

What was the Impact of the New MI Definition in Israel?
A. Porath, A. B. Jotkowitz, N. Lieberman, V. Novack1
Departments of Internal Medicine, Soroka University Medical Center, Beer‐Sheba, Clalit Health Services, Israel;1Harvard Clinical Research InstituteBoston, USA. Clalit Health Services, Tel‐Aviv, Israel
Objective: To assess the impact of change in diagnostic criteria on the incidence, management, and outcome of all major types of ACS: non‐ST elevation acute coronary syndrome (NSTE ACS): unstable angina (UA) and non‐ST elevation myocardial infarction (NSTE MI), and ST‐elevation myocardial infarction (STEMI).
Design: Retrospective cohort analysis from a large, integrated data base of the Clalit Health Services.
Setting: Non‐governmental, not‐for profit, acute hospitals in Israel.
Patients: Patients' population was comprised from all STEMI and NSTE ACS admissions during a 5 year period (1999–2004). During period 1 CK‐MB was the biomarker for the diagnosis of myocardial infarction, while during period 2 troponin was used for this diagnosis. 35,790 consecutive patients with ACS, 20,206 recruited before (period 1) and 15,584 after (period 2) the transition to the new diagnosis guidelines. Among these, 14,037 were admitted for NSE‐ACS in perio1 and 11,643 in period 2.
Findings:
While global incidence of ACS and STEMI remained unchanged, there was redistribution in NSTE ACS diagnoses from UA cases to NSTEMI.
There was an immediate increase in rate of PCA in NSTE ACS.
A minimal change in length of hospital stay was noted.
Total disease costs increased by 10%.
Despite a period‐effect decline in 1‐year mortality for NSTE ACS [from 8.5% to 7.7% for UA and from 28.1% to 24.6% for NSTE MI], and a time‐trend decline in STEMI mortality, the global ACS Mortality remained unchanged, as a result of a statistical paradox [the Simpson's Paradox].
The gender difference in NSTE ACS mortality that was prominent in period 1 (higher mortality rate in women), has disappeared in period 2.
The marked time‐trend decrease in mortality was strongly driven by improved secondary prevention. Each of the 4 major drug categories: Beta blockers, ACE‐I /ARBs, Aspirin and Statins, as assessed by post‐discharge purchasing data, have eliminated the significance of a time‐trend effect in multivariable survival analysis.
Conclusion: This national‐scale data indicates that the new guidelines had an important and positive effect on the management and outcomes of ACS.
Figure 1. Monthly Incidence by Period, stratified by type of ACS. Months before(period 1) and after transition (period 2).
Figure 2. 1‐year Mortality, by type of ACS. Months before (period 1) and after transition (period 2).
Current Status of the Chest Pain Unit
E. A. Amsterdam, MD, Chief of Cardiology
University of California at Davis, Sacramento CA, USA
Evaluation of patients presenting to the ED with chest pain (CP) remains a major challenge despite the development of an array of innovative diagnostic methods. CP accounts for over 8 million ED visits/yr and 2 million hospital admissions in the U.S. at a cost of more than 8 billion dollars. However, a coronary event is confirmed in less than one‐third of these patients. This patient population poses a dilemma for the clinician because failure to admit a patient with ACS may result in catastrophic outcome while unnecessary admission for a benign process is costly and may involve needless tests and risk.
At the time of the development of the CCU 50 years ago, Lown advocated that “patients should be admitted to the CCU solely on suspicion of having a myocardial infarction”. This approach persisted until recently because of the focus on patient welfare and the litigation potential of missed MI. The most recent data on missed ACS indicates a rate of ∼4% but this reflects data from over a decade ago. However, a consequence of a low admission threshold is large numbers of unnecessary hospitalization, suboptimal management and inefficient resource utilization. The recent development of CPUs is a response to these challenges by development of a safe, accurate and cost‐effective approach to patients presenting with possible ACS.
CPUs are centers for management of low (but not no) risk patients presenting to the ED with CP. Well established indicators of low risk include clinical stability, no ECG evidence of ischemia/injury and normal initial cardiac injury markers. These patients can be observed in the CPU where they receive an accelerated diagnostic protocol (ADP) which comprises observation, serial ECGs and injury markers over a 4–8 hour period. If this evaluation confirms absence of ischemia/injury at rest, patients undergo a further test to exclude inducible ischemia, usually by exercise treadmill testing. However, depending on expertise, custom and resources, this test may be stress myocardial scintigraphy, echocardiography, contrast perfusion echocardiography, multslice CT coronary angiography, invasive angiography, MRI or other evolving approaches. If the final test is negative, the patient may be discharged for outpatient follow‐up. The importance of the predischarge test cannot be overemphasized, as it is the final step in supporting clincal stability. This approach has demonstrated confirmation of ACS in <5% of patients admitted to the CPU. Patients in whom clinical status, ECG, or markers indicate an ACS while under observation in the CPU are hospitalized directly from the CPU, as are those with a positive predischarge stress test.
Opinions vary on the optimal cardiac test following negative serial markers and ECGs in the CPU. The diverse methods, expertise and resources have given rise to many studies demonstrating the advantages and limitations of each approach. The majority of experience is with treadmill exercise testing but stress scintigraphy and echocardiography have also been utilized with excellent results. A substantial minority (25–30%) of patients cannot exercise and undergo pharmacologic imaging studies. Recently, CT coronary angiography has been applied in low risk patients presenting to the ED with CP. While this method is reliable when completely normal, there is a relatively high rate of uncertain diagnostic results, for which patients then receive invasive coronary angiography entailing a second contrast load and raditation exposure. Studies requirng confirmatory invasive coronary angiography after CT angiography occur in up to 40% of patients and the majority of these have not shown obstructive CAD, indicating a low positive predictive value of CT angiography.
As indicated above, low risk in patients presenting with CP is indicated by clinical stability, normal (or unchanged) ECG, and negative initial injury markers. At UC Davis, patients with a prior history of CAD who fulfill these criteria are included in the CPU population. Additionally, it is emphaszied that the TIMI risk score for patients with NSTE ACS (age >65, >3 CAD RFs, known CAD, ASA past 7 days, >2 CP episodes past 24 hrs., ST abn, + marker) does not apply to candidates for the CPU, since this score is based on patients with documented ACS based on objective evidence (ECG or markers) of ischemia/injury. The presence of these latter factors precludes admission to the CPU since they reflect high risk.
Experience with the CPU approach has established its utility. Low risk patients are identifiable. An ADP that includes a cardiac functional test (or other method for detection of ischemia/CAD) detects the small minority of this group with ACS. There are no reports of adverse effects of ET as part of an ADP. The rate of positive treadmill tests is ∼15% (0–25%) and the positive predictive value is ∼33%. Although the latter value might appear poor, it is important to note that it represents 1/3 of only 15% of patients. This is in contrast to CT coronary angiography in which the proportion of patients requiring confirmatory invasive coronary angiography is substantially higher. Follow‐up of 30 days to over 6 months in patients with negative ADPs using ET, nuclear or echo stress studies indicates a very low rate of cardiac events: ∼1%, with no mortality in our UC Davis series of >5000 patients evaluated by our method during the past decade and a half.
It has been shown that exercise testing as part of an ADP is more readily available and more cost‐effective than nuclear or other stress imaging studies and its safety and accuracy are excellent. Endpoints of the test differ from those in outpatients referred for elective testing. Although we employ maximum, symptom‐limited stress testing, the test is stopped at the initial evidence of ischemic symptoms or signs. For patients who are unable to exercise (∼1/3 of our CPU population), we utilize stress imaging (nuclear or echo).
The optimal strategy for this group of patients continues to evolve and newer methods are receiving careful evaluation. In addition to those noted above, we are evaluating peripheral arterial tonometry by digital plethysmography to assess peripheral endothelial function, which provides insight into coronary endothelial function and the likelihood of CAD and ACS. We are also assessing the utility of myeloperoxidase, a recently refined biomarker of inflammation and cardiac ischemia/injury, for early detection of plaque instability and rupture. CT coronary angiography continues to improve and should require fewer confirmatory invasive angiograms. Cardiac MRI has also been introduced for assessment of this population of patients. Whether these newer approaches will extend or replace the established strategies awaits further trials.
CPUs are established centers for assessment of low risk patients presenting to the ED with symptoms suggestive of ischemia. Most CPUs utilize an ADP that culminates in an exercise test (or other functional/anatomic test) in patients with negative observation data. If this evaluation is negative, the patient is discharged; if positive, the patient is admitted. The utility of this strategy is excellent and has afforded optimal utilization of resources while maintaining patient safety. A variety of newer diagnostic approaches are currently being applied to this patient population with the goal of further improving their evaluation.
Hand‐carried ultrasound for evaluation of chest pain in the ER
Shaul Atar, MD
Cardiac Intensive Care Unit, Ha'emek Medical Center, Afula, Israel
The hand‐carried cardiac ultrasound (HCU) device is a portable echocardiography device, battery‐operated, lightweight in the size of a laptop computer Citation[1]. Several recently published studies have demonstrated a remarkable increase in diagnostic accuracy by both cardiologists and non‐cardiologists when they added a brief cardiac ultrasound study to their conventional physical examination. A study by Rugolotto Citation[2] found that a 6 minute HCU examination in 55 patients in an intensive care unit changed 40% of their initial diagnosis or diagnostic likelihood and modified management in 24% of the patients. Severe left ventricular dysfunction, severe aortic stenosis, pericardial effusion with tamponade were among the 22 unexpected pathologies found by the HCU operator.
Its bedside availability makes it useful for the rapid and efficient detection of wall motion abnormalities in the emergency room (ER), as well as the detection of non‐cardiac etiologies for chest pain and risk stratification. Emergency and critical care physicians after short training in ultrasonography have used compact ultrasound units as complement of their physical examination to triage of patients with chest trauma, to identify treatable causes of pulseless cardiac activity, and to diagnose pericardial effusion and pulmonary embolism. Using a focused ultrasound examination, emergency physicians changed their first diagnosis in 26% and their management in 18% of the patients Citation[1].
Acute chest pain is a common complaint for patients presenting to emergency departments. ECG results and biochemical markers have strong positive predictive value, yet HCU may have a strong negative predictive value in these cases. Weston et al. Citation[3] studied 150 patients with symptoms suggestive of acute coronary syndrome (ACS), non‐diagnostic ECG, and normal biochemical markers, and hypothesized that HCU‐documented normal left ventricular function is not associated with a clinical diagnosis of acute myocardial ischemia or infarction, nor an ischemic event within 30 days of follow‐up. The incidence of acute myocardial infarction was 2.5% in the normal HCU group and 20% in the abnormal HHE group (P = .002). The negative predictive value of HHE was 91%. The authors concluded that the results suggest a possible role for HCU in providing additional diagnostic and prognostic information in the examination of patients with a low likelihood of myocardial ischemia or infarction and symptoms suggestive of ACS.
A study by Atar et al. Citation[4] showed that in 70 patients admitted to the ER with chest pain and a normal or non‐diagnostic ECG, HCU had a high concordance with patient's discharge diagnosis of ACS, with a kappa value of 0.80. HCU detected wall motion abnormalities in 14 patients – 5 with previously described as well as new wall motion abnormalities, and 9 patients had new wall motion abnormalities. HCU had 100% sensitivity for the detection of ACS, 93% specificity, 71% and 100% positive and negative predictive value, respectively. This study as well shows that HCU has additional clinical value for expediting ER evaluation of chest pain as well as improving the diagnostic accuracy of current algorithms, mainly through its high negative predictive value in patients without regional wall motion abnormalities during an acute episode of chest pain.
However, the diagnosis of segmental wall motion abnormalities, right ventricular dysfunction, and clinically significant pericardial effusion requires a high level of expertise. For instance, the rate of agreement between HCU and standard transthoracic echocardiography for the assessment of regional wall motion by cardiologists with limited echocardiographic training was 80% versus 96% by experienced echocardiologists Citation[5], and residents missed 56% of the cases of right ventricular dysfunction compared to 26% of misdiagnosis by experienced cardiologists Citation[6]. Nevertheless, HCU may increase the sensitivity and predictive value of chest pain triage algorithms, expedite patient triage and assist in decision‐making in the ER, especially in patients presenting a normal or non‐diagnostic ECG.
The role of CT Angiography in acute chest pain triage
E. Konen
Department of Diagnostic Imaging, Sheba Medical center, affiliated to Sackler Faculty of Medicine, Tel‐Aviv University, Ramat Aviv, Israel
Chest pain is the most common presenting symptom of coronary artery disease. Accurate and efficient screening for patients with an acute coronary syndrome is essential. It is estimated that 2% to 10% of patients with an acute coronary syndrome are inappropriately sent home from emergency departments Citation[1]. Missed diagnosis of acute myocardial infarction is associated with significant morbidity, and it is the leading contributor to malpractice claims paid by emergency physicians Citation[2]. The development of Chest Pain Units tries to address these issues using diagnostic protocols which commonly include serial cardiac serum marker evaluations and ECGs, followed by stress testing, with or without radionuclide imaging Citation[3]–Citation[4].
The introduction of the multi‐row detector scanners in the early 2000's ‐ known also as “multi‐detector CT” (MDCT) ‐ was a major technological breakthrough for cardiac imaging. Those scanners use several parallel rows of detectors which enable significant reduction in scan time and reduction in slice width (down to 0.625mm) resulting in improved spatial resolution, a most important factor for imaging of small vessels such as the coronary arteries. Studies comparing 64‐slice multidetector CT with invasive coronary angiography have shown that multidetector CT performs well in the detection of significant coronary stenosis, with sensitivities ranging from 82% to 95% and specificities of 82% to 98%.
Recent articles suggest an important role for MDCT in the evaluation of patients in chest pain units. Gallagher et al. showed that the accuracy of MDCT is at least as good as that of stress nuclear imaging for the detection and exclusion of an acute coronary syndrome in low‐risk chest pain patients. [Ann Emerg Med. 2007;49:125–136]. Appropriateness Criteria for Cardiac Computed Tomography published on October 2006 in JACC rated the appropriate Median score for MDCT in the context of acute chest pain with no ECG changes and serial enzymes negative to be 7 out of 9. Our preliminary experience in Sheba Medical Center using MDCT in the triage of patients submitted to our Chest Pain Unit shows that about 10% of those patients will require coronary catheterization due to MDCT results.
The image bellow on the left shows a cardiac CT angiographic delineation of a tight non‐calcified plaque in the proximal LAD in a 62‐year‐old woman who presented with a non‐specific chest pain, no ECG changes or cardiac enzymes elevation during the previous 24 hours. On the right, one can appreciate the similarity of the respective catheterization image.

Conclusion: Cardiac CTA is a promising technique for the evaluation of patients with acute chest pain.
Pre‐hospital reperfusion – a historic overview
A. Teddy Weiss, M.D. F.A.C.C., Intensive Coronary Care
Hadassah University Hospital, Mount Scopus, Jerusalem, Israel
27 years ago it was recognized that most cases of AMI are caused by a thrombotic occlusion of an epicardial artery Citation[1], an understanding which changed the treatment and outcome of this common and frequently fatal disease. It soon became clear that the intracoronary use of streptokinase, the first thrombolytic agent in use, could dissolve the clot and restore coronary flow Citation[2], resulting in relief of pain, ST segment resolution in ECG, and improved survival rates – yet, without evidence for myocardial salvage, due to the long time interval (∼4 hours) between onset of pain and thrombolytic agent administration related to the logistical delays of the intracoronary use Citation[3]. Those who believed in reperfusion injury even raised doubts about the value of this treatment. The “wave front” phenomenon of necrosis after coronary occlusion in a dog model suggested that there is a time window during which restoration of blood flow in the infarct‐related artery could limit infarct size Citation[4]. Intravenous thrombolysis with a higher dose of the drug allowed earlier, easier wider and cheaper initiation of thrombolysis Citation[5].
The idea of pre‐hospital administration of the drug emerged, while I joined the group of Dr Ganz at Cedars‐Sinai hospital, who proved the efficacy of intravenous thrombolysis Citation[6] but found great difficulty in shortening the time between onset of pain and drug administration; it was implemented 2 years later, upon my return to Jerusalem to our group led by Dr.Gotsman. This city was the ideal environment in which to begin, since the mobile intensive care unit was physician operated (since 1972), with a very short arrival time and a good public alertness to call them immediately for help. The logistics of the treatment in the patient's home were quite simple and speedy. The physician on the ambulance( Dr.Appelbaum) was already well trained to obtain the patient's history and symptoms, use the EKG to diagnose ST elevation MI, check for contraindications and start the thrombolytic agent infusion(750.000u intravenous streptokinase), at the patient's home, continuing it during the transfer to the hospital. Simple telephone call to the in‐hospital cardiologist allowed direct transfer to the coronary care unit, bypassing the busy emergency room. On March 1984 the first home‐thrombolysis patient diagnosed with acute anterior MI, received treatment 30 minutes after pain onset and upon arrival to our CCU, 20 min later‐the patient already presented the classical signs of reperfusion. The pre‐hospital‐treated group received thrombolysis earlier than the similar group of patients treated in‐hospital (on average 1.1 versus 1.7 hours), but even this minor time difference resulted in significant myocardial salvage, as shown by improved left ventricular function in a subsequent left ventriculography, smaller peak CPK and ECG scores Citation[7]–CitationCitation[9]. Long‐ time follow‐up of these patients showed a significant reduction in heart failure signs and symptoms and improved quality of life Citation[10]. The impact of very early treatment was clearly shown later in the initial GISSI Trial, which demonstrated a 47% reduction in mortality in infarct patients treated within the first hour of symptoms, subsequently rightly called ‐ the “golden hour” of thrombolysis Citation[11].
It was another few years before prospective randomized trials were organized and published. In EMIP Citation[12], an European collaborative trial, ambulance physicians randomized 5500 patients either pre‐hospital or in‐hospital treatment of 30u anistreplase and aspirin; their pre‐hospital group received lytic therapy 55 minutes earlier than the in‐hospital group, resulting in a 16% lower mortality, that raised to 50 %, when the time difference exceeded 1 hour. In the GREAT trial) general practitioners randomized 311 pts to 30u of iv anistreplase given at home or in‐hospital Citation[13]. The longer distances to hospital in this rural area in Scotland caused large differences in time delays to treatment: 101 minutes for the pre‐hospital group vs.240 minutes for the in‐hospital group and resulted in a large mortality benefit: 6.7%and 11.5% respectively, which became even more evident at a 1year follow‐up: 10.4% vs.21.6%.
The Myocardial Infarction, Triage and Intervention (MITI) phase‐1 project lead by Weaver in Seattle proved the feasibility and safety of pre‐hospital initiation of thrombolytics by trained paramedics using a computerized EKG diagnosis Citation[14]. In phase‐2, 360 patients with chest pain less than 6 hrs, were randomized to 100mg reteplase pre‐, or in‐hospital. Due to shorter mean time delays in both groups (77min for the pre‐hospital vs.110min for in‐hospital treated group), no significant difference in mortality and infarct size was found. Yet, in a secondary analysis of the effect of treatment on outcome, when treatment was started within 70 min of pain onset, it resulted in a major reduction in mortality (1.2%vs 8.7%) and in infarct size, by thallium SPECT (4.9%vs.11.2%) and in higher ejection fraction (53%VS.49%).These findings suggest that the time‐ window for preserving the maximum amount of myocardium at risk is short and delays must be minimized Citation[15].
The advantage of shorter time delivery of thrombolysis is hampered by the failure to achieve coronary patency in 20% of cases, with subsequent need for rescue angioplasty, a 30%rate of recurrent ischemia or re‐infarction and an increased rate of bleeding. Primary angioplasty emerged as a more effective, alternative means of coronary flow restoration, since it achieves higher patency rates and lower rates of re‐infarction, bleedings and stroke. Its wider use is limited by readily available cathlabs and experienced interventional cardiologists to open immediately the occluded coronary artery. This may be solved by fast inter‐hospital transport, such as in the Prague area Citation[16]. The debate over superiority between these two competing strategies continued : while seems to be a” thrombolytic ceiling”‐a plateau that pharmacologic reperfusion may not pass without an increased bleeding risk, the introduction of better wires, balloons, stents and strategies of facilitated angioplasty shifted the optimal approach toward mechanical reperfusion. A recent meta‐analysis of 23 randomized trials of primary angioplasty versus intravenous thrombolytic therapy Citation[17] proved that in experienced centers and operators‐ mechanical reperfusion was superior to in‐hospital thrombolysis in reducing mortality (7% versus 9%), non‐fatal MI (3% vs7%) and stroke (1vs2%).
The CAPTIM trial Citation[18] was designed to compare pre‐hospital thrombolysis to primary angioplasty in 840pts.The time to lytics onset: 130min vs. 190min‐time to first balloon inflation resulted in similar outcome: mortality was slightly lower in the pre‐hospital group (3.8vs4.8%) while re‐infarction and stroke slightly higher. For patients randomized within 2 hrs of pain onset, there was a strong trend toward lower 30‐day mortality (2.2%versus 5.7%) and less frequent cardiogenic shock (1.3%versu 5.3%).It has to be stressed that all patients were transported to a hospital with cathlab facilities, that allowed fast rescue angioplasty in 26% of the thrombolytic group with persistent ischemia.
It seems that the optimal treatment of ST elevation AMI is very early diagnosis and choosing then the fastest available reperfusion strategy: primary angioplasty, if readily available ‐within the next hour, or thrombolysis, especially within the first “golden” hour of pain onset. Adjunct anti‐platelet and anti‐thrombotic therapy on the way to cathlab was considered and tried. Aspirin and heparin given in the pre‐hospital phase versus in‐hospital, raised infarct‐related artery patency (Timi2/3 flow) from 20 to31% in the Zwolle pre‐hospital trials Citation[19]. Platelet glycoprotein receptor inhibitors pre‐hospital versus in‐hospital use was tried by the same group( using tirofiban bolus and infusion) resulting in a significantly higher infarct‐related coronary patency (TIMI 2/3 flow):43 versus 34%,and lower rate of thrombus and fresh occlusion, that facilitated subsequent angioplasty Citation[20].
Pre‐hospital diagnosis of acute myocardial infarction is the only strategy that may expedite enough early diagnosis and reduce the delay in time to onset of treatment to the absolute minimum feasible; therefore, it is here to stay. In the future, early EKG detection of transmural ischemia in patient's home and more effective thrombolytic and/or antiplatelet agents will further help to improve outcome. Regardless of the strategy chosen, pharmacological in the pre‐hospital phase, and / or mechanical reperfusion in the cathlab, it is crucial to shorten the time to reperfusion, since this is what will ultimately determine infarct size, and patient's prognosis.
What is the role of thrombolytic therapy in 2007?
Gianfranco Mazzotta, MD
Department of Cardiology, “Galliera” Hospital, Genova, Italy
The benefit of lytic reperfusion in the acute phase of STEMI is time‐dependent. Thrombolysis saves lifes when administered within 12 hours from onset of symptoms, but a major myocardial salvage can be achieved within 3 hours Citation[1]–CitationCitation[3]. The benefit in survival is maximum in the first 2 hours after the onset of chest pain, and is particularly high in the first “golden” hour. Door‐to‐needle (DN) time should be under control, and strictly kept within 30 minutes.
Reperfusion with thrombolytic agents is suboptimal as for the degree of the restoration of coronary flow. Coronary angioplasty is superior in this respect, and this may explain the clear advantage of primary angioplasty over pharmacological thrombolysis. Door‐to‐balloon (DB) time should be restricted to 90 minutes maximum, resulting in an acceptable “differential time” (DB‐DN) of 60 minutes: over this hour differential delay, the benefit of PTCA begins to be lost. Registries seem to tell us that the real world is much different from the trials, and that delays tend to be greater than in controlled conditions. The risk is that many patients with STEMI will not receive proper reperfusion therapies in time, and that candidates to either thrombolysis or PTCA will not receive any of the two.
Then which place can thrombolysis have in ST segment elevation in 2007?
The first and main question in front of a patient with STEMI is: when did the pain start? As a matter of fact, there is a clear difference in the advantages given by the 2 reperfusion strategies in different periods of the acute phase of a STEMI. In the first 2 hours, results are unclear, and thrombolysis is still an approach with a very high efficacy. On the other hand, from the 3rd hour on, a better impact with primary angioplasty seems definitively demonstrated.
In the first 2 hours after chest pain onset, pre‐hospital thrombolys have demonstrated to be able to anticipate any in‐hospital therapy by 60 min. (average), and to be clearly superior in life‐saving compared to in‐hospital lysis Citation[4]. In the CAPTIM study, mortality with thrombolysis has been at least non inferior to that of PTCA when drug is administered within 2 hours and one hour before PTCA be performed; however, this result is achieved sending patients to hub cardiac care units with prompt possibility of proceeding to rescue PTCA, in the case of unsuccessful pharmacological reperfusion Citation[5].
Pre‐hospital thrombolysis can be performed by physician or nurses able to interview patients for chest pain and to obtain an expert ECG reading. The administration of key drugs (enoxaparin and tenecteplase) is particularly easy, as they are administered as boluses. As a general criterion, thrombolysis (pre‐hospital or in‐hospital) should be preferred within 3 hours of onset of chest pain when PTCA can not be performed in less than another hour. Within 3 and 12 hours, lysis may be preferred, if angioplasty can not be performed within 90 minutes.
Probably the main reference for the judgement of the delays, time intervals, and the choice of the proper reperfusion modality is the analysis of the data generated by more than 190000 patientys in the NRMI Citation[6]. This manuscript shows in detail the delivery and results of reperfusion therapies in the real world, limited to the USA (meaning that this does not automatically apply to other Countries, not even to Europe). As expected, the advantages of PTCA decline with the increase of DB time. The higher the DB minus DN time, the higher the survival advantage with thrombolysis, and the vice versa for the advantage with PTCA. When DB‐DN is less than 85 minutes, the advantage of PTCA over lysis is clear, while the contrary apply when DB‐DN exceeds 114 minutes.
The advantage of PTCA is lost sooner in patients with STEMI presenting earlier. On the other hand, age (which is included in the TIMI risk score) shifts the benefit of PTCA to a larger time delay population, and the threshold to reconsider thrombolyisis for over 65 presenting with chest pain lasting more than 2 hours is 179 minutes. This time delay seems to be of only 40 minutes in younger patients presenting within 2 hours of symptoms. Thus, the best choice of reperfusion therapy depends not only on time delays, but also on patients' clinical characteristics, as expected.
Up to now, there is no evidence that pre‐hospital thrombolyisis may be a beneficial pre‐treatment for primary PTCA. Even though, a few recent studies has shown the possibility of obtaining very good results in terms of reperfusion by administering thrombolysis first, and then proceeding to primary PTCA Citation[7]. Proper trials should compare strategy of primary PTCA vs. pre‐hospital thrombolyisis with prompt rescue PTCA in case of failure. Rescue PTCA in selected patients may easily carry less bleeding risk than a systematic strategy of facilitated PTCA.
The second main question is: are there patients to be mandatory sent to a hub centre for PTCA and “high tech” level? I will discuss briefly of a few subgroups of STEMI. Patients with contraindication to thrombolysis must be sent immediately to primary angioplasty. Patients with failing thrombolysis should be sent to prompt rescue PTCA. Patients at high risk of death, in whom PTCA has demonstrated a high benefit in terms of live saving results, must be sent to PTCA. Patients with STEMI at particular high risk are those with: cardiogenic shock; pulmonary edema; heart rate over 100 b.p.m.; systolic blood pressure lower than 100 mmHg; more than 4 ECG leads involved in ST segment elevation; reinfarction in an ECG area different than the previous one; reinfarction and a previous by pass grafting; TIMI score more than 5 Citation[8,9].
In any area in the world, there should be an efficient network system for fast and proper transportation of at least these patients to a primary PTCA facility. They seem to be a quarter of the entire population of STEMI, they really need the benefit of primary PTCA and for them is worth the effort to create a network to transport them to a hub centre fast Citation[10]. Low risk patients (75% of STEMI) can probably be managed without any increase of risk with either prompt PTCA (if possible) or prompt thrombolysis and a guaranteed rescue PTCA as needed.
Conclusion. Thrombolysis is still a major treatment in STEMI. Resources should be available to increase the possibility for patients to receive thrombolysis in the pre‐hospital setting, saving time that is particularly worth during the first 2–3 hours of symptoms. Thrombolysis is still the first choice when PTCA can not be performed within 1 hour, and symptom onset is within 3 hours; after 3 hours, given the increasing, compared benefit of PTCA, thrombolysis remains an option if time to PTCA exceeds 90 minutes. Patients at high clinical risk, derived from simple clinical and ECG variables, should be object of mandatory planning of primary PTCA network in any area of the world, with the clear aim of predefining ways to send them to a high‐technology, hub centre as soon as possible. Still, if the foreseen waiting exceeds 1 hour, also high risk patients should undergo thrombolysis, but they deserve urgent coronary arteriography as soon as they reach the proper cardiological setting.
Optimal adjunctive therapy after thrombolysis for STEMI
Jean Pierre Bassand, MD
Department of Cardiology, University Hospital Jean‐Minjoz, Boulevard Fleming, 25030 Besançon Cedex, France
Until the recent past, the armamentarium for patients submitted to thrombolytic therapy was limited to aspirin and unfractionated heparin (UFH), which furthermore depended on the thrombolytic agent used.
More recently, low molecular weight heparins (LMWH) and fondaparinux have been proposed as adjunctive anticoagulant to thrombolysis in ST elevation myocardial infarction (STEMI) as well as clopidogrel (with or without a loading dose), and glycoprotein IIb/IIIa inhibitors.
Aspirin has become mandatory since the publication of the ISIS‐2 study, which showed that a 3% absolute risk reduction for death at 30 days could be achieved with aspirin versus no‐aspirin. The situation with UFH was less clear until recently. Indeed, UFH was recommended only after fibrin‐specific agents, despite the fact that it was only demonstrated that UFH had a positive impact on the patency rate at 90 minutes, without significant impact on the risk of death and MI, but with an increased risk of bleeding. Most recent guidelines recommended careful use of UFH, based on body weight.
In non‐fibrin specific agents like streptokinase, no trials or meta‐analysis have shown a positive impact of UFH, irrespective of the route of administration (intravenous or subcutaneous) Citation[1,2].
Two trials have recently shown (COMMIT CCS2, CLARITY) that clopidogrel for 1 months, with or without loading dose, reduced the rate of death and MI (CLARITY) and the rate of death (COMMIT CCS2) at 30 days, without any excess of bleeding. Clopidogrel has thus become mandatory adjunctive therapy to thrombolytic treatment, as well as aspirin in STEMI. The only question remaining is about the duration of the treatment, which was tested for only 30 days in clinical trials.
Glycoprotein IIb/IIIa inhibitors, whatever the compound, are not recommended in addition to thrombolytic treatment, whatever the dose, since they have been shown to have a negative impact on the risk of bleeding complications.
Enoxaparin was recently tested in the EXTRACT‐TIMI 25 study Citation[3] in 20,000 patients submitted to thrombolytic treatment within 12 hours after onset of symptoms for STEMI. Four different thrombolytic agents, including streptokinase, were tested. Enoxaparin was given at the usual dose, except in patients older than 75 years of age, who received only 1 daily injection of 1mg/kg, vs UFH. Enoxaparin was administered for 1 week, or until hospital discharge, whereas UFH was given at the currently recommended dose for a duration of 48 hours. In this trial, there was a significant risk reduction for death and MI at 30 days, but this was achieved at the cost of a significant increase in the risk of major bleeding, including a significant increase in the risk of fatal bleeds. The net clinical benefit was in favour of enoxaparin.
In Oasis‐6, fondaparinux was tested in patients submitted to thrombolytic treatment with either streptokinase or fibrin‐specific agents, as well as in sub‐groups of patients with no reperfusion, or undergoing primary PCI Citation[4]. Fondaparinux was tested versus placebo in patients submitted to streptokinase, and vs UFH in patients receiving fibrin‐specific agents. Overall, there was a significant risk reduction for death and MI, as well as death at 30 days and maintained at 6 months, in the whole trial. There was a significant risk reduction for death and MI in patients submitted to thrombolytic treatment without heterogeneity when comparing patients receiving fibrin specific or non‐fibrin specific thrombolytic agents. This was achieved without any increase in the risk of bleeding, and indeed with a non‐significant 18% risk reduction for bleeding.
As decision‐making for the use of treatments should be based on the efficacy‐safety profile of available agents, clopidogrel is strongly recommended in this situation, since the benefit is achieved without an excess of bleeding. However, the discussion remains open concerning the best possible adjunctive treatment between enoxaparin or fondaparinux, particularly when considering the efficacy‐safety profile of both drugs.
Optimal pathways to achieve reperfusion in STEMI
Jean Pierre Bassand, MD
Department of Cardiology, University Hospital Jean‐Minjoz, Boulevard Fleming, 25030 Besançon Cedex, France
Data from registries show that among patients suffering from ST elevation myocardial infarction (STEMI), a sizeable proportion (25–40% depending on the country) are not submitted to reperfusion Citation[1]. These patients have a much higher risk of death at 30 days and long‐term than those who undergo reperfusion. Among those who are submitted to reperfusion, some receive thrombolytic treatment pre‐hospital or in‐hospital, while others receive primary percutaneous coronary intervention (PCI). These subsets of patients have better outcome after reperfusion than patients who are not submitted to any reperfusion. However, in many cases, it would appear that excessive delays between first medical contact and administration of reperfusion are observed.
Reperfusion therapy encompasses five different approaches, with varying efficacy and levels of recommendation. Primary PCI (with or without transfer) has been shown to be superior to thrombolytic treatment. On the other hand, thrombolysis, especially pre‐hospital, has been shown in some registries to lead to equivalent benefit as primary PCI when administered within 3 hours after onset of symptoms.
Other large registries, such as RIKS‐HIA, have shown that primary PCI is superior to thrombolysis, whatever the form and timing between onset of symptoms and start of reperfusion Citation[2,3].
Rescue PCI after thrombolytic therapy is mandatory in patients who do not achieve reperfusion. After successful thrombolysis, the indication for post‐thrombolysis next‐day PCI remains debated. Some voices consider that it should be done on a systematic basis, but the evidence in favour of this comes from clinical trials with rather small samples sizes. Others advocate invasive strategy and reperfusion only in case of recurrence of symptoms or demonstrable residual ischemia Citation[4].
“Facilitated” PCI is a dead concept, as shown in meta‐analyses and ASSENT‐4, as it may even lead to worse outcome as compared to primary PCI Citation[5].
In this context, the role of adjunctive therapies has significantly evolved over the last 2 years. In Oasis‐6, it was shown that the administration of fondaparinux improves the outcome of patients not submitted to reperfusion Citation[6]. In patients submitted to thrombolytic treatment, dual antiplatelet therapy is now mandatory. Enoxaparin was shown to be superior to unfractionated heparin, but led to a higher risk of bleeding. However, the net clinical benefit was in favour of enoxaparin. Fondaparinux was shown to be superior to unfractionated heparin, with a significant risk reduction for death and MI in patients submitted to thrombolytic treatment, without any excess of bleeding. Abciximab given before or during primary PCI has been shown in a meta‐analysis to lead to a significant risk reduction for death at 6 months, and has also become mandatory during primary PCI.
In practice, the organisation of networks of reperfusion is best way to achieve reperfusion therapy within the shortest possible time after onset of symptoms and first medical contact, and for the highest number of patients. Networks have been established in many European countries. From registries, it is known that the transfer time for primary PCI, when this strategy is chosen, is very often longer than 90 minutes, and can even be up to 180 minutes in some countries (including the USA). Strict and efficient organisation of networks can reduce transfer, door‐to‐balloon and door‐to‐needle times, and eventually thereby improve outcome. It is now recommended that patients suffering from chest pain should ring a call centre, which would dispatch an ambulance with 12‐lead ECG facilities, so that the ECG can be recorded and transmitted directly to a heart centre. Depending on the expected transfer time, the treatment decision can be made at this stage (thrombolytic therapy or primary PCI). In any case, patients are directed to a tertiary centre where they can receive the appropriate reperfusion and adjunctive therapies. They are then discharged to an intermediate care centre, before moving to rehabilitation facilities or a primary hospital.
The efficiency of networks of reperfusion has to be checked, and their efficacy evaluated on a regular basis. The main messages arising from network experiences are as follows:
Main objective: to achieve at least 75% reperfusion therapy, within the shortest possible time (ideally <3 hours after onset of symptoms, and maximum 90 minutes after first medical contact if primary PCI is chosen).
Organisation of networks of reperfusion at regional and national level is key, and implies close collaboration between hospitals, emergency medical systems, medically or paramedically staffed ambulances, high volume tertiary centres, private practice cardiologists, primary care physicians.
Protocols must be written and agreed on for the type of reperfusion, and adjunctive therapies to be given during transfer to hospital.
Every effort must be made to shorten delays. In particular, early diagnosis of STEMI is essential. Coordination between hospitals selected to administer reperfusion, and direct access to the cathlab bypassing emergency rooms and CCU if primary PCI is recommended.
Primary PCI is the preferred option, with experienced staff and high‐volume centres.
Thrombolytic therapy is a valid option if primary PCI cannot be carried out in a timely manner.
Quality control with well defined indicators, establishment of registries, is key to control efficacy.
Information is essential to improve the visibility and efficacy of the reperfusion networks. Publicity aimed at physicians, cardiologists and the public (especially patients known to suffer from the coronary artery disease) is vital.
How to shorten door to balloon time in the real world
Nahir Menachem1, Hazanov Yevgeni1, Qarawani Daud1, Ganem Diab1, Abboud Mouein1, Nahum Sagi2, Hasin Yonathan1
1Cardivascular Institute, Baruch Padeh Medical Center, Porria, Tiberias, Israel;2Red Magen David & the Biology department, Haifa University, Israel
Primary angioplasty is the treatment of choice for ST elevation myocardial infarction (STEMI)Citation[1], especially when the ischemic time is longer then two hours Citation[2]. Every minute of delay in revascularization affects infarct size and may increase 1‐year mortality, even after adjustment for baseline characteristics Citation[3,4,5]. The ESC and ACC/AHA guidelines recommend that the time elapsed from first medical contact to first balloon inflation of the culprit artery would not exceed 90 minutes Citation[6,7], since longer delay is associated with reduced outcome. Nevertheless, in real life, door to balloon time often exceed this recommendation Citation[8].
In‐hospital time delay is a major determinant of the outcome of direct PCI for STEMI patients Citation[9], regardless of the time from symptoms onset to presentation and regardless of baseline risk of mortality Citation[10,11]. Recent surveys have shown that only about 20% of hospitals across the United States have been able to reach the 90‐miutes benchmark Citation[12]. This delay is attributed to the need for ER evaluation and diagnosis, cardiologist/ICCU staff, cath lab staff recruitment and transporting to the cath lab.
In order to close the gap between written recommendation and real life, Ortolani et al. Citation[13] investigated the effectiveness of a unique prehospital diagnosis program of STEMI patients with direct referral to PCI compared with conventional referral strategies. An innovative referral system was implemented whereby all STEMI patients are directly transported to the PCI center after prehospital, telemedicine diagnosis. Ambulance personnel perform the first diagnostic ECG in the patient's home, transmitting the ECG via GSM network to the ICU where it is seen by a cardiologist. In confirmed cases, patients are transported directly to the catheterization laboratory. From January 2003 to December 2004, 658 STEMI patients were referred for primary PCI at one of the two provincial interventional centers. The new prehospital diagnosis strategy was associated with a >45 minute reduction in treatment delay compared with traditional referral strategies (P = .001). However, significant differences in in‐hospital mortality were observed, in the overall study population.
Only recently another method of prehospital diagnostic technique was introduced. Dhruva et al Citation[14] used a wireless technology for transmission of a 12 lead ECG from the emergency medical services (EMS) in the community to an offsite cardiologist in the emergency department. A comparison of a small group of patients (20 patients with confirmed AMI out of 80 suspected) to comparison to the recorded cases of a previous calendar year should, a significant improvement in mean door to balloon time (80.1 vs. 145.6 min, p<0.001) .
In our center we further shorten the time by rearranging the organization of treatment for STEMI patients. We took advantage of the new structure and organization of the intensive care unit, as recommended by the ESC working group on acute cardiac care Citation[15], in particular performing cardiac catheterization in the special treatment room of the CCU. This room is an integral part of the ICCU, and it serves as the first site for evaluating patients with suspected acute cardiac conditions. It is equipped with a cardiac OEC/GE medical 9800 mobile C‐arm enabling fluoroscopy and cine image acquisition, and a Solar 8000 M (GE medical system) monitor connected to the central nursing work station of the ICCU enabling continuous online monitoring of 12 lead ECG, ST trend, invasive and non invasive blood pressure and non invasive O2 saturation. Also the room is equipped with all disposables needed for coronary angiography and angioplasty.
The suspected STEMI patients are transferred either from the ER or from the ambulance directly to the special procedure room for initial evaluation, including a short anamnesis, physical examination, 18 lead ECG and a short echographic study.
Since 2001, 227 patients had been transferred directly from the ambulance to the ICCU, and 244 patients had gone through the traditional emergency room evaluation. In the direct admission group the mean door to balloon time was 65.47±33.6 minutes (median 60.0 min.), and 85.3% of the patients had the first balloon inflation in 90 minutes or less, In the ER first group the mean door to balloon time was120.9±64.7 min (P value <0.0001, Mann Whitney test) and only 37.5% with time to balloon within the 90 min (p<.0001).
No difference in door to needle time was found between procedures performed during usual working hours (64.7±76.7min) to those performed during non working hours (69.5±56.2min). (p value = 0.18).
Conclusion: Pre‐hospital diagnosis of ST elevation acute myocardial infarction patients and direct admission to a dedicated procedure room in the intensive care unit, bypassing the emergency room, may reduce the time from admission to the balloon inflation in 60 minutes, and increase the percentage of patients being treated according to the guidelines significantly.
Validity of Rescue and of Facilitated Angioplasty for ST Elevation Myocardial Infarction
Peter Berger, MD, Director
Center for Clinical Studies, Interventional Cardiologist, Geisinger Clinic, Danville, PA
July 2007
Contact information: Peter Berger, MD, Geisinger Center for Health Research, 100 North Academy Avenue, MC 44‐00, Danville,PA 17822, USA; Telephone: 570 214 5057, Email: [email protected]
There is no longer any doubt that primary PCI is the preferred reperfusion strategy for acute ST elevation MI when it can be done rapidly and expertly. Controversy continues to exist, however, about how best to manage patients in whom primary PCI can not be performed. There remain important questions about the best way to manage patients who have received fibrinolytic therapy.
Facilitated angioplasty. The concept that administering fibrinolytic therapy to “facilitate” the performance of a percutaneous coronary intervention (PCI) that is performed as rapidly as possible after the fibrinolytic agent is administered, termed “facilitated angioplasty”, has been attractive, and until recently poorly studied. It was believed that the fibrinolytic agent might restore patency in at least some patients and reduce the thrombus burden and increase the safety of the PCI procedure in others. But it is now clear that facilitated angioplasty is neither a safe nor effective strategy.
Several trials had been performed evaluating the administration fibrinolytic agents, glycoprotein IIb/IIIa inhibitors, and a combination of fibrinolytics and a GP IIb/IIIa inhibitor before primary PCI could be performed Citation[1]. Until recently, all of these trials had enrolled relatively small numbers of patients. However, now a strategy of facilitated PCI has been evaluated in a large trial.
In the Assessment of the Safety and Efficacy of a New Treatment Strategy with Percutaneous Coronary Intervention (ASSENT‐ 4 PCI) trial, patients with symptoms of an ST‐segment elevation acute myocardial infarction for less than 6 hour in whom primary PCI was planned with an anticipated delay of 1 to 3 hours were randomized to full‐dose tenecteplase followed by PCI, or PCI without antecedent TNK (primary PCI) Citation[2]. All patients received aspirin and a bolus of unfractionated heparin. Although it had been planned that 4000 patients would be enrolled, only1667 patients had been enrolled when the Data and Safety Monitoring Board recommended that enrollment be terminated because of a higher in‐hospital mortality in the facilitated PCI arm (6.6% vs. 3.6%, p<0.013). After all patients had been analyzed, the primary endpoint of the study, death, congestive heart failure, or shock within 90 days, had been reached in 18.6% of patients assigned to facilitated PCI vs. 13.4% in those randomized to primary PCI (p = 0.005).
Subsequently, a meta‐analysis of all of the randomized trials of facilitated PCI provided even stronger evidence that ASSENT‐4 that facilitated PCI was not beneficial and may in fact be harmful Citation[1].
Much remains to be learned about the most appropriate therapy in patients with acute MI. But what is known is that the studies evaluating a strategy of facilitated PCI, analyzed individually and together, indicate no benefit at all from the strategy, and that it ought not be routinely pursued.
Rescue PCI. Trials of rescue PCI are difficult to perform, and bias in favor of a strategy of rescue PCI has long existed. The ACC/AHA guidelines considered rescue PCI to be a class 1 indication long before trials indicating the superiority of such an approach.
Four small randomized controlled trials of rescue PTCA versus medical therapy alone for failed fibrinolysis (TIMI 0‐1) were performed Citation[3]. These suggested benefit, but none came close to statistical significance, even when analyzed together Citation[3]. Following them, the Middlesbrough Early Revascularization to Limit Infarction (MERLIN) trial, was published in 2004 Citation[4]. A total of 307 patients who had evidence of persistent occlusion (less than 50% reduction in ST‐segment elevation) were randomized 60 minutes after fibrinolytic therapy to emergency angiography with rescue PCI, if the coronary anatomy was suitable, vs. conservative management. Although 30‐day mortality did not differ between the rescue and conservative arms (9.8% and 11.0%, respectively; p = 0.7), the trial was clearly underpowered to determine a survival advantage. But the composite, secondary endpoint of death, reinfarction, stroke, subsequent revascularization, or heart failure was lower in the rescue arm (37.3% vs. 50.0%; p = 0.02), driven mainly be less need for subsequent revascularization (6.5% versus 20.1%; p<0.01). The frequency of reinfarction and heart failure rates did not differ between groups, although the frequencies of stroke and transfusion rates were both significantly higher in the rescue arm.
In late 2004, the results of the Rescue Angioplasty versus Conservative treatment or repeat Thrombolysis (REACT) trial, an even larger trial, were published Citation[5]. In REACT, 427 patients with acute MI and failed reperfusion after thrombolytic therapy were randomized into one of three treatment strategies: IV heparin (conservative therapy), repeat thrombolysis (a fibrin specific agent, either accelerated tPA or reteplase), or coronary angiography with rescue PCI if appropriate. The primary endpoint of the trial, a composite of death, nonfatal repeat MI, stroke, or significant heart failure at 6 months, was significantly lower in the rescue arm than both the repeat thrombolysis or conservative arms (15.3% for rescue PCI versus 31.0% for repeat thrombolysis and 29.8% for conservative therapy). In the rescue PCI arm, 86.7% of patients were free of the need for repeat revascularization at 6 months, greater than the 76.5% frequency in the repeat thrombolysis group and 79.3% frequency in the conservative management group. Major bleeding occurred more frequently in the rescue PCI group compared with the other groups.
A meta‐analysis has been performed that adds to the evidence supporting the performance of rescue percutaneous coronary intervention after failed fibrinolytic therapy for ST elevation myocardial infarction (STEMI) Citation[6]. Although meta‐analyses themselves are rarely definitive, and this one is limited by the existence of important differences between trials included in the analysis, the data are compelling enough to support the routine performance of rescue PCI and for it to be appropriately considered a class 1 indication in the STEMI guidelines.
Counterbalancing the reduction in re‐infarction, heart failure, and trend toward a lower mortality with rescue PCI in the meta‐analysis was an increased risk of bleeding. One way to reduce the risk of procedural bleeding in such patients involves radial artery access for the procedure. Such an approach has been shown to lower bleeding rates; such an approach may be particularly beneficial in this setting.
Many important questions about rescue PCI remain unanswered. For example, the most appropriate duration of time beyond which one ought to consider fibrinolytic therapy to have failed remains unknown. In the 6 rescue PCI studies included in the meta‐analysis, the time from symptom onset to rescue PCI ranged from 257 minutes to 546 minutes; the time from the administration of fibrinolytic therapy until it was considered to have failed also varied greatly. Some of the variability is a consequence of the duration of transport from institutions without on site PCI where the fibrinolytic therapy had been administered to a PCI center for the rescue procedure. Whether the reduction in mortality with rescue PCI be greater if the time to rescue PCI shortened is not known. However, if the time to rescue PCI were too short, rescue PCI might begin to resemble the routine performance of PCI as early as possible after fibrinolytic therapy, which is facilitated PCI, and which appears to increase rather than decrease morbidity and mortality.
Whether a IIb/IIIa inhibitor ought to be administered during rescue PCI is also not known. The apparent benefit from administering a IIb/IIIa inhibitor during rescue PCI suggested by prior analyses Citation[7,8] is heavily confounded, since patients least likely to suffer major bleeding complications have preferentially been given such therapy. Selecting younger and healthier patients falsely exaggerates what true benefit may exist. And administering a IIb/IIIa inhibitor shortly after the administration of a full dose of a fibrinolytic agent clearly increases bleeding (9). Similarly, the observed increase in bleeding with such therapy is likely minimized by selection bias.
Another unanswered question relates to whether patients receiving fibrinolytic therapy ought be immediately transferred to a center capable of performing PCI, given the now proven benefits of rescue PCI. Such a recommendation will have the political and economic implications and will be resisted in many quarters.
Adjunctive pharmacotherapy
Raffaele De Caterina, M.D., Ph.D.
G. dAnnunzio University Chieti, and CNR Institute of Clinical Physiology, Pisa, Italy
Correspondence to: Raffaele De Caterina, MD, PhD, Chair and Postgraduate School of Cardiology, “G. d'Annunzio” University – Chieti, Ospedale San Camillo de Lellis, Via C. Forlanini, 50,66100 Chieti; tel.: +39‐0871‐41512, fax: +39‐0871‐402817, E‐mail: [email protected]
Adjunctive therapy in primary PCI or for thrombolysis refers to drugs (mainly antithrombotic drugs), which are given in addition to the primary treatment (primary PCI or thrombolysis) intended to achieve prompt recanalization of the occluded infarct‐related artery. These are essentially antiplatelet drugs and anticoagulants. There is currently a reasonable consensus for the oral antiplatelet drugs to use (at the moment aspirin and clopidogrel in combination Citation[1,2], both started with a bolus Citation[2], and then maintained long term ‐ most would say for one year, based on the extrapolation of data from non‐ST elevation acute coronary syndromes Citation[3]. There are shortcomings for the use of clopidogrel (as well as for the first‐generation thienopyridine available, ticlopidine), due to the slow onset and the slow offset of action. The standard “loading” dose for clopidogrel, 300 mg, has been recently tested against higher doses (600 and even 900 mg). A number of studies having employed 600 mg have demonstrated more rapid inhibition of platelet aggregation than achieved with 300 mg. However, no large scale outcome clinical trials have tested these higher doses of clopidogrel so far. Experience suggests that faster platelet inhibition with these higher loading doses (600 mg or more) may be more effective in reducing clinical endpoints (reviewed in Citation[4]). Definitive evidence of risk vs benefit will be provided by ongoing large‐scale clinical trials. New drugs now being tested may overcome such a problem. Such drugs include prasugrel, more potent than clopidogrel, now being tested in the TRITON‐TIMI38 trial (results probably being presented in November 2007), cangrelor, an injectable non‐thienopyridine reversible inhibitor of the P2Y12 receptor, and AZD16140, an oral non‐thienopyridine reversible inhibitor of the same receptor.
There is some dispute regarding the use of intravenous glycoprotein IIb/IIIa antagonists (abciximab mostly). The overall data for the use of abciximab as an adjunct to primary PCI with stenting are inconsistent. There is a suggestion that the earlier such treatment is given, the larger the benefit, but conclusive proof for this is still lacking.
Further dispute exists regarding the many alternatives available for anticoagulation, which include unfractionated heparin, low molecular weight heparins (essentially enoxaparin and reviparin), bivalirudin, and fondaparinux Citation[5]. In the setting of primary PCI, UFH should be preferred to low molecular weight heparins in high‐risk NSTE‐ACS patients with planned invasive strategy because of its shorter half‐life and easier reversibility. However, switching from UFH to a LMWH and vice versa should generally be avoided. If a LMWH has been administered prior to PCI, the administration of additional anticoagulant therapy depends on the timing of the last dose of LMWH. If the patient is already being treated with a LMWH, the following management (tested in trials with enoxaparin) is recommended: in patients undergoing PCI within 8 h of the previous s.c. dose, no additional anticoagulation is required; when PCI is performed within 8–12 h following an s.c. LMWH injection, supplemental treatment with a lower dose either of i.v. LMWH bolus (enoxaparin 0.3 mg/kg i.v. bolus) or of UFH could be given. There is so far no conclusive evidence on the use of LMWHs in the setting of primary PCI for STEMI as an initial choice Citation[5]. The pentasaccharide fondaparinux, which is an effective alternative to other anticoagulants in the setting of STEMI not treated with primary PCI on the basis of the OASIS‐6 Study Citation[6], should not be administered alone (without the addition of unfractionated heparin) in the setting of primary PCI because of an excess risk of catheter thrombosis. Currently, the use of bivalirudin in STEMI patients undergoing primary PCI in comparison to using UFH with a GPIIb/IIIa is being tested in a large randomized controlled trial (HORIZONS).
The optimal antithrombotic cocktail, designed as the optimal compromise between efficacy and safety (bleeding), is not an easy choice, and more than one option exists. This is an area of large interest where several new players are entering and where considerable development is expected in the near future.
Can post reperfusion no reflow be predicted on admission?
Doron Zahger, Arik Wolak, Jonathan Buber, Yochai Birnbaum, Carlos Cafri, Reuben Ilia
Department of Cardiology, Soroka University Medical Center, Ben Gurion University of the Negev
Failure of tissue reperfusion despite adequate restoration of epicardial patency, widely known as the “no reflow” phenomenon, is a major limitation of current reperfusion techniques in patients with ST elevation myocardial infarction (STEMI). No reflow complicates up to 50% of cases of otherwise successful reperfusion and has been associated with larger infarct size and worse prognosis. Although many agents and devices have been examined for their ability to treat no reflow there is currently no well established and effective treatment for this serious complication of reperfusion. Furthermore there is no established way to predict the occurrence of no reflow prior to reperfusion.
We hypothesized that if an effective bedside method could be found to predict the no reflow phenomenon upon admission this might allow prophylactic therapy to prevent this complication in high risk patients.
The grade of ischemia is an electrocardiographic classification of the morphology of the terminal portion of the QRS complex in patients with acute myocardial infarction. Grade 1 ischemia indicates the absence of ST elevation. Grade 3 ischemia is present when there are no S waves in the right precordial leads and/or the take‐off of the ST segment is above 50% of the amplitude of the R waves in any other lead. When ST elevation is present which does not fulfill criteria for grade 3 ischemia the tracing is classified as grade 2 ischemia. Grade 3 ischemia has been repeatedly shown to be a strong predictor of worse outcome in patients with STEMI but the mechanism remained unknown. We hypothesized that grade 3 ischemia might predict no reflow.
We first studied retrospectively 180 patients who received thrombolysis for a first anterior myocardial infarction at our institution between 1996 and 2002. Multiple demographic, clinical and electrocardiographic variables which were available upon admission were analyzed in an effort to predict failure of ST resolution post thrombolysis. We used failure of ST segment resolution as a surrogate indicator for no reflow as failure of ST resolution has been shown to be closely associated with this phenomenon; furthermore, failure of ST resolution is a well established marker of adverse outcome even among patients who achieve TIMI grade 3 flow in the infarct related artery. After multivariate analysis we found that failure of ST resolution at 2 hours was predicted by grade 3 ischemia (OR: 6.77 [3.27–13.95]) and by the absence of prior beta blockade (OR: 4.71 [1.56–13.98]). Grade 3 ischemia was the strongest independent predictor of failure of ST resolution at 24 hours and the strongest predictor of the need for rescue PCI. We concluded therefore that among the parameters available on admission grade 3 ischemia is the strongest independent predictor of failure of ST resolution following thrombolysis.
To extend these observations to patients undergoing primary percutaneous coronary intervention (PCI) we conducted a prospective study in which we included 100 consecutive patients who presented with a first STEMI and underwent primary PCI. Multiple demographic, clinical and electrocardiographic variables which were available upon admission were analyzed as predictors of post PCI coronary flow as well as of the degree of ST resolution. Electrocardiograms were read blindly in a core laboratory. We found grade 2 ischemia in 71 patients and grade 3 ischemia in 29. Complete ST resolution was achieved in 59% of patients with grade 2 ischemia as compared to 28% of patients with grade 3 ischemia (p = 0.004). Grade 3 ischemia was the only independent predictor of failure of ST resolution (OR: 0.26 [0.1–0.72]) and the strongest predictor of failure to achieve TIMI grade 3 flow and TIMI myocardial perfusion grade 3 after PCI.
We conclude that grade 3 ischemia is a powerful predictor of failure of ST resolution and of adequate angiographic reflow following reperfusion therapy for STEMI. This association probably explains the adverse outcome associated with this electrocardiographic pattern. Future attempts to prevent no reflow should probably concentrate in these patients who are at the highest risk for this serious complication.
Recognition of no reflow
Bojan Cercek, MD, PhD
Cedars‐Sinai Medical Center, David Geffen School of Medicine at UCLA, Los Angeles, California, USA
The no reflow phenomenon is defined as profound reduction in antegrade coronary flow in the absence of epicardial coronary artery obstruction. It occurs in approximately 2% of patients undergoing percutaneous coronary intervention (PCI) and up to 30% after PCI for acute coronary syndrome Citation[1,2].
EKG determination of successful reperfusion (reduction of ST segment elevation ). Persistent ST elevation is a simple and a very reliable method to assess adequacy of myocardial perfusion, including adequate epicardial flow and microvascular flow. The extent of ST elevation decrease corresponds well with invasive measurement of myocardial perfusion, like TMPG or Doppler wire velocities and clinical outcome Citation[3].
Coronary artery flow consists largely of 2 components:
(1) epicardial flow (open artery):
The assessment of epicardial flow is usually done by assessing the TIMI flow, grades 0‐III or more precisely by TIMI Frame count, >28 frames or greater for abnormal flow. (3).
(2) microvasculature flow (open vasculature):
Microvasculature can be assessed by angiography with myocardial perfusion grade, myocardial contrast echocardiography, coronary flow reserve by Doppler velocity wire and by Coronary Tomography and magnetic resonance (MR) imaging. Traditional nuclear imaging studies and positron emission tomography are used less for detection of no reflow Citation[4,5].
TIMI myocardial perfusion grades (TMPG): are divided in 4 grades: grade 3: normal ground glass appearance of myocardial blush diffusely, and at the end of the wash‐out phase, dye is only madly persistent or gone. Grade 2 the dye enters the myocardium but persists beyond the washout phase. Grade 1 the dye does not leave the myocardium until the next injection. Grade 0 the dye does not enter the myocardium and there is no blush.
The TIMI myocardial perfusion grade is a multivariate predictor of mortality independent of TIMI flow grade Citation[4].
TMPG correlates well with other tools for assessment of tissue perfusion (EKG changes, contrast echocardiography, Doppler wire velocities).
Myocardial contrast echocardiography (MCE): gas filled bubbles are injected continuously until steady state is achieved with their concentration proportional to the blood volume. The bubbles are then destroyed by high energy ultrasound probe and time to reappearance of the measured. This reflects blood flow velocity. Myocardial blood flow volume fraction and velocity reflect myocardial microvascular flow. The no reflow area is detected as the area with absent bubble enhancement and has been diagnosed in 30–60% of patients with reperfusion for STEMI
MCE determined no reflow includes also regions with microembolism, vasoconstriction (functional no reflow) and may improve over next 48 hours Citation[5,6].
Doppler wire coronary flow studies: with no reflow there is systolic flow reversal, reduced antegrade systolic flow and antegrade diastolic flow with brisk deceleration slope. In 105 patients with TIMI grade 2 flow, all patients with no reflow had systolic flow reversal, but only 1 in 10 with sole decrease in antegrade flow by Doppler wire had no reflow. These findings suggest that patients with TIMI 3 flow need special method for detecting no reflow Citation[7]–CitationCitation[9].
Magnetic resonance imaging (MRI) with gadolinium contrast agent detects no reflow as area of hypoenhancement early, within 2 minutes, after contrast injection. That area converts to partial orb complete hyperenhancement over the next 15–30 minutes (early hypoenhancement, late hyperenhancement pattern). Hypoenhancement is caused by decreased blood flow into area of interest, while late hyperenhancement is due to persistence of the in the intracellular space of damaged myocardium.
Similarly coronary tomography(CT) detects hypoperfusion, decreased volume of the vascular bed, early, within first few minutes after injection of the dye that later, 7–10 minutes turns into hyperenhancement because of the increased volume of the interstitial space and reduced excretion of the dye from myocardium with no reflow. With both methods 3 general patterns of enhancement have been described: 1) no early perfusion defect with late enhancement, 2) early perfusion defect and late hyperenhancement and 3) early perfusion defect with persisting late perfusion defect and partial late hyperenhancement. The pattern 3 is associated with worst decrease in left ventricular function and clinical outcomes Citation[3],Citation[10]–CitationCitation[12].
New NSTE‐ACS Guidelines
Jean Pierre Bassand, MD
Department of Cardiology, University Hospital Jean‐Minjoz, Boulevard Fleming, 25030 Besançon Cedex, France
The new guidelines of the European Society of Cardiology (ESC) on the management of non ST segment elevation acute coronary syndromes (NSTE‐ACS)1 were published in June 2007, 5 years after the last version. The penury of revolutionary data published in the field explains why the update was undertaken so long after the first version. The new guidelines were written in a different spirit to the previous version: the authors of the new version have taken into account the efficacy‐safety profile of the treatments (pharmacological or not) proposed for the management of NSTE‐ACS. In the past, only the efficacy was considered in the gradation of guidelines. However, bleeding complications have been shown to have a strong impact on short and long‐term outcome of these patients, and therefore, it was considered important to evaluate safety when recommending a therapeutic approach.
The authors decided to take into account only robust available data. In particular, only clinical randomised trials with adequate sample size, robust endpoints, double‐blind design, and using recent pharmacological and non‐pharmacological approaches (e.g. use of stents in case of PCI) were taken into consideration. Data from old trials were not considered.
The new guidelines describe the pathophysiology of NSTE‐ACS, as well as clinical and ECG presentation. They also address the role of biomarkers, particularly troponins, in the diagnosis and management strategies among these patients, focussing on new markers such as BNP, pro‐BNP and markers of renal function.
Risk stratification is an important component of the decision‐making process. The GRACE risk score is now proposed as the reference risk calculator for the management of NSTE‐ACS patients. This does not mean that clinicians should rely only on this score; it should be considered only as added information on top of the clinical, ECG and biochemistry markers of risk.
Treatment approaches encompass anti‐ischemic and antiplatelet agents, anticoagulants, and revascularisation strategies. While no major changes have been witnessed in the field of anti‐ischemic and anti‐platelet agents, much new information has come to light concerning two new agents that are now available for treatment, namely fondaparinux and bivalirudin, in addition to unfractionated and low molecular weight heparins. In this regard, a hierarchy has been established for the use of anticoagulants, both as a direct pharmacological approach and in the setting of PCI, based on the efficacy‐safety profile of these agents. Revascularisation is a major element of the management strategy, and is proposed according to three different scenarios, depending on initial clinical severity.
These guidelines cover several practice‐oriented aspects of the management of NSTE‐ACS that are not usually addressed in clinical practice guidelines. Among these are resistance to anti‐platelet agents, withdrawal of anti‐platelet agents, management of complications (specially bleeding), special populations, with particular emphasis on elderly, women, diabetes, chronic kidney disease and baseline anaemia. Long‐term treatment and rehabilitation are also addressed.
Last but not least, comprehensive management strategies are presented in a very clear manner:
Patients at highest risk, presenting in life‐threatening conditions, are proposed for invasive strategy within 2 hours.
Patients at intermediate to high risk, without features of life‐threatening conditions, should be submitted to invasive strategy with 72 hours after initial therapy including triple antiplatelet therapy, anticoagulant and anti‐ischemic agents, plus revascularisation whenever possible.
No invasive strategy is recommended for patients presenting without high‐risk features, and with no significant ECG changes or troponin elevation. These patients should be managed conservatively.
Evidence for anti‐atherogenic effects of N‐3 PUFAs from human studies
Raffaele De Caterina, M.D., Ph.D.
“G. d'Annunzio” University – Chieti, and CNR Institute of Clinical Physiology, Pisa, Italy
Correspondence to: Raffaele De Caterina, MD, PhD, Chair and Postgraduate School of Cardiology, “G. d'Annunzio” University – Chieti, Ospedale San Camillo de Lellis, Via C. Forlanini, 50, 66100 Chieti; tel.: +39‐0871‐41512, fax: +39‐0871‐402817, E‐email: [email protected]
Dietary intake of n‐3 polyunsaturated fatty acids (PUFAs) is likely to be cardioprotective. The American Heart Association recommends that all adults eat fatty fish twice a week as a mean of coronary heart disease prevention Citation[1]. Due to the multi‐factorial nature of ischemic heart disease, the precise anti‐atherogenic effects of n‐3 fatty acid in humans are not well‐established. Autopsy studies comparing Alaskan natives (who consumed high amounts of seafood‐derived products) and non‐natives (who mostly consumed Western‐type diets) provide circumstantial evidence that the extent of atherosclerosis is decreased in populations who consume high levels of n‐3 PUFAs. Newman et al. reported decreased percent of intima covering with fatty streaks and raised lesions in the aortas of Alaskan natives with high consumption of n‐3 PUFA Citation[2], vs non‐natives Citation[3]. The magnitude of the differences in fatty streaks and raised lesions appeared larger in younger age groups Citation[3], suggesting a stronger effect of diet in the earlier stages of atherogenesis. Prospective studies also suggest an antiatherosclerotic effect of n‐3 PUFAs Citation[4]. One randomized trial failed to show an effect of high‐dose n‐3 PUFAs therapy on coronary artery disease progression Citation[5], but the subsequent well‐controlled SCIMO trial showed a slower progression in subjects supplemented with n‐3 PUFAs (1.65 g/d) Citation[6]. A trial among individuals following coronary bypass surgery indicated that n‐3 PUFAs significantly reduced vein graft stenosis Citation[8], a process which may be regarded as an accelerated form of atherosclerosis. Results of trials evaluating the effects of n‐3 PUFA on restenosis following percutaneous coronary angioplasty were contradictory, possible due to differences in study design Citation[9,10]. Restenosis following percutaneous revascularization is the result of a mechanical injury to an already diseased vessel wall, and its relevance to native atherosclerosis is controversial.
The JELIS trial recently tested the effect of adding eicosapentaenoic acid (EPA, 1800 mg/d) to statin therapy in 18,645 Japanese subjects, among whom the baseline intake of dietary n‐3 PUFAs is very high compared to Western populations Citation[11]. The study examined whether supplementation with EPA could reduce CHD events in a combined primary and secondary prevention population, using a prospective open‐label study with blinded adjudication of endpoints. During an average follow‐up of 4.6 years, a significant 19% reduction (p = 0.01) was seen in the combined primary endpoint (sudden cardiac death, fatal and nonfatal MI, unstable angina, coronary revascularization), mainly due to reduction in unstable angina and revascularization. This benefit was independent from changes in serum cholesterol Citation[12]. This trial provides indirect evidence for an antiatherosclerotic effect of n‐3 PUFAs in humans, suggesting a reduction in either the progression of atherosclerosis or the propensity for acute complications, such as plaque rupture and coronary thrombosis.
PUTATIVE MECHANISMS. In humans, n‐3 PUFAs decrease serum triglycerides, an effect that is most pronounced in patients with marked hypertriglyceridemia. VLDL‐cholesterol is reduced, while LDL‐cholesterol tends to be either elevated or unchanged Citation[13,14]. In patients with mixed hyperlipidemia or marked hypertriglyceridemia, n‐3 PUFAs are a highly effective in reducing both triglycerides and VLDL. Thus, n‐3 PUFAs reduce these atherogenic risk factors. However, these effects are highly dose‐dependent, and the relevance of triglyceride‐lowering effects to clinical benefits seen with dietary n‐3 PUFA consumption is unclear.
Dietary n‐3 PUFAs, such as eicosapentaeonic acid (EPA) and docosahexaenoic acid (DHA), are incorporated into the phospholipids of cell membranes, in part replacing arachidonic acid (AA). Originally, the beneficial effects of n‐3 PUFAs on the cardiovascular system were attributed to their substitution of AA. Metabolic derivatives of n‐3 PUFAs (from the actions of the enzymes cyclooxygenase, lipoxygenase, and cytochrome P‐450 monoxygenase) are less pro‐thrombotic and vasoconstrictive compared to the corresponding AA derivatives. Both EPA and DHA have vascular effects, but some of these effects appear more pronounced for DHA. DHA, in contrast to EPA, is a poor substrate for metabolization into eicosanoids, and thus non‐eicosanoid effects of n‐3 PUFAs are likely to play a role in preventing atherogenesis.
Several direct effects of n‐3 PUFAs on endothelial activation have been demonstrated:
reduced production of cytokines such as IL‐1 and TNF in LPS‐stimulated monocytes Citation[15];
reduced production of the mitogen and smooth muscle cell attractant platelet‐derived growth factor (PDGF –A and ‐B) protein and m‐RNA Citation[16,17];
reduced expression of tissue factor by monocytes Citation[18];
increase of endothelial nitric oxide bioavalability Citation[19];
specific downregulation of gene expression for MCP‐1 Citation[20], and
reduced expression of endothelial adhesion molecules, which are essential for monocyte adhesion to sites of inflammation and dysfunctional endothelium Citation[21].
Effects on endothelial‐leukocyte interactions provide particularly compelling examples of how n‐3 PUFAs may impact atherogenesis. We demonstrated inhibition of NF‐κB activation by DHA (the most potent fatty acid inhibitor of endothelial activation), which paralleled production of hydrogen peroxide by cultured endothelial cells. This reactive oxygen species (or one of its downstream unstable products) appears to be a critical mediator of NF‐κB activation. Both baseline production and IL‐1 or TNF‐stimulated production of intracellular hydrogen peroxide (and its downstream products) were reduced after cell membrane enrichment with DHA. Saturated fatty acids served as a negative control in these experiments. Our current hypothesis is that fatty acid peroxidability, determined by the presence and number of double bonds, of the membrane fatty acids is directly related to endothelial cell responses Citation[22] (). There may also be earlier effects on signal transduction, for example on activation of cytokine receptors embedded in the plasma membrane, the characteristics of which are modified by the incorporation of highly unsaturated fatty acids Citation[22].
Figure 1. A scheme of the putative site of action of n‐3 PUFAs on endothelial activation, the most potent of which appears to be docosahexaenoic acid (DHA), thus potentially decreasing early atherogenesis. N‐3 PUFAs likely act immediately downstream to receptors for various atherogenic stimuli (e.g., minimally modified LDL (mmLDL), the advanced glycation endproducts (AGEs) or inflammatory cytokines), in part at the level of reactive oxygen species (ROS), the most relevant of which appears to be hydrogen peroxide (H2O2). ROS activate the nuclear factor‐κB (NF‐κB) system of transcription factors, likely through the activation of the degradation of the inhibitor I‐κB, allowing the free active NF‐κB heterodimers (rel A‐p50) to translocate into the nucleus, bind to specific consensus sequences in a number of NF‐κB‐responsive genes (including genes for vascular cell adhesion molecule‐1 (VCAM‐1), intercellular adhesion molecule‐1 (ICAM‐1), E‐selectin, monocyte chemoattractant protein‐1 (MCP‐1), interleukin(IL)‐6 and IL‐8, and cyclooxygenase‐2 (COX‐2)), driving their increased transcription. By inhibiting ROS generation, in part through the generation of active metabolites (including resolvins and protectins), n‐3 PUFAs would decrease atherogenesis.
NonSTE ACS: Invasive Approach
E. A. Amsterdam, MD, Chief of Cardiology
University of California at Davis, Sacramento CA, USA
The acute coronary syndromes (ACS) comprise the spectrum of acute ischemic coronary disease: ST elevation MI (STEMI) and nonSTE (nSTE) ACS (unstable angina and STEMI). nSTE ACS are diagnosed by the combination of symptoms and objective evidence of myocardial ischemia (ST‐T alterations [unstable angina] and/or elevation of cardiac injury markers [nSTEMI]). The underlying pathophysiologic event in nSTE ACS is usually rupture of an unstable coronary atherosclerotic plaque resulting in subtotal thrombotic coronary occlusion, in contrast to STEMI in which thrombotic occlusion is characteristically total. Coronary vasospasm associated with or without atherosclerotic CAD can also cause nSTE ACS. In contrast to these etiologies of low flow ischemia/injury, ACS can also result from severe demand ischemia (e.g., hyperthyroidism, hypertensive crisis).
It is now recognized that although nSTE ACS may be associated with lower initial morbidity and mortality than STEMI, the former syndrome confers higher longterm coronary risk than does STEMI. It is unclear whether this outcome is related to differing extent and type of CAD, associated risk factors, or the intensive acute and posthospital management that is standard of care for STEMI patients compared to a frequently less rigorous approach practiced in the nSTE ACS group, despite more rigorous guideline recommended therapy.
Two therapeutic strategies for nSTE ACS have been intensively evaluated in over 10,000 patients during the last two decades in trials that have compared a routine, early invasive approach with conservative (medical) therapy that includes selective invasive methodology. Current guidelines advocate an invasive approach for evaluation and management of high risk patients with nSTE ACS, who are defined by elevation of cardiac markers and/or ischemic ECG changes, refractory symptoms, cardiac failure, marked mitral regurgitation or ventricular arrhythmias. Since ischemic ECG changes and/or elevation of cardiac markers are inherent in the definition of nSTE ACS, virtually all patients with these syndromes fulfill criteria of high risk. This definition therefore, has profound implications for the management of patients with nSTE ACS.
Advocacy of an early invasive approach, which entails coronary angiography within 24–48 hours of admission and revascularization in suitable patients, is based on evidence from a majority of clinical trials that have reported superior outcomes with this strategy compared to conservative management. The invasive approach should also include intensive medical therapy (antiplatelet and antithrombotic agents, beta blockers, nitrates, and statins, and it may also include calcium channel blockers and ACE inhibitors). The conservative strategy selects patients for angiography based on risk stratification by noninvasive cardiac testing or clinical assessment.
Because therapy for ACS continues to rapidly evolve, much of the data from clinical trials is outdated by the time of its availability. Other limitations of current trials include variability in definitions of endpoints (e.g., MI) and flaws in design such as unblinded or unmasked treatment groups and absence of optimal therapy, or unclear therapy, in the conservatively treated patients. Meta‐analyses have been applied to help clarify the comparative utility of the two therapeutic strategies. In general, the invasive strategy has been associated with a reduced risk of combined clinical endpoints, which have generally comprised both “hard” events (death and MI) and “soft” events (symptoms, inducible ischemia, rehospitalization for ACS, revascularization). Reduced risk of these combined endpoints by the invasive strategy has been largely due to the decrease in soft clinical events, many of which are subjective and physician‐driven, but the meta‐analyses suggest a reduction in the risk of MI and death by the invasive approach. However, the benefits of the latter strategy have been shown to be directly related to the level of clinical risk. Data are mixed regarding the results of invasive strategy in women.
Two recent reports, RITA‐3 and ICTUS, have yielded noteworthy findings that reflect the complexity and controversy in comparing the two therapeutic strategies. After 1 year, the ICTUS trial of 1200 nSTE ACS patients demonstrated no differences in cumulative endpoints (early invasive 22.7%, conservative 21.2% ) and mortality (2.5% in both groups). In the early invasive group, MI was more frequent (15.0% vs. 10.0%, p<0.005) but rehospitalization was less frequent (10.9% vs. 7.4%, p = 0.04). After 3 years, these comparisons between the two strategies were not altered: combined endpoint was 26% in the conservative group and 30% in the invasive group (n.s.), MI was more frequent in the invasive group (18% vs. 12%, p = 0.002) and after 4 years there were no differences in all‐cause or CV mortality. The investigators concluded that either therapeutic approach was acceptable. It is notable that this trial was the first to utilize optimal medical therapy in a comparative study of treatment for nSTE ACS.
In contrast to ICTUS, RITA‐3, which did not show differences in hard endpoints between the two treatment strategies after 1 year, revealed significant reductions in these events by the invasive strategy over conservative management at 5 year follow‐up: mortality/nonfatal MI 16.6% vs. 20.0%, p = 0.04) and a trend toward reduction in death (12% vs. 15%, p<0.054). These benefits were mainly seen in patients at high risk of death or MI, as reflected by a 50% reduction in event rate in high risk patients while there was no difference in outcome in the low risk group. The investigators concluded that in patients with nSTE ACS, a routine invasive strategy reduces longterm risk of mortality and nonfatal MI, mainly in high risk patients. In assessing these results, it should be recognized that while a high proportion of patients in the medical group were on recommended therapy, no data are available on whether therapeutic targets (e.g., BP, lipids) were attained.
Management of nSTE ACS is a complex issue in which evolving therapy presents major opportunities as well as challenges. Clarification of these issues will require further assessment of the roles of individual patient risk, advantages and limitations of treatment modalities and careful analysis of ongoing trials.
Every patient with acute coronary syndrome should have coronary angiography
Ayelet Shauer, MD, Chaim Lotan, MD
Two different treatment strategies may be followed after initial medical treatment of unstable angina and non‐ST‐segment elevation MI (UA/NSTEMI): an early invasive strategy of coronary angiography and revascularization if needed; or a conservative (“ischemia guided”) strategy in which patients undergo coronary angiography and revascularization only if there is objective evidence of ischemia (e.g. recurrent infarction, angina at rest, dynamic ST changes on ECG or inducible ischemia on provocative testing).
Early trials failed to demonstrate the superiority of the early invasive approach, presumably because of less experience, fewer revascularizations, the unavailability of stents for routine use and the lack of using glycoprotein IIb/IIIa inhibitors. As an example, the VANQWISH trial, the largest of its kind, showed a significantly worse clinical outcomes, including death or MI, in the patients treated with invasive strategy during the first year of follow‐up compared with those treated with a conservative strategy Citation[1]. Therefore current ACC/AHA guidelines for the management of patients with UA/NSTEMI Citation[2] endorse prompt angiography without risk stratification (Class Ia) only for those patients who have new ST depression or elevated troponins, or that are not readily stabilized by intensive medical therapy.
Nevertheless, recent evidence supports the assumption that early determination of coronary anatomy can be used to better tailor therapy, avoid lengthy hospital stays and prevent further ischemic events. These newer trials “add wood to the fire” of an ongoing debate regarding this burning question, and may change future approach.
The first trial that showed the benefit of an early invasive strategy was FRISC‐II Citation[3]. This trial showed, for the first time, a significant six months event rate reduction (risk ratio [RR] 0.78; 95% confidence interval, 0.62 to 0.98; p = 0.031 for death, MI or both) in these patients. A subsequent trial such as TACTICS TIMI‐18 Citation[4] that used GP IIb/IIIa receptor antagonist before randomization to invasive versus conservative strategy showed similar results (odds ratio for the primary outcome of death, MI, and rehospitalization for ACS [OR], 0.78; p = 0.025).
Results from a later trial, the RITA‐3 Citation[5], reinforced the results of the previous trials with a better primary end point outcome of death, MI, or refractory angina at four months in the early invasive group compared with the conservative group (RR, 0.66; p = 0.001).
A newer trial, the ICTUS, is exceptional among these more contemporary trials, in that it showed the opposite results and challenged the hypothesis of early invasive approach superiority over the conservative one Citation[6]. It should be emphasized, however, that the discrepancy between this and previous trials could be attributed in part to the small difference in revascularization rates between the two study groups and the high overall rate of revascularization before discharge (76% in the routine invasive and 40% in the selective group).
A meta analysis that included these four trials and three earlier randomized trials showed that in patients with unstable angina and NSTEMI, a routine invasive strategy is superior to a selective invasive (i.e. conservative) strategy in reducing long‐term major cardiovascular events, as well as severe angina and rehospitalizations Citation[7].
Another meta analysis published a year later included seven trials after the exclusion of trials before the era of enhanced antiplatelet therapy and coronary stents. GP IIb/IIIa receptor antagonist use was available in all but one trial and follow up beyond 1 year was reported in four of the studies Citation[8]. The incidence of the primary outcome of all‐cause mortality was 4.9% versus 6.5% (risk ratio [RR] 0.75, 95% confidence interval [CI] 0.63 to 0.90, p = 0.001). The number needed to treat with early invasive therapy to save one life was 62 patients (p = 0.001).
Finally, in a Cochrane database review that was recently published Citation[9] it was found that patients with UA/NSTEMI who undergo routine angiography with the appropriate use of stenting have a better outcome regardless of GP IIb/IIIa receptor antagonists use. The most consistent and robust findings of this review are that an invasive strategy in UA/NSTEMI results in a significant 33% relative risk reduction for both the end points of refractory angina and rehospitalization at 6–12 months. The available data suggests also a significant 25% relative risk reduction for both the end points of death and myocardial infarction assessed at 2–5 years. These new data are brought together in the most recently published ECS guidelines for the diagnosis and treatment of non ST‐elevation acute coronary syndromes Citation[10]. These guidelines indicate early invasive strategy in every patient with acute coronary syndrome, excluding patients with no recurrence of chest pain, no signs of heart failure, no abnormalities in the initial ECG and no elevation of troponins (arrival and at 6–12 h). All other patients should have coronary angiography within 72 hours of admission (class Ia)
Anemia, bleeding and blood transfusion in patients with acute coronary syndromes
Doron Aronson, M.D.
From the Department of Cardiology, Rambam Medical Center and the Bruce Rappaport Faculty of Medicine, Haifa, Israel
Recent studies have shown that anemia on admission is an independent indicator of mortality in patients with acute coronary syndromes (ACS).1, 2 Pharmacological interventions such as antithrombotic and thrombolytic therapy, dosing errors, and the widespread use of aggressive revascularization procedures, have all been associated with bleeding complication and worsening anemia during hospitalizations for ACS.3‐5 Age, renal function, and use of invasive procedures have been consistently shown to predict bleeding complications in patients with ACS.6 Importantly, recent data indicates that bleeding should no longer be regarded as an acceptable complication in ACS, because bleeding itself is associated with adverse outcomes, including myocardial infarction and death.7 In fact, bleeding reduction is an attractive therapeutic goal that may lead to improved survival among patients with ACS.
However, it is important to emphasize that anemia can develop or worsen during hospitalization even in the absence of overt bleeding, in a gradual progressive manner.5 Therefore, the prevalence of anemia increases dramatically during hospital course in patients with ACS. Using the World Health Organization definitions (haemoglobin<13 g/dL in men and<12 g/dL in women), we have recently shown that anemia was present in 17.8% of patients with acute myocardial infarction on admission. The prevalence of anemia increased to 48.0% during hospital course and 36.1% of patients were discharged with anemia. This striking increase in the prevalence of anaemia during hospital course was associated with increased risk of death and heart failure long after hospital discharge ().5 Nadir hemoglobin levels during hospital course remained strongly associated with long‐term mortality after adjustment for multiple clinical variables and for left ventricular ejection fraction. The adjusted hazard ratios for death of patients with nadir haemoglobin in the 3rd, 2nd and 1st quartiles, as compared with those in the 4th quartile, were 1.1 [95% CI, 0.5 to 2.1], 2.0 [95% CI, 1.1–3.9], and 3.3 [95% CI, 1.8 to 6.3], respectively (P for trend <0.0001). These results emphasize the deleterious effects of anemia that develops during the course of hospital stay on long‐term mortality after hospital discharge.
Correction of anemia with the use of red blood cell transfusions is often considered in patients with ACS. However, recent studies came to different conclusions regarding optimal hematocrit or hemoglobin level in patients with ACS.1, 8–10 Furthermore, there are data that now call into question the cardiovascular safety of in patients with ACS.8, 10 Currently, the appropriate “transfusion trigger” in ACS patients is unknown. Notwithstanding, collectively, all studies appear to support the potential danger of aggressive blood transfusion in the setting of ACS.
Finally, preliminary data suggests that with current anti‐platelet regimens, unrecognized and unreported minor bleeding events may transform into a chronic and clinically significant blood loss and development of chronic anemia. We studied 828 patients with acute myocardial infarction who survived the acute event. Hemoglobin levels were obtained at hospital discharge and >1 month post discharge (median 7 month). Anemia was present in 295 patients at hospital discharge (36.8%). At follow up, anemia was present in 141 (47.8%) and 88 (17.0%) pts with and without anemia at hospital discharge, respectively. During a median follow up of 12 months (range 2 to 26) after the post‐discharge hemoglobin measurements, 67 patients died (8.1%). In a multivariable Cox regression model, the hazard ratio for mortality in patients with decreasing hemoglobin after hospital discharge was 2.5 (95% CI 1.4–4.4, P = 0.001) compared with patients with increasing hemoglobin level (). The development of persistent anemia following acute coronary syndromes is an important area of future research.
Figure 1. Kaplan‐Meier plot showing the crude cumulative incidence of death after hospital discharge according to quartiles of nadir hemoglobin obtained during hospital course in patients with acute myocardial infarction.
Figure 2. Survival according to hemoglobin change after hospital discharge.
Fondaparinux – The Hematological Perspective
Benjamin Brenner, MD
Thrombosis & Hemostais Unit, Rambam – Health Care Campus, Haifa, Israel
Correspondence author: B. Brenner, MD, Prof. of Hematology, Dept. of Hematology, Thrombosis & Hemostais Unit, Rambam Medical Center, P.O.B. 9602, Haifa 31096, Israel. Tel.: +972‐4‐8543520, Fax: +972‐4‐8543886, E‐mail: [email protected]
Fondaparinaux (Arixtra), the first synthetic factor Xa inhibitor approved for clinical use, has been in the focus of medical research of anticoagulants for the past 20 years.
Fondaparinux is based on the chemical structure of Pentasaccharide which is found in unfractionated and low molecular weight heparins Citation[1]. The antithrombin binding of the synthetic compound is stronger compared to the natural pentasacharide and Fondaparinux increases by 300 folds factor Xa neutralization by antithrombin Citation[2] .
Due to the shortness of the pentasaccaride molecule, Fondaparinux has no activity against thrombin. Fondaparinux has no effect on several clotting assays including prothrombin time and thrombin time with a weak effect on the activated partial thromboplastin time. The best way to monitor Arixtra when indicated, is by the anti‐Xa assays Citation[3]. One milligram of Fondaparinux has an anti‐Xa specific activity of ∼850IU. Fondaparinux does not influence platelet aggregation, and heparin induced thrombocytopenia (HIT) is a very rare occurrence Citation[4]. Fondaparinux half life is between 17 to 21 hours and therefore a single daily subcutaneous injection is sufficient. There is no specific anti‐dot and in case of uncontrollable bleeding fresh frozen plasma and coagulation factors concentrates can be used to reverse Fondaparinux effect.
Fondaparinux does not cross the placenta in an animal model, but information in pregnant women is limited.
Fondaparinux rarely causes skin reactions and in fact, it has been used as a substitute in cases of skin reactions to LMWH. Prolong use of heparin has been reported to be potentially associated with bone loss. Results of limited in‐vitro studies suggest that Fondaparinux does not inhibit bone metabolism.
Arixtra has been extensively evaluated in clinical trials of prevention and treatment of venous thromboembolism (VTE) as well as in the setting of arterial thromosis. In prophylaxis for orthopedic surgery Arixtra at a dose of 2.5mg/d has been compared to LMWH and Vitamin K antagonists. In hip replacement (Ephesus Citation[5] and Pentathlon 2000 Citation[6] trials), total knee arthroplasty (PENTAMAKS study Citation[7]) and hip fracture ((Pentifra study Citation[8]). Arixtra was found to be more effective than Enoxaparin or Warfarin in prevention of VTE, with no differences in clinically important bleeding.
Fondaparinux was also evaluated in patients with major abdominal surgery. The PEGASUS investigators compared the efficacy and safety of Arixtra and Dalteparin in patients undergoing high risk abdominal surgery Citation[9]. The results showed camparable efficacy and safety of Fondaparinux 2.5mg/d and Dalteparin 5000U/day.
Fondaparinux was also evaluated for thromboprophylaxis in acutely ill medical patients. In the Artemis trial Fondaparinux at 2.5mg/day significantly reduced VTE rates by venogram compared to placebo (5.6% Vs 10.5% P = 0.03) in acutely ill medical patients Citation[10].
Arixtra was also evaluated in the treatment of VTE. In the MATISSE DVT study, fondaparinux was shown to be at least as effective as Enoxaparin in patients with acute symptomatic deep vein thrombosis Citation[11]. In the MATISSE PE study Citation[12], Fondaparinux was demonstrated to be least as safe and effective compared to unfractionated heparin in patients with symptomatic acute pulmonary embolism.
Due to lack of interaction with platelet factor four Arixtra has been advocated in the management of heparin induced thrombocytopenia.
Fondaparinux is contraindicated in patients with severe renal impairment (creatinine clearance <30ml/mi). In patients with moderate renal impairment (creatinine clearance 30–50ml/mi) Fondaparinux should be used with caution.
Caution should also be exercised when Fondaprinux is administered to nursing mothers as it is not known whether Arixtra is excreted in human milk.
Anticoagulation in NSTEMI: the role of dose adjustment
Yoseph Rozenman, MD
The E. Wolfson Medical Center, Holon, Israel
Routine invasive strategy is the currently recommended approach to patients with non ST elevation acute coronary syndrome (NSTE‐ACS) Citation[1]. Until the culprit plaque is stabilized with a percutaneous coronary intervention (PCI) antithrombotic therapy is required with a combination of antiplatelets and antithrombins. Unfractionated heparin (UFH) was the agent of choice for many years however two recent trials (ESSENCE, TIMI 11B) demonstrated the superiority of low molecular weight heparin (enoxaparin ‐ Enox) over UFH Citation[2]–CitationCitation[4].
The SYNERGY trial enrolled approximately 10000 high risk ACS patients and compared Enox to UFH in the setting of early invasive strategy (median time to cardiac catheterization and PCI <24 hours) Citation[5]. The primary endpoint of death or myocardial infarction (MI) was similar in Enox and UFH and so were death and MI rates. Major bleeding was more common in the Enox group. One of the main conclusions from this study is that best results are obtained in patients with consistent therapy (UFH or Enox) throughout hospitalization. Switching therapy from one antithrombin to the other was associated with reduced efficacy and increased bleeding. Additionally, excess bleeding rate with Enox was limited to patients with impaired renal function as determined by creatinine clearance.
Analysis of large data base of patients with ACS led to the conclusion that bleeding is not just an “inconvenient” event; in fact it is associated with long term mortality. The impact of bleeding on survival is similar to that of recurrent MI. Rao et al. Citation[6] analyzed data from >25000 patient with NSTE ACS and concluded that mild, moderate and severe bleeding are associated with 1.4, 2.1, and 7.5 hazard ratio's for 6 months mortality. Current European guidelines emphasize the importance of bleeding prevention; the goal is to adjust the intensity of antithrombotic therapy to achieve the optimal balance between prevention of thrombotic and bleeding events.
The OASIS 5 trial Citation[7] compared Enox to Fondaparinux (Fonda) in patients with NSTE ACS. The primary efficacy endpoint of combined death or MI or refractory ischemia at 9 days was similar in both groups (Fonda non‐inferior to Enox). However, Fonda had much better safety profile, with hazard ratio of 0.53 (p<0.00001) for major bleeding at 9 days compared to Enox. Mortality at 30 days and 6 months (secondary study endpoint) was significantly lower in patients treated with Fonda. The data suggest that the increased mortality with Enox is related strongly to the excess bleeding – supporting prior conclusion regarding the detrimental prognostic effect of bleeding in patients with ACS.
It is unclear whether excess bleeding with Enox in OASIS 5 is inevitable or whether different dosing schedule could have influenced outcome. Enox dose was 1mg/Kg q 12 hours for enrolled patients (creatinine <3mg/dL). There was no dose adjustment based on calculated creatinine clearance or for patients treated with glycoprotein IIb/IIIa antagonists Citation[8]. Furthermore, patients subjected to PCI (6 hours after last Enox dose) got additional full dose UFH exposing them clearly to over‐anticoagulation. Patients on Fonda in whom invasive strategy was used suffered from higher frequency of catheter thrombosis, exposing them to major complications during PCI. It is recommended that these patients should be treated with additional UFH, however it is not exactly clear what is the appropriate dose and what are the bleeding consequences.
The STEEPLE trial Citation[9] compared UFH to Enox in patients undergoing PCI. There was no difference in ischemic complications. With the dose used, bleeding rate was significantly lower with Enox, suggesting that with the appropriate dose Enox can be an attractive antithrombin during PCI.
Summary and conclusions: Early trials concluded that outcome of patients with NSTE ACS can be improved with Enox as compared with UFH. When an early invasive strategy is used careful dose adjustment is essential in order to get the full benefit from Enox and additional UFH should be strictly avoided. Fonda is an attractive antithrombin only in patients treated conservatively since it is not effective enough in the setting of cardiac catheterization.
Platelet Aggregation: Physiology and Clinical Assessment
Steven R. Steinhubl, MD, Charles L. Campbell, MD
From the Gill Heart Institute, University of Kentucky, Lexington, Kentucky
Address for Correspondence: Steven R. Steinhubl, MD, 900 S. Limestone St., 326 CT Wethington Bldg., Lexington, KY 40536‐0200; Phone: 859‐323‐8040, Fax: 859‐323‐6475, E‐mail: [email protected]
The assessment of platelet function, and in particular predicting the clinical benefit or safety of an antiplatelet agent based on a test of platelet function is far from straightforward. Multiple tests exist that have been shown to identify changes in function following a therapeutic intervention, but the results of these tests frequently do not correlate with each other and the clinical meaning therefore remains to be defined.
Developed in the 1960's, the historical gold standard for the characterization of platelet activity remains turbidometric platelet aggregometry. In this assay, platelet rich plasma (PRP), isolated from citrated whole blood, is stimulated by agonists such as Adenosine Diphosphate (ADP), thrombin receptor activating peptide (TRAP), collagen or epinephrine. As platelets aggregate, light transmission through the sample is attenuated. Utilizing this method, investigators have been able to correlate clinical events with platelet activity. Gum et al., followed 326 aspirin‐treated patients with stable coronary artery disease (CAD) and found that high levels of baseline platelet activity as determined by PRP aggregometry independently predicted recurrent cardiac events Citation[1]. Matetzky et al., evaluated 60 patients treated with aspirin, clopidogrel and the glycoprotein IIb/IIIa inhibitor eptifibatide, undergoing PCI for ST‐elevation myocardial infarction (STEMI), and found that recurrent events clustered among patients in the highest quartile of platelet activity as determined by PRP aggregometry Citation[2]. The wide spread use of this assay is limited by the significant technical demands and cost.
The Platelet Function Analyzer (PFA‐100, Dade‐Behring, Deerfield Ill) is a point‐of‐care assay that evaluates high‐shear platelet function by passing citrated whole blood past an aperture coated with collagen and either epinephrine or ADP. The time required for platelet plug formation or for aperture closure is used as measures of platelet activation. Fossard et al., found that increased platelet activity as measured by the time to platelet plug formation was significantly elevated among 216 patients with STEMI and predicted myocardial necrosis Citation[3]. The test is rapid, and easy to perform on small volumes of blood, but has been may be very sensitive to serum concentrations of von Willebrands factor.
The VerifyNow Rapid Platelet Function Assay (RPFA, Accumetrics San Diego, California) was initially developed to monitor therapy with GP IIb/IIIa inhibitors, but has subsequently been modified to monitor the effects of aspirin and thienopyridines. In this test, whole blood is added to a cartridge containing fibrinogen‐coated beads and one of several possible platelet agonists. A fibrinogen‐platelet interaction, via the GP IIb/IIIa receptor, causes agglutination of the beads and attenuation of light transmission. In one study of 485 patients undergoing elective PCI with GP IIb/IIIa inhibition, the level of platelet inhibition as measured by the VerifyNow was found to significantly correlate with the risk of peri‐PCI thrombotic events Citation[4]. Likewise, Chen et al found that, among 151 patients undergoing elective PCI that non‐responsiveness to aspirin was associated with a significantly higher thrombotic event rate Citation[5].
Flow cytometric methods have been utilized to evaluate platelet function by characterizing the expression of activation‐dependent markers such as P‐selectin, the GP IIb/IIIa receptor, and perhaps more importantly, quantifying platelet‐monocyte aggregates. In three small studies, levels of platelet‐monocyte aggregates were found to distinguish patients with myocardial infarction (MI) from those with unstable angina or noncardiac chest pain. In one of these, platelet‐monocyte aggregate levels were elevated in the setting of acute MI and PCI, while surface P‐selectin expression remained at baseline Citation[6]. The technical difficulties and specialized instrumentation required to perform flow cytometric analyses limit this technique, for the most part, to research applications.
Conclusion. No single test can capture all aspects of platelet functions but there are multiple tests that have various advantages and disadvantages in terms of clinical applicability Citation[7]. While some studies – all small ‐ have shown associations between clinical outcomes and platelet function, others have not. A number of ongoing, large‐scale clinical trials are indirectly studying whether higher levels of platelet inhibition translate into greater efficacy and what impact this might have on safety. The results of these trials will have major implications for the future use of platelet function testing.
Is there a role for IIb/IIIa receptor antagonists in the pre‐hospital setting?
Elena Vasilieva, Alexander Shpektor
Cardiology Department, Moscow State University of Medicine and Dentistry, Moscow, 103473, Russia; Tel/fax:+7(495)9153887, E‐mail: [email protected]
Key Words: IIb/IIIa receptor antagonists, pre‐hospital, ST‐elevated myocardial infarction
Primary percutaneous coronary intervention (PCI) is at present the most efficient treatment of ST‐elevated myocardial infarction (STEMI) Citation[1]. The efficiency of glycoprotein IIb/IIIa (Gp IIb/IIIa) inhibitors in combination with PCI in patients with STEMI was proven in many studies. Meta‐analysis of several trials showed that 30‐day mortality and reinfarctions were decreased by about 30% after the use of IIb/IIIa inhibitors Citation[2,3]. It remains controversial what is the best method of application of these drugs: whether they should be used immediately after STEMI was diagnosed, i.e. in the ambulance or the emergency department or, alternatively, in the catheterisation laboratory just before PCI. To answer this question several randomized trials have been performed. Meta‐analysis of these trials made by Montelesco et al.Citation[3] and Keely et al.Citation[4] revealed that the “early” administration of Gp IIb/IIIa inhibitors appears to improve the coronary patency (TIMI grade III flow, etc). However clear‐cut benefit in clinical outcomes was not observed. The number of major bleedings also did not differ in the two groups. During the last year the results of two additional randomized trials, TITAN –TIMI 34 Citation[5] and RELAx‐AMI Citation[6], were published. Both these trials did not reveal a significant difference in clinical outcomes although one of them Citation[6] showed a significant difference in the frequency of the TIMI III flow in the “early” group. Our analysis, adding the two last trials, confirmed the results of the two previous meta‐analyses ().
How one can explain the apparent contradictions between an improvement of coronary flow and the absence of a clear‐cut effect on clinical outcome? One possibility is that the specific type of Gp IIb/IIIa inhibitor used should be taken into account in the meta‐analysis. Two largest trials, ON TIME Citation[7] and TITAN –TIMI 34 Citation[5], where tirofiban and eptifibatide were used did not show significant differences neither in clinical outcomes nor in frequency of TIMI III grade flow (). On the other hand, significant improvement in the pre‐PCI angiographic findings and in 1‐ month left ventricular function recovery were found in the third large trial, RELAx‐AMI, where abciximab was used Citation[6]. When we performed a separate analysis of 5 trials with tirofiban and eptifibatid and of 6 trials with abciximab, it was found that in the case of ‘early’ infusion of abciximab an increase in TIMI III flow grade was more frequent as compared to that of tirofiban and eptifibatide (p<0.04,χ2). The ‘early’ infusion of tirofiban and eptifibatide did not provide any improvement of clinical outcome. In contrast the mortality rate after the ‘early’ infusion of abciximab was less than a half that after its ‘late’ infusion, although the difference was just below statistical significance (P = 0.06, ). Unlike tirofiban and eptifibatide no one trial with abciximab showed advantage of the “late” infusion for clinical outcome. For further clarification of this problem we should await the publication of the results of just finished large randomized trial, FINESSE Citation[8,9].
Table. Summary of 11 trials comparing ‘early’ and ‘late’ administration of glycoprotein IIb/IIIa inhibitors with primary percutaneous coronary intervention
The Role of Clopidogrel in ST Elevation Myocardial Infarction
Peter Berger, MD, Director
Center for Clinical Studies, Interventional Cardiologst, Geisinger Clinic, Danville, PA
July 2007
Contact information: Peter Berger, MD, Geisinger Center for Health Research, 100 North Academy Avenue, MC 44‐00, Danville, PA 17822, USA; Telephone: 570 214 5057, E‐mail: [email protected]
Until recently, the role of clopidogrel in patients suffering a ST elevation myocardial infarction (STEMI) was unclear. But now there are data that can and should be used to guide the appropriate use of clopidogrel to patients suffering a STEMI .
Patients treated with fibrinolytic therapy. For STEMI patients in whom fibrinolytic therapy is planned, the CLARITY trial provides relevant information. In CLARITY, 3,491 patients suffering a STEMI were randomly assigned to receive a 300 mg loading dose of clopidogrel followed by 75 mg per day, or placebo Citation[1]. All patients received aspirin; any fibrinolytic agent could be used. The primary endpoint was an unusual one, a combination of clinical and surrogate endpoints ‐ a composite of an occluded infarct‐related artery (defined by a Thrombolysis in Myocardial Infarction flow grade of 0 or 1) on angiography 48 to 192 hours after enrollment, or death or recurrent myocardial infarction before angiography could be performed. The results indicate a reduction in the frequency with which the primary endpoint was reached with clopidogrel (a 6.7% absolute reduction in the rate and a 36% reduction in the odds of the end point with clopidogrel [95 percent confidence interval, 24 to 47 percent]; P<0.001). The difference was driven by a reduction in the frequency of an occluded artery on protocol angiography; the differences in the other components of the primary endpoint did not come close to reaching statistical significance. At 30 days, however, clinically and statistically significant differences in outcome did exist. Clopidogrel therapy reduced the composite end point of death from cardiovascular causes, recurrent myocardial infarction, or recurrent ischemia leading to urgent revascularization within 30 days by 20% (from 14.1% to 11.6%, P = 0.03). The frequency of major bleeding was similar in the two groups. The late improvement in clinical outcome is believed to be the result of that fact that patients who underwent a percutaneous coronary intervention (PCI) and had been randomized to clopidogrel had, as a result, been pretreated with clopidogrel; other studies have shown that pretreatment with clopidogrel reduces procedural infarction and other adverse events Citation[4,5]. Although it has been shown that a 600 mg loading dose is more rapid and slightly more potent than a 300 mg loading dose, it is not recommended that 600 mg be given to patients receiving fibrinolytic therapy; the safety of such a strategy has not been examined.
However, it is important to remember that patients older than 75 years of age were excluded form CLARITY Citation[1]; such patients are at the greatest risk of bleeding. Should the CLARITY data derived from patients 75 and younger be generalized to patients older than 75 years of age? Most believe not. The most appropriate management of such patients ought be guided by the results of the COMMIT trial, in which the 45,852 patients with suspected acute myocardial infarction in China of any age were randomized to receive 75 mg of clopidogrel without a loading dose vs. no clopidogrel.(6) Clopidogrel led to a highly significant 9% proportional reduction in death, reinfarction, or stroke (9·2% vs 10·1%, p = 0·002), corresponding to nine fewer events per 1000 patients treated. There was also a significant 7% reduction in death (7·5% vs 8·1%, p = 0·03). The reduction in death, reinfarction, and stroke was consistent across a wide range of patients and independent of other treatments being used. There was no significant excess risk of fatal, transfused, or cerebral bleeds with clopidogrel, either overall or in older patients. And what was fascinating about the study is that the benefits became manifest within 24 hours, even though it takes 5–7 days for clopidogrel to achieve maximal inhibition of aggregation. In COMMIT, the risk reduction in the first 24 hours was greater than that in nearly all subsequent time periods reported.(6)
Primary PCI. There are no data yet to guide one's decisions whether and, if so, when and how much clopidogrel to administer to patients with STEMI in whom primary PCI is planned. However, in the absence of data, it seems most appropriate to administer 600 mg at the time of diagnosis, as soon as possible before PCI. Usually there is sufficient delay between the time of diagnosis and the PCI procedure that substantial antiplatelet affect will have become manifest. Since this has been shown to be beneficial in other settings, it is likely that it is in this setting as well. If the time to PCI is very brief, there may not yet be substantial antiplatelet activity; however, it is certainly unlikely to be associated with harm. The only patients who might be expected to suffer from such a strategy would be patients in whom diagnostic angiography reveals coronary disease requiring coronary artery bypass surgery. However, the frequency with which bypass surgery is required to treat patients suffering STEMI has never been lower, and less than 5% in nearly all series. Even when surgical anatomy is found, it is often most appropriate to treat the infarct artery and perform surgery in the days or weeks to come, after clopidogrel affect has had time to wear off.
Summary. The data, where they exist, and logic, where they do not, suggest that clopidogrel ought to be given to all patients suffering STEMI (unless contraindications exist). Patients 75 years of age or younger in whom fibrinolytic therapy is planned ought to receive a 300 mg loading dose of clopidogrel as soon as possible, followed by 75 mg per day. Patients in whom fibrinolytic therapy is planned who are older than 75 ought receive 75 mg of clopidogrel, without a loading dose, followed by 75 mg per day. In the absence of direct data, it seems most appropriate to recommend that patients in whom primary PCI is planned receive a 600 mg loading dose followed by 75 mg per day.
Clopidogrel: For Whom? For How Long?
Peter Berger, MD, Director
Center for Clinical Studies, Interventional Cardiologist, Geisinger Clinic, Danville, PA
July 2007
Contact information: Peter Berger, MD, Geisinger Center for Health Research, 100 North Academy Avenue, MC 44‐00, Danville, PA 17822, USA; Telephone: 570 214 5057, Email: [email protected]
The most appropriate duration of clopidogrel remains a subject of great interest, sparked by recent concern over the increased risk of late stent thrombosis among patients who have received a drug‐eluting stent. There have now been several randomized controlled trials comparing clopidogrel vs. placebo in patients in many different clinical situations; several shed light on the most appropriate duration of clopidogrel.
Acute coronary sydnromes. In the Clopidogrel in Unstable Angina (CURE) study, 12,562 patients with an acute coronary syndrome were randomly assigned to receive aspirin and clopidogrel or aspirin and placebo for a mean duration of follow‐up of 9 months, and no longer than one year.Citation[1] There was an approximately 20% relative reduction in the risk of vascular death, myocardial infarction, and stroke associated with clopidogrel. The difference between the two arms of the trial continued to widen throughout the study period. These data provide strong evidence of benefit for long‐term clopidogrel (at least 9 months) among ACS patients.
Although the CURE study prohibited medical centers that performed PCI in the majority of patients with an acute coronary syndrome from participating in the trial, a sub‐study of 2,658 CURE patients (21%) who underwent PCI in the CURE trial a median of 10 days after enrollment, not by study protocol but by physician preference, was subsequently reported.Citation[2] Among these PCI patients, the reduction in events (cardiovascular death, MI, or an urgent repeat revascularization procedure) from the PCI procedure through 30 days was an absolute 1.9% (6.4% vs. 4.5%), a relative reduction of 30% (p = 0.03); the difference reflects the benefits of pretreatment with clopidogrel prior to the PCI, since both arms received open label clopidogrel following the procedure. From 30 days after the PCI procedure through the remainder of follow‐up, there was a non‐significant absolute relative risk reduction of 21% (3.9?–3.1%, p = NS).
An interesting finding in PCI‐CURE was that clopidogrel appeared to be as beneficial among the 19% of patients who did not receive a coronary stent as among the 81% of patients who did.Citation[2] These are the only data suggesting benefit from thienopyridines use among patients undergoing balloon angioplasty; an earlier small retrospective study examining thienopyridine use among balloon angioplasty patients had not indicated benefit.Citation[3]
To summarize, therefore, CURE provides strong evidence of benefit from long‐term clopidogrel among ACS patients treated medically, and weaker evidence of benefit from longer‐term clopidogrel among patients undergoing PCI with either bare metal stents or balloon angioplasty alone.
Bare metal stent placement. Following CURE, two randomized trials specifically examined short term vs. longer term clopidogrel after PCI with a bare metal stent. In the Clopidogrel for the Reduction of Events During Observation (CREDO) trial, 2116 patients were randomized assigned to received a 300 mg loading dose of clopidogrel 3–6 hours prior to the PCI proceeded and 12 months of clopidogrel after the procedure vs. 75 mg of clopidogrel at the time of the PCI and only clopidogrel for only 28 days after the procedure.Citation[4] Although this study design is confounded by the difference in therapy on the first day of the therapy, the study provides relatively strong evidence of benefit from longer‐ term clopidogrel, which reduced the combined frequency of death, MI, or stroke by 26.9% (p = 0.02). Importantly, the benefit arose not from preventing stent thrombosis; only two weeks of a thienopyridine appears to be all that is necessary to prevent most cases of stent thrombosis after bare metal stent placement. Rather, the benefit arose from prevention thrombotic events elsewhere in the coronary circulation.
A second randomized trial, the The Randomized Argentine Clopidogrel Cardiology Society (RACS) trial, compared one month vs. 6 months of clopidogrel in 1004 patients after bare metal stent placement.Citation[5] Between 30 days and 6 months, patients assigned to 6 months of clopidogrel reached the primary endpoint of death, MI, and stroke less frequently (1.74% vs. 4.99%, p = 0.010), representing a relative risk reduction of 65%. This study had important limitations; the trial was open label, permitting the possibility of both physician and patient bias. The estimated event rate was much higher than the observed event so the study was undersized, and the differences that existed between the two groups may have resulted from an alpha error, or the play of chance. The study was stopped prematurely by the DSMC following the publication of CREDO, based on an unscheduled analysis without prespecified stopping rules. Nonetheless, it too indicates that longer term clopidogrel was superior to one month of clopidogrel among patients receiving bare metal stents.
Drug eluting stents. Drug eluting stents were approved because of enormous efficacy at reducting the need to repeat procedures and no evidence of increased risk in the 9 or so months after their placement. Subsequently, there have been many reports of stents thrombosing beyond this time frame, even years after their placement.Citation[6] Although controversial, the data suggest that the risk of stent thrombosis is likely greater among patients who receive DES vs. BMS in the 1–5 years after placement. Although clearly late thrombosis may occur among patients who continue to take aspirin and clopidogrel, some studies have suggested a greater risk among patients who discontinue clopidogrel beyond the 3–6 months initially recommended by the United States Food and Drug Administration based solely on the duration required for inclusion in the pivotal trials that led to their approval, and not on the actual duration of tiem that the medications were actually taken. This has led to an advisory endorsed by the American Heart Association, American College of Cardiology, Society for Coronary Angiogrpahy and Intervention, American College of Surgeons, and American Dental Association that clopidogrel be continued for at least one year among patients who receive DES for on label use, and for longer, perhaps, in patients who receive DES for lesions or in clinical situations that are believed to be associated with an increased risk of thrombosis.Citation[6] The recommendaitons seem prudent although it should be emphasized that the optimal duration of clopidgrel after DES in any situation remains unknown.
However, the controversy of whether patients with DES ought to receive 3–6 months of clopidogrel or longer term clopidogrel fails to take into account the proven benefits of clopidogrel throughout the vasculature, at sites remote from the stented site Citation[4,5]. So whether or not clopidogrel is required to reduce the risk of thrombosis of DES long after their placement, the issue is somewhat moot if long term clopidogrel is beneficial for other reasons, as suggested by CREDO and RACS Citation[4,5].
Stable patients with vascular disease. In the Clopidogrel for High Atherothrombotic Risk and Ischemic Stabilization, Management, and Avoidance (CHARISMA) trial, aspirin and clopidogrel were compared in stable patients who had either been diagnosed as having coronary, peripheral, or cerebrovascular disease, or, who had a combination of risk factors for vascular disease.Citation[7] The results indicated that there was not a significant reduction in cardiovascular death, myocardial infarction, or stroke from clopidogrel; the 7.7% reduction in relative risk was not significant. However, patients with established disease (n = 12053) had a larger and statistically significant reduction in risk (6.9 percent with clopidogrel and 7.9 percent with placebo (relative risk, 0.88; 95 percent confidence interval, 0.77 to 0.998; P = 0.046). Patients with multiple risk factors for vascular disease (n = 3284) not only had no benefit but actually had an increased risk. Accordingly, controversy exists whether dual antiplatelet therapy ought to be recommended for patients with established vascular disease based on a subgroup analysis, admittedly a very large one. It is clear that patients with only risk factors for vascular disease ought not receive dual antiplatelet therapy with aspirin and clopidogrel.
Clopidogrel beyond one year. Among patients who receive clopidogrel for one year and are tolerating the drug, it remains unclear whether clopidogrel ought to be continued for a longer duration of time. There are no data to suggest benefit from longer term therapy (except from the CHARISMA trialCitation[7]); the issue has not been addressed by any other studies. It has been shown that the risk of bleeding becomes very low among patients who have been on clopidogrel for more than 6 months and have not suffered a bleeding complication; the risk of bleeding is surely less during the second year of therapy than the first year. Nonetheless, whether patients of any sort benefit from longer term than one year of clopidogrel is speculative. The speculation has been heightened by concerns about late thrombosis of DES; even among DES patients, however, the optimal duration of clopidogrel remains unknown.
Summary. Data from randomized trials indicate that patients with an acute coronary syndrome managed medically, patients receiving a BMS, patients receiving a DES, and probably patients undergoing balloon angioplasty benefit from one year of clopidogrel more than shorter durations of clopidogrel. Data also suggest benefit from long term clopidgrel in patients with stable vascular disease, although these data are derived from analysis of a subgroup; although the subgroup is large, the recommendation is controversial. Whether clopidogrel ought to be continued for greater than one year in any of these groups remains unclear.
Novel Anti‐platelet Therapies
Eli I. Lev, MD
Cardiology Department, Rabin Medical Center, Israel
Anti‐platelet drugs have a pivotal role in the treatment of patients with acute coronary syndromes (ACS), as well as adjuvant treatment given to patients undergoing percutaneous coronary intervention (PCI). Although dual anti‐platelet therapy with aspirin and a thienopyridine has resulted in marked advances in the settings of ACS and PCI, both ACS and PCI are still associated with significant rates of morbidity and mortality from thrombotic – ischemic complications. Furthermore, significant limitations exist among the current anti‐platelet agents; mainly, a slow onset of action, and wide variability in response, which translates into relatively high rates of low response or “resistance” to the anti‐platelets effects of these drugs. Therefore, there is vital need for the development of improved anti‐platelet drugs. Two classes of anti‐platelet drugs are currently being investigated: new generation P2Y12 inhibitors and inhibitors of the platelet PAR‐1 receptor to which thrombin binds ‐ known as a thrombin receptor antagonists (TRA).
Prasugrel (CS‐747), AZD6140, and cangrelor are platelet P2Y12 receptor antagonists that offer faster acting inhibition of ADP‐induced platelet aggregation. They inhibit the same platelet receptor as clopidogrel, but have different pharmacodynamic properties. Prasugrel is an orally administered novel potent thienopyridine that provides faster, higher, and more consistent inhibition of platelet aggregation than clopidogrel. The results of Phase II testing suggest that the risk of bleeding with prasugrel is similar to clopidogrel. The drug is currently tested in a large phase III trial of ACS patients taken to PCI (TRITON‐TIMI 38). AZD6140 is another orally administered platelet inhibitor with rapid and reversible action. Phase II testing also suggests similar bleeding risk to clopidogrel and a phase III trial is underway. Cangrelor is an intravenously administered, reversible, short‐acting agent with a rapid onset of activity. Phase II studies in the PCI setting have shown similar bleeding risk and clinical outcomes to that achieved with abciximab. A phase III PCI trial will soon embark.
The first platelet PAR‐1 (thrombin) receptor inhibitor to be evaluated is TRA‐SCH 530348. In a phase II trial the agent showed a trend toward fewer ischemic events without increasing bleeding when added to standard anti‐platelet therapy with aspirin and clopidogrel in patients undergoing PCI. Two major phase 3 trials with TRA‐SCH 530348 are now planned; one for the treatment of ACS patients and the other for secondary‐prevention in patients with a prior MI, stroke or existing peripheral arterial disease.
The results of large Phase III clinical trials (with over 40,000 patients in total) will hopefully demonstrate whether agents from both groups will be able to improve outcomes in ACS and PCI‐treated patients by providing faster, and more potent and consistent platelet inhibition.
Impact of prior heart failure and prosthetic heart valves in acute coronary syndrome patients
Zaza Iakobishvili, MD, PhD1,2
1The Cardiology Department, Rabin Medical Center, Petah‐Tikva;2Sackler Faculty of Medicine, Tel‐Aviv University
Heart failure (HF) is a well‐documented complication of all types of acute coronary syndromes (ACS), associated with increased morbidity and mortality. Even mild‐to‐moderate HF is a frequent and ominous complication of MI, especially when it does not resolve or develops after admission Citation[1]. A proportion of ACS patients experience HF before the index ACS hospitalization.
Little is known regarding the impact of prior HF on the mode of presentation of ACS, the clinical characteristics of ACS patients with prior HF, or their management and outcomes. Iakobishvili et al. Citation[2] prospectively analyzed all ACS patients admitted in all cardiology wards in Israel during February‐March, 2004. Of the 2098 patients, 156(7.4%) had P‐HF. These patients were older (75[66.5–81] vs. 63[53–74] years, (p<0.001)) and more often female (38.5% vs. 25.0%, p<0.001)), with a higher prevalence of coronary artery disease risk factors, prior cardiac disease and procedures, and other co‐morbidities. They more often presented with atypical angina and heart failure and less with ST‐elevation (18.6% vs. 51.3%, p<0.0001). In‐hospital heart failure developed more frequently (15.4% vs 6.1%, p = 0.00001), including cardiogenic shock (7.1% vs 2.9%, p = 0.005), as did persistent atrial fibrillation (6.4% vs 0.7%, p<0.001), but not ischemic complications. After adjustment for differences, P‐HF was not independently associated with 30d or 6‐month mortality. P‐HF, however, was independently associated with increased incidence of heart failure upon admission or thereafter in‐hospital (OR = 4.3, 95% CI 2.8–6.6).
P‐HF ACS patients had high‐risk features, lower incidence of ST‐elevation, and higher 30d and 6‐month unadjusted, but not adjusted, mortality rates. P‐HF was independently associated with in‐hospital heart failure, suggesting they should be monitored vigilantly.
Another unique subgroup of ACS patients is the patients with pre‐existing valvular heart disease – before as well as after corrective surgery. Patients with ACS and pre‐existing VD constitute about 5% of all ACS patients; they have high‐risk features and poor prognosis Citation[3]. There are few reports regarding acute coronary syndromes (ACS) in patients with prosthetic heart valves (PHV), mostly attributing the ACS to a PHV‐derived coronary embolus. According to the results of case‐series from a small subset of PHV patients from the referral single‐center database patients with PHV and ACS is a rare subgroup, more likely to be elderly with risk factors for atherosclerotic disease and to present with non‐ST‐segment‐elevation ACS. The pathogenesis for ACS is felt to be commonly coronary atherosclerotic disease rather than PHV‐derived emboli Citation[4].
High dose statins – are they safe?
Yaakov Henkin, MD
Dept. of Cardiology, Soroka Medical Center, Beer Sheva, Israel
Results of recent clinical trials of statin therapy in patients with coronary heart disease support the concept that achievement of very low LDL cholesterol levels reduces cardiovascular morbidity and mortality, often associated with regression of atherosclerotic plaques. This resulted in recommendations to aim for LDL cholesterol levels as low as 70 mg/dL in certain patient categories considered at very high risk for cardiovascular events. Achievement of such ambitious LDL cholesterol target goals often requires utilization of high doses of potent statins, sometimes in combination with additional lipid‐modifying drugs. The safety of such treatment regimens is continually being questioned.
Although generally considered as having a very favorable safety profile, statins can cause a number of adverse effects, the most important of which are liver and muscle toxicity. Elevated hepatic transaminases to levels 2–3 times normal generally occur at a frequency of less than 1% and are dose‐dependent. While rarely, if ever, progressing to irreversible liver disease, prolonged transaminase elevations warrant dose‐reduction and/or change of drug regimen. It has been suggested that the frequency of transaminase elevation approaches 2% in patients treated with atorvastatin at a dose of 80 mg daily, but a recent analysis of pooled data from atorvastatin clinical trials showed that the actual frequency of this problem is much less.
A more worrisome adverse‐effect of statins is muscle toxicity. Minor muscle aches are frequent in real‐world observational data, occurring in up to 10% of patients treated by high‐dose statins. In randomized clinical trials myalgia frequently occurs in both statin and placebo‐treated patients, but significant myositis associated with CPK elevations greater than 10 times normal are infrequent and often related to interaction with other drugs. With the exception of cerivastatin, which was withdrawn from use because of an unexpected high rate of rhabdomyolysis‐related mortality, the occurrence of rhabdomyolysis with other statins is rare. Factors that increase this risk include advanced age, female gender, small body frame, renal disease and treatment with multiple medications, especially those that affect the cytochrome P‐450 system. Analysis of controlled trials using high‐doses of simvastatin, atorvastatin and rosuvastatin suggest that the incidence of significant myositis related to the treatment is less than 0.5%.
Having said all that, it is important to remember that the treatment of dyslipidemia, especially in patients with CHD, usually entails life‐long therapy with a statin. Randomized clinical trials of limited duration that enroll meticulously selected patients cannot always reveal adverse effects that are either rare and/or develop after years of continuous exposure to the drug. Detection of these will require long‐term post‐marketing registries of non‐selective statin‐treated patients. In the meantime, prolonged high‐dose statin therapy should be reserved for patients with very high baseline LDL cholesterol levels and patients with a clear indication for aggressive lipid‐lowering. The most important category of patients with the latter indication is those with vulnerable plaques, as exemplified by the occurrence of a recent acute coronary event. Patients with stable atherosclerotic disease rendered at very high risk by virtue of the persistence of uncontrolled risk factors such as diabetes, smoking, very low HDL cholesterol levels or a combination of major risk factors (especially as part of the metabolic syndrome) should also be considered suitable candidates.
Statin therapy in patients with coronary artery disease: The lower LDL – the better
Yoseph Rozenman, MD
The E. Wolfson Medical Center, Holon, Israel
Statin therapy is used worldwide to decrease low‐density lipoprotein cholesterol (LDL‐C) and the associated morbidity and mortality from cardiovascular disease. Recently, data is accumulating to suggest that these effects can be augmented when aggressive (as compared to standard therapy) is used to reduce LDL‐C to well below 100 mg/dL.
Both the PROVE‐IT Citation[1] and REVERSAL Citation[2] compared the effect of standard therapy with 40mg of pravastatin daily to that of 80 mg atorvastatin. Intravascular ultrasound (IVUS) was used in REVERSAL to quantitate treatment related change in atheroma volume. In PROVE‐IT combined clinical endpoint (death, myocardial infarction, hospitalization for unstable angina, revascularization, or stroke) was used to compare among therapies. Atorvastatin therapy reduced median LDL‐C to 62mg/dL (compared to 95mg/dL with pravastatin) and was associated with highly significant 16% reduction in the primary study endpoint. Similarly, while atheroma volume progressed significantly with pravastatin there was no change from baseline in atheroma volume in those treated with atorvastatin. Approximately 90% of atorvastatin treated patients in PROVE‐IT achieved LDL‐C lower than 100mg/dL. The lower the achieved LDL‐C the better was the clinical outcome and those achieving values lower than 40mg/dL had 40% lower event rate than those with levels of 80–100mg/dL. Similarly the greater the reduction in LDL‐C the more pronounced was the effect on atheroma volume ‐ reduction of more than 50% in LDL‐C was associated with atheroma regression. The anti‐inflammatory effect of therapy (as determined by C reactive protein –CRP) was associated similarly with changes in clinical outcome and in atheroma volume Citation[3]. We could thus conclude from the combined analysis of PROVE‐IT and REVERSAL that there is remarkable duality between IVUS and clinical endpoints. Significant reduction and lower achieved level of LDL‐C were associated with attenuation of coronary atherosclererosis progression (regression) and reduction of cardiovascular morbidity and mortality. The ASTEROID Citation[4] trial examined the effect of an even more aggressive LDL‐C lowering (40mg of rosuvastatin) on atheroma volume. Mean LDL‐C was reduced from 130 to 61mg/dL (75% of patients achieving levels lower than 70mg/dL) and was associated with significant regression of atheroma volume.
The advantage of aggressive therapy to reduce LDL‐C was also examined in the TNT trial Citation[5], comparing 10mg to 80mg of atorvastatin in 10000 patients with stable coronary artery disease. High dose atorvastatin was associated with further 23% reduction in LDL‐C and 22% reduction in major cardiovascular events. When patients were divided according to quintiles of achieved LDL‐C, a significant gradual increase in event rates could be demonstrated in higher quintiles. Meta‐analysis of 4 trials Citation[6]–CitationCitation[8] comparing standard to aggressive statin therapy (including more than 25000 patients) demonstrated highly significant 16% reduction in the combined endpoint of death or myocardial infarction.
In summary: The association between on therapy LDL‐C to atherosclerosis progression and the resulting cardiovascular events is now well demonstrated for LDL‐C values as low as 40mg/dL. Aggressive statin therapy to lower targets of LDL‐C than are currently recommended by clinical guidelines is effective to achieve regression of coronary atherosclerosis and to reduce cardiovascular events.
Emergency situations in valvular heart disease
Alec Vahanian
Service de Cardiologie, Hoptal Bichat, Paris, France
Hemodynamic distress may occur in patients with pre‐existing severe valvular disease as was the case in 8% of the patients included in the first SHOCK registry.
We shall review the problem in patients with native valve disease and in those with valve prosthesis.
Patients with native valve disease
Aortic Stenosis. The incidence of cardiogenic shock in patients with aortic stenosis is unknown but should not be ignored in Western countries.
The clinical diagnosis may be difficult in critically ill patients as the valve disease may be unknown or previously known in patients who did not receive appropriate care.
The diagnosis using echocardiography may be difficult because of the concomitance of low gradient and low ejection fraction. In such cases the diagnosis will result from an integrative approach focused on the extent of valve classification and dobutamine stress echocardiography when feasible.
An attempt at medical therapy is mandatory in all cases. Emergency surgical aortic valve replacement is associated with high mortality and morbidity but should, however; be considered and carefully discussed with surgeons. If the intervention seems to be too high risk balloon aortic valvuloplasty may be used as a bridge to a secondary valve replacement. In the future a new percutaneous aortic valve implantation could be attractive in this setting.
Aortic Regurgitation. Acute aortic regurgitation is mostly observed during endocarditis and here again the diagnosis relies on clinical findings and echocardiography. Urgent intervention is mandatory in this setting, despite its high risk.
Mitral Regurgitation. Acute mitral regurgitation can also be observed during endocarditis even if less frequent than aortic regurgitation. It is most often observed due to papillary muscle rupture during acute myocardial infarction. The rupture of the papillary muscle should be confirmed by echocardiography where the diagnosis should be sought for on the combination of shock and hyperdynamic heart. Here again surgery is mandatory, mostly using mitral valve replacement.
Mitral Stenosis. In mitral stenosis the occurrence of cardiogenic shock is rare. It may be observed in a young patient with undiagnosed mitral stenosis or in the elderly at the very end stage of the disease. Balloon mitral valve commissurotomy or, if this is not feasible, mitral valve replacement is the treatment of choice.
Patients with valve prosthesis
The diagnosis of obstructed valve thrombosis should always be looked for using emergency echocardiography and fluoroscopy in a patient with valve prosthesis presenting with cardiogenic schock. In left heart valve prosthesis, emergency surgery should always be considered as the first option. However, fibrinolysis can be performed if patients are critically ill and if surgery is not immediately available, contraindicated, or very high risk. On the other hand fibrinolysis is the first choice in case of obstruction of a right heart valve.
Conclusion. In conclusion, underlying valve disease should always be looked for in patients with cardiogenic shock even if it is rarer than ischaemic heart disease or cardiomyopathy. Successful management relies on a prompt combination mostly based on echocardiography and intervention, which is surgical in most cases and interventional in selected cases. In the future these very high‐risk patients could be candidates for the new percutaneous valve interventions.
Echocardiography for the diagnosis of acute emergencies in the CCU
Alexander Sagie, MD
Rabin Medical Center, Israel
Echocardiography, both transthoracic and transesophageal has gained a mandatory pivotal role in the assessment of patients presenting with acute heart failure Citation[1].
Cardiac catheterization which was so important in the past to diagnose many of these pathologies is seldom needed for the diagnosis and is done mainly for those patients who need emergent surgery to rule out coronary artery disease. Most hemodynamic parameters such as pulmonary pressure, end diastolic pressure, shunts calculations, valves area and severity of valve regurgitation are easily obtained by echocardiography Citation[2].
Echocardiography (TTE or TEE) is the best imaging modality to diagnose the etiology of acute hemodynamic deterioration and should be performed as soon as possible Citation[3]–CitationCitation[5]. It can be done at bedside without the need to transfer the patient away from the intensive care setting to CT or MRI laboratory where monitoring of the patient is not ideal. In most of the cases simple tansthoracic echocardiography in expert hands is enough to make most of the diagnoses needed Citation[6]. TEE is sometimes acquired but in many cases can be done later on in the operating room when needed. By echocardiography we can differentiate between cardiogenic and non cardiogenic reasons for the patient's acute deterioration. By ruling out other reasons for shock it can direct the physician to the diagnosis of septic shock. It can easily diagnose significant LV or RV dysfunction as the cause for shock, critical stenosis or severe valvular regurgitation, mechanical complication of acute myocardial infarction, acute tamponade, hypovolemia, acute aortic dissection, and also directing the physician for the possibility of acute pulmonary emboli.
Of special emphasis is the value of echocardiography on the diagnosis and treatment of patients with native and prosthetic valvular emergencies. Acute or chronic dysfunction of native and prosthetic valves may cause hemodynamic deterioration resulting in cardiogenic shock and should be considered in its differential diagnosis. In the shock trial registry Citation[7] of 1190 patients with cardiogenic shock, 8% suffered from a preexisting severe valvular disease, which caused or worsened their hemodynamic status. A rapid diagnosis of a valvular etiology in a patient with acute hemodynamic deterioration is very important because emergency intervention such as intensive medical therapy, percutaneous balloon valvuloplasty Citation[8]–CitationCitation[10], or emergent valve replacement can be effective, and, at times, life saving. Clinical clues (from the patient's history, symptoms and signs) suggesting valvular etiology are very important.
The use of new percutaneous valve interventions
Alec Vahanian
Bichat Hospital, Paris, France
New percutaneous treatments are now front line in patients with coronary artery disease and have been performed in patients with valve disease for more than 20 years.
Today percutaneous mitral commissurotomy has virtually replaced surgical commissurotomy and is the complement of valve replacement.
On the other hand percutaneous aortic valvuloplasty in isolation is very seldom performed because of the limited efficacy and high risk.
The quest continues for new techniques in patients with aortic stenosis and mitral regurgitation, and the rationale for this approach is that there still remain many patients, especially elderly, who are high risk for surgery or are even untreated as they are not referred for surgical treatment by their physicians.
Aortic valve implantation was performed for the first time by Alain Cribier in 2002.Today, more than 500 patients have been treated with this technique using either the transfemoral or transapical approach. Two devices are used. Both are valves mounted in stents, however, one is balloon expandable and the other self‐expandable.
Current results show that the technique is feasible and provides good valve function. However, the risk remains high which is due both to the critical condition of the patients submitted to the treatment so far and also to procedural complications, mostly related to the high profile of the device resulting in potential vascular damage when using the transfemoral approach.
Percutaneous mitral valve repair was first performed slightly later. Two major techniques have been explored. The first one is edge‐to‐edge mitral valve repair, which replicates the Alfieri operation. It is a difficult technique requiring transseptal catheterization and the tip of both valves must be caught during systole. Ongoing registries show that in expert hands the technique is feasible, carries a low risk and results in a significant decrease in the degree of regurgitation in two‐thirds of cases. These results being stable in 2‐year follow‐up.
The second approach consists of percutaneous mitral annuloplasty via the coronary sinus. The technique is easier. The results reported concern a primary series of less than 100 patients. They show the feasibility of the procedure, however, efficacy data are still lacking.
Thus, the first steps of the new percutaneous valve interventions have shown that these techniques are feasible. The development of theses techniques will require close collaboration between interventionists, echocardiographists and surgeons. Results should be compared carefully to surgery and contemporary medical treatment. The potential candidates could be those at high risk for surgery or with contraindications to surgery, and may expand to less sick patients in the future.
Ventricular Assist Device Support and Heart Transplantation in Postmyocardial Infarction Cardiogenic Shock
Jacob Lavee, MD
Heart Transplantation Unit, Department of Cardiothoracic Surgery, Sheba Medical Center, Tel Hashomer, Israel
Cardiogenic shock (CS) is the leading cause of death in patients with acute myocardial infarction (AMI), with a reported incidence of 7% to 10% and a mortality rate of 60% to 80% Citation[1]–CitationCitation[3]. The international SHOCK trial demonstrated that in patients with AMI complicated by CS early mechanical re‐vascularization reduced 6‐ and 12‐month mortality compared with initial medical stabilization Citation[2,3], however long term survival, even with the use of intra‐aortic balloon pumping, remains grim. In recent years several studies have shown that circulatory support, including the use of extracorporeal membrane oxygenator (ECMO) and/or left ventricular assist device (LVAD) as bridge to heart transplantation in carefully selected patients with post‐infarction CS, represents the most effective therapy with short‐ and long‐term survival benefits when compared to either conservative medical therapy or even to re‐vascularization ()Citation[4]–CitationCitation[6]. Efforts have been made to develop VADs capable of providing complete hemodynamic support, readily connected to the patient's circulation by interventional methods without the need for extracorporeal oxygenation or surgical procedures. This review will present the current LVAD experience in the CS setting, starting from percutaneous extracorporeal support up to bridge therapy with surgically implanted devices.
The most recent data regarding the use of the following devices in patients with CS will be reviewed: ABIOMED BVS 5000 (Abiomed, Inc, Danvers, MA), a short‐term pulsatile paracoroporeal device implanted surgically via mid‐sternotomy; TandemHeart LVAD (Cardiac Assist, Pittsburgh, PA), a short‐term, percutaneously implanted, paracorporeal centrifugal device; Levitronix Centrimag LVAD (Levitronix LLC, Waltham, MA), a short‐term paracorporeal centrifugal device implanted surgically via mid‐sternotomy; Impella Recover LD (Cardiosystem AG, Aachen, Germany), a short‐term micro‐axial pump, implanted inside the left ventricle either surgically or percutaneously; Thoratec pneumatic VAD (Thoratec Corp, Pleasanton, CA), a long‐term paracorporeal pulsatile device implanted surgically; HeartMate vented electric LVAD (Thoratec Corp, Pleasanton, CA), a long‐term intra‐corporeal pulsatile device, and Jarvik 2000 FlowMaker LVAD (Jarvik Heart, Inc., New York, NY), a long‐term intra‐ventricular axial flow device implanted surgically. While the percutaneously implanted devices avoid the need to cannulate the acutely infracted and friable left ventricular apex, recent data, as well as our own results, have shown that surgically implanted LVADs can be safely implanted into acutely infarcted myocardium by modifying surgical technique. As the percutaneously implanted devices are generally intended for shorter‐term use compared to the surgically implanted devices, the choice of each particular device, based on its performance and the expected availability of donated heart for transplant, will be discussed.
The cumulative data obtained from the use of these devices has shown that LVAD support in patients with post AMI CS is a safe and effective therapy which should be incorporated into the standard treatment paradigm for appropriate patients presenting with this lethal disease. Expanded use of LVAD in this setting may reduce mortality and provide a bridge to transplant and perhaps even recovery of adequate left ventricular function in a small percentage of patients.
Figure 1. Kaplan–Meier 5‐year survival for sub‐groups of patients with post AMI cardiogenic shock treated with PCI/CABG (n = 77) vs ECMO/LVAD/OHT (n = 18) (PCI, percutaneous coronary intervention; CABG, coronary artery bypass graft; ECMO, extracorporeal membrane oxygenation; LVAD, left ventricular assist device; OHT, orthotopic heart transplant). (From Ref # 4).
Nitric Oxide Synthase Inhibitors in Post‐Myocardial Infarction Cardiogenic Shock‐ An Unfulfilled Promise?
Edo Kaluski, MD, FACC, Marc Klapholz, M.D., FACC
Department of Cardiology, University Hospital and the University of Medicine and Dentistry, Newark, NJ
Correspondence: Edo Kaluski, M.D., F.A.C.C, Director of Cardiac Catheterization Laboratories, 185 South Orange Ave. MSB I‐538, Newark, NJ, 07101, USA. Tel: 973‐738‐2603, Fax: 973‐972‐8927, E‐mail: [email protected]
Abstract: Cardiogenic shock (CS) is the leading cause of mortality among hospitalized patients with myocardial infarction. Even with contemporary primary percutaneous coronary revascularization (PCR), CS carries a case fatality rate of 40–50%. CS victims succumb as a consequence of profound systemic metabolic abnormalities and inflammatory activation (with nitric‐oxide overproduction) that is accompanied by severe myocardial stunning and dysfunction. Most survivors, however, enjoy a satisfactory quality of life. In view of the systemic nature of CS, therapies counteracting or mitigating nitric‐oxide (NO) overproduction, were evaluated. Summarized is the data available regarding safety and efficacy of NO synthase (NOS) inhibitors in CS resulting from myocardial infarction.
Key words: Nitric oxide, Nitric oxide synthase inhibitors, Cardiogenic shock, ST‐elevation myocardial infarction.
Abbreviations: Nitric Oxide (NO), Cardiogenic shock (CS), ST‐elevation myocardial infarction (STEMI), percutaneous coronary revascularization (PCR), nitric oxide synthase (NOS),
Nitric Oxide Synthase Physiology: Three NOS isoforms convert L‐arginine to NO and citrulline. NO (a highly reactive free radical), is metabolized within seconds to yield nitrite (NO2−), nitrate (NO3−), nitrosothiols and N‐nitrosoproteins. These serve as NO storage pools, and indicators of NO levels Citation[1]. NO executes numerous signaling and regulatory functions in all mammalian tissues and systems. ST‐elevation myocardial infarction (STEMI) with subsequent CS causes a systemic inflammatory response Citation[2], excessive activation of inducible NOS and NO overproduction. NO promotes vasodilation, and myocardial dysfunction. The potential mechanisms of myocardial dysfunction are 1) Peroxynitrite overproduction and toxicity (produced from superoxide and NO), 2) Impaired mitochondrial function and respiration Citation[3], 3) Abnormal calcium handling and response to cathecolamines Citation[4]. These adversities are partially alleviated by NOS inhibition Citation[5].
CS in STEMI‐ beyond PCR: CS occurs in 5.5–14% of STEMIs, and is best treated with early PCR accompanied by comprehensive cardio‐respiratory support. However, within 30 days following emergency PCI, 45% –47% Citation[6], of CS patients will succumb to their illness. STEMI related post‐PCI CS results from extreme pump failure from suboptimal myocardial reperfusion or salvage and profound myocardial stunning. Since 75% Citation[6] of CS survivors have minimal residual symptoms it is believed that the myocardial dysfunction observed during CS is to a large extent reversible.
NOS inhibitors in PCI refractory CS
Seeking a relatively safe agent that would counteract the profound hypotension and myocardial depression in CS without precipitating tachycardia or arrhythmias, CS investigators studied NOS inhibitors. Cotter Citation[7] assessed L‐NMMA (NG‐monomethyl‐L‐Arginine (1mg/kg intravenous bolus, and 1 mg/kg/h IV drip for 5 hours) efficacy and safety in 11 patients, who remained in refractory CS after PCI for STEMI. The investigators reported. The blood pressure rise was accompanied by significantly improved cardiac power index. Urinary output nearly tripled during the initial 24 hours of therapy. Of the 11 patients treated, 8 (73%) were discharged from the CCU, and 7 (63%) remained alive at 3 months.
A single‐center randomized trial, assessed the efficacy of L‐NAME (NG‐Nitro‐L‐Arginine‐Methyl Ester Hydrochloride)] 1mg/kg bolus and 1mg/kg/h drip for 5 hours, in 30 consecutive patients with PCR‐refractory cardiogenic shock Citation[8]. Thirty day mortality was 27% in the L‐NAME treated patients and 67% in the control arm (p = 0.008). Mean arterial blood pressure 24 h post randomization was 86±20 in the active treatment arm and 66±13 in the placebo arm. Urine output, intra‐aortic counter‐pulsation and mechanical ventilation duration were all favorably affected. L‐NAME did not increase the cardiac index but had an impressive effect (80% rise increase at 24h) on cardiac power index.
The NIH sponsored a multi‐center, randomized, phase II, study (SHOCK 2) to assess dosing, efficacy and safety of L‐NMMA (dose range 0.15–1.5 mg/kg bolus and 0.15–1.5 mg/kg/h for 5 hours) in PCI refractory cardiogenic shock The primary and secondary endpoints of this study were blood pressure response at 2 h after drug administration and mortality at 1 and 6 months respectively. Additional parameters assessed were urine output, cardiac power (at 2, 6 and 24 h), and duration of vasopressor administration, intra‐aortic counter‐pulsation and ventilation support.
This study was unfortunately handicapped by several limitations Citation[9]: Uneven distribution of high‐risk predictors (i.e. anterior vs other location of STEMI) between study groups and down‐titration of inotropes complicated data interpretation. Significant treatment‐related increases in systemic blood pressure response were observed at 15 minutes but not at 2 hours. Neither mortality benefit nor safety issues were noted.
The recently published TRIUMPH Citation[6] trial, was a phase 3, multi‐center, prospective, randomized, double blind, placebo‐controlled study to assess the safety and efficacy of NOS inhibitor, Tilarginine acetate, in CS. The study was well designed and meticulously executed. The study was terminated after 398 patients were enrolled based on pre‐specified futility analysis. Tilarginine therapy did not favorably affect 30 day (48% versus 42% p = 0.24) and 6 month mortality, duration of CS, or survivors' functional class. Drug effect on 2 hour systolic blood pressure was noted () and was predictive of favorable outcome. It is still possible that the drug was administered in insufficient dose or duration.
Summary: Contemporary therapy of STEMI related post‐PCR CS carries a case fatality rate of 45%. It is estimated that 200,000 patients will die annually from CS in Europe and the USA. Two large scale randomized trials of NOS inhibitors failed to demonstrate meaningful hemodynamic or clinical benefits in the doses tested. The disappointing results of TRIUMPH create a considerable void in therapy for CS that hopefully will be filled by other pharmacological, mechanical or cell‐based innovations.
Table 1. Results of TRIUMPH
The Intraaortic Balloon Pump: Current status and new technologies
Ayzenberg O., Gandelman G.
Department of Cardiology, Kaplan Medical Center, Rehovot, Israel
During the last three decades, the Intraaortic Balloon Pump (IABP), has played a key role in the treatment of high risk cardiac patients. By reducing afterload, left ventricular wall tension and oxygen demands on the one hand and improving coronary flow on the other, the prospects of stabilizing patients with severe ischemia and and/or severe left ventricular dysfunction, are improved . In this way, crucial time needed to perform percutaneous interventions or cardiac surgery is achieved. Early stabilization and prompt treatment contribute to the significant reduction seen today in morbidity and mortality.
The main indications for IABP includes :
Cardiogenic shock complicating acute myocardial infarction is the leading cause of mortality and Is the most common cause for IABP usage, Accounting for about 20% of the insertions in the USA Citation[2]. Among 23,180 subjects with acute MI and cardiogenic shock in which about third of patients have undergone IABP insertion, those who received trombolytic therapy and IABP insertion, had in hospital mortality of 49% as opposed to a mortality of 67% in patients with no IABP insertion (p<0.001) Citation[3].
Cardiogenic shock due to severe mitral regurgitation caused by papillary muscle rupture, ventricular septal rupture and severe cardiac arrythmias are less common indications but nevertheless important ones for IABP insertions Citation[2],Citation[4,5].
High risk percutaneous intervention with or without myocardial infarction is an important indication for IABP. In ever growing group of patients with low ejection fraction, severe triple vessel disease , left main disease, sometimes associated with unstable angina or hemodynamic instability, one should strongly consider IABP insertion.
Elective versus Rescue IABP is a major dilemma. The technological advances on the one hand and improved peri procedural medications on the other, are associated with decreased morbidity and mortality resulting in increased operator confidence, thus decreasing the use of IABP electively. However, in spite of these encouraging results, high risk PCI patients could rapidly and irreversibly deteriorate. One should aim to assess the risk prior to the procedure avoiding periprocedural complications and achieving lower in hospital mortality. Elective IABP insertion in high risk patients was associated with higher success rates, lower in hospital mortality and lower major adverse cardiac events . At 6 months the mortality and major adverse cardiac events rates were lower in the prophylactic IABP group ( 8% vs 29%, p<0.01, and 12% vs 32% p = 0.02 respectively). Multivariate analysis showed that prophylactic insertions of an IABP is the only independent predictor at 6 months Citation[6].
Patients with unprotected left main are a growing challenge , data are strongly supporting elective IABP insertion rather than rescue. Although the elective IABP group had higher Euroscore, it had no episodes of hemodynamic instability and was characterized by lower major adverse cardiac events (1.5% vs 9.5% p = 0.032) . Elective IABP support and presence of Euroscore greater than 6,and bifurcation lesion, were the independent predictors of intra procedural events (OR 5.49, 95% CI 1.47–20.51, p = 0.011 ) Citation[7].
Coronary bypass grafting in high risk patients prior to and post surgery is another important indication for IABP insertion. It has been shown to improve outcome Citation[8]. Nowadays, a growing number of high risk patients are undergoing off – pump coronary artery bypass grafting. Elective insertion of IABP showed no significant differences in mortality, but allowed early hospital discharge and lower incidence of acute renal failure Citation[9]. Apart for the Euroscore, attempts were made to define a more specific IABP score, predicting survival based on adrenalin requirement, left atrial pressure, urine output, and mixed venous saturation Citation[9]. A partially different risk score based on four parameters: mean arterial pressure, adrenalin dose, central venous pressure and blood lactate concentration was also proposed Citation[10]. In those with a very high risk score, the insertion of IABP will not suffice and ventricular assist device should be considered Citation[9,10].
Responding to the challenging demands, the industry developed IABP with better sensitivity to detection of the dicrotic notch at higher ventricular rates with association with arrythmias. lower French size catheters were also developed. Properly timed IABP decreased left ventricular end systolic volume by 6.1% (p<0.0001) and left ventricular end systolic pressure by 17.5% (p<0.0001) due to decreased aortic impedence Citation[11].
Limb ischemia is one of the major risks in IABP insertion. Peripheral vascular disease and Diabetes Mellitus were found to be significant risk factors for leg ischemia ,sheathed method of insertion would increase the probability of ischemia almost 35 times, thus sheatless insertion is highly recommended. and therefore should be the method of choice in those patients Citation[12].
The early identification and immediate treatment of high risk cardiac patients, combined with advanced technologies, will allow interventional cardiologists and cardiac surgeons to achieve better immediate and long term results.
The management of sub‐massive pulmonary embolism
Hanoch Hod, MD, FACC, FESC
Intensive Cardiac Care Unit, Heart Institute, Sheba Medical Center, Tel Hashomer, and Sackler School of Medicine, Tel Aviv University, Tel Aviv, Israel
Pulmonary embolism is a common and often fatal disease. As many as 650,000 cases are estimated to occur each year in the US. Overall three‐month mortality rate for all patients who present with pulmonary embolism (PE) is 15%, for those in shock the mortality rate is nearly 50%. In the immediate course, 10% of symptomatic PE is fatal within 1 hour of symptom onset.
For clinical purposes PE can be classified as: massive and non‐massive. Patients with massive PE presenting with shock/hypotension typically have >50% obstruction of pulmonary vasculature. Patients with non‐massive PE are normotensive. A sub‐group of patients with non‐massive PE who have one‐third or more obstruction of pulmonary vasculature, may be identified by echocardiographic signs of right ventricular hypokinesia. This group is defined as “sub‐massive PE”.
Frequently patients with this condition have elevated high troponin levels and BNP. The prognosis of this sub‐massive group of patients may be worse than those with non‐massive PE and normal RV. They are at higher risk for recurrent PE and many of them may require escalation therapy with hemodynamic support and mechanical ventilation.
The management of sub‐massive PE should be focused on two major points:
Detection and immediate relief of right heart failure.
Prevention of recurrent PE.
Anticoagulation is a critical component of the management of patients with sub‐massive PE and is the “gold standard” of treatment.
In 1960 Barrit et al published a placebo‐controlled, randomized trial in Lancet utilizing unfractionated heparin (UFH) in PE. There were no deaths or recurrent PE in the treated group, whereas in control mortality was 26% and recurrent PE 26%. Although weight‐adjusted SC LMWH has been shown to be as safe and effective as UFH in treating non‐massive hemodynamically stable PE, the data utilizing LMWH in sub‐massive PE are still limited. The same is true for fondaprinux an indirect Factor Xa inhibitor and direct thrombin inhibitors such as argatroban and lepirudin.
Although thrombolitic therapy is indicated in patients with massive PE, the use of thrombolytic therapy in patients with sub‐massive PE (normotensive with RV hypokinesia) is controversial. In the MAPPE‐3 trial patients with sub‐massive PE were randomized to UFH plus Alteplase vs UFH plus placebo. Although the in‐hospital mortality was similar in the two groups, the incidence of clinical deterioration requiring escalation of treatment was higher in the UFH plus placebo group.
The current available data provide no evidence to demonstrate a benefit of thrombolytic therapy compared with heparin for the treatment of all patients with acute PE.
A clear benefit is suggested among those at higher risk of recurrence or death, particularly patients with hemodynamic instability. More studies are needed for better definition of the risk benefit ratio for thrombolytic therapy in sub‐massive PE patients.
Acute pulmonary thrombectomy has a limited role in massive PE. Surgical embolectomy has been used in critically ill patients when thrombolysis is contra‐indicated. The peri‐operative mortality is as high as 44%, and the indication for surgery is currently: a) patients with acute massive PE; b) patients with contra‐indication to thrombolytic therapy; c) patients who lack a response to intensive medical treatment including thrombolyis. There are very limited data on the role of surgical embolectomy in sub‐massive PE.
There is also no evidence of a beneficial effect with the use of mechanical fragmentation technique in sub‐massive PE.
Inferior vena cava filters (IVC) may be used in patients with PE when anticoagulation is contraindicated and in patients with recurrent PE, despite well‐documented anticoagulation. Recently removable IVC filters have become available, however more experience is needed to define whether these devices may offer effective, short‐term protection against recurrent PE without the negative long‐term sequelae associated with permanent IVC filter placement.
All patients who experience PE should be anticoagulated: patients with a first episode of PE should be anticoagulated for at least 3 months, if they have a reversible risk factor, and for 6 months if they have idiopathic VTE. Oral anticoagulation should be continued for a longer period, possibly indefinitely, in patients with recurrent VTE or continuing risk factors such as cancer.
Because sub‐massive PE may cause significant morbidity and mortality when under‐treated, early risk stratification based on clinical assessment, cardiac bio‐markers, ECG, echocardiography, chest CT and V/Q scan, is crucial in the selection of optimal therapy in this sub‐group of patients.
Every center involved in the treatment of these patients should establish a multi‐disciplinary team that includes: an ER physician, a cardiologist, a general intensivist, a hematologist, a roentgenologist, and a cardiac surgeon. This team should build an algorithm/protocol for rapid and accurate risk assessment and treatment.
CPR in 2007 – What's new?
Rudolph W. Koster, M.D.
Department of Cardiology, Academic Medical Center, Amsterdam, The Netherlands
New Guidelines 2005. Guidelines on Cardio‐Pulmonary Resuscitation (CPR) have changed the way cardiac arrest is handled, most recently in December 2005.Citation[1] These guidelines have consequences for management by lay rescuers and professionals, both pre‐hospital and in‐hospital.
Many of the changes are intended to increase the amount of chest compressions delivered per minute by minimizing interruptions for other tasks. The most prominent changes are in the compression:ventilation ratio, that increased from 15:2 to 30:2. Also, the protocol for defibrillation changed by introducing the single‐shock scenario without a check for the outcome of that shock and immediate resumption of chest compressions for two minutes before analysing the heart rhythm again. Already one study suggests that this new scenario may be effective.Citation[2]
For lay persons, identifying the need for CPR are simplified. Instead of looking for signs of (absence of) circulation, including lack of responsiveness, absence of movement and breathing, now only the combination of unconciousness and absence of NORMAL breathing are sufficient to start CPR. One of the main reasons to this change was the appreciation that gasping was very confusing to lay witnesses and it resulted in the inappropriate conclusion that the patient was breathing and did not require CPR. The instruction for hand position is simplified by avoiding the positioning guided by the xyphoid, but new instructions simply tell to position the hands “in the middle of the chest”.
The role of drugs in Advanced Life Support (ALS) is not increased. Adrenalin and amiodarone remain key drugs, but the role of vasopressin is not emphasized, nor is bicarbonate for correction of acidosis during arrest.
In post‐resuscitation care the importance of therapeutic hypothermia is confirmed and the indication extended to coma after in‐hospital arrest, after other rhythms than ventricular fibrillation and to coma after arrest in children.
Implementation of guidelines. A major task, after publication of new guidelines is to ensure that they are implemented. This is no simple task: it implies instructions to many lay and professional rescuers and ajustment of manual and especially automated external defibrillators (AEDs). This may be a prolonged effort that needs to be monitored. The same is true for in‐hospital changes, where investment and training in hypothermia equipment is needed.
New developments. Several new issues are in the focus of attention. These all are related to the renewed recognition of the importance of minimally interrupted chest compressions during CPR, while maintaining optimal rate and depth of compressions. It has been shown abundantly that these aspects are not well perfomed by lay and professional rescuers. Feedback mechanisms are studied to assist the rescuer in these tasks: metronomes and compression depth feedback systems are now being implemented in new devices. Chest compressions require force and endurance of the rescuer, who by fatigue quickly loses the capability for adequate chest compressions. Therefore, new mechanical devices are being introduced, that could be helpful in taking over this task from the rescuer. Unfortunately, new data do not demonstrate improved outcome, while incidental reports suggest the possibility for damage of internal organs by these devices.Citation[3]–CitationCitation[5] New studies are being undertaken to demonstrate the expected benefit, learning from earlier possible mistakes in study design.
A recent study challenced the usefulness of ventilation in CPR, demonstrating increased survival when mouth‐to‐mouth ventilation was not done and chest compressions were given uninterrupted.Citation[6] However, this restrospective observational study had several design flaws that make the conclusions not simply acceptable.Citation[7]
Guidelines 2010. The International Liaison Committee on Resuscitation (ILCOR) is currently starting up the process of revision of the Guidelines 205, to be published late 2010. Many gaps in knowledge are identified and studies are being performed to fill the gaps. It can be expected that new and important insights, developments and techniques will be published in the next 3 years, justifying revesion of guidelines in this process.
The New Atrial Fibrillation Guidelines
Amos Katz
Cardiology Department Barzilai Medical Center Ashkelon and Faculty of Health Sciences Ben Gurion University, Israel
Atrial fibrillation (AF) is the most common cardiac rhythm disturbance and as such represents a substantial challenge to cardiologists. Over the past 20 years, hospital admissions for AF have increased by 66%, and AF now accounts for about one third of US hospitalizations for cardiac rhythm disturbances. The annual cost in the US of treating the disease is about $3600 per patient, making AF one of the costliest public health problems. Although not directly life‐threatening, AF significantly increases the risk of all‐cause mortality, primarily from cardiovascular‐related causes such as heart failure and, of primary concern, stroke.
Effective management of AF is critically important in the prevention of stroke. Proper management of AF requires a thorough knowledge of therapeutic approaches including a strong understanding of the relative benefits of rate control vs. rhythm control, use of antiarrhytmic drugs, ablation therapy or implantable devices and the use of anticoagulation therapy.
Based on the wealth of recent clinical trial data, the American College of Cardiologists/American Heart Association/European Society of Cardiology has updated their guidelines for the management of patients with AFCitation[1], Citation[2]. This lecture is designed to help cardiologists understand the key changes to the new AF management guidelines in order to help them use this information to improve the treatment of patients in their own practices
There are essentially 3 important changes in clinical recommendations in the new guidelines. The first is the inclusion of catheter ablation for AF as one of the therapeutic options for patients with more persistent AF. The second is a striking change in the anticoagulation guidelines. The threshold for anticoagulation has been raised and the guidelines are quite specific about risk factors for stroke in various risk groups. The third change reflects the data from the great number of studies on rate vs. rhythm control that have come out in the past few years. As a result, the guidelines include an expanded section on rate control drugs in both acute and chronic settings. There are also some minor changes with respect to which antiarrhythmic drugs should (and should not) be used.
PURPOSE/GOAL: To inform cardiologists and other healthcare professionals of how the 2006 Atrial Fibrillation Management guidelines will impact the management of patients with atrial fibrillation.
EDUCATIONAL OBJECTIVES
Describe the impact of the new 2006 ACC/AHA/ESC treatment guidelines for the optimization of AF management.
Understand the key changes in the AF guidelines, especially with regard to anticoagulation, antiarrhythmic and ablation therapy.
Discuss how to make appropriate choices for AF management in specific patient populations based on the new guideline recommendations.
Mechanisms of ventricular remodelling
Roberto Ferrari, G. Guardgli
University Hospital of Ferrara, Italy
Chronic heart failure (CHF) is a common and disabling syndrome with a poor prognosis. It is a major and increasing health problem, closely associated with advanced age. Despite optimum treatment with neuroendocrine antagonists – such as angiotensin‐converting enzyme (ACE)‐inhibitors, β‐blockers and antialdosterone compounds‐, prognosis of CHF remains poor. Patients complain of persistent and often progressive reduction in their exercise capacity and quality of life. Fatigue and shortness of breath, the two common and disabling symptoms in patients with CHF, are very often associated to further enlargement of the affected ventricle with relative changes in its shape, geometry and function. This phenomenon has been named “ventricular remodelling”. It occurs mainly as a consequence of large infarction or of pressure and volume overload. It consists of two main phases: a – early remodelling – which occurs at the site of myocardial damage (necrosis in the case of ischaemic remodelling) and results in thinning of the ventricular wall, scar formation and consequent enlargement and re‐shaping of the ventricular chamber; b – late phase remodelling – which might occur months or even years after the initiating insult in the still viable myocytes (i.e. in region of the ventricle not affected by the infarction). While the first phase of remodelling can be considered a positive, repairing process allowing the formation of a scar, the second phase, involving the myocytes, is deleterious and responsible for the progression of the syndrome Citation[1]. The full molecular mechanism if late phase remodelling is not completely understood Citation[2]. Remodelling myocytes shows a typical switch towards the embryonic phenotype (i.e. they re‐express atrial natriuretic peptides in the ventricles, embryonic myofilaments and Ca++ related proteins such as the embryonic sarcoplasmic reticulum Ca2+ ATP‐ase) and classical features of apoptosis and/or hypertrophy. Interestingly, these two processes, although activated and regulated by similar intracellular cascade, represent opposite signals for the myocytes: a signal of death – apoptosis and a signal of life – hypertrophy. This is not at all surprising as the so called “cell life and death cycle” is an intrinsic component of nature itself. Almost every cell of the organism undergoes “the cell cycle” (i.e. a red blood cell lives for 120 days; a neutrophil for 7 hours!). The adult myocytes, however, is a terminal cell; usually it is not able to reproduce and death is not genetically programmed (apoptosis) but occurs by necrosis as consequence to a non‐expected event (i.e. the occlusion of a coronary artery by a thrombus). The embryonic myocytes, contrary to the adult one, undergoes the full cell cycle: it dies by apoptosis and it is able to reproduce. Thus, it has been postulated that the re‐instatement of apoptosis and development of hypertrophy – which occurs during remodelling – is part of the switch towards the embryonic phenotype with re‐instatement of the early embryonic genetic programme. The problem is that life or reproduction cannot be completed, leading to hypertrophy while death by apoptosis can occur leading to progressive myocytes loss and fibrosis Citation[3,4,5].
Thus, hypertrophy and apoptosis can be considered as “sons” of the same “mother”: the local tissue neuroendocrine‐neurohumoral response to a mechanical stretch of the myocytes (). The stretch is consequent to the geometric changes imposed on the viable myocytes by the necrotic ones by volume and pressure ovearload. Recognized stimuli for the switch are angiotensin II, norepinephrine and aldosterone although many other inducers are likely to play a role. This explains the anti‐remodelling effect of ACE‐inhibitors, β‐blockers and anti‐aldosterone substances. As expected, life and death cycle is very closely regulated by several autocrine systems one of which is linked to the interleukine‐6 family via a regulatory protein named GP‐130. Activation if the GP‐130 slows down the death signals, thus favouring hypertrophy and reducing fibrosis Citation[6,7,8]. Although hypertrophic myocytes cannot be considered normal, it has been suggested that when they are matching the myocyte loss, CHF is in a steady state. However, when apoptosis takes prevalence over hypertrophy, the disease progresses towards terminal stages. (). This “molecular‐genetic” view of the remodelling processes is interesting not only from the physiopathological point of view, but also from a therapeutical one, suggesting that antiapoptotic and pro‐life agents could be considered in the near future as novel treatment for CHF.
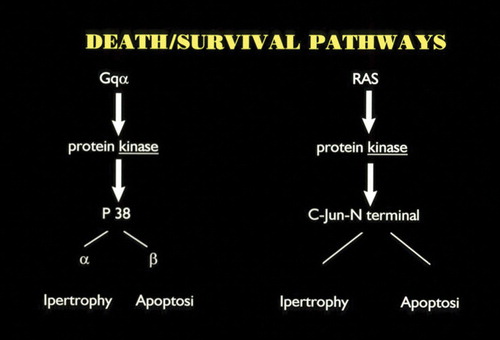
Biomaterials to repair the infarcted heart
Jonathan Leor, MD.1, Natali Landa, BSc1, Liron Miller, MSc1, Micha S. Feinberg, MD1, Smadar Cohen, PhD2
1Neufeld Cardiac Research Institute, Sheba Medical Center, Tel‐Aviv University, Tel‐Hashomer, Israel;2Department of Biotechnology Engineering, Ben‐Gurion University of the Negev, Beer‐Sheva, Israel
Correspondence: Jonathan Leor, MD, Neufeld Cardiac Research Institute, Sheba Medical Center, Tel‐Hashomer 52621, Israel; Tel: 972‐3‐534 2278, 972‐3‐635 1672, Fax: 972‐3‐535 1139, E‐mail: [email protected]
Heart failure after myocardial infarction (MI) is often precipitated by early and progressive extracellular matrix (ECM) degradation and pathological remodeling of the left ventricle (LV).Citation[1] In response to MI, a series of molecular, cellular and physiological responses are triggered, which can lead to early infarct expansion, scar thinning, which may result in early ventricular rupture or aneurysm formation and the transition to heart failure.Citation[1] Late remodeling involves the left ventricle globally and is associated with time‐dependent dilatation, and the distortion of ventricular shape. The failure to normalize increased wall stresses results in progressive dilatation, recruitment of border zone myocardium into the scar, and deterioration in contractile function.Citation[1] Current anti‐remodeling therapies are clearly limited, as many ventricles continue to enlarge and mortality and morbidity remain significantly high Citation[1,2].
An emerging paradigm links adverse remodeling and progression of heart failure after myocardial infarction (MI) to excessive damage to the cardiac extracellular matrix (ECM).Citation[3] This paradigm has potential therapeutic implications as several recent reports have suggested that direct injection of biomaterials, such as alginate, fibrin, collagen, and self‐assembling peptide into the infarct, alone or together with cells, immediately or a few days after MI could replace the damaged ECM and prevent adverse LV remodeling and heart failure Citation[4]–CitationCitationCitationCitationCitationCitation[10].
Enlargement and spherical deformation of the left ventricle with a concomitant increase in wall stress are key elements in the pathogenesis of adverse remodeling after MI. Injectable biomaterials can reduce wall stress by increasing scar thickness and stabilizing chamber size Citation[4,5],Citation[7]–CitationCitation[9]. By thickening the scar, wall stress is reduced (Laplace law) and the degree of outward motion of the infarct that occurs during systole (paradoxical systolic bulging) is reduced. This is a significant effect since one of the most important predictors of mortality in patients with MI is the degree of LV systolic dilatationCitation[11]. Wall et al. Citation[8] recently presented computational models that suggest that the injection of passive materials alone may improve ejection fraction and reduce wall stress in the ventricle. Returning wall stress closer to its normal value might improve the stress‐induced changes to the electrical and mechanical properties of myocytes Citation[12].
Several recent reports show that biomaterials with or without cells can be directly injected into the infarcted heart of small animal and improve healing, remodeling and function. Such biomaterials include fibrin glue, Citation[13,14] collagen, Citation[9], self‐assembled nanopeptide, Citation[6] and alginate Citation[4],Citation[15,16]. The most likely mechanism is increased scar thickness, and reduced wall stress that lead to progressive adverse remodeling and heart failure. Injectable biomaterial can also create an instructive environment for myocardial repair, Citation[5],Citation[7] as well as a platform for controlled delivery of therapeutic genes and proteins Citation[15],Citation[17]–CitationCitation[19].
In recent years, we investigated the therapeutic potential of alginate biomaterial for myocardial tissue engineering Citation[20,21]. Alginate, a polysaccharide found in brown sea weed has been used extensively in the food, pharmaceutical and medical device industries. It is biocompatible, and in the form of cross‐linked hydrogel ‐ has similar structure to ECM Citation[20],Citation[22]. Transplantation of biografts from alginate scaffolds reduced remodeling and dysfunction in rat model of MI Citation[20]. Recently, we developed an aqueous solution of calcium cross‐linked alginate displaying relatively low viscosity at room temperature. The alginate biomaterial was developed to enable a simple and easy delivery of the biomaterial via a needle into the infarct. Once in contact with the infarct, the low viscosity calcium cross‐linked alginate solution undergoes a rapid phase transition into a solid hydrogel, resembling the myocardial ECM. This occurs as the local calcium ion concentration increases in the alginate solution, possibly due to elevated calcium ion levels in the infarct and/or due to water diffusion from the injected formulation out to the surrounding infarct. Both these processes can shift the equilibrium towards hydrogel formation.
Our preliminary findings shows that injection of in‐situ forming alginate hydrogel into recent and old infarct increases scar thickness and attenuates adverse cardiac remodeling and systolic and diastolic dysfunction both in small and big animals Citation[23]–CitationCitationCitation[26]. A major advantage of the alginate solution, is that it is non‐thrombogenic and indeed, its feasibility to be injected into the systemic circulation has already been described, Citation[27] and confirmed by us in both small and large animals. Thus, after myocardial infarction and revascularization, this biomaterial solution can be injected safely into the infarct related coronary artery and delivered into the infarcted zone by selective intracoronary approach.
The bioabsorable alginate hydrogel implant is presumed to provide mechanical and physical support to the damaged cardiac tissue post MI, replacing some of the functions of the damaged ECM. Its presence during the LV remodeling period post‐MI provides physical scaffolding and stabilizes the infarct preventing it from dilatating and expanding. With time, the dissolvable hydrogel gradually disappears and the water‐soluble alginate chains are evacuated and excreted by the kidneys Citation[28].
Most encouraging was the finding that these beneficial effects of alginate implant were comparable to those achieved by fetal cardiomyocyte transplantation in recent infarct Citation[26]. This finding support previous evidence suggesting that cell therapies can increase wall thickness and prevent ventricular dilation and dysfunction by restoration of the ECM, independent of systolic activation of the implanted cells Citation[29,30].
To summarize, our preliminary experiments provide a novel proof of concept for an acellular approach of injectable, bioresorbable, alginate implant to preserve cardiac function after recent and old MI. The injectable implant increases scar thickness and provide physical support for improved healing and repair in order to attenuate early and late LV remodeling. The alginate solution is non‐thrombogenic and can be delivered into the infarct by a catheter‐based approach. The next clinical frontiers lie in the development of “smart” biomaterials that will not only provide physical support but will also guide the healing and self‐repair after infarct.
Disclosures. The research was supported by a grant from the Israel Science Foundation: No. 793/04, applied research grant from Ben‐Gurion University and BiolineRx.
JL and SC applied for a patent on injectable alginate for myocardial repair via Ben‐Gurion University.
Resident Cardiac Stem Cells and Their Role in Myocardial Regeneration and Repair
Ayelet Itzhaki, MSc, Jonathan Leor, MD, Israel M. Barbash, MD
Neufeld Cardiac Research Institute, Sheba Medical Center, Tel‐Aviv University, Israel
During fetal embryogenesis, the heart consists of rapidly proliferating cardiomyocytes. However, this growth pattern ceases in late fetal life, and is replaced by hypertrophic growth. Until recently, the heart was thus considered terminally differentiated without any significant regenerative potential. In 1994, Pierro Anversa and collaborators suggested, based on mitotic indices, that cardiomyocytes actually divide in certain pathologic conditions such as heart failure or myocardial infarction. Further support to the concept of the cardiac rejuvenation was achieved with the identification of several cell types within the myocardium that are capable of proliferation and differentiation, named cardiac stem or progenitor cells. Several surface markers have been suggested to identify these cells.
The first and the most common is the C‐kit (CD117) which is the receptor for stem cell factor. C‐kit+ cells have an immature phenotype and contribute to the regeneration of infarcted myocardium.Citation[1] When injected into an ischemic heart, lin− c‐kit+ cells reconstitute the ischemic myocardium by forming new vessels and anatomic, biochemical, and functional properties of young cardiomyocytes. Our, as well as others experience Citation[1]–Citation[2] suggest that c‐kit+ cells may actually be resident cardiac precursor cells which have stem cell characteristics and have the capability to differentiate into multiple lineages. Another suggested marker for resident cardiac stem cell was identified on a subset of endogenous muscle precursor cells distinguished by their expression of the islet‐1 (isl1) gene. The transcription factor isl1 marks a cell population that contributes especially to the right sided structures of the embryonic heart and outflow tract, and clusters of isl1+ cardioblasts were observed in rats, as well as in heart tissue taken from five human newborns.Citation[3]Sca1 is a marker for murine stem cells, it is not found on human cells, thus, it has no practical role in studying human tissues. Sca1+ cells were shown to have increased levels of telomerase reverse transcriptase activity and to have the capability to home into the myocardium and differentiate with and without fusion into cardiomyocytes following azacytidine treatment.
Finally, in the bone marrow, a special stem cell population was defined as “side‐population” cells. These cells can actively pump out several vital dyes (e.g. Hoechst dye) by the multidrug resistance protein (mdr, or p‐glycoprotein). This property of expelling the Hoechst dye gives characteristic appearance after fluorescent‐activated cell sorting, hence the name ‘side population’. By this method bone‐marrow‐ and muscle‐derived multipotent stem cells were isolated. Based on the same approach, a subpopulation of cardiac derived cells was defined as cardiac side population cells.
A major issue in the cardiac stem cells research is the “stem cells niche” or the identification of the exact location were the cardiac stem cells are the most abundant. We and others have identified that the right side of the heart and especially the right atrium possess the largest amount of cardiac progenitor cells and these cells differentiate more efficiently into multiple lineages.Citation[2]
Although the revolutionary concept of resident cardiac stem cells shows a great progress in the last 5 years, there are still large areas of uncertainty in this area of research. In the upcoming talk, the controversial and established ideas will be discussed.
Cell Therapy for Cardiovascular Diseases
Shmuel Fuchs, MD, Itsik Ben‐Dor, MD, Alexander Battler, MD
Cardiology Department, Rabin Medical Center, Petach‐Tikva, and the Sackler School of Medicine, Tel‐Aviv University, Tel‐Aviv, Israel
Cell therapy is an emerging investigational therapeutic strategy aims to improve symptoms and quality of life in patients with ischemic cardiovascular diseases. The rational for this approach is the limited ability of the human heart to significantly repair myocardial damage, ensuing in chronic ischemia and heart failure states. Three sources of autologous stem cells have been clinically evaluated: bone marrow (BM) derived cells (mononuclear cells, CD133+ enriched cells and mesenchymal stem cells), circulating progenitor cells and skeletal myoblasts (SM) Citation[1]–CitationCitationCitationCitationCitation[6]. The safety and subsequently potential efficacy of administration of those cells were examined in three different patient populations: 1) patients with refractory stable angina due to severe chronic ischemia, Citation[4,5] 2) patients with reduced left ventricular function and documented myocardial scar, Citation[6] and 3) patients who underwent successful primary percutaneous intervention for ST elevation myocardial infarction Citation[1]–CitationCitation[3]. Routs of cell administration included intramyocardial and intracoronary injections. Percutaneous, catheter‐based transendocardial injection was uniformly used in patients with refractory angina, Citation[4,5] while direct transepicardial injection, either as a standalone or as adjunct to coronary artery bypass grafting (CABG) surgery, was used in patients with LV dysfunction and myocardial scar.Citation[6] In the largest studied patient population – post STEMI cohort, intracoronary injection was consistently used as mode of delivery Citation[1]–CitationCitation[3]. The concept of bone marrow cell mobilization rather than direct cell injection was also evaluated in patients who sustained STEMI Citation[7].
As of today, clinical experience is based on multiple small phase I and II studies. The high safety profile of hematopoietic cell administration (BM‐derived and circulating progenitor cells) seen in animal studies was reproduced in those trials.
Importantly, the incidence of death, MI, stroke, arrhythmia and worsening of heart failure was similar among treated patients and controls. Although restenosis rate was reported to be higher in one controlled study, the overall data suggest no increase in restenosis rate and/or acceleration of atherosclerosis Citation[8]. In addition, unwarranted myocardial tissue response, such as myocarditis, calcifications, bone formation and tumor growth was not reported and few postmortem studies confirmed those clinical assessments. The main reported adverse event following SM administration was ventricular arrhythmias. In the first series of 10 patients with ischemic cardiomyopathy and documented scar tissue who underwent SM injections as adjunct to CABG, implantable cardioverter‐defibrillator was used in 5 patients due to ventricular arrhythmias. In a similar study but using different cell preparation technique, non‐sustained VT was documented in 3 out of 24 patients. Interestingly, no significant arrhythmias were observed among 10 patients who underwent catheter‐based injection of SM Citation[6].
Efficacy endpoints were evaluated in multiple small randomized and non‐randomized studies. Primary endpoints in patient with refractory angina were ischemic related, including CCS class, exercise test and nuclear imaging. In patients who underwent BM‐derived cells injection following successful primary PCI, change in LV function was the primary endpoints. Similar endpoint was also used in SM injection studies. In the latter, however, the magnitude of cell related therapeutic effect was difficult to asses due to concomitant surgical revascularization. A recent meta‐analysis of 18 BM‐derived cell injection randomized clinical trails (999 patients) suggest significant, albeit modest improvement in LV ejection fraction (3.7% absolute difference) and a reduction in infarct size of 5.4% compared to controls Citation[8]. It is important to recognize that those studies differ in multiple aspects including number and concentration of injected cells, timing of injection, number of progenitor cells and follow‐up duration.
The current clinical experience thus suggests intermediate‐term safety and modest potential efficacy. Several fundamental questions, however, still remain open requiring additional extensive bench work to further explore which of the BM‐derived cell(s) is the most potent to induce myocardial functional recovery and enhancement of perfusion and by what mechanism(s)? What are the cellular and molecular interactions between injected and myocardial cells and how those communications may affect myocardial tissue regeneration? What is the role of cardiac stem cells in myocardial regenerative process and can it be affected by local cell injection. Answers to those and other questions such as the potential role of ex‐vivo cell expansion and modifications along with identification of the most efficient cell number, concentration and route of delivery, will allow optimizing cell therapy and facilitate its incorporation into clinical practice.
Vasopressin Antagonism in Heart Failure
Tuvia Ben Gal, MD
Rabin Medical Center, Beilinson Campus, Petach Tikva, Israel
Evidence based therapy of chronic heart failure (HF) is based on neurohormonal inhibition of the renin‐angiotensin‐aldosterone system (with angiotensin‐converting enzyme inhibitors, angiotensin receptor blocking agents and aldosterone antagonists) and of the adrenergic nervous system (with beta‐adrenergic blocking agents). Although this therapy has been found successful in reducing morbidity and mortality in chronic HF patients, the outcome of these patients remains poor Citation[1]. The treatment of hospitalized patients with acute decompensated heart failure (ADHF) is even more frustrating with high readmission and mortality rates of approximately 20% each within 60 days. Besides frequent re‐admissions, ADHF patients commonly suffer from chronic and difficult to treat congestion, renal failure and hyponatremia Citation[2]. Symptom relief is rapidly achieved in ADHF patients with the use of loop diuretics. In the non‐hypotensive ADHF patients, retrospective data suggests better outcome with the use of vasodilators compared to inotropes. Amongst the vasodilators, nesiritide has been shown to be superior to nitroglycerin for symptom relief Citation[3] though its safety and effects on renal function are not clear yet. Inotropes are indicated in the hypotensive ADHF patients with no long term prognostic benefit. Some studies on the first calcium sensitizer "Levosimendan", showed conflicting results Citation[4] on its long term effect on survival but other small studies showed promising short term benefit.
A new potential therapy target in patients with HF is antagonism of the Arginine Vasopressin (AVP) system. Plasma AVP levels are unexplainably elevated in the presence of left ventricular dysfunction even in the absence of clinical HF. Plasma AVP levels are definitely a marker of poor prognosis. It may well be that excessive AVP secretion contributes directly to the syndrome of HF. Excessive AVP secretion increases blood volume by promoting free water retention and hyponatremia through the V2 AVP receptor located on renal cortical collecting ducts. AVP also leads to vasoconstriction and possibly cardiac hypertrophy through the cardiac V1a receptor resulting in elevation of the left ventricular wall stress. V1a activation also directly suppresses myocardial function. Plasma AVP levels do not predict the hemodynamic response to an effective AVP antagonist. In animal models, V1a antagonism produced hemodynamic improvement which is augmented when coupled with inhibition of the RAAS and blocking the adrenergic nervous system. V2 antagonism causes “aquaresis”: sustained diuresis. Several effective V2 antagonists (Lixivaptan and Tolvaptan) and Combined non‐selective V1a/V2 antagonists (Conivaptan) have been developed. Clinical studies using V2 antagonists in HF demonstrated quick and sustained increases in urine output and free water clearance, thus these agents may be considered as a new class of diuretics (“aquaretics”) differing from the traditional diuretics which are “saliuretics”. The use of V2 antagonists does not cause depletion of other electrolytes and in comparison with furosemide causes less stimulation of the RAAS and catecholamine system.
The most studied V2 antagonist is the oral, nonpeptide, selective vasopressin V2‐receptor antagonist, Tolvaptan. It was found to cause sustained aquaresis in patients with mild HF, some with hyponatremia. Body weight remained below baseline, and a small rise in serum sodium for the whole group was observed. The hyponatremic patients maintained an improvement in serum sodium. The only side effect reported was thirst. In the ACTIV in CHF study (Acute and Chronic Therapeutic Impact of a Vasopressin Antagonist in Congestive Heart Failure): a placebo‐controlled study in ADHF patient with ejection fraction <40%, the effect of oral Tolvaptan on in‐hospital body weight 24 h after drug administration and on worsening HF at 60 days was compared with placebo. The Tolvaptan group demonstrated significantly greater reduction in body weight during the first 24 h. This difference was maintained during follow‐up. Further body weight decrease was observed in the Tolvaptan group until discharge. Although the body weight declined while on Tolvaptan, there were no statistically significant differences in the signs and symptoms of clinical congestion. Disappointingly, at 60 days, there was no difference in worsening HF between the groups. Patients randomized to Tolvaptan used less furosemide and maintained a lower body weight. There were no differences in heart rate, blood pressure, or renal function between the groups. If serum sodium was low, it normalized and remained so throughout the study period. Although not powered for mortality, a post‐hoc analysis suggested a reduction in mortality in the higher‐risk patients (those with “severe” congestion and elevated blood urea nitrogen) Citation[5].
In the first of the EVEREST (Efficacy of Vasopressin Antagonism in Heart Failure: Outcome Study with Tolvaptan) Clinical Status Trials, there was no beneficial effect of 30 mg a day of oral Tolvaptan on ventricular remodeling when compared to placebo. Time to readmission or death was favorable for the Tolvaptan group but no reduction in clinical events was observed Citation[6]. In the first of two more recent studies from the EVEREST Clinical Status Trials published this year in the JAMA, the short‐term effect of Tolvaptan compared to placebo when added to standard therapy including diuretics in a cohort of approximately 4000 patients hospitalized with HF was evaluated. Tolvaptan was found to improve some HF symptoms. This statistically significant improvement was largely due to the greater change in body weight in the Tolvaptan group, as the global clinical score was not different at day 7 or discharge. Secondary end points of the short term study revealed modest improvements in dyspnea and edema. No serious adverse events like worsening renal function were recorded Citation[7]. The high safety profile is extremely important since no other therapeutic intervention in ADHF has been demonstrated in large‐scale randomized, placebo‐controlled studies to positively influence symptoms without generating some adverse events. In the second study, the overall long‐term effects of Tolvaptan in terms of safety and clinical outcomes in a cohort of 4133 patients with worsening HF requiring hospitalization was evaluated. Tolvaptan did not reduce mortality or HF‐related morbidity at 1 year. Hyponatremia, when present, was improved Citation[8]. The findings of those studies suggest some short‐term benefit for Tolvaptan on certain acute symptoms of ADHF with no evidence for harm.
Animal studies with the first combined V1a/V2 antagonist Conivaptan demonstrated V1a and V2‐blocking effects in the peripheral circulation and kidney. Conivaptan was able to block the recently described myocellular effects of V1a stimulation. A large single‐dose experience in patients with chronic stable HF showed that acute administration of Conivaptan produced a fall in cardiac filling pressures together with a water diuresis. There were no effects of the compound on blood pressure, cardiac output, or systemic vascular resistance. Current plans for convipatan are focused on treatment of ADHF and hyponatremia, but only for the acute use in view of significant cytochrome P450 interactions Citation[9,10].
The up to date data from the clinical trials on AVP antagonism in HF suggest that this may be a new therapeutic modality for the growing HF population however, evidence for long‐term benefit is lacking. The most appropriate patient expected to benefit from AVP antagonism has not been defined yet. More research is needed in order to better understand the role of AVP antagonism in HF before we add it to the armamentarium of the evidence based therapy of HF.
Levosimendan for the treatment of acutely decompensated heart failure: rationale and clinical experience
John T. Parissis, MD, FESC
Heart Failure Clinic, Attikon University Hospital, Athens, Greece
Corresponding author: Dr. John T. Parissis, Aftokratoros Irakliou 17, 15122 Maroussi, Athens, Greece; Tel: ++30‐210‐6123720, Fax: ++30‐210‐5832351, E‐mail: [email protected]
ABSTRACT. The calcium sensitizer levosimendan is a new cardiac enhancer with peripheral vasodilatory effects that seems to be more effective than classical inotropes such as dobutamine. It is improves cardiac contractility and central hemodynamics, and reduces congestion, without causing cardiomyocyte death and increased oxygen demand or interacting with the background treatment such as beta‐blockers. However, recent randomized trials REVIVE‐2 and SURVIVE showed that levosimendan is not superior to placebo or dobutamine in improving one‐ and six‐month mortality, although it caused a greater reduction of dyspnea and plasma BNP. More data are needed regarding the optimum regimen and dosing of levosimendan in the daily clinical practice as well as the identification of the ideal patient subpopulations responding to this treatment. Finally, pulsed infusions of the drug based on clinical criteria and plasma BNP may be a promising approach in order to prevent the worsening of cardiac function after each exacerbation of the syndrome.
Key words: acute heart failure, inotropes, calcium sensitizers, randomized trials.
Short‐term inotropic support of the failing heart is required for the attenuation of peripheral hypoperfusion and improvement of central hemodynamics in ADHF patients with acute decompersated heart failure (ADHF) Citation[1]. The ideal inotropic agent would improve systolic and diastolic cardiac function and reduce systemic and pulmonary vascular resistance. It should have a neutral or favorable effect on mortality without increasing myocardial oxygen consumption and worsening cardiac metabolic status. Classical inotropes, such as beta‐agonists and phosphodiesterase inhibitors, improve acutely the hemodynamic and clinical status of ADHF patients, but promote and accelerate adverse pathophysiologic mechanisms, increasing myocardial oxygen uptake, causing further myocardial injury through necrosis and apoptosis (especially in the presence of hibernating myocardium), and leading to increased short‐ and long‐term mortality Citation[1,2].
The new cardiac enhancer levosimendan meets most of the goals of treatment in ADHF, also promoting cardioprotection and beneficial lusitropic effects Citation[3]. The drug is a pyridazinone‐dinitrile derivative molecule that has positive inotropic properties by increasing the sensitivity of the cardiomyocyte contractile apparatus to intracellular calcium. Moreover, levosimendan is a powerful opener of ATP‐sensitive potassium channels causing peripheral arterial and venous dilatation. This biologic action is responsible for the drug‐induced reduction of peripheral vascular resistance and cardiac afterload. Thus, levosimendan can lead to significant increase of cardiac output through its combined positive inotropic and peripheral vasodilatory properties. Immunomodulatory and anti‐apoptotic properties of levosimendan may be an additional biologic mechanism that prevents further cytotoxic and hemodynamic consequences of abnormal immune and oxidative responses in ADHF, leads to cadioprotection and beneficially intervenes in the progression of the syndrome Citation[4]. Other advantages of levosimendan in the clinical use are: the preservation of its hemodynamic effects for a long period (for up to at least a week) after the initial infusion as well as the fact that the drug does not interact with the background treatment of ADHF such as beta‐blockers Citation[3]. No tolerance to the levosimendan effects or rebound worsening in hemodynamic variables after the drug withdrawal have been described in various clinical studies. Finally, headache and hypotension have been the most frequently reported adverse events in levosimendan‐treated patients in most placebo‐controlled studies Citation[3].
Intravenous levosimendan has been studied in more than 3000 patients and several medium‐ and large‐scale studies have been carried out. Mortality or mortality and morbidity combined have been prespecified end points in several of these studies. In the RUSSLAN study Citation[5] four doses of levosimendan (bolus doses of 6–24 µg/kg and continuous infusions of 0.1–0.4 µg/kg/min) or placebo were randomly given for 6 hours to 504 patients with decompensated heart failure after an acute myocardial infarct. The patients randomized to levosimendan were less likely to die than placebo patients during the 14‐day follow‐up after the study (11.7% versus 19.6%; p = 0.031) and this difference was maintained up to 6 months post treatment (22.6% versus 31.4%; p = 0.053). In the LIDO study Citation[6], mortality was followed prospectively for 31 days following randomization. At 31 days, 7.8% of patients assigned to levosimendan and 17.0% assigned to dobutamine had died (p = 0.049). The follow‐up was retrospectively extended to 180 days, by which time the mortality rates were 26.2% and 38.0% (p = 0.029) with levosimendan and dobutamine, respectively. The recent trials REVIVE‐1 and ‐2 and SURVIVE showed that levosimendan was superior to placebo or dobutamine, in producing clinical improvement and beneficial neurohormonal modulation (as expressed by the reduction of plasma BNP) in patients with ADHF. However, levosimendan failed to lead in a greater reduction of in‐hospital and six‐month mortality compared with placebo (REVIVE‐2: secondary end‐point) or dobutamine (SURVIVE: primary end‐point) in these patients. More specific, in the REVIVE‐2 study Citation[7], the 90‐day all‐cause mortality was 15.1% in the levosimendan group and 11.6% among controls (p = 0.210). The SURVIVE trial randomized 1327 patients with ADHF and a left ventricular ejection fraction of 30% or less, who required intravenous inotropic therapy because of insufficient response to intravenous diuretics and/or vasodilators. The patients received standard treatment with the random addition of a 12‐µg/kg bolus of levosimendan followed by a stepped dose regimen of 0.1‐0.2 µg/kg/min infusion for a maximum of 24 hours or dobutamine at a dose of at least 5 µg/kg/min for at least 24 hours. In the SURVIVE trial Citation[8] the primary end point ‐ all‐cause mortality at 6 months ‐ showed similar results with both levosimendan and dobutamine (26.2% and 27.9%, respectively; p = 0.401). Likewise, there were no differences between the treatment groups for the secondary end point of death at 1 month, with corresponding death rates of 12% and 14%, nor in a post‐hoc analysis of death at 5 days, occurring in 4% and 6% of levosimendan and dobutamine patients, respectively. However, evaluation of pre‐specified end‐points showed that the use of levosimendan caused greater reduction of in‐hospital mortality in patients on beta–blocker treatment at hospital admission as well as in patients with previous history of heat failure than dobutamine use.
Potential causes of non‐superiority of levosimendan versus placebo or dobutamine in reducing overall 6‐month mortality are: i) the heterogeneous study population including both ADHF and de novo acute heart failure patients, ii) the inclusion of patients in the REVIVE‐2 and SURVIVE studies was based only on clinical criteria and not on strict hemodynamic criteria with continuous invasive monitoring (LIDO), thus, increasing the risk of excessive preload reduction or vasodilation, iii) the high bolus dosing of levosimendan causing hypotensive episodes and fatal arrhythmias, and, finally, iii) the concomitant therapies consisting of other vasodilators, milrinone or neseritide, especially in REVIVE‐2 trial Citation[1].
More clinical data, deriving from specific sub‐analyses of the existing trials or new clinical trials, are needed in order to identify clinical criteria of treatment response as well as the optimal and safest dosing and regimen of levosimendan administration. According to the recently published European Society of Cardiology Guidelines on the diagnosis and treatment of acute heart failure Citation[9], levosimendan is indicated in the presence of peripheral hypoperfusion (hypotension, decreased renal function) with or without congestion or pulmonary oedema refractory to diuretics and vasodilators at optimal doses (Class IIa recommendation, level of evidence B). Finally, a promising approach in order to prevent new exacerbations of heart failure and inhibit progressive cardiac remodeling seems to be the pulsed 24‐hour infusions of levosimendan every 3 to 4 weeks based on clinical criteria and evaluation of plasma BNP levels in a outpatient clinical setting Citation[10]. However, these preliminary findings should be tested in large‐scale randomized clinical trials.
Notes
The authors have no financial association that might pose a conflict of interest in connection with the submitted article.