
Introduction
In 2010, the World Health Organisation (WHO) reported 733 million people with visual impairment (VI) world-wide and predicted an increase to 929 million by 2020 [Citation1]. Their updated report from late 2019 revealed a massive 2.2 billion people with VI or blindness, far exceeding their prior expectation [Citation2]. In 2003, the World Health Service survey conducted in 70 countries across 6 continents found that, in low- and middle-income countries (LMICs), 23–24% of adults reported visual difficulty, whereas, in high-income countries, the rate was 13%. It was also reported that 5–6% of adults in LMICs suffered from severe to extreme visual difficulty, whereas in high-income countries (HICs) the rate was 2% [Citation3]. This uneven distribution of prevalence and burden appears secondary to insufficient access to health care and rehabilitative support services [Citation2]. Recent results of studies in LMICs highlighted the lack of access to healthcare services, medical rehabilitation (e.g., vision rehab) and assistive devices [Citation4–7]. The delay in needed medical evaluations and preventive care inevitably leads to increases in both correctable and uncorrectable VI with concomitant increases in the economic burden on social and medical systems. The total health care expenditure was forecasted to be $2.77 trillion in 2020, a rise from $2.30 trillion in 2010[Citation8]. In addition, the WHO reported that the global economic impact associated with just absenteeism and productivity loss, indirect medical costs, would be $176 billion in 2020 [Citation8].
Visual impairment (VI) engenders disability across the severity spectrum as access to spatial information is lost, impeding the ability to complete critical activities of daily living. Vision plays a crucial role in the effective capture and integration of sensory information from the surrounding environment; this complex process enables individuals to localize and recognize objects, apprehend three-dimensional relationships among objects including one’s own location relative to nearby objects (egocentric), and, on a meta-level, build spatial cognition [Citation9]. Thus, virtually all aspects of a visually impaired individual’s life are affected. More broadly, VI leads to difficulties in performing activities of daily living, reduced mobility and social participation, resulting in diminished independence and quality of life, and an increased risk of depression. Aside from the individual’s sensory limitations, there are physical/environmental (e.g., lack of accessible infrastructure) and social factors (e.g., discrimination) that may magnify the impact of the loss of vision.
Over the past few decades, global initiatives have started to address barriers regarding engagement for persons with VI, including ways to streamline social integration; however, the data reveal that social participation is certainly not satisfactory [Citation1,Citation10–13]. In order to aid the scientific community in a progressive set of next steps, we elaborate in this paper on critical needs with the hope that a more comprehensive perspective will galvanize stakeholders. We review VI in the International Classification of Functioning (ICF) conceptual framework, discuss international and national regulations, delineate overarching goals, and propose potential solutions.
Framework
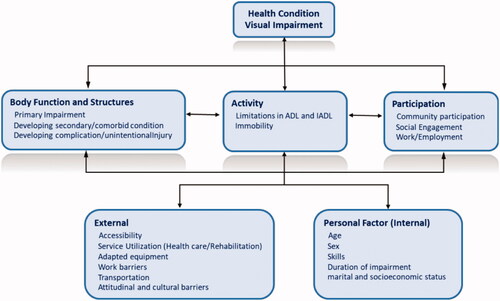
The International Classification of Functioning, Disability and Health (ICF) established a standardized language to describe health and its associated states, matching health actions on the same subject, helping in the decision-making for the individualized rehabilitation process [Citation14]. Here we will use the ICF, , as a framework to explore VI and its associated disability-related ramifications.
Figure 1. Adopted from WHO, how to use ICF? VI involves bidirectional cause and effect relations between Activity, Body Function and Structure and Participation.
Impairment: Aetiology and sequelae
Globally, the most common causes of VI are uncorrected refractive errors, cataracts, age-related macular degeneration, glaucoma, diabetic retinopathy, corneal opacities, and trachoma. The leading causes of VI vary by country: in LMICs, VI caused by cataracts is more common than in high-income countries. On the other hand, VI in high-income countries is mainly attributable to diabetic retinopathy, glaucoma, and age-related macular degeneration [Citation15]. Regardless of aetiology, health and wellbeing are attacked by vision loss, engendering mobility losses, un- or underemployment, illness and premature mortality [Citation16]. Once the downward comorbidity spiral begins, individuals with VI are at higher risk than the general population for secondary impairment (e.g., as a result of an accident, fall and hip fractures), chronic conditions, and mental and/or social health dysfunction, as a direct or indirect result of their primary impairment [Citation16–21]. 74% of individuals with VI report worrying about their vision, and 50% experience irritability or frustration due to their vision [Citation22,Citation23]. As compared to a healthy population, the risk of clinical depression is 3-times higher, and attempted suicide is increased by 5% [Citation24]. This leaves considerable swaths of the population poor, disenfranchised, and on the receiving end of adverse health outcomes [Citation21,Citation25–29].
Activity limitation
Visual impairment produces deficits in performing requisite activities of daily living (ADL) and instrumental activities of daily living (IADLs); these activities include ambulation, eating, shopping, cleaning, cooking, mobility inside and outside the home (navigation), and transportation, all critical building blocks of life. VI is associated with substantial increases in trips, falls and long-bone fractures [Citation21,Citation25–29]. The result is feelings of anxiety and insecurity in an unknown or busy environment during walking, that is, fear of falling; once a critical point is reached many require help or companionship to travel outside of the home; this leaves many stressed, constrained in their overall mobility and functionally limited. It is not surprising that VI is an important factor in limiting engagement in physical activity generally, and, in particular, limiting activities that require travel away from home [Citation22,Citation30–32]. The frequency with which a VI person leaves home varies depending on the type of walking aid deployed for assistance during navigation and training [Citation18,Citation32]; however, the overall rate for leaving one’s domicile is strikingly low at 10%, meaning 90% are homebound [Citation18]. These startling facts, although true in almost every high-income country, tend to be even more severe in LMICs. Studies have highlighted the significant association of VI with decreased daily activity and, perhaps most devastatingly, barriers to inclusive higher education in Thailand [Citation20,Citation33–36].
Participation restriction
Although studies have shown that people with disabilities are productive at work and can perform a variety of jobs, the unemployment rate of people with disabilities is much higher both in LMICs and HICs [Citation37–42]. Data from the U.S. Bureau of Labour Statistics suggest that only 22% of the 4 million visually impaired blind in the US are employed [Citation43]. These statistics reveal massive inequities, especially when compared to a current population-wide U.S. unemployment rate of 4%. Employment opportunities are often restricted by employer attitudes about perceived difficulties in hiring, including challenges related to obtaining adaptive equipment and providing necessary accommodations [Citation11,Citation13,Citation44,Citation45]. Environmental difficulties limit physical access to job interviews, workplace-centered spatial structures, and even work-related social events [Citation12,Citation46,Citation47]. Lack of access to transportation is also a frequent reason for a person with a disability to feel discouraged when seeking work.
New challenges arise related to increases in online social participation through communication platforms that interface with mobile and/or computer technology. Although there are substantive benefits for people with disabilities and particularly those with VI through the use of assistive technologies, this group is at the highest risk of exclusion from information access [Citation48]. Inaccessibility of online content is therefore a significant barrier for people who have VI [Citation49]. More specifically, access to the rapidly growing world of lifestyle in-home delivery and transportation services using apps such as Uber, Grab and Grub Hub, on smartphones is mostly limited to people with normal or correctable vision, and accessibility options are often “bolted-on” and of limited use.
Interventions and goals: a call to action
Overcoming obstacles that people with VI encounter requires interventions that either eliminate or overcome environmental and social barriers. Considering the magnitude of VI, there is a global imperative to identify, study, and address barriers, with the goal of decreasing the global burden of visual disability. These efforts must “stand on the shoulders of” previous comprehensive approaches that have been carried out by government leaders, healthcare policymakers, and healthcare professionals. Federal-level legislation such as the Rehabilitation Act of 1973 or the Americans with Disabilities Act (ADA) of 1990, are landmarks in the United States, and conventions spearheaded by stakeholders at the United Nations have aided international efforts (). A touchstone that may prove useful as an archetype for federal and international expansion was the U.S. Department of Veterans Affairs (VA) Blind Rehabilitation Service policy that was implemented in 2008 to include comprehensive rehabilitation for individuals with VI into their health care benefits. This integration included not only the related medical and rehabilitation services but also funding for cutting-edge assistive technologies. These efforts have led to increased physical and social accessibility for those living with disabilities, including VI, and serve as the bedrock for future policies and programming worldwide.
Table 1. Global concerted action. A few examples of legislation that have been carried out by government leaders, healthcare policymakers, and healthcare professionals.
In addition to eco-systematic interventions, personal- and individual-level interventions should be emphasized and layered into a broader agenda. Primary (preventive measures) and secondary (diagnosis and treatment) prevention policies and programs have been implanted to reduce the prevalence of avoidable causes of VI, but prevalence continues to grow [Citation50]. As the number of people with irreversible visual impairment increases, it is crucial to expand rehabilitation interventions (tertiary prevention: disability limitation) [Citation51]. Rehabilitation has been shown to be beneficial in 75% of people with disabilities [Citation6], with dramatic effects on quality of life [Citation52–54].
Rehabilitation, and in particular, rehabilitation coupled with assistive technologies (AT), has the potential to empower individuals by improving functional ability and capacity. In the United States of America, data over 15 years from the National Long-Term Care Survey found that increasing the use of technology was associated with a decreased report of disability among people aged 65 years and older [Citation55]. Another study from the United States showed that users of ATs such as mobility aids and equipment for personal care reported less need for support services.
AT It can be defined as any item, equipment or product (e.g., low vision devices, hearing aids, augmentative and alternative communication devices, and computer vision technologies) that sustain or increase the functional capabilities of individuals with a disability [Citation56]. The goal of AT should be to increase the activity and participation opportunities for individuals with impairments and to break down pre-existing and to-be-encountered barriers.
More specifically for blind and visually impaired end users, AT has long been part of the rehabilitation process (mobility canes, optical magnifiers, Braille). As technologies expand, more sophisticated devices are becoming available to assist with ADLs and IADLs, including electronic aids such as eyeglass-mounted devices with optical character recognition (OCR) coupled with text-to-speech output, and distance and ranging sensor-based or computer vision-based systems (e.g., headset “wearable” platforms or “smart” cane “add-ons” for indoor navigation [Citation57]). Many of these tools can be broadly categorized as (1) infrastructure-based assistive technology [IB-AT], for example, accessible pedestrian signals at intersections for road crossing assistance, and (2) infrastructure-free assistive technology [IF-AT], for example, advanced wearables that independently provide function without leveraging environmental assets. Although the value of IB is clearly palpable, these platforms are complicated and expensive to deploy at scale and to maintain with standards when the scale is factored in. On the other hand, IF-AT has the potential to perform “out of the box” and remain unwed from infrastructure. IF-AT has the potential to overcome the gap between what individuals want to do and what current infrastructure allows them to do. This being said, “plugging” wearables into existing infrastructure [IF/B-AT], a hybrid approach (), would limit the scope and scale of infrastructural assets and advanced the capabilities of the IF-AT systems in high-need locations.
Table 2. Moving forward.
In general, IF-AT wearables have advanced immensely based on innovations from the driverless car space and the integration of multiple, miniaturized electronic sensors, such as stereoscopic-vision systems and proximity-detection platforms [Citation58]. These components can be seamlessly integrated into wearables that feature both haptic and audio outputs (human-machine interfaces), such as bone conduction headsets with synthetic speech outputs or vibrating belts or bracelets, such as the VIS4ION system (Visually Impaired Smart Service System for Spatial Intelligence and Onboard Navigation). This platform provides real-time situational and obstacle awareness in one’s immediate environment, allowing individuals to travel more safely in three-dimensional (3D) space and pays particular attention to low-body, mid-body, and high-body/head hazards [Citation59–62].
Accessibility and affordability towards the united nations sustainable development goals (SDGs)
An ability to acquire and use IF-AT or IF/B-AT in the daily life of impaired persons at an affordable price shall be the deployment goal of this call to action, in direct response to two of the UNs SDGs for Good Health and Well-Being and Sustainable Cities and Communities. Affordable and ubiquitous computing within a connected world is what unlocks the potential of this goal and the tremendous advances in telecommunication technology (4G, 5G) validates the planning.
The potential is intense for state-of-the-art IF-AT technologies, not only as alternative solutions but also as ultimate solutions that can address present and future barriers on the path to total societal integration and complete enablement for persons with visual disability. Despite the fact that major problems abound within the universe of disability and the diversity of constraints that individuals face seems limitless, the expansion of IF-AT focussed on tailored capabilities will speed up the delivery of on-demand function to individuals in-need within efficient and deployable models that are modular and built for global use with universal design. Once fully envisioned, powerful and connected wearables will ensure that visually impaired persons are independent and productive citizens of the world.
Future
Now it is time that policymakers and stakeholders examine the success rate of prevailing legislation and programmatic policy and review and revise, in order to recognize gaps and barriers and to overcome them accordingly. Globalizing the VA Blind Rehabilitation Service model that encompasses an array of rehabilitative services and provides state-of-the-art assistive technology services should be fashioned into international policy and considered for implementation at the UN. National and international accessibility standards should be adapted to ensure new buildings, public spaces, transportation, and information delivery are accessible for people with disabilities across the age span and without geographic constraints. Collaborative efforts should be taken to couple and interlink the latest IF-AT with IB-AT in order to fulfil the goal of building enabling environments to empower individuals living with visual disability and beyond and remove the barriers that prevent them from engaging in the community, including accelerated gainful employment and adaptive infrastructure at the government level. At the eco-systemic level, international and national legislation should be evaluated and revised for more cross-pollination and inter-operability. At a personal level, special attention should be given to rehabilitation, and to AT, serving as an operational intervention to implement these advances. We propose strengthening and expanding IF-AT or IF/B-AT, which has the potential to empower the visually disabled to pursue opportunities that would be experienced in independent life, working, attending school, and accessing health care. We believe interventions and strategies for improving life opportunities across the ICF framework for persons with visual impairment should be prioritized. Given the time constraints, it is important that stakeholders, policymakers and health professionals take immediate action, the centrepiece of which should be the promotion of independent living at the earliest possible stage.
Consent for publication
The manuscript was reviewed and approved by all authors.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- World Health Oraganization. Visual impairment and blindness. WHO Fact Sheet, 282. Geneva (Switzerland): WHO; 2010.
- World Health Oraganization. World report on vision. Geneva (Switzerland): WHO; 2020.
- Freeman EE, Roy-Gagnon M-H, Samson E, et al. The global burden of visual difficulty in low, middle, and high income countries. PLoS One. 2013;8(5):e63315.
- Eide AH, Nhiwathiwa S, Muderedzi J, et al. Living conditions among people with activity limitations in Zimbabwe. A representative regional survey. Trondheim (Norway): SINTEF; 2003.
- Eide AH, Loeb M. Living conditions among people with activity limitations in Zambia. A national representative study. SINTEF Rapport. Trondheim (Norway): SINTEF; 2006. (SINTEF rapport A262).
- World Health Organization. World report on disability 2011. Geneva (Switzerland): WHO; 2011.
- O’Keefe P. People with disabilities in India: from commitments to outcomes. Geneva (Switzerland): WHO; 2007.
- Gordois A, Pezzullo L, Cutler H. The global economic cost of visual impairment. AMD Alliance; 2010.
- Giudice NA. Navigating without vision: principles of blind spatial cognition. In: Montello DR, editor. Handbook of behavioral and cognitive geography. Cheltenham (UK): Edward Elgar Publishing; 2018. p. 260.
- Scott AW, Bressler NM, Ffolkes S, et al. Public attitudes about eye and vision health. JAMA Ophthalmol. 2016;134(10):1111–1118.
- Crudden A, McBroom LW, Skinner AL, et al. Comprehensive Examination of Barriers to Employment among Persons Who Are Blind or Visually Impaired. Mississippi (MS): Mississippi State University; 1998.
- Crudden A, Sansing W, Butler S. Overcoming barriers to employment: strategies of rehabilitation providers. J Visual Impairment Blind. 2005;99(6):325–335.
- McDonnall MC, Crudden A, O’Mally J. Predictors of employer attitudes toward people who are blind or visually impaired as employees. J Vocational Rehabil. 2015;42(1):41–50.
- Silva SM, Corrêa JCF, Pereira GS, et al. Social participation following a stroke: an assessment in accordance with the international classification of functioning, disability and health. Disabil Rehabil. 2019;41(8):879–886.
- Blindness and vision impairment [Internet]. Geneva (Switzerland): World Health Organization; 2018. Available from: https://www.who.int/news-room/fact-sheets/detail/blindness-and-visual-impairment
- Zhang T, Jiang W, Song X, et al. The association between visual impairment and the risk of mortality: a meta-analysis of prospective studies. J Epidemiol Comm Health. 2016;70:836–842.
- Patrick DL. Rethinking prevention for people with disabilities Part I: a conceptual model for promoting health. Am J Health Promot. 1997;11(4):257–260.
- Manduchi R, Kurniawan S. Mobility-related accidents experienced by people with visual impairment. AER J: Res Pract Visual Impairment Blind. 2011;4(2):44–54.
- Branch LG, Horowitz A, Carr C. The implications for everyday life of incident self-reported visual decline among people over age 65 living in the community [Research Support, U.S. Gov’t, Non-P.H.S. Research Support, U.S. Gov’t, P.H.S.]. Gerontologist. 1989;29(3):359–365.
- Carabellese C, Appollonio I, Rozzini R, et al. Sensory impairment and quality of life in a community elderly population. J Am Geriatr Soc. 1993;41(4):401–407.
- Felson DT, Anderson JJ, Hannan MT, et al. Impaired vision and hip fracture. The Framingham Study. J Am Geriatr Soc. 1989;37(6):495–500.
- de Haan GA, Heutink J, Melis-Dankers BJM, et al. Difficulties in daily life reported by patients with homonymous visual field defects. J Neuro-Ophthalmol. 2015;35(3):259–264.
- Wang MY, Rousseau J, Boisjoly H, et al. Activity limitation due to a fear of falling in older adults with eye disease. Invest Ophthalmol Vis Sci. 2012;53(13):7967–7972.
- Lam BL, Christ SL, Lee DJ, et al. Reported visual impairment and risk of suicide: the 1986-1996 national health interview surveys. Arch Ophthalmol. 2008;126(7):975–980.
- Klein BEK, Klein R, Lee KE, et al. Performance-based and self-assessed measures of visual function as related to history of falls, hip fractures, and measured gait time. The Beaver Dam Eye Study. Ophthalmology. 1998;105(1):160–164.
- Black A, Wood J. Vision and falls. Clin Exp Optom. 2005;88(4):212–222.
- Harwood RH. Visual problems and falls. Age Ageing. 2001;30(4):13–18.
- Lamoreux EL, Chong E, Wang JJ, et al. Visual impairment, causes of vision loss, and falls: the Singapore Malay Eye Study. Invest Ophthalmol Vis Sci. 2008;49(2):528–533.
- Ivers RQ, Norton R, Cumming RG, et al. Visual impairment and risk of hip fracture. Am J Epidemiol. 2000;152(7):633–639.
- Sengupta S, Nguyen AM, van Landingham SW, et al. Evaluation of real-world mobility in age-related macular degeneration. BMC Ophthalmol. 2015;15(1):9.
- Ramulu PY, Hochberg C, Maul EA, et al. Glaucomatous visual field loss associated with less travel from home. Optometry Vision Sci. 2014;91(2):187–193.
- van Landingham SW, Willis JR, Vitale S, et al. Visual field loss and accelerometer-measured physical activity in the United States. Ophthalmology. 2012;119(12):2486–2492.
- Bualar T. Barriers to inclusive higher education in Thailand: voices of blind students. Asia Pacific Educ Rev. 2018;19(4):469–477.
- Chotikavanich S, Chanvarapha N, Loket S, et al. A 5-year retrospective record review of hospital-based low-vision rehabilitation in Thailand. OPTO. 2018;10:41–50.
- Dilokthornsakul P, Chaiyakunapruk N, Ruamviboonsuk P, et al. Health resource utilization and the economic burden of patients with wet age-related macular degeneration in Thailand. Int J Ophthalmol. 2014;7(1):145–151.
- Yiengprugsawan V, Seubsman S-a, Sleigh AC. Association between vision impairment and health among a national cohort of 87,134 Thai adults. Asia Pac J Public Health. 2015;27(2):NP194–NP202.
- Domzal C, Houtenville A, Sharma R. Survey of employer perspectives on the employment of people with disabilities: technical report. Washington (DC): Office of Disability Employment Policy, Department of Labor; 2008.
- Houtenville AJ. Counting working-age people with disabilities: what current data tell us and options for improvement. Kalamazoo (MI): WE Upjohn Institute; 2009.
- Kennedy T, Jr. Hiring people with disabilities is good business. The New York Times [Internet]. 2018 Dec 27. Available from: https://www.nytimes.com/2018/12/27/opinion/disability-rights-employment.html.
- Mitra S, Posarac A, Vick B. Disability and poverty in developing countries: a snapshot from the World Health Survey. Washington (DC): World Bank; 2011.
- Persons with a Disability: Labor Force Characteristics Summary [Internet]. 2018. Available from: https://www.bls.gov/news.release/pdf/disabl.pdf
- World Health Organization. World report on disability 2011. Geneva (Switzerland): WHO; 2011.
- Sherrod CE, Vitale S, Frick KD, et al. Association of vision loss and work status in the United States. JAMA Ophthalmol. 2014;132(10):1239–1242.
- Dahl PR. Maximizing vocational opportunities for handicapped clients. Voc Guidance Quart. 1982;31(1):43–52.
- Corn AL, Erin JN. Foundations of low vision: clinical and functional perspectives. Arlington (VA): American Foundation for the Blind; 2010.
- World Health Organization. World report on disability: World Health Organization (WHO); 2011.
- Gold D, Simson H. Identifying the needs of people in Canada who are blind or visually impaired: Preliminary results of a nation-wide study. Int Congress Ser. 2005;1282:139–142.
- Brophy P, Craven J. Web accessibility. Library Trends. 2007;55(4):950–972.
- Butler S, Crudden A, LeJeune B, et al. Employment barriers: access to assistive technology and research needs. J Visual Impairment Blind. 2002;96(9):664–667.
- Thylefors B. A global initiative for the elimination of avoidable blindness. Community Eye Health. 1998;11(25):1–3.
- Markowitz SN. State-of-the-art: low vision rehabilitation. Can J Ophthalmol. 2016;51(2):59–66.
- Aciem TM, Mazzotta MJDS. Autonomia pessoal e social de pessoas com deficiência visual após a reabilitação. Rev bras oftalmol. 2013;72(4):261–267.
- Bittencourt Z, Montilha RCL, Gasparetto MERF, et al. Diabetic retinopathy and visual disabilities among patients in a rehabilitation program. Rev Brasoftalmol. 2011;70(6):342–348.
- Lamoureux EL, Pallant JF, Pesudovs K, et al. The effectiveness of low-vision rehabilitation on participation in daily living and quality of life. Invest Ophthalmol Vis Sci. 2007;48(4):1476–1482.
- World Health Organization. World report on disability. Geneva (Switzerland): World Health Organization; 2011.
- World Health Organization. Disability prevention and rehabilitation. Geneva (Switzerland): World Health Organization; 1991.
- Feng C, Valaee S, Au AWS, et al. Anonymous indoor navigation system on handheld mobile devices for visually impaired. Int J Wireless Inf Netw. 2012;19(4):352–367.
- Cicchino JB. Effectiveness of forward collision warning and autonomous emergency braking systems in reducing front-to-rear crash rates. Accid Anal Prev. 2017;99(A):142–152.
- Li X, Cui H, Rizzo J-R, et al. Cross-safe: a computer vision-based approach to make all intersection-related pedestrian signals accessible for the visually impaired. Advances in Computer Vision. Paper presented at the Computer Vision Conference; Las Vegas, NV; 2019 May 2–3.
- Niu L, Qian C, Rizzo J-R, et al. A wearable assistive technology for the visually impaired with door knob detection and real-time feedback for hand-to-handle manipulation. Paper presented at the ICCV Workshop; 2017 October 22–29; Venice, Italy.
- Rizzo J-R, Pan Y, Hudson T, et al. Sensor fusion for ecologically valid obstacle identification: Building a comprehensive assistive technology platform for the visually impaired. Paper presented at the 2017 7th International Conference on Modeling, Simulation, and Applied Optimization (ICMSAO); 2017 April 4–6; Sharjah, UAE.
- Shoureshi RA, Rizzo J-R, Hudson TE. Smart wearable systems for enhanced monitoring and mobility. Adv Sci Technol. 2016;100:172–178.