
Abstract
Purpose
Little is known regarding what assistive technology (AT) exists and how it is used in welfare services for people with intellectual disabilities (ID). This study aimed to explore healthcare staff's perspectives and insights regarding AT in daily support and welfare services for people with ID. We also sought to explore the associations between the use of AT and workplace-related factors and background characteristics (e.g., gender, age, and experience).
Materials and methods
Three focus group discussions were conducted with 11 informants (8 women, 3 men) working in home-based and day services. Also, 176 healthcare staff (43 men, 133 women) who worked in municipal home-based services and day services completed a questionnaire comprised of background questions and 14 items with a five-point answer scale.
Results
Number of years using AT was positively associated with a positive attitude and use of AT among the staff. Staff were mainly positive towards AT and believed that it could represent various possibilities in the everyday lives of people with ID and their own service delivery. However, the staff expressed uncertainties and ethical concerns regarding AT, and they experienced a lack of knowledge, focus, and awareness about technology in services for this group. The quantitative results mainly showed positive associations between believing in AT's usefulness and using it in services for people with ID.
Conclusions
The findings indicate that providing equipment and resources, personal interests, and staff attitudes are essential factors in successfully implementing AT for people with ID.
Healthcare staff have a positive attitude towards using AT for people with intellectual disabilities, but they also perceive uncertainty and ethical concerns.
The staff believe that there is a broad range of AT devices and systems available that can support the independence and participation of people with intellectual disabilities.
The staff need to receive more training and technical supports from their workplace and AT-related experience is associated positively with the use of assistive technology by the staff.
Implications for rehabilitation
Introduction
Modern healthcare includes the use of technologies to support treatment, delivery of care, and daily activities [Citation1]. The World Health Organisation (WHO) defines assistive technology (AT) as "assistive products and related systems and services developed for people to maintain or improve functioning and thereby promote well-being" [Citation2]. AT is an umbrella term and includes technologies from low tech to high tech, such as information and communication technologies (ICT), telecare services, and technology for security [Citation3]. AT enables and improves inclusion and participation, particularly among people with disabilities, ageing populations, and people with non-communicable diseases [Citation2]. In the Nordic countries, these technologies are often referred to as "welfare technology" [Citation4]. In this study, we address all forms of assistive technologies and use "assistive technology" to refer to any technology (including ICT) that can improve the quality of life for individuals with disabilities.
There has recently been growing interest in utilising AT to improve the quality of life of people with disabilities and older people the balance of the population is shifting towards more senior citizens as the population of Scandinavian countries ages [Citation5–7]. For example, AT is considered an innovative concept and policy area in Scandinavian countries [Citation6]. Many believe it’s necessary to invest in technologies that support healthcare services and information exchange between all individuals involved in the assistive system [Citation8]. AT offers to save time, money, and personnel and to enhance the quality of life, independence, and health management in everyday life [Citation9–11]. However, some implementation challenges include cost, complex design, the rapid pace of technological change, and disagreements about technological priorities [Citation12,Citation13]. In the literature, the targeted group for AT has been mainly the elderly [Citation6,Citation14], and other groups, like people with intellectual disabilities (ID), have received less attention despite their needs.
People with ID often need support in daily tasks [Citation15], and the literature indicates that appropriate AT can improve quality of life, daily functioning, and societal activities and facilitate ongoing inclusion efforts among people with ID [Citation9,Citation16–18]. Despite some initiatives, use of AT by people with ID is a neglected area of research and practice [Citation9]. Recent initiatives mainly consist of technologies for alarms and sensors, localisation, and ICT [Citation19]. Previous studies have extensively investigated the use of AT by people with physical disabilities or health conditions [Citation20], yet few research studies have studied persons with ID [Citation21].
A first step towards utilising AT fully is to explore the perceptions and experiences of service users and relevant stakeholders [Citation22]. Previous research on this topic has mainly focussed on the usefulness and relevance or subjective experiences of using AT in people with ID [Citation10,Citation12,Citation23–25]. However, support staff are often key agents in the lives of people with ID; therefore, their perceptions and experiences of using AT are important [Citation12,Citation26]. Mirza and Hammel reported that the involvement and motivation of support staff are necessary for developing a successful AT intervention [Citation27]. In a study, authors found that support staff were generally positive towards the use of eHealth, but they also reported challenges, such as ethical concerns towards privacy and a lack of training [Citation12]. Accordingly, little is known about the actual implementation and how healthcare staff perceive the use of AT in welfare services for people with ID.
Therefore, this study was designed to investigate healthcare staff’s perspectives and insights regarding AT in welfare services for people with ID in Norway. The main objective was to explore the possibilities, limitations, and challenges of using AT in the context of welfare services and day services for people with ID. We also sought to explore the associations between using AT and workplace-related factors and background characteristics (e.g., gender, age, and experience).
Method
The current study was a collaboration between the Disability Nurse program at the Norwegian University of Science and Technology and a municipality in mid-Norway. The study context was welfare services and day services in the municipality. In the study context, Norwegian welfare services and day services represent specialised municipal services for people with ID who need adapted housing or activity services. In Norway, disability nurses complete a bachelor’s three-year university program, including social, pedagogical, and natural science subjects, which qualifies for a health personnel authorisation. Both quantitative and qualitative methods were used in this study. All participants received written and oral information about the study and were notified that they could withdraw from the study at any time and the data would be handled confidentially. Written consent was collected before participation, and the study was approved by the Norwegian Centre for Research Data.
Quantitative part
This part of the study included a paper-and-pencil questionnaire comprised of background questions and 14 items with a five-point answer scale (completely disagree to completely agree) (). A questionnaire was developed for healthcare staff who worked with people with ID in welfare services and day centres. This part aimed to reveal technology utilisation and any observations on technology needs. Study descriptions, written informed consent, and questionnaires were sent to the managers of these services. The managers then distributed the questionnaire to their eligible staff, and participation was voluntary. In this study, the staff consisted of a wide array of healthcare professionals caring for persons with ID, including nurses, disability nurses, psychologists, medical care assistants, and caregivers. A total of 176 healthcare staff who worked in the study contexts participated in this part (). Inclusion criteria were working directly with people with ID, age 19–67 years old, and willingness to fill out the questionnaire.
Table 1. Spearman’s correlation between the items of the questionnaire and background characteristics.
Table 2. Demographic and work characteristics of participants (n = 176).
Qualitative part
Focus group discussions utilising a qualitative design were conducted to investigate staff perspectives about possibilities, limitations, and challenges of using AT in the context of welfare services and day services for people with ID. Three focus group discussions took place with 11 informants (8 women, 3 men), including staff in welfare services and day services. The focus group discussions were moderated by four authors (AEW, VH, LK, and MR). There was no relationship between the moderators and the informants apart from the study. Each focus group discussion lasted 1–2 h. All discussions were recorded and transcribed verbatim.
Focus group discussion was selected as the method for data collection because it is suitable to understand how participants discuss and make sense of the topic of interest [Citation28]. The informants learned about the main themes at the beginning of the interviews, and they were encouraged to reflect on their experiences, situations, and thoughts regarding the main topics. Being among others who share several experiences in a permissive environment can help informants to express both negative and positive opinions more efficiently [Citation29]. Thus, participants may provide researchers some perspectives through their words as well as their interactions with each other.
A semi-structured interview guide was used, including questions about the possibilities, limitations, and challenges of using AT in the context of welfare services and day services for people with ID. Examples of questions included: What kind of technology is in use in your workplace? What are your expectations of AT in your workplace? What opportunities are there to learn more about AT in your municipality? What possibilities can AT represent in future healthcare services? Do you see any challenges when using AT? Do you see any limitations in using AT?
Data analysis
Quantitative data were presented as means ± standard deviations (SDs). Statistical analyses were performed using SPSS version 24. The normal distribution was assessed for all variables. Cronbach’s alpha (α) was used to measure internal consistency for the questionnaire. Descriptive variables were compared between the males and females using independent t-tests with a statistical significance level of 0.05. Spearman’s correlation analysis was performed to explore associations between the items on the questionnaire and background characteristics. Due to the high number of comparisons, a level of significance of 0.001 was chosen to reduce the risk of false positive results.
A constant comparative method of analysis, inspired by Charmaz, was applied to analyse the qualitative data [Citation30]. This method was chosen because it represents flexible yet systematic guidelines for analysing qualitative data inductively. The analysis process included constant comparisons of initial codes and data from each focus group discussion. All authors performed initial coding separately and discussed and performed focussed coding together at several meetings. The last author did the final part of the focussed coding analysis, together with the second author. After thorough discussions and reflections, the focussed coding process was discussed with the research group and resulted in three themes with sub-themes (). The first theme was labelled “staff’s associations with technology.” Examples of the initial coding process reflecting this theme were items such as mentioning communication aids, roll talk, epilepsy alarms, and stove guards. These initial codes were part of the preliminary focussed code “associations of technology solutions” and finally included in the sub-theme “different technology products.”
Table 3. Themes and sub-themes.
Another example from the analysis process led to the second theme, “the function of AT in daily service delivery.” Examples of preliminary focussed coding that fall under this theme include looking at technology from different perspectives, technology affects residents’ participation in daily life, technology facilitates service delivery, and technology involves reduced human contact in service delivery. These preliminary focussed codes were eventually incorporated into the sub-theme “possibilities and concerns.”
The third theme was labelled “staff’s own roles and responsibilities.” Examples from the analysis process leading from preliminary focussed coding to the sub-theme “lack of professionalised approach” included need for professionalisation, lacking accountability among staff, increased consciousness among staff, and superficial knowledge among staff.
Results
Quantitative findings
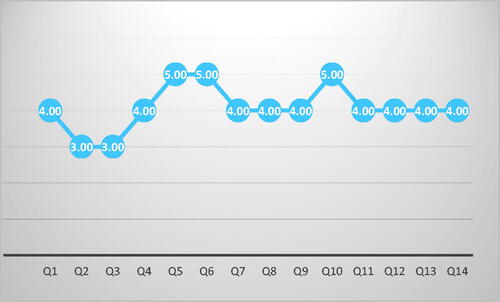
The questionnaire was completed by 176 healthcare staff (43 men, 133 women) who worked in municipal home-based services and day services (). Participants had a mean age of 35.9 years (range: 19–64) and worked within the intellectual disability field for 9.8 years on average (range: 0–40). shows the median values for the 14 items on the questionnaire rated using a five-point answer scale (1: completely disagree to 5: completely agree). The demographic and work characteristics of participants are listed in . The goal was to study potential associations between the use of AT and workplace-related factors and demographic characteristics (gender, age, experience) among the staff. The between-gender analysis revealed no significant differences in participants regarding age or work experience. Several significant correlations with various coefficients (rho) were found among the items on the questionnaire. This finding mainly indicates positive associations between believing in the usefulness of AT and using it in services for people with ID.
Figure 1. The median values for the 14-item questionnaire with a five-point answer (1: completely disagree to 5: completely agree). Note. (Q1) AT is a topic in my workplace. (Q2) I have the competence to assist/train service users to use AT. (Q3) It is educated whom I would contact to evaluate AT services. (Q4) AT is relevant in my workplace. (Q5) AT is relevant to people with ID. (Q6) AT can increase the service user’s daily mastering. (Q7) AT can be resource-saving at my workplace. (Q8) People with ID get offers about AT solutions. Q9) People with ID can use AT. (Q10) I would have benefitted from more information about AT opportunities. (Q11) I want to utilize/use AT solutions at my job. (Q12) AT can give more freedom to the person we assist. (Q13) AT is exciting. (Q14) I like to identify opportunities for new solutions.
Correlation values between the questionnaire items and background characteristics are shown in . There were also positive correlations between number of years of using welfare technology and items 1, 2, 3, and 4. In other words, more years using AT was positively associated with AT being a topic in the workplace, having the competence to assist/train service users to use welfare technology, where to address questions about welfare technology solutions, and AT being relevant in the workplace. However, no statistically significant correlations were found between the measured items and age, gender, or number of years working with people with ID.
Qualitative findings
In general, the participants were mainly positive towards AT and believed that this technology could represent various possibilities in the everyday lives of people with ID and their own service delivery. However, the participants also experienced uncertainties towards technology, and they were concerned about a lack of knowledge, focus, and awareness about technology in services for persons with ID.
Staff’s associations with technology
When sharing their associations with technology in general, participants first mentioned different aids like communication aids (e.g., roll talk and communication apps for iPads) but also technical aids like automatic light switches for the elderly, Aqua clean toilets, and warning and safety solutions such as GPS, epilepsy alarms, and stove guards. Another category mentioned was timers, like clocks that count down minutes before a planned activity or routine.
Across the focus group discussions, an interesting association that came to participants’ minds was a specific advertisement—a commercial on Norwegian television—featuring an older woman living in a virtual “smart house” with different sensors and voice control systems for a variety of functions like automatic watering of plants, turning the lights and the coffee machine on and off, and detection alarms for finding things like keys and bags. Some of the participants talked enthusiastically about the different solutions in that home. They seemed convinced that this is the way to go, but also expressed ambivalence about AT potentially replacing human relations.
Thus, AT was associated with the concrete and known examples in their lives, but also as something less known to them (like the smart home technology) as well as something representing the future, such as robots, robot cleaners/vacuum cleaners, and driverless cars. They expressed that future technology scenarios would likely be a bit scary, and it was related to feelings of ambivalence.
The function of at in daily service delivery
The participants’ experiences with AT in their own work with persons with ID were mostly related to the concrete examples mentioned above. The participants reflected on different AT in use, and their reflections and experiences were related to the possibilities they represented as well as their own concerns about possible drawbacks. The participants believed that AT had the potential to increase residents’ independence, coping, and simplification of daily life. One participant expressed:
Yes, he has a warning aid. A point in time for when he shall take his medicine is prescheduled. He is very proud that he can use it. Very proud of his own coping.
Dignity was a highlighted aspect of independence and coping. The participants expressed that AT should be used with dignity and ensure the dignity of the residents who used them. Accordingly, another participant stated:
I am applying for an Aqua clean toilet for one of the residents I work with. I think it does quite a lot with dignity; it really does. She doesn’t have to have staff into her apartment to help her at the toilet several times a day, so that you can manage on your own instead, hopefully. And I do believe that it does a lot with both coping and dignity and everything; I hope so, anyway.
Although that participant focussed on the possibilities for coping and dignity for the resident, he also expressed concern. Concern was also expressed in participants’ experiences with safety technology, which they believed represented opportunities for resident safety as well as possibilities of increased surveillance.
This duality is expressed here:
“We have a door alarm, but that is regarded as safety. Eeh, the residents have a risk of going out and getting lost, and then we can be notified when they go out. One disadvantage is that a person is really kept under surveillance, and it does reduce freedom; however, the advantage is that we can be attentive and hinder if another person goes out in cold weather and gets into big troubles.
Although the participant mentioned that the door alarm was legally approved, the example illustrates that AT includes various dilemmas. Also, the various advantages and disadvantages may differ among residents and between residents and healthcare staff.
It turned out that the majority of the participants were aware of a variety of communication aids—like supplementary and alternative communication (SAC)—and expressed that there were many possibilities following the use of such AT for persons with communication problems. One participant said:
It makes it possible to communicate at all, and it creates so much good. It makes it possible for them to say what they want. I really support this kind of technology.
However, the participants were concerned about their own situations when working with people with communication problems and highlighted that the use of AT in service delivery should represent a “win-win” situation for both parties. One participant shared the following:
I think of how practical it can make my working day, especially regarding a person that can’t tell me anything. Because I have huge frustrations too when I can’t reach him, like “what do you want?”and “what would you like to do?” While maybe, it would be easy to just touch a key with symbols, right? Things happen; AT can make my workday so much better, too. Not physically, but mentally.
It turned out that the main concern among participants was the possibility of technology taking over for face-to-face human interaction. Further, the participants were concerned about the quick pace of technology development and were concerned about possible consequences. One participant presented the following scenario:
Systems that make us get away with not looking up people, not having to visit anyone, what you see in Japan. Like you shouldn’t have to see other people, you can sit in your own living room, and you don’t have to do anything to communicate. And I think it’s kind of scary, but that’s where society goes. You’re not supposed to talk to each other, obviously. And people don’t dare to call each other anymore. So, that’s what I think of (laughs a little).
Although the participants meant that AT should not replace people and were concerned that it would, they also saw another more positive side of this issue:
I know that many of the residents I work with have fantasies and dreams of being like everyone else, living in their own flats, and functioning like the rest…and yes. And not having that person (staff) coming to you all the time.
Staff’s own roles and responsibilities
According to the study participants, there is little talk of or reflection on AT among healthcare staff working with persons with ID in shared housing. Thus, they believed that AT has not been sufficiently professionalised as an issue, and instead is a more a personal affair depending on the staff’s own interests. A general view was that staff should become more conscious about the possibilities of AT.
When asked about where they had gained their knowledge of technology, most participants interestingly stated that they had gained it through advertisements, Facebook, and by watching the TV program “Norwegians Got Talent.” Only a few had knowledge of municipal resources, like an exhibition flat with a variety of technological solutions and information. However, some knew about technical aid centres driven by county authorities, and a few had recently attended a seminar about technology in their municipality.
Participants did not talk about themselves as driving forces in obtaining technology for residents. For example, one of the participants expressed:
It’s like I haven’t even thought about it, so it’s something just to recognize it.
During the focus group discussions, the staff acknowledged their own responsibility. However, a lack of self-confidence was apparent:
When I was going to apply, I didn’t have a clue about how to do it. So, I called the technical aid centre and asked how to do it, and then I got an explanation. So, it’s something about knowing how, and what is it called again, yes, the technical aid centre, and maybe other units that can help me.
Other aspects influencing participants’ lack of self-confidence and insecurity were concerns that the municipal economy and high cost of new technology would influence their opportunities to try new technology. They believed that new technology would be expensive and thus inaccessible. The participants did not blame others like the municipal organisation for this, but recognised and emphasised their own insufficient knowledge and insecurity about technology. They realised that they had a responsibility to help persons with ID to obtain AT.
However, it turned out that the participants had a stronger belief in future disability nurses and social workers promoting AT in the field of intellectual disability than themselves. They believed that disability nurse students in clinical practice in their working context were more competent when it comes to technology than themselves. One of the participants expressed:
As long as we haven’t got any, it’s a bit hard to teach students something I haven’t competence in and don’t know anything about. Except for that stove guard, right?
However, they emphasised that students should learn about ethics concerning the use of welfare technology, such as dilemmas related to surveillance.
Discussion
This study comprehensively investigated the perspectives and insights healthcare staff have regarding the possibilities, limitations, and challenges of using AT in daily support and day services for people with ID. We also explored the associations between using AT and workplace-related factors and background characteristics (e.g., gender, age, and experience). Findings from both quantitative and qualitative aspects of the study show that healthcare staff generally had positive attitudes towards AT and believed that it brings various possibilities to the everyday lives of people with ID. The findings also indicate that the participants interpreted and prioritised the use of AT services differently. Moreover, support and services for people with ID vary across different service contexts. The current study supports the enthusiasm of individual staff members as crucial for the successful implementation of AT [Citation27,Citation31].
The quantitative portion of this study indicates that the lowest ratings were generally related to the staff’s self-esteem in assisting users and to having a source to evaluate AT services. Conversely, the highest ratings were for the relevance of AT for people with ID, the potential for AT to increase the users’ daily mastering, and the benefits of receiving more information/training about AT opportunities. In general, the staff were very positive towards the use of AT for people with ID and believed that it is resource-saving, beneficial, and offers more freedom to service users.
The findings mainly indicate positive associations between believing in the usefulness of AT and using it in services for people with ID. Age, gender, and number of years of working with ID did not affect the use of AT by the staff nor their beliefs. The number of years using AT was positively associated with a positive attitude and use of AT among the staff. However, we are not able to interpret the casual effect of these associations.
The staff expressed the potential and positive future use of AT, which was associated with AT's regular and successful use for both home-based and day services. Although the participants in this study were positive towards AT, various ethical concerns were mentioned during group discussions. Participants’ main concern was the possibility that new technology takes over face-to-face interactions at an undesirable level. They expressed uncertainty if human relations are replaced with AT. This is a common concern reported by staff and different groups of users in previous studies [Citation14,Citation32–34]. These technologies should be employed to support staff instead of replacing them [Citation33]. Moreover, privacy and negative surveillance were another concern among the staff in the present study, especially when users do not control their own sensitive data. This is particularly related to ICT and monitoring technology which is in alignment with previous research [Citation11,Citation12,Citation35]. It has been suggested that permission should be acquired from service users or their legal representatives [Citation33,Citation34,Citation36]. The fast development of technology and its consequences concerned the participants. They stated that future technology situations could be a little scary, and they felt ambivalence. In fact, these findings may indicate that the concern is not only related to AT but also new technologies in general due to the rapid pace of technological change [Citation13,Citation14].
Participants in the present study discussed diverse AT categories in use, possibilities, and possible drawbacks by describing their experiences and reflections. The participants emphasised the importance of a “win-win” situation for both healthcare staff and service recipients. The potential benefits of increasing users’ independence, coping, and simplification of daily life were underlined. Similarly, previous studies have shown that AT can positively affect the lives and independence of people with ID and promote the rights of inclusion and choice for this group [Citation9–11,Citation24]. AT can also improve interaction and communication with other people, essential for emotional and social well-being; without access to AT, people with ID can be excluded and left behind [Citation37,Citation38]. Interestingly, dignity was a highlighted aspect of independence and coping, and the staff believed that AT should be used in a conscious way to ensure the dignity of people with ID. Woensdregt et al. [Citation33] highlighted that professionals need to ensure their users have as normal a life as possible.
The influence of policy and institutional regulations on using AT have been documented [Citation9,Citation39], and efforts have been made at the international policy level to promote the use of AT for people with disabilities [Citation3,Citation40]. Nevertheless, the use of such technology has been limited in people with intellectual disabilities, and they use less AT compared to their non-intellectually disabled peers [Citation9]. Therefore, there is a complex interaction between ID, health, well-being, and AT, and other factors may play important roles in successful AT implementation. In line with our findings, previous research highlighted that merely providing equipment and resources does not automatically lead to acceptance and use of AT, and that the attitudes and beliefs of healthcare staff play an essential role in the successful implementation of AT [Citation6,Citation41,Citation42]. Attitudes and beliefs may also affect service quality and staff performance. For example, staff’s attitudes and beliefs considerably influence the participation of people with ID in various leisure activities [Citation43].
According to the staff, a lack of knowledge in staff/leaders is a key obstacle to using AT extensively for people with ID. Therefore, increased competencies are required on both sides to tackle this situation and facilitate AT’s use [Citation9,Citation32,Citation42]. There were no established sources to gain the necessary information, and the participants had to use various sources (e.g., exhibition flat, technical aid centres, or technology seminar). The participants did not talk about themselves as driving forces in obtaining technology for users, but they realised their own responsibility during the group discussions. They seemed to define their own role in the use of AT; however, a lack of self-confidence was apparent. The participants’ belief in future disability nurses and social workers regarding the use of AT in people with ID may be understood in light of these findings.
Another important issue is that understandable information, instruction, and supports should be provided and adapted to service users’ intellectual and emotional levels [Citation42,Citation44]. Participants in the present study expressed a lack of comprehensive strategies and administrative support for the use of AT in services, which is consistent with previous works [Citation39,Citation45]. The staff were responsible for providing information about AT for people with ID despite the lack of support and training. Therefore, technical support, staff availability, and training should be addressed as organisational factors [Citation32,Citation46].
In line with other studies [Citation45], our findings revealed that the staff are aware of problems and discussed them with colleagues, but not with the leaders. Participants believed that AT was not sufficiently professionalised as an issue in services, and it was considered as a personal interest rather than a routine method to deliver services. However, the participants seemed to define their own role in the use of AT and that they should become more conscious about the possibilities of AT. Two factors, including the need for AT and an increase in knowledge and awareness of AT, can facilitate the use of AT for people with ID [Citation9]. Buying and installing AT equipment is necessary, but it is not enough. Several factors have been suggested for the successful use of AT, such as staff support, attitudes, and beliefs about AT’s usefulness in a broader context in service delivery [Citation46]. Involving staff in planning for the implementation of AT may improve the idea that AT is useful and relevant for service users. Service managers should be responsive to develop and adjust AT provision to meet better the needs of the staff who support service users [Citation32].
Furthermore, the participants stated other environmental factors (e.g., the municipal economy), which could affect the possibility of testing new technology. During the group discussions, the high costs of obtaining AT were stated as a significant obstacle. This may reflect that the participants were experiencing barriers and feelings of having fewer opportunities. Lack of funding and cost of AP has been reported as a significant barrier to the use of AT [Citation9,Citation12]. Although small suppliers have usually developed costly AT for users with specific needs, mainstream technology companies are increasingly producing their own AT, particularly telecommunications and other electronic and information technologies [Citation47]. Considering the cost, there are differences between bespoke vs. mainstream devices. Bespoke devices are often high cost and can go out of date, whereas mainstream devices, on the other hand, are relatively low cost and are continually updated by the giant companies who develop them [Citation15]. For example, For example, mainstream smart speakers provide cost-effective inclusive support for speech and communication improvement among individuals with ID [Citation48]. However, there is a big range of different devices under the umbrella term of AT, and sometimes, we do not have mainstream alternatives.
Our findings indicate that advantages, disadvantages, and dilemmas might be different between healthcare staff and users, but there is a mutual challenge between them. We know that individuals with ID can have different perspectives from staff around technology [Citation15]. For example, they are often more optimistic about their abilities than staff. We missed the voice of people with ID in this study to compare their perspectives with the staff. The importance of involving key participants in research is increasingly becoming recognised.
Limitations
The findings of this study should be interpreted with caution due to the potential limitations. First, this study was based on the Scandinavian welfare system model. Also, the small-scale sample size in only one municipality was another limitation. We had a low number of performed focus-group interviews. The absence of service users (i.e., people with ID) as participants was another limitation. In further research, it would be beneficial to involve service users and family members to investigate possible ways of encouraging centre managers to facilitate AT use.
Conclusions
In conclusion, the current study provides new knowledge of how healthcare staff define and understand AT in welfare services for people with ID. It also highlights the various possibilities, concerns, and obstacles to use AT. Although healthcare staff expressed a positive attitude, our findings indicate that they perceived uncertainty and ethical concerns towards using AT. The findings show that not only providing equipment and organisational support but also personal interests and attitudes of healthcare staff play essential roles in the successful implementation of AT. The staff need to receive more training and technical supports from their workplace. The year of using AT was positively associated with the positive attitude and use of AT among the staff. This study’s findings may also indicate that disability nurse education should provide general knowledge for using AT in services for people with ID.
Ethical approval
All participants received written and oral information about the study, and that they could withdraw from the study at any time, and the data will be handled confidentially. Written consent was collected before participation, and the study was approved by the Norwegian Centre for Research Data.
Author contributions
LK and AEW designed the study. LK, VSH, MR and ALW performed and analysed the interviews. OR collected the data, performed the analyses and wrote the original draft. LK, VSH, MR and ALW read and revised the manuscript. All authors read and approved the final manuscript.
Acknowledgments
The authors would like to thank the participants for their valuable contributions. This study was funded by the Department of Mental Health, Norwegian University of Science and Technology.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The datasets generated and analysed during the current study are available from the corresponding author upon request.
Additional information
Funding
References
- Oude Weernink C, Sweegers L, Relou L, et al. Lost and misplaced items and assistive devices in nursing homes: identifying problems and technological opportunities through participatory design research. Technol Disabil. 2018;29(3):129–140.
- WHO. Assistive technology; 2018. Available from: https://www.who.int/news-room/fact-sheets/detail/assistive-technology.
- Smith RO, Scherer MJ, Cooper R, et al. Assistive technology products: a position paper from the first global research, innovation, and education on assistive technology (GREAT) summit. Disabil Rehabil Assist Technol. 2018;13(5):473–485.
- Kamp A, Obstfelder A, Andersson K. Welfare technologies in care work. NJWLS. 2019;9:1–12.
- Zander V, Gustafsson C, Landerdahl Stridsberg S, et al. Implementation of welfare technology: a systematic review of barriers and facilitators. Disabil Rehabil Assist Technol. 2021:1–16. DOI:10.1080/17483107.2021.1938707
- Frennert S, Baudin K. The concept of welfare technology in Swedish municipal eldercare. Disabil Rehabil. 2021;43(9):1220–1227.
- Hofmann B. Ethical challenges with welfare technology: a review of the literature. Sci Eng Ethics. 2013;19(2):389–406.
- Hagen K. Innovation in the care services. Norwegian Ministry of Health and Care Services (Ed.). Official Norwegian Reports NOU. 2011;11:181s.
- Boot FH, Owuor J, Dinsmore J, et al. Access to assistive technology for people with intellectual disabilities: a systematic review to identify barriers and facilitators. J Intellect Disabil Res. 2018;62(10):900–921.
- Wass S, Moeb CE, Thygesenc E, et al., editors. Use of welfare technology to increase employment of individuals with intellectual disabilities. The 16th Scandinavian conference on health informatics. Aalborg (Denmark): Linköping University Electronic Press, Linköpings universitet; 2018.
- Jamwal R, Jarman HK, Roseingrave E, et al. Smart home and communication technology for people with disability: a scoping review. Disabil Rehabil Assist Technol. 2020:1–21. DOI:10.1080/17483107.2020.1818138
- Clifford Simplican S, Shivers C, Chen J, et al. "With a touch of a button": staff perceptions on integrating technology in an Irish service provider for people with intellectual disabilities”. J Appl Res Intellect Disabil. 2018;31(1):e130–e139.
- Braddock D, Rizzolo MC, Thompson M, et al. Emerging technologies and cognitive disability. J Spec Educ Technol. 2004;19(4):49–56.
- Sanchez VG, Anker-Hansen C, Taylor I, et al. Older people's attitudes and perspectives of welfare technology in Norway. J Multidiscip Healthc. 2019;12:841–853.
- Smith E, Sumner P, Hedge C, et al. Smart-speaker technology and intellectual disabilities: agency and wellbeing. Disabil Rehabil Assist Technol. 2020:1–11. DOI:10.1080/17483107.2020.1864670
- Ramsten C, Martin L, Dag M, et al. Information and communication technology use in daily life among young adults with mild-to-moderate intellectual disability. J Intellect Disabil. 2020;24(3):289–308.
- Owuor J, Larkan F. Assistive technology for an inclusive society for people with intellectual disability. Stud Health Technol Inform. 2017;242:805–812.
- Wehmeyer ML, Smith SJ, Palmer SB, et al. Technology use and people with mental retardation. In: Glidden LM, editor. International review of research in mental retardation. Vol. 29. San Diego: Academic Press; 2004. p. 293–337.
- NBoHa W. Ehealth and welfare technology in the municipalities. Sweden: National Board of Health and Welfare; 2018.
- Lidström H, Hemmingsson H. Benefits of the use of ICT in school activities by students with motor, speech, visual, and hearing impairment: a literature review. Scand J Occup Ther. 2014;21(4):251–266.
- Werner S, Shpigelman CN. Information and communication technologies: where are persons with intellectual disabilities? Isr J Health Policy Res. 2019;8(1):6.
- O'Neill SJ, Smyth S, Smeaton A, et al. Assistive technology: understanding the needs and experiences of individuals with autism spectrum disorder and/or intellectual disability in Ireland and the UK. Assist Technol. 2020;32(5):251–259.
- Ferreras A, Poveda R, Quílez M, et al. Improving the quality of life of persons with intellectual disabilities through ICTs. Stud Health Technol Inform. 2017;242:257–264.
- Ørvig K, Claussen T. Welfare technology dilemmas facing young people with intellectual impairment – some illustrated theoretical explorations. Nordic Soc Work Res. 2018;8(3):235–248.
- Chadwick DD, Fullwood C. An online life like any other: identity, self-determination, and social networking among adults with intellectual disabilities. Cyberpsychol Behav Soc Netw. 2018;21(1):56–64.
- Ramsten C, Martin L, Dag M, et al. A balance of social inclusion and risks: Staff perceptions of information and communication technology in the daily life of young adults with mild to moderate intellectual disability in a social care context. J Policy Pract Intellect Disabil. 2019;16(3):171–179.
- Mirza M, Hammel J. Consumer-Directed goal planning in the delivery of assistive technology services for people who are ageing with intellectual disabilities. J Appl Res Intellect. 2009;22(5):445–457.
- Krueger RA, Casey MA. Focus groups: a practical guide for applied research. London; Thousand Oaks (CA): Sage Publications; 2014.
- Ivanoff SD, Hultberg J. Understanding the multiple realities of everyday life: basic assumptions in focus-group methodology. Scand J Occup Ther. 2006;13(2):125–132.
- Charmaz K. Constructing grounded theory: a practical guide through qualitative analysis. London; Thousand Oaks (CA): Sage; 2006.
- Nilsen ER, Dugstad J, Eide H, et al. Exploring resistance to implementation of welfare technology in municipal healthcare services – a longitudinal case study. BMC Health Serv Res. 2016;16(1):657.
- Aaen J. Competing concerns in welfare technology innovation: a systematic literature review. 10th Scandinavian conference on information systems; 2019. https://aisel.aisnet.org/scis2019/3
- Woensdregt G, D’Addabbo G, Scholten H, et al. Sensors in the care of persons with visual- or visual-and-intellectual disabilities: Use, needs, practical issues, and ethical concerns. TAD. 2020;32(1):15–24.
- Wolbring G, Leopatra V. Sensors: views of staff of a disability service organization. J Pers Med. 2013;3(1):23–39.
- Sanchez VG, Taylor I, Bing-Jonsson PC. Ethics of smart house welfare technology for older adults: a systematic literature review. Int J Technol Assess Health Care. 2017;33(6):691–699.
- Al Ameen M, Liu J, Kwak K. Security and privacy issues in wireless sensor networks for healthcare applications. J Med Syst. 2012;36(1):93–101.
- Dyzel V, Oosterom-Calo R, Worm M, et al. Assistive technology to promote communication and social interaction for people with deafblindness: a systematic review [systematic review]. Front Educ. 2020;5:164.
- Owuor J, Larkan F, MacLachlan M. Leaving no-one behind: using assistive technology to enhance community living for people with intellectual disability. Disabil Rehabil Assist Technol. 2017;12(5):426–428.
- Bygstad B, Lanestedt G. Expectations and realities in welfare technologies a comparative study of Japan and Norway. TG. 2017;11(2):286–303.
- Boot FH, Dinsmore J, Khasnabis C, et al. Intellectual disability and assistive technology: Opening the GATE wider. Front Public Health. 2017;5:10.
- Granger CA, Morbey ML, Lotherington H, et al. Factors contributing to teachers' successful implementation of IT. J Comp Assist Learn. 2002;18(4):480–488.
- Kersten MCO, Taminiau EF, Schuurman MIM, et al. How to improve sharing and application of knowledge in care and support for people with intellectual disabilities? A systematic review. J Intellect Disabil Res. 2018;62(6):496–520.
- Hall SA. Community involvement of young adults with intellectual disabilities: their experiences and perspectives on inclusion. J Appl Res Intellect Disabil. 2017;30(5):859–871.
- Knarvik U, Rotvold GH, Bjørvig S, et al. Kunnskapsoppsummering: Velferdsteknologi. Nasjonalt Senter for e-Helseforskning; 2017. p. 1–43. https://ehealthresearch.no/rapporter/kunnskapsoppsummering-velferdsteknologi.
- Ramsten C, Marmstal Hammar L, Martin L, et al. ICT and intellectual disability: a survey of organizational support at the municipal level in Sweden. J Appl Res Intellect Disabil. 2017;30(4):705–713.
- Aspinall A, Hegarty JR. ICT for adults with learning disabilities: an organisation‐wide audit. Br J Educ Technol. 2001;32(3):365–372.
- IoMCoDi A. Assistive and mainstream technologies for people with disabilities. The future of disability in America. Washington (DC): National Academies Press (US); 2007. Available from http://www.ncbi.nlm.nih.gov/books/NBK11418.
- Smith E, Sumner P, Hedge C, et al. Smart speaker devices can improve speech intelligibility in adults with intellectual disability. Int J Lang Commun Disord. 2021;56(3):583–593.