
Plain Language Summary
People affected by a medical disorder, usually called patients, develop a very special expertise by living with it every day. They know, better than anyone else, how it affects their lives, what they go through to get a diagnosis and treatment, how treatments affect them, how symptoms or side effects impact their daily life, and what it is like to interact with the health care system. The people who share their lives, usually close family members like parents, partners, or siblings, develop similar knowledge. When it comes to research, patients are usually seen only as subjects. In the recent National Hemophilia Foundation State of the Science Research Summit and the subsequent National Research Blueprint project, people with inherited bleeding disorders and their family members were invited to participate in creating an agenda of the most important research that needs to be done, and in designing the approach to do the research. As full members of State of the Science Working Groups, and in leadership roles in the National Research Blueprint, they realized they needed a title that recognizes and clearly communicates their unique expertise, so that the people they work with understand what they bring to the table. They chose the term lived experience expert (LEE). Especially in rare disorders, LEEs have unique, valuable expertise to contribute to all stages of research (e.g. planning and designing, participating and recruiting participants, communicating its importance and results). Including LEEs in leadership roles will make research stronger.
1. Introduction
The role of the patient [Citation1] in shared decision-making with their comprehensive care team has been well established in inherited bleeding disorders (BD) [Citation2,Citation3]. In contrast, recognition of patients’ value and expertise in BD research has not been well defined, despite government [Citation4–6] and non-government agencies (especially Patient-Centered Outcomes Research Institute [PCORI]) [Citation7,Citation8] increasingly calling for their input. Individuals with BDs are becoming more involved in research; their contributions should be accorded recognition and respect based on their unique and important perspectives. A title or label for people affected by BDs involved in research that sends a strong message, clearly and concisely conveying their role, is desirable.
In 2020 the National Hemophilia Foundation (NHF), a US patient advocacy organization serving people with BDs, sought to identify the issues of greatest importance to their stakeholders. In addition to health care providers (HCP), researchers, government representatives, and related nonprofit organizations, NHF invited input from people with BDs. Ensuring diverse representation of gender, race and ethnicity, geography, and language, they solicited their brightest vision for the future, irrespective of limiting factors [Citation9]. The results renewed NHF’s focus on research to improve the lives of people affected by BDs.
At the September 2021 State of the Science Research Summit, hosted by NHF and the American Thrombosis and Hemostasis Network (ATHN), the community identified and ranked research priorities important to them [Citation9]. The subsequent effort, developing a US National Research Blueprint for Inherited Bleeding Disorders, seeks to enhance the conduct of research and embrace people-centric principles [Citation10]. It became apparent, through the State of the Science and National Research Blueprint initiatives, that people with BDs and their families are keen to participate in research, but not just as human subjects. They want to engage in all phases of the research process, treated as equals and respected for their expertise. As these initiatives evolved, so did the role of people with BDs and the title they felt most appropriate.
2. The progressive role of people affected by bleeding disorders in research
Six interdisciplinary State of the Science Research Summit working groups (WG) were recruited to determine and prioritize concrete research questions/initiatives to address the top community concerns [Citation11–16]. WGs featured diverse members of the comprehensive care team (e.g. hematologists, nurses, physiotherapists, psychosocial workers, etc.), other medical specialists, researchers from within and beyond the BD community, and representatives of industry, government, and regulatory agencies. Recognizing that people with BDs and their family members acquire unique knowledge and perspectives invaluable to research prioritization, NHF and ATHN recruited several into each WG, as subject matter experts (SME). Designating them SMEs, NHF and ATHN intended to formalize recognition of their expertise [Citation9] and ‘level the playing field’; erase, or at least mitigate, hierarchical barriers impeding open communication and learning; and balance the research power dynamic. NHF and WG co-chairs fostered an environment in which SME input was valued and their participation in all aspects of the prioritization process encouraged. SMEs were full WG members and coauthored resulting publications, leading writing of certain sections [Citation11–16].
Each BD community member brings important expertise to the table; greater diversity of expertise is a richness. Researchers and clinicians offer vast knowledge and experience of the research endeavor; the rigors of the scientific process; and the biology, pathophysiology, etiology, diagnosis, management, etc. of a disorder. While some SMEs also have specialized medical/scientific or other professional expertise, the intimate real-life knowledge of the physical and psychosocial impacts of BDs that they amass is truly unique. They are well positioned to illuminate challenges to accessing the health care system, barriers to prompt and optimal diagnosis and care, and impacts of social determinants of health, disparities, and inequities. SMEs have unique perspectives that even the most genuinely empathetic and engaged clinician/researcher cannot emulate.
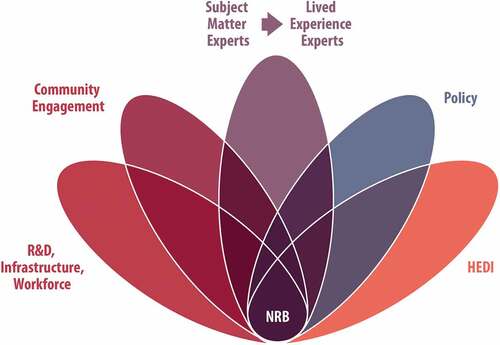
Having established research priorities to address community-identified needs, NHF and ATHN set out to develop a National Research Blueprint with a collaborative infrastructure and workforce, to facilitate and accelerate the prioritized research [Citation10]. This ongoing initiative seeks to improve the current research paradigm by making it more efficient, effective, and collaborative following patient-centered and health equity, diversity, and inclusion (HEDI) principles. The State of the Science Research Summit highlighted the need to integrate SMEs into every aspect of research. From prioritization of research topics to infrastructure and workforce development, governance, funding, design, conduct, and communication; every facet of the research endeavor can benefit from SME leadership. Five new WGs were formed to advance the National Research Blueprint, collaborating tightly with frequent inter-group consultation ().
Figure 1. National Research Blueprint Working GroupsHEDI: health equity, diversity, and inclusion; NRB: National Research Blueprint; R&D: research and development.
3. Evolving self-determination: from SME to LEE
Words are powerful. Titles and labels send messages; they can build relationships and cause confusion and conflict. SME is not a new term, it is commonly defined as someone with an exceptionally deep understanding of a particular subject – such as a process, piece of equipment, software solution, medical specialization, etc [Citation17]. Thus defined, SMEs have usually amassed their knowledge through intensive education or years of professional experience [Citation17].
While people living with BDs undoubtedly develop an exceptionally deep understanding of their disorder, they may not have extensive medical education or related professional experience. People habituated to these connotations may be confused, even skeptical, if they encounter people with BDs as SMEs. Some HCPs and researchers/clinicians may consider themselves or their colleagues to be SMEs and have difficulty equating this term with those they think of as patients. People with BDs interacting with established research stakeholders beyond the NHF State of the Science Research Summit and National Research Blueprint WGs were sometimes burdened with justifying the SME designation or assumed to have advanced medical knowledge they did not. The resulting confusion and, at times, tension, did not always empower contribution of their expertise.
Discussing their experiences, including this tension and confusion, the National Research Blueprint SME WG identified the need for a title to clearly communicate their expertise, requiring no explanations or justification, and avoiding potential resentment or negativity from collaborators. They selected the self-explanatory: lived experience expert (LEE, ). This term plainly and indubitably asserts that their lived experiences constitute a unique expertise. The LEEs claim ownership of this expertise, no more and no less, and hope this term will facilitate collaboration with all stakeholders, garnering respect and equality.
4. LEEs in research leadership
An important progression from constituting a few members of each State of the Science Research Summit WG, LEEs lead and make up an entire National Research Blueprint WG, collaborating closely with the other WGs (), each of which solicit their input. The National Research Blueprint LEE WG has been charged with defining the role of LEEs in BD research, working with the other WGs to ensure they are included in every stage of the research endeavor and that all initiatives and products are enriched with LEE expertise. The National Research Blueprint LEE WG recognizes that NHF and ATHN have previously advocated for the adoption of the term, SME [Citation9,Citation18], and that espousing a different appellation now may cause some confusion. Facilitating clear communication and constructive collaboration is worth the effort required to dispel any confusion. Determining their own title was an important manifestation of empowerment as LEEs step ever more confidently into leadership roles in the National Research Blueprint.
The term ‘lived experience expert’ appears to have similar and current use particularly in consultations regarding experiences with mental health and social services [Citation19–21]. The value of LEE contributions to the design and conduct of kidney disease and juvenile idiopathic arthritis research has recently been recognized [Citation22,Citation23]. LEEs have also coauthored recommendations on mental health care services [Citation24] and co-designed addiction research tools [Citation25]. The authors hope for wide adoption of this term and for all areas of health research, and especially the BD community, to benefit from integrating LEEs into leadership.
Not every LEE may wish, or be able, to take on research leadership roles, nor are they obliged to. Involvement exists on a continuum: from awareness of research and its importance, through research consumption (e.g. discussing findings with HCPs in the context of shared decision-making), and participation in studies, to contributing leadership to research prioritization, design, conduct, communication, etc. LEEs must be invited and enabled to occupy the position on this continuum that is right for them. All research stakeholders (e.g. comprehensive care team professionals, specialized researchers, LEEs) have a responsibility to actively raise LEE awareness of the continuum of opportunities and the importance of engagement. It is essential to meet LEEs where they are, both physically and metaphorically, and empower them to contribute to research. Examples of initiatives to advance these goals include:
Communicating research opportunities and findings to the BD community (e.g. newsletters, webinars, talks at community events)
Facilitating understanding of the research endeavor, medical concepts, and terminology through plain language educational resources, including languages other than English
Providing tools to build confidence speaking to groups or authority figures
Dismantling barriers to participation (e.g. compensation for time off work, scheduling around life commitments such as work and family, meeting in the community rather than an institutional conference room)
Recognizing and challenging personal and institutional biases and power dynamics
Relationships between people with BDs and clinicians/researchers vary widely; authentic engagement and relationships take time to develop. Some collaborators embrace prioritization of LEE perspectives, however systemic adaptation and change is required. All stakeholders must work together to foster open dialogue that values all expertise and be transparent about and disclose any potential conflict of interest. In countries with different societal and cultural norms, significant resource constraints on access to diagnosis/care, and other influencing factors (e.g. demographics, geography, systems of government, public health priorities) the path to empowerment of LEEs in BD research will likely differ to that which we describe [Citation26]. To better understand international perspectives on BD research priorities () and the role of LEEs in research (), readers are invited to contribute to two surveys developed by NHF (Supplementary Tables S1 and S2). Anonymized responses will be collected through a Health Insurance Portability and Accountability Act (HIPAA) compliant, password protected site which stores them on its secure server. Aggregate data may, in the future, be shared through scientific posters, articles, and similar communications.
Figure 2. QR codes linking to ongoing surveys of international perspectives on (A) bleeding disorders research priorities and (B) the role of LEEs in research.
LEE: lived experience expert, QR: quick response
5. Conclusions
The involvement of people with bleeding disorders has evolved with the State of the Science Research Summit and National Research Blueprint conceptualization, elaboration, and operationalization [Citation10]. Lived experience experts (LEE) defined a title that clearly communicates their role and expertise and are increasingly empowered to step into leadership positions within the research endeavor. This progression is not without challenges; all stakeholders must continue to invest in relationship building and open receptive dialogue to design and conduct the most effective and meaningful research together. Particularly in rare disorders, LEEs have invaluable expertise to contribute at all stages of the research endeavor.
Abbreviations
Declaration of interest
M Kim declares payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educations events from Speaker, Takeda La Voz Group; leadership or fiduciary roles in other board, society, committee or advocacy group paid or unpaid from BioMarin North American Patient Advocacy Forum, BioMarin US Patient Advocacy Panel. ME Santaella is an employee of NHF.
The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Reviewer disclosures
Peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
Acknowledgments
The Executive Committee of the National Hemophilia Foundation National Research Blueprint initiative were actively engaged in the conception, design, preparation, and oversight of each of the State of the Science manuscripts in this supplement. Maria E. Santaella actively engaged with the lived experience expert (LEE) WG members throughout the process, empowering their inclusion and participation. The Executive Committee consisted of: Kevin Mills, Michael Recht, Michelle L. Witkop, Maria E. Santaella, Donna DiMichele, Keri L. Norris, Esmeralda Vázquez and Brett Spitale.
The authors wish to thank the members of the National Research Blueprint Subject Matter Expert/Lived Experience Expert Working Group for their collaboration in selecting the term lived experience expert (LEE): Erin Cirelli, Kyle Davis, Patricia DeRatto, Michael Glenzer, Regina Legere, Andrew Park, Ray Stanhope, Sammie Valadez, and Esmeralda Vázquez.
The authors also acknowledge Fiona Robinson, PhD, for providing professional medical writing support during manuscript development paid for by NHF, and Matt Evans for the creation of professional medical illustrations, paid for by NHF.
Additional information
Funding
References
- Karazivan P, Dumez V, Flora L, et al. The patient-as-partner approach in health care: a conceptual framework for a necessary transition. Acad Med. 2015;90(4):437–441.
- Baker JR, Crudder SO, Riske B, et al. A model for a regional system of care to promote the health and well-being of people with rare chronic genetic disorders. Am J Public Health. 2005;95(11):1910–1916.
- Hermans C, Noone D, Benson G, et al. Hemophilia treatment in 2021: choosing the”optimal” treatment using an integrative, patient-oriented approach to shared decision-making between patients and clinicians. Blood Rev. 2022;52:100890.
- National Institutes of Health. NIH clinical center patient handbook [cited 2022 Dec 11]. Available from: https://clinicalcenter.nih.gov/sites/nihinternet/files/internet-files/participate/_pdf/pthandbook.pdf.
- U.S. Food and Drug Administration. FDA patient engagement overview [cited 2022 Dec 13]. Available from: https://www.fda.gov/patients/learn-about-fda-patient-engagement/fda-patient-engagement-overview.
- National Institute for Health and Care Excellence. Nominating patient experts: a factsheet for patient and carer organisations [cited 2022 Nov 16]. Available from: https://www.nice.org.uk/Media/Default/About/NICE-Communities/Public-involvement/Developing-NICE-guidance/Nominating-Patient-Experts.pdf.
- Institute for Clinical and Economic Review. Our patient engagement program [cited 2022 Dec 13]. Available from: https://icer.org/our-approach/methods-process/patient-engagement/.
- Patient-Centered Outcomes Research Institute. The patient-centered outcomes research institute strategic plan: generating evidence to achieve more efficient, effective, and equitable health care and improve health for all 2022. [cited 2022 Dec 13]. Available from: https://www.pcori.org/sites/default/files/PCORI-Strategic-Plan.pdf.
- Valentino LA, Witkop ML, Santaella ME, et al. Building the blueprint: formulating a community-generated national plan for future research in inherited bleeding disorders. Haemophilia. 2022;28(5):760–768.
- Valentino LA, Witkop ML, Santaella ME, et al. The National Hemophilia Foundation State of the Science Research Summit initiative: executive summary. Expert Rev Hematol. 2023;16(S1):129–134. DOI: 10.1080/17474086.2023.2181782.
- Baldwin MK, Ahmadzia HK, Bartlett DL, et al. Building the foundation for a community-generated national research blueprint for inherited bleeding disorders: research to advance the health of people with inherited bleeding disorders with the potential to menstruate. Expert Rev Hematol. 2023;16(S1):71–86. DOI: 10.1080/17474086.2023.2175660.
- Byams VR, Baker JR, Bailey C, et al. Building the foundation for a community-generated national research blueprint for inherited bleeding disorders: research priorities in health services; diversity, equity, and inclusion; and implementation science. Expert Rev Hematol. 2023;16(S1):87–106. DOI: 10.1080/17474086.2023.2183836.
- Nugent D, Acharya SS, Baumann KJ, et al. Building the foundation for a community-generated national research blueprint for inherited bleeding disorders: research priorities for ultra-rare inherited bleeding disorders. Expert Rev Hematol. 2023;16(S1):55–70. DOI: 10.1080/17474086.2023.2175661.
- Ragni MV, Young G, Batsuli G, et al. Building the foundation for a community-generated national research blueprint for inherited bleeding disorders: facilitating research through infrastructure, workforce, resources and funding. Expert Rev Hematol. 2023;16(S1):107–127. DOI: 10.1080/17474086.2023.2181781.
- Sidonio RF Jr., Bryant PC, Di Paola J, et al. Building the foundation for a community-generated national research blueprint for inherited bleeding disorders: research priorities for mucocutaneous bleeding disorders. Expert Rev Hematol. 2023;16(S1):39–54. DOI: 10.1080/17474086.2023.2171983.
- Tran DQ, Benson CC, Boice JA, et al. Building the foundation for a community-generated national research blueprint for inherited bleeding disorders: research priorities to transform the care of people with hemophilia. Expert Rev Hematol. 2023;16(S1):19–37. DOI: 10.1080/17474086.2023.2171981.
- iSixSigma. An overview: what are subject matter experts (SMEs)? [cited 2022 Dec 13]. Available from: https://www.isixsigma.com/dictionary/subject-matter-expert-sme/.
- Robinson F, Wilkes S, Schafer N, et al. Patient-centered pharmacovigilance: priority actions from the inherited bleeding disorders community. Ther Adv Drug Saf. 2023;14:1–23.
- Scottish Government. Getting involved in designing the National Care Service [cited 2022 Dec 13]. Available from: https://www.gov.scot/publications/getting-involved-designing-national-care-service-easy-read/pages/2/.
- Huron Perth Public Health. Lived experience expert panel [cited 2022 Dec 13]. Available from: https://www.hpph.ca/en/partners-and-professionals/lived-experience-expert-panel.aspx.
- British Institute of Human Rights. Lived experience experts [cited 2022 Dec 13]. Available from: https://www.bihr.org.uk/our-work/lived-experience/our-lived-experience-experts.
- University of Calgary. UCalgary researchers lead international program to develop value framework on socioeconomic impact of living with rare disease [cited 2022 Dec 27]. Available from: https://educationnewscanada.com/article/education/level/university/1/948599/ucalgary-researchers-lead-international-program-to-develop-value-framework-on-socioeconomic-impact-of-living-with-rare-disease.html.
- Kidney Foundation. Bringing people together in a time of need - Kidney Foundation 2021 impact report [cited 2022 Dec 27]. Available from: https://issuu.com/kidney/docs/kidney-foundation-impact-and-research-report-2021-?e=1151137/92025185.
- Hopkins L, Saraf S, Foster A. Establishing Recovery Colleges in mental healthcare services: a Royal Commission recommendation. Aust N Z J Psychiatry. 2023;57(1):17–20.
- McCabe J, Wilcock M, Atkinson K, et al. General practitioners’ and psychiatrists’ attitudes towards antidepressant withdrawal. BJPsych Open. 2020;6(4):e64.
- Witkop ML, Robinson F, DiMichele D. Soliciting international perspectives on an American national research agenda for inherited bleeding disorders. Exp Rev Hem. 2023;16(S1):13–17. DOI: 10.1080/17474086.2023.2178411.