
ABSTRACT
Patellar tendon (PT) complaints are frequent throughout the population, with increased occurrence in athletes and, particularly, in youth competitive alpine skiers. Timely detection and treatment might improve prospects of recovery. Diagnostic modalities in clinical use to date rely on pain symptoms, manual palpation, and potentially, magnetic resonance imaging (MRI); however, MRI-based imaging yields limited sensitivity. Quantitatively measuring the morphological and mechanical properties of PTs by means of B-mode ultrasound and shear wave elastography (SWE), instead, may allow improved diagnosis or even early detection. We performed B-mode scans and three-dimensional ultrasound shear wave velocity (SWV) mapping and MRI of the PT in 106 youth skiers. A prospective one-year survey on health problems combined with clinical assessments served to categorize symptomatic and asymptomatic youth skiers. Skiers suffering from distal or proximal tendon complaints showed lower SWV in the respective tendon region than asymptomatic skiers (p = 0.035 and p = 0.019, respectively). Youth skiers with distal tendon complaints additionally exhibited decreased SWV in the proximal region compared to asymptomatic counterparts (p = 0.020). Cross-validated analysis of retrospective prediction indicated sensitivity and specificity in detecting tendon complaints in the range of 0.606–0.621 and 0.536–0.650, respectively. MRI detected distal tendon complaints with a sensitivity of 0.410 (12/29) but failed to detect any proximal cases. This study agrees with the most recent literature in that SWE holds promise as a valuable adjunct modality for the diagnosis of PT complaints or even the detection of subclinical prestages. However, to evaluate its prospective predictive value, long-term studies are warranted.
Highlights
Patellar tendon complaints are a frequent complaint in athletes, particularly in youth competitive alpine skiers, but timely quantitative detection of related tendon properties remains challenging.
Quantitative B-mode US and three-dimensional ultrasound shear wave elastography assessments and magnetic resonance imaging were performed in youth competitive alpine skiers.
Three-dimensional shear wave elastography was able to discern symptomatic from asymptomatic patellar tendons both in the distal and proximal tendon regions, whereas magnetic resonance imaging failed to detect any proximal cases.
Introduction
Overuse injuries are common among athletes in various sports, (Franco et al., Citation2021) but also in competitive alpine skiing (Fröhlich et al., Citation2020a; Fröhlich et al., Citation2021). In this sport, the knee and especially the patellar tendon are exposed to high forces and adverse loading patterns. In skiing, athletes make tens of thousands of turns per season, with ground reaction forces several times their body weight (Gilgien, Reid, Raschner, Supej, & Holmberg, Citation2018; Spörri, Müller, & Kröll, Citation2022). These loading patterns, in combination with positions with strongly flexed and forward pushed knees, induce already during “normal” (i.e. controlled) skiing significant activation of the knee extensors (Spörri et al., Citation2022) and, thus, on the PT. Moreover, the off-snow physical fitness training of skiers typically includes large amounts of plyometric jump and heavy weight strength training, further exerting large loads on the PT. It is therefore not surprising that already youth competitive alpine skiers suffer from a remarkably high rate of complaints at the proximal and distal PT (Fröhlich et al., Citation2020b).
Traditionally, PT complaints are clinically diagnosed through pain reported by the patient and manual palpation of the PT and adjacent tissues. Such a primarily symptom-related diagnostic approach is, however, problematic regarding its reproducibility and may yield limited value in assessing the efficacy of treatments (Docking, Ooi, & Connell, Citation2015; Fredberg & Stengaard-Pedersen, Citation2008). Therefore, various imaging modalities are currently employed as an adjunct to clinical examination, assisting in the diagnosis and possibly screening of those at risk. In this context, ultrasound (US) brightness-mode (B-mode) imaging is typically used to qualitatively visualize radiological signs accompanying clinical complaints such as thickening of the tendon, fibre orientation disruption, intratendinous calcifications, localized hypoechoic regions, bursitis and increased vascularity (Fredberg & Stengaard-Pedersen, Citation2008; Obst et al., Citation2018). However, the correlation between such radiological signs and the occurrence of symptoms is limited (Cook, Khan, Kiss, Coleman, & Griffiths, Citation2001; Coombes et al., Citation2018). For example, it has been demonstrated that tendons with visible morphological alterations may be asymptomatic, while symptomatic tendons may possibly not show any visible structural changes on US B-mode (McAuliffe, McCreesh, Culloty, Purtill, & O’Sullivan, Citation2016). Similarly, magnetic resonance imaging (MRI) can visualize tendon thickening and an increase in intratendinous signal as a result of the higher water content following alterations in fibrillar alignment and proteoglycan accumulation, (Docking et al., Citation2015) but its value in tendinopathy detection remains debated, primarily due to its limited sensitivity and high cost (Khan et al., Citation2003; Tsehaie, Poot, Oei, Verhaar, & de Vos, Citation2017; Warden et al., Citation2007). Better diagnostic performance can be observed for PT complaints that primarily affect the bony attachment (Osgood-Schlatter disease or Sinding-Larsen Johansson syndrome) are prevalent (Fischer, Citation2021; Ladenhauf, Seitlinger, & Green, Citation2020).
In recent years, US shear wave elastography (SWE) has gained attention in the field of musculoskeletal soft tissue imaging. In contrast to traditional qualitative radiological diagnostic approaches, this relatively new method allows a quantitative assessment of local tissue mechanical properties by emitting a focused acoustic radiation pulse and observing the propagation of the resulting shear motion through the region of interest. The instantaneous velocity of this shear wave is related to the tissue’s material properties, with stiffer material leading to higher shear wave velocity (SWV). Although the histological features of tendinopathic tissue with collagen disarray and disruption and a lower content of type I collagen would conceivably decrease tendon stiffness, previous studies remain inconclusive (Coombes et al., Citation2018; Dirrichs et al., Citation2016; Obst et al., Citation2018; Zhang, Ng, Lee, & Fu, Citation2014). As pointed out by other authors, a major shortcoming of previous investigations is the fact that SWE examination was limited to discrete locations, which may not be representative of the entire structure, thus increasing measurement uncertainty (Docking et al., Citation2015; Obst et al., Citation2018). To overcome these limitations, we recently devised a procedure that enables three-dimensional (3D) mapping of unidirectional SWV based on optical tracking of the US transducer during free-hand scanning, which we have already validated in a previous study (Götschi et al., Citation2021). The advantages of this method are that it not only provides robust regional SWV statistics, but also the underlying standard US B-mode data can be used to extract quantitative tendon morphological properties such as tendon length or cross-sectional area (CSA).
Therefore, the aim of the current study was (1) to examine the quantitative PT properties (morphological and mechanical) shear of the PT using quantitative B-mode US and 3D mapping of SWV in a large athletic cohort of youth competitive alpine skiers as a function of demographic factors, (2) to identify distinct regional PT properties of skiers with distal and/or proximal PT complaints vs. skiers with healthy PTs, and (3) to compare the sensitivity and specificity of this novel US SWE approach with the diagnostic accuracy of MRI as the gold standard approach to detect PT complaints.
Materials and methods
Study design and study population
This prospective case–control study included 3D US SWV mapping (including quantitative B-mode US), MRI assessments and a 12-month prospective health observation regarding PT complaints in 106 youth competitive alpine skiers (40 female, 66 male) aged 13–15 years. A consensus statement recommends the use of the term “tendinopathy” to describe persistent proximal patellar tendon pain related to mechanical loading, regardless of any structural changes/imaging abnormalities that may be present in the tendon (Scott et al., Citation2020). PT tendon complaints in athletes may, however, also relate to anatomical regions other than the proximal PT (Cassel et al., Citation2015). While complaints related to the proximal PT can include, for instance, cases of Sinding-Larsen-Johansson syndrome in youth athletes or Jumper's knee in general, complaints in the distal portion of the PT around the growth spurt are typically cases of Osgood-Schlatter disease (Sørensen et al., Citation2021). Accordingly, in this manuscript, we refer to “PT complaints”, defined by symptoms during motion- and palpation-induced pressure pain in either the proximal, mid or distal portions of the PT, as this term may better reflect the different types and locations of clinical conditions that athletes may suffer from. Previous work has suggested the presence of bilateral tendon deficits in patients with unilateral pathologies (Docking & Cook, Citation2016; Obst et al., Citation2018). Accordingly, asymptomatic patellar tendons of subjects with unilateral PT were thus excluded from this study and compared to the tendons of asymptomatic subjects only. Further exclusion criteria were the diagnosis of a knee sprain at the time of US SWE and MRI examination and systemic pathologies such as inflammatory arthritis or diabetes mellitus; however, none of the skiers willing to participate fulfilled these criteria. Participation in the study was voluntary, and skiers were included in the study if they were members of a certified regional performance centre of Swiss Ski, i.e. if they embodied the best skiers in the corresponding age group in Switzerland. Whereas the exact training load was not assessed in the current study, in winter, i.e. during the competition season, youth competitive alpine skiers typically perform 3.5 on-snow and 4.5 off-snow training units per week (Schoeb et al., Citation2020). In summer, i.e. during the preseason period, they train on average one time on snow and 6.5 times off snow per week (Schoeb et al., Citation2020). This study was approved by the local ethics committee (KEK-ZH-NR: 2017-01395). All participants were informed in writing about the measurement procedures and provided written consent.
Shear wave elastography and quantitative B-mode US assessments
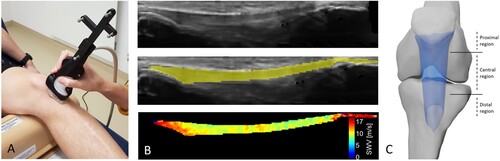
SWE measurements were conducted in accordance with our validation study (Götschi et al., Citation2021). Briefly, the subject was in the supine position with adjustable support underneath the knee with a knee flexion angle of approximately 20 degrees. The subject was positioned five minutes before the assessment and was instructed to remain relaxed throughout the procedure to avert measurement bias due to tendon loading (Payne, Watt, & Webborn, Citation2018). Measurements of shear wave group velocity were acquired as provided by the US device (Aixplorer Ultimate, SuperSonic Imagine, Aix-en-Provence, France) using a linear 5 cm transducer (SuperLinear SL18-5, SuperSonic Imagine, Aix-en-Provence, France). The transducer position was tracked synchronously to image acquisition with an optical tracking system (FusionTrack 500, Atracsys LLC, 7 Hz sampling frequency, tracking accuracy 0.09 mm (RMS)) (A). The US transducer was oriented parallel to the fibre axis of the tendon by observing and maximizing the fibrillar appearance of the intratendinous structure in relation to transducer rotation. Volumetric sampling of the volume of interest was achieved by manually moving the US transducer orthogonal to the imaging plane in a continuous motion (< 5 mm/s). Two-dimensional B-mode and SWE measurements were projected into 3D space and sampled onto an isometric regular grid (0.5 mm resolution). The patellar tendon was then segmented manually on the B-mode reconstruction, and the resulting volumetric mask was subdivided into distal, central and proximal tendon regions with two cuts positioned 10 mm proximal to the tibial insertion and 10 mm distal to the patellar origin (B, C). These masks provided information on tendon morphology, including tendon volume and length, as defined by the distance between the two anatomical landmarks described above, which were used to derive the average cross-sectional area of the central region of the tendon. SWV characteristics were summarized with regional averages and associated standard deviations within each region.
Figure 1. Three-dimensional mapping of tendon shear wave velocity. A: The ultrasound transducer position was recorded using optical markers during B-mode and elastography data acquisition. B: Three-dimensional B-mode imagery (top row) is used for manual segmentation of the patellar tendon (middle row) and subsequent masking of the elastography measurements (bottom row). C: Volumetric shear wave velocity data of the patellar tendon are partitioned into 3 regions based on anatomical landmarks.
Magnetic resonance imaging and assessment of clinical complaints
All skiers underwent MR imaging (3 Tesla, MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany) with a dedicated knee coil, which was assessed by an experienced radiologist for the presence of a wide range of knee pathologies within the scope of a different study (Fröhlich et al., Citation2020b). An isotropic (0.63 mm resolution) fat-suppressed T2-weighted 3D sequence (SPACE) with an echo time (TE) of 108 ms, repetition time (TR) of 1000 ms, receiver bandwidth of 415 Hz/Px, and parallel imaging acceleration factor of 4 was used. Positive findings pertaining to degenerative tendon disorders were adopted for the current study. These potential findings included the presence of structural changes, thickening or areas with increased signal intensity in the patellar tendon. The tendon insertions were additionally examined for the presence of ossicles, fragmentation of the apophysis and tissue irritation, as they are typically present in symptomatic youth athletes with conditions such as Osgood Schlatter disease (Demirag, Ozturk, Yazici, & Sarisozen, Citation2004; Sørensen et al., Citation2021). Their respective localization led to the MRI-based positive finding of distal, mid-portion and proximal pathological changes.
Prior to the US SWE and MRI assessments, a prospective year-long health observation using the Oslo Sports Trauma Research Centre (OSTRC) questionnaire on health problems was conducted at two-week intervals. The self-reported OSTRC data were supplemented and verified by a clinical examination and a retrospective interview performed by an experienced physician prior to the imaging examinations. The clinical examination entailed inspection, palpation, evaluation of range of motion and stability in the sagittal and frontal plane (Fröhlich et al., Citation2020b). These data were then used by the same physician to classify the study-relevant conditions into distal, mid-portion and proximal patellar tendon complaints and to categorize symptomatic and asymptomatic skiers. Specifically, the athlete’s report of recurring pain during physical activity and pain on palpation of the respective anatomical location led to a positive clinical finding of PT complaints.
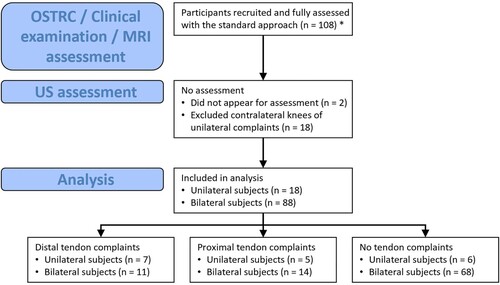
Regarding the MRI examination and the OSTRC survey, the results of an overlapping intersecting part of the underlying dataset had already been published in a previous study (Fröhlich et al., Citation2020b). However, in the present study, these data were reanalysed for the purpose of allowing a direct comparison between the novel SWE approach and standard methods of assessing PT complaints ().
Figure 2. Study flow diagram of the study-related assessments and subject categorization. Note: Eight knees were diagnosed with both distal and proximal patellar tendon complaints. n: Number of subjects. * Dataset published in Fröhlich et al. (Citation2021) (Fröhlich et al., Citation2020b)
Statistical analysis
Tendon morphology and SWV characteristics (overall, distal, central and proximal) were described and presented as the mean ± standard deviation for the entire sample, as well as for corresponding sex (female vs. male) and age groups (under 15 years – U15 and under 16 years – U16). The effects of demographical parameters on tendon characteristics were assessed using multivariate (main effects only) mixed-effects linear models with a restricted maximum likelihood (REML) procedure based on variance components structure to account for the potential intraindividual side-to-side correlation. Symptomatic groups were compared with the tendons of asymptomatic skiers with an analogous model. Parameters yielding significant group effects were further assessed for their performance in predicting tendon symptoms with a leave-one-out cross-validated receiver-operator characteristics (ROC)-based optimal cut-off approach. In an iterative process, one case is held out, and based on the remaining cases, the categorization cut-off maximizing discrimination accuracy (Youden’s index) is determined, which is used to categorize the held out (i.e. unseen) case. This process is repeated until each case has been categorized. The performance of significant parameters was then quantified by their average area under the ROC curve, sensitivity, specificity and accuracy in predicting tendon symptoms.
Results
Among the demographic parameters analysed, gender was found to have a significant association with mean SWV (estimated effect ± std. error female sex: 0.444 ± 0.206 m/s, p = 0.032) for the central tendon region, whereas subject age and body mass index showed no significant association (p = 0.979 and p = 0.796, respectively). No associations with the other tendon regions were found. Within-region variability in SWV differed between the sexes in the entire tendon (female sex: −0.169 ± 0.043 m/s, p < 0.001) and the distal region (female sex: −0.153 ± 0.054 m/s, p = 0.005). Additionally, athlete age showed a significant negative association with SD SWV (−0.169 ± 0.043 m s−1 year−1, p < 0.001) in the central PT region. Female sex was associated with shorter PTs (−2.78 ± 1.05 mm, p = 0.009). Similarly, the PTs of female skiers were lower in the cross-sectional area (−21.9 ± 4.9 m/s, p < 0.001). Supplementary Table A displays the PT SWE characteristics and morphology of the total dataset stratified by sex and age.
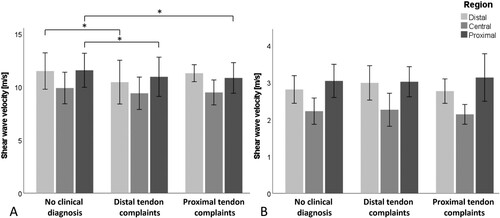
Of the 194 knees examined, 62 were diagnosed with distal (29) and proximal (33) PT complaints. No subjects were diagnosed with mid-portion PT complaints (). Tendon morphological characteristics were comparable among the three groups with clinical symptoms, with neither average cross-sectional area (control vs. distal PT complaints: p = 0.179, control vs. proximal PT complaints: p = 0.062) nor tendon length (control vs. distal PT complaint group: p = 0.056, control vs. proximal PT complaint group: p = 0.528) yielding statistically significant differences. Mean SWV was, however, lower in skiers suffering from distal PT complaints (estimated effect ± std. error: −0.752 ± 0.355 m/s, p = 0.035) and proximal PT complaints (−0.721 ± 0.305 m/s, p = 0.019) in the respective tendon region compared to the tendons of asymptomatic skiers (A). Moreover, the mean SWV was decreased in skiers with distal PT complaints in the proximal tendon region (−0.770 ± 0.328 m/s, p = 0.020). Regional variation in SWV did not differ between the groups with statistical significance in any of the performed comparisons (B).
Figure 3. Shear wave velocity. Mean average (A) and standard deviation (B) shear wave velocity within the analysed patellar tendon regions after clinical categorization into symptomatic and asymptomatic groups of respective anatomical locations. Error bars: SD. Asterisk: p < 0.05.
Cross-validated categorization of tendons based on regional mean SWV yielded sensitivity in detecting symptomatic skiers in the range of 0.606–0.621 (). On MRI, however, only 12 in 29 (sensitivity 0.414) and none in 33 tendons (sensitivity 0.000) showed any pathological alterations in knees diagnosed with distal and proximal PT complaints, respectively (Supplementary Table B). Three tendons displayed alterations consistent with pathological alterations without the corresponding finding during clinical examination (in the distal region).
Table 1. Cross-validated performance of the regional mean shear wave velocity (SWV) in discriminating proximal or distal patellar tendon complaints from healthy tendons.
Discussion
Knee overuse injuries, and PT complaints in particular, are frequent among youth competitive alpine skiers (Bergstrøm, Brandseth, Fretheim, Tvilde, & Ekeland, Citation2001). Indeed, 47% of competitive alpine skiers aged between 13 and 15 years were found to suffer from overuse-related knee complaints, of which 68% were diagnosed with PT complaints in a previous publication based on a subject population intersecting the current cohort (Fröhlich et al., Citation2020b). Skiing exposes the PT to high mechanical stress that can adversely accumulate over the career if adequate recovery is not ensured. In particular, the knee joint must accommodate repeated phases of eccentric, concentric and quasi-isometric muscle contractions, in which the knee is pushed anteriorly (Alhammoud, Hansen, Meyer, Hautier, & Morel, Citation2020). In addition, off-snow training consists of a high proportion of maximal/explosive strength and jump training, adding mechanical demand on the PT (Gilgien et al., Citation2018). Timely detection of inadequate response to loading may allow practitioners and trainers to intervene accordingly and potentially avert the development of severe symptoms. Imaging modalities in current clinical use, however, are limited in their capability in visualizing impending symptoms. For instance, B-mode US imaging was unable to predict current or future PT symptoms any better than past history of symptoms in previous studies (Cook et al., Citation2001; Emerson, Morrissey, Perry, & Jalan, Citation2010; Khan et al., Citation1997). Similarly, MRI imaging has shown limited association with current PT complaints (sensitivity: 0.57, specificity: 0.82 (Warden et al., Citation2007) and an inability to predict future symptoms (Tsehaie et al., Citation2017).
Tissue stiffness has been utilized as a diagnostic marker for centuries by means of palpation. Whereas manual palpation yields qualitative information and requires large stiffness changes in disease, SWE provides a quantitative estimate with high accuracy (Li & Cao, Citation2017). Tendinopathic degeneration is associated with collagen disarray and disruption and an increased proportion of ground substance (Fredberg & Stengaard-Pedersen, Citation2008). Tensile mechanical testing has linked these structural changes to a decrease in stiffness (Wiesinger, Seynnes, Kösters, Müller, & Rieder, Citation2020). Measuring voluntary joint torque and the corresponding change in tendon length to derive its stiffness is a valuable tool in understanding tendon structural homeostasis. Its implementation in a clinical setting is, however, impeded by technical and methodological limitations, including human limitations in neuromuscular control, (Peltonen, Cronin, Stenroth, Finni, & Avela, Citation2013) considerable potential for measurement bias and large time constraints (Lichtwark & Cresswell, Citation2013). Furthermore, this method yields global tendon stiffness estimates masking potential local variations. In contrast, the measurement procedure for SWE assessment is relatively straightforward and yields spatially resolved measurements. Indeed, we found SWV to be decreased in symptomatic tendons, with the largest difference seen at the location of the origin of symptoms. Accordingly, the mean SWV proved to be successful in discriminating skiers with symptomatic and asymptomatic tendons in both anatomical locations, albeit with limited accuracy.
The literature yields conflicting evidence on the association of tendon complaints with tendon shear behaviour as assessed with US SWE, particularly in the case of the PT. The structural organization of the tendon renders its mechanical response highly dependent on the load direction and modality. Changes in tensile behaviour therefore do not necessarily equate to analogous changes in shear behaviour. Whereas (Coombes et al., Citation2018) and (Zhang et al., Citation2014) found increased SWV in symptomatic PTs, (Dirrichs et al., Citation2016; Dirrichs et al., Citation2018) reported decreased SWV in two separate studies. These discrepancies may in part have arisen due to differences in their approach of positioning measurements (Obst et al., Citation2018). The former studies performed their measurements on the same anatomical location, whereas Dirrichs et al. analysed the most conspicuous tendon region as evaluated on US B-mode in one study and the region yielding the highest SWV in the second study. Tendinopathic stiffness alterations may well be spatially variable, which poses limitations when analysing single discrete locations. Our approach circumvents these limitations by sampling the entirety of the tendon and aggregating these measurements into reproducible parameters (Götschi et al., Citation2021). In both studies, Dirrichs et al. reported a higher sensitivity of SWE in detecting subjects with PT complaints compared to the current study. These studies, however, were based on a cohort of athletes seeking medical care for their tendon complaints, whereas the current study was conducted on a representative cohort of youth competitive skiers. Nevertheless, high intragroup measurement variability evidently will need to be addressed before potential transition of the method from the research setting to regular widespread athlete screening. The identification of confounding variables and the formulation of appropriate adjustment schemes may permit a reduction in measurement noise. The finding of decreased SWV in both the distal and the proximal regions in PTs with distal complaints has not been reported previously.
Among the demographic factors analysed, only sex had a significant effect on the mean SWV, with females showing higher velocities, which is in disagreement with previous investigations, (Hsiao, Chen, Lin, Chen, & Wang, Citation2015) who found decreased SWV in females. The cohort of the current study has a very narrow age range (13.8–15.8 years), and females at this age generally have a higher biological maturity. We therefore conjecture that the observed effect was a result of different sex-related biological maturities at the time of assessment. Previous studies found an association between SWV and subject age;(Hsiao et al., Citation2015) however, potentially owing to the narrow age range in the current study, we did not find such an association. On the other hand, we found that female sex and older age were associated with lower within-tendon SWV variability. From a functional perspective, these differences might again be a result of advanced tissue maturation. The cross-sectional area of the PT remains relatively constant throughout most of its length, and variations in material properties are therefore unlikely to be advantageous (Seynnes et al., Citation2009).
MRI assessment yielded high accuracy (0.882) in detecting distal PT complaints, albeit with limited sensitivity (0.414). On the other hand, no abnormalities in the proximal tendon region were detected by MRI, neither in asymptomatic nor in symptomatic tendons. Distal PT complaints in the studied age group primarily relate to Osgood Schlatter disease, which manifests as fragmentation of the tibial tubercle (Cairns et al., Citation2018; Sørensen et al., Citation2021). It is insofar unsurprising that many cases of distal PT complaints were associated with respective abnormalities on MRI. Our finding of decreased regional SWV in these cases, however, implies additional involvement of soft tissue alterations. Previous studies came to similar conclusions reporting distal tendon thickening in subjects suffering from Osgood Schlatter disease (Sørensen et al., Citation2021). A different situation was evident in the proximal PT region, where complaints are evidently primarily associated with nonosseous alterations, as indicated by the inability of MRI assessment to detect any conspicuous local alterations in this region.
There are limitations of this study that need to be considered. Variations in the measurement procedure likely affect the retrieved parameters. For instance, rotation of the US transducer relative to the tendon fibre orientation results in changes in SWV. We tried to minimize this effect by ensuring that the plane of measurement is always parallel to the fibre orientation. This procedure, however, cannot account for situations where the fibres are not colinear over the entire measurement frame. Tendon loading, either before or during the measurement, also influences the results. For this reason, we positioned the subjects five minutes prior to the assessment and gave the instruction to remain relaxed throughout the procedure. The physical activity during the preceding hours before assessment, however, was beyond our control. In confined structures with a diameter in the range of millimetres (such as the tendon), the acoustic pulse during SWE generates a guided wave, which alters the material’s mode of excitation and the resulting SWV. The tendon’s geometrical dimensions may therefore have a nonnegligible effect on the measured SWV. In our dataset, however, tendon cross-sectional area had a nonsignificant effect on SWV (data not shown). Rather than MR imaging, B-mode US assessment is the method of choice by many practitioners, owing to its wide availability and the capability to visualize tendon structural appearance (Dirrichs et al., Citation2016; Dirrichs et al., Citation2018). Due to organizational constraints, in the current study, we did not include an assessment of the US B-mode appearance of the tendons. Assessment of tendon B-mode appearance is highly dependent on the experience of the assessor, (Sunding, Fahlström, Werner, Forssblad, & Willberg, Citation2016) and within the context of regular screening of at-risk athletes, methods with a low assessor skill ceiling are of priority. Tendon swelling, a key feature in the B-mode diagnosis of tendinopathy, can readily be assessed with the technique of study by inspecting the 3D B-mode reconstruction. Whereas reports of tendon symptoms were collected prospectively, predictions thereof were performed retrospectively, which may bias performance estimates. We attempted to mitigate this limitation by performing cross-validation of the predictions.
Conclusion
In agreement with the most recent literature, we found a lower SWV in skiers suffering from patellar tendon complaints than in asymptomatic skiers. 3D mapping of shear wave speeds was significantly associated with tendon complaints, albeit with moderate retrospective prediction accuracy. The identification of confounders related to subject characteristics and the measurement and analysis procedure may reduce noise and thereby improve prediction performance. Nevertheless, the current results warrant examination of SWE in predicting tendon complaints in a prospective prognostic setting.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Alhammoud, M., Hansen, C., Meyer, F., Hautier, C., & Morel, B. (2020). On-field ski kinematic according to leg and discipline in elite alpine skiers. Frontiers in Sports and Active Living, 2, 56.
- Bergstrøm, K. A., Brandseth, K., Fretheim, S., Tvilde, K., & Ekeland, A. (2001). Activity-related knee injuries and pain in athletic adolescents. Knee Surgery, Sports Traumatology, Arthroscopy, 9(3), 146–150.
- Cairns, G., Owen, T., Kluzek, S., Thurley, N., Holden, S., Rathleff, M. S., & Dean, B. J. F. (2018). Therapeutic interventions in children and adolescents with patellar tendon related pain: A systematic review. BMJ open sport & exercise medicine, 4(1), e000383.
- Cassel, M., Baur, H., Hirschmüller, A., Carlsohn, A., Fröhlich, K., & Mayer, F. (2015). Prevalence of Achilles and patellar tendinopathy and their association to intratendinous changes in adolescent athletes. Scandinavian Journal of Medicine & Science in Sports, 25, e310–e318.
- Cook, J. L., Khan, K. M., Kiss, Z. S., Coleman, B. D., & Griffiths, L. (2001). Asymptomatic hypoechoic regions on patellar tendon ultrasound: A 4-year clinical and ultrasound followup of 46 tendons. Scandinavian journal of medicine & science in sports, 11(6), 321–327.
- Coombes, B. K., Tucker, K., Vicenzino, B., Vuvan, V., Mellor, R., Heales, L., … Hug, F. (2018). Achilles and patellar tendinopathy display opposite changes in elastic properties: A shear wave elastography study. Scandinavian Journal of Medicine & Science in Sports, 28, 1201–1208.
- Demirag, B., Ozturk, C., Yazici, Z., & Sarisozen, B. (2004). The pathophysiology of Osgood-Schlatter disease: A magnetic resonance investigation. Journal of Pediatric Orthopaedics B, 13, 379–382.
- Dirrichs, T., Quack, V., Gatz, M., Tingart, M., Kuhl, C. K., & Schrading, S. (2016). Shear Wave Elastography (SWE) for the Evaluation of Patients with Tendinopathies. Academic Radiology, 23, 1204–1213.
- Dirrichs, T., Quack, V., Gatz, M., Tingart, M., Rath, B., Betsch, M., … Schrading, S. (2018). Shear wave elastography (SWE) for monitoring of treatment of tendinopathies: A double-blinded, longitudinal clinical study. Academic radiology, 25, 265–272.
- Docking, S. I., & Cook, J. (2016). Pathological tendons maintain sufficient aligned fibrillar structure on ultrasound tissue characterization (UTC). Scandinavian journal of medicine & science in sports, 26(6), 675–683.
- Docking, S. I., Ooi, C. C., & Connell, D. (2015). Tendinopathy: Is imaging telling us the entire story? Journal of Orthopaedic & Sports Physical Therapy, 45, 842–852.
- Emerson, C., Morrissey, D., Perry, M., & Jalan, R. (2010). Ultrasonographically detected changes in Achilles tendons and self reported symptoms in elite gymnasts compared with controls - An observational study. Manual therapy, 15(1), 37–42.
- Fischer, A. N. (2021). Sinding-Larsen-Johansson Syndrome. Common Pediatric Knee Injuries.
- Franco, M. F., Madaleno, F. O., de Paula, T. M. N., Ferreira T, V., Pinto, R. Z., & Resende, R. A. (2021). Prevalence of overuse injuries in athletes from individual and team sports: A systematic review with meta-analysis and GRADE recommendations. Brazilian Journal of Physical Therapy, 25(5), 500–513.
- Fredberg, U., & Stengaard-Pedersen, K. (2008). Chronic tendinopathy tissue pathology, pain mechanisms, and etiology with a special focus on inflammation. Scandinavian Journal of Medicine & Science in Sports, 18, 3–15.
- Fröhlich, S., Helbling, M., Fucentese, S. F., Karlen, W., Frey, W. O., & Spörri, J. (2021). Injury risks among elite competitive alpine skiers are underestimated if not registered prospectively, over the entire season and regardless of whether requiring medical attention. Knee surgery, sports traumatology, arthroscopy, 29(5), 1635–1643.
- Fröhlich, S., Pazeller, S., Cherati, A. S., Müller, E., Frey, W. O., & Spörri, J. (2020a). Overuse injuries in the knee, back and hip of top elite female alpine skiers during the off-season preparation period: Prevalence, severity and their association with traumatic preinjuries and training load. BMJ Open Sport & Exercise Medicine, 6(1), e000892.
- Fröhlich, S., Peterhans, L., Stern, C., Frey, W. O., Sutter, R., & Spörri, J. (2020b). Remarkably high prevalence of overuse-related knee complaints and MRI abnormalities in youth competitive alpine skiers: a descriptive investigation in 108 athletes aged 13–15 years. BMJ Open Sport & Exercise Medicine, 6, e000738.
- Gilgien, M., Reid, R., Raschner, C., Supej, M., & Holmberg, H.-C. (2018). The training of olympic alpine ski racers. Frontiers in physiology, 9, 1772.
- Götschi, T., Schulz, N., Snedeker, J. G., Hanimann, J., Franchi M, V., & Spörri, J. (2021). Three-dimensional mapping of shear wave velocity in human tendon: A proof of concept study. Sensors (Basel), 21(5), 1655.
- Hsiao, M. Y., Chen, Y. C., Lin, C. Y., Chen, W. S., & Wang, T. G. (2015). Reduced patellar tendon elasticity with aging: In vivo assessment by shear wave elastography. Ultrasound in Medicine & Biology, 41, 2899–2905.
- Khan, K. M., Cook, J. L., Kiss, Z. S., Visentini, P. J., Fehrmann, M. W., Harcourt, P. R., … Wark, J. D. (1997). Patellar tendon ultrasonography and jumper’s knee in female basketball players: A longitudinal study. Clinical journal of sport medicine: official journal of the Canadian Academy of Sport Medicine, 7(3), 199–206.
- Khan, K. M., Forster, B. B., Robinson, J., Cheong, Y., Louis, L., Maclean, L., & Taunton, J. E. (2003). Are ultrasound and magnetic resonance imaging of value in assessment of Achilles tendon disorders? A two year prospective study. British journal of sports medicine, 37(2), 149–153.
- Ladenhauf, H. N., Seitlinger, G., & Green, D. W. (2020). Osgood-Schlatter disease: A 2020 update of a common knee condition in children. Current Opinion in Pediatrics, 32, 107–112.
- Li, G. Y., & Cao, Y. (2017). Mechanics of ultrasound elastography. Proceedings of the Royal Society A: Mathematical, Physical and Engineering Sciences, 473(2199), 20160841.
- Lichtwark, G. A., & Cresswell, A. G. (2013). Commentaries on Viewpoint: On the hysteresis in the human Achilles tendon. Journal of Applied Physiology, 114, 518.
- McAuliffe, S., McCreesh, K., Culloty, F., Purtill, H., & O’Sullivan, K. (2016). Can ultrasound imaging predict the development of Achilles and patellar tendinopathy? A systematic review and meta-analysis. British Journal of Sports Medicine, 50, 1516–1523.
- Obst, S. J., Heales, L. J., Schrader, B. L., Davis, S. A., Dodd, K. A., Holzberger, C. J., … Barrett, R. S. (2018). Are the mechanical or material properties of the achilles and patellar tendons altered in tendinopathy? A systematic review with meta-ANALYSIS. Sport Med Springer International Publishing 48:1–20.
- Payne, C., Watt, P., & Webborn, N. (2018). Shear wave elastography measures of the Achilles Tendon: Influence of time of day, leg dominance and the impact of an acute 30-minute bout of running. Applied Sciences, 8(7), 1170.
- Peltonen, J., Cronin, N. J., Stenroth, L., Finni, T., & Avela, J. (2013). Viscoelastic properties of the achilles tendon in vivo. Springerplus, 2, 1–8.
- Schoeb, T., Peterhans, L., Fröhlich, S., Frey, W. O., Gerber, C., & Spörri, J. (2020). Health problems in youth competitive alpine skiing: A 12-month observation of 155 athletes around the growth spurt. Scandinavian Journal of Medicine & Science in Sports, 30, 1758–1768.
- Scott, A., Squier, K., Alfredson, H., Bahr, R., Cook, J. L., Coombes, B., … Zwerver, J. (2020). ICON 2019: International scientific tendinopathy symposium consensus: Clinical terminology. British Journal of Sports Medicine, 54, 260–262.
- Seynnes, O. R., Erskine, R. M., Maganaris, C. N., Longo, S., Simoneau, E. M., Grosset, J. F., & Narici, M. V. (2009). Training-induced changes in structural and mechanical properties of the patellar tendon are related to muscle hypertrophy but not to strength gains. Journal of applied physiology, 107(2), 523–530.
- Sørensen, L. B., Rathleff, M. S., Dean, B. J. F., Oei, E., Magnusson, S. P., Olesen, J. L., & Holden, S. (2021). A systematic review of imaging findings in patients with Osgood-Schlatter disease. Translational Sports Medicine, 4, 772–787.
- Spörri, J., Müller, E., & Kröll, J. (2022). “When you’re down, stay down”: A lesson for all competitive alpine skiers supported by an ACL rupture measured in vivo. Journal of Sport and Health Science, 11, 14–20.
- Sunding, K., Fahlström, M., Werner, S., Forssblad, M., & Willberg, L. (2016). Evaluation of Achilles and patellar tendinopathy with greyscale ultrasound and colour Doppler: using a four-grade scale. Knee Surgery, Sport Traumatol Arthrosc Springer Berlin Heidelberg, 24, 1988–1996.
- Tsehaie, J., Poot, D. H. J., Oei, E. H. G., Verhaar, J. A. N., & de Vos, R. J. (2017). Value of quantitative MRI parameters in predicting and evaluating clinical outcome in conservatively treated patients with chronic midportion Achilles tendinopathy: A prospective study. Journal of Science and Medicine in Sport, 20(7), 633–637.
- Warden, S. J., Kiss, Z. S., Malara, F. A., Ooi, A. B. T., Cook, J. L., & Crossley, K. M. (2007). Comparative accuracy of magnetic resonance imaging and ultrasonography in confirming clinically diagnosed patellar tendinopathy. The American Journal of Sports Medicine, 35, 427–436.
- Wiesinger, H. P., Seynnes, O. R., Kösters, A., Müller, E., & Rieder, F. (2020). Mechanical and Material Tendon Properties in Patients With Proximal Patellar Tendinopathy. Frontiers in Physiology, 11, 1–11.
- Zhang, Z. J., Ng, G. Y. F., Lee, W. C., & Fu, S. N. (2014). Changes in morphological and elastic properties of patellar tendon in athletes with unilateral patellar tendinopathy and their relationships with pain and functional disability. PLoS One, 9, 1–9.