
ABSTRACT
This paper presents results from a simulation case study analyzing care strategies for elderly patients in a regional healthcare system (HCS) in Sweden. Three strategies to reduce emergency visits, hospitalisations, and stays were evaluated: care coordinators at emergency departments, mobile health clinics visiting fragile patients in their homes, and proactive primary care. Using system dynamics modelling and empirical data, the impact on the regional HCS was explored considering the reduced care demand and demographic changes. Subsequently, the impact on the population's health status was assessed. Combining strategies yielded the best outcome, but improving patients' health status may increase long-term care demand. The study emphasizes the importance of implementing these strategies to offer better care for elderly patients and reduce healthcare costs. Findings highlight the potential long-term effects of improving health status and the need for a comprehensive approach to address the evolving care demands of an ageing population.
1. Introduction
Decision-makers are always challenged to make the best decisions or apply the best policies to improve or design their organisations. In healthcare, these decisions are focused on offering high-quality care, providing good service times, and still being resource-efficient (Goienetxea Uriarte et al., Citation2017; Larisch et al., Citation2016), while designing systems that will be sustainable in the future (Lyons & Duggan, Citation2015). This is not an easy task, especially considering that healthcare systems (HCS) are characterised by having many interdependencies between different stakeholders and processes, being self-organising and having emergent behaviour, having time lags, feedback loops, non-linearity, and at the same time being path-dependent (Lipsitz, Citation2012). Moreover, each patient is unique and the required services as well as the time spent in a specific part of the HCS will be dependent on the individual’s health status (Penny et al., Citation2022). Additionally, the expected demographic changes, and especially the rise in life expectancy, will make this task even more difficult as the demand for healthcare and the economic pressure on healthcare providers is expected to increase. According to the United Nations (Citation2017), the actual world population aged 60 years or over will be doubled by 2050 and according to Lindgren (Citation2016), the rates of chronic diseases and multimorbidity will also increase in elderly patients.
The healthcare infrastructure can be defined by different factors (Lyons & Duggan, Citation2015): 1) exogenous factors associated with population dynamics (demographics, lifestyle, etc.); and 2) internal decision variables associated with policy measurements as well as the development of the healthcare services to respond to the existing demand by the exogenous factors. This paper takes into account some exogenous factors and their impact on the elderly population dynamics, yet the main focus is on internal system variables to analyse different policies to offer better care for elderly patients (65 years or older), to support minimising the care they require from the emergency departments (ED) and the subsequent hospitalisations and days staying at the hospital. Offering timely and effective care for these patients proactively, e.g., via primary care (PC), can even reduce the need for reactive care in form of unnecessary hospitalisations and the complications that are associated with hospitalising these fragile patients (Boyd et al., Citation2008). At the same time, a reduction in unnecessary visits to the ED can even contribute to reducing overcrowding and the long waiting times that characterise EDs all over the world (El-Zoghby et al., Citation2016). A key aspect when defining policies or making decisions is to have a clear understanding of the problem at hand. Therefore, it is vital to obtain knowledge about the system’s behaviour and the impact that improvements may have before any decisions are taken (Slack & Lewis, Citation2011). There are different operations management and operational research methods and tools that can support healthcare policymakers to make better decisions. While approaches like Lean, Six Sigma or Business Process Re-engineering are extensively implemented to support the improvement of HCSs (Radnor, Citation2010), their inherent trial and error approach makes them limited to tackling the complexity of HCSs. Operational research and management sciences methods, such as simulation, heuristics, Markov processes, mathematical programming, or queueing theory (Hulshof et al., Citation2012), can offer a better foundation for decision-making by modelling the problem and trying to find the optimal solution for it (Anderson et al., Citation2002).
Simulation is one of the most used techniques within operations research (Hillier & Lieberman, Citation2015). Studies employing simulation to support HCS design and improvement have been reviewed by several authors (S. C. Brailsford et al., Citation2009; Katsaliaki & Mustafee, Citation2011; Mielczarek & Uziałko-Mydlikowska, Citation2012; Salleh et al., Citation2017). Although there are different simulation paradigms, when the problem under study has a dynamic nature, as is the case in the presented study, and an understanding of different interconnections between the various parts involved in the system is needed, System Dynamics (SD) is an appropriate tool (Linnéusson et al., Citation2018). SD enables multiple testing of scenarios to reach the objectives and question own mental models, and at the same time, question the assumptions and values governing the system (Senge & Sterman, Citation1992). Additionally, it also provides the possibility to analyse policy-level and strategic decisions (Vanderby et al., Citation2015). Several authors have reviewed the use of SD in healthcare (Cassidy et al., Citation2019; Chang et al., Citation2017; Kunc et al., Citation2018), and defended the need for a systems thinking perspective to analyse HCSs (De Savigny et al., Citation2017), as well as studied how to restructure HCSs via SD (Homer & Hirsch, Citation2006; Mitropoulos et al., Citation2022), or applied it for resource planning and policy development in HCS via SD (Faeghi et al., Citation2021; Vanderby et al., Citation2015). In the review by Cassidy et al. (Citation2019), an analysis of different healthcare settings modelled using SD is presented, these being cardiology care, elderly care or long-term care services, emergency or acute care, hospital waste management, accountable care organisation and health insurance schemes, maternal, and child health, as well as orthopaedic care. Among the articles identified by the authors, several applied SD to reduce visits to EDs using policies that target specifically elderly patients (Cassidy et al., Citation2019). One of those, presented by Ansah et al. (Citation2014), explored different policies to manage the long-term care of elderly patients. They identified that policymakers should pose attention to expanding long-term care services instead of building more capacity in the EDs to provide better care and reduce ED overcrowding. Similarly, S. Brailsford et al. (Citation2004) concludes in her study that the total occupancy of hospital beds could be reduced significantly by offering care to elderly patients in more appropriate services than the ED, such as those offered by community care facilities. Desai et al. (Citation2008) investigate with SD the future demand for social care services from elderly people and present an approach to reduce ED visits by offering care packages to those with critical needs as well as improving home care services rather than residential care.
This paper presents the results of a study using SD to analyse and evaluate closer care policies for elderly patients, including elderly with multimorbidity and frequent attender (FA) behaviour, to offer better care and at the same time reduce the number of unnecessary visits to the ED and the overall cost for the HCS. Additionally, the paper also reflects upon some challenges encountered during the study that may be useful for simulation practitioners.
The article is structured as follows: Section 2 presents the background, problem context, and the main objectives of this study; Section 3 describes the method in detail and describes why SD was a suitable approach; Section 7.1 presents a simplified causal loop diagram (CLD) over the dynamics of elderly patients seeking care in the HCS; Section 4 describes the developed SD model and the tested scenarios; Section 5 presents an extended analysis of the SD model to investigate how the health status of elderly patients may be impacted; Section 6 discusses and reflects on the study and its results; finally, Section 7 reveals the conclusions.
2. Background
The Swedish region of Västra Götaland (VGR) has defined a strategy to transition the HCS to meet the challenges of an increasingly older population (Västra Götalandsregionen, Citation2018). One initiative to tackle this challenge is to offer closer care to patients, meaning that the care often needed in the first instance should be provided closer to the patient (e.g., primary care, home care, etc.) and outside the EDs. Some of the main motivations are to decrease existing waiting times, queues, and rising costs for hospitals, but most importantly to increase the quality of the care provided (Taylor & Dangerfield, Citation2005). However, the lack of coordination and availability, as well as a reactive and non-person-centred focus which usually has characterised PC, has influenced the behaviour of patients that prefer to go to the ED, sometimes unnecessarily, contributing therefore to the ED overcrowding (Moskop et al., Citation2009).
Due to their continuous care need, elderly patients require a considerable amount of visits to the ED and they also count for a high number of hospitalisations (LaCalle & Rabin, Citation2010). According to data from 2016, elderly people (65 or older) in VGR were around 320.000. Of these, around 14% were patients with multimorbidity, and around 1,56% of them were FA in the ED, which means that they visited the ED at least four times in one year (the most common definition of FA, according to LaCalle and Rabin (Citation2010)). These types of patients have considerably higher rates of visits to the ED, hospitalisations, and length of stay at the hospital compared to non-elderly patients. These variables are especially high when analysing elderly multimorbidity patients, who also count for the highest avoidable hospitalisation rates (15%) and have a high probability of revisiting the ED within a month.
An important input to this study has been knowledge from previous successful pilot projects in the region including (Kjellström et al., Citation2019): 1) the introduction of care coordinators in the ED to coordinate the care offered to elderly patients in the different instances of the HCS; 2) the use of mobile health clinics to visit unstable patients or those in need for palliative care at home; and 3) proactive care provided in the PC facilities. These pilot cases showed that the introduction of care coordinators helped reduce the amount of time the patients were waiting in the ED, reduced the number of patients being hospitalised, and reduced considerably the number of patients returning to the ED within a month. Regarding mobile health clinics, they reported positive results with a higher quality of care, high-continuity, person-centred care, as well as a reduction in the visits to the ED, and the number of days being hospitalised. Finally, the proactive care offered in PC implied that visits were pre-booked systematically and more time was assigned to physicians and nurses to meet and treat elderly patients. This proved to reduce 20% of the visits to the ED, minimising, in consequence, the number of hospitalisations.
Consequently, the main objectives of this study were 1) to analyse and model the dynamics of elderly patients’ care-seeking behaviour using CLD; 2) to simulate how the results of pilot closer care actions could impact the overall HCS of the region considering aspects such as the number of visits in the ED, hospitalisations, and the corresponding cost savings; and 3) to demonstrate for the regional healthcare board the possibilities of using simulation for decision-making support.
3. Research design
The study was conducted in Sweden and the analysis focused on the data obtained from the HCS of the region of Västra Götaland. Different stakeholders were involved in different ways during the simulation model-building process. These can be divided into three main groups: 1) the modelling team, who developed the simulation model and carried out the investigations and data collection; 2) the regional healthcare board, the decision-makers and customers of the simulation model results; and 3) experts from primary and specialist care interviewed during the study.
The modelling team consisted of six persons, three were from the Department of data management and analysis with knowledge in statistics, data analytics, and logistics. A fourth member was a senior physician with expert knowledge of the studied regional HCS and its improvement initiatives, and she was also a member of the regional healthcare board. The team was completed with two researchers from the university with expertise in discrete-event (DES) and system dynamics (SD) simulation due to enabling either approach to be evaluated in the initial discussions and study buy-in step described in . Furthermore, a wide group of people from primary and specialist care with different knowledge and expertise were interviewed to get knowledge and information about the system under study. The result of the modelling project was reported to the regional healthcare board (the decision-makers) who were also involved at specific points in time to provide feedback on the process.
Table 1. The overall method for the modelling case.
Table 2. Description of the scenarios tested in the model.
Table 3. Overview of approximate effects from the closer care strategies to key parameters. Updated from Linnéusson and Goienetxea Uriarte (Citation2021).
The overall method to conduct the study included multiple steps described in and are also graphically represented in Linnéusson and Goienetxea Uriarte (Citation2021). The knowledge obtained about the problem under study increased greatly after each step in the iterative process represented in , which needed to be redefined several times based on new information or knowledge gained during the process.
The problem formulation, setting of objectives, and model conceptualisation steps consumed most of the time from the study, leaving less time for experimentation.
4. Understanding the dynamics of elderly patients in the healthcare system
Multiple aspects were considered important to represent the care-seeking behaviour of elderly patients. These were included in a CLD to visualise the causal relations and feedback loops leading to the reinforcement of the pressure that elderly population visits add to the EDs.
A description of the complete resulting CLD can be found in Linnéusson and Goienetxea Uriarte (Citation2021). However, below in , a simplified version of the CLD is depicted including two central feedback loops: one reinforcing feedback loop detailing the care-seeking behaviour of elderly patients at the EDs, Reactive and acute care, and one balancing feedback loop detailing the desired proactive care by rerouting patients through PC instead, Proactive and preventive care.
Figure 1. Simplified CLD over elderly patients’ care-seeking behaviour.
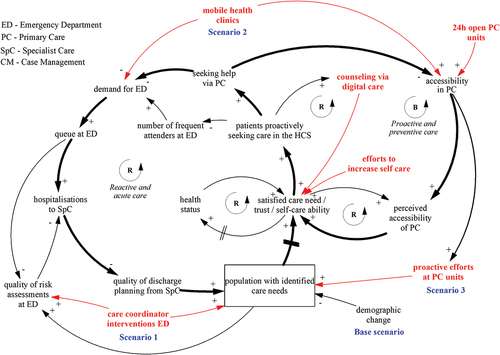
The main factors of these two feedback loops together with some important variables are included in . Variables in red represent some of the discussed closer care strategies during modelling, and highlighted in blue are the ones studied in the subsequent simulation study (see sections 4 and 6). Studying the reinforcing loop of Reactive and acute care one finds the considered main contributing factors behind the development of increased demand for ED on the aggregated level, where, increased demand for ED increments in the queue at the ED, having the effect that more elderly than necessary are subject to hospitalisations to SpC (specialist care). Yet, this leads to higher pressure on the personnel at SpC and lowers the quality of discharge planning from SpC. This contributes to fewer people being risk identified, and therefore, keeping the level of population with identified care needs low. Not having individual records of patients’ care need leads eventually to a lower degree of satisfied care need, decreased trust for the HCS, and a diminished self-care ability of the elderly. And subsequently, the patients proactively seeking care in the HCS are becoming fewer. This leads to fewer elderly seeking help via PC, due to not knowing their diagnoses and further increasing the demand for ED in a long-term escalating loop. However, to turn the loop around, efforts to increase the population with identified care needs were considered essential, since introducing continuously more new elderly, due to demographic change, without being risk identified is continuously growing the problem to the worse. The effect expected of the demographic changes was one of the main reasons not to continue business as usual in the studied problem. Hence, the effect of demographic changes on the HCS was considered important to include in the Base scenario of the simulation model. Also, patient surveys showed that patients perceived the accessibility of PC as low and this was a reason behind fewer elderly seeking help via PC. The main issue behind this was the low accessibility in PC (e.g., not opened 24 hours or 7 days a week), potentially working as a blocking mechanism to reroute patients towards the desired proactive and preventive care.
Using CLD enabled mapping of how the different closer care initiatives could intervene with the system behaviour. As depicts, the three selected scenarios support avoiding the undesired dynamics: Scenario 1) by increasing the quality of the reactive and acute care, thereby, reducing the number of hospitalisations, as well as effectively contributing to improving the risk identification of the population and identifying their care needs; Scenario 2) by consulting the most fragile patient groups in their homes, and thereby, directly reducing the visits to the ED and lowering the demand at ED, as well as increasing the accessibility in PC; and Scenario 3) by using more actively PC to risk identify the elderly patients.
Altogether, defining the CLD supported having a systems thinking perspective to articulate and reason around potentially existing feedback explanations to the observed phenomena. Also, it unified the modelling team to attain a common understanding of the problem dynamics before defining the SD model. The use of CLD facilitated the definition of the system boundary over the care-seeking behaviour of elderly patients, from which multiple potential simulation scenarios were considered possible. The SD model focused on a narrower system boundary to specifically calculate the consequences of the three closer care initiatives of which empirical data existed from pilot case studies. Consequently, the quantitative SD model studied a sub-set of the CLD.
5. Analysing the impact of closer care strategies with SD
The first step when building the SD model was to identify the appropriate structure and data to enable replicating the care-seeking behaviour of the elderly population and its effects on the visits to the ED and consequent hospitalisation days. Thereafter, the modelling team started with the scenario planning of the closer care strategies. Studying the statistical data of healthcare consumption by the elderly and how they could be categorised into different target groups were vital steps to specify the appropriate model structures.
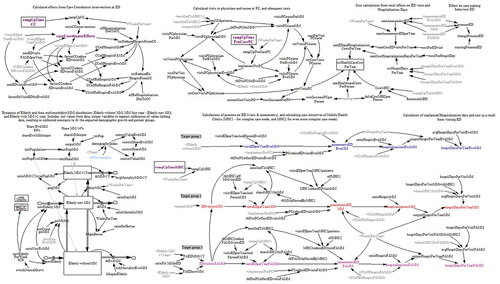
depicts an overview of the parts of the model, mimicking the layout of the complete model structure found in . A complete list of all the equations used in the model is presented in Table A1.
Figure 2. Overview of the parts in the SD model.
In BS1 (base structure) a stock and flow structure over the elderly population’s dynamics to generate the current level of care need is modelled. This serves to calculate its resulting care load on the HCS. The elderly population is divided into different cohorts based on their health status. This is due to the level of severe morbidity being identified to impact the population’s growth and decay mechanisms more significantly than age. For example, a healthy 90-year-old needs less care and is thus less likely to be close to dying than a 65-year-old with multimorbidity. The base structure is further defined in BS2 by sorting the elderly into three target groups: Gr1) elderly without multimorbidity (EwoMM), Gr2) elderly with multimorbidity (MM), and Gr3) elderly with multimorbidity having FA behaviour (FAMM). There were very few FAs in EwoMM and, therefore, this target group was omitted. The calibration of the BS1 part of the model used available healthcare data and government estimations on the regional population growth for the coming 10-year period. Studying the existing data over four years indicated a stable portion between the target groups. The inflows of new elderly utilised these findings (ratioNewEwMM) and the flows of the BS1 were also calibrated towards keeping a balanced ratio of the stock EwoMM, compared to the total elderly population (totPop). The stocks of the elderly with debuting multimorbidity during the first year (Elderly new MM) and those remaining with multimorbidity (Elderly MM >1 Year) until the end of life, were also calibrated to be kept approximately stable based on the same reasoning. These population levels were then used as inputs to the BS2 part of the base structure where the care load was calculated.
In BS2, the number of visits to the ED, the subsequent visits to specialist care and further hospitalisations, and their average length of stay was calculated for each target group. In BS3, each visit to the ED and hospitalisation days generate a cost which is summed up. The impact of these scenarios on the capacity of PC and ED was not analysed. The base scenario was simulated and verified towards available data.
The model structure also includes variables to enable simulating the three closer care strategies as scenarios as presented in .
Hence, for all scenarios, the reduced care load on the HCS was calculated in BS2 and the consequences on the total costs of the provided care and selected strategies were calculated in BS3.
Three years was considered sufficient to reach the effects of full implementation of the closer care strategies on a regional level. It was included as a gradual ramp-up function (zero to full implementation in three years) for the different key parameters it concerned (see Table A1 for detailed equations).
In the data from the base scenario are provided together with the effects that the different closer care scenarios, described in , have on key parameters that were employed in the model. All these scenarios reduced the number of unnecessary visits to the ED and the number of subsequent hospitalisations. For the length of stay per hospitalisation, the effects from the closer care strategies were absent, except for the target Gr2 in the MHC scenario, where a nearly 7% increase was observed. This is a result of increased quality of care for Gr2 in their homes or nursing homes reducing their need to visit the ED in the first place, where, those who finally visit the ED will to a larger extent be hospitalised for having more acute care needs. Regarding the costs, the CC scenario and MHC scenarios had already been funded by the region, so no further investments were needed to be included in the simulation, while the PC scenario required additional investments. See .
Some of the major results from the simulations are presented in . The result graphs depict an initial gradual improvement due to initiating the closer care strategies and their implementation effects the first three years, combined with the impacts of demographic growth throughout the simulated period. summarises the overall cost effects for all the scenarios, where the base scenario represents the current reference on cost estimations due to demographic growth. The resulting graph depicts that the MHC scenario is the most effective individual scenario. However, the combination of all the scenarios (CC+MHC+PC scenario) provides even better results regarding the overall cost reductions. One of the main objectives of the closer care strategies was to reduce visits to the EDs, this is shown in where the CC scenario marginally reduces the visits, while the MHC and PC scenario have nearly the same effect. In the combined scenario the individually simulated benefits melt into each other. presents the cost for total hospitalisations, which are the main cost contributors to the overall costs, also following a similar pattern of absorbing some of the individual benefits when the scenarios are combined.
Figure 3. Total healthcare costs for the different scenarios.
Figure 4. Total visits at the EDs per year for the different scenarios.
Figure 5. Total hospitalisation costs for the different scenarios.
Figure 6. Hospitalization days for all patient groups for the different scenarios.
In , the hospitalisation days per year for the combined CC+MHC+PC scenario compared to the base scenario are shown. This illustrates which patients generate the largest care load and thus cost. The largest effect in numbers is found in reducing the hospitalisation days for the target Gr2 (MM). While the largest improvement in percentage is found for Gr3 (FAMM). A small improvement effect is observed for Gr1 (EwoMM), which is the healthier elderly group considered in this study.
The experiments were developed to calculate the scaled-up consequences of applying the results of the different local pilot cases at a regional HCS level. Hence, much investigation was centred on identifying the appropriate data for the targeted population, having valid extrapolations, and a good representation of equations and model structure. However, the healthcare experts in the modelling team decided to include only empirically founded data in the model which had known and verified effects. This implied that the simulation model excluded assumptions of dynamic dependencies that could explain the reasons behind the observed phenomena leading to better care in the pilot cases. Consequently, the above scenarios applied the SD model as a visualised calculation model, neglecting its potential use as a vehicle for deeper analysis and testing of dynamic assumptions. Hence, the concluding results from the experimentations resembled how the Department of data management and analysis usually compiled these kinds of investigations. However, due to the thorough investigation during the case study, further modelling was conducted to explore to which extent the developed SD model could investigate some of the dynamic assumptions discussed by the modelling team.
6. Towards getting more knowledge: Exploring dynamic scenarios
During the modelling team meetings, considerable discussions were held about the relations between target groups, their care need, their health degradation, and the effects of different health policies on the target groups. The BS1 structure of the model included a detailed stock and flow structure to generate the demographic changes based on the separate target groups’ health degradation patterns and their relations to each other. The calibrations of the BS1 structure were made to fit the data from the HCS database and official data from the Swedish Government. Then, further studies were conducted to identify and explore how the target groups’ health status may change due to the closer care strategies.
At first, the BS1 structure was modified to enable sensitivity analyses of the parameters regulating the flows. The tested parameter ranges were manipulated at least twice the expected uncertainty (Sterman, Citation2000). However, the significant variables did not affect the model behaviour in any incoherent way. Then, based on the knowledge of the effects of the closer care strategies, revealed by the modelling team discussions, a design of experiments (DOE) was defined. Hence, the assumptions in the DOE were designed to test the reasoning behind the success of the modelled closer care strategies.
The DOE in presents the assumptions of how the respective closer care strategy (CC, MHC, and PC scenarios) could affect the flows regulating the dynamic transitions of the modelled population cohorts in the BS1 structure directly. In contrast, the presented results in section 4 used the BS1 structure to calculate the overall population and thereafter the increase in care load by each target group during the simulated period was directly proportional to the demographic growth. However, the DOE apply changes to the flows inside the BS1 structure, affecting the equilibrium between patient cohorts as a consequence of the policies. In consequence, the structural dependencies and the transitions of resulting rates continuously re-calculate the size of the target groups based on the feedback implications between the stocks and flows.
Table 4. Description of the DOE for the dynamic scenarios.
Each experiment in the DOE was implemented according to and analysed towards the outcome of the extrapolated results from the empirically derived calculations in . The specified improvements for the Target group, Average number of visits to ED per year, etc., in were not inserted as reduction effects in the new experiments. The simulated results revealed that the dynamic CC scenario exposed significant similarities to the CC scenario, see the depicted comparisons of the hospitalisation days in and the total healthcare costs in . Hence, the assumptions for how the underlying population health status may be affected in the dynamic CC scenario, , and the subsequent care need they generated, matched rather well with the previously calculated CC scenario. It also resulted in a healthier population of elderly and, in consequence, in increased population growth.
Figure 7. Hospitalization days for the respective patient groups for the CC scenarios.
Figure 8. Total healthcare costs for the CC scenarios.
However, the two remaining closer care strategies did not show such a clear fit, see and 10. In the dynamic MHC scenario the population’s health status was improved by providing care to the most fragile elderly patients. The results from this scenario indicate a need for further experimentation with the model. This was partially the case for the dynamic PC scenario as well. Therefore, additional experiments were carried out which activated the ramp-up switches rampUpTimeMHC and rampUpTimeProCarePC for the respective scenario (adding a “w” (with) at the end of the scenario name).
Figure 9. Total healthcare cost per year for the MHC scenarios.
depicts how both dynamic MHC & MHC(w) scenarios resulted in higher total costs than the previous MHC scenario. Despite neither of the two dynamic scenarios having an expected fit, these findings exposed an insight worth mentioning where the result could be traced to the lowered death rate for the Elderly MM >1 Year cohort. This, in turn, led to a rather high increment in the same population size of the elderly in need of higher levels of care as a consequence of the better quality of care offered by the MHC strategy. This is something that should be further investigated by the decision-makers if mobile health clinics are considered to be applied on a large scale in the region, since the long-term effects of this initiative may lead to a growing population of elderly with a high care need and consequently higher costs.
For the dynamic PC scenario, a rather good fit was identified considering the elderly with MM and FAMM, which was not the case in the dynamic PCw scenario, see . However, for the stock Elderly withoutMM, a clear growth pattern of healthier 65+ patients was evident, with the explanation that the dynamic PC scenario is impacting the health status of patients 65+ by keeping them in good health long into the declining years, creating a delayed development of multimorbidity and thus a delayed care load on the HCS.
Figure 10. Hospitalization days for FAMM and MM patient groups for the PC scenarios.
In conclusion, the dynamic scenarios indicate that it is plausible that closer care strategies will positively impact the health status of the elderly population as expected. However, additional insights regarding the potential long-term consequences of implementing the policies have also been identified. An example regards the most reactive strategy, implementing the MHC, which in the simulation experiment, described in Section 4, had the most beneficial impact on the overall cost performance. However, a side-effect discovered in the subsequent dynamic scenario, was that there might be unintended cost effects due to extended life expectancy and thus a growing population of elderly with high care needs. Possibly, for those already extremely ill in this group of patients, it could also include a prolonged period of poor life quality. These potential long-term effects were not considered during the model-building discussions and were not exposed until the experiments in were studied. Additionally, the scenarios in also indicate the need for further studies on the CC and PC scenarios. These policies may instead increase the portion of elderly with better health, leading to a longer life expectancy overall, and potentially also leading to a larger population as a consequence. The pilot case data had only depicted reduction effects on restricted cases and had neither been implemented for that long – where any proof of delayed consequences from an improved health status of the population on the regional level was not yet available. Consequently, based on these simulation analyses of how the closer care strategies may impact the development of the patient cohorts, further investigations to explore these consequences are recommended. SD simulation modelling would surely support the understanding of the delayed ripple effects that are likely to occur in the system, creating a larger care load on the HCS in the long run. In all, the complex interactions of these aspects also change the total cost performance as well.
7. Discussion
This section presents some of the reflections on the method chosen to conduct the study, the lessons learned, the limitations of the study, as well as the results obtained.
7.1. The importance of stakeholder involvement
The importance of stakeholder involvement in simulation projects is not new, and specific challenges arise when dealing with healthcare simulation projects such as having distributed decision-making structures (Tako & Kotiadis, Citation2015), stakeholders having conflicting interests and perspectives (S. C. Brailsford & Vissers, Citation2010; Eldabi, Citation2009), too heavy a staff workload (Jahangirian et al., Citation2015) or lack of experience or culture of using simulation in the healthcare context (Pitt et al., Citation2016). These are some of the challenges faced even during the development of this study as described in the following paragraphs.
Already from the beginning of the study, it was explained to the healthcare experts in the modelling team the importance of a clear problem formulation within a rather limited boundary and not a general definition such as “better quality of care to less cost”. Although there was a willingness to define a clear problem, the different views and perspectives on the project at hand, the limited stakeholder experience in dynamic modelling, the lack of knowledge of the complexity of the problem, as well as not having the decision-makers involved actively in the modelling team at the beginning of the project, made the initial stages of defining the problem and establishing the objectives an extremely difficult and unnecessarily time-consuming task. The problem focus shifted many times from offering closer care to all the patients in the region, to just focusing on those with chronic diseases, or to those with FA behaviour, to finally focusing on elderly patients. This group was finally chosen due to their care needs, the expected changes in demographics, and existing empirical data and pilot projects related to elderly patients. The long process of deciding the focus of the study involved searching for dynamic hypotheses through analysing multiple data from many different perspectives, having workshops and discussions with diverse stakeholders, and many frustrating meetings within the modelling team. The positive side of this process was that the modelling team learned from the process and the researchers gained substantial knowledge from the HCS. The researchers also came to realise that one important driver of the stakeholders was the need to deliver something that the decision-makers on the top management of the regional HCS would want to hear to buy into the concept of simulation as a decision support tool even for future studies. Due to this, the modelling process suffered from many ups and downs even during the final stages of model translation and experimentation, since including qualitative parameters that lacked established evidence or statistical data were considered not adequate to adopt even for experimentation purposes by the stakeholders in the modelling team. This greatly limited the possibilities of using the model for scenario experimentation. This was later on approached by the researchers outside the project boundaries by testing different dynamics scenarios, as presented in Section 5.
A key aspect when working with non-experienced stakeholders in any simulation project is probably to provide education not just to the stakeholders who will have an active part in the modelling team but also to the decision-makers so that the benefits, possibilities, and limitations of simulation as a method are clearly described. Introductory presentations to simulation provided to the modelling team did not prove to be sufficient.
The group of decision-makers had very limited time due to their workload and participated just at three specific points in time during the project: 1) deciding to start the study; 2) acknowledging the problem formulation; and 3) during the presentation of the results. As different authors point out, the active involvement of stakeholders, especially decision-makers, during the simulation study is crucial to ensure the acceptance of simulation as a decision-support tool (Tako & Kotiadis, Citation2015; Van der Zee, Citation2007). After facing the challenges of the problem formulation stage, a member of the decision-maker group was included in the modelling team, so that the knowledge gained about simulation as a tool for decision-making support and the knowledge gained about the HCS could be transferred to the group of decision-makers.
After many years of working with simulation in the healthcare sector, it seems that there are still many barriers to overcome for the extended use of simulation in the healthcare context (S. Brailsford, Citation2005; Tyler et al., Citation2022). More experiences like the one presented in this paper are surely needed as an addition to courses or training for healthcare personnel, decision-makers, and policymakers to show the potential of the method to support decision-making.
7.2. Discussion about the chosen method
Simulation was chosen already from the beginning of the study as an effective technique to analyse the closer care strategies and their impact on the HCS. Although both DES and SD were identified as possible methods, finally SD was chosen for its capabilities of including feedback effects as well as the possibility of studying short- and long-term dynamics. But also because the problem at hand required to have a system-wide perspective. However, the stakeholders were unfamiliar with feedback thinking when analysing their data, and during the discussions the one-year statistical data perspective was prominent. Thinking in terms of changes over several years was experienced as abstract and very difficult to understand. At this point, CLD became an essential tool for discussion and creative systems thinking.
An additional general benefit of using SD was to provide a base for rich discussions including a systemic perspective. Even though the modelling team worked on the definition and construction of the model, which provided them with very rich knowledge about the dynamics of elderly patients in the HCS, the decision-makers did not make use of the CLD nor tried to understand the simulation model. They just pursued specific results regarding a reduction in the number of visits to the ED and the number of hospitalisations, as well as the knowledge of the economic gain and loss depending on the scenario tested. Unfortunately, this perspective limited the use of the simulation model and its results. Therefore, the additional dynamic scenarios presented in this paper were developed to provide insights not considered in the initial modelling interventions. However, further studies are required to complete the model and include more dynamic considerations to draw upon more reliable analyses for the specific HCS.
7.3. Limitations of the study
Different assumptions have been taken during the study that may affect or limit the results and reporting of the simulation model.
The pilot studies applying closer care strategies demonstrated a positive impact in real-world settings. This positive effect was subsequently incorporated into the simulation model, and as anticipated, the results revealed a positive outcome concerning the health of the elderly. However, the extended analysis of the SD model not only highlighted the immediate benefits of specific strategies but also revealed their long-term effects, which would have been challenging to predict without the model.
On the other hand, in the studied case, large portions of the required costs to implement the closer care strategies had already been invested in the real world and were therefore not accounted for in the simulation model. Potential investment costs must be carefully evaluated and added to any future implementation utilising these findings to assure an appropriate evaluation of the cost-benefit trade-off between the desired effects on population health and the quality of care, and the total costs required to achieve those benefits.
Additionally, with regards to the presented SD model, a limitation exists regarding the lack of longer-term data on the proportion of the elderly with multi-morbidity. Although the available data covered a four-year period and demonstrated a relatively stable distribution among the target groups, discussions on the potential consequences of different health policies in isolation highlighted the need for more comprehensive data. Nevertheless, the modelling team upheld the integrity of the developed SD model by calibrating it with stable proportions, as only empirically founded data was included, omitting assumptions about dynamic dependencies.
Subsequently, in the extended analysis of the SD model, potential dynamic consequences resulting from the isolated reasoning of the considered closer care strategies were incorporated. This integration provided valuable insights into the combined effects of policies on multi-morbidity within the elderly population. However, it is important to acknowledge that the accuracy and robustness of these analyses could significantly benefit from the inclusion of longer-term data in the future. Acquiring more extensive data in the forthcoming years would strengthen and refine the findings of our analyses.
8. Conclusions
This paper presents a case study where SD modelling and simulation have been used to quantify and analyse different closer care strategies to offer better care for elderly patients and at the same time, reduce the number of visits to the EDs, the subsequent hospitalisations, as well as the total costs for the healthcare system (HCS).
The first part of the modelling process included defining a qualitative model using causal loop diagrams (CLD), which helped to provide a deeper understanding of the problem under analysis and a common view in the modelling team about the existing dynamics of elderly care-seeking behaviour in the HCS. It also supported defining the focus of the SD simulation model on the three closer care strategies: 1) implementing care coordinators in the ED; 2) implementing mobile health clinics; and 3) employing proactive care in PC. Inputs to these scenarios were based on existing pilot case studies and their empirical results. The simulation results showed that the combination of all three scenarios provided the best output and that benefits from individual scenarios partly overlap. Based on the learnings gained during model building, the study also included tests to explore dynamic assumptions of how the closer care strategies may impact the health of the modelled population. These experiments analysed the possible transitions between patient cohorts, developing from healthier elderly to those with severe care needs, and showed how the closer care strategies impact the elderly population. Besides, leading to better health and quality of care, studying the dynamic effects also exposed potential long-run responses that create a larger load on the HCS due to the increment in the number of elderly people and an increase in their life expectancy. Moreover, an extended life expectancy leads to an increment of the overall healthcare costs, even if the individual healthcare cost is reduced. These insights regarding long-term system responses from the simulation strongly suggest that further studies to investigate the system dynamics of healthcare policies are needed to better inform decision-makers before implementing any extensive HCS policies.
In addition to the description of the model and its results, this paper also discusses and reflects upon the problems encountered when building the simulation model. This reflection may serve other simulation modellers, especially those working in the healthcare domain.
Acknowledgments
The authors gratefully acknowledge the region of Västra Götaland (VGR) for funding the project. The authors are especially thankful to the project team members from the Department of data management and analysis of VGR Catarina Karlberg, Anna Norman Kjellström, Karin Fröjd, and Malin Lönnbark for their engagement during the whole development of the project. We would also like to thank the reviewers for their thoughtful comments and efforts towards improving our manuscript.
Disclosure statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
- Anderson, D., Sweeney, D., & Williams, T. (2002). An introduction to management science: Quantitative approaches to decision making (10th edition ed.). South Western Publishing Company.
- Ansah, J. P., Eberlein, R. L., Love, S. R., Bautista, M. A., Thompson, J. P., Malhotra, R., & Matchar, D. B. (2014). Implications of long-term care capacity response policies for an aging population: A simulation analysis. Health Policy, 116(1), 105–113. https://doi.org/10.1016/j.healthpol.2014.01.006
- Banks, J., Carson, J. S., II, Nelson, B. L., & Nicol, D. M. (2014). Discrete-event system simulation (Fifth ed.). Pearson Education Ltd.
- Barlas, Y. (1996). Formal aspects of model validity and validation in system dynamics. System Dynamics Review: The Journal of the System Dynamics Society, 12(3), 183–210. https://doi.org/10.1002/(SICI)1099-1727(199623)12:3<183:AID-SDR103>3.0.CO;2-4
- Bertrand, J. W. M., & Fransoo, J. C. (2002). Operations management research methodologies using quantitative modeling. International Journal of Operations & Production Management, 22(2), 241–264. https://doi.org/10.1108/01443570210414338
- Boyd, C. M., Ritchie, C. S., Tipton, E. F., Studenski, S. A., & Wieland, D. (2008). From bedside to bench: Summary from the American geriatrics society/national institute on aging research conference on comorbidity and multiple morbidity in older adults. Aging Clinical and Experimental Research, 20(3), 181–188. https://doi.org/10.1007/BF03324775
- Brailsford, S. (2005). Overcoming the barriers to implementation of operations research simulation models in healthcare. Clinical and Investigative Medicine, 28(6), 312–315. PMID: 16450620.
- Brailsford, S. C., Bolt, T., Connell, C., Klein, J. H., & Patel, B. (2009). Stakeholder engagement in health care simulation (I. assoc. comput. mach.: special, s. group, e. institute of industrial, s. inst. oper. res. manag. sci.: Simul, M. The society for & i. simulation, trans.) 2009 Winter Simulation Conference, WSC 2009 (pp. 1840–1849). Austin, TX.
- Brailsford, S., Lattimer, V. A., Tarnaras, P., & Turnbull, J. C. (2004). Emergency and on-demand health care: Modelling a large complex system. Journal of the Operational Research Society, 55(1), 34–42. https://doi.org/10.1057/palgrave.jors.2601667
- Brailsford, S. C., & Vissers, J. (2010). OR in healthcare: A European perspective. European Journal of Operational Research, 212(3), 223–234. https://doi.org/10.1016/j.ejor.2010.10.026
- Cassidy, R., Singh, N. S., Schiratti, P. R., Semwanga, A., Binyaruka, P., Sachingongu, N., Chama-Chiliba, C. M., Chalabi, Z., Borghi, J., & Blanchet, K. (2019). Mathematical modelling for health systems research: A systematic review of system dynamics and agent-based models. BMC Health Services Research, 19(1). https://doi.org/10.1186/s12913-019-4627-7
- Chang, A. Y., Ogbuoji, O., Atun, R., & Verguet, S. (2017). Dynamic modeling approaches to characterize the functioning of health systems: A systematic review of the literature. Social Science and Medicine, 194, 160–167. https://doi.org/10.1016/j.socscimed.2017.09.005
- Desai, S. M., Penn, M. L., Brailsford, S., & Chipulu, M. (2008). Modelling of Hampshire adult services—gearing up for future demands. Health Care Management Science, 11(2), 167–176. https://doi.org/10.1007/s10729-007-9049-0
- De Savigny, D., Blanchet, K., & Adam, T. (2017). Applied systems thinking for health systems research : A methodological handbook. McGraw-Hill Education.
- Eldabi, T. (2009). Implementation issues of modeling healthcare problems: Misconceptions and lessons. In M. D. Rosseti, R. R. Hill, B. Johansson, A. Dunkin, & R. G. Ingalls (Eds.), Proceedings of the 2009 Winter Simulation Conference. Austin, Texas, USA, 13-16 December 2009. (pp.1831–1839).
- El-Zoghby, J., Farouk, H. A., & El-Kilany, K. S. (2016, March 8–10).An integrated framework for optimization of resources in emergency departments (E. P. B. w. wide, IEEE informs, E. official airline partner & siemens, trans.) 6th International Conference on Industrial Engineering and Operations Management in Kuala Lumpur, IEOM 2016, Malaysia (pp. 1621–1632). IEOM Society.
- Faeghi, S., Lennerts, K., & Nickel, S. (2021). A system dynamics model application to operating room planning and management. Journal of Simulation, 17(1), 58–75. https://doi.org/10.1080/17477778.2021.1932622
- Goienetxea Uriarte, A., Ruiz Zúñiga, E., Urenda Moris, M., & Ng, A. H. C. (2017). How can decision makers be supported in the improvement of an emergency department? A simulation, optimization and data mining approach. Operations Research for Health Care, 15, 102–122. https://doi.org/10.1016/j.orhc.2017.10.003
- Hillier, F., & Lieberman, G. J. (2015). Introduction to operations research (Tenth edition ed.). McGraw-Hill Education.
- Homer, J. B., & Hirsch, G. B. (2006). System dynamics modeling for public health: Background and opportunities. American Journal of Public Health, 96(3), 1431–1451. https://doi.org/10.2105/AJPH.2005.062059
- Hulshof, P. J. H., Kortbeek, N., Boucherie, R. J., Hans, E. W., & Bakker, P. J. M. (2012). Taxonomic classification of planning decisions in health care: A structured review of the state of the art in OR/MS. Health Systems, 1(2), 129–175. https://doi.org/10.1057/hs.2012.18
- Jahangirian, M., Taylor, S., Eatock, J., Stergioulas, L. K., & Taylor, P. M. (2015). Causal study of low stakeholder engagement in healthcare simulation projects. Journal of the Operational Research Society, 66(3), 369–379. https://doi.org/10.1057/jors.2014.1
- Katsaliaki, K., & Mustafee, N. (2011). Applications of simulation within the healthcare context. The Journal of the Operational Research Society, 62(8), 1431–1451. https://doi.org/10.1057/jors.2010.20
- Kjellström, A., Karlberg, C., Fröjd, K., Lönnbark, M., Linnéusson, G., & Goienetxea Uriarte, A. (2019). Simulering av insatser i nära vård för de mest sjuka äldre: med avseende att minska vård på akutmottagning och inom slutenvård. VGR analys (45), 28. V. Götaland, Sweden.
- Kunc, M., Mortenson, M. J., & Vidgen, R. (2018). A computational literature review of the field of system dynamics from 1974 to 2017. Journal of Simulation, 12(2), 115–127. https://doi.org/10.1080/17477778.2018.1468950
- LaCalle, E., & Rabin, E. (2010). Frequent users of emergency departments: The myths, the data, and the policy implications. Annals of Emergency Medicine, 56(1), 42–48. https://doi.org/10.1016/j.annemergmed.2010.01.032
- Larisch, L. M., Amer-Wåhlin, I., & Hidefjäll, P. (2016). Understanding healthcare innovation systems: The Stockholm region case. Journal of Health Organization and Management, 30(8), 1221–1241. https://doi.org/10.1108/JHOM-04-2016-0061
- Lindgren, B. (2016). The rise in life expectancy, health trends among the elderly, and the demand for health and social care. https://doi.org/10.3386/w22521
- Linnéusson, G., & Goienetxea Uriarte, A. (2021). Analyzing closer care strategies for elderly patients: Experience and reflections from modeling with system dynamics. In D. R. M. Fakhimi & T. Boness (Eds.), Proceedings of the Operations Research Society Simulation Workshop 2021 (SW21), Loughborough University (pp. 117–126). Operational Research Society.
- Linnéusson, G., Ng, A. H. C., & Aslam, T. (2018). Towards strategic development of maintenance and its effects on production performance by using system dynamics in the automotive industry. International Journal of Production Economics, 200, 151–169. https://doi.org/10.1016/j.ijpe.2018.03.024
- Lipsitz, L. A. (2012). Understanding health care as a complex system: The foundation for unintended consequences. JAMA, 308(3), 243–244. https://doi.org/10.1001/jama.2012.7551
- Lyons, G. J., & Duggan, J. (2015). System dynamics modelling to support policy analysis for sustainable health care. Journal of Simulation, 9(2), 129–139. https://doi.org/10.1057/jos.2014.15
- Mielczarek, B., & Uziałko-Mydlikowska, J. (2012). Application of computer simulation modeling in the health care sector: A survey. SIMULATION, 88(2), 197–216. https://doi.org/10.1177/0037549710387802
- Mitropoulos, P., Adamides, E., & Mitropoulos, I. (2022). Redesigning a network of primary healthcare centres using system dynamics simulation and optimisation. Journal of the Operational Research Society, 74(2), 574–589. https://doi.org/10.1080/01605682.2022.2096499
- Moskop, J. C., Sklar, D. P., Geiderman, J. M., Schears, R. M., & Bookman, K. J. (2009). Emergency department crowding, part 1—concept, causes, and moral consequences. Annals of Emergency Medicine, 53(5), 605–611. https://doi.org/10.1016/j.annemergmed.2008.09.019
- Penny, K. E. E., Bayer, S., & Brailsford, S. (2022). A hybrid simulation approach for planning health and social care services. Journal of Simulation, 1–14. https://doi.org/10.1080/17477778.2022.2035275
- Pitt, M., Monks, T., Crowe, S., & Vasilakis, C. (2016). Systems modelling and simulation in health service design, delivery and decision making. BMJ Quality & Safety, 25(1), 38–45. https://doi.org/10.1136/bmjqs-2015-004430
- Radnor, Z. J. (2010). Review of business process improvement methodologies in public services. AIM Research.
- Salleh, S., Thokala, P., Brennan, A., Hughes, R., & Booth, A. (2017). Simulation modelling in healthcare: An umbrella review of systematic literature reviews. PharmacoEconomics, 35(9), 937–949. https://doi.org/10.1007/s40273-017-0523-3
- Sargent, R. G. (2011). Verification and validation of simulation models Proceedings of the 2011 Winter Simulation Conference (WSC), Phoenix Arizona (pp. 183–198).
- Senge, P. M., & Sterman, J. D. (1992). Systems thinking and organizational learning: Acting locally and thinking globally in the organization of the future. European Journal of Operational Research, 59(1), 137–150. https://doi.org/10.1016/0377-22179290011-W
- Slack, N., & Lewis, M. W. (2011). Operations Strategy (3rd edition ed.). Prentice Hall.
- Sterman, J. (2000). Business dynamics: Systems thinking and modeling for a complex world. Irwin McGraw-Hill.
- Tako, A., & Kotiadis, K. (2015). PartiSim: A multi-methodology framework to support facilitated simulation modelling in healthcare. European Journal of Operational Research, 244(2), 555–564. https://doi.org/10.1016/j.ejor.2015.01.046
- Taylor, K., & Dangerfield, B. (2005). Modelling the feedback effects of reconfiguring health services. Journal of the Operational Research Society, 56(6), 659–675. https://doi.org/10.1057/palgrave.jors.2601862
- Tyler, J., Murch, B., Vasilakis, C., & Wood, R. M. (2022). Improving uptake of simulation in healthcare: User-driven development of an open-source tool for modelling patient flow. Journal of Simulation, 1–18. https://doi.org/10.1080/17477778.2022.2081521
- United Nations. (2017). World population prospects: The 2017 revision, key findings and advance tables. https://doi.org/10.18356/b19523c6-en
- Vanderby, S. A., Carter, M. W., Noseworthy, T., & Marshall, D. A. (2015). Modelling the complete continuum of care using system dynamics: The case of osteoarthritis in Alberta. Journal of Simulation, 9(2), 156–169. https://doi.org/10.1057/jos.2014.43
- Van der Zee, D. J. (2007). Developing participative simulation models—framing decomposition principles for joint understanding. Journal of Simulation, 1(3), 187–202. https://doi.org/10.1057/palgrave.jos.4250020
- Västra Götalandsregionen. (2018). Handling plan 2018-2019: Omställning av hälso- och sjukvården i Västra Götalandsregionen. HS 2018-00460.
Appendix
Figure A1. System dynamics model over the care needs of elderly patients in the healthcare system.
Appendix
Table A1. List of Equations ofthe SD modelover the Care Need of Elderly Patients in the Healthcare System.
