
Abstract
Purpose
The benefits of advanced hydraulic microprocessor controlled knee (MPK) joints have been well established and repeatedly confirmed. The Genium knee was introduced in 2011 containing an enhanced control concept including additional sensors and improved algorithms enabling a range of new functions for transfemoral amputees (TFAs). A systematic review was conducted to evaluate the effect of the Genium knee on ambulation, mobility, activities of daily living (ADLs) and quality of life compared to standard MPKs.
Materials and Methods
The review was conducted according to PRISMA Guidelines and Recommendations of the State-of-Science Evidence Report Guidelines of the American Academy of Orthotists & Prosthetists.
Results
Twelve articles were included in the review and reported primarily on active subjects (MFCL-3/4) transitioning from C-Leg to Genium knee systems. The overall validity of the evidence was medium to high with the exception of one article having low validity. Synthesis of biomechanical analyses concludes that gait during level walking, stairs and ramps is more physiological and symmetric following accommodation and use of the Genium in community ambulating TFAs. Further, sound side loading and compensatory motions are reduced. Transitioning from C-Leg to the Genium knee additionally resulted in significant improvements in mobility, quality of life and the performance in activities of daily living (ADLs).
Conclusion
A high level of evidence was identified when assessing the ability of Genium to improve gait quality and safety and performance in ADLs. While individual studies report significant improvements in terms of quality of life and mobility, additional studies are needed to increase the evidence level.
Microprocessor controlled prosthetic knees (MPKs) are well-established devices to serve patients with transfemoral amputation. Studies conducted mostly with the C-Leg MPK show that such knees significantly increase patient safety, ambulation, mobility, performance in activities of daily living and quality of life.
Genium MPK includes advanced features which enable a range of new functions and functional benefits to patients. Transitioning from conventional MPKs (i.e., C-Leg) to Genium MPK resulted in more physiological gait, more equally distributed loading between the prosthetic and sound limbs, as well as reduced compensatory movements on the sounds side. These outcomes could potentially reduce the long-term risks of secondary physical complications in prosthetic users (i.e., osteoarthritis, osteoporosis). Genium significantly improved mobility, performance in activities of daily living, and quality of life in the patients using a conventional MPK (C-Leg).
Different functioning principles of the MPKs presently available are responsible for different performance levels the knees offer to users. The amount of clinical evidence is also knee-dependent, with the C-Leg knee being most extensively tested in clinical studies. This systematic review concludes that Genium offers further advantages to transfemoral patients as compared to conventional MPKs (C-Leg).
Implications for rehabilitation
Introduction
A person living with transfemoral amputation (TFA) faces distinct challenges, such as increased ambulatory energy requirements, balance problems, and limitations in the ability to perform activities of daily living (ADLs) [Citation1–3]. Adequate selection of prosthetic components, especially the knee, is of high importance to ensure optimal rehabilitation outcomes. In addition to restoring physiological biomechanics, the knee must provide maximum safety and stability. Microprocessor controlled prosthetic knees (MPKs) are well-established devices to serve patients with TFA. Different functioning principles of the MPKs presently available (i.e., hydraulic units, magnetorheologic fluid) are responsible for different performance levels these knees offer to users [Citation4–8]. The C-Leg (Otto Bock Healthcare, Duderstadt, Germany) is a hydraulic MPK and the most researched prosthetic device in clinical studies to date with 55 publications reporting safety and performance outcomes compared to non-microprocessor controlled knees (NMPK) [Citation9–27]. In contrast to most other MPKs, the C-Leg utilizes a default stance setting, which means that it always offers high stance flexion resistance to support the body weight unless its stance control is disengaged, reflecting its highest priority to provide safety [Citation5].
Perhaps the most clinically relevant benefit of MPKs (C-Leg) is increased safety. Published literature suggests that falling is a major challenge for TFAs with recurrent falls and fear of falling leading to long-term functional deterioration, activity avoidance, decreased mobility and independence [Citation28,Citation29]. Research on MPKs, in particular on C-Leg, suggests that it reduces the number of falls, stumbles and fear of falling by up to 85%, 59% and 65.5%, respectively [Citation9–14]. Significant improvements have also been reported for validated clinical instruments such as the Berg Balance Scale or the Timed up and Go test [Citation10,Citation15,Citation16]. The effect of MPKs (i.e., C-Leg) on ambulation has been extensively studied by means of biomechanical analysis and assessments during level walking and various obstacle parcours have reported an increase in walking velocity [Citation11,Citation12,Citation17–21]. Improved gait symmetry and gait pattern harmonization have also been reported as well as more physiological swing phase control during varying speeds [Citation14,Citation18,Citation22]. Transitioning from a NMPK to the MPK resulted in faster and more symmetrical gait during ramp ascent and descent [Citation9,Citation12,Citation14,Citation23] but also improved overall stair mobility with the knee enabling increased loading on the prosthetic side during step-over-step descent [Citation11,Citation12,Citation24]. Significant improvements in mobility have been shown in both limited (MFCL-2) and unlimited (MFCL-3) community ambulators [Citation11,Citation12]. The cumulative effect of the aforementioned benefits of MPKs contribute to improved performance in ADLs and better quality of life [Citation11,Citation12,Citation25,Citation26].
A new MPK, Genium (Otto Bock Healthcare Duderstadt, Germany), was introduced in 2011 and is also, similar to the C-Leg, a hydraulic default stance MPK. Advanced features (i.e., new sensors and algorithms) enable the knee to offer a range of new functions and functional benefits to patients [Citation30]. A new core function of the knee is called “Optimized Physiological Gait.” This contains several novel features supporting more physiological gait such as four degrees of pre-flexion at initial contact which purportedly promotes increased stance flexion and shock absorption, reciprocal ramp and stair descent. Additionally, adaptive yielding control assists with stance flexion and extension, dynamic stability control ensures appropriate timing of swing release in different directions, while swing phase uses adaptive control to provide speed-independent knee flexion for proper toe clearance. Furthermore, there is a new function to support ascending stairs and crossing over obstacles, a walk to run function, a stance function that blocks knee flexion when the user is standing still, second modes that could be used for programing of other activities (MyModes), and saltwater-resistance which is included in the Genium X3 version. The knee also features a novel, user-friendly software (X-Soft) which guides prosthetists through the alignment, adjustment and coordination of the entire system in a step by step manner. The Computer Assisted Alignment feature provides a wireless read-out of the Genium’s sensors in real-time and provides a graphical representation of force application points and force vectors to facilitate correct alignment [Citation30,Citation31].
It is currently unclear if the novel features of the Genium MPK system translate into improved clinical function of the patient. Therefore, the objective of this systematic review was to analyze the available evidence on the effects of the Genium knee on ambulation, mobility, ADL performance and quality of life in patients with TFA. In particular, it was of interest to assess potential additional benefits it may provide compared to currently available conventional MPK.
Materials and methods
The systematic review was conducted according to the PRISMA Guidelines and following the recommendations of the State-of-Science Evidence Report Guidelines of the American Academy of Orthotists & Prosthetists [Citation32,Citation33].
The databases PubMed, Cinahl and Cochrane Database of Systematic Reviews were electronically searched for eligible studies on January 18th, 2017. Search terms used were: (Genium) OR (knee AND microprocessor AND control*) OR X2 knee. Term “X2 knee” was used in the search because it refers to the product name used during the final stages of Genium development. It is equivalent in terms of safety and performance to the current Genium knee which was subsequently introduced to the market. The results were limited to journal articles and publications since 2012. Pertinence assessment was performed by screening the titles and abstracts in a first step and reading the full-text article in a second step if pertinence was unclear for inclusion criteria by one reviewer (L. R.). In case of uncertainty, a second reviewer was consulted (M. P. M.). Publications were eligible if they were published in the English language and included subjects with transfemoral amputation or knee disarticulation. Included were studies that compared ambulation, mobility, ADLs and quality of life with the Genium or X2 prosthetic knee to any other non-microprocessor controlled knee (NMPK) or MPK. Single-case studies were excluded. Additionally, the references of identified articles were screened for additional relevant literature.
A data extraction sheet was developed. Refinements were made according to the applicability of the form. Data extracted from each included study were the following: (1) characteristics of study participants (amputation level, aetiology of the amputation, mean age, mean time since amputation, activity level); (2) study design (intervention, randomization, duration of treatment, accommodation period); and (3) outcome (type of outcome measure, results). The risk of bias was evaluated by three reviewers (M. P. M., L. R., and M. J. H.) independently by applying the State-of-Science Evidence Report Guidelines of the American Academy of Orthotists & Prosthetists [Citation33]. The study design was classified according to the Study Design Classification Scale [Citation33] (). The risk of bias (and therefore the quality) of the included studies was assessed in terms of 18 potential threats to internal and 8 potential threats to external validity. Items were classified as not applicable to the design of prosthetic studies in some cases. Publications were classified as having “high” validity if they met >80% of criteria, “moderate” if they met 60–80% of criteria, and “low” if they met <60% of the criteria [Citation45]. Internal and external validity was rated separately while the lower of the two was used in defining overall validity. The results of the reviewers were compared and discussed in case of disagreement to reach a consensus. In cases where consensus was not reached, the lead evidence report author (M. P. M.) reached the final decision.
Table 1. Body of evidence.
The included publications were used to develop the evidence statements (ESs) [Citation33]. They were grouped into four outcome topics (ambulation, mobility, activities of daily living and quality of life), summarizing the statistically significant findings. The ESs were developed if one or more publications reported results pertaining to a single outcome group. The ESs were then evaluated by examining: the number of publications contributing to the ES, the overall methodological quality of contributing studies and whether the findings were consistent or conflicting. A level of evidence for the individual ESs was defined as “high,” “moderate,” “low” or “insufficient.” “High” evidence level was assigned to the ES when multiple peer-reviewed publications of moderate to high overall methodological quality reported consistent results in support of the statement. A “moderate” evidence level was assigned when multiple peer-reviewed publications of low to moderate overall methodological quality reported consistent results. A “low” evidence level was assigned when there was a single peer-reviewed publication of moderate to high overall methodological quality, or multiple peer-reviewed studies of low methodological quality or if substantial findings among studies were inconsistent or conflicting. Finally, “inconsistent” was used to describe insufficient evidence to support the statement due to multiple studies with conflicting results.
Results
Study selection, characteristics and risk of bias
The database search identified 57 articles (). Additionally, two articles were identified through reference searching. The titles and abstracts of 51 articles were screened, 34 of which were excluded for obvious non-pertinence. Seventeen full-text articles were assessed for pertinence. After the elimination of duplicates and non-eligible articles, 12 publications remained for detailed analysis in this review ().
Figure 1. Flowchart of literature search and analysis.
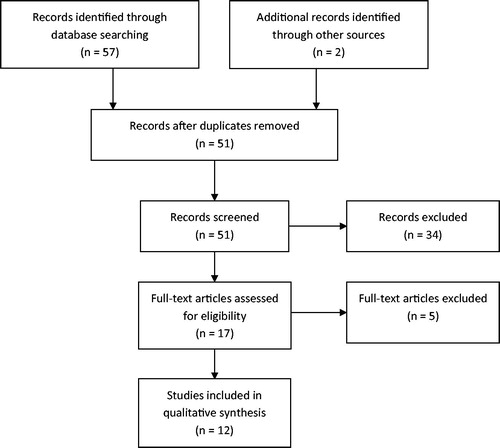
Table 2. Study characteristics.
Six publications utilized randomized controlled cross-over design [Citation30,Citation35,Citation36,Citation38,Citation40,Citation41], five publications before-and-after design [Citation37,Citation39,Citation42–44] and one study used a cross-sectional design [Citation34]. In many of the publications, the sample sizes were between 10 and 25, with the exception of one cross-sectional study that reported data of 899 subjects. Follow-up duration ranged across the publications from 2 days to 3 months. All the studies except for one reported on subjects with the mobility grades MFCL-3 and MFCL-4 as defined by the Medicare Function Classification Level. All subjects were long-term prosthetic users and trauma was the most common aetiology of the amputation. All but two included studies described subjects previously fitted with C-Leg transitioning to Genium.
Bias risk was assessed by evaluating internal and external validity (). In terms of internal validity, the number of studies scoring high, moderate and low was 5, 6 and 1, respectively. None of the studies used blinding (Internal validity (IV) criteria 6) which represents a threat. Additional common threats to the internal validity observed in included studies were: lack of the protocol addressing fatigue and learning (IV 9), no effect size reported (IV 15), attrition not explained and more than 20% (IV 11), attrition not equal between groups (IV 12) and not free of conflict of interest (IV 18). External validity was ranked as high for all the included studies. Finally, when considering both internal and external validity, there were five studies of high, six of moderate and one of low overall validity.
Ambulation
Nine articles focused on ambulation, in particular on level walking, stairs and ramps () [Citation34–39,Citation41,Citation43,Citation44].
Table 3. Summary of evidence.
Level walking
Four publications of moderate to high overall validity that investigated the effect of Genium on level walking focused on biomechanical analyses but also stability and exhaustion commonly used to asses prosthetic components [Citation34,Citation38,Citation41,Citation43]. Walking speed and perceived exertion were not significantly different between Genium and C-Leg, however numerous parameters suggest more physiological and safer gait. Peak knee flexion angle in swing and stance phase was significantly increased (p < 0.05) with Genium and closer to values of able-bodied subjects, especially during slow and medium speeds and under additional weight simulating heavier footwear [Citation38,Citation43]. Speed dependency of maximum knee flexion angle in swing phase that is an important determinant of toe clearance was further decreased with Genium, while the peak knee flexion during swing in small steps significantly increased [Citation43]. Due to four degrees of pre-flexion at initial contact, lower vertical and horizontal ground reaction forces were seen at weight acceptance on the prosthetic side. Increased knee flexion moments on the prosthetic side indicating increased weight-bearing were observed across different velocities but were significant only for fast speed. Asymmetry of step length at different velocities significantly decreased [Citation43]. While postural stability control was not different between the knees, in terms of limits of stability there were some differences with C-Leg significantly improving directional stability (p ≤ 0.05) anterolaterally over the prosthesis, whereas Genium use resulted in greater (p ≤ 0.05) posterolateral directional stability over the sound side [Citation41].
Walking on Ramps
Five publications reported on ramp walking outcomes [Citation34,Citation36–38,Citation43]. Walking speed with Genium was evaluated in two studies which reported either no change or improvement with Genium [Citation36,Citation37]. Peak knee flexion in swing phase was significantly increased with Genium during both ramp ascent and descent at various speeds and inclinations indicating increased toe clearance [Citation37,Citation38,Citation43]. During ramp descent, Genium use resulted in significantly more flexion at initial contact and higher peak knee flexion, while peak knee flexion during ascent was not significantly different from C-Leg [Citation37,Citation38]. Increased loading on the prosthetic side representing increased weight-bearing during descent was found by a significant increase in sagittal external knee flexion moments, which resulted in a trend of decreased contralateral vertical ground reaction forces and, thus, unloading of the sound side, at weight acceptance [Citation43]. Additional gait harmonization was also reported in terms of reduction of knee moment asymmetry, reduction of variance in peak knee flexion moments, increased prosthetic limb step length, increased prosthetic limb impact peaks and peak symmetry [Citation36,Citation37]. The ability of the knee to support standing on ramps was also assessed [Citation43]. Average loading and, thus, weight-bearing, during 3 min of standing on a 10 degree ramp was significantly increased with Genium (prosthetic side), while hip moments on the prosthetic side were significantly reduced, representing a reduction in hip compensation, as was postural sway.
Walking on stairs
Five publications assessed the performance of subjects with Genium on stairs [Citation34,Citation35,Citation39,Citation43,Citation44]. Studies suggest that between 64% and 80% of subjects were able to ascend stars by using a step-over-step method when using the Genium knee [Citation34,Citation39,Citation44]. While being more physiological, the duration to ascend stairs significantly increased during step-over-step pattern in comparison to the common step-to pattern of TFA [Citation35,Citation44]. The ability to utilize the step-over-step ascent method resulted in the more physiological increase in knee and hip range of motion on the prosthetic side and decrease of compensations on the sound side [Citation39,Citation43,Citation44]. Increased ankle movement on the contralateral side was also reported and comparable to able-bodied subjects (p < 0.01) [Citation44]. During the step-over-step method, loading of the contralateral knee (p < 0.05) and hip (p = 0.33) was reduced [Citation43]. While the maximum residual limb extension power on the prosthetic side with Genium was increased and comparable to able-bodied subjects (p = 0.63), a reduction was measured for contralateral knee extension power (p = 0.13) [Citation43,Citation44]. Finally, ankle joint power on the contralateral side was increased with the step-over-step method [Citation44]. Stair assessment index (SAI) was used in two studies reporting significant qualitative improvements during stair ascent represented by an average score increase from 5 or 6, respectively, with the C-Leg (5: “without rail or assistive device, step-to”; 6: “with rail or assistive device, skipping step pattern”) to 11 with Genium (“with rail, step-over-step pattern”) [Citation35,Citation39]. A significant improvement was also reported for the SAI descent score, but much smaller in magnitude [Citation35]. Duration to descend stairs was unchanged when transitioning from C-Leg to Genium [Citation35]. Finally, while sagittal external knee flexion moments on the prosthetic side at midstance were significantly increased with Genium, vertical ground reaction forces on the contralateral side were not affected [Citation43].
The ES was defined as “Genium results in more physiological gait, unloading and reduced compensatory mechanisms of the sound side compared to conventional MPKs.” Due to nine publications of high to moderate quality and consistent findings, a “high” evidence level was assigned to the statement.
Mobility
One article of high overall validity addressed the effect of Genium on subjects’ mobility () [Citation35]. Four square step test completion times were significantly reduced (small effect size). Furthermore, transitioning from C-Leg to Genium resulted in the significant increase in the Amputee Mobility Predictor (AMP) by 2 points. Highsmith et al. used StepWatch (Orthocare Innovations. Edmonds, Washington) devices to record step activity derived functional levels [Citation35]. Following two weeks of recording of step activity, the data was uploaded into the Galileo cloud whose software generated the activity report and functional level (MFCL or “K”-level). The functional level calculation was based on multiple factors, including cadence variability, potential to ambulate, ambulation requirement and the clinician’s observation of functional level. The calculated average functional level was significantly improved from 3.4 with C-Leg to 3.6 with Genium.
The following ES was developed: “Genium improves mobility of unilateral TF amputees when compared to conventional MPKs.” Due to the existence of only one high quality publication, the evidence level “low” was assigned to the ES.
Activities of daily living
Effect of Genium use on ADL performance was reported in four publications having an overall validity ranging from low to high () [Citation30,Citation34,Citation35,Citation42]. Scores on a validated instrument, short form Continuous Scale – Physical Functional Performance (CS-PFP10), was significantly improved when transitioning from C-Leg to Genium. Significant improvements were shown in three domains (Upper-body flexibility, Balance and Endurance) and positive trends in two domains (Upper-body strength and Lower-body strength). Able-bodied controls demonstrated significantly better CS-PFP10 scores in only one domain (Endurance) as compared to TFA using Genium but in four domains (Endurance, Lower-body strength, Upper-body strength, Balance and coordination) as compared to the same TFA using C-Leg. In two other studies, a non-validated questionnaire was used to evaluate the patient-perceived safety and difficulty of 45 ADLs with Genium as compared to C-Leg [Citation35,Citation42]. Both publications report significant improvements in perceived safety and difficulty, especially in activities dealing with Family and Social Role and Mobility and Transportation. Kannenberg et al. reported clinically relevant gain in safety for 27 out of 45 of ADLs (60%) and greater ease of performing 24 out of 45 ADLs (53%) [Citation42]. Finally, prosthetists appraised that over 70% of tested Genium users showed ‘clear’ or ‘very clear’ improvement in the ability to perform advanced manoeuvres (i.e., door test, carrying objects, obstacle and uneven terrain, toileting) [Citation34]. Similar feedback was obtained from the patients themselves, who reported benefits in performing activities such as carrying heavy loads, navigating in busy crowds, pushing a trolley or heavy door in 80–90% of cases.
The following ES was developed: “Genium use improves performance in and safety of conducting ADLs compared to conventional MPKs.” Due to three high or moderate quality publications with consistent findings, it was decided that a single low-validity publication should not be allowed to dilute the overall evidence level. Therefore, a high evidence level was assigned to the statement.
Quality of life
Quality of life was addressed in one article having moderate validity () [Citation40]. Significant improvements in Prosthetic Evaluation Questionnaire (PEQ) domain scores were reported after 3 months when transitioning from C-Leg to Genium. Four scales were significantly improved: Perceived Response, Social Burden, Utility, and Well-Being (all p < 0.05), while positive trends were observed in two scales (Appearance and Sounds). No difference was found in the scales of Ambulation, Frustration and Residual Limb Health. Seven out of ten PEQ items related to physical performance were significantly improved with the Genium (comfort while standing, walking in tight spaces, walking down stairs, walking steep hills, walking slippery surfaces, satisfaction with walking; p < 0.025). An ES was developed stating “Genium further improves prosthesis-related quality of life of unilateral TF amputees as compared to conventional MPKs.” Due to the availability of only one moderate-quality publication, the evidence level “low” was assigned to the ES.
Discussion
Summary of the evidence
Twelve publications reporting on TFAs (MFCL-3 and 4) predominantly transitioning from C-Leg to Genium were included in the systematic review. The overall quality of the evidence was moderate to high with the exception of one article having low methodological quality. The studies were selected and their results evaluated to assess the effects of Genium on ambulation, mobility, ADL performance and quality of life in above-knee amputees as compared to conventional MPK and NMPK.
The effect of Genium on ambulation was assessed for level walking, ramps and stairs. While there was no significant influence on the speed of conducting those activities, biomechanical findings suggest that gait kinetics and kinematics as well as several spatiotemporal parameters were more physiological with Genium than with conventional MPKs. The evidence supports more physiological knee flexion in both stance and swing phase, representing increased weight-bearing and improved toe clearance, reduction of speed-dependency of maximum knee flexion angle in swing phase, representing more consistent speed-independent toe clearance, improved symmetry of step length, as well as increased toe clearance especially during small steps and simulating heavier footwear during level walking. The new stair function enabling up to 80% of subjects to perform step-over-step stair ascent resulted in more physiological movement patterns on the prosthetic side but also significant reductions in compensatory movements on the sound side. While weight acceptance on the prosthetic side was more comfortable as shown by reduced ground reaction forces, the flexion moments on the hip and knee suggest greater prosthetic side loading, i.e., weight-bearing. This finding was statistically significant for fast walking. Gait analyses on ramps showed increased maximum knee flexion angle and, thus, foot clearance similar to those measured on the sound side. The new standing function resulted in significantly more loading and, thus, weight-bearing, on the prosthetic side during standing on ramps.
The reported improvements in kinetic gait parameters as well as loading symmetry, representing a more even distribution of the body weight with Genium may be clinically relevant. Published evidence on the amputee population suggests that asymmetry, especially in loading is related to long-term consequences to the locomotor system resulting in secondary physical complications among lower limb prosthetic users, such as knee osteoarthritis [Citation46,Citation47]. A recent systematic review examining the risk of degenerative changes in lower limb amputees concluded that 56% of amputees suffer from back pain, 35% of patients from osteoarthritis of the sound knee, and 15% and 20% from hip osteoarthritis on the prosthetic and sound side, respectively [Citation47]. Reduced bone density was observed in 87% of patients in their prosthetic side hip, and all amputees exhibited residual limb muscle atrophy. The prevalence of back pain and knee osteoarthritis was shown to increase in more proximal amputations. Similar conclusions were reached in a review by Gailey et al. [Citation46]. Asymmetry, especially in terms of loading, has been identified as a major cause for those observations. Long-term exposure to high repetitive loading forces leads to the degeneration of weight-bearing joints that can contribute to joint pain [Citation48,Citation49]. Burke et al. attributed gait asymmetry and increased load to the intact limb to the higher incidence of osteoarthritis in long-term prosthesis users [Citation50]. While optimized prosthetic fitting may reduce these risks, prosthetic components such as the Genium knee, may do so as well by facilitating a more physiologic gait as demonstrated by the aggregate results of the included studies [Citation36–39,Citation43,Citation44]. More symmetrical gait and more physiological, more evenly distributed loading of the sound and prosthetic sides could reduce the long-term risks of secondary physical complications in prosthetic wearers.
Validated clinical instruments, such as the AMP and MFCL-level derived from StepWatch, recordings were used to assess mobility with Genium. Significant improvements were observed. However, conclusions regarding clinical relevance cannot be drawn due to lack of established reference values for the lower limb amputee population. A validated instrument assessing ADL performance further suggested that Genium reduced the functional gap between able-bodied subjects and prosthetic users. It is interesting that significant improvements were observed in upper-body flexibility that researchers attributed to greater lower body stability and reduced necessary concentration on lower extremity function as the foundation for performing upper extremity activities. Significant improvements in both perceived endurance and balance measured by a non-validated ADL questionnaire were supported by the same performance-based validated instrument (CS-PFP10). Not a single item of 45 activities was rated easier or safer to perform by subjects when done with a conventional MPK. Many activities were improved with Genium both in terms of safety and ease of execution. Prosthesis-related quality of life as measured by the PEQ was significantly improved when transitioning from C-Leg to Genium, particularly in the subscales of Perceived Response, Social Burden, Utility and Well-Being. Finally, approximately 80% of previous C-Leg users preferred Genium after training with and using it for approximately 3 months.
The reviewed results were used to develop four ES. The statements related to the ability of Genium to improve gait quality, and that regarding safety of and performance in ADL execution were evaluated as having “high” evidence levels. The other two statements assessing the ability of Genium to affect quality of life and mobility were rated as “low evidence level” due to the availability of a single high or moderate quality study only. Therefore, additional studies are needed to further corroborate the evidence of these two statements.
It should also be noted that in most studies subjects were specifically trained in the use of the Genium features and assessed for accommodation prior to assessing outcomes. One study reported for example that, when using the Genium, subjects required 0.7 ± 1.0 additional visits (0–4) for post-fitting prosthetic adjustments. Subjects required additional 3.0 ± 1.8 visits (1–8) with the study physical therapist for functional training to master new features with the Genium knee, including stance locking (i.e., the so-called intuitive stance), reciprocal stair ascent, obstacle crossing, and stance flexion feature. Subjects required 67.9 ± 27.1 d (18–119 d) to successfully complete the accommodation test with the Genium knee [Citation30]. Results and outcomes reported in that studies are the result of the reported accommodation and training. Outcomes observed in the present review may not be generalizable in cases where training was not provided.
Limitations
Several systematic reviews conducted so far on various prosthetic components concluded that evidence in prosthetic research is of mostly low to moderate quality [Citation51,Citation52]. While very much true for older studies, it should be acknowledged that several attempts were made in recent years to improve the quality of studies in prosthetics. This trend is already apparent in the evidence reviewed in this systematic review with the oldest article published in 2012, resulting in most articles having moderate to high quality. Randomization (of the order of interventions) was implemented in several reviewed studies to reduce bias. On the other hand, the absence of blinding was still observed in all included studies. While subject blinding may be difficult in prosthetic research, blinding of assessors should be possible in future studies. The acclimation period when transitioning from MPKs (predominantly hydraulic knees) to Genium in most publications was three months or longer. This was considered sufficient as studies assessing transitioning from NMPKs to MPKs report similar duration of acclimation [Citation9,Citation53]. The acclimation period in a few studies was only two days. While this period is short, the conclusions reached in the studies were similar to those reached in studies having longer acclimation periods [Citation37,Citation38].
The sample size in most publications was between 10 and 25 subjects with the exception of a larger cross-sectional study, yet samples were sufficient to obtain several significant results. Internal validity of the reviewed studies could be further improved by including information addressing fatigue and learning, effect size calculation and reporting attrition rate as well as conflict of interest.
The order in which the effect of prosthetic knees was assessed varied across studies. In all the studies, subjects entering the study were using the C-Leg (or NMPK). Five publications that utilized a controlled before-and-after design assessed the patients with the C-Leg (or NMPK) prior to fitting and subsequent assessment with Genium [Citation37,Citation39,Citation42–44]. In six publications where a randomized order controlled design was used, the C-Leg accommodated patients were randomized to either the C-Leg or Genium and allowed to accommodate prior to their first assessment [Citation30,Citation35,Citation36,Citation38,Citation40,Citation41]. After the cross-over, they were fitted with the other device prior to re-assessment. Therefore, the order in which prostheses were assessed varied and, therefore, an order effect on the results was reduced.
Conclusions
Most of the reviewed evidence reports on active, community ambulating transfemoral amputees transitioning from C-Leg to Genium. The quality of the evidence is predominantly moderate and high showing improvements in outcomes when compared to conventional MPKs and NMPKs. Accommodation with and use of Genium resulted in more physiological gait during level walking, ramp and stair ambulation, as well as reduced loading and compensatory mechanisms of the sounds side. More symmetrical gait and more physiological, evenly distributed loading of sound and prosthetic sides could perhaps contribute to reducing the long-term risks of secondary physical complications in prosthetic users (i.e., osteoarthritis, osteoporosis). Mobility and functional levels were both significantly improved, while positive effects on performance in and safety of activities of daily living were demonstrated by both performance-based and patient-reported outcome measures. Significant improvements in quality of life, as measured by the PEQ, were also reported. At this time, it is unclear if results are generalizable beyond unilaterally involved, community ambulators with TFA.
Acknowledgements
M. P. Mileusnic, L. Rettinger and M. J. Highsmith were responsible for reviewing the bias risk and for drafting the manuscript. A. Hahn provided input during drafting of the manuscript and provided critical review.
Disclosure statement
M. J. Highsmith has no financial disclosures related to preparation and drafting of this manuscript. The other authors (M. P. Mileusnic, L. Rettinger and A. Hahn) are employees of Otto Bock Healthcare Products (Vienna, Austria), the manufacturer of the MPK subject to this review. The company did not influence the design and execution of the review nor the interpretation of results. However, Ottobock allowed the authors to work on this systematic review during their regular office hours and to use the company’s office equipment (computers, software, Internet access, database access).
References
- Davies B, Datta D. Mobility outcome following unilateral lower limb amputation. Prosthet Orthot Int. 2003;27:186–190.
- Robbins CB, Vreeman DJ, Sothmann MS, et al. A review of the long-term health outcomes associated with war-related amputation. Mil Med. 2009;174:588–592.
- Van Velzen JM, van Bennekom CA, Polomski W, et al. Physical capacity and walking ability after lower limb amputation: a systematic review. Clin Rehabil. 2006;20:999–1016.
- Thiele J, Westebbe B, Bellmann M, et al. Design and performance of microprocessor-controlled knee joints. Biomed Tech (Berl). 2014;59:65–77.
- Bellmann M, Schmalz T, Blumentritt S. Comparative biomechanical analysis of current microprocessor-controlled prosthetic knee joints. Arch Phys Med Rehabil. 2010;91:644–652.
- Hafner BJ, Askew RL. Physical performance and self-report outcomes associated with use of passive, adaptive, and active prosthetic knees in persons with unilateral, transfemoral amputation: randomized crossover trial. J Rehabil Res Dev. 2015;52:677–700.
- Prinsen EC, Nederhand MJ, Olsman J, et al. Influence of a user-adaptive prosthetic knee on quality of life, balance confidence, and measures of mobility: a randomized cross-over trial. Clin Rehabil. 2015;29:581–591.
- Prinsen EC, Nederhand MJ, Sveinsdottir HS, et al. The influence of a user-adaptive prosthetic knee across varying walking speeds: a randomized cross-over trial. Gait Posture. 2017;51:254–260.
- Hafner BJ, Willingham LL, Buell NC, et al. Evaluation of function, performance, and preference as transfemoral amputees transition from mechanical to microprocessor control of the prosthetic knee. Arch Phys Med Rehabil. 2007;88:207–217.
- Wong CK, Rheinstein J, Stern MA. Benefits for adults with trans-femoral amputations and peripheral artery disease using microprocessor compared with nonmicroprocessor prosthetic knees. Am J Phys Med Rehabil. 2015;94:804–810.
- Kahle JT, Highsmith MJ, Hubbard SL. Comparison of nonmicroprocessor knee mechanism versus C-Leg on Prosthesis Evaluation Questionnaire, stumbles, falls, walking tests, stair descent, and knee preference. J Rehabil Res Dev. 2008;45:1–14.
- Hafner BJ, Smith DG. Differences in function and safety between Medicare Functional Classification Level-2 and -3 transfemoral amputees and influ-ence of prosthetic knee joint control. J Rehabil Res Dev. 2009;46:417–433.
- Highsmith MJ, Kahle JT, Shepard NT, et al. The effect of the C-Leg Knee Prosthesis on sensory dependency and falls during sensory organization testing. Technol Innov. 2014;15:343–347.
- Hahn A, Lang M. Effects of mobility grade, age and etiology on functional benefit and safety of subjects evaluated in over 1200 C-Leg trial fittings in Germany. J Prosthet Orthot. 2015;27:86–94.
- Burnfield JM, Eberly VJ, Gronely JK, et al. Impact of stance phase microprocessor-controlled knee prosthesis on ramp negotiation and community walking function in K2 level transfemoral amputees. Prosthet Orthot Int. 2012;36:95–104.
- Wong CK, Wilska J, Stern M. Balance, balance confidence, and falls using nonmicroprocessor and microprocessor knee prostheses. J Prosthet Orthot. 2012;24:16–18.
- Orendurff MS, Segal AD, Klute GK, et al. Gait efficiency using the C-Leg. J Rehabil Res Dev. 2006;43:239–246.
- Segal AD, Orendurff MS, Klute GK, et al. Kinematic and kinetic comparisons of transfemoral amputee gait using C-Leg and Mauch SNS prosthetic knees. J Rehabil Res Dev. 2006;43:857–870.
- Mâaref K, André JM, Paysant J, et al. Kinematics in the terminal swing phase of unilateral transfemoral amputees: microprocessor-controlled versus swing-phase control prosthetic knees. Arch Phys Med Rehabil. 2010;91:919–925.
- Seymour R, Engbretson B, Kott K, et al. Comparison between the C-leg microprocessor-controlled prosthetic knee and non-microprocessor control prosthetic knees: a preliminary study of energy expenditure, obstacle course performance, and quality of life survey. Prosthet Orthot Int. 2007;31:51–61.
- Meier MR, Hansen AH, Gard SA, et al. Obstacle course: users' maneuverability and movement efficiency when using Otto Bock C-Leg, Otto Bock 3R60, and CaTech SNS prosthetic knee joints. J Rehabil Res Dev. 2012;49:583–596.
- Kaufman KR, Frittoli S, Frigo CA. Gait asymmetry of transfemoral amputees using mechanical and microprocessor-controlled prosthetic knees. Clin Biomech. 2012;27:460–465.
- Highsmith MJ, Kahle JT, Miro RM, et al. Ramp de-scent performance with the C-Leg and interrater reliability of the Hill Assessment Index. Prosthet Orthot Int. 2013;37:362–368.
- Schmalz T. Leistungsfähigkeit verschiedener Prothesenkniegelenke beim Treppabgehen von Oberschenkelamputierten. Orthopädie-Technik Quart. 2002;7:1–6.
- Cutti AG, Lettieri E, Del Maestro M, et al. Stratified cost-utility analysis of C-Leg versus mechanical knees: findings from an Italian sample of transfemoral amputees. Prosthet Orthot Int. 2017;41:227–236.
- Theeven P, Hemmen B, Geers R, et al. Influence of advanced prosthetic knee joints on perceived performance and everyday life activity level of low-functional persons with a trans-femoral amputation or knee disarticulation. J Rehabil Med. 2012;44:454–461.
- Otto Bock Clinical Research 2017. Retrieved from: https://www.ottobock.com/en/company/clinical-research/
- Miller WC, Speechley M, Deathe B. The prevalence and risk factors of falling and fear of falling among lower extremity amputees. Arch Phys Med Rehabil. 2001;82:1031–1037.
- Miller WC, Deathe AB, Speechley M, et al. The influence of falling, fear of falling, and balance confidence on prosthetic mobility and social activity among individuals with a lower extremity amputation. Arch Phys Med Rehabil. 2001;82:1238–1244.
- Highsmith MJ, Kahle JT, Miro RM, et al. Functional performance differences between the Genium and C-Leg prosthetic knees and intact knees. J Rehabil Res Dev. 2016;53:753–766.
- Otto B. Genium leg prosthesis. Retrieved July 2019. from https://www.ottobockus.com/prosthetics/lower-limb-prosthetics/solution-overview/genium-above-knee-system/
- Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097.
- Hafner B. State-of-the-Science Evidence Report Guidelines. Washington (DC): American Academy of Orthotists & Prosthetists; 2008.
- Hahn A, Lang M, Stuckart C. Analysis of clinically important factors on the performance of advanced hydraulic, microprocessor-controlled exo-prosthetic knee joints based on 899 trial fittings. Medicine (Baltimore). 2016;95:e5386.
- Highsmith MJ, Kahle JT, Wernke MM, et al. Effects of the Genium Knee System on functional level, stair ambulation, perceptive and economic outcomes in transfemoral amputees. Technol Innov. 2016;18:139–150.
- Highsmith MJ, Klenow TD, Kahle JT, et al. Effects of the Genium Microprocessor Knee System on knee moment symmetry during hill walking. Technol Innov. 2016;18:151–157.
- Bell EM, Pruziner AL, Wilken JM, et al. Performance of conventional and X2® prosthetic knees during slope descent. Clin Biomech (Bristol, Avon). 2016;33:26–31.
- Lura DJ, Wernke MM, Carey SL, et al. Differences in knee flexion between the Genium and C-Leg microprocessor knees while walking on level ground and ramps. Clin Biomech. 2015;30:175–181.
- Aldridge Whitehead JM, Wolf EJ, Scoville CR, et al. Does a microprocessor-controlled prosthetic knee affect stair ascent strategies in persons with transfemoral amputation? Clin Orthop Relat Res. 2014;472:3093–3101.
- Highsmith MJ, Kahle JT, Miro RM, et al. Perceived differences between the Genium and the C-Leg microprocessor prosthetic knees in prosthetic-related function and quality of life. Technol Innov. 2014;15:369–375.
- Highsmith MJ, Kahle JT, Lura DJ, et al. Short and mid-distance walking and posturography with a novel microprocessor knee. Technol Innov. 2014;15:359–368.
- Kannenberg A, Zacharias B, Mileusnic M, et al. Activities of daily living: Genium bionic prosthetic knee compared with C-Leg. J Prosthet Orthot. 2013;25:110–117.
- Bellmann M, Schmalz T, Ludwigs E, et al. Immediate effects of a new microprocessor-controlled prosthetic knee joint: a comparative biomechanical evaluation. Arch Phys Med Rehabil. 2012;93:541–549.
- Bellmann M, Schmalz T, Ludwigs E, et al. Stair ascent with an innovative microprocessor-controlled exoprosthetic knee joint. Biomed Tech. 2012;57:435–444.
- Highsmith MJ, Andrews CR, Millman C, et al. Gait training interventions for lower extremity amputees: a systematic literature review. Technol Innov. 2016;18:99–113.
- Gailey R, Allen K, Castles J, et al. Review of secondary physical conditions associated with lower-limb amputation and long-term prosthesis use. J Rehabil Res Dev. 2008;45:15–30.
- Pröbsting E, Blumentritt S, Kannenberg A. Changes in the locomotor system as a consequence of amputation of a lower limb. Z Orthop Unfall. 2017;155:77–91.
- Radin EL, Parker HG, Pugh JW, et al. Response of joints to impact loading. 3. Relationship between trabecular microfractures and cartilage degeneration. J Biomech. 1973;6:51–57.
- Hurwitz DE, Sumner DR, Block JA. Bone density, dynamic joint loading and joint degeneration. A review. Cells Tissues Organs. 2001;169:201–209.
- Burke MJ, Roman V, Wright V. Bone and joint changes in lower limb amputees. Ann Rheum Dis. 1978;37:252–254.
- Van der Linde H, Hofstad CJ, Guerts ACH, et al. A systematic literature review of the effect of different prosthetic components on human functioning with a lower-limb prosthesis. J Rehabil Res Dev. 2004;41:555–570.
- Carey SL, Lura DJ, Highsmith MJ. Differences in myoelectric and body-powered upper-limb prostheses: systematic literature review. J Rehabil Res Dev. 2015;52:247–262.
- Highsmith MJ. Microprocessor knees: considerations for accommodation and training. J Prosthet Orthot. 2013;25:60–64.