip and was located at the bottom of the ledge (Baláš et al., Citation2012). The elbow, shoulder, and hip joints had to remain fully extended while hanging on the lap. The time the climber could maintain this position on the ledge was defined as the specific muscle endurance parameter (hang time in seconds).
Lap climbing
The third measurement of the test trials was lap climbing (LC) to assess sport climbing endurance performance. Climbing time to exhaustion was found to be a climbing performance determinant in sport climbers and therefore adequate to assess intermittent isometric endurance in combination with upward movements (España-Romero et al., Citation2009). In LC, the participants had to climb a predefined route as often as possible on top rope belay with no rest between the ascents. The route was set one UIAA grade below the maximum onsight climbing level assessed during the familiarisation trial (e.g. if climbing ability was VIII, the LC route would be VII). To standardise the potential influence of recovery strategies on climbing performance (Baláš et al., Citation2016), participants were not allowed to chalk or shake their hands during climbing or lowering. The LC had to be accomplished until a fall due to fatigue. The climbing time (LCT) in minutes and the total covered climbing distance (LCD) in metres were assessed using video analysis. After the subject had to cease because of fatigue, capillary blood samples (20 μl) were collected immediately and 2, 4, 6 and 8 min after the LC trials to assess blood lactate values. Capillary blood samples were taken from the earlobe while participants were sitting next to the climbing wall without any further physical activity. Blood lactate measurements were conducted directly after the LC trials (Biosen S-Line, EKF-diagnostic GmbH, Magdeburg, Germany). The maximum post-exercise lactate concentration (Lamax) was used for statistical analyses.
Statistical analyses
Data are presented as means ± standard deviations. The Shapiro–Wilk test was used to identify all departures from the normal distribution. Paired sample t-tests were used to compare the parameters FI, Fmax, hang time, Lamax, LCT, and LCD between the TAPE and CONTROL conditions. We also examined for a potential confounding effect by comparing the first and second test trials independent of the KT application (TRIAL 1; TRIAL 2) for the variables FI, Fmax, hang time, and Lamax using a paired-sample t-test. Cohen’s d (d) was used to calculate effect sizes, with 0.2 considered to indicate small effects, 0.5 considered to indicate medium effects, and 0.8 considered to indicate large effects (Cohen, Citation1992). When variables were not normally distributed (LCT TAPE; LCD TAPE), Wilcoxon tests were used to identify differences between the TAPE and CONTROL conditions and the first and second test trials. Correlation coefficients (r) were used to calculate effect sizes. Intra-individual performance changes between the TAPE and CONTROL conditions were calculated as Δ values (TAPE – CONTROL). Two-sample t-tests were used to detect possible differences in Δ values between male and female participants and Cohen’s d (d) was used to calculate effect sizes. When variables were not normally distributed (Δ LCT, Δ LCD), the Mann–Whitney U test was used, and correlation coefficients (r) were used to calculate effect sizes. Pearson’s correlation test was used to identify associations between the climbing ability parameter IRCRA climbing ability and the performance changes (Δ FI, Δ Fmax, Δ hang time), as well as the associated physiological response (Δ Lamax). When variables were not normally distributed (Δ LCT, Δ LCD), the Spearman correlation test was used. The correlation coefficient was classified as trivial (0–0.09), small (0.10–0.29), moderate (0.30–0.49), large (0.50–0.69), very large (0.70–0.89), or nearly perfect (0.90–0.99) (Hopkins). An a priori power calculation indicated that 17 participants were needed to detect a significant difference between the TAPE and CONTROL conditions, based on an estimated α level of 0.05 and a power of 80% (based on muscular endurance enhancement results (time to failure task) after KT from an earlier study with an effect size of d = 0.65 (Álvarez-Álvarez et al., Citation2014)). The alpha level was set at p ≤ 0.05, and all analyses were conducted using SPSS 25 (IBM Corp., Armonk, NY, USA).
Results
Hand grip strength and endurance
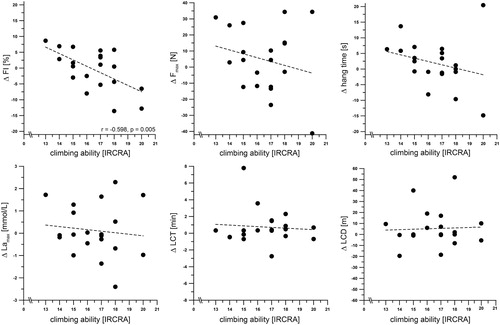
No significant differences were observed between the TAPE and CONTROL trials for FI (TAPE: 27.6 ± 6.4, CONTROL: 28.0 ± 6.9 %; p = 0.770, d = 0.07) and Fmax (TAPE: 374.8 ± 80.1, CONTROL: 370.1 ± 75.1 N; p = 0.318, d = 0.23) ( a, b). There was no difference between the two test trials for FI (TRIAL 1: 27.0 ± 6.9, TRIAL 2: 28.6 ± 6.3 %; p = 0.275, d = 0.19) and Fmax (TRIAL 1: 374.8 ± 80.1, TRIAL 2: 370.1 ± 75.1 N; p = 0.982, d = 0.05), suggesting that there was no period effect that may have negatively influenced our test results. There was no difference between male and female participants in Δ FI (MALE: −0.2 ± 6.6, FEMALE: −0.8 ± 6.6 %; p = 0.784, d = 0.08) and Δ Fmax (MALE: 9.6 ± 23.7, FEMALE: −0.2 ± 16.2 N; p = 0.295, d = 0.27). A large correlation was found between Δ FI and IRCRA climbing ability (r = −0.598, p = 0.005). However, Δ Fmax showed no correlation with IRCRA climbing ability (r = −0.224, p = 0.342) ().
Figure 2. Performance measurements with (TAPE) and without (CONTROL) kinesio tape application for a) fatigue index (FI), b) peak grip force (Fmax), c) hang time, d) Lamax, e) lap climbing time (LCT), and f) lap climbing distance (LCD). Data points represent individual values (○). Bar charts are means ± SD. See METHODS for further details.
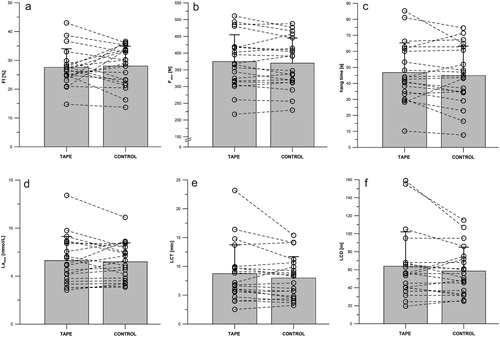
Figure 3. Relationships between IRCRA climbing ability and the intra-individual performance changes between the TAPE and CONTROL conditions (Δ FI, Δ Fmax, Δ hang time, Δ LCT, Δ LCD), as well as the associated physiological response (Δ Lamax). Data points represent individual values. See METHODS for further details, *p < 0.05.
Finger hang
We found no significant differences in hang time between the TAPE (44.9 ± 18.4 s) and CONTROL conditions (46.7 ± 18.5 s) (p = 0.291, d = 0.24) ( c). No significant difference was observed between the two test trials in hang time (TRIAL 1: 45.3 ± 17.4, TRIAL 2: 46.3 ± 19.5 s; p = 0.557, d = 0.09), suggesting that there was no period effect. There was no difference between male and female participants in Δ hang time (MALE: −0.6 ± 9.7, FEMALE: 4.4 ± 4.5 s; p = 0.159, d = 0.41). In addition, Δ hang time showed no correlation with IRCRA climbing ability (r = −0.261, p = 0.267) ().
Lap climbing
Lamax showed no significant differences between the TAPE (6.6 ± 2.5 mmol/L) and CONTROL (6.5 ± 2.0 mmol/L) (p = 0.642, d = 0.11) conditions ( d). No significant differences were found between the TAPE and CONTROL trials for LCT (TAPE: 8.7 ± 5.0, CONTROL: 8.0 ± 5.0 min; p = 0.151, r = 0.322) and LCD (TAPE: 63.9 ± 38.2, CONTROL: 58.6 ± 26.6 m; p = 0.287, r = 0.238) ( e, f). We found a significant difference between the two test trials for Lamax (TRIAL 1: 6.3 ± 2.0, TRIAL 2: 6.8 ± 2.5 mmol/L; p = 0.019, d = 0.69). However, there was no difference between the two test trials for LCT (TRIAL 1: 8.3 ± 3.9, TRIAL 2: 8.5 ± 4.9 min; p = 0.970, r = 0.103) and LCD (TRIAL 1: 58.1 ± 28.1, TRIAL 2: 64.4 ± 37.0 m; p = 0.061, r = 0.482). We found no difference between male and female participants in Δ Lamax (MALE: 0.3 ± 1.1, FEMALE: 0.0 ± 1.3 mmol/L; p = 0.623, d = 0.12), Δ LCT (MALE: 0.4 ± 1.0, FEMALE: 1.1 ± 2.8 min; p = 0.684, r = 0.093), and Δ LCD (MALE: 6.8 ± 16.5, FEMALE: 3.9 ± 18.2 m; p = 0.739, r = 0.085). In addition, there was no correlation between IRCRA climbing ability and Δ Lamax (r = −0.111, p = 0.642), Δ LCT (r = 0.201, p = 0.396), and Δ LCD (r = 0.051, p = 0.832) ().
Discussion
This investigation aimed to examine if KT over the finger flexor muscles had immediate effects on sport climbing performance and diminished the effect of muscle fatigue. Our results showed that there was no effect of KT over the finger flexor muscles on sport climbing related muscle strength and muscle endurance parameters or physiological responses. The findings are in contrast to our original hypothesis and to the positive effects of KT on muscle strength and endurance claimed by KT manufacturers and believed in by many athletes and physiotherapists. The results only suggested a possible relationship between the IRCRA climbing ability of our participants and an influence on the fatigue index under TAPE conditions ().
These results, however, are consistent with recent findings of no strength enhancing effects immediately following KT in healthy populations. Several studies could not find positive effects of KT on muscle strength in healthy participants for different muscle groups (Cai et al., Citation2016; Karahan et al., Citation2017; Strutzenberger et al., Citation2016; Vercelli et al., Citation2012), and even a recent meta-analysis concluded that KT to facilitate muscular contraction had no or only negligible effects on muscle strength (Csapo & Alegre, Citation2015). However, there are a few recent studies that have investigated the effects of KT on muscle endurance that have suggested that KT influences processes that lead to muscle fatigue positively. Zhang et al. (Citation2016) showed a decrease in work fatigue and the rate of decline in the moment of finger flexors after KT during repeated isokinetic wrist flexion. In addition, Álvarez-Álvarez et al. (Citation2014) observed differences between the time to failure task measuring trunk extensor muscular endurance of a KT group and a control group demonstrating that participants with KT were able to maintain the test position longer. Within the current study, there was no evident effect of improved muscle endurance either in hand grip endurance measurements or in finger hang or lap climbing. Our results only indicated a possible relationship between climbing ability and the influence of KT application on the fatigue index assessed in hand grip endurance measurements, with climbers with a higher IRCRA climbing ability showing possible positive effects rather than less skilled climbers. However, this single result should be interpreted with caution. Therefore, we suggest that future research should focus on highly trained, advanced to elite climbers with an IRCRA onsight climbing ability of at least VII+ (female) and VIII+ (male) (Draper et al., Citation2015), to detect possible influences of KT on the muscles’ resistance to fatigue. To our knowledge, there are only a few studies on the effectiveness of KT on sports performance abilities with complex movement situations or that investigate elite athletes. Moreover, the reported results of these studies have been contradictory and have lacked compelling evidence, with some studies supporting the strength- and endurance-enhancing effect of KT (Lumbroso et al., Citation2014; Trecroci et al., Citation2017; Vered et al., Citation2016), and others reporting no effects on a wide variety of sports–performance abilities (Boozari, Sanjari, Amiri, & Ebrahimi Takamjani, Citation2018; Reneker, Latham, McGlawn, & Reneker, Citation2018; Schiffer, Möllinger, Sperlich, & Memmert, Citation2015).
However, regardless of the uncertain evidence regarding the effects of KT on muscle performance, there is a persistent popularity of KT for various applications among athletes and physiotherapists. A potential reason for this may be the placebo effect, which alters muscle strength and endurance as a result of psychological variables such as motivation, expectancy and conditioning, and the interaction of these variables with physiological variables leading to better sport performance outcomes (Álvarez-Álvarez et al., Citation2014; Beedie & Foad, Citation2009). Vercelli et al. (Citation2012) already stated that 45% of the participants reported a perceived strength-enhancing effect of KT, although KT did not increase performance outcome measurements. Therefore, several studies have suggested that subjects and assessors should be blinded, as well as the inclusion of a placebo taping group to ensure methodological quality (Csapo & Alegre, Citation2015; Williams et al., Citation2012). The lack of a placebo group is therefore a limitation of our study, although this limitation would be of particular importance if there were significant differences between the TAPE and CONTROL conditions and a false positive error had to be assumed. Since we did not observe any differences, we do not believe that a placebo effect affected our results. Nevertheless, the use of an additional placebo group is recommended in future investigation.
The present study had several limitations that should be mentioned. One is the low test-power of all comparisons between the TAPE and CONTROL conditions. An a priori power calculation was conducted within the present study, which indicated a sample size of 17 participants for the detection of differences between the TAPE and CONTROL conditions. The a priori power calculation was based on muscular endurance enhancement results of a time-to-failure task from an earlier study, which reported a 35.5-second enhancement in Biering-Sorensen test score with an effect size of d = 0.65 with KT. However, smaller effect sizes were conducted within the current investigation and a sample size of 20 participants resulted in a test power of 25%, ranging between 8.9 and 38%, for the effect of taping on performance measurements. Power calculations of correlations reported within this study provided a test power ranging between 5.5 and 32%, except for the large correlation between Δ FI and IRCRA climbing ability (test power of 83%). This indicates an underpowered trial for the effect of taping, so detecting a significant difference between the TAPE and CONTROL conditions was very unlikely. Thus, because of the small effects we probably could not detect a possible difference with the small sample size of 20 participants, and therefore were not able to exclude a type 2 error within our interpretation. Nevertheless, we assume that possible undetected differences were too small to contribute to an overall sport climbing performance enhancement, as already speculated by other authors (Strutzenberger et al., Citation2016). We also examined for a potential confounding effect by comparing the first and second test trials (independent of the KT application) using paired-sample t-tests. There were no differences between both trials for most of the measured variables. However, there was a difference between the two trials for Lamax, suggesting that there was a period effect that may have negatively influenced our test results in lap climbing, although the related parameters LCT and LCD did not show any differences. The period effect may be explained by a habituation to the test protocol and therefore by a training effect, but this needs to be verified in future research. An additional aspect to be considered is the question whether certain KT application techniques might influence muscular strength- and endurance-enhancing effects. It has been a subject of controversial debates in recent years if KT either from the muscle origin to insertion or from the insertion to origin would result in augmented muscle strength and endurance (Csapo & Alegre, Citation2015). Traditional assumptions of the KT method suggested that origin to insertion application stimulates the muscle and insertion to origin application relaxes the muscle (Vered et al., Citation2016). However, newer findings have shown these traditional assumptions to be false and suggest that taping from insertion to origin helps to increase muscle strength and endurance (Fukui, Otake, & Kondo, Citation2017; Vered et al., Citation2016). Therefore, we do not expect that the applied taping technique within the current study negatively influenced the assessed performance outcomes.
In summary, our results suggested that KT over the finger flexor muscles enhanced neither hand grip strength and endurance nor the sport climbing performance parameters of finger hang, lap climbing distance and time, and maximum blood lactate values after lap climbing, but indicated a possible relationship between climbing ability and the influence of KT application on the fatigue index. However, the use of KT for performance improvement in sport climbing and bouldering could not be confirmed within this study and should be considered with caution.
Acknowledgments
We are grateful to the subjects for participating in this study. We thank our laboratory staff for their contributions and support. We thank PINO Pharmaceuticals GmbH for the free provision of the kinesio tape used in the study. No grant or funding support was provided for this study. We thank Peter Mittwede for editing a draft of this manuscript
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Álvarez-Álvarez, S., José, F. G.-M. S., Rodríguez-Fernández, A. L., Güeita-Rodríguez, J., & Waller, B. J. (2014). Effects of kinesio®tape in low back muscle fatigue: Randomized, controlled, doubled-blinded clinical trial on healthy subjects. Journal of Back and Musculoskeletal Rehabilitation, 27(2), 203–212. doi: 10.3233/BMR-130437
- Baláš, J., Michailov, M., Giles, D., Kodejška, J., Panáčková, M., & Fryer, S. (2016). Active recovery of the finger flexors enhances intermittent handgrip performance in rock climbers. European Journal of Sport Science, 16(7), 764–772. doi: 10.1080/17461391.2015.1119198
- Baláš, J., Pecha, O., Martin, A. J., & Cochrane, D. (2012). Hand–arm strength and endurance as predictors of climbing performance. European Journal of Sport Science, 12(1), 16–25. doi: 10.1080/17461391.2010.546431
- Basset, K., Lingman, S., & Ellis, R. (2010). The use and treatment efficacy of kinaesthetic taping for musculosceletal conditions: A systematic review. New Zealand Journal of Physiotherapy, 38(2), 56–62.
- Beedie, C. J., & Foad, A. J. (2009). The placebo effect in sports performance: A brief review. Sports Medicine, 39(4), 313–329. doi: 10.2165/00007256-200939040-00004
- Bökelberger, A., & Lehner, O. (2015). Kinesiologisches Taping: Das Arbeitsbuch (2nd ed). Bern: Hogrefe Verlag.
- Boozari, S., Sanjari, M. A., Amiri, A., & Ebrahimi Takamjani, I. (2018). Effect of gastrocnemius kinesio taping on countermovementjump performance and vertical stiffness following muscle fatigue. Journal of Sport Rehabilitation, 27(4), 306–311. doi: 10.1123/jsr.2017-0009
- Cai, C., Au, I. P. H., An, W., & Cheung, R. T. H. (2016). Facilitatory and inhibitory effects of kinesio tape: Fact or fad? Journal of Science and Medicine in Sport, 19(2), 109–112. doi: 10.1016/j.jsams.2015.01.010
- Chang, H.-Y., Chou, K.-Y., Lin, J.-J., Lin, C.-F., & Wang, C.-H. (2010). Immediate effect of forearm kinesio taping on maximal grip strength and force sense in healthy collegiate athletes. Physical Therapy in Sport, 11(4), 122–127. doi: 10.1016/j.ptsp.2010.06.007
- Cohen, J. (1992). A power primer, Psychological Bulletin.
- Csapo, R., & Alegre, L. M. (2015). Effects of kinesio(®) taping on skeletal muscle strength-A meta-analysis of current evidence. Journal of Science and Medicine in Sport, 18(4), 450–456. doi: 10.1016/j.jsams.2014.06.014
- Draper, N., Giles, D., Schöffl, V., Konstantin Fuss, F., Watts, P., Wolf, P., … Abreu, E. (2015). Comparative grading scales, statistical analyses, climber descriptors and ability grouping: International rock climbing research Association position statement. Sports Technology, 8(3-4), 88–94. doi: 10.1080/19346182.2015.1107081
- España-Romero, V., Ortega Porcel, F. B., Artero, E. G., Jiménez-Pavón, D., Gutiérrez Sainz, A., Castillo Garzón, M. J., & Ruiz, J. R. (2009). Climbing time to exhaustion is a determinant of climbing performance in high-level sport climbers. European Journal of Applied Physiology, 107(5), 517–525. doi: 10.1007/s00421-009-1155-x
- Fryer, S., Stoner, L., Lucero, A., Witter, T., Scarrott, C., Dickson, T., … Draper, N. (2015). Haemodynamic kinetics and intermittent finger flexor performance in rock climbers. International Journal of Sports Medicine, 36(2), 137–142. doi: 10.1055/s-0034-1385887
- Fukui, T., Otake, Y., & Kondo, T. (2017). The effects of new taping methods designed to increase muscle strength. Journal of Physical Therapy Science, 29(1), 70–74. doi: 10.1589/jpts.29.70
- Hopkins, W. G. A new view of statistics. Retrieved from http://www.sportsci.org/resource/stats/index.html
- Karahan, A. Y., Yildirim, P., Kucuksarac, S., Ordahan, B., Turkoglu, G., Soran, N., … Zinnuroglu, M. (2017). Effect of kinesio taping on elbow muscle strength in healthy individuals: A randomized trial1. Journal of Back and Musculoskeletal Rehabilitation, 30(2), 317–323. doi: 10.3233/BMR-160529
- Kase, K., Wallis, J., & Kase, T. (2013). Clinical therapeutic applications of the kinesio taping method (3rd ed.). [New Mexico]: Kinesio Taping Association.
- Kim, J. Y., & Kim, S. Y. (2016). Effects of kinesio tape compared with non-elastic tape on hand grip strength. Journal of Physical Therapy Science, 28(5), 1565–1568. doi: 10.1589/jpts.28.1565
- Kouhzad Mohammadi, H., Khademi Kalantari, K., Naeimi, S. S., Pouretezad, M., Shokri, E., Tafazoli, M., … Kardooni, L. (2014). Immediate and delayed effects of forearm kinesio taping on grip strength. Iranian Red Crescent Medical Journal, 16(8), e19797. doi: 10.5812/ircmj.19797
- Lee, N. H., Jung, H. C., Ok, G., & Lee, S. (2017). Acute effects of kinesio taping on muscle function and self-perceived fatigue level in healthy adults. European Journal of Sport Science, 17(6), 757–764. doi: 10.1080/17461391.2017.1294621
- Lemos, T. V., Pereira, K. C., Protássio, C. C., Lucas, L. B., & Matheus, J. P. C. (2015). The effect of kinesio taping on handgrip strength. Journal of Physical Therapy Science, 27(3), 567–570. doi: 10.1589/jpts.27.567
- Lumbroso, D., Ziv, E., Vered, E., & Kalichman, L. (2014). The effect of kinesio tape application on hamstring and gastrocnemius muscles in healthy young adults. Journal of Bodywork and Movement Therapies, 18(1), 130–138. doi: 10.1016/j.jbmt.2013.09.011
- Magalhães, I., Bottaro, M., Mezzarane, R. A., Neto, F. R., Rodrigues, B. A., Ferreira-Júnior, J. B., & Carregaro, R. L. (2016). Kinesiotaping enhances the rate of force development but not the neuromuscular efficiency of physically active young men. Journal of Electromyography and Kinesiology, 28, 123–129. doi: 10.1016/j.jelekin.2016.04.003
- Michailov, M. (2014). Workload characteristics, performance limiting factors and methods for strength and endurance training in rock climbing. Medica Sportiva, 18(3), 97–106.
- Ozimek, M., Staszkiewicz, R., Rokowski, R., & Stanula, A. (2016). Analysis of tests evaluating sport climbers’ strength and isometric endurance. Journal of Human Kinetics, 53, 249–260. doi: 10.1515/hukin-2016-0027
- Philippe, M., Wegst, D., Müller, T., Raschner, C., & Burtscher, M. (2012). Climbing-specific finger flexor performance and forearm muscle oxygenation in elite male and female sport climbers. European Journal of Applied Physiology, 112(8), 2839–2847. doi: 10.1007/s00421-011-2260-1
- Reneker, J. C., Latham, L., McGlawn, R., & Reneker, M. R. (2018). Effectiveness of kinesiology tape on sports performance abilities in athletes: A systematic review. Physical Therapy in Sport, 31, 83–98. doi: 10.1016/j.ptsp.2017.10.001
- Schiffer, T., Möllinger, A., Sperlich, B., & Memmert, D. (2015). Kinesio taping and jump performance in elite female track and field athletes and jump performance in elite female track and field athletes. Journal of Sport Rehabilitation, 24(1), 47–50. doi: 10.1123/jsr.2013-0111
- Strutzenberger, G., Moore, J., Griffiths, H., Schwameder, H., & Irwin, G. (2016). Effects of gluteal kinesio-taping on performance with respect to fatigue in rugby players. European Journal of Sport Science, 16(2), 165–171. doi: 10.1080/17461391.2015.1004372
- Trampisch, U. S., Franke, J., Jedamzik, N., Hinrichs, T., & Platen, P. (2012). Optimal Jamar dynamometer handle position to assess maximal isometric hand grip strength in epidemiological studies. The Journal of Hand Surgery, 37(11), 2368–2373. doi: 10.1016/j.jhsa.2012.08.014
- Trecroci, A., Formenti, D., Rossi, A., Esposito, F., & Alberti, G. (2017). Acute effects of kinesio taping on a 6 s maximal cycling sprint performance. Research in Sports Medicine, 25(1), 48–57. doi: 10.1080/15438627.2016.1258644
- Vercelli, S., Sartorio, F., Foti, C., Colletto, L., Virton, D., Ronconi, G., & Ferriero, G. (2012). Immediate effects of kinesiotaping on quadriceps muscle strength: A single-blind, placebo-controlled crossover trial. Clinical Journal of Sport Medicine, 22(4), 319–326. doi: 10.1097/JSM.0b013e31824c835d
- Vered, E., Oved, L., Zilberg, D., & Kalichman, L. (2016). Influence of kinesio tape application direction on peak force of biceps brachii muscle: A repeated measurement study. Journal of Bodywork and Movement Therapies, 20(1), 203–207. doi: 10.1016/j.jbmt.2015.04.004
- Vigouroux, L., Goislard de Monsabert, B., & Berton, E. (2015). Estimation of hand and wrist muscle capacities in rock climbers. European Journal of Applied Physiology, 115(5), 947–957. doi: 10.1007/s00421-014-3076-6
- Watts, P. B. (2003). Anthropometry of young competitive sport rock climbers. British Journal of Sports Medicine, 37(5), 420–424. doi: 10.1136/bjsm.37.5.420
- Watts, P. B., Martin, D. T., & Durtschi, S. (1993). Anthropometric profiles of elite male and female competitive sport rock climbers. Journal of Sports Sciences, 11(2), 113–117. doi: 10.1080/02640419308729974
- Williams, S., Whatman, C., Hume, P. A., & Sheerin, K. (2012). Kinesio taping in treatment and prevention of sports injuries: A meta-analysis of the evidence for its effectiveness. Sports Medicine, 42(2), 153–164. doi: 10.2165/11594960-000000000-00000
- Yeung, S. S., Yeung, E. W., Sakunkaruna, Y., Mingsoongnern, S., Hung, W. Y., Fan, Y. L., & Iao, H. C. (2015). Acute effects of kinesio taping on knee extensor peak torque and electromyographic activity after exhaustive isometric knee extension in healthy young adults. Clinical Journal of Sport Medicine, 25(3), 284–290. doi: 10.1097/JSM.0000000000000132
- Zhang, S., Fu, W., Pan, J., Wang, L., Xia, R., & Liu, Y. (2016). Acute effects of kinesio taping on muscle strength and fatigue in the forearm of tennis players. Journal of Science and Medicine in Sport, 19(6), 459–464. doi: 10.1016/j.jsams.2015.07.012