
ABSTRACT
Stochastic distribution methods were used to construct patient flow simulation sub-models such as patient inflow, length of stay (LoS), cost of treatment (CoT) and clinical pathways (CPs). However, the patient inflow rate demonstrates seasonality, trend, and variation due to natural and human-made factors. LoS, CoT and CPs are determined by social-demographics factors, clinical and laboratory test results, resource availability and healthcare structure. For this reason, patient flow simulation models developed using stochastic methods have limitations including uncertainty, not recognising patient heterogeneity, and not representing personalised and value-based healthcare. This, in turn, results in a low acceptance level and implementation of solutions suggested by patient flow simulation models. On the other hand, machine learning becomes effective in predicting patient inflow, LoS, CoT, and CPs. This paper, therefore, describes why coupling machine learning with patient flow simulation is important, proposes a conceptual architecture for machine learning integrated patient flow simulation and demonstrates its implementation with examples.
1. Introduction
Computer simulation has been applied to model and analyse patient flow into and within an existing or a proposed healthcare system (German Anatoli, Citation2013; Gualandi et al., Citation2019; Kreindler, Citation2017) from a clinical and/or operational perspectives (Côté, Citation2000) in a single or multiple units/departments.
Patient flow analysis supports decision-making in healthcare services and operations management (Monks et al., Citation2016) by reducing the probability of failure, achieving specifications, eradicating unpredicted bottlenecks, preventing under or over-utilisation of resources, decreasing overcrowding, and improving clinical pathways and healthcare system performance (Maria & Anu, Citation1997). Discrete-event simulation (DES), agent-based simulation (ABS) and system dynamics (SD) are the main types of patient flow simulation methods (Gunal, Citation2012).
Stochastic distribution methods, such as discrete and continuous distributions, have been used to build DES of patient flow components/sub-models such as patient inflow, length of stay (LoS), cost of treatment (CoT) and clinical pathways (CPs) models. However, patients’ inter-arrival rate exhibits seasonality and trend, changes over time (Nas & Koyuncu, Citation2019) due to natural and human-made factors. Besides, LoS, CoT and CP are significantly determined by a patient’s attributes, clinical and laboratory test results, previous history, accessibility of resources and organisational structure of a healthcare institute (Bramkamp et al., Citation2007; Noohi et al., Citation2020; Siddiqui et al., Citation2018; W. Zhang et al., Citation2010). For this reason, traditional patient flow simulation models are criticised for ignoring heterogeneity (Zaric, Citation2003). As a result, the credibility, acceptance, and implementation of the findings from patient flow simulations have been low. Mohiuddin et al. (Citation2017) mentioned that only a few simulation studies (n = 3; 14%) report the implementation of the proposed changes.
According to Nas and Koyuncu (Citation2019), the adoption of different sources and types of data and advanced methods for modelling components of patient flow simulation is important because stochastic distributions do not allow consideration of different characteristics and/or data of patient flow.
Electronic health records (EHR) (Ambinder, Citation2005) have been producing big data that can be used to construct data-driven clinical and/or operational decision support tools that help to model, analyse, predict and manage healthcare processes (El-Bouri et al., Citation2021).
Machine learning (ML) (Ngiam & Khor, Citation2019), using EHR as an input, has been widely used to analyse, discover patterns and predict demand for healthcare (Asheim et al., Citation2019; Hong et al., Citation2018; Luo et al., Citation2017), LoS (Al Taleb et al., Citation2017; Daghistani et al., Citation2019), CoT (Bremer et al., Citation2018; Jödicke et al., Citation2019), and CP (Allen et al., Citation2019; Funkner et al., Citation2017; Kovalchuk et al., Citation2018; Prokofyeva & Zaytsev, Citation2020), to mention a few.
This paper, hence, aims to 1) describe why coupling machine learning with patient flow simulation is important, 2) propose a conceptual architecture/model for constructing machine learning integrated patient flow simulation, and 3) provide a proof of concept by demonstrating its implementation with examples.
The proposed architecture aims to increase the credibility and acceptance of patient flow simulation models by reducing uncertainties and improving the accuracy of patient flow simulation models. Furthermore, the proposed solution fosters personalised and value-based healthcare as it promotes individual-patient-based healthcare instead of a “one-model-fits-all” approach. This, in turn, will improve the acceptance level of patient flow simulation models among healthcare administrators and thereby increase the implementation of solutions proposed by patient flow simulation models.
The rest of the paper is organised as follows: Section 2 discusses related works; Section 3 elaborates why machine learning integrated patient flow simulation is important; Section 4 describes methods used; Section 5 illustrates the conceptual model of machine learning integrated patient flow simulation followed by its implementation with an example in Section 6, and Section 7 presents the conclusions of our work.
2. Related works
Several studies have employed computer simulation methods for modelling and analysing patient flow in a single department or multiple departments of a hospital. Santibáñez et al. (Citation2009) used simulation to analyse the simultaneous impact of operations, scheduling, and resource allocation on patient wait time, clinic overtime, and resource utilisation in the ambulatory care unit. Konrad et al. (Citation2013) studied the impact of changing patient flow processes in ED using DES. Hurwitz et al. (Citation2014) developed a flexible simulation platform to quantify and manage emergency department crowding. Cocke et al. (Citation2016) conducted a simulation study of patient flows in the ED at the University of Virginia under alternative demand scenarios, staffing levels, and operating practices. Antonelli et al. (Citation2014) employed a simulation-based analysis of patient flow in elective surgery. Schoenfelder et al. (Citation2021) implemented a simulation model to evaluate an operating room management policy. Azari-Rad et al. (Citation2014) employed DES to model the perioperative process in the general surgery service, aiming to reduce the number of surgical cancellations and thereby improve the overall process. Christensen (Citation2012) tried to improve ICU patient flow through discrete-event simulation.
On the other hand, Abuhay et al. (Citation2016) illustrated a simulation of patient flow and load of multiple departments in a specialised medical centre using DES. Suhaimi et al. (Citation2018) built a DES model for modelling multiple outpatient orthopaedic clinics. Bosbach et al. (Citation2021); Bovim et al. (Citation2021); and Tavakoli et al. (Citation2022) investigated simulation of COVID-19 patient flow process and predicted the future entry of patients in a hospital as a case study. Garcia-Vicuña et al. (Citation2022) assessed the preparedness of a hospital during COVID-19 epidemics using simulation.
These studies, however, used stochastic distribution methods, to construct sub-models such as patient inflow, LoS, waiting time, CoT and CP models. To minimise the uncertainties and improve the accuracy of traditional patient flow simulation, data-driven methods were proposed. For example, Kovalchuk et al. (Citation2018) studied process and data mining techniques for model identification to develop simulation models of patient flow in multiple healthcare units. ML was applied to identify classes of clinical pathways, capturing rare events and variations in patients. Nas and Koyuncu (Citation2019) proposed an ED capacity planning tool using a Recurrent Neural Network (RNN) and simulation. The outcomes of the ML model, hourly patient arrival rate prediction, were used as input. Abuhay et al. (Citation2020a, Citation2020b) implemented complex network analysis to study the collaboration of departments and identify the most important ones to develop holistic patient flow simulation using system thinking. Nevertheless, these studies inadequately described why machine learning integrated patient flow simulation is important. Nor did they propose an architecture that shows how to couple machine learning with patient flow simulation and demonstrate the concept with examples. Hence, this study aims to fill this gap.
3. Methods used
This study was conducted following a mixed (conceptual and empirical) research design approach. The conceptual research design (Mishra & Alok, Citation2017) was employed to investigate weaknesses of the existing patient flow simulation models from data and methodological perspectives, assess why machine learning integrated patient flow simulation is important and propose a conceptual model. The empirical research design (Jasti & Kodali, Citation2014) was then used to prove the proposed conceptual framework with examples. Secondary data which was collected from the Almazov National Medical Research Centre,Footnote1 Saint Petersburg, Russia was employed and data pre-processing methods such as missing value handling methods (median for numerical values, maximum for categorical values), first-order differencing to maintain the stationarity of the time series data, Searching for Uncorrelated List of Variables algorithm and Recursive XGBoost (Seshadri, Citation2020) for feature engineering, standard scaler to normalise data, and a combination of Tomek Link and SMOTE (Swana et al., Citation2022) to handle class imbalance, were applied to make the dataset suitable for machine learning algorithms.
A holistic patient flow simulation model that was developed by Abuhay et al. (Citation2020a) for the Almazov National Medical Research Centre was adopted in this study. To develop the model, Abuhay et al. (Citation2020a) used system thinking, complex network/graph analysis (Tabassum et al., Citation2018), DES (Gunal, Citation2012), probability law/transition matrices, Poisson distribution (Banks, Citation2005), Kernel Density Estimation (KDE) (Y.-C. Chen, Citation2017), First Come First Served (FCFS) queueing theory, data and face validation and a Python module called SimPy,Footnote2 process-based discrete-event simulation framework based on standard Python. Processes in SimPy are defined by Python generator functions and may, for example, be used to model active components like customers, vehicles or agents. SimPy also provides various types of shared resources to model limited capacity congestion points (like servers, checkout counters and tunnels).
Machine learning algorithms, namely Auto-Regressive Integrated Moving Averages (ARIMA), Prophet, and eXtreme Gradient Boosting (XGBoost), were employed to develop patient inflow and length of stay prediction models which were later integrated with the patient flow simulation. The performance of the machine learning models was evaluated using MAE, and accuracy.
4. Why machine learning integrated patient flow simulation?
A holistic patient flow simulation model generally contains two main sub-models: a patient inflow simulation model and an in-hospital patient flow simulation model. The first sub-model simulates patients’ arrival at a specific department of a hospital in hourly, daily, weekly, or monthly periods. Discrete stochastic distribution methods, mainly Poisson distribution (Banks, Citation2005), have been used to develop the patient arrival rate simulation model. However, patient inflow or inter-arrival rate reveals seasonality, nonlinear trend, and association with time (Nas & Koyuncu, Citation2019; Y. Zhang et al., Citation2020).
Patient flows to a hospital are also affected by both natural and human-made factors such as pandemics/epidemics (COVID-19, Ebola, Zika) and disasters (war, civil unrest, flood, train, car and plane accidents). Hong et al. (Citation2018) also showed that the inclusion of patient history and information (e.g., previous healthcare usage statistics, past medical history, labs and vitals, prior imaging counts, and outpatient medications, and demographic details such as insurance and employment status) significantly improved patient inflow prediction performance. This makes modelling patients’ admission rates using stochastic distributions difficult because stochastic distributions, e.g., Poisson distribution, do not allow taking different factors into account.
The second sub-model, which is an in-hospital patient flow simulation model, mimics the movement of patients through multiple departments/units. This model has sub-models such as LoS, CoT and CP prediction models.
LoS and CoT have been used as a surrogate to evaluate the utilisation of resources, quality and efficiency of care, patient experience, and capacity planning in a hospital (Papi et al., Citation2016; Verburg et al., Citation2014). Both LoS and CoT prediction sub-models are usually developed using univariate density estimation methods such as Lognormal, Weibull, and Gamma. As the probability distribution of both LoS and CoT is positively skewed, multi-modal and significantly varies between diagnosis-related groups (DRGs), none of these methods seemed to fit satisfactorily in a wide variety of samples (Houthooft et al., Citation2015; Ickowicz et al., Citation2016; Lee et al., Citation2001).
Besides, LoS, and CoT are significantly determined by a patient’s attributes such as age, gender, comorbidity, genomic makeup, clinical and laboratory test results, previous history, availability of resources and structure of a healthcare institute (Bramkamp et al., Citation2007; Noohi et al., Citation2020; Siddiqui et al., Citation2018; W. Zhang et al., Citation2010). These attributes determine how a given patient responds to a given set of circumstances such as timing and resource demand (Karnon et al., Citation2012). For this reason, patient flow simulation models are criticised for ignoring heterogeneity (Zaric, Citation2003). As a result, their contribution to personalised medicine (Schleidgen et al., Citation2013) and value-based healthcare (Brown, Citation2005; Traoré et al., Citation2019) is limited as both concepts promote individual-patient-based healthcare with high-quality, low cost and wide access instead of a “one-model-fits-all” approach.
Another sub-model of an in-hospital patient flow simulation is a CP prediction model. CPs specify trajectories of care that need to be conducted for a group of patients until they are discharged from a hospital (Aspland et al., Citation2019). CPs have been generally modelled using transition matrices based on probability law. However, patient in-hospital flow is a very complex process due to dissimilar and multiphase pathways and the innate uncertainty and variability of care processes due to patients’ attributes and their previous history. Karnon et al. (Citation2012) mentioned that the types of past events influence the likelihood and timing of subsequent events. CPs identification and prediction also involve the analysis of comprehensive patient information (Aspland et al., Citation2019; Kovalchuk et al., Citation2018) which cannot be achieved with transaction matrices.
On top of this, there is significant uncertainty in the patient flow simulation models due to a lack of consistency, completeness, and correctness of medical data (Morquin & Ologeanu-Taddei, Citation2016), low coverage of rare cases with CPs (Huang et al., Citation2012), and weak formalisation and high uncertainty in core medical knowledge (Mandrola, Citation2015). This, in combination with methods (using stochastic distribution methods) of patient flow simulation construction, reduces decision makers’ confidence in the validity of patient flow simulations and so impacts the acceptance and implementation of the findings from patient flow simulations. This is made evident with underreporting of the implementation of changes/solutions proposed by simulation models. Mohiuddin et al. (Citation2017) mentioned that only a few studies (n = 3; 14%) report the implementation of the proposed changes.
5. Conceptual model of machine learning integrated patient flow simulation
A conceptual model is a non-software-specific description of a computer simulation model that describes the objectives, inputs, outputs, content, assumptions, and simplifications of the model (Robinson, Citation2008a, Citation2008b, Citation2013, 2017). We formally describe the proposed model using STRESS guidelines (Allen et al., Citation2019) in this section and section 6.
Our conceptual model, see , shows potential inputs (sources and types of data), data integration and pre-processing tasks, types and applications of machine learning algorithms used to construct components of holistic patient flow simulation, outputs (ML models) and how the ML models can be integrated with patient flow simulation.
Figure 1. The conceptual model of machine learning integrated patient flow simulation.
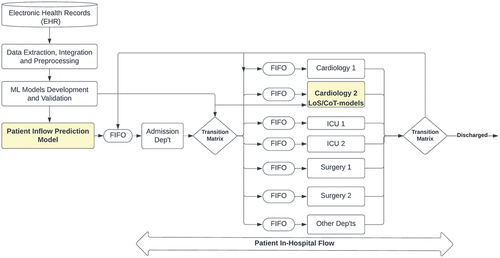
The main aim of the study is to demonstrate the importance and feasibility of machine learning-integrated patient flow simulation, the output is a machine learning-integrated patient flow simulation model, in particular, ML-based prediction models were developed for patient inflow and LoS sub-models, and the experiment aims to compare machine learning-integrated patient flow simulation with the traditional patient flow simulation models which were developed using stochastic distribution methods.
In this model, the entities are ACS patients that move from one department to another department over time to get healthcare which can be considered as activities. The movement of the patients across departments is governed by transition matrices, see . Patients access limited resources (departments) based on a first come first served queuing theory. The admission department is the entry point which is modelled as a time series problem using a machine learning method and the patient flow simulation terminates (patient discharges) at one of the departments based on the transition matrices.
Table 1. Transition matrices.
Input data (patient inter-arrival rate, LoS, CoT, attributes of patients, clinical and laboratory test results, and clinical pathways) were extracted from the EHR. Third-party data, such as weather, demographic, pandemic, disaster and other data, can also be integrated with the EHR which enables us to develop a data-driven patient flow simulation (Ambinder, Citation2005).
Data integration and pre-processing tasks (such as handling missing data, outliers, resampling, removing trends and seasonality, data standardization/normalisation and features engineering) were applied to make the data suitable for ML algorithms.
Instead of modelling patient inflow using stochastic distributions (Poisson distribution), it was formulated as a time series problem and modelled using ML algorithms for times series analysis and prediction (Frank et al., Citation2001). As a result, the seasonality and trend of patient inflow might be captured and different factors affecting patient flow to a hospital can be also considered.
Patient inflow can be modelled as univariate or multivariate data. In the case of modelling patient inflow as univariate data, hourly, daily, weekly, monthly, or yearly number of patient admission will be extracted and used as input. Patient inter-arrival rate (hourly, daily, weekly, monthly, or yearly) can also be integrated with third-party data and used as input to model patient inflow as multivariate data. In the case of multivariate modelling, the inputs will be a date (date of a week, month in a year, and year, season) and different factors (e.g., weather, demography, pandemic, natural and/or human-made disaster and other data) and the output will be the number of patients in each period.
Y. Zhang et al. (Citation2020) and Khaldi et al. (Citation2019), for example, forecasted weekly patient visits to ED by combining Artificial Neural Networks (ANNs) with an Ensemble Empirical Mode Decomposition (EEMD). Seven years of univariate time series data of weekly demand was collected from ED and the models were evaluated using root mean square error (RMSE), mean absolute error (MAE) and correlation coefficient (R).
In our proposed solution, the ML-based patient inflow prediction model serves as a starting point for the patient flow simulation process and as a tool to assess future demands for emergency care. The ML-based patient inflow prediction model can also be developed for each department so that healthcare demand and supply will be analysed, forecasted, and managed at the department or operational level.
As we have discussed in Section 4, different factors affect LoS, CoT and CP. Formulating LoS and CoT as a regression (Angelini, Citation2019) or multi-class classification (Pillay and Nyathi, Citation2021) problem allows consideration of different determinate factors, such as characteristics of patients, clinical, physical and laboratory tests results and co-morbidities, while predicting LoS and CoT.
Linear and nonlinear models can be used to model and predict LoS. Muhlestein et al. (Citation2019), for instance, trained 29 ML algorithms, on 26 preoperative variables, to predict LoS of patients with a brain tumour. The root mean square logarithmic error (RMSLE) was applied to evaluate the performance of the model. Mekhaldi et al. (Citation2020) also compared two ML methods, the Random Forest (RF) and the Gradient Boosting model (GB), to predict LoS based on an open-source dataset and the Mean Square Error (MSE), the R-squared (R2) and the Adjusted R-squared (Adjusted R2) metrics were used to evaluate the performance of the models. The same approach can also be applied to develop a CoT prediction model, as both LoS and CoT demonstrate similar behaviour.
Clinical pathways or patient trajectories analysis and prediction can be formulated as a clustering (Al-Jabery et al., Citation2020) or classification (disposition prediction) problem. Goto et al. (Citation2018), for example, investigated machine-learning approaches for predicting the disposition of asthma and Chronic obstructive pulmonary disease (COPD) exacerbations in the ED. Kovalchuk et al. (Citation2018) also employed ML to identify classes of clinical pathways and captured rare events and variations in patients. Prokofyeva and Zaytsev (Citation2020) analysed clinical pathways in medical institutions using hard and fuzzy clustering methods and public data. Allen et al. (Citation2019) also proposed data-driven modelling of clinical pathways using EHR to cluster patients into groups based on their movements/clinical pathways during their stay in the hospital.
A separate ML-based LoS, CoT, and CPs prediction models should be developed and integrated with each department because different clinical procedures require different LoS and CoT (Abuhay et al., Citation2020a). So that demand and supply can be analysed, forecasted, and managed at an operational level.
To attach/integrated ML-based prediction models to each department/healthcare service in the in-hospital patient flow simulation, a generator (de Brito et al., Citation2015) of patient characteristics was constructed using continuous and/or discrete probability functions based on the data type of the patient’s characteristics. The next section discusses building and validating our proposed model.
6. Constructing machine learning integrated patient flow simulation
6.1. Model development
This section provides a proof of concept for constructing a machine learning integrated patient flow simulation by presenting a case study. To this end, anonymised data about Acute Coronary Syndrome (ACS) patients were extracted from the EHR of the Almazov National Medical Research Centre,Footnote3 Saint Petersburg, Russia. These data contain information about ACS patients’ inter-arrival rate, characteristics, clinical, laboratory and physical test results, and the start and end date and time of each diagnosis and treatment process.
A holistic patient flow simulation model (Abuhay., Citation2020a) that was constructed for the Almazov National Medical Research Centre was adopted in this study. To develop the model, Abuhayet al. (Citation2020a) used:
Complex network/graph analysis to study the interaction of hospital departments and identify the most important ones (see ) in the diagnosis and treatment process of ACS patients.
Seven years, from 2010 to 2016, event log data that describes the movement of 24,902 ACS patients from department to department with the associated timestamp, LoS, and CoT were used. A directed and weighted network of 227 departments with 4305 edges was constructed using Gephi.Footnote4
The analysis result shows that both degree and weighted degree distributions are positively skewed and the average degree and weighted degree account for 19 and 5800, respectively. The result also shows that the Laboratory department, Functional Diagnostic department, Cardiology departments, Surgery departments and Intensive Care Unit (ICU) departments are receiving more requests from other departments as well as sending more results to other departments. In other words, these departments are significant in giving support to and influencing the function of other departments during the diagnosis and treatment processes of ACS patients. These departments are also fundamental in connecting communities of departments as they have high betweenness and closeness centrality.
Finally, the results were validated by domain experts at Almazov National Medical Research Centre, and the domain experts suggested considering the admission department, two cardiology departments, two ICU departments and two surgery departments for constructing a holistic patient flow simulation. To consider the impact of other departments, the rest of the departments were also modelled as one department.,
DES to construct a holistic (multiple departments) patient flow simulation model, which was implemented using SimPy.
Transition matrices to govern the movement of ACS patients from one department to another department. Each row of the transition matrices sums to 1 and was extracted from the event log data, see . The relationship among departments is either one way or two ways represented by one or two directional arrows, see .,
The Poisson distribution to develop a patient inflow prediction model,
Kernel density estimation (KDE) to build LoS and CoT prediction models,
First come first served (FCFS) queueing theory to manage patients’ access to limited resources/departments,
Data and face validation to validate the model, and
SimPyFootnote5 module, a process-based DES framework based on standard Python, for simulation model development. Processes in SimPy are defined by Python generator functions and may, for example, be used to model active components like customers, vehicles, or agents. SimPy also provides various types of shared resources to model limited capacity congestion points (like servers, checkout counters and tunnels).
To test the concept of integrating machine learning with patient flow simulation, this study, hence, modified the model of Abuhay et al. (Citation2020a) by constructing ML-based models to predict patient inflow and LoS, see yellow-coloured rectangles in .
A monthly patient inflow prediction model for the admission department and LoS prediction model for the cardiology1 department were developed as follows. Seventy-six months (1/1/2010–31/04/2016) dataset of 10,661 ACS patients were extracted from the admission department, which is the entry point to the hospital and serves as a starting point of our patient flow simulation model. The mean monthly patient visits account for 140, see for basic statistics of the monthly patient inflow. The autocorrelation coefficient of monthly patient inflow is equal to 0.898 which shows that monthly patient inflows are highly correlated and predictable (see ).
Figure 2. Monthly patient inflow trend and autocorrelation results.
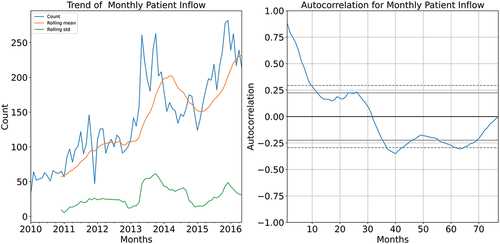
Table 2. BasIc statistic of monthly patient inflow.
As the monthly patient inflow demonstrates significant autocorrelation (see ), Auto-Regressive Integrated Moving Averages (ARIMA) and Prophet were selected for developing a prediction model. ProphetFootnote6 is an open-source software for forecasting time series data based on an additive model where non-linear trends are fit with yearly, weekly, and daily seasonality, plus holiday effects. The dataset was divided into training (the first 72 months) and testing (the last four months) datasets.
To determine the tuning parameters (p, d, q) of the ARIMA model, pmdarima,Footnote7 which is an AutoML framework for the ARIMA model, was applied. It automatically identifies the most optimal p, d, and q parameters and returns a fitted ARIMA model. The hyperparameters of Prophet were also tuned using Optuna,Footnote8 an open-source hyperparameter optimisation framework.
A dataset about LoS of 2412 ACS patients was extracted from the Cardiology1 department. The dataset contains information about patients’ age, gender, and results of several laboratory tests, see for basic statistics of each attribute and LoS. We considered only features/data that were taken at the time of admission to the Caradiology1 department meaningful; subsequent tests that were taken during patients’ stay in the department were not considered while developing the LoS prediction model.
Table 3. Basic statistics of los and predicting features (except gender).
The dataset was pre-processed using different methods to make it suitable for classification algorithms. We modelled the LoS as a classification problem. Missing values of each attribute were replaced with the median value for numerical features and the maximum count for categorical features. Besides, the average value was calculated for similar laboratory test measures such as 1) Bilirubin, Bilirubin Straight and Bilirubin Indirect, 2) AP-High and AP-Low, 3) Acid-base analysis true base excess and Acid-base analysis pHv, 4) Prothrombin (according to Quick) and Prothrombin and 5) Cholesterol, VLDL Cholesterol and HDL Cholesterol. This means that 12 attributes were removed and replaced with the 5 attributes containing mean results. As a result, 28 attributes were left for further use, see .
Then the LoS data were binned into four bins/classes (0–15 days, 15–30 days, 30–40 days, and >40 days) based on the distribution of the dataset. The class imbalance was treated using a combination of Tomek Link and SMOTE (Swana et al., Citation2022) because oversampling performs better than under-sampling for different classifiers (Mohammed et al., Citation2020; Swana et al., Citation2022). Finally, the data were randomly divided into training and testing sets based on an 80/20 ratio.
An eXtreme Gradient Boosting (XGBoost) algorithm, which is an implementation of a generalised gradient boosted decision trees algorithm with state-of-the-art performance on classification, regression and ranking tasks (Chen & Guestrin, Citation2016), was implemented to develop a LoS prediction model. The hyperparameters of XGBoost were tuned using Optuna. Both models were developed using scikit-learnFootnote9 which is a machine learning library/module for the Python programming language.
6.2. Model validation
The fine-tuned ARIMA (order = (2, 1, 0)) scores a Mean Absolute Error (MAE) of 48, whereas the Prophet (with changepoint_prior_scale = 0.3, holidays_prior_scale = 0.4,seasonality_mode=“additive”, daily_seasonality=True, yearly_seasonality=True, holidays = holiday (list of Russian holidays during the time frame of the study data)) scores an MAE of 12.25 to predict a monthly patient inflow. As a result, the monthly patient inflow prediction model developed with Prophet was selected.
Then the best-performing patient inflow prediction model was integrated with the traditional patient flow simulation model and the performance was measured by comparing its results with the Poisson distribution model. i.e., we have two patient flow simulation models −1) a traditional patient flow simulation model developed using Poisson probability distribution and 2) our proposed model developed using ML. The comparative analysis is presented here below.
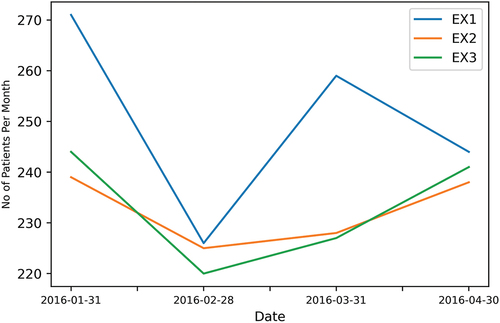
The Poisson distribution-based patient inflow prediction model was developed based on the number of patients (958) who visited the admission department in the last four months, from January 1 2016 to May 1 2016 which is equal to 120 days (i.e., 172,800 minutes, which was calculated as 120 days in four months × 24 hours of in a day × 60 minutes in an hour). This means that the patients arrive every 180.4 minutes (172800 minutes/958 patients in five months) on average. The model’s run time was four months (the timeframe of testing data) or 172800 minutes. The model was run three times (EX1, E×2 and E×3) to control randomness and the average of the three experiments is reported in and .
Figure 3. Comparison of inflow prediction results from traditional and the new simulation model.
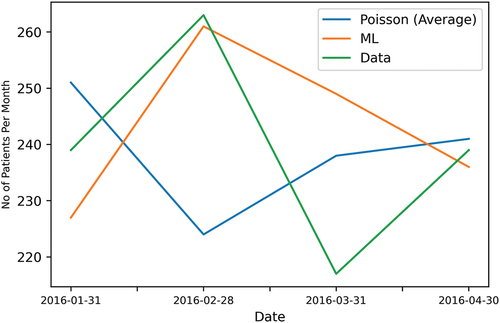
Table 4. Comparison of inflow prediction results from traditional and the new simulation model.
and present the results of both models as compared to the real data. As a result, the ML-based patient flow prediction model outperforms the Poisson distribution model which has been widely used to develop the traditional patient flow simulation model. The mean absolute error of the ML-based model is 12.25, whereas the Poisson distribution model scores an MAE of 18.5, see and . This means that our ML-based patient inflow model improved the accuracy of the traditional patient flow simulation by 34%.
Besides, the Poisson model exhibits variability over three experiments, see and , which affects the credibility of patient flow simulation models and made evident that using ML is better and more reliable. We believe that more data size and modelling the patient inflow prediction as multivariate data, with additional features about different factors that may affect patient inflow, will further improve the performance of the ML model.
Figure 4. Variability of Poisson distribution experiment results.
The LoS prediction model (with n_estimators = 71, max_depth = 36, learning_rate = 0.06, subsample = 0.78, colsample_bytree = 0.80) scores an accuracy of 76%. Then this model was saved (serialized/pickled) using Joblib,Footnote10 a set of tools that provide lightweight pipelining in Python (we used the same method for our inflow prediction model). The saved model was imported/loaded and integrated with the adopted patient flow simulation model to predict patients’ LoS in the Cardiology1 department. To predict the LoS using the ML model, generators of patient characteristics were developed using probability distribution methods, KDE for continuous data and discrete probability for discrete data (e.g., gender). Then two models (the traditional patient flow simulation which was developed using discrete probability distribution and our new model) were run concurrently for one year period, and a comparison analysis is performed, see and . The reason we modelled the LoS using discrete probability distribution in the traditional simulation model is to make it comparable with our ML-based LoS prediction model which was formulated as a multiclass (4 classes) classification problem.
Figure 5. Comparison of LoS prediction results from traditional and the new simulation model.
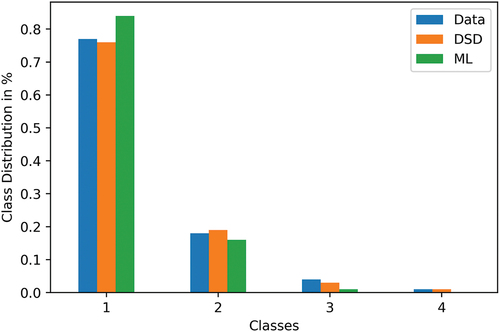
Table 5. Comparison of LoS prediction results from traditional and the new simulation model.
As a result, the ML-based LoS prediction model with 76% accuracy produced a promising result with an MAE of 0.035, whereas the discrete probability model scored 0.002 MAE. As the ML performance mainly depends on the size of the training dataset, we believe that more data will further improve the prediction accuracy of the proposed model.
The results show that ML can be used to develop sub-models of patient flow simulation and produced realistic results which, in turn, fosters value-based and personalised healthcare and improve the confidence of decision-makers in the findings of patient flow simulation models. However, constructing machine learning integrated patient flow simulation requires well-preprocessed and more data, time, and effort.
7. Conclusion
Traditional statistical methods such as stochastic distribution (discrete and continuous) methods have been used to construct sub-models (e.g., patient inflow, Length of Stay (LoS), Cost of Treatment (CoT) and clinical pathways models) of the patient flow simulation model. However, patients’ admission data demonstrate seasonality, trend, and variation over time. LoS, CoT and clinical pathways are also significantly determined by a patient’s attributes such as age, gender, comorbidity, genomic makeup, and clinical and laboratory test results. For this reason, patient flow simulation models have been criticised for ignoring heterogeneity which makes their contribution to personalised medicine and value-based healthcare limited. On the other hand, machine learning methods have proven to be efficient to study and predict patients’ admission rate, bed capacity, LoS, CoT, and clinical pathways.
In this paper, hence, the weaknesses of current patient flow simulation model development trends and the reason why machine learning integrated patient flow simulation is important are discussed in detail. A conceptual framework that shows how to integrate machine learning with patient flow simulation is proposed. The framework illustrates sources of data, components of the proposed model, and potential methods that can be used to develop the components of the proposed model based on STRESS guidelines. Finally, case studies were conducted to prove the proposed model with examples. As a result, our proposed model improved the accuracy of traditional patient flow simulation by 34%.
Acknowledgments
The authors thank Almazov National Medical Research Centre (Saint Petersburg, Russia) for providing the anonymized data for this study.
Disclosure statement
No potential conflict of interest was reported by the authors.
Notes
References
- Abuhay, T. M., Krikunov, A. V., Bolgova, E. V., Ratova, L. G., & Kovalchuk, S. V. (2016). Simulation of patient flow and load of departments in a specialized medical center. Procedia computer science, 101, 143–151. https://doi.org/10.1016/j.procs.2016.11.018
- Abuhay, T. M., Mamuye, A. L., Robinson, S. L., & Kovalchuk, S. V. (2021). Why machine learning integrated patient flow simulation? The Operational Research Society Simulation Workshop 2021 (SW21), 22–26 March 2021, Online, (pp. 375–384). https://www.theorsociety.com/media/5897/sw21-proceedings.pdf
- Abuhay, T. M., Metsker, O. G., Yakovlev, A. N., & Kovalchuk, S. V. (2020a). Constructing holistic patient flow simulation using system approach. In Computational Science – ICCS 2020 (Vol. 12140, pp. 418–429). Nature Publishing Group. https://doi.org/10.1007/978-3-030-50423-6_31
- Abuhay, T. M., Nigatie, Y. G., Metsker, O. G., Yakovlev, A. N., & Kovalchuk, S. V. (2020b). Investigating coordination of hospital departments in delivering healthcare for acute coronary syndrome patients using data-driven network analysis. In Computational Science – ICCS 2020 (Vol. 12140, pp. 430–440). Nature Publishing Group. https://doi.org/10.1007/978-3-030-50423-6_32
- Al-Jabery, K. K., Obafemi-Ajayi, T., Olbricht, G. R., & Wunsch, D. C., II. (2020). Clustering algorithms. Computational Learning Approaches to Data Analytics in Biomedical Applications, 29–100. https://doi.org/10.1016/B978-0-12-814482-4.00003-6
- Allen, M. (2019). Can clinical audits be enhanced by pathway simulation and machine learning? An example from the acute stroke pathway. British Medical Journal Open, 9(9), e028296. https://doi.org/10.1136/bmjopen-2018-028296
- Al Taleb, A. R., Hoque, M., Hasanat, A., & Khan, M. B. (2017). Application of data mining techniques to predict length of stay of stroke patients. In 2017 International Conference on Informatics, Health and Technology, ICIHT 2017, 21–23 Feb 2017, Riyadh, Saudi Arabia. (pp. 1–5). Institute of Electrical and Electronics Engineers Inc. https://ieeexplore.ieee.org/document/7899004
- Ambinder, E. P. (2005). ElecTronic health records. Journal of Oncology Practice, 1(2), 57–63. https://doi.org/10.1200/jop.2005.1.2.57
- Angelini, C. (2019). Regression Analysis. Encyclopedia of Bioinformatics and Computational Biology: ABC of Bioinformatics, 1–3, 722–730. https://doi.org/10.1016/B978-0-12-809633-8.20360-9
- Antonelli, D., Bruno, G., & Taurino, T. (2014). Simulation-based analysis of patient flow in elective surgery. In Proceedings of the International Conference on Health Care Systems Engineering, May 22 and 24, 2013, Milan, Italy. (Vol. 61, pp. 87–97). Springer Cham. https://doi.org/10.1007/978-3-319-01848-5
- Ardabili, S. F. (2020). COVID-19 outbreak prediction with machine learning. Algorithms, 13(10), 249. https://doi.org/10.3390/a13100249
- Asheim, A., Bache-Wiig Bjørnsen, L. P., Næss-Pleym, L. E., Uleberg, O., Dale, J., & Nilsen, S. M. (2019). Real-time forecasting of emergency department arrivals using prehospital data. BMC Emergency Medicine, 19(1), 42. https://doi.org/10.1186/s12873-019-0256-z
- Aspland, E., Gartner, D., & Harper, P. (2019). Clinical pathway modelling: A literature review. Health Systems, 10(1), 1–23. https://doi.org/10.1080/20476965.2019.1652547
- Azari-Rad, S., Yontef, A., Aleman, D. M., & Urbach, D. R. (2014). A simulation model for perioperative process improvement. Operations Research for Health Care, 3(1), 22–30. https://doi.org/10.1016/j.orhc.2013.12.003
- Banks, J. (2005). Prentice-Hall International Series in Industrial and Systems Engineering. Discrete-event system simulation (Fourth). Retrieved from 03 March 2020 http://syndetics.com/index.php?isbn=0131293427/lc.jpg&client=brlibt&type=xw12
- Bosbach, W. A., Heinrich, M., Kolisch, R., & Heiss, C. (2021). Maximization of open hospital capacity under shortage of sars-cov-2 vaccines—an open access, stochastic simulation tool. Vaccines, 9(6), 546. https://doi.org/10.3390/VACCINES9060546
- Bovim, T. R., Gullhav, A. N., Andersson, H., Dale, J., & Karlsen, K. (2021). Simulating emergency patient flow during the COVID-19 pandemic. Journal of Simulation, 1–15. https://doi.org/10.1080/17477778.2021.2015259
- Bramkamp, M., Radovanovic, D., Erne, P., & Szucs, T. D. (2007). Determinants of costs and the length of stay in acute coronary syndromes: A real life analysis of more than 10 000 patients. Cardiovascular Drugs and Therapy, 21(5), 389–398. https://doi.org/10.1007/s10557-007-6044-0
- Bremer, V., Becker, D., Kolovos, S., Funk, B., Van Breda, W., Hoogendoorn, M., & Riper, H. (2018). Predicting therapy success and costs for personalized treatment recommendations using baseline characteristics: Data-driven analysis. Journal of Medical Internet Research, 20(8), e10275. https://doi.org/10.2196/10275
- Brockwell, P. J. (2010). Time series analysis. In International Encyclopedia of Education (pp. 474–481). Elsevier Ltd. https://doi.org/10.1016/B978-0-08-044894-7.01372-5
- Brown, G. (2005). Value-based medicine: The new paradigm. Current Opinion in Ophthalmology, 16(3), 139–140. https://doi.org/10.097/01.icu.0000164165.17432.ae
- Chen, Y.-C. (2017). A Tutorial on Kernel Density Estimation and Recent Advances. http://arxiv.org/abs/1704.03924
- Chen, T., & Guestrin, C. (2016). Xgboost: A scalable tree boosting system. Proceedings of the ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 13-17-August-2016, (pp. 785–794). https://doi.org/10.1145/2939672.2939785
- Christensen, B. A. (2012). Improving ICU patient flow through discrete-event simulation. Massachusetts Institute of Technology. Retrieved from 21 December 2020 https://dspace.mit.edu/handle/1721.1/73436#files-area
- Cocke, S. (2016). UVA emergency department patient flow simulation and analysis. 2016 IEEE Systems and Information Engineering Design Symposium (SIEDS), Charlottesville, VA, USA, (pp. 118–123). https://doi.org/10.1109/SIEDS.2016.7489282
- Côté, M. J. (2000). Understanding patient flow. Decision Line. Retrieved from 27 October 2020 http://web.uvic.ca/~h351/hinf351_course_data/Cote
- Daghistani, T. A., Elshawi, R., Sakr, S., Ahmed, A. M., Al-Thwayee, A., & Al-Mallah, M. H. (2019). Predictors of in-hospital length of stay among cardiac patients: A machine learning approach. International Journal of Cardiology, 288, 140–147. https://doi.org/10.1016/j.ijcard.2019.01.046
- de Brito, C. C. R., Rêgo, L. C., & de Oliveira, W. R. (2015). Method for generating distributions and classes of probability distributions: the univariate case. Hacettepe Journal of Mathematics and Statistics, 48(3), 897–930. https://doi.org/10.15672/hjms.2018.619
- El-Bouri, R., Taylor, T., Youssef, A., Zhu, T., & Clifton, D. A. (2021). Machine learning in patient flow: A review. Progress in Biomedical Engineering, 3(2), 022002. https://doi.org/10.1088/2516-1091/ABDDC5
- Frank, R. J., Davey, N., & Hunt, S. P. (2001). TiMe series prediction and neural networks. Journal of Intelligent & Robotic Systems, 31(1/3), 91–103. https://doi.org/10.1023/A:1012074215150
- Funkner, A. A., Yakovlev, A. N., & Kovalchuk, S. V. (2017). Data-driven modeling of clinical pathways using electronic health records. In Procedia computer science (Vol. 121, pp. 835–842). Elsevier B.V. https://doi.org/10.1016/j.procs.2017.11.108
- Garcia-Vicuña, D., Esparza, L., & Mallor, F. (2022). Hospital preparedness during epidemics using simulation: The case of COVID-19. Central European Journal of Operations Research, 30(1), 213–249. https://doi.org/10.1007/s10100-021-00779-w
- German Anatoli, D. R. (2013). Prospective healthcare decision-making by combined system dynamics, discrete-event and agent-based simulation. In Proceedings of the 2013 Winter Simulation Conference, December 8–11, Washington D.C., USA. (pp. 270–281). https://ieeexplore.ieee.org/document/6721426
- Goto, T., Camargo, C. A., Faridi, M. K., Yun, B. J., & Hasegawa, K. (2018). Machine learning approaches for predicting disposition of asthma and COPD exacerbations in the ED. The American Journal of Emergency Medicine, 36(9), 1650–1654. https://doi.org/10.1016/J.AJEM.2018.06.062
- Gualandi, R., Masella, C., & Tartaglini, D. (2019). Improving hospital patient flow: A systematic review. In Business process management journal. Emerald Group Publishing Ltd. https://doi.org/10.1108/BPMJ-10-2017-0265
- Gunal, M. M. (2012). A guide for building hospital simulation models. Health Systems, 1(1), 17–25. https://doi.org/10.1057/hs.2012.8
- Hong, W. S., Haimovich, A. D., & Taylor, R. A. (2018). Predicting hospital admission at emergency department triage using machine learning. PLos One, 13(7), 1–13. https://doi.org/10.1371/journal.pone.0201016
- Hoot, N. R., LeBlanc, L. J., Jones, I., Levin, S. R., Zhou, C., Gadd, C. S., & Aronsky, D. (2009). Forecasting emergency department crowding: A prospective, real-time evaluation. Journal of the American Medical Informatics Association: JAMIA, 16(3), 338–345. https://doi.org/10.1197/JAMIA.M2772
- Houthooft, R. (2015). Predictive modelling of survival and length of stay in critically ill patients using sequential organ failure scores. Artificial Intelligence in Medicine, 63(3), 191–207. https://doi.org/10.1016/J.ARTMED.2014.12.009
- Huang, Z., Lu, X., & Duan, H. (2012). On mining clinical pathway patterns from medical behaviors. Artificial Intelligence in Medicine, 56(1), 35–50. https://doi.org/10.1016/J.ARTMED.2012.06.002
- Hurwitz, J. E., Lee, J. A., Lopiano, K. K., McKinley, S. A., Keesling, J., & Tyndall, J. A. (2014). A flexible simulation platform to quantify and manage emergency department crowding. BMC Medical Informatics & Decision Making, 14(1), 50. https://doi.org/10.1186/1472-6947-14-50
- Ickowicz, A., Sparks, R., & Wiley, J. (2016). Modelling hospital length of stay using convolutive mixtures distributions. Statistics in Medicine, 36(1), 122–135. https://doi.org/10.1002/sim.7135
- Jasti, N. V. K., & Kodali, R. (2014). A literature review of empirical research methodology in lean manufacturing. International Journal of Operations & Production Management, 34(8), 1080–1122. https://doi.org/10.1108/IJOPM-04-2012-0169
- Jödicke, A. M. (2019). Prediction of health care expenditure increase: How does pharmacotherapy contribute? BMC Health Services Research, 19(1), 953. https://doi.org/10.1186/s12913-019-4616-x
- Karnon, J., Stahl, J., Brennan, A., Caro, J. J., Mar, J., & Möller, J. (2012). MoDeling using discrete event simulation: A Report of the ISPOR-SMDM modeling good research practices task force-4. Value in Health, 15(6), 821–827. https://doi.org/10.1016/J.JVAL.2012.04.013
- Khaldi, R., Afia, A. E., & Chiheb, R. (2019). Forecasting of weekly patient visits to emergency department: Real case study. In ProCedia computer science (Vol. 148, pp. 532–541). Elsevier B.V. https://doi.org/10.1016/j.procs.2019.01.026
- Konrad, R., DeSotto, K., Grocela, A., McAuley, P., Wang, J., Lyons, J., & Bruin, M. (2013). Modeling the impact of changing patient flow processes in an emergency department: Insights from a computer simulation study. Operations Research for Health Care, 2(4), 66–74. https://doi.org/10.1016/j.orhc.2013.04.001
- Kovalchuk, S. V., Funkner, A. A., Metsker, O. G., & Yakovlev, A. N. (2018). Simulation of patient flow in multiple healthcare units using process and data mining techniques for model identification. Journal of Biomedical Informatics, 82, 128–142. https://doi.org/10.1016/j.jbi.2018.05.004
- Kreindler, S. A. (2017). The three paradoxes of patient flow: An explanatory case study. BMC Health Services Research, 17(1), 481. https://doi.org/10.1186/s12913-017-2416-8
- Lee, A. H., Ng, A. S. K., & Yau, K. K. W. (2001). Determinants of maternity length of stay: A Gamma mixture risk-adjusted model. Health Care Management Science, 4(4), 249–255. https://doi.org/10.1023/A:1011810326113
- Liashchynskyi, P., & Liashchynskyi, P. (2019). Grid search, random search, genetic algorithm: A big comparison for NAS. arXiv preprint. https://doi.org/10.48550/arXiv.1912.06059
- Luo, L., Luo, L., Zhang, X., & He, X. (2017). Hospital daily outpatient visits forecasting using a combinatorial model based on ARIMA and SES models. BMC Health Services Research, 17(1), 469. https://doi.org/10.1186/s12913-017-2407-9
- Mandrola, J. (2015, August 19). Doctor doesn’t always know best Discloures. Retrieved January 16, 2022, from https://www.medscape.com/viewarticle/849689
- Maria, A., & Anu. (1997). Introduction to modeling and simulation. In Proceedings of the 29th conference on Winter simulation - WSC ’97 (pp. 7–13). December 7–10, 1997, New York, New York, USA: ACM Press. https://doi.org/10.1145/268437.268440
- Mekhaldi, R. N., Caulier, P., Chaabane, S., Chraibi, A., & Piechowiak, S. (2020). UsiNg machine learning models to predict the length of stay in a hospital setting. In Advances in Intelligent Systems and Computing (Vol. 1159, pp. 202–211). AISC. https://doi.org/10.1007/978-3-030-45688-7_21
- Mishra, S. B., & Alok, S. (2017). Handbook of research methodology. https://www.researchgate.net/publication/319207471
- Mohammed, R., Rawashdeh, J., & Abdullah, M. (2020). Machine learning with oversampling and undersampling techniques: Overview study and experimental results. 2020 11th International Conference on Information and Communication Systems, ICICS 2020, 07–09 April, Irbid, Jordan, 243–248. https://doi.org/10.1109/ICICS49469.2020.239556
- Mohiuddin, S. (2017). Patient flow within UK emergency departments: A systematic review of the use of computer simulation modelling methods. British Medical Journal Open, 7(5), e015007. https://doi.org/10.1136/BMJOPEN-2016-015007
- Monks, T., Worthington, D., Allen, M., Pitt, M., Stein, K., & James, M. (2016). A modelling tool for capacity planning in acute and community stroke services. BMC Health Services Research, 16(1), 1–8. https://doi.org/10.1186/s12913-016-1789-4
- Morquin, D., & Ologeanu-Taddei, R. (2016). Professional facing coercive work formalization: Vicious circle of the Electronic Medical Record (EMR) implementation and appropriation. Retrieved from 23 September 2020 https://hal.archives-ouvertes.fr/hal-02138238
- Muhlestein, W. E., Akagi, D. S., Davies, J. M., & Chambless, L. B. (2019). Predicting inpatient length of stay after brain tumor surgery: DeveloPing machine learning ensembles to improve predictive performance. Clinical Neurosurgery, 85(3), 384–393. https://doi.org/10.1093/neuros/nyy343
- Nas, S., & Koyuncu, M. (2019). Emergency department capacity planning: A recurrent neural network and simulation approach. Computational & Mathematical Methods in Medicine, 2019, 1–13. https://doi.org/10.1155/2019/4359719
- Nau, R. (2020). Data transformations and forecasting models: What to use and when, Duke University. Retrieved January 16, 2022, from https://people.duke.edu/~rnau/whatuse.htm
- Ngiam, K. Y., & Khor, I. W. (2019). Big data and machine learning algorithms for health-care delivery. In The lancet oncology. Lancet Publishing Group. May, 1. https://doi.org/10.1016/S1470-2045(19)30149-4.
- Noohi, S., Kalantari, S., Hasanvandi, S., & Elikaei, M. (2020). Determinants of length of stay in a psychiatric ward: A retrospective chart review. The Psychiatric Quarterly, 91(2), 273–287. https://doi.org/10.1007/s11126-019-09699-0
- Papi, M., Pontecorvi, L., & Setola, R. (2016). A new model for the length of stay of hospital patients. Health Care Management Science, 19(1), 58–65. https://doi.org/10.1007/s10729-014-9288-9
- Pillay, N., & Nyathi, T. (2021). Automated Design of Classification Algorithms. Natural Computing Series, 171–184. https://doi.org/10.1007/978-3-030-72069-8_10
- Prokofyeva, E., & Zaytsev, R. (2020). Clinical pathways analysis of patients in medical institutions based on hard and fuzzy clustering methods. Business Informatics, 14(1), 19–31. https://doi.org/10.17323/2587-814x.2020.1.19.31
- Ram, S. (2020). GitHub - AutoViML/featurewiz: Use advanced feature engineering strategies and select the best features from your data set fast with a single line of code. https://github.com/AutoViML/featurewiz
- Robinson, S. (2008a). Conceptual modelling for simulation part I: Definition and requirements. The Journal of the Operational Research Society, 59(3), 278–290. https://doi.org/10.1057/PALGRAVE.JORS.2602368
- Robinson, S. (2008b). Conceptual modelling for simulation part II: A framework for conceptual modelling. The Journal of the Operational Research Society, 59(3), 291–304. https://doi.org/10.1057/PALGRAVE.JORS.2602369
- Robinson, S. (2013). Conceptual modeling for simulation. Winter Simulation Conference, 08–11 December, Washington, DC, USA, (pp. 377–388). https://doi.org/10.1109/WSC.2013.6721435
- Santibáñez, P., Chow, V. S., French, J., Puterman, M. L., & Tyldesley, S. (2009). Reducing patient wait times and improving resource utilization at British Columbia cancer agency’s ambulatory care unit through simulation. Health Care Management Science, 12(4), 392–407. https://doi.org/10.1007/s10729-009-9103-1
- Schleidgen, S., Klingler, C., Bertram, T., Rogowski, W. H., & Marckmann, G. (2013). What is personalized medicine: Sharpening a vague term based on a systematic literature review. BMC Medical Ethics, 14(1), 55. https://doi.org/10.1186/1472-6939-14-55
- Schoenfelder, J., Kohl, S., Glaser, M., McRae, S., Brunner, J. O., & Koperna, T. (2021). Simulation-based evaluation of operating room management policies. BMC Health Services Research, 21(1), 1–13. https://doi.org/10.1186/s12913-021-06234-5
- Siddiqui, N., Dwyer, M., Stankovich, J., Peterson, G., Greenfield, D., Si, L., & Kinsman, L. (2018). Hospital length of stay variation and comorbidity of mental illness: A retrospective study of five common chronic medical conditions. BMC Health Services Research, 18(1), 498. https://doi.org/10.1186/s12913-018-3316-2
- Suhaimi, N., Vahdat, V., & Griffin, J. (2018). Building a flexible simulation model for modeling multiple outpatient orthopedic clinics. In 2018 Winter Simulation Conference (WSC), December 9–12, Gothenburg, Sweden. (pp. 2612–2623). IEEE. https://doi.org/10.1109/WSC.2018.8632451
- Swana, E. F. ;, Doorsamy, W. ;, Bokoro, P. T., Link, S., Fezeka Swana, E., Doorsamy, W., & Bokoro, P. (2022). Tomek link and SMOTE approaches for machine fault classification with an imbalanced dataset. Sensors 2022, 22(9), 3246. https://doi.org/10.3390/S22093246
- Tabassum, S., Pereira, F. S. F., Fernandes, S., & Gama, J. (2018). Social network analysis: An overview. Wiley Interdisciplinary Reviews. Data Mining and Knowledge Discovery, 8(5), 1–21. https://doi.org/10.1002/widm.1256
- Tavakoli, M., Tavakkoli-Moghaddam, R., Mesbahi, R., Ghanavati-Nejad, M., & Tajally, A. (2022). Simulation of the COVID-19 patient flow and investigation of the future patient arrival using a time-series prediction model: A real-case study. Medical & Biological Engineering & Computing, 60(4), 969–990. https://doi.org/10.1007/s11517-022-02525-z
- Traoré, M. K., Zacharewicz, G., Duboz, R., & Zeigler, B. (2019). Modeling and simulation framework for value-based healthcare systems. SIMULATION, 95(6), 481–497. https://doi.org/10.1177/0037549718776765
- Verburg, I. W. M., Keizer, N. F. D., Jonge, E. D., Peek, N., & Salluh, J. I. F. (2014). Comparison of Regression Methods for Modeling Intensive Care Length of Stay, 9(10), 9(10. https://doi.org/10.1371/journal.pone.0109684
- Zaric, G. S. (2003). The impact of ignoring population heterogeneity when Markov models are used in cost-effectiveness analysis. Medical Decision Making, 23(5), 379–386. https://doi.org/10.1177/0272989X03256883
- Zhang, W., Emrich, S., & Zeng, E. (2010). A two-stage machine learning approach for pathway analysis. In Proceedings - 2010 IEEE International Conference on Bioinformatics and Biomedicine, BIBM 2010, 18–21 December, Hong Kong, China. (pp. 274–279). https://doi.org/10.1109/BIBM.2010.5706576
- Zhang, Y., Luo, L., Zhang, F., Kong, R., Yang, J., Feng, Y., & Guo, H. (2020). Emergency patient flow forecasting in the radiology department. Health Informatics Journal, 26(4), 146045822090188. https://doi.org/10.1177/1460458220901889
