
ABSTRACT
To date, few data on how the COVID-19 pandemic and restrictions affected children’s physical activity in Europe have been published. This study examined the prevalence and correlates of physical activity and screen time from a large sample of European children during the COVID-19 pandemic to inform strategies and provide adequate mitigation measures. An online survey was conducted using convenience sampling from 15 May to 22 June, 2020. Parents were eligible if they resided in one of the survey countries and their children aged 6–18 years. 8395 children were included (median age [IQR], 13 [10–15] years; 47% boys; 57.6% urban residents; 15.5% in self-isolation). Approximately two-thirds followed structured routines (66.4% [95%CI, 65.4–67.4]), and more than half were active during online P.E. (56.6% [95%CI, 55.5–57.6]). 19.0% (95%CI, 18.2–19.9) met the WHO Global physical activity recommendation. Total screen time in excess of 2 h/day was highly prevalent (weekdays: 69.5% [95%CI, 68.5–70.5]; weekend: 63.8% [95%CI, 62.7–64.8]). Playing outdoors more than 2 h/day, following a daily routine and being active in online P.E. increased the odds of healthy levels of physical activity and screen time, particularly in mildly affected countries. In severely affected countries, online P.E. contributed most to meet screen time recommendation, whereas outdoor play was most important for adequate physical activity. Promoting safe and responsible outdoor activities, safeguarding P.E. lessons during distance learning and setting pre-planned, consistent daily routines are important in helping children maintain healthy active lifestyle in pandemic situation. These factors should be prioritised by policymakers, schools and parents.
To our knowledge, our data provide the first multi-national estimates on physical activity and total screen time in European children roughly two months after COVID-19 was declared a global pandemic.
Only 1 in 5 children met the WHO Global physical activity recommendations.
Under pandemic conditions, parents should set pre-planned, consistent daily routines and integrate at least 2-hours outdoor activities into the daily schedule, preferable on each day. Schools should make P.E. lessons a priority. Decision makers should mandate online P.E. be delivered by schools during distance learning. Closing outdoor facilities for PA should be considered only as the last resort during lockdowns.
Highlights
Introduction
Children have been largely spared from the direct health consequences of the coronavirus disease 2019 (COVID-19) pandemic (Bialek et al., Citation2020; Götzinger et al., Citation2020). There are, however, other health effects that are equally concerning, particularly in the long-term (United Nations, Citation2020). While it is a priority to mitigate immediate impact, the pandemic’s longer-term effects can exacerbate the epidemic of childhood obesity and other chronic diseases and can increase mental health problems (Loades et al., Citation2020; Rundle, Park, Herbstman, Kinsey, & Wang, Citation2020).
Governments in Europe responded to the first wave of the COVID-19 outbreak with various measures intended to slow down the transmission of the virus. These nation-wide restrictions, particularly the closure of schools, parks, playgrounds and recreational facilities, obviously reduced the possibilities of children for maintaining an active and healthy lifestyle. Schools offer important options for physical activity through commuting to and from home, physical education (P.E.), recess, and intra- and inter-mural sports (Capel & Blair, Citation2019). These opportunities – which might be the only organised and safe options for many children – were not possible as a result of school closures. Additionally, children lost access for physical activity and sports outside of school. Finally, via these school closures, daily schedules of children were disrupted. Schedules are important for children (American Academy of Pediatrics, Citation2007). According to the structured days hypothesis children engage in a greater number of unhealthy behaviours on less-structured days (Brazendale et al., Citation2017) – the extended exposure to unstructured days during COVID-19 may also resulted in a less active lifestyle.
Current recommendations are that children and adolescents should accumulate at least 60 min of moderate- to vigorous-intensity physical activity (MVPA) and engage in no more than two hours of sedentary recreational screen time per day (Bull et al., Citation2020; Okely et al., Citation2017; Tremblay et al., Citation2016). Restrictions during COVID-19 were likely to impact on a child’s ability to meet these recommendations. Available data from other countries such as China, Canada and U.S. or from small samples demonstrated decline in physical activity and remarkable increase in screen time during the first wave of the COVID-19 pandemic (Dunton, Do, & Wang, Citation2020; Moore et al., Citation2020; Pietrobelli et al., Citation2020; Xiang, Zhang, & Kuwahara, Citation2020). However, knowledge is limited about the impact in Europe and about possible mitigations.
To understand the effects of the COVID-19 pandemic and resulting control measures on physical activity and screen time in Europe, we administered an online survey roughly 2 months after COVID-19 was declared a global pandemic by the World Health Organization (World Health Organization, Citation2020). The survey aimed to examine physical activity and screen time among European school children during this period and to understand which factors may be associated with adherence to physical activity and screen time guidelines during these special circumstances. The focus was on those factors which can be influenced by decision makers, schools and families to be able to identify possible mitigation measures for the second wave. The a priori hypotheses were that milder severity of COVID-19 in countries, lower status of restrictions, not residing in a household under self-isolation, following a structured daily schedule, spending more time playing outdoors, and participating in online physical education (P.E.) would be associated with meeting physical activity and screen time recommendations.
Materials and methods
Study design, sampling and ethical approval
This was a multi-national, cross-sectional study. Researchers from six countries with the highest COVID-19 case numbers in Europe were approached (Loades et al., Citation2020). Of these, the Russian Federation, Spain, Italy, Germany, and France agreed to participate. England refused to take part as they had their own national dataset (Sport England, Citation2020). Researchers from six less affected countries were also invited, and they were all interested to contribute (Belgium (Flemish Region), Portugal, Romania, Hungary, Poland and Slovenia). Data collection methods were standardised across all countries. Due to time constraints and feasibility considerations, it was not possible to generate a representative sample within each country. Target recruitment was a minimum of 200 children per country collected via convenience sampling. Parents of children in the defined age group who resided in the participating countries were eligible to participate. The link to the questionnaire was disseminated via 2 communication channels: first, personal and professional contacts were used to ask principals and teachers to distribute the link within their school. Second, personal contacts and social media were used to invite parents directly, via Facebook, Twitter, and WhatsApp. All recipients were encouraged to further distribute the link. The survey was active in the countries for 7–18 days between 15th May and 22nd June, 2020 (Supplementary Table 1). Parents and caregivers were informed about the survey in their national language at the landing page of the distributed link. Ethical approval for multi-centre study was obtained by the leading partner and the study protocol was approved by the Scientific and Research Ethics Committee of the Medical Research Council in Hungary (Approval Number: IV/5613-3/2020/EKU). Besides, each centre informed the related local research and ethics committee about the study and its protocol.
Survey instrument
A 7-day recall measure was used to assess the physical activity and screen time of the children. Questions regarding self-isolation and total screen time were taken from a similar online survey conducted in Canada (Moore et al., Citation2020). Question around daily scheduling was developed specifically for this study and asked “Do you follow a structured schedule on weekdays since the COVID-19 outbreak and related restrictions?” Response options were “Yes, on every day”, “Yes, mainly”, “Yes, rarely”, or “No, I do not have a schedule”. Questions assessing physical activity included a single-item physical activity question and five PAQ(C) items which were adapted to the special circumstances (i.e. distance learning) (Kowalski, Crocker, & Donen, Citation2004; Scott, Morgan, Plotnikoff, & Lubans, Citation2015). Specifically, the respondents were asked,
In the last 7 days, on how many days have you done a total of 60 minutes or more of physical activity, which was enough to raise your breathing rate? This may include sport, exercise and brisk walking or cycling for recreation or to get to and from places.
For online P.E. respondents reported whether they have participated in online lessons and if yes, how often were they very active during the online P.E. classes. The final questionnaire contained 20 items. For older children (>12 years) the questionnaire was self-administered. Parents of children aged ≤12 years were asked to help their child complete the questionnaire. The survey instrument is available as an online-only document (Text file in the Supplement).
Country contexts
A summary of regulations which were imposed at the national level in the participating countries at the time of data collection and which may be associated with participation in physical activity and screen time in children are listed in Supplementary Table 1.
At the time of the data collection, the Russian Federation was the third most affected country in the world with strict control measures and a stay-at-home order still in force in some regions. In countries that were suffering a serious but earlier outbreak such as Italy and Spain, lockdown restrictions started to ease by early May 2020. In France, the 55-day long mandatory home confinement with the closure of most public places ended on 11th May 2020 and the first phase of lockdown lifting had started. In Germany, although the number of cases were high, the mortality rate was relatively low. Restrictions started to lift in early May; outdoor sports without physical contact resumed and schools were re-opened with special rules. Portugal was in middle range in terms of case numbers and partly re-opened schools, while Poland and Romania were more conservative in this regard and kept schools closed nationwide. Hungary and Slovenia were the least affected among the participating countries in regard of the COVID-19 infection prevalence, but these countries implemented quite different approaches. In mid-May, Slovenia has already re-opened their playgrounds, parks and schools for younger children, and only the indoor facilities remained closed; meanwhile in Hungary all places including schools were closed with some re-openings occurring in the capital.
Treatment of data and analysis
Survey data were obtained from the online platforms, pooled, cleaned and imported for analysis using R language for statistical computing (R version 3.6.1; R Core Team, Vienna, Austria). Data from Belgium were not used in this analysis as the target number of 200 respondents was not achieved. Children were classified as meeting the physical activity recommendation based on the single-item 60-minute MVPA question. As no international benchmark exists for school-aged children for total screen time, authors used the ‘no more than 2 hours/day’ cut off from the American Academy of Pediatrics. (Council on Communications and Media, Citation2016) Based on the accessibility of public spaces, sports and recreational facilities, and the state of school closures, countries were categorised into three groups: (1) strict control measures (the Russian Federation), (2) lifting of the first phase of restrictions (Spain, Italy, Poland, Romania, Hungary), and (3) lifting of the second phase of restrictions (Slovenia, Germany, France, Portugal). As case number in the first group was relatively low, group 1 and 2 were merged which resulted in a more balanced distribution. Countries were also grouped according to the level of impact from COVID-19. This grouping considered the total case and total death numbers as at 31st May 2020, and the proportion of families who were under a self-isolation or quarantine order (European Centre for Disease Prevention and Control, Citation2020). The 5 most affected countries formed Group 1 (Spain, Italy, France, Russia, Portugal), while the 5 less impacted comprised Group 2 (Germany, Romania, Poland, Slovenia, Hungary).
Data were presented as frequencies (%) with 95% confidence intervals (CI, using Clopper–Pearson formula) or medians with corresponding 95% CI (using exact formula based on sign test) for categorical and continuous (ordinal) data, respectively. The difference between screen time on weekdays and weekends was tested with Wilcoxon signed-rank test with continuity correction, separately for each country. A nonparametric CI and an estimate for the pseudo-median for the difference of the location parameters was computed. The association between the outcome (meeting the recommendations for physical activity and screen time) and the predetermined independent variables (age, gender, urban–rural status, schedule, online P.E., quarantine or self-isolation, status of restrictions, level of COVID-19 severity, and outdoor play time on weekdays) was estimated with multivariate binary logistic regression with country ID as a random effect (including random slopes for residence, play, and schedule as suggested by the Wolf test). The analysis was also stratified by age (6–11 years and 12–18 years) and level of COVID severity. Results are presented as ORs with corresponding 95% CIs.
Results
Of the 8997 respondents who completed the survey, 602 were excluded leaving a final analytic sample of 8395 children (). Due to the convenience sampling design, information on the response rate and non-responders characteristics were unavailable. reports the characteristics of the sample. Girls were slightly overrepresented (53.1%), as were participants living in urban areas (57.6%) and those from Hungary (31.3%). In total, 15.5% of children and adolescents reported to be in self-isolation or quarantine ().
Figure 1. Flow diagram of participants throughout the study. Abbreviations: PA = physical activity; ST = screen time. Mildly affected countries: Germany, Romania, Poland, Slovenia, Hungary. Severely affected countries: Spain, Italy, France, Russia, Portugal.
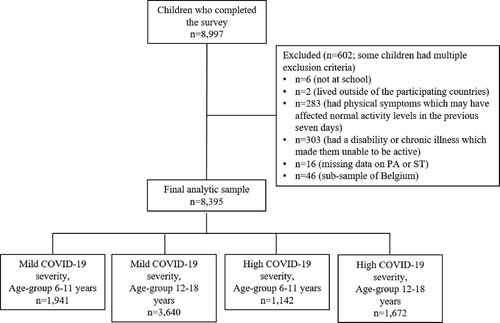
Table 1. Characteristics of survey respondents by country (6–18 years; n = 8395).
Approximately two-thirds of children followed a structured schedule (66.4% [95%CI, 65.4–67.4]) and more than half were active sometimes, often or always during online P.E. lessons (56.6% [95%CI, 55.5–57.6]). Country-based descriptive statistics for physical activity and screen time are shown in . In most countries, less than 20% of children and adolescents met the physical activity recommendation. Slovenia and Romania had the highest proportion of sufficiently active children; and children in these countries spent the most time playing outdoor on weekdays and weekend days (). Slovenia also had the highest proportion of children who met the screen time recommendation. Around 70% of participants exceeded the recommended 2 h/day of total screen time on weekdays in the whole sample, and just under two-thirds of participants exceeded the screen time recommendation on weekends.
Table 2. Key study variables by country in school-aged children and adolescents (6–18 years; n = 8395).
Factors associated with meeting the physical activity recommendation
The status of restrictions, the extent to which a country was affected by the COVID-19 pandemic and being in quarantine or self-isolation were not associated with the odds for meeting the physical activity recommendation (). Compared with children and adolescents who did not follow a structured daily routine, those who did were more likely to meet the physical activity recommendation (OR = 1.62 [95%CI, 1.24–2.13]). In the sub-analyses this was observed in the mildly affected countries but not in severely affected ones. Children and adolescents who played outdoors for more than 2 h per day were more likely to meet the physical activity recommendation (OR = 2.56 [95%CI, 1.98–3.32]). In strongly affected countries this was more apparent for adolescents than for children. Being active during online P.E. was also associated with healthy level of physical activity (OR = 1.27 [95%CI, 1.12–1.44]) with this being observed in the strongly affected countries for adolescents but not for children.
Table 3. Multivariate logistic regression for meeting the physical activity and screen time recommendation.
Factors associated with meeting screen time recommendation
Children from mildly affected countries were more likely to meet the screen time recommendation as those who lived in severely impacted countries, particularly on weekdays when the difference in odds were more than threefold (OR = 3.25 [95%CI, 2.38–4.45]) (). Residing in a country with lower level of restrictions also increased the odds for healthy screen time habits (weekdays OR = 1.42 [95%CI, 1.07–1.90] and weekend OR = 1.74 [95%CI, 1.28–2.37], respectively), with this being more apparent among children than adolescents. Being in quarantine or self-isolation or time spent playing outside were not associated with meeting the screen time recommendation. Following a daily schedule increased the odds for meeting the screen time recommendation, but more so in countries mildly affected than in those strongly affected. Those who were active in online P.E. classes were more likely to meet the screen time recommendation than their respective reference group (weekdays OR = 1.20 [95%CI, 1.08–1.38] and weekend OR = 1.21 [95%CI, 1.09–1.34], respectively). On weekdays, this association was more apparent for children compared to adolescents. On weekends this association was not observed for children from strongly affected countries.
Discussion
To our knowledge, this is the first multi-national study to provide data on physical activity and total screen time in children in relation to the COVID-19 pandemic. Our data showed that, two months after the WHO declared COVID-19 as a global pandemic, 81% (95% CI, 80.1–81.8) of European students aged 6–18 years did not meet physical activity guidelines. We found commonly observed sex- and age-related differences (McCormack & Meendering, Citation2016 Troiano et al., Citation2008). There was no clear pattern according to being in self-isolation or quarantine order. In addition, neither the severity of the COVID-19 pandemic nor the status of restrictions within a country influenced the odds to be sufficiently active.
Until the present analysis, no large set of multi-national data existed on the impact of COVID-19 pandemic on physical activity and screen time in children. Hall, Laddu, Phillips, Lavie, & Arena (Citation2020) theoretically discussed the question of “Is COVID-19 making the world move even less active than before?”. As insufficient physical activity is already a global issue these authors highlighted that further decrease would be very concerning. Unfortunately, given the cross-sectional nature of our survey and the limited validity of self-reported data, we are not in a position to directly answer this question. Our data suggest, however, that as a whole the quantity and frequency of physical activity among European adolescents remained roughly at the same low level in May 2020 than before the pandemic (Guthold, Stevens, Riley, & Bull, Citation2020). In contrast, surveys conducted in March and April 2020 in China and Canada found considerable decrease in physical activity (Moore et al., Citation2020; Xiang et al., Citation2020). This can be either due to the earlier collection of their data or to the regional differences in impact. In line with this latter idea, we found remarkable inter-country differences in Europe, and countries such as Spain, Poland, Germany, and Portugal where, among boys only, the prevalence of insufficient activity increased compared to the pre-COVID-19 level estimated by the HBSC data (Supplementary Figure 1) (Inchley et al., Citation2020).
In 8 of the 10 countries, at least two thirds of participants exceeded 2 h per day of total screen time on weekdays, demonstrating widespread usage of screen-based media during this period of restrictions and distance learning. The association with being in quarantine was not significant, but both high levels of restrictions and high COVID-19 severity decreased the likelihood of meeting the screen time recommendation. Although assessment methods in previous studies varied widely, our results seem to exceed the pre-pandemic values (Verloigne et al., Citation2016). This finding is similar to what was shown in the Canadian and Chinese surveys, which both reported much higher screen time than before the pandemic (Moore et al., Citation2020; Xiang et al., Citation2020). Similar to insufficient PA, increased screen time has been shown to be an independent predictor of adverse health outcomes, (Tremblay et al., Citation2011) meaning that future interventions need to be designed to mitigate this effect and to avoid this higher level of screen time becoming the new normal.
What are the responses that can support maintaining a healthy and active lifestyle among school-aged children during the second wave of the pandemic, which is currently being experienced globally? The prevalence of being characterised as sufficiently active was larger among children who reported playing outside for more than 2 h/day. This finding aligns with recently published research from Canada and reinforces the evidence that time spent outdoors is associated with physical activity (Guerrero et al., Citation2020). Children are more active outside than inside, and our data suggest that, despite the limited outdoor opportunities, this trend persisted during the outbreak. Thus, policy, parents and caregivers should be informed about the benefits of outdoor play and should be encouraged to facilitate and integrate at least 2-h of outdoor time into the daily routines in a safe and responsible manner. Given the importance of outdoor play, closing outdoor facilities for physical activity should be considered only as the last resort during lockdowns.
Of interest was the higher odds of meeting the physical activity and screen time recommendations among children who followed a structured daily schedule. This is consistent with evidence showing that, among some groups such as adolescent girls, poor time management skills was associated with lower physical activity participation (Biddle, Whitehead, O’Donovan, & Nevill, Citation2005). Others have found that in the periods with less structured time, such as summer holidays or weekends, children and adolescends tend to be less active, more sedentary and have longer periods of screen time. (Fairclough, Boddy, Mackintosh, Valencia-Peris, & Ramirez-Rico, Citation2015; Weaver et al., Citation2020;) This suggests that setting daily routines by following the usual school schedule and organising the remaining daily time during home schooling might be another promising intervention strategy to increase physical activity and limit sedentary screen time for the benefits of metabolic health in children and adolescents. Thus, pre-planned, segmented structures on a consistent manner and parent rules related to screens should be promoted in these situations to regulate unhealthy behaviours.
Being actively engaged in online P.E. was found to be an other important predictor of meeting the recommendations. This supports the literature showing a positive association between school P.E. programmes and overall physical activity (Kokkonen, Yli-Piipari, Kokkonen, & Quay, Citation2019 Meyer et al., Citation2013). Consequently, education policies should aim to mandate online P.E. be delivered by schools if remote learning is taking place. As schools build their remote teaching capacity, P.E. should be made a priority. Where schools are sending home lesson plans for math and grammar, they should also send home lesson plans for P.E. For schools or teachers who have the capacity, P.E. classes should be streamed online. The number of P.E. lessons should be at least the same as under non-pandemic conditions.
There were a number of limitations present in this study that should be considered when interpreting the findings. First, self- and parent-reported instruments were used to assess time spent in physical activity. Self-reported data are heavily prone to recall bias and social desirability (Ekelund, Tomkinson, & Armstrong, Citation2011). Also, there were factors, like active breaks, which was difficult for the respondents to accurately interpret and report in relation to home schooling. Moreover, the cross-sectional and non-representative nature of the data limits the possibility of comparing our data to pre-COVID values (e.g. to the HBSC study results). The methodological standardisation across survey centres, in which the same instruments were used in different cultural and language contexts, can also carry costs in terms of precision. This, together with the convenience sampling, may explain some of the between-country differences and the differences to pre-COVID data taken from the HBSC survey. Furthermore, the question on meeting the 1-hours of MVPA daily, taken from the HBSC study, presents a challenge of its own due to individual differences of experiencing fatigue between fit and unfit children. Another weakness is the lack of details about the intensity of physical activity. We assume, that many of the high intensity activities (e.g. P.E. classes, sports club trainings) have been replaced by light or moderate intensity activities such as walking or jogging during the lockdowns. On this way, although the amount of physical activity remained the same, the intensity dropped which may led to an impaired cardiovascular fitness. This deconditioning effect of the COVID-19 pandemic was detected in Autumn, 2020 in some countries in Europe (i.e. in Slovenia via their SLOfit monitoring system and in the UK – unpublished data), and also in a recently published small-scale study (Dayton et al., Citation2021). More work using more accurate methods such as accelerometer or heart rate monitor would be needed to capture the decrease in the intensity of physical activity in pandemic situation and to prove this theory. Also, the question about being in self-isolation or quarantine asked about the last seven days, however this period could have started later and lasted shorter and on this way it may happen that this variable might not fully capture the degree of reduced physical mobility. This would explain why we have not found any significant effect in this regard except for adolescents in mildly affected countries. Finally, in the absence of global guidelines for sedentary screen time for school-aged children and adolescents, we used the Australian and Canadian guidelines which recommend limiting sedentary recreational screen time to no more than 2 h per day. However, the question we used in this study did not ask respondents to report recreational screen time. As such, it is likely that our values include time spent using screens for educational purposes and for attending online P.E. as well, which are outside the scope of these guidelines.
The current findings complement the growing evidence on the prevalence of insufficient physical activity and unhealthy screen time in children in reaction to the COVID-19 pandemic. We strongly advise parents, schools, and authorities to set up aggressive countermeasures, that incorporate the promotion of structured schedules, the safeguarding of P.E. lessons during distance learning, and the promotion of time spent outdoors. All these were found to make important contributions to increased physical activity and reduced screen time among European children and adolescents during the COVID-19 pandemic period.
Declaration of interest statement
The authors declare that they have no competing interests.
Acknowledgements
We thank the children and parents who generously volunteered and participated in this survey. We are also grateful for the participating institutes for supporting the field work in the countries. In particular, we thank the Belgium partners around Herman Van Driessche, for their efforts in distributing the questionnaire, and we regret that we had to exclude the Belgium data from the final analysis. We gratefully acknowledge the technical help of Dr. Joao Breda and Stephen Whiting from the WHO European Office for Prevention and Control of Noncommunicable Diseases in setting up the survey team. The study was co-funded by the Slovenian Research Agency within the research program Bio-psycho-social context of kinesiology (P5-0142).
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- American Academy of Pediatrics. (2007). The Importance of Family Routines. 2007. Available at: https://www.healthychildren.org/English/family-life/family-dynamics/Pages/The-Importance-of-Family-Routines.aspx [accessed 30.05.2020].
- Bialek, S., Gierke, R., Hughes, M., McNamara, L. A., Pilishvili, T., & Skoff, T. (2020). Coronavirus Disease 2019 in children - United States, February 12-April 2, 2020. MMWR. Morbidity and Mortality Weekly Report, 69(14), 422–426. doi:10.15585/mmwr.mm6914e4
- Biddle, S. J., Whitehead, S. H., O’Donovan, T. M., & Nevill, M. E. (2005). Correlates of participation in physical activity for adolescent girls: A systematic review of recent literature. Journal of Physical Activity and Health, 2(4), 423–434. doi:10.1123/jpah.2.4.423
- Brazendale, K., Beets, M. W., Weaver, R. G., Pate, R. R., Turner-McGrievy, G. M., Kaczynski, A. T., … von Hippel, P. T. (2017). Understanding differences between summer vs. School obesogenic behaviors of children: The structured days hypothesis. International Journal of Behavioral Nutrition and Physical Activity, 14(1), 100. doi:10.1186/s12966-017-0555-2
- Bull, F. C., Al-Ansari, S. S., Biddle, S., Borodulin, K., Buman, M. P., Cardon, G., … Dempsey, P. C. (2020). World Health Organization 2020 guidelines on physical activity and sedentary behaviour. British Journal of Sports Medicine, 54, 1451–62. doi:10.1136/bjsports-2020-102955
- Capel, S., & Blair, R. (2019). Debates in physical education. London: Routledge.
- Council on Communications and Media. (2016). Media use in school-aged children and adolescents. Pediatrics, 138(5), e20162592. doi:10.1542/peds.2016-2592
- Dayton, J. D., Ford, K., Carroll, S. J., Flynn, P. A., Kourtidou, S., & Holzer, R. J. (2021 Jan 4). The deconditioning effect of the COVID-19 pandemic on unaffected healthy children. Pediatric Cardiology, 1–6. doi:10.1007/s00246-020-02513-w
- Dunton, G. F., Do, B., & Wang, S. D. (2020 Sep 4). Early effects of the COVID-19 pandemic on physical activity and sedentary behavior in children living in the U.S. BMC Public Health, 20(1), 1351. DOI: 10.1186/s12889-020-09429-3. PMID: 32887592; PMCID: PMC7472405.
- Ekelund, U., Tomkinson, G. R., & Armstrong, N. (2011). What proportion of youth are physically active? Measurement issues, levels and recent time trends. British Journal of Sports Medicine, 45(11), 859–865. doi:10.1136/bjsports-2011-090190
- European Centre for Disease Prevention and Control. (2020). COVID-19 Coronavirus data. Available at: https://data.europa.eu/euodp/en/data/dataset/covid-19-coronavirus-data [accessed 04.05.2020].
- Fairclough, S. J., Boddy, L. M., Mackintosh, K. A., Valencia-Peris, A., & Ramirez-Rico, E. (2015). Weekday and weekend sedentary time and physical activity in differentially active children. Journal of Science and Medicine in Sport, 18(4), 444–449. doi:10.1016/j.jsams.2014.06.005
- Götzinger, F., Santiago-García, B., Noguera-Julián, A., Lanaspa, M., Lancella, L., Carducci, F. I. C., … Krivec, U. (25 June 2020). COVID-19 in children and adolescents in Europe: A multinational, multicentre cohort study. The Lancet Child & Adolescent Health, 4(9), 653–661. doi:10.1016/S2352-4642(20)30177-2
- Guerrero, M. D., Vanderloo, L. M., Rhodes, R. E., Faulkner, G., Moore, S. A., & Tremblay, M. S. (2020). Canadian children's and youth's adherence to the 24-h movement guidelines during the COVID-19 pandemic: A decision tree analysis. Journal of Sport and Health Science, 9(4), 313–321. doi:10.1016/j.jshs.2020.06.005
- Guthold, R., Stevens, G. A., Riley, L. M., & Bull, F. C. (2020). Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1·6 million participants. The Lancet Child & Adolescent Health, 4(1), 23–35. doi:10.1016/S2352-4642(19)30323-2
- Hall, G., Laddu, D. R., Phillips, S. A., Lavie, C. J., & Arena, R. (2020). A tale of two pandemics: How will COVID-19 and global trends in physical inactivity and sedentary behavior affect one another? Progress in Cardiovascular Diseases, S0033-0620(20), 30077–3.
- Inchley, J., Currie, D., Budisavljevic, S., Torsheim, T., Jåstad, A., Cosma, A., … Samdal, O. (2020). Spotlight on adolescent health and well-being: Findings from the 2017/2018 health behaviour in school-aged children (HBSC) survey in Europe and Canada, International report. Volume 2. Key data. Copenhagen: WHO Regional Office for Europe.
- Kokkonen, J., Yli-Piipari, S., Kokkonen, M., & Quay, J. (2019). Effectiveness of a creative physical education intervention on elementary school students’ leisure-time physical activity motivation and overall physical activity in Finland. European Physical Education Review, 25(3), 796–815. doi:10.1177/1356336X18775009
- Kowalski, K. C., Crocker, P. R., & Donen, R. M. (2004). The physical activity questionnaire for older children (PAQ-C) and adolescents (PAQ-A) manual. Saskatoon: College of Kinesiology, University of Saskatchewan.
- Loades, M. E., Chatburn, E., Higson-Sweeney, N., Reynolds, S., Shafran, R., Brigden, A., … Crawley, E. (2020 Jun 3). Rapid systematic review: The impact of social isolation and loneliness on the mental health of children and adolescents in the context of COVID-19. Journal of the American Academy of Child & Adolescent Psychiatry, S0890-8567(20), 30337–3.
- McCormack, L. A., & Meendering, J. (2016). Diet and physical activity in rural vs urban children and adolescents in the United States: A narrative review. Journal of the Academy of Nutrition and Dietetics, 116(3), 467–480. doi:10.1016/j.jand.2015.10.024
- Meyer, U., Roth, R., Zahner, L., Gerber, M., Puder, J. J., Hebestreit, H., & Kriemler, S. (2013). Contribution of physical education to overall physical activity. Scandinavian Journal of Medicine & Science in Sports, 23(5), 600–606.
- Moore, S. A., Faulkner, G., Rhodes, R. E., Brussoni, M., Chulak-Bozzer, T., Ferguson, L. J., … Tremblay, M. S. (2020). Impact of the COVID-19 virus outbreak on movement and play behaviours of Canadian children and youth: A national survey. International Journal of Behavioral Nutrition and Physical Activity, 17(1), 85. doi:10.1186/s12966-020-00987-8
- Okely, A. D., Ghersi, D., Hesketh, K. D., Santos, R., Loughran, S. P., Cliff, D. P., … Sherring, J. (2017). A collaborative approach to adopting/adapting guidelines – The Australian 24-hour movement guidelines for the early years (birth to 5 years): an integration of physical activity, sedentary behavior, and sleep. BMC Public Health, 17(5), 869. doi:10.1186/s12889-017-4867-6
- Pietrobelli, A., Pecoraro, L., Ferruzzi, A., Heo, M., Faith, M., Zoller, T., … Heymsfield, S. B. (2020). Effects of COVID-19 lockdown on lifestyle behaviors in children with obesity living in Verona, Italy: A longitudinal study. Obesity, 28(8), 1382–1385. doi:10.1002/oby.22861
- Rundle, A. G., Park, Y., Herbstman, J. B., Kinsey, E. W., & Wang, Y. C. (2020 Jun). COVID-19-Related school closings and risk of weight gain among children. Obesity (Silver Spring), 28(6), 1008–1009. doi:10.1002/oby.22813. Epub 2020 Apr 18. PMID: 32227671; PMCID: PMC7440663.
- Scott, J. J., Morgan, P. J., Plotnikoff, R. C., & Lubans, D. R. (2015). Reliability and validity of a single-item physical activity measure for adolescents. Journal of Paediatrics and Child Health, 51(8), 787–793. doi:10.1111/jpc.12836
- Sport England. (2020). Children’s experience of physical activity in lockdown. Insight July 2020. 2020. Available at: https://www.activecumbria.org/files/6715/9489/1306/Childrens_experience_of_physical_activity.pdf [accessed 07.06.2020].
- Tremblay, M. S., Carson, V., Chaput, J. P., Connor Gorber, S., Dinh, T., Duggan, M., … Janssen, I. (2016). Canadian 24-hour movement guidelines for children and youth: An integration of physical activity, sedentary behaviour, and sleep. Applied Physiology, Nutrition, and Metabolism, 41(6), S311–SS27. doi:10.1139/apnm-2016-0151
- Tremblay, M. S., LeBlanc, A. G., Kho, M. E., Saunders, T. J., Larouche, R., Colley, R. C., … Gorber, S. C. (2011). Systematic review of sedentary behaviour and health indicators in school-aged children and youth. International Journal of Behavioral Nutrition and Physical Activity, 8(1), 98. doi:10.1186/1479-5868-8-98
- Troiano, R. P., Berrigan, D., Dodd, K. W., Masse, L. C., Tilert, T., & McDowell, M. (2008). Physical activity in the United States measured by accelerometer. Medicine & Science in Sports & Exercise, 40(1), 181–188.
- United Nations. (2020) Policy Brief: The Impact of COVID-19 on children. April 15, 2020. Available at: https://unsdg.un.org/sites/default/files/2020-04/160420_Covid_Children_Policy_Brief.pdf [accessed 29.05.2020].
- Verloigne, M., Loyen, A., Van Hecke, L., Lakerveld, J., Hendriksen, I., De Bourdheaudhuij, I., … van der Ploeg, H. P. (2016). Variation in population levels of sedentary time in European children and adolescents according to cross-European studies: A systematic literature review within DEDIPAC. International Journal of Behavioral Nutrition and Physical Activity, 13(1), 69. doi:10.1186/s12966-016-0395-5
- Weaver, R. G., Armstrong, B., Hunt, E., Beets, M. W., Brazendale, K., Dugger, R., … Youngstedt, S. D. (2020). The impact of summer vacation on children's obesogenic behaviors and body mass index: A natural experiment. International Journal of Behavioral Nutrition and Physical Activity, 17(1), 153. doi:10.1186/s12966-020-01052-0
- World Health Organization. (2020) WHO announces COVID-19 outbreak a pandemic. 2020. Available at: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/news/news/2020/3/who-announces-covid-19-outbreak-a-pandemic [accessed 03.05.2020).
- Xiang, M., Zhang, Z., & Kuwahara, K. (2020). Impact of COVID-19 pandemic on children and adolescents’ lifestyle behavior larger than expected. Progress in Cardiovascular Diseases, 63(20), 531–537.