
Abstract
Background and aim
This study investigated the current state of wheelchair services in Bangalore Rural district, as provided by Bangalore Baptist Hospital, and identified areas for improvement.
Method
a cross-sectional survey was held among 50 wheelchair users. Data was collected on demographics, satisfaction, wheelchair skills and level of disability using QUEST, WST-Q and CHART-SF questionnaires.
Result
Overall satisfaction can be described as more or less satisfied, scoring 3.8 out of 5. Wheelchair users were less satisfied with the services compared to the wheelchair itself. The skills a wheelchair users had were strongly correlated with satisfaction scores (p < 0.01). Differences in satisfaction between genders were observed and related to multiple factors.
Conclusion
Wheelchairs should be easy to use with support services being easily accessible. A wheelchair should be delivered together with a training program to provide the user with the skills to operate and maintain the wheelchair. There are gender-wise differences in satisfaction towards wheelchair services that influence satisfaction.
Training of wheelchair skills should be part of the delivery process as this positively impacts satisfaction of wheelchair users and increases their independent mobility.
Requirements towards a wheelchair and its support service are gender specific. Recognizing and acting upon the differing needs between male and female wheelchair users should be an integral part of a wheelchair provision service.
Wheelchair users should take part in the development and implementation of novel technologies, policies and service delivery schemes as their need is not always answered. This could lead to a reduced uptake, or even failure, of innovations in (wheelchair) services.
The financial situation of a wheelchair user is a factor that influences satisfaction. Therefore, empowering and/or enabling wheelchair users to take part in activities that earns them an income should be part of a wheelchair service.
Implications for rehabilitation
Introduction
The World Health Organization (WHO) declared disability as global public health issue during the 66th World Health Assembly in 2013. Based on a report by the World Bank and WHO, disability was acknowledged to be a Global Health problem because “people with disability, throughout the life course, face widespread barriers in accessing health and related services, such as rehabilitation, and have worse health outcomes than people without disability” [Citation1]. That report also found that around one billion people are living with a disability, which comes down to roughly 15% of the world population [Citation2]. It is expected that the number of people living with disability will rise to 2 billion by the year 2050.
Assistive technologies are pieces of equipment or products that are used to maintain or improve the functional capabilities of people with disability [Citation2]. From the viewpoint of the medical model of disability, assistive technology might be seen as correcting the “shortcomings of an individual”, while from a social model perspective it is considered “an enabler that reduces barriers in a disabling environment” [Citation3]. There is an unmet need for assistive technologies. The WHO estimated that only 1 out of 10 people who need assistive technology have access to it [Citation4].
One example of assistive technology for which there is a large demand but low supply, is the wheelchair. Currently, there are 75 million people who need a wheelchair [Citation5]. For low and middle-income countries, the population of people that need a wheelchair and have access to it ranges somewhere between 2 and 5% [Citation6]. These statistics are in contrast to the benefits that a wheelchair provides its user with. It is known that wheelchairs increase the mobility of the users (they leave their homes more frequently), range of travel is increased and users can be employed and earn an income [Citation7]. Improved outcomes are also seen with regard to quality of life and the International Classification of Functioning, Disability and Health (ICF) domain [Citation7]. Besides this, wheelchairs have proven to positively impact societal inclusion, access to education and social services and contribution to family life [Citation8].
However, having a wheelchair does not automatically mean that it serves the individual needs. Actually, there are reasons why there is a gap between met and unmet needs [Citation9–12]. Multiple factors contribute to this, one of them being due to private donors aiming to providing large numbers of wheelchairs but not focussing on providing the recipient with support services [Citation13]. Another reason could be the fragmentation of wheelchair provision services, meaning that if a government does not have an organized structure in place there is a high chance for devices of poor quality being delivered, maintenance being left to the user and devices being discarded because they are not used [Citation14]. End user function and participation are not improved by simply providing a wheelchair to the individual in need of it, but also ongoing support services are needed [Citation13–15].
A framework () that has been conceptualized by Kamaraj et al. [Citation16] lays bare the complex interdependencies of different characteristics, both personal and service specific, that determine the effectiveness of the wheelchair provision services.
Figure 1. Conceptual framework for the evaluation of wheelchair services.
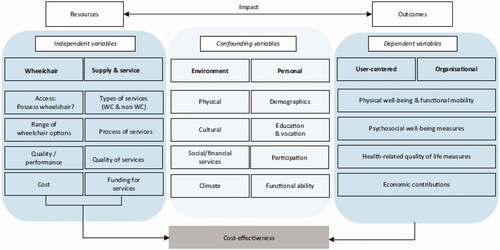
As the framework in makes clear, there is a relationship between dependent and independent variables. This relationship is confounded by environmental and personal factors. Independent variables focus more on the physical characteristics of the wheelchair and the services through which it is provided whereas the dependent variables represent the factors that influence the user’s everyday life. Confounding variables such as demographics, quality and source of wheelchair and level of wheelchair skills have a profound impact on the effectiveness of wheelchair provision.
The Indian context
The Convention on the Rights of Persons with Disabilities (CRPD) has two articles that emphasize the importance of governmental responsibility for delivering these support services [Citation2,Citation8]. Assistive technology, including wheelchairs, should be available through these services and include components that ensure daily functioning and user handling of the wheelchair [Citation12,Citation17]. The Indian government ratified the CRDP and passed a law that implements the core principles of the convention, called the Rights of Persons with Disabilities Act 2016 (RPDA). Under its predecessor, out of the year 1995, 16% of people with disabilities in India had acquired an assistive device. Out of this 16%, only 1 out of 5 got their assistive device through a government scheme [Citation18]. These numbers indicate the inadequate functioning of the social system, as people with disabilities were more likely to seek help and assistive devices from paid services rather than free government provided services [Citation19]. The RPDA of 2016 is expected to empower people with disabilities. Although the improvements of the RPDA are recognized [Citation20], its implementation is challenging due to delayed legislative processing, limited translations (2 our of 21 official languages in India), no initiation of special advisory boards and so on [Citation21].
Problem statement
It has been recognized that the available evidence on assistive technology, including wheelchairs, in resource-constraint environments is limited in quantity and not evenly distributed across the multiple different types of assistive technologies [Citation10]. Also the types of study designs that are used in order to create this literature seem to be relatively homogenous. The approach of research into disability and assistive technology so far has contributed to having a rather large pool of knowledge about outcomes in terms of ICF-domains, where the functions domain is over-represented and participation and activities domain are silenced [Citation22].
This study has multiple goals. It aims to evaluate the current state of wheelchair services in a specific region in India by investigating the usability of wheelchairs as perceived by the wheelchair user’s; the service provision and the links between factors that influence wheelchair usage. These objectives were formulated into a research question: what is the current state of wheelchair- and support services, and what outcomes are there after receiving a manual wheelchair as perceived by persons with disabilities in Bangalore Rural district, India?
Methodology
Design
This study was done with a cross-sectional descriptive design using questionnaires. The questionnaires were administered in person by a social worker under observation of the researcher. The questionnaires were chosen for their ability to measure the usability of wheelchairs as perceived by wheelchair users and which independent and confounding variables potentially influence this. The questionnaires used in this study were: QUEST, WST-Q, CHART-SF and VAS. The QUEST version 2.0 was chosen for its ability to capture perceived satisfaction on the wheelchair itself and the services through which it was provided [Citation23]. The WST-Q measured to what extent the wheelchair user was capable of performing wheelchair skills needed for activities of daily living [Citation24]. The CHART-SF was used to measure the level of disability caused by a particular impairment using a more holistic approach [Citation25]. The VAS was used to assess to what extent persons would be willing to donate a particular amount of money as sign of gratitude towards the current service [Citation26]. All measurement tools were translated into the local language and were assessed for suitability during a pilot study with wheelchair users (n = 5). The data was gathered at one moment in time.
Ethical clearance
Ethical clearance was obtained from the Ethical Committees of Maastricht University (FHML/GH_2019.005) and Bangalore Baptist Hospital. Informed consent was read, verbally explained to and signed by all participants. Written permission was obtained by the authors of the questionnaires that required this.
Measures (variables)
Variables were selected according to their correspondence with independent, dependent and confounding variables as proposed by Kamaraj et al. [Citation16] and relevance to the research question. The QUEST (and related variables) are related to the independent variable described in the framework, however for this study this variable is considered as dependent, being an outcome variable. This seems, and is, paradoxal but is explained by an etymological reason. Kamaraj et al. [Citation16] write in their article that “factors pertaining to the wheelchair constituted the first domain of the independent variables. The factors pertaining to the wheelchair and the eight steps from WHO were discussed under two domains of independent variables.” The first domain covers the design, the production and ultimately the wheelchair itself. The second domain recognizes factors related to wheelchair supply and service delivery [Citation16]. They then continue their argument that the interaction between both independent domains, under influence by confounding factors, leads to a particular impact, defined as dependent variables covering factors such as physical well-being and health-related Quality of Life (QoL) among others. And although this model might hold true in reality, this study used a statistical approach wherein the outcome measure, in this study satisfaction towards wheelchair services, becomes the dependent variable. The Assistive Device and Services sections were segregated from the total score. The CHART-SF (and related variables) is considered a subject variables for this study. The WST-Q variable translates as an independent variable in Kamaraj”s framework. The measurement tools do not cover all the variables that are part of the framework as proposed by Kamaraj [Citation16].
Data analysis
All data was entered into a Microsoft Excel 2013 database and then transferred into IBM SPSS version 25 software. Descriptive statistics were gathered for all variables using scatter plots and frequency tables.
Items in the measurement tools that corresponded with one particular topic were grouped. E.g. question 1 through 8 of the QUEST are all linked to device satisfaction and question 9 through 12 are all linked to service satisfaction. The CHART-SF has questions 1 (physical domain), 2 and 3 (cognitive domain), 4 through 6 (mobility domain), 7 through 11 (occupation domain), 12 through 17 (social domain) and finally 18 and 19 (economic domain) that were grouped because they correspond with one particular topic. The WST-Q has 33 questions that are scored on 3 scales (capacity, confidence and performance). All 33 answers on 1 of those scales were grouped. Then descriptive statistics were derived. The same was done for the CHART-SF and the WST-Q. Subscores were analyzed using instructions as provided by the authors of the measurement tools. After descriptive statistics were obtained, the relation between satisfaction and independent, dependent and subject variables was analyzed. Using Pearson’s correlation coefficient, the association between variables was investigated in a bivariate correlation analysis [Citation27]. Confidence interval was set at 95% for a two-tailed correlation.
Sample
The study was conducted on a population that consisted of wheelchair users (n = 50) that have locomotor disability as primary cause of their health problem (). A convenience sampling method was applied, recruiting participants through an existing database of government issued wheelchairs and community referral. House visits were performed with a social worker. All participants lived in Bangalore Rural district. Under-aged or hearing/speech impaired wheelchair users were visited with the presence of a proxy who answered the questionnaires on the users” behalf. The proxy was either a parent or legal guardian.
Table 1. Inclusion criteria used for sample collection.
Results
A total of 50 persons with disability participated in this study (). 32% was female (n = 16) and 68% was male (n = 34). Average age of the sample was 42.1 years with the oldest participant being 90 years old and the youngest 12. 36% of the population was currently employed and 36% was employed before they obtained their impairment/disability. Only 12% (n = 6) were able to maintain their original employment or find different work after acquiring a disability. The average education level was 5th grade, or primary education. The minimum was no education at all and the maximum was a master degree. The registered caste was known for 60% (n = 30) of the study population. 40% of the population did either not report their caste or mentioned a caste that was only known to the local area. Wheelchairs being used by the sample were hospital-style manual transport wheelchairs (n = 17; ), rough-terrain wheelchairs (n = 15; ), tricycles (n = 16; ) and paediatric wheelchairs (n = 2; ).
Figure 2. Hospital style WC.

Figure 3. Rough terrain WC.

Figure 4. Tricycle.

Figure 5. Paediatric WC.

Table 2. Demographic characteristics of the sample.
Quebec user evaluation of satisfaction with assistive technology
Satisfaction, measured by the QUEST, was found to be depending on multiple factors. Despite statistical insignificance, a few findings are noteworthy (). On average female wheelchair users were more satisfied with the wheelchair itself (p > 0.05) and had higher rates of disability (p > 0.05) compared to men. Male wheelchair users were more satisfied with the support services (p > 0.05) and were less capable in wheelchair skills than women (p < 0.05). A total of 34 participants (9 female/25 male) obtained their wheelchair through services of a District Disability Rehabilitation Centre, which is supported by the government (). Sixteen participants (7 female/9 male) obtained their wheelchair from private sources (). A private source could either be a professional, commercial service or a non-professional source such as neighbours, family, spouse etc.
Table 3. QUEST scores per question for private-obtained wheelchairs.
Table 4. QUEST scores per question for government-issued wheelchairs.
Female wheelchair were more satisfied about the wheelchair (QUEST 3.95) than men (QUEST 3.70). However, they scored more diverse in terms of satisfaction with a range of 4.00 points on the wheelchair. Men had a range of 3.25 points. Male wheelchair users scored higher on satisfaction related to the services with an average of 3.69 points compared to female wheelchair users that scored on average 3.67 points. Female wheelchair users had a range of 2.75 points on satisfaction of the services, where male wheelchair users had a range of 4.00 points.
Questions 3 and 6 were scored worse compared to other questions related to the wheelchair. These questions measured satisfaction towards ease of adjustment and easy to use. The type of wheelchairs that were delivered allowed very little to none adjustment. The rough-terrain wheelchair was the only chair that allowed little adjustment of the seat cushion and back- and footrest. The other wheelchairs were built out of rigid frames that allowed no adjustment at all. A significant correlation was found between easy to use (question 6 on QUEST) and the outcome of the Wheelchair Skill Test (p < 0.01).
Questions 10 and 12 scored worse on the service section of the QUEST. Repairs and servicing (question 10) was also mentioned as a priority for female wheelchair users, meaning they emphasized the proximity of such services. Feedback on this question commonly revolved around the distance wheelchair users, both male and female, had to travel for repairs. It was hard to find spare parts in their proximity. And even if they travelled 1–4 h to reach the nearest city, they still did not know where to go exactly. Getting repairs to the wheelchair was commonly described as a day-filling activity. Question 12 scored satisfaction on the follow-up services. Twenty-two subjects indicated no follow-up visits were done after wheelchair delivery for both government and private services. All wheelchair users that did not receive follow-up rated lower satisfaction scores for the support services than the wheelchair itself.
Both male and female wheelchair users were less satisfied about the support services (p > 0.05) then the wheelchair itself (p > 0.05). Female wheelchair users named easy to use [the wheelchair], comfort [of the wheelchair], repairs and servicing [provisions for the wheelchair] and effectiveness [of the wheelchair to meet their needs] as most important aspects of wheelchairs and support services. Male subjects named safety [of the wheelchair], ease of use [the wheelchair] and effectiveness [of the wheelchair to meet their needs] as most important aspects of wheelchairs and support services.
Age was found to be negatively related to satisfaction. The older a wheelchair user got, the less satisfied he or she was. For our study population, increasing in age with 1 year resulted in a loss on the QUEST score (p > 0.05). Gender was found to be related to satisfaction scores. Being male led to a decrease in satisfaction (p > 0.05). Duration of the disability was also found to be related to satisfaction. The longer a disability was present, the more satisfied a wheelchair user was (p > 0.05). It was also found that having a higher level of education was related to better satisfaction scores (>0.05). Current status of employment, meaning the wheelchair user was employed during the time of data collection, was related to satisfaction at a 90% confidence interval (CI). Other variables that score p > 0.05 scored lower than 90% CI. In our study, it was found that being employed was negatively related to satisfaction. Status of employment before the disability was present, was also related to satisfaction. If the wheelchair user was unemployed before the disability was obtained, QUEST scores were lower (p > 0.05). A relation between marital status and satisfaction scores was found. A wheelchair user that was not married, scored lower than someone who was, or has been, married (p > 0.05). Household size was also found to be related to satisfaction, with an increase in househould size (in persons) led to an increase in satisfaction (p > 0.05). Wheelchair users that were not able to operate their wheelchair for themselves, and were dependent upon others pushing and moving them around, also showed a lower satisfaction score. Not being able to operate a wheelchair independently was related with a decrease on the QUEST score (p > 0.05).
Cause of disability was not related with other variables, however categorization of the cause of disability happened at practical convenience and is therefore not transferable to the context. The same goes for the variable wheelchair source.
Some factors, mentioned above, are to be seen in a nuanced context. For example, a private wheelchair source might also mean that the wheelchair user obtained the assistive device from a neighbour or community member directly without the involvement of a professional service. This might affect satisfaction. Next, the household size seemed both positively and negatively affecting satisfaction. Households that contain up to 7 members show increasing satisfaction. However, if the household is smaller than 3 and larger than 7 members, satisfaction seems to decline. The effect of household size on disability has been investigated before by Donohue, Bornman, and Granlund [Citation28].
The caste a wheelchair user belongs to seems to be related with satisfaction towards wheelchair services. While there was no statistical significance, it was found that those wheelchair users coming from a lower caste were more satisfied about the services they received. Kamaraj et al. [Citation16] indicated a direction in their conceptual framework where demographics (including social status) are related to wheelchair services, which is supported by this observation. Female wheelchair users coming from the lower castes Scheduled Tribe (ST) and Scheduled Caste (SC) (n = 4) had a higher average QUEST outcome, 4.04 and 4.54 respectively, then those coming from the higher castes Other Backward Caste (OBC) and General (n=5) with the Backward Caste (BC) being an exception. OBC and General scored 3.33 and 3.96 respectively with BC scoring 4.17. Male wheelchair users coming from the lower castes (ST and SC, n = 5) had a higher average QUEST outcome, 4.29 and 4.50 respectively, then those coming from the higher castes (OBC, BC and General, n=15). However, there was no statistically significant correlation between the caste someone was coming from and their gender.
Ten subjects lived under the international poverty line which is significantly correlated (p < 0.05) with (poorer) QUEST scores.
Craig handicap assessment and reporting technique – short form
Wheelchair users with a higher degree of physical disability (lower scores on CHART-SF, red.) had significant lower satisfaction related to the wheelchair (p < 0.05) but this was non-significant for support services (p > 0.05) (). The CHART-SF has six domains on which a score between 0 and 100 can be scored. A score of 100 on one domain indicates no difference with “normal-abled” persons. A score of 0 indicates complete dependency with that particular domain. The negative score was caused by one case, in which the wheelchair user indicated there was no income and high health-related expenses. Although this might be an outlier, it was important to include this case as this is an empirical observation related to satisfaction.
Table 5. CHART-SF outcomes.
Despite the physical and functional consequences of disability, average scores for female wheelchair users were lower on all subscores. Physical independence indicates that the subject of this study needed little to no help with personal care activities for both genders. Variables that seemed related to this were education (p < 0.05) and wheelchair functioning (p < 0.01). Female wheelchair users had a higher range in scores on this subscore compared to their male counterparts.
Cognitive independence was correlated with education (p < 0.01), duration of the disability (p < 0.05), current occupation (p < 0.05) and wheelchair functioning (p < 0.01). The time a wheelchair user was effectively mobile, meaning he was out of bed and going out of the house, was related to gender (p < 0.05) and wheelchair functioning (p < 0.05). Female wheelchair users had a higher range in scores on this subscore compared to their male counterparts.
Occupation, meaning daily activities such as work and housekeeping, was significantly related to education (p < 0.01), current occupation (p < 0.01) and wheelchair functioning (p < 0.01). There were 6 female and 12 male wheelchair users that had all been to school (4 of them did not finish elementary school), were employed at the time of the data collection and with the exception of one, were all independently mobile in their wheelchair. The one person that was dependent upon others to being pushed around in the wheelchair, had a shop at home and thus needed relatively little help. Some of them still had lower occupation scores on the CHART-SF, but this was mostly relatable to their spouse doing household activities while the wheelchair users was involved in paid occupation.
Social integration of the wheelchair users is related to their education (p < 0.01), current occupation (p < 0.01), occupation history (p < 0.05) and household size (p < 0.05). The 10 highest educated participants (of which 2 were female) were either employed currently, or had been employed previously. Those employed previously had such severe disability that they could not practice their original occupation. They all had household sizes ranging from 2 through 8. Female wheelchair users had a higher range in scores on this subscore compared to their male counterparts.
Economic self-sufficiency was found to be related upon household size (p < 0.05) and satisfaction (QUEST score) (p < 0.05). The negative minimum score was caused by a case wherein there was no reported income and expenditures worth 15.000 INR (=230.34 USD). Among the most self-sufficient wheelchair users, there was a notion that juxtaposed the benefits of a free-of-cost service to the benefits of a paid service. Many of the richer or more self-sufficient participants indicated that they were willing to pay for the wheelchair service. Not directly expecting better services, and thus acquire greater satisfaction, most of them mentioned that their paid contribution to the wheelchair service might improve accessibility of the service to those who have no too little financial resources.
Wheelchair skills test – questionnaire
The level of wheelchair skills (), and the independence this leads to, were significantly correlated with gender (p < 0.01) and wheelchair functioning (p < 0.01). A correlation between WST-Q scores and satisfaction was found (p < 0.01).
Table 6. Wheelchair Skill Test – Questionnaire outcome.
The more a wheelchair user was skilled in operating the device, the more satisfied they were on the device itself and the support services that were received. There is a large difference in what wheelchair skills people have. Some wheelchair users indicated that rolling forward over a distance of 10 metres was impossible, whereas others fluently operated the wheelchair in their daily lives. Male wheelchair users who did not receive follow-up were less capable of performing daily activities with their wheelchair with this score being, on average, 44.88 as measured by the WST-Q. Female wheelchair users who did not receive follow-up score lower than average as well, with 41.75.
Other findings
The VAS questionnaire was dropped from the results and discussion section. This was done because the VAS was too difficult to understand for the participants. A handful of participants were able to answer the VAS, only after lengthy explanation by the researcher and translator. Results that were obtained were too biased to be reliable. Hence, the decision was made to leave the VAS out of further analysis.
Discussion
The results of this study provide insight into the current state of wheelchair- and support services and factors influencing the outcome of these services. Overall, persons with disabilities living in Bangalore Rural district are more or less satisfied with the services they have received until now. A few observations have been made that could explain this score, and might at the same time give insight in what measures could be taken to improve the satisfaction of wheelchair users towards the wheelchair services.
The most prominent finding was the significant contribution that the presence or absence of wheelchair skills has on the level of satisfaction. In this study, wheelchair users that had higher skill levels (measured with WST-Q) scored higher on satisfaction. This is in line with previous research that stresses the importance of having adequate skills to operate the wheelchair [Citation29–31]. In other words, providing a person with only a wheelchair is less effective than providing that person with a wheelchair and the necessary training to operate and maintain that wheelchair. Both male and female wheelchair users thought that the wheelchair being easy to use was one of the most important characteristics the wheelchair and its support services should have. This emphasizes the importance of the finding that wheelchair skills are significantly contributing towards satisfaction. Follow-up activities after wheelchair provision should thus include a form of wheelchair skills training.
Variance in the scores between the subscales capacity [to do a particular activity/skill], confidence [in ability to do the activity/skill safe and well] and performance [how often the activity/skill is performed] was caused by a number of reasons. A participant might say that they are capable of doing a wheelchair skill partially (low score on capacity) but are very confident in doing it safely and well (high score on confidence). Another participant might be able to do a skill very well (high score on capacity) but receives support and thus has no need to perform that skill whenever needed or necessary (low score on performance). Or in one case, a wheelchair user was partly confident in a particular skill (low score on confidence) but received no support from others and thus needed to perform that skill always when needed (high score on performance).
Another finding of importance was the difference in outcomes from a gender perspective. Female wheelchair users had overall lower satisfaction scores compared to male wheelchair users in terms of satisfaction towards the support services. In terms of satisfaction towards the wheelchair, women had a higher average score but also more variance, a greater range. Their disability caused more limitations in their daily lives. When asked what priorities a wheelchair service should have, a difference was found between male and female wheelchair users. Female wheelchair users found the comfort of the wheelchair and proximity of repairs and servicing shops important. Easiness in using the wheelchair was a common priority among both genders. Male wheelchair users tend to focus more on specific, technical characteristics of the wheelchair itself.
It was difficult to find female wheelchair users to participate in this study. Whenever the researchers approached local health workers or consulted the database of known wheelchair users, the majority directed us towards male wheelchair users. The 16 female wheelchair users required lots of effort, driving hours, phone calls etc. With the first 40 participants that were included, only 6 were women.
It has been recognized that women with disabilities are extra vulnerable [Citation32,Citation33]. They have a disability that presents functional limitations in a society where gender equity is not yet fully accepted. A good wheelchair service would then not only provide good quality wheelchairs and support services, but also be able to answer to the different needs that female wheelchair users ask for, as opposed to what male wheelchair users expect. This could mean, for example, that wheelchairs become more comfortable and repair- and servicing shops are in a close proximity.
Priorities that were given to the wheelchair services by the users themselves, were surprising from time to time. Technological advancements and policy-level innovations are central topics in present-day research and development [Citation2,Citation34]. However, participants in this study did not necessarily acknowledge a need for these developments from their perspective. A wheelchair that was made out of light materials was not trusted in its ruggedness. It ended up being discarded. A wheelchair that was made out of imported parts broke down and could not be repaired by the local mechanic. It ended up being discarded. An old and worn-out wheelchair got replaced by a brand new one. The new wheelchair had a different propulsion mechanism than the old one. The user was not comfortable with it, did not know how to safely operate the new wheelchair and ended up discarding it.
Including end-users as actors in the service delivery program has been proven to be effective, and might reduce the non-use of wheelchairs and other assistive devices [Citation2,Citation35].
The aim of this study was to evaluate the current state of wheelchair services as perceived by wheelchair users in Bangalore Rural district. Results of this study can be used to improve wheelchair services in that region for current and future wheelchair users. Despite being based on a relatively small sample, these results can also function as grounds for extended research to try and understand the underlying patterns and factors for satisfaction better.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- WHO. WHO global disability action plan 2014–2021. Better health for all people with disability. In: WHO, editor. WHO global disability action plan 2014–2021. Geneva: WHO; 2015. p. 32.
- WHO. World report on disability; 2011. Available from Malta: http://www.who.int/disabilities/world_report/2011/report.pdf
- Roulstone A. Enabling Technology: Disabled People, Work, and New Technology. Open University Press; 1998.
- WHO. Fact sheet on wheelchairs; 2010. Available from: http://www.searo.who.int/entity/disabilities_injury_rehabilitation/wheelchair_factsheet.pdf
- GATE. Assistive technology: key facts; 2018. Available from: https://www.who.int/en/news-room/fact-sheets/detail/assistive-technology.
- Sheldon S, Jacobs NA. Report of a consensus conference on wheelchairs for developing countries, 6–11 November 2006. Bengaluru, India: ISPO; 2008.
- Shore S, Juillerat S. The impact of a low cost wheelchair on the quality of life of the disabled in the developing world. Med Sci Monit. 2012;18(9):CR533–CR542.
- Borg J, Lindstrom A, Larsson S. Assistive technology in developing countries: a review from the perspective of the convention on the rights of persons with disabilities. Prosthet Orthot Int. 2011;5(1):20–29.
- Devi S, Goyal S, Ravindra S. Evaluation of environmental barriers faced by wheelchair users in India. Disabil CBR Inclus Develop. 2013;24(3):61–74
- Matter R, Harniss M, Oderud T, et al. Assistive technology in resource-limited environments: a scoping review. Disabil Rehabil. 2017;12(2):105–114.
- WHO. Global priority research agenda for improving access to high-quality affordable assistive technology. Geneva: World Health Organization; 2017. Licence: CC BY-NC-SA 3.0 IGO
- Williams E, Hurwitz E, Obaga I, et al. Perspectives of basic wheelchair users on improving their access to wheelchair services in Kenya and Philippines: a qualitative study. BMC Int Health Human Right, 2017;17(1):22.
- Visagie S, Eide AH, Mannan H, et al. A description of assistive technology sources, services and outcomes of use in a number of African settings. Disabil Rehabil. 2017;12(7), 705–712.
- Eide AH, Øderud T. Assistive technology in low-income countries. In: Maclachlan M, Swartz L, editors. Disability and international development: towards inclusive global health. New York (NY): Springer; 2009. p. 149–160.
- Pearlman J, Cooper RA, Krizack M, et al. Lower-limb prostheses and wheelchairs in low-income countries. IEEE Eng Med Biol Mag. 2008;27(2):12–22.
- Kamaraj DC, Bray N, Rispin K, et al. A conceptual framework to assess effectiveness in wheelchair provision. Afr J Disabil. 2017;6:355.
- Toro ML, Eke C, Pearlman J. The impact of the World Health Organization 8-steps in wheelchair service provision in wheelchair users in a less resourced setting: a cohort study in Indonesia. BMC Health Serv Res. 2016;16(1):26.
- Das MB. Do traditional axes of exclusion affect labor market outcomes in India?; 2006
- O'Keefe PB. People with disabilities in India: from commitments to outcomes; 2007. Available from Washington, DC: http://documents.worldbank.org/curated/en/358151468268839622/People-with-disabilities-in-India-from-commitments-to-outcomes.
- Balakrishnan A, Kulkarni K, Moirangthem S, et al. The rights of persons with Disabilities Act 2016: mental health implications. Indian J Psychol Med. 2019;41(2):119–125.
- DRIF. Two year of the Rights of Persons with Disabilities (RPWD) Act 2016 – status of implementation in the states and UTs of India. Available from https://www.ncpedp.org/sites/all/themes/marinelli/documents/Report_of_Status_of_RPWD_Act_Final.pdf
- Magnusson D, Sweeney F, Landry M. Provision of rehabilitation services for children with disabilities living in low- and middle-income countries: a scoping review. Disabil Rehabil. 2017;41:1–8.
- Demers L, Weiss-Lambrou R, Ska B. The Quebec user evaluation of satisfaction with assistive technology (QUEST 2.0): an overview and recent progress. Technol Disabil. 2002;14(3):101–105.
- Rushton PW, Kirby RL, Routhier F, et al. Measurement properties of the Wheelchair Skills Test – Questionnaire for powered wheelchair users. Disabil Rehabil. 2016;11(5):400–406.
- Whiteneck G, Brooks C, Charlifue M, et al. Criag handicap assessment and reporting technique. CHART; 1992, 51. Available from SRALAB website: https://www.sralab.org/rehabilitation-measures/craig-handicap-assessment-and-reporting-technique
- Hjermstad MJ, Fayers PM, Haugen DF, et al. Studies comparing Numerical Rating Scales, Verbal Rating Scales, and Visual Analogue Scales for assessment of pain intensity in adults: a systematic literature review. J Pain Symp Manage. 2011;41(6):1073–1093.
- Field AP. Discovering statistics using IBM SPSS statistics. 5th ed. London: SAGE Publications; 2018.
- Donohue DK, Bornman J, Granlund M. Household size is associated with unintelligible speech in children who have intellectual disabilities: A South African study. Develop Neurorehabil. 2015;18(6):402–406.
- Best KL, Miller WC, Huston G, et al. Pilot study of a peer-led wheelchair training program to improve self-efficacy using a manual wheelchair: a randomized controlled trial. Arch Phys Med Rehabil. 2016;97(1):37–44.
- Hosseini SM, Oyster ML, Kirby RL et al. Manual wheelchair skills capacity predicts quality of life and community integration in persons with spinal cord injury. Arch Phys Med Rehabil. 2012:93(12):2237–2243.
- Paulisso DC, Schmeler MR, Schein RM, et al. Functional mobility assessment is reliable and correlated with satisfaction, independence and skills. Assist Technol, 2019;1–7.
- Chowdhury N. Women with disabilities: India's 'invisible victims'. Al Jazeera. 2018.
- Sengupta M, Agree EM. Gender and disability among older adults in North and South India: differences associated with coresidence and marriage. J Cross Cult Gerontol. 2002;17(4):313–336.
- AAATE. Global challenges in assistive technology: research, policy & practice. Paper presented at the AAATE 2019 Conference – Global Challenges in Assistive Technology: Research, Policy & Practice, Bologna, Italy; 2019.
- Harniss M, Samant Raja D, Matter R. Assistive technology access and service delivery in resource-limited environments: introduction to a special issue of disability and rehabilitation: assistive technology. Oxfordshire: Taylor & Francis; 2015.