
ABSTRACT
Purpose: As the proportion of older adults in Germany continues to grow, so does the need for physical activity as a strategy for health promotion. The purpose of this study is to gain insights into the belief system underlying older adults’ physical activity and its interplay with motivation by integrating Theory of Planned Behaviour and Self-Determination Theory.
Methods: We conducted 20 semi-structured interviews with residents of Germany who were 65 years of age or older. Transcripts of interviews were analysed with a coding frame of deductive main categories and inductive subcategories.
Results: Part of our results is a typology that divides our sample into four groups based on the intensity and perceived sufficiency of their physical activity. These groups mainly differ in their intrinsic vs. extrinsic motivation and how they deal with barriers to physical activity, i.e., control beliefs.
Conclusion: Messages to promote physical activity should be tailored regarding older adults’ varying beliefs and motivation. To overcome barriers, intrinsic motivation plays a crucial role. Intrinsic motivation is closely linked to activities that are joyful and satisfy basic psychological needs. Moreover, it is important for older adults to be able to adjust their activities to age-related physical limitations and chronic diseases.
People worldwide are living longer. In 2019, there were 703 million people aged 65 years or older worldwide and this number is estimated to double until 2050 (United Nations, Citation2019). The pace of population ageing is accelerating. While the proportion of the German population over 67 years of age accounted for 19% of the total population in 2018, it will increase to a proportion of 24 to 30% in 2060 (Federal Statistical Office, Citation2019). The prevalence and incidence of chronic health conditions that require treatment is significantly higher in this age group compared to younger people. While some conditions can be attributed to the biological processes of ageing and the associated susceptibility to illness, others are related to lifestyle practices, such as sedentary behaviour and a lack of physical activity. Regular physical activity, as numerous studies have shown, can counter risk factors and age-related health conditions. It contributes to healthy ageing (Hamer et al., Citation2014) by preventing e.g., fall-related injuries (Pereira et al., Citation2008), diabetes (Smith & Hamer, Citation2014), cognitive decline (Sanchez-Lopez et al., Citation2018), and dementia (Ahlskog et al., Citation2011). In addition, physical activity increases older adults’ mental health (Ku et al., Citation2016; Teixeira et al., Citation2013). Thus, physical activity can contribute to physical and psychological well-being as well as increase the number of healthy life years in older people. Despite these benefits, physical activity levels among older adults overall remains below the recommended 150 minutes of moderate-to-intense activity per week in Germany (Robert Koch-Institute, Citation2017; World Health Organization [WHO], Citationn.d. a). Because of wide-ranging differences in their biographies, living conditions, social and ethnic backgrounds, and overall physical and psychological conditions, as well as interdependencies between some of these factors, this age group is more heterogeneous than younger generations (Federal Centre for Health Education, Citation2013). Despite their many distinctive characteristics, activity levels and health status are especially low among vulnerable population groups. In the context of health, vulnerable population groups are described as those groups that are more susceptible to health problems resulting from their personal circumstances as well as other influences, including lower socioeconomic status (SES), migrant background, or chronic diseases (Schaeffer et al., Citation2017). As the proportion of older adults in Germany continues to grow, so too does the need for physical activity as a strategy for prevention and health promotion. Thus, it is important to take into account the different needs of this extremely diverse population group. Health promotion strategies should be based on theory and evidence regarding these needs (Rossmann, Citation2015).
Research into health behaviours, including physical activity, has been conducted from several different theoretical perspectives. Prominent theories include the Self-Determination Theory (SDT) and Theory of Planned Behaviour (TPB). Among these, the TPB has frequently been used to explain factors that determine behavioural intentions and different types of behaviours, including physical activity among older population groups (Alexandris et al., Citation2007; Armitage, Citation2005; Gretebeck et al., Citation2007). Deci and Ryan’s (Citation2000) SDT allows further insight into the motivational characteristics that are associated with certain behaviours. While independent empirical findings using either theory could explain variations in health-related behaviours, both theories have their shortcomings: the TPB has proven to be effective in explaining variations in intentions and behaviours, yet it does not identify the origins of the antecedents of behaviour (Hagger & Chatzisarantis, Citation2009) and the SDT does not model the exact process of how motivational orientations become intentions and behaviour. Researchers have recently begun to integrate the two theories because they are considered to be complementary (Hagger & Chatzisarantis, Citation2009). Thus, integrating the constructs of both theories may improve our understanding of the motivational processes and the social cognitive belief systems that underlie physical activity intention and behaviour among various social groups aged 65 years and above in Germany. Accordingly, this article suggests an integrative model that is derived from both theories. To explore older adults’ beliefs and the interplay between beliefs and motivation regarding physical activity, we conducted a qualitative study. Results of our study provide the base for tailored approaches in promoting increased and age-appropriate uptake of physical activity among older adults.
The theory of planned behaviour and physical activity
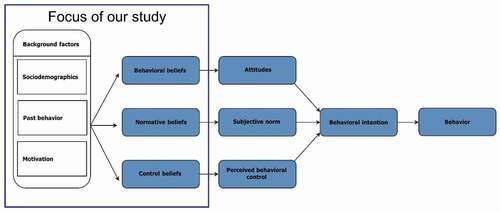
The TPB is a social-cognitive theory that was developed to understand the complexity of people’s behavioural intentions and behaviour (see e.g., Ajzen, Citation2005; Fishbein & Ajzen, Citation2010; in the context of physical activity see Hagger et al., Citation2002). It focuses on a three-part set of beliefs concerning: a) behavioural consequences and their evaluation; b) social expectations of important others towards the behaviour and the motivation to comply with these expectations; and c) perceived control factors and their power to facilitate or inhibit the performance of the behaviour. These beliefs determine an individual’s attitude, subjective norm, and perceived behavioural control towards a behaviour, which, in turn, influences behavioural intention (see ). The intention to engage in physical activity is its most immediate predictor; the stronger the intention, the more likely physical activity will be performed or increased.
Figure 1. Research model and focus of the study
Various meta-analyses confirmed that TPB is well suited to explain physical activity (Downs & Hausenblas, Citation2005b; Hagger et al., Citation2002; Hausenblas et al., Citation1997). However, the predictive value of subjective norms on behavioural intention was significantly lower than for attitude and perceived behavioural control among those aged 60 years and above (Alexandris et al., Citation2007; Gretebeck et al., Citation2007). The above-mentioned meta-analysis of Hagger et al. (Citation2002) identified age as a moderator of the relationship between intention and behaviour. Thus, it appears that older aged adults are more likely to translate their intentions to become physically active into action than those of a younger age. Regarding the preceding beliefs about physical activity, research shows some general beliefs that hold true for different populations, but also specific beliefs for different age groups and cultural backgrounds (Downs & Hausenblas, Citation2005a). It must be considered that older adults share some beliefs with other populations, but also hold particular beliefs about physical activity. In their review, Downs and Hausenblas (Citation2005a) cited five studies with samples older than 60 years (Brenes et al., Citation1998; Conn, Citation1998; Courneya, Citation1995; Helm, Citation1987; Michels & Kugler, Citation1998). It should be noticed that these studies’ identification of beliefs is based on rather small samples and that most of these studies did not cover all three types of beliefs. There are some recent studies of older adults‘ beliefs about physical activity (Dye & Wilcox, Citation2006; Kosteli et al., Citation2016; Schmidt et al., Citation2016), but studies actually based on TPB are scant in the current state of research (Benjamin et al., Citation2005; Lin et al., Citation2007). Therefore, it is necessary to identify the salient TPB beliefs for our specific target group—older adults in Germany. We seek to answer the following research question:
RQ1: What are the behavioural, normative, and control beliefs of older adults in Germany with respect to physical activity?
The self-determination theory and physical activity
While physical activity studies using the TPB have successfully predicted and established relationships between the direct determinants of intention—attitude, subjective norms, and behavioural control—the influence of their underlying beliefs has been largely neglected in current research among older people. Moreover, the theory itself has its limitations in explaining physical activity behaviour for two reasons. First, even though the TPB acknowledges that some background factors, including media influences or demographic attributes (Ajzen, Citation2005), it does not account specifically for other influences that are likely to factor into behavioural intention and the performance of physical activity of the population aged 65 years and above. These include individual, social, or structural constraints, and past behaviour. Second, the TPB does not explicitly distinguish between the quality of motives, which would indicate why certain beliefs and resulting determinants are pursued (Hagger & Chatzisarantis, Citation2009). Thus, integrating another theoretical perspective with the TPB may improve our understanding of the motives associated with starting and maintaining (or not) physical activity. In contrast to the TPB, the SDT is a theory of human motivation. It predicts the quality of motivation, and thereby the motivational reasons for the performance, commitment, and persistence of individual behaviours. Therein, the theory distinguishes a continuum of different degrees of motivations, ranging from the two extremes self-determination (autonomy) to non-self-determination (control). Behaviours that are driven by intrinsic motivation, integrated regulation, and identified regulation are considered to be forms of self-determination. In contrast, introjected regulationand external regulation are considered to be externally controlled (Deci & Ryan, Citation2008).
The SDT postulates that the main force behind adopting self-determined, intrinsic forms of motivations is people’s desire to satisfy three innate psychological needs: autonomy, competence, and relatedness (Deci & Ryan, Citation2008). Autonomy refers to the need to experience one’s actions as volitional. Competence means to be able to effectively enact a behaviour. Relatedness concerns people’s need to seek intimate relationships with others. Autonomous motivation is associated with increased psychological well-being and persistence with health-related behaviours. However, strongly controlled motivation is associated with negative psychological outcomes and avoidance of tasks (Deci & Ryan, Citation2000, Citation2008).
Numerous studies confirm SDT’s usefulness in investigating and promoting physical activity (Biddle et al., Citation1999; D’Angelo & Reid, Citation2007; Edmunds et al., Citation2008; Russell & Bray, Citation2009; Springer et al., Citation2013; Wilson et al., Citation2008). Some studies have already shown its relevance for older adults as well: Older adults who maintain physical activity show higher levels of self-determined motivations than older adults who quit being active (Kirkland et al., Citation2011; Stephan et al., Citation2010). Even if motivation is shown to be one important determinant of physical activity, however, just applying the SDT misses out other important determinants known from the TPB. Therefore, an integrative perspective should provide the most comprehensive approach to explain physical activity.
Indeed, some successful attempts have been made previously to integrate TPB and SDT in order to explain physical activity. A meta-analysis of 36 studies showed that not only past behaviour was an important background factor but also motivation. Both influenced behavioural intention mediated by the TPB components attitudes, subjective norm, and perceived behavioural control (Hagger & Chatzisarantis, Citation2009). Therefore, in addition to sociodemographics, we integrate motivation and past behaviour as background factors in our research model (see ).
Our second research question integrates all aspects of our research interest (see marked focus of our study in ). Although there have been some quantitative studies that integrated TPB and SDT, we still need to gain a deeper understanding of the interplay of beliefs and motivation. Therefore, our second research question is:
RQ2: How are variations in physical activity associated with motivational factors, TPB beliefs, and sociodemographic characteristics?
Methods
Due to our limited understanding of the motivations and beliefs behind physical activity within our target group and the relationship between the two theories, we applied a qualitative approach and conducted 20 semi-structured interviews with residents of Germany, who were 65 years of age or older.
Participants and procedure
Twenty adults aged 65 years or older, residing in care facilities or living independently in the community in both rural and urban areas, were recruited through non-governmental organizations, community groups, and postings on notice boards at community and sports facilities in two German federal states: North Rhine-Westphalia, Germany’s most densely-populated state, and Thuringia, one of the territories of the former German Democratic Republic. People with dementia or insufficient language skills in either German or English were excluded.
Our sample purposefully included vulnerable and hard-to-reach groupsFootnote1 within this age groups for the following reasons: 1) among older people in general, vulnerable groups are not only more likely to have or develop multimorbidity, but also engage in considerably less physical activities. Thus, it is important to promote the causality between these two aspects and enable active and healthy ageing among all older groups in Germany; and 2) the older aged population is very heterogeneous, and vulnerability applies to a variety of different aspects such as SES, immigrant status, or the genetic disposition of the disease. To motivate vulnerable older people to increase their physical activity, an understanding of varying motivations and beliefs towards physical activity is required for a targeted approach.
Participants were interviewed individually in their homes or at a mutually convenient location. Before taking part in the study, participants provided informed consent and agreed to audio recording of responses. Interviews ranged from 30 to 60 minutes and were conducted in July 2018. One interview was conducted in English, and the remaining interviews were conducted in German. Errors in grammar and choice of words by non-native German participants were intentionally kept and reflected in the translation of the quotes. Each study participant received 20 Euros for their participation.
Study participants included ten men and ten women aged between 65 and 91 years old. Of the 20 participants (see and II), nine were widowed, one was divorced, and ten were married. Two of the widowed participants lived in care facilities, the remaining respondents either lived with their partners or on their own in apartments or houses. All but one participant had completely retired from any income-generating work and six of the respondents reported that they worked as volunteers in religious or community activities. Three-quarters of the participants reported that they engaged in physically demanding everyday activities, and household and gardening chores several times per week. This includes climbing several flights of stairs, carrying shopping bags, house cleaning, weeding, or renovating work. Spending time at clubs or local associations, going on excursions, relaxing at home, and reading were the most frequently mentioned leisure activities. Nine study participants lived near their children and grandchildren and reported that they were considerably involved in the lives of their close relatives. Overall, our sample reported high levels of regular physical activity. Twelve respondents reported that they exercised intentionally by going for extended walks or on cycling tours, working out in a gym or sports club, swimming, or practicing gymnastics.
Table I. Participants’ characteristics
Because our study is based on existing theories, we conducted semi-standardized interviews to ensure that all relevant constructs were discussed during the interviews, while preserving the necessary openness of qualitative research (Flick, Citation2009). Apart from a short questionnaire with demographic questions, our theory-based interview guide consisted of six sections, each of which with a set of main questions as well as prompts. The first two sections included questions about the participants’ background regarding living arrangements and health attitudes. The following sections reflected the core constructs of our research model (see ): status quo of physical activity, including past behaviour and motivation, and TPB beliefs. In addition, we asked the respondents about their attitudes towards ageing.
Data analysis
All interviews were transcribed and analysed using qualitative content analysis (Schreier, Citation2012). Each participant was assigned a pseudonym that reflected his or her gender and cultural background (see ). Data analysis was supported by the software MAXQDA (VERBI Software, Citation2018). A first coding frame was built from our theory-based research interest by phrasing deductive main categories for each topic. For example, TPB beliefs were differentiated into the main categories of behavioural, control, and normative beliefs (Fishbein & Ajzen, Citation2010), and motivational factors were distinguished based on the SDT into intrinsic motivation, integrated regulation, identified regulation, introjected regulation, external regulation, and amotivation (Deci & Ryan, Citation2000). In the next step, relevant sections of the interviews were marked and coded using the corresponding main categories. Thereafter, all text passages within each category were considered to substantiate the main categories with subcategories (see ). For example, different subcategories of control beliefs, i.e., barriers and facilitators, were identified: social support or sport fellows, the weaker self, physical limitations, infrastructure, resources, instrumental support, weather conditions, time, joy, and variety. Hence, this step of data analysis resulted in a coding frame that was built from theory (deductive main categories) as well as data (inductive subcategories) (Kuckartz, Citation2013; Schreier, Citation2014).
Table II. Participants
Table III. Beliefs
This coding frame provides an overview of the different dimensions of all relevant constructs and can be used to compare the interviews concerning the coded subcategories. RQ1 is answered by describing the subcategories of the beliefs towards physical activity in detail. To answer RQ2, additional analyses were performed, and the interviewees were grouped based on their reported past activity level, taking into account their everyday and leisure activities, sports, and frequency of other physical activities. Relying on existing classifications (WHO, Citationn.d. a, Citationn.d. b) it seems reasonable to differentiate between vigorous and moderate intensity of physical activity. We defined working out at a gym or sports club, swimming, and cycling as vigorous activity; and walking, gymnastics, gardening, and climbing stairs as moderate activity. Combined with the interviewees’ own evaluation of their activity level, each participant was assigned to one of four groups. These four groups were compared based on the subcategories of our coding frame—focusing on motivational factors and beliefs—and sociodemographic variables.
Ethical considerations
This study followed the Declaration of Helsinki (World Medical Association, Citation2013) and was approved by the Ethics Committee of the University of Erfurt. Participants received both verbal and written information about the project and gave written consent. All participants could withdraw from the project at any time without any explanation. All names of individuals and places were removed to anonymize the interview transcripts.
Results
Beliefs towards physical activity (RQ1)
Behavioural beliefs
Participants were aware of and broadly endorsed the importance of physical activity and particularly negative consequences of physical inactivity (see ). A decline in physical activity among those being active was perceived to potentially increase health problems and negatively impact their mobility and muscle strength: “I would have died 3 or 4 years ago. But I am still alive” (Anton, 70); ”I came to realize that my muscles declined, that’s a result from last year’s winter, sitting for too long, not moving because the joints hurt, for instance. I rather remained seated, but the result was that I was having more difficulties to climb the stairs. Climbing stairs became strenuous” (Jochen, 70).
The negative influence of physical inactivity on psychological well-being was expressed by many respondents, for example: “I assume I would become depressed” (Anna, 76), and “I would be in a very bad mood, I have to do something” (Hans, 65).
However, all respondents elicited a range of perceived benefits of being physically active. As much as inactivity was detrimental to the overall health status and mobility, these two were also the most commonly cited benefits of physical activity: “I somehow feel better afterwards and I don’t feel any pain” (Christine, 68); “Yes, I think it’s necessary in old age to train the muscles, so that those who become inactive will find it all the way more difficult to become active again” (Inge, 82); and “Yes, this [stretching] makes my body strong” (Edward, 82). In addition, some participants mentioned specific physical consequences of activity regarding the cardiovascular system and body weight.
Various facets of psychological well-being were also associated with regular physical activity. Some participants described feeling at ease with themselves during and after their exercise: “It calms me down, I do my exercise and let my thoughts wander” (Georg, 76); and “So afterwards I feel at ease and I can say to myself ‘this did me a lot of good’ ” (Christine, 68). In addition, participants mentioned positive consequences of physical activity that can be linked to the satisfaction of basic psychological needs. Specifically, participants described experiencing feelings of competence and autonomy by exercising: “It’s somehow a self-affirmation to be still capable in the old age” (Andreas, 69); “I always do this in the morning to activate myself. I want this … . To be independent” (Annelise, 89). Last, physical activity is also linked to relatedness: “I also do it to get in touch with people” (Kathrin, 85).
When asked about perceived negative consequences of physical activities, half of the respondents did not see any negative consequences. Overdoing it (overexertion) and consequently suffering from fatigue and muscle pain was mentioned by three of the interviewees. Two participants noted the accident risk associated with physical activity.
Normative beliefs
None of the participants could think of any people who would disapprove of their physical activity, but they identified a variety of different groups or people they believed would approve and support them if they maintained or increased their physical activity (see ). The most salient reference people were children and grandchildren as well as friends: “My daughter, she pays attention that I do my gymnastics and she inquires about it” (Anna, 76); “Yes, when I was still living over there, next to my children, they often came and said ‘You have to go out, you have to do more’ and so on. And I did it” (Bettina, 83); “They [friends] say ‘We look at you’. At me, they are all a little younger than I and as I am always the first, they have to do it likewise” (Olga, 82); and “And then they all called me Grandpa. ‘Grandpa, you are in such a good physical condition, keep it up, stay active’” (Heinrich, 88).
For some people neighbours and acquaintances from cultural or religious groups were relevant reference groups regarding physical activity. Additionally, medical professionals and—for those who were not yet widowed—their spouse, were considered important influential people.
Control beliefs
The study participants cited several perceived internal and external barriers to physical activity (see ). The two most frequently reported control beliefs inhibiting regular physical activity were the weaker self and physical limitations: “I am not sick and actually a little lazy and sluggish in the old age” (Christine, 68); and “When I feel that it is so hard. Walking is harder for me than it used to be 2 or 3 years back. I feel that I am getting older” (Olga, 82).
A lack of a sport fellow or social support was mentioned as an impeding factor by those who could not rely on one: “There’s nobody here in this care facility who could still do it. I’ve already asked around, including my neighbour, but she says she can’t do it anymore” (Heinrich, 88). In contrast, those who exercised together with others perceived it as a facilitator: “I think when you’re walking with someone, you can go much further—no problem. But when you walk alone, you think ‘Oh, it hurts, I will stop’ or ‘Take a short-cut’. And when you walk with someone, you talk and distract yourself, that’s it” (Kathrin, 85).
There were two main reasons for a lack of fellow exercisers: participants experienced that their former exercising partners had either passed away or were unable to exercise for physical or mental reasons and they could not find new partners. Very active participants reported that people who were their age felt overexerted when exercising together, whereas the very active participants felt overexerted when they joined groups or people who were considerably younger than their age.
Other barriers, that were mentioned less often, referred to bad or challenging infrastructure (e.g., unsafe bike- and footpaths), lacking resources (e.g., financial constraints), poor weather conditions or time shortage. In contrast, joyful and diverse activities (joy and variety) may serve as facilitators. However, especially those living in rural areas, lack instrumental support such as transportation to get some change and engage in their preferred activities.
Association of variations in physical activity with motivational factors, TPB beliefs, and sociodemographic characteristics (RQ2)
Based on their reported intensity and the perceived sufficiency of physical activity, we classified study participants into four groups: 1) mastering, 2) adapting, 3) persevering, and 4) struggling. (see ). Intra- as well as inter-group characteristics with regards to motivational factors, beliefs, and sociodemographic variables were compared.
Table IV. Comparison of groups with varying frequency and intensity of physical activity
Mastering
Nine out of 20 participants reported that they engaged in vigorous-intense physical activity, and they perceived their overall activity level as sufficient. Mastering participants engaged in a variety of different moderate and vigorous-intense activities several times a week, including hiking, cycling, working out in a gym, swimming, and doing household as well as gardening chores. Two-thirds of study participants assigned to this group were women, among whom five were single. Among the three men, two were married and one was widowed. Whereas no clear trends can be seen regarding net income, age, and ethnic backgrounds, seven of the participants reported that they experienced some form of chronic physical limitations. Compared to the other groups, the onset of growing limitations within this group was connected to an uptake of increased or specific types of physical activity. Whereas most study participants named some health-related and symptom-easing benefits of physical activity, the motivation to engage in physical activity with the main intention of halting or easing experienced physical problems was strongest in this group: “I have to do that [exercise]. If I stop listening to myself or my body, what he wants or what he does or what he tells me, I will die” (Anton, 70); and “If I do not move around, I become very stiff. My legs will not keep going” (Olga, 82).
Consciously confronting one’s own increasing physical decline by exercising is supported by a high health awareness within this group as well as active consultation of health information by searching the Internet, reading expert literature, and talking to medical personnel and other people.
The perceived negative consequences of inactivity were diverse in this group, ranging from a loss in mobility and muscle strength to increased pain, gain in body weight, and feelings of sadness. However, besides its physical benefits, participants valued the psychological benefits of their physical activities among which relatedness was mentioned the most: “I do not like to exercise on my own, like jogging or anything that is so monotonous” (Jochen, 70). Engaging in physical activity is an important remedy to satisfy the need for relatedness: “There are people at the swimming pool whom I meet every week and then we chat ‘How are you?’, ‘I had a cold, I could not come and I am glad to be here again’ or something like this. Well, I think I’m fundamentally a person who likes to be with other people” (Inge, 82).
While mastering participants in general referred to only few negative consequences of physical activity, it stood out that physical overexertion and resulting physical pain were mentioned only in this group.
Mastering participants were aware of both internal and external constraints to their physical activity. The most important internal barriers were laziness or the weaker self and physical limitations. However, they find ways to challenge these internal barriers: “Sometimes you don’t really feel like it, but I’m the kind of guy who says ‘I’ll do it anyway’ and I also noticed that once I go back to exercising at the gym, it’s okay. You just have to, as we say, overcome your weaker self” (Jochen, 70).
External barriers included a lack of exercise partners and for those with lower SES, scarce financial resources. However, participants did not perceive these constraints as obstacles, as they either tended to ignore them (e.g., lacking exercise partners or weaker self) or adapt to the circumstances by, for instance, choosing to exercise outdoors instead of at a paid gym.
Despite strongly treating physical activity as means to an end, all participants identified at least one activity that they intrinsically enjoyed and engaged in for pleasure: “Dancing, dancing. And tennis, table tennis. But dancing is the most important thing. Because there is music and you can express anything what is in your heart and how you feel” (Olga, 82).
Enjoying nature and being outside was repeatedly stated: “The landscape is magnificent and we [participant and his dog] just walk” (Jürgen, 82); and “When I walk, I see a lot. I can observe nature, I can watch the animals” (Anton, 70). This is consistent with an overall positive, but realistic, attitude towards ageing within this group. Self-knowledge and personal development were perceived to be the gains of ageing whereas increasing limitations and the loss of social contacts were mentioned as negative aspects, yet these aspects were considered to be normal.
Adapting
With only four participants assigned, the adapting group is considerably smaller than the previous group and overall the most heterogeneous group. For sociodemographic characteristics, only two stand out: both of the study participants who resided in care facilities were found in this group, and three out of four were male participants. Furthermore, chronic physical limitations that resulted in a decline in the physical activity levels were found in all four participants in this group. While their physical constraints affected the intensity and frequency of physical activity, these participants described that they had adapted to their limitations and therefore considered their activity level to be sufficient. Going for walks and doing stretches were mentioned most often as intentional physical activity in addition to some household or gardening chores.
For two of the participants, their physical activity was attributed to physical benefits, but more importantly to psychological well-being, specifically to socializing with others through physical activity: “I have two good friends. One comes every Thursday and Sunday and the other one comes as well and we walk. It is wonderful” (Bettina, 83).
No negative consequences of physical activity were mentioned in this group whereas inactivity was associated with a decrease in overall health and psychological well-being: “Oh, I would be worse off. What would I do? Well, I would have to become mentally active” (Albert, 91).
The three male participants in this group experienced competence when they managed to achieve goals such as walking a longer distance and, conversely, a perceived loss of competence when they were unable to meet their goals because of physical limitations: “I added another kilometre once in a while, expanding my walk bit by bit. This makes walking worthwhile” (Heinrich, 88); and “It is a loss. … Yes, that I can’t achieve anymore what I used to achieve” (Albert, 91).
While enjoyment, and thus intrinsic motivation, was not mentioned in connection to physical activity within this group, psychological satisfaction, particularly regarding competence and relatedness, was mentioned as both a perceived consequence and motivation to engage in physical activity.
The above-described acceptance of the participants’ physical limitations and resulting decline in activity is reflected in this group’s perception of ageing: while they are looking forward to further positive experiences in their lives, they perceive their physical limitations as a personal, but normal, loss.
Persevering
Three participants indicated that they exercise both with moderate and vigorous intensity but considered their activity level to be insufficient. Although this group is rather small compared to the mastering group, assigned participants share many characteristics. All members in this group are in the younger age group, less than 80 years of age, and have a high net income and no migrant background. All are married and in regular contact with their children, and participants in this group considered their close relatives, such as partners, children and grandchildren, to be the most influential reference groups, followed by friends.
The two male participants experienced chronic diseases and resulting physical limitations, and the only woman in this group indicated that she had some physical constraints including joint pain because she was overweight.
The awareness of a wide range of physical benefits of exercise was noticeable among these participants: better sleep, fewer cardiovascular problems and other risk factors associated with chronic and age-related diseases, lower body weight, and an overall improved health status were mentioned. Similarly, more heart problems, weight gain, and a loss of energy were associated with inactivity.
Additionally, participants also appeared to value psychological benefits accompanying physical activity: “I would potentially have more social relationships, because exercising in a group brings pleasure” (Andreas, 69); and “It calms me down. You follow a predetermined cycle of exercises and just let your mind wander” (Georg, 76).
Whereas persevering participants were the only ones who did not mention any external barriers such as a lack of financial resources, internal barriers were perceived to be high. The two male participants were both involved in gardening and caretaking activities around their houses, which resulted in a lack of time for exercise. Moreover, all participants cited that they struggled with their weaker self, specifically when they felt exhausted from other assignments or because of physical limitations. Two participants perceived increased pleasure and consequently higher willingness to participate in exercise if they were part of a group: “It’s more fun to be with others than being on your own. No, that’s not enjoyable” (Christine, 68).
All participants identified one physical activity that they truly enjoyed and which elicited a feeling of “ease”Footnote2 (Christine, 68) or pleasure in them. However, none of the participants performed their favourite activity regularly and the exercise they participated in was rather extrinsically motivated to manage chronic disease or related risk factors. Despite perceiving local exercising offers as sufficient, respondents indicated that they very seldom participated in these activities.
A positive perspective towards getting older was found among all participants in this group and the hope of spending more years with their loved ones: “Some more shared experiences with my wife. Who knows who has to go first?” (Georg, 76).
Struggling
Four participants who cited that they did not exercise with vigorous intensity and an overall insufficient activity level were assigned to the group struggling. Three out of four participants were 80 years of age or older and all but one experienced multiple and mutually enhancing chronic physical limitations that impeded vigorous intense physical activities completely and even moderate activities on some days. For other sociodemographic characteristics such as gender, marital status, migration background, and net income, this group is heterogeneous.
The articulated perceived benefits of being physically active and, conversely, negative consequences of inactivity, were diverse in this group. Feelings of autonomy, psychological well-being, and increased mobility and muscle strength were most cited whereas only one participant mentioned an impact of exercising on the ageing process.
Notably missing in this group were feelings of pleasure or joy connected to physical activity. Doing stretches and going for walks, the two most commonly cited practices or activities, were described as sometimes painful or in other ways demotivating: “As an old person, you have to be very much alert when you go out. You first have look around to not be run over … One has to pay attention, as some people jostle” (Anna, 76).
Moreover, three participants cited staying at home and reading as their favourite pastime.
Close relatives as important reference people were not as important in this group as in other groups because two of the participants were widowed and only one out of four reported to be closely in touch with their children. An overall lack of social support was perceived as a factor impeding increased physical activity for some participants. In the case of an immigrant, however, who reported to miss his home country and the many contacts he used to have, the lack of social support initiated increased activity as he sought to meet other like-minded people at a local mosque or community centre: “In the mosque where I am, there are many many Muslim people, more than 1,000 are in the mosque. We divide them into different parties where we speak. Sometimes they say ‘this man, he will speak, he should speak’ and I enjoy it” (Edward, 82).
While participants in this group perceived some positive aspects of ageing such as increased self-knowledge, the negative implications of getting older tended to prevail in this group: “It becomes clear that some things will never come back. The pleasant period of life is over. This is one of those cases when you would say ‘that’s it’ ” (Karl, 80).
Comparison and contrast between groups
The classification of four groups, divided by different intensity and perceived sufficiency of activity levels, allowed us to identify older adults with similar as well as distinctive beliefs and motives towards physical activity.
The presence or absence of chronic diseases and physical limitations did not appear to be a distinctive feature within our sample, because most participants reported having some constraints. However, participants differed in how they dealt with physical limitations. While some used physical activity to soften the impact of chronic diseases (mastering) or maintained enjoyable physical activities within their capabilities (adapting), others failed to engage in physical activities due to chronic pain (struggling) or due to internal barriers and rather extrinsic motivation (persevering).
Participants who perceived their activity level as sufficient (mastering and adapting) appeared to be more self-determined and intrinsically motivated to engage in physical activity than the two remaining groups. Among these participants, physical activity contributed to the satisfaction of basic physiological needs. Those engaging in joint physical activity tended to emphasize perceived relatedness in the process of physical activity, and competence and autonomy were described as consequences of physical activity. Unlike those with insufficient activity levels, mastering and adapting respondents all cited at least one regularly performed activity that elicited joy and pleasure within them.
Behavioural beliefs towards physical activity were overwhelmingly positive within these two groups and the only negative consequences cited among the mastering participants were attributed to their own overexertion. Participants in both groups were well aware of their own physical, internal, and external constraints. However, they did not perceive these barriers as obstacles impeding their physical activity but found a way to overcome them or adapt their activities to them.
About one-third of study participants, divided into two groups (persevering and struggling), perceived that their physical activity level was insufficient. Whereas age did not appear to be a distinctive factor among the two previous groups, those classified as persevering were younger and realized intensifying limitations; participants struggling to maintain moderate physical activity were considerably older and reported more physical limitations. The behavioural beliefs encompassing wide ranging benefits and almost complete absence of negative consequences of physical activity were similar to the previous groups. While persevering participants emphasized the preventative contribution of physical activity in reducing the risk of further constraints, struggling participants attributed it to maintaining their mobility and independence. Participants in these groups appeared to perceive multiple influential control factors that impeded their physical activity behaviour. A perceived lack of joy and pleasure in their regularly performed physical activity was a noticeable and distinguishing characteristic among insufficiently active groups compared to those with self-reported satisfying activity levels. Moreover, various internal and external constraints and resulting control beliefs appeared to prevail and hinder participants from becoming more active. The weaker self and a lack of partners in exercise were commonly mentioned in both groups. While persevering participants cited a lack of time and energy after their daily chores as barriers, struggling respondents associated pain and an inadequate infrastructure as obstructive barriers.
Discussion
A worldwide, increased life expectancy and the impact of physical inactivity on age-related and chronic diseases support the pressing need to better understand the factors that enable and impede age-appropriate physical activity of individuals aged 65 years and above.
Due to differences in people’s biographies, living conditions, social and ethnic backgrounds, as well as their overall physical and psychological conditions, our target group is very heterogeneous. However, the complex relationship between these factors as well as motivations and beliefs underlying physical activity behaviour remain under-theorized and under-researched for this age group. This knowledge gap was addressed in our study by combining two well-established theories in physical activity research: TBP and SDT. In order to explore the complex relationships between the different theoretical constructs and to meet the specific perceptions of our target group, we used a qualitative approach. Our study had two purposes: first, to explore different beliefs about physical exercise among older adults in Germany and second, to examine the interplay of motivational factors, TPB beliefs, and sociodemographic characteristics with variations in physical activity.
Regarding the first aspect, beliefs about physical activity, our findings are largely consistent with other study’s findings (Benjamin et al., Citation2005; Brenes et al., Citation1998; Conn, Citation1998; Courneya, Citation1995; Dye & Wilcox, Citation2006; Helm, Citation1987; Kosteli et al., Citation2016; Lin et al., Citation2007; Michels & Kugler, Citation1998; Schmidt et al., Citation2016), yet add various new aspects. In accordance with all previous studies, older adults in our research perceived a large variety of positive consequences of physical activity for their physical as well as their psychological health. Apart from known factors such as increased mobility and weight loss, participants in this study mentioned that physical activity may slow down the ageing process. In addition, we were able to classify consequences for the psychological well-being more profound by referring to SDT and the satisfaction of the three basic psychological needs—relatedness, competence, and autonomy. Some previous studies have already mentioned beliefs that refer to these aspects but did not link them to SDT. Relatedness is reflected in other study results indicating that physical activity may serve to meet and interact with other people (Kosteli et al., Citation2016) and limit loneliness (Lin et al., Citation2007). Feelings of competence as a result of older adults’ physical activity have been mentioned in other studies as perception of confidence (Conn, Citation1998) or achievement (Kosteli et al., Citation2016). Especially for our male participants it was important to be able to still achieve goals in spite of growing older. Last, we found that physical activity may be linked to autonomy. This is in line with the fact that it is crucial for older adults to maintain their independence (Michels & Kugler, Citation1998). Negative consequences of physical activity were noted scarcely by our participants, but were related to overexertion and accident risk, as the fear of falling is a relevant issue for older adults (Schmidt et al., Citation2016).
Seniors across various studies have mentioned medical professionals, friends, and close family members as important reference groups that have a normative influence on whether they become active (Benjamin et al., Citation2005; Brenes et al., Citation1998; Conn, Citation1998; Helm, Citation1987; Lin et al., Citation2007; Michels & Kugler, Citation1998). For older adults, not just children but also grandchildren should be considered. Apart from that, our study highlighted influential social connections from cultural and religious groups as well as neighbours. With regard to control beliefs participants mentioned a range of barriers and facilitators that have been cited in previous studies (Benjamin et al., Citation2005; Brenes et al., Citation1998; Conn, Citation1998; Courneya, Citation1995; Dye & Wilcox, Citation2006; Kosteli et al., Citation2016; Lin et al., Citation2007; Schmidt et al., Citation2016) such as social support/sport fellows, adequate infrastructure, resources, time, joy, weather conditions, physical limitations and the “weaker self”, meaning a lack of motivation. For some people, this results from a lack of variety in the possibilities of being physically active. Moreover, older adults may depend on instrumental support (Benjamin et al., Citation2005), for example, in terms of transportation. These specific barriers may be related to the residential environment of older adults. In our sample, about half of the participants lived in structurally weak areas, i.e., in rural areas or on the outskirts of cities.
To address our second research purpose, we classified participants into four different groups based on their reported past activity level. By this we provide practical insights into the underpinning factors that precede physical (in)activity in this diverse age group. These findings may be used to inform the conceptualization of interventions to promote increased physical activity in old age. For example, the knowledge of physical and psychological benefits resulting from physical activity and the negative consequences of inactivity was high across the entire sample population. However, people differed regarding intrinsic vs. extrinsic motivation and the ability to overcome barriers to physical activity. While intrinsic motivation is characterized by an inherent pleasure to perform an activity and is highly autonomous, extrinsically motivated behaviour is solely performed because of external pressures, like reward, punishment, or social influences. People who failed to engage in more physical activities were rather extrinsically motivated. Existing research underlines the high relevance of intrinsic motivation for the maintenance of physical activity (Kirkland et al., Citation2011; Springer et al., Citation2013; Stephan et al., Citation2010). Intrinsic motivation is closely linked to the satisfaction of basic psychological needs (Deci & Ryan, Citation2000). Our results show that physical activity can fulfil older adults’ needs of competence, relatedness, and autonomy. Communicating not only the health-related benefits of physical activity, but also its relation to feeling competent, related to others, and autonomous, may foster intrinsic motivation. Concrete messages could be for example, “Physical activity can give you that good feeling of being able to accomplish something”, “A positive side effect of physical activity is that it allows you to connect with other people”, and “Exercising can help you to maintain your independence”. Moreover, older adults who perceived their activity levels as sufficient, found ways to challenge their weaker self or adapt their activities to external barriers. In contrast, older adults who perceived their activity level as insufficient, perceived a lot of internal and external barriers, e.g., chronic pain and lack of support. Health promotion strategies should address these constraints and show older adults how to adapt activities to age-related physical limitations and where to find support. Especially for people with physical limitations, it can be difficult to find like-minded people who share the same activity level. Different health promotion programmes should therefore be offered to people with different abilities and varying prior experience regarding exercising. Interactive elements may be incorporated into the programmes so that participants can connect with each other. Ideas for group activities outside the programme (e.g., joint walks) could also be communicated.
Limitations
However, these results have to be interpreted against the background of some limitations. First, the response rate of older migrants was low. Whereas migrants from Eastern European countries and Russia are represented in the sample, we were not able to recruit participants with a Turkish background, the largest ethnic minority in Germany (Federal Institute for Population Research, Citation2018). Second, we did not partition beliefs for different types of physical activity categories. Studies suggest, however, that control, normative, and behavioural beliefs are relative and might differ for different target behaviours (Rhodes et al., Citation2007), e.g., walking, exercising at a gym, and doing physically demanding domestic work. This suggests that further differentiation between various types of physical activity and their associated beliefs might be necessary. Our third limitation resides in relying exclusively on self-assessment of physical activity behaviour by the respondents, which may be biased. Finally, our analysis and resulting group typology reflect our data collected from a fairly active sample. Our findings may not be exhaustive or applicable to a different context.
Future research should test the assumptions of SDT and TPB simultaneously to identify their relevance for predicting and promoting physical of activity. Our findings already showed that the combination of these two theories may be useful and can explain more compared to focusing on just one of these theories. Studies with a quantitative design could show which aspects of SDT and TPB are decisive and should be addressed in health campaigns. Particularly, it must be clarified which of the numerous beliefs do have the strongest influence on determinants of being physically active in different sub-groups of older adults.
Conclusion
Despite its methodological limitations, the results of our study indicate that older adults differ with regards to their predispositions and motivational states, which in turn shapes their behavioural beliefs and activity behaviour. To support older people in overcoming their physical limitations or other specific barriers and finding appropriate physical activity strategies, these differences should be taken into account. Combining SDT and TPB provides explanations for many of the antecedents of physical activity, integrating different qualities of motivations as well as individual belief systems.
Disclosure of potential conflicts of interest
The authors declare that there is no conflict of interest.
Ethics approval
The Ethics Committee of the University of Erfurt provided approval for this study.
Additional information
Funding
Notes on contributors
Paula Stehr
Paula Stehr is currently working as a postdoctoral researcher at the University of Erfurt on a project funded by the German Federal Institute for Risk Assessment. She wrote her thesis on the exchange of social support in online communication modes with a focus on the role of those acting prosocially. Moreover, her research deals with evidence-based health communication, health information behavior, and the use of mHealth technologies.
Hanna Luetke Lanfer
Hanna Luetke Lanfer is a researcher at the School of Public Health at the University of Bielefeld. She obtained her PhD in 2021, researching the conditions for effective health campaigns in low-income environments. She focuses on participatory methods with vulnerable groups in different health contexts.
Constanze Rossmann
Constanze Rossmann is professor of communication at the University of Erfurt, Germany. She is cofounder of the Health Communication Division within the German Communication Association. Her research interests generally include health and crisis communication, media use, and media effects. Currently, she focuses on health information seeking, health campaign research, and mobile health in various health contexts.
Notes
1. To ensure integration of these perspectives, the quota plan included three attributes of vulnerable/hard-to-reach groups: migrant background, low SES (concerning income and education), and living in a structurally weakarea. For each of these attributes, at least seven people should be interviewed, whereby it was also possible for more than one characteristic to apply to a single respondent. The actual distribution of participants’ characteristics can be found in .
2. For the full quote from Christine see the paragraph regarding behavioural beliefs in “Beliefs towards physical activity (RQ1)”.
References
- Ahlskog, J. E., Geda, Y. E., Graff-Radford, N. R., & Petersen, R. C. (2011). Physical exercise as a preventive or disease-modifying treatment of dementia and brain aging. Mayo Clinic Proceedings, 86(9), 876–14. https://doi.org/https://doi.org/10.4065/mcp.2011.0252
- Ajzen, I. (2005). Attitudes, personality and behavior. Open University Press/McGraw Hill.
- Alexandris, K., Barkoukis, V., & Tsormpatzoudis, C. (2007). Does the theory of planned behavior elements mediate the relationship between perceived constraints and intention to participate in physical activities? A study among older individuals. European Review of Aging and Physical Activity, 4(1), 39–48. https://doi.org/https://doi.org/10.1007/s11556-007-0014-1
- Armitage, C. J. (2005). Can the theory of planned behavior predict the maintenance of physical activity? Health Psychology: Official Journal of the Division of Health Psychology, American Psychological Association, 24(3), 235–245. https://doi.org/https://doi.org/10.1037/0278-6133.24.3.235
- Benjamin, K., Edwards, N. C., & Bharti, V. K. (2005). Attitudinal, perceptual, and normative beliefs influencing the exercise decisions of community-dwelling physically frail seniors. Journal of Aging and Physical Activity, 13(3), 276–293. https://doi.org/https://doi.org/10.1123/japa.13.3.276
- Biddle, S., Soos, I., & Chatzisarantis, N. (1999). Predicting physical activity intentions using goal perspectives and self-determination theory approaches. European Psychologist, 4(2), 7. https://doi.org/https://doi.org/10.1027//1016-9040.4.4.83
- Brenes, G. A., Strube, M. J., & Storandt, M. (1998). An Application of the theory of planned behavior to exercise among older adults1. Journal of Applied Social Psychology, 28(24), 2274–2290. https://doi.org/https://doi.org/10.1111/j.1559-1816.1998.tb01371.x
- Conn, V. S. (1998). Older women’s beliefs about physical activity. Public Health Nursing (Boston, Mass.), 15(5), 370–378. https://doi.org/https://doi.org/10.1111/j.1525-1446.1998.tb00362.x
- Courneya, K. S. (1995). Understanding readiness for regular physical activity in older individuals: An application of the theory of planned behavior. Health Psychology: Official Journal of the Division of Health Psychology, American Psychological Association, 14(1), 80–87. https://doi.org/https://doi.org/10.1037//0278-6133.14.1.80
- D’Angelo, M. S., & Reid, R. D. (2007). A model for exercise behavior change regulation in patients with heart disease. Journal of Sport & Exercise Psychology, 29(2), 208–224. https://doi.org/https://doi.org/10.1123/jsep.29.2.208
- Deci, E. L., & Ryan, R. M. (2000). The ‘what’ and ‘why’ of goal pursuits: Human needs and the selfdetermination of behaviour. Psychological Inquiry, 11(4), 227–268. https://doi.org/https://doi.org/10.1207/S15327965PLI1104_01
- Deci, E. L., & Ryan, R. M. (2008). Self-determination theory: A macrotheory of human motivation, development, and health. Canadian Psychology/Psychologie Canadienne, 49(3), 182–185. https://doi.org/https://doi.org/10.1037/a0012801
- Downs, D. S., & Hausenblas, H. A., [Heather A.]. (2005a). Elicitation studies and the theory of planned behavior: A systematic review of exercise beliefs. Psychology of Sport and Exercise, 6(1), 1–31. https://doi.org/https://doi.org/10.1016/j.psychsport.2003.08.001
- Downs, D. S., & Hausenblas, H. A., [H. A.]. (2005b). The theories of reasoned action and planned behavior applied to exercise: A meta-analytic update. Journal of Physical Activity & Health, 2(1), 76–97. https://doi.org/https://doi.org/10.1123/jpah.2.1.76
- Dye, C. J., & Wilcox, S. (2006). Beliefs of low-income and rural older women regarding physical activity: You have to want to make your life better. Women & Health, 43(1), 115–134. https://doi.org/https://doi.org/10.1300/J013v43n01_07
- Edmunds, J., Ntoumanis, N., & Duda, J. L. (2008). Testing a self-determination theory-based teaching style intervention in the exercise domain. European Journal of Social Psychology, 38(2), 375–388. https://doi.org/https://doi.org/10.1002/ejsp.463
- Federal Centre for Health Education. (2013). Alte Menschen - Expertise zur Lebenslage von Menschen im Alter zwischen 65 und 80 Jahren [Older adults - Expertise on the living conditions of people between 65 and 80 years] (No. 44). Bundeszentrale für gesundheitliche Aufklärung. http://www.alter-sucht-pflege.de/Informationsmaterial/pdf/BZgA_Menschen%20zwischen%2065%20und%2080.pdf
- Federal Institute for Population Research. (2018). Bevölkerung mit Migrationshintergrund nach den häufigsten Herkunftsländern/-regionen [Population with migration background according to the most common countries/regions of origin]. Bundesinstitut Für Bevölkerungsforschung. https://www.bib.bund.de/DE/Fakten/Fakt/B48-Bevoelkerung-mit-Migrationshintergrund-Herkunft.html;jsessionid=CFE82DA171852983D44B00F9FC7FF403.1_cid389?nn=9992206
- Federal Statistical Office (Ed.). (2019, June 27). Bevölkerung im Wandel [Changing population]: Annahmen und Ergebnisse der 14. koordinierten Bevölkerungsvorausberechnung [Assumptions and results of the 14th coordinated population projection]. https://www.destatis.de/DE/Presse/Pressekonferenzen/2019/Bevoelkerung/pressebroschuere-bevoelkerung.pdf;jsessionid=018DFAE48C510FA2489E542FBB5F56FD.internet8732?__blob=publicationFile
- Fishbein, M., & Ajzen, I. (2010). Predicting and changing behavior. The reasoned action approach. Taylor & Francis.
- Flick, U. (2009). An introduction to qualitative research. Sage.
- Gretebeck, K. A., Black, D. R., Blue, C. L., Glickman, L. T., Huston, S. A., & Gretebeck, R. J. (2007). Physical activity and function in older adults: Theory of planned behavior. American Journal of Health Behavior, 31(2), 203–214. https://doi.org/https://doi.org/10.5993/AJHB.31.2.9
- Hagger, M. S., & Chatzisarantis, N. L. D. (2009). Integrating the theory of planned behaviour and self-determination theory in health behaviour: A meta-analysis. British Journal of Health Psychology, 14(2), 275–302. https://doi.org/https://doi.org/10.1348/135910708X373959
- Hagger, M. S., Chatzisarantis, N. L. D., & Biddle, S. J. H. (2002). A meta-analytic review of the theories of reasoned action and planned behaviour in physical activity: Predictive validity and the contribution of additional variables. Journal of Sport & Exercise Psychology, 24(1), 3–32. https://doi.org/https://doi.org/10.1123/jsep.24.1.3
- Hamer, M., [Mark], Lavoie, K. L., & Bacon, S. L. (2014). Taking up physical activity in later life and healthy ageing: The English longitudinal study of ageing. British Journal of Sports Medicine, 48(3), 239–243. https://doi.org/https://doi.org/10.1136/bjsports-2013-092993
- Hausenblas, H. A., [Heather A.], Carron, A. V., & Mack, D. E. (1997). Application of the theories of reasoned action and planned behavior to exercise behavior: A meta-analysis. Journal of Sport & Exercise Psychology, 19(1), 36–51. https://doi.org/https://doi.org/10.1123/jsep.19.1.36
- Helm, G. R. (1987). Exercise and exercise intentions on the part of the older adult: An examination of the theory of reasoned action and measurement of the subjective norm. University of Nebraska. BibTeX. https://core.ac.uk/display/18189214
- Kirkland, R., Karlin, N., Stellino, M., & Pulos, S. (2011). Basic psychological needs satisfaction, motivation, and exercise in older adults. Activities, Adaptation & Aging, 35(3), 181–196. https://doi.org/https://doi.org/10.1080/01924788.2011.596764
- Kosteli, M. C., Williams, S. E., & Cumming, J. (2016). Investigating the psychosocial determinants of physical activity in older adults: A qualitative approach. Psychology & Health, 31(6), 730–749. https://doi.org/https://doi.org/10.1080/08870446.2016.1143943
- Ku, P. W., Fox, K. R., & Chen, L. J. (2016). Leisure-time physical activity, sedentary behaviors and subjective well-being in older adults: An eight-year longitudinal research. Social Indicators Research, 127(3), 1349–1361. https://doi.org/https://doi.org/10.1007/s11205-015-1005-7
- Kuckartz, U. (2013). Qualitative text analysis: A guide to methods, practice & using software. Sage. https://books.google.de/books?id=9B2VAgAAQBAJ
- Lin, Y. C., Huang, L. H., Young, H. M., & Chen, Y. M. (2007). Beliefs about physical activity - focus group results of Chinese community elderly in Seattle and Taipei. Geriatric Nursing (New York, N.Y.), 28(4), 236–244. https://doi.org/https://doi.org/10.1016/j.gerinurse.2006.12.003
- Michels, T. C., & Kugler, J. P. (1998). Predicting exercise in older Americans: Using the theory of planned behavior. Military Medicine, 163(8), 524–529. https://doi.org/https://doi.org/10.1093/milmed/163.8.524
- Pereira, C. L. N., Vogelaere, P., & Baptista, F. (2008). Role of physical activity in the prevention of falls and their consequences in the elderly. European Review of Aging and Physical Activity, 5(1), 51–58. https://doi.org/https://doi.org/10.1007/s11556-008-0031-8
- Rhodes, R. E., Blanchard, C. M., & Matheson, D. H. (2007). Motivational antecedent beliefs of endurance, strength, and flexibility activities. Psychology, Health & Medicine, 12(2), 148–162. https://doi.org/https://doi.org/10.1080/13548500500429346
- Robert Koch-Institute. (2017). Health-enhancing physical activity during leisure time among adults in Germany. Journal of Health Monitoring, 2(2), 35–42. https://doi.org/https://doi.org/10.17886/rki-gbe-2017-040
- Rossmann, C. (2015). Strategic health communication: Theory- and evidence-based campaign development. In D. Holtzhausen & A. Zerfass (Eds.), The Routledge handbook of strategic communication (pp. 409–423). Routledge.
- Russell, K. L., & Bray, S. R. (2009). Self-determined motivation predicts independent, home-based exercise following cardiac rehabilitation. Rehabilitation Psychology, 54(2), 150–156. https://doi.org/https://doi.org/10.1037/a0015595
- Sanchez-Lopez, J., Silva-Pereyra, J., Fernández, T., Alatorre-Cruz, G. C., Castro-Chavira, S. A., González-López, M., & Sánchez-Moguel, S. M. (2018). High levels of incidental physical activity are positively associated with cognition and EEG activity in aging. PLoS One, 13(1), e0191561. https://doi.org/https://doi.org/10.1371/journal.pone.0191561
- Schaeffer, D., Berens, E. M., & Vogt, D. (2017). Health literacy in the German population. Deutsches Ärzteblatt International, 114(4), 53–60. https://doi.org/https://doi.org/10.3238/arztebl.2017.0053
- Schmidt, L., Rempel, G., Murray, T. C., McHugh, T. L., & Vallance, J. K. (2016). Exploring beliefs around physical activity among older adults in rural Canada. International Journal of Qualitative Studies on Health and Well-Being, 11(1), 32914. https://doi.org/https://doi.org/10.3402/qhw.v11.32914
- Schreier, M. (2012). Qualitative content analysis in practice. Sage.
- Schreier, M. (2014). Varianten qualitativer Inhaltsanalyse: Ein Wegweiser im Dickicht der Begrifflichkeiten [Ways of doing qualitative content analysis: Disentangling terms and terminologies]. Forum Qualitative Sozialforschung/Forum: Qualitative Social Research, 15(1), 27. https://doi.org/https://doi.org/10.17169/fqs-15.1.2043
- Smith, L., & Hamer, M. (2014). Television viewing time and risk of incident diabetes mellitus: The English Longitudinal Study of Ageing. Diabetic Medicine: A Journal of the British Diabetic Association, 31(12), 1572–1576. https://doi.org/https://doi.org/10.1111/dme.12544
- Springer, J. B., Lamborn, S. D., & Pollard, D. M. (2013). Maintaining physical activity over time: The importance of basic psychological need satisfaction in developing the physically active self. American Journal of Health Promotion: AJHP, 27(5), 284–293. https://doi.org/https://doi.org/10.4278/ajhp.110211-QUAL-62
- Stephan, Y., Boiché, J., & Le Scanff, C. (2010). Motivation and physical activity behaviors among older women: A self-determination perspective. Psychology of Women Quarterly, 34(3), 339–348. https://doi.org/https://doi.org/10.1111/j.1471-6402.2010.01579.x
- Teixeira, C. M., Vasconcelos-Raposo, J., Fernandes, H. M., & Brustad, R. J. (2013). Physical activity, depression and anxiety among the elderly. Social Indicators Research, 113(1), 307–318. https://doi.org/https://doi.org/10.1007/s11205-012-0094-9
- United Nations. (2019). World population ageing 2019. https://www.un.org/en/development/desa/population/publications/pdf/ageing/WorldPopulationAgeing2019-Report.pdf
- VERBI Software. (2018). MAXQDA - Software für qualitative Datenanalyse [Computer software].
- Wilson, P. M., Mack, D. E., & Grattan, K. P. (2008). Understanding motivation for exercise: A self-determination theory perspective. Canadian Psychology/Psychologie Canadienne, 49(3), 250–256. https://doi.org/https://doi.org/10.1037/a0012762
- World Health Organization. (n.d. a). Physical activity and older adults. http://www.who.int/dietphysicalactivity/factsheet_olderadults/en/
- World Health Organization. (n.d. b). What is moderate-intensity and vigorous-intensity physical activity? http://www.who.int/dietphysicalactivity/physical_activity_intensity/en/
- World Medical Association. (2013). WMA Declaration of Helsinki – Ethical principles for medical research involving human subjects. https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects