
ABSTRACT
This 40-week cluster-randomised controlled trial (RCT) examines the effects of football and Zumba on self-perceived job satisfaction, work role functioning and sick leave among Norwegian female hospital employees. Hundred-and-seven employees, mainly consisting of nurses (80%), were allocated into three groups; Football (FG), Zumba (ZG) and Control (CG). The exercise groups were offered two to three and one to two 1-h weekly sessions during the first 12 and last 28 weeks, respectively, with an actual weekly exercise frequency of 2.4 ± 0.5 and 0.9 ± 0.2 in FG and 2.3 ± 0.3 and 0.8 ± 0.2 in ZG. Outcome variables were measured at baseline, 12 and 40 weeks. In comparison to CG (4.8 days 95% CI 3.2–6.4), ZG (1.9 days, 95% CI 0.4–3.5) had a significant lower overall mean days of sickness absence during last sick leave period (−2.9 days, 95% CI −5.1 to −0.7, p = .011) which corresponded to a moderate effect size (d = 0.60). Between baseline (88.5%, 95% CI 84.3–92.6) and 12 weeks (93.8%, 95% CI 89.4–98.2), ZG showed significant within-group improvement in total score of the Work Role Functioning Questionnaire (WRFQ) (5.3%, 95% CI 0.6–10.1, p = .029), corresponding to a moderate effect size (d = 0.40). This study indicates that two to three 1-h weekly Zumba sessions can have a preventive effect on sick leave in female hospital employees.
Highlights
Participants in Zumba exercise organised by the workplace showed a significant lower number of sick leave days compared with the controls.
Despite a correspondingly significant reduction in exercise adherence in both groups in the last 28 weeks, only FG showed tendencies for group improvement in job satisfaction and total WRFQ in this period.
Workplace promotion of exercise and physical activity can thus be beneficial for both the workers and the organisation.
Introduction
Due to an aging workforce, declining recruitment and high turnover intentions based on affective conditions, the shortage of health care workers is increasing worldwide (Coomber & Barriball, Citation2007; Duvall & Andrews, Citation2010). In combination with longer life expectancy and higher number of people living with chronic diseases, the need for health care workers will increase and make the situation even more critical (Roelen et al., Citation2013). Therefore, it is a growing global consensus that investing in the health of health care workers not only improves their quality of life and longevity, but also yields substantial economic gains (Darzi & Evans, Citation2016). According to the World Health Organisation (WHO), there is an increased global demand for health and social care staff with creation of 40 million new jobs by 2030 (World Health Organization, Citation2016).
A large proportion of health care workers feel they are underpaid and overworked (Goodare, Citation2017). Thus, improving job satisfaction might be key to reduce the turnover and strengthening retention of health care workers (Halcomb et al., Citation2018). Furthermore, health care workers have a relatively high prevalence of poor health due to inadequate health and fitness promoting leisure physical activity and unhealthy diet (Petrelli et al., Citation2018; Stanulewicz et al., Citation2020) that in combination with relatively demanding work tasks (Bridgeman et al., Citation2018) make them particularly vulnerable to sick leave and early retirement (Klein et al., Citation2018).
Thus, it does not seem like health care workers gain the health benefits from their occupational physical activity as they could expect from leisure time physical activity (Allesøe et al., Citation2015), termed the physical activity paradox (Holtermann et al., Citation2018). This paradox, which implies that leisure physical activity promotes health while high occupational physical demands impairs health, indicates that a prerequisite for physical activity to be health-promoting is that it either takes place as self-selected participation in leisure time and/or that it consists of exercises that are sufficiently intensive for a positive effect on cardiovascular, metabolic and musculoskeletal fitness (Krustrup et al., Citation2018).
We have previously demonstrated that both football and Zumba exercise improve the aerobic capacity and body composition (Barene et al., Citation2013; Barene et al., Citation2014a), as well as muscle pain (Barene et al., Citation2014b) and muscle strength (Barene et al., Citation2016) of female hospital employees. As there is little evidence from previous workplace physical activity interventions of beneficial effects on job satisfaction, work role functioning or sick leave, we investigated the potential effects of football and Zumba on these outcomes among female hospital employees.
Methods
Study design
This 40-weeks RCT among employees at a larger Hospital in Norway was performed between January and October 2011. The inclusion criteria for participation in the study were hospital employees of either sex aged 25–65 years, with pregnancy, angina pectoris and life-threatening diseases as exclusion criteria. However, due to the relatively low number of male participants, only females were included in the statistical analyses. The study was ethically approved by the Regional Committees for Medical and Health Research Ethics, Norway (2010/2385-8), and registered in the International Standard Randomised Controlled Trial Number Register (ISRCTN61986892). All participants gave their written informed consent to participate in the study.
Recruitment of participants
The recruitment process has previously been presented (Barene et al., Citation2013). In short, out of 660 female hospital employees invited to participate in the study, 161 completed the screening questionnaire that was distributed during the initial information meetings prior to the baseline tests. A total of 109 females completed the baseline tests, whereas 107 fulfilled the inclusion criteria and consented to participate in the study. The participants were divided into clusters based on proximity to those who worked together on everyday basis, which were randomly allocated to the following groups; Football (FG), Zumba (ZG) or Control (CG).
Randomisation procedure
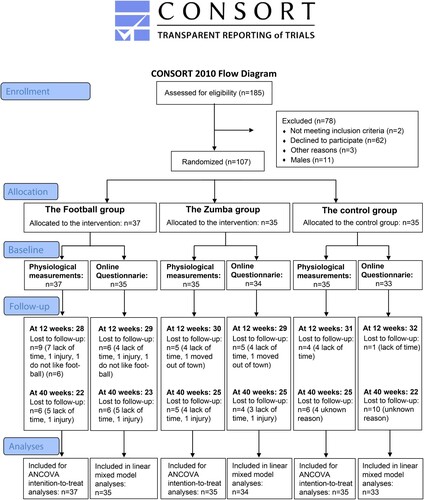
The randomisation procedure was conducted by the project leader and is previously reported (Barene et al., Citation2013). In short, hospital employees in a single department working together on everyday basis formed cluster 1 (n = 28). In the next step, two almost equal-sized clusters, cluster 2 (n = 27) and 3 (n = 28) were matched on sex, body mass index (BMI), age and job seniority, with the remaining consenters assigned into three smaller clusters, cluster A (n = 7), B (n = 8) and C (n = 9) matched on the same variables as above. The randomisation was made by lot by blinded staff and composed as follows; FG: cluster 3 + C (n = 37), ZG: cluster 2 + B (n = 35) and CG: cluster 1 + A (n = 35) (Barene et al., Citation2013). Because of the relatively low number of male participants (n = 11) and the fact that all males in ZG (n = 3) withdrew from the study within the first 3 weeks of the exercise intervention, and that only half of the male participants in FG (n = 2) completed the intervention period, only females were included in the statistical analyses. The number of participants in this study, which is based on the data from the online questionnaire, is presented in .
Figure 1. Flow chart of recruitment and adherence during the 40-week intervention period with specification of the number of participants who completed (i) the physiological measurements and (ii) the online questionnaire.
Intervention content
The exercise intervention was conducted between January 11 and March 31 in 2011 and is previously described (Barene et al., Citation2016). In short, both exercise groups were offered exercise outside working hours three 1-h sessions per week during the first 12 weeks, and two 1-h sessions per week during the last 38 weeks. Participant in both exercise groups had little or no previous experience with the activities.
FG performed football sessions consisting of ordinary three-a-side or four-a-side matches in a traditional gymnastics hall (10 × 20 m) owned by the hospital, and/or five-a-side, six-a-side, seven-a-side matches in a municipal sports hall (20 × 40 m) located 3 km from the hospital. Each exercise session was initiated by a 5-min low-intensity warm-up period and included a 5-min half-time break. The football exercise sessions were fully supervised by an instructor throughout the 12-week intervention period. Because only a few participants had previous experience with football, there was a 30-min introduction of basic technical exercises in the first exercise session. The Zumba sessions were conducted at a fitness centre located 3 km from the hospital and comprised continuous dance-movements to Latin music with varying intensity level throughout the sessions. Each session was initiated with low-intensity movements for the first 5 min, followed by an increasing intensity throughout the workout. At the end of the exercise session, the intensity was gradually reduced. The Zumba sessions were supervised by three certified Zumba instructors, each responsible for regular sessions per week.
Measurement procedures pre, during and post the intervention
The participants were invited to several measurements at baseline (January 2011) and at follow-up tests after 12 (April 2011) and 40 weeks (October 2011), respectively. In addition to the online questionnaire, all three test rounds consisted of the following measures: (1) fasting blood samples obtained from the antecubital vein using Vacuette EDTA and serum tubes (Greiner Bio-One, Kremsmünster, Austria) (Barene et al., Citation2013; Barene et al., Citation2014a), (2) dual-energy X-ray absorptiometry (DEXA) scans to examine total body and regional fat, muscle, and bone mass (QDR Discovery Wi, Hologic, Inc., Bedford, Massachusetts, USA) (Barene et al., Citation2013; Barene et al., Citation2014a), (3) systolic and diastolic blood pressure (HEM-709; OMRON, Vernon Hills, Illinois, USA) (Barene et al., Citation2013; Barene et al., Citation2014a), (4) pulmonary gas exchange (VMAX Spectra Series, SensorMedics Corporation, Yorba Linda, California, USA), (5) heart rate (Polar Team System, Polar Electro Oy, Kempele, Finland) and (6) blood lactate (LactatePro™ LT-1710, ARKRAY, Inc., Kyoto, Japan) were obtained during a standardised bicycle test (Barene et al., Citation2013; Barene et al., Citation2014a), (7) isometric muscle strength was measured with Newtest Isometric Force System dynamometer (Newtest, Oy, Oulu, Finland) (Barene et al., Citation2016), and (8) maximal jump height were performed on a force platform (OR6-5-2000, AMTI, Watertown, MA, USA) (Barene et al., Citation2016). Those responsible for conducting and evaluating the physiological measurements mentioned above were blinded to intervention group affiliation.
Leisure physical activity
Information about the participants’ leisure physical activity level was obtained through a screening questionnaire prior to the baseline tests containing the following question: “How much have you been physically active in your leisure time during the past twelve months?” The four answering categories were; (1) Sedentary leisure time: you spent most of your time reading, watching television, going to the movies or other sedentary activity during leisure time. You walk, ride a bike or engage in physically active in some other way less than 2 h a week; (2) Moderate physical activity during leisure time: You walk, ride a bike or engage in physical activity in some other way for a minimum of 2 h a week, often without perspiring. This also includes walking or riding a bike to or from work, Sunday walks, ordinary gardening, fishing, table tennis and bowling; (3) Moderate, regular physical activity during leisure time: you exercise regularly one to two times a week, each time for a minimum of 30 min, with jogging, swimming, tennis, badminton or other activity that makes you perspire, and (4) Regular physical activity and exercise: you are active with running, swimming, tennis, badminton, aerobics or something similar at least three times/week (Hopstock et al., Citation2019; Palmlöf et al., Citation2016).
Job satisfaction
Perceived job satisfaction was measured on a four-point Likert scale with an option of (I) satisfied, (II) fairly satisfied, (III) fairly dissatisfied, and (IV) dissatisfied (Quinn et al., Citation1974).
The work role functioning questionnaire (WRFQ)
Potential intervention effects on work-related functioning were evaluated through a modified version of the WRFQ (Amick et al., Citation2000). The WRFQ has previously been reported to be a reliable and valid instrument for measuring the perceived difficulties in meeting work demands among employees given their physical health or emotional problems (Abma et al., Citation2018). The original WRFQ comprises 27 items focusing on the following four subscales; (I) work scheduling and output demands (10 items), (II) physical demands (5 items), (III) mental and social demands (7 items) and (IV) flexibility demands (5 items). For each item, the participant is asked to indicate the percentage of time having difficulties performing job demands, with responses ranging from 0 (difficult all of the time, 100%) to 4 (difficult none of the time, 0%). Total WRFQ are calculated by averaging responses and are transformed so that higher total scores indicate better work role functioning; scores greater than 90 are considered to indicate “good work role functioning”, while a score 95–100 is indicative of “successful work role functioning” (Cochrane et al., Citation2018). From the original form, a total of 17 items were derived with the following distribution on the various subscales; 5 (work scheduling and output demands), 3 (physical demands), 4 (mental and social demands), and 5 (flexibility demands). Single summated average was calculated for 17 of the items and multiplied by 25 which represents a work role functioning measure varying between 0 (difficulty meeting all 17 work demands 100% of the time) and 100 (able to meet all the 18 work demands 100% of the time). Work scheduling demands (six items) assess the worker’s ability to manage the workday, whereas the items focusing on physical (eight items), mental (four items), social (three items) and output (five items) demands measure a range of physical loads, work cognitive requirements, interaction with other people at work and job completion/satisfaction, respectively.
Sick leave
Self-reported sick leave was derived from responses to the following questions: (I) “During the past 3 months, how many days have you been absent from work due to general health problems (illness, treatment or medical evaluation)?” and (II) “How many days were you absent from work the last sick leave period?”
Statistical analyses
All statistical analyses were performed using SPSS version 27.0. The changes from baseline to 12- and 40-week follow-up were evaluated using a linear mixed model. For the best model-fit (Faraway, Citation2016), age and baseline BMI were included as fixed factors in addition to subject-specific random effects. Restricted maximum likelihood with degrees of freedom based on the Satterthwaite approximation was used as estimation method. The estimates for the difference obtained from the least square means, hereinafter referred to as the overall mean, form the basis for the effect measures on the outcome variables and the corresponding 95% confidence intervals and p-values. P levels less than .05 were accepted as statistically significant. For outcome variables that showed significant differences/changes, the effect sizes were estimated using Cohen’s d according to the principle of average difference divided by the total standard deviations and multiplied with a correction factor (0.95) due to the small group sizes (N < 50). The following power sizes for Cohen’s d were used; weak (<0.3), moderate (0.3–0.6) and strong (>0.6) (Lipsey & Wilson, Citation1993).
Results
Baseline characteristics
The age, BMI and job seniority of the participants included in the baseline questionnaire were on average 46.1 ± 9.2 years, 25.4 ± 3.1 kg/m2 and 74.5 ± 64.7 months, respectively (), with no significant between-group differences observed at baseline.
Table 1. Baseline characteristics of age, anthropometry, physical activity level, job seniority, job satisfaction, the four subscales in the Work Role Functioning Questionnaire; (i) work scheduling and output demands, (ii) physical demands, (iii) mental and social demands, (iv) flexibility demands, as well as (v) the calculated total score, and self-reported sick leave for the Football Group (n = 35), the Zumba Group (n = 34), and the Control Group (n = 33), respectively.
Self-reported physical activity level the past 12 months was measured on a Likert scale from 1 (being almost completely inactive) to 4 (regular hard physical exercise several times per week) showing an overall average of 2.5 ± 0.6, with no significant between-group differences (p = .678).
Exercise frequency
As we have reported previously (Barene et al., Citation2014a), the participant’s average total number of exercise sessions during the first 12 weeks were 28.2 ± 6.0 sessions (2.4 ± 0.5 per week) vs. 27.7 ± 4.0 sessions (2.3 ± 0.3 per week) in FG and ZG, respectively. The corresponding adherence rate during the last 28 weeks was 24.4 ± 5.7 sessions (0.9 ± 0.2 per week) vs. 19.8 ± 4.9 sessions (0.8 ± 0.2 per week) in the two respective groups, which means a reduced exercise frequency of 63 and 65% in FG and ZG, respectively.
Job satisfaction
Based on the linear mixed model analyses, no between-group differences nor within-group changes were observed in job satisfaction during the 40 weeks intervention period (). However, by examining the intervention groups’ changes between 12 and 40 weeks, i.e. with a simultaneous reduction in exercise adherence, FG showed a tendency for increase in job satisfaction (0.03 on a four-point scale, 95% CI, −0.02 to 0.01), whereas the opposite pattern was observed in ZG (−0.1, 95% CI, −0.4, 0.2).
Table 2. Within-group changes and between-group differences in the Football group (n = 35), the Zumba group (n = 34) and the Control group (n = 33) during 12 and 40 weeks of exercise.
The work role functioning questionnaire (WRFQ)
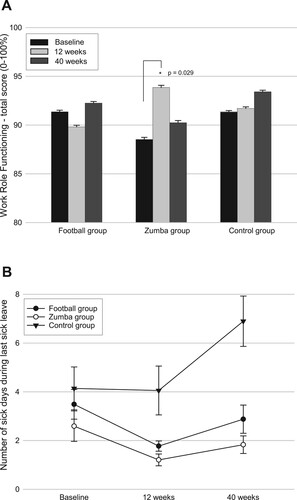
In comparison to CG, no significant between-group differences were observed in total score of WRFQ neither in FG (−1.6%, 95% CI −6.5 to 3.2, p = .501) nor ZG (−1.7%, 95% CI −6.4 to 3.1, p = .494) (). However, in ZG significant within-group improvements with associated moderate effect sizes were observed for the subscales physical demands between baseline and 12 (6.7%, 95% CI 1.2–12.2, p = .017, d = 0.45) and 40 (8.2%, 95% CI 2.5–13.9, p = .005, d = 0.54) weeks, respectively, and mental and social demands between baseline and 12 weeks (6.0%, 95% CI 0.4–11.6, p = .037, d = 0.40) (), with an associated within-group improvement in the total score of WRFQ (5.3%, 95% CI 0.6–10.1, p = .029, d = 0.40) ((A)). No such within-group improvements were observed in FG nor in CG. However, between 12 and 40 weeks (i.e. the period of reduced exercise adherence), a tendency for increase in total score of WRFQ was observed in FG (2.4%, 95% CI, −4.2 to 9.1) with an adverse tendency for reduction in ZG (−3.6%, 95% CI −10.1 to 3.0).
Figure 2. (A) Within-group changes in total score of WRFQ, and (B) between-group differences in the number of sick days during last sick leave throughout the intervention period. Error bars are presented as standard error.
Sick leave
During the 40-weeks intervention period, ZG revealed a significant lower overall mean in number of sick days during last sick leave period compared to CG (−2.9 days, 95% CI −5.1 to −0.7, p = .011, d = 0.60) ((B)) with an associated lower overall mean in number of sick days due to general health problems the past four weeks (−0.6 days, 95% CI −1.2 to −0.0, p = .043, d = .33) (). Although no significant differences in sick leave were observed between FG and CG, the study revealed tendencies towards favourable lower overall mean with corresponding moderate effect sizes in both the number of sick days during last sick leave period (−1.9 days, 95% CI −4.1 to 0.3, p = .093, d = .39), as well as due to general health problems the past 4 weeks (−0.5 days, 95% CI −1.1 to 0.0. p = .065, d = .43) also in FG ().
Discussion
The aim of our study was to examine the effects of football and Zumba exercise, respectively on job satisfaction, work demands related to work role functioning, and sick leave from work. In comparison to CG, ZG had a significant lower overall mean of sick days during last sick leave period, as well as number of sick days due to general health problems past four weeks. With regards to work role functioning, no between-group differences were observed in neither of the exercise groups compared to CG. However, in ZG significant within-group improvements were revealed for the two subscales physical demands and mental and social demands, as well in total score of WRFQ between baseline and 12 weeks. No intervention effects were observed in job satisfaction.
It is worth noting that the reported sick leave in the present study applies to general health problems, and not a specific cause. Nevertheless, the significant lower overall means in number of sick leave days with corresponding moderate effects sizes observed in ZG, can be considered beneficial both from a health perspective as well as from an employer perspective. In this context, it should also be mentioned that the tendencies towards lower overall means and correspondingly moderate effect sizes for FG compared to CG can be considered advantageous.
We have previously documented physiological health improvements after both football and Zumba exercise (Barene et al., Citation2013; Barene et al., Citation2014a), which may be a potential explanation for the observed lower number of sick days in the last period of sick leave as well as number of sick days due to general health problems past four weeks. Moreover, as regular physical activity is associated with beneficial self-reported health, self-efficacy and well-being, this may represent potential factors explaining the observed positive effects on sick leave days (Barene & Krustrup, Citation2022). Furthermore, as previous studies have suggested that social relations may affect sick leave (Löve et al., Citation2012; Melchior et al., Citation2003; Rydström et al., Citation2017), another explanation may be increased perceived social affiliation through participation in group-based exercises. We can only speculate on potential reasons for the within-group change from baseline to 40 weeks in CG. However, since daylight is believed to affect human health (Aries et al., Citation2015), this may be a potential explanation for the trend of reduced number of sick leave days in all three groups between baseline (January) and 12 weeks (March) which represents the period in Northern Norway (located 150 km north of the arctic circle) from very dark time to gradually brighter spring days.
Although previous studies have suggested that workplace interventions may have positive effects on musculoskeletal disorders (Sundstrup et al., Citation2020) and work ability (Oakman et al., Citation2018), previous systematic reviews on workplace interventions have demonstrated scarce evidence to support that physical activity is effective in reducing sick leave (Amlani & Munir, Citation2014; Pereira et al., Citation2015). Based on a 15-month prospective observational study on health care workers, a lower risk of long-term sick leave was reported for those who were engaged in regular aerobics and gym activities compared to those who did not exercise regularly (Eriksen et al., Citation2003), which may be comparable to ZG in the present study. However, it is difficult to conclude whether the associations in the study by Eriksen et al. (Citation2003) were due to effects of exercise or to the fact that healthy individuals are more inclined to and have the resources to participate in physical activities.
No between-group differences were observed in any of the subscales of the WRFQ, and consequently nor in the total score. However, in ZG significant improvements characterised by moderate effect sizes were observed in the subscales of physical demands and mental and social demands, respectively, as well as in total score of WRFQ between baseline and 12 weeks. These findings are in accordance with a previous systematic review and meta-analysis reporting significant improvements in physical functioning outcomes after supervised resistance and/or aerobic exercise interventions (Chase et al., Citation2017), and may be linked to the simultaneous improvements in ZG related to both strength, lower limb lean mass and postural sway (Barene et al., Citation2016), as well as self-reported muscle pain (Barene et al., Citation2014b). The improvement in perceived work role functioning related to mental and social demands observed for ZG is in accordance to a previous systematic review reporting favourable effects in perceived job stress after aerobic exercises (Chu et al., Citation2014). Regarding FG, no significant within-group changes were observed in work role functioning during the 40-week intervention period.
The lack of effect on job satisfaction in both exercise groups is in line with previous workplace physical activity intervention studies failing to demonstrate effects (Daane, Citation2018), but in contrast to others reporting beneficial effects (Arslan et al., Citation2019). A potential explanation for the lack of positive trends in within-group changes in both job satisfaction, total score of WRFQ and sick leave days in ZG the past 28 weeks, may be the significant reduction (p < .001) in exercise adherence between 12 and 40-week follow-up. In contrast, FG showed tendencies for within-group improvements in both job satisfaction and total score of WRFQ the past 28 weeks despite a corresponding reduction (p < .001) in exercise adherence. A possible explanation for this phenomenon may be the uniqueness of the football exercise, in the sense that there is most likely to be a greater social group affiliation among football players compared to Zumba, and which may have an impact on psychosocial factors at work.
Limitations
Limitations of the study were the relatively modest exercise adherence during the last 28 weeks (36%), as well as the use of self-reported outcome measures. Apart from information on the average age of the total population (n = 660), which indicated that the sample was representative, we have no supplementary data to confirm the sample’s representativeness, which could potentially represent a weakness of the study. Moreover, the lack of control over the participants’ physical activity level during leisure as well as information on their dietary habits may represent additional biases to the results.
Conclusions
This study showed that Zumba exercise may have a preventive effect on the number of sick leave days among female hospital employees over a 40-week intervention period compared to controls, with only a tendency for preventive effect from football exercise. Furthermore, ZG revealed within-group improvements in perceived total work role functioning (WRFQ) between baseline and 12-weeks follow-up. Based on the promising preventive effect on sick leave from both forms of exercise, we recommend that similar physical activity workplace interventions are implemented in the future.
Acknowledgements
Dr Mehmet Sinan Iyisoy for excellent statistical support related to the Linear Mixed Model. Dora Barene, Harald Oseland and Ingrid Haugen are greatly acknowledged for their contribution to data collection. Furthermore, we are grateful for the grants allocated from the University of Nordland, Nordland Hospital, the Municipality of Bodø and the Stamina Fitness Centre.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Abma, F. I., Bültmann, U., Amick, B. C., Arends, I., Dorland, H. F., Flach, P. A., van der Klink, J. J. L., van de Ven, H. A., & Bjørner, J. B. (2018). The work role functioning questionnaire v2. 0 showed consistent factor structure across six working samples. Journal of Occupational Rehabilitation, 28(3), 465–474. https://doi.org/10.1007/s10926-017-9722-1
- Allesøe, K., Holtermann, A., Aadahl, M., Thomsen, J. F., Hundrup, Y. A., & Søgaard, K. (2015). High occupational physical activity and risk of ischaemic heart disease in women: The interplay with physical activity during leisure time. European Journal of Preventive Cardiology, 22(12), 1601–1608. https://doi.org/10.1177/2047487314554866
- Amick, B. C., Lerner, D., Rogers, W. H., Rooney, T., & Katz, J. N. (2000). A review of health-related work outcome measures and their uses, and recommended measures. Spine, 25(24), 3152–3160. https://doi.org/10.1097/00007632-200012150-00010
- Amlani, N. M., & Munir, F. (2014). Does physical activity have an impact on sickness absence? A review. Sports Medicine, 44(7), 887–907. https://doi.org/10.1007/s40279-014-0171-0
- Aries, M., Aarts, M., & van Hoof, J. (2015). Daylight and health: A review of the evidence and consequences for the built environment. Lighting Research & Technology, 47(1), 6–27. https://doi.org/10.1177/1477153513509258
- Arslan, S. S., Alemdaroğlu, İ, Karaduman, A. A., & Yilmaz, ÖT. (2019). The effects of physical activity on sleep quality, job satisfaction, and quality of life in office workers. Work, 63(1), 3–7. https://doi.org/10.3233/WOR-192902
- Barene, S., Holtermann, A., Oseland, H., Brekke, O.-L., & Krustrup, P. (2016). Effects on muscle strength, maximal jump height, flexibility and postural sway after soccer and Zumba exercise among female hospital employees: A 9-month randomised controlled trial. Journal of Sports Sciences, 34(19), 1849–1858. https://doi.org/10.1080/02640414.2016.1140906
- Barene, S., & Krustrup, P. (2022). Football and Zumba training in female hospital staff: Effects after 12 and 40 weeks on self-reported health status, emotional wellbeing, general self-efficacy and sleep problems. International Journal of Environmental Research and Public Health, 19(3), 1685. https://doi.org/10.3390/ijerph19031685
- Barene, S., Krustrup, P., Brekke, O. L., & Holtermann, A. (2014a). Soccer and Zumba as health-promoting activities among female hospital employees: A 40-weeks cluster randomised intervention study. Journal of Sports Sciences, 32(16), 1539–1549. https://doi.org/10.1080/02640414.2014.906043
- Barene, S., Krustrup, P., & Holtermann, A. (2014b). Effects of the workplace health promotion activities soccer and Zumba on muscle pain, work ability and perceived physical exertion among female hospital employees. PLoS One, 9(12), 1–14. https://doi.org/10.1371/journal.pone.0115059
- Barene, S., Krustrup, P., Jackman, S. R., Brekke, O. L., & Holtermann, A. (2013). Do soccer and Zumba exercise improve fitness and indicators of health among female hospital employees? A 12-week RCT. Scandinavian Journal of Medicine & Science in Sports, 24(6), 990–999. https://doi.org/10.1111/sms.12138
- Bridgeman, P. J., Bridgeman, M. B., & Barone, J. (2018). Burnout syndrome among healthcare professionals. American Journal of Health-System Pharmacy, 75(3), 147–152. https://doi.org/10.2146/ajhp170460
- Chase, J.-A. D., Phillips, L. J., & Brown, M. (2017). Physical activity intervention effects on physical function among community-dwelling older adults: A systematic review and meta-analysis. Journal of Aging and Physical Activity, 25(1), 149–170. https://doi.org/10.1123/japa.2016-0040
- Chu, A. H. Y., Koh, D., Moy, F. M., & Müller-Riemenschneider, F. (2014). Do workplace physical activity interventions improve mental health outcomes? Occupational Medicine, 64(4), 235–245. https://doi.org/10.1093/occmed/kqu045
- Cochrane, A., Higgins, N. M., Rothwell, C., Ashton, J., Breen, R., Corcoran, O., FitzGerald, O., Gallagher, P., & Desmond, D. (2018). Work outcomes in patients who stay at work despite musculoskeletal pain. Journal of Occupational Rehabilitation, 28(3), 559–567. https://doi.org/10.1007/s10926-017-9748-4
- Coomber, B., & Barriball, K. L. (2007). Impact of job satisfaction components on intent to leave and turnover for hospital-based nurses: A review of the research literature. International Journal of Nursing Studies, 44(2), 297–314. https://doi.org/10.1016/j.ijnurstu.2006.02.004
- Daane, K. C. (2018). Yoga as a means of increasing job satisfaction in the workplace. [Masters dissertation]. University of Wisconsin-Stout. https://minds.wisconsin.edu/bitstream/handle/1793/79755/2018daanek.pdf?sequence=1&isAllowed=y
- Darzi, A., & Evans, T. (2016). The global shortage of health workers – An opportunity to transform care. The Lancet, 388(10060), 2576–2577. https://doi.org/10.1016/S0140-6736(16)32235-8
- Duvall, J. J., & Andrews, D. R. (2010). Using a structured review of the literature to identify key factors associated with the current nursing shortage. Journal of Professional Nursing, 26(5), 309–317. https://doi.org/10.1016/j.profnurs.2010.02.002
- Eriksen, W., Bruusgaard, D., & Knardahl, S. (2003). Work factors as predictors of sickness absence: A three month prospective study of nurses’ aides. Occupational and Environmental Medicine, 60(4), 271–278. https://doi.org/10.1136/oem.60.4.271
- Faraway, J. J. (2016). Extending the linear model with R: Generalized linear, mixed effects and nonparametric regression models. Chapman and Hall/CRC.
- Goodare, P. (2017). Literature review: Why do we continue to lose our nurses? Australian Journal of Advanced Nursing, 34(4), 50–56. https://search.informit.org/doi/10. 3316/informit.947634096009471
- Halcomb, E., Smyth, E., & McInnes, S. (2018). Job satisfaction and career intentions of registered nurses in primary health care: An integrative review. BMC Family Practice, 19(1), 136. https://doi.org/10.1186/s12875-018-0819-1
- Holtermann, A., Krause, N., van der Beek, A. J., & Straker, L. (2018). The physical activity paradox: Six reasons why occupational physical activity (OPA) does not confer the cardiovascular health benefits that leisure time physical activity does. British Journal of Sports Medicine, 52(3), 149–150. https://doi.org/10.1136/bjsports-2017-097965
- Hopstock, L., Løvsletten, O., Johansen, H., Tiwari, S., Njølstad, I., & Løchen, M.-L. (2019). Folkehelserapport: Den sjuende Tromsøundersøkelsen 2015-16 (Report No. 2387-4597). https://septentrio.uit.no/index.php/SapReps/article/view/4862/4678.
- Klein, M., Wobbe-Ribinski, S., Buchholz, A., Nienhaus, A., & Schablon, A. (2018). Nurse-work instability and incidence of sick leave – Results of a prospective study of nurses aged over 40. Journal of Occupational Medicine and Toxicology, 13(1), 31. https://doi.org/10.1186/s12995-018-0212-y
- Krustrup, P., Williams, C., Mohr, M., Hansen, P., Helge, E., Elbe, A. M., … Brito, J. (2018). The “football is medicine” platform – Scientific evidence, large-scale implementation of evidence-based concepts and future perspectives. Scandinavian Journal of Medicine & Science in Sports, 28(S1), 3–7. https://doi.org/10.1111/sms.13220
- Lipsey, M. W., & Wilson, D. B. (1993). The efficacy of psychological, educational, and behavioral treatment. Confirmation from meta-analysis. The American Psychologist, 48(12), 1181–1209. https://doi.org/10.1037//0003-066x.48.12.1181
- Löve, J., Holmgren, K., Torén, K., & Hensing, G. (2012). Can work ability explain the social gradient in sickness absence: A study of a general population in Sweden. BMC Public Health, 12(1), 1–9. https://doi.org/10.1186/1471-2458-12-163
- Melchior, M., Niedhammer, I., Berkman, L., & Goldberg, M. (2003). Do psychosocial work factors and social relations exert independent effects on sickness absence? A six year prospective study of the GAZEL cohort. Journal of Epidemiology & Community Health, 57(4), 285–293. https://doi.org/10.1136/jech.57.4.285
- Oakman, J., Neupane, S., Proper, K. I., Kinsman, N., & Nygård, C.-H. (2018). Workplace interventions to improve work ability: A systematic review and meta-analysis of their effectiveness. Scandinavian Journal of Work, Environment & Health, 44(2), 134–146. https://doi.org/10.5271/sjweh.3685
- Palmlöf, L., Holm, L. W., Alfredsson, L., Magnusson, C., Vingård, E., & Skillgate, E. (2016). The impact of work related physical activity and leisure physical activity on the risk and prognosis of neck pain – A population based cohort study on workers. BMC Musculoskeletal Disorders, 17(1), 219–229. https://doi.org/10.1186/s12891-016-1080-1
- Pereira, M. J., Coombes, B. K., Comans, T. A., & Johnston, V. (2015). The impact of onsite workplace health-enhancing physical activity interventions on worker productivity: A systematic review. Occupational and Environmental Medicine, 72(6), 401–412. https://doi.org/10.1136/oemed-2014-102678
- Petrelli, F., Scuri, S., Tanzi, E., Nguyen, C., & Grappasonni, I. (2018). Public health and burnout: A survey on lifestyle changes among workers in the healthcare sector. Bio-Medica de L'Ateneo Parmense, 90(1), 24–30. https://doi.org/10.23750/abm.v90i1.7626
- Quinn, R. P., Staines, G. L., & McCullough, M. R. (1974). Job satisfaction: Is there a trend? Manpower Research Monograph No. 30: U.S. Department of Labor.
- Roelen, C. A. M., Magerøy, N., van Rhenen, W., Groothoff, J. W., van der Klink, J. J. L., Pallesen, S., Pallesen, S., Bjorvatn, B., & Moen, B. E. (2013). Low job satisfaction does not identify nurses at risk of future sickness absence: Results from a Norwegian cohort study. International Journal of Nursing Studies, 50(3), 366–373. https://doi.org/10.1016/j.ijnurstu.2012.09.012
- Rydström, I., Dalheim Englund, L., Dellve, L., & Ahlstrom, L. (2017). Importance of social capital at the workplace for return to work among women with a history of long-term sick leave: A cohort study. BMC Nursing, 16(1), 38. https://doi.org/10.1186/s12912-017-0234-2
- Stanulewicz, N., Knox, E., Narayanasamy, M., Shivji, N., Khunti, K., & Blake, H. (2020). Effectiveness of lifestyle health promotion interventions for nurses: A systematic review. International Journal of Environmental Research and Public Health, 17(1), 17–52. https://doi.org/10.3390/ijerph17010017
- Sundstrup, E., Seeberg, K. G. V., Bengtsen, E., & Andersen, L. L. (2020). A systematic review of workplace interventions to rehabilitate musculoskeletal disorders among employees with physical demanding work. Journal of Occupational Rehabilitation, 30(4), 588–612. https://doi.org/10.1007/s10926-020-09879-x
- World Health Organization. (2016). Global strategy on human resources for health: Workforce 2030 (Report No. 9241511133). https://apps.who.int/iris/bitstream/handle/10665/250368/?sequence=1