
Abstract
Purpose
Engagement with arts, recreation and leisure is highly valued by older adults, with positive links to their continued wellbeing. Despite an availability of new music technology, these devices are rarely designed with older adults in mind. This project explores the needs and preferences of older adults in residential care as they interact with digital music interfaces in a group music-making context.
Materials and methods
Twenty participants at an Australian residential aged-care facility were involved in a user-centred design process (20 sessions across six months) to develop digital music interfaces suitable for group music-making. Participants’ verbal comments were audio-recorded and transcribed, supported by further written observation notes made by the activity facilitators.
Results
A hybrid inductive and deductive approach to thematic analysis revealed three main themes: individual music-making, ensemble music-making and social engagement. Our results suggest that when interfaces are designed with older adults in mind, technology-assisted group music-making can facilitate bringing together residents with different experiences and abilities.
Conclusions
These findings suggest implications for rehabilitation in developing a range of musical devices for older adults to account for required flexibility, whilst maintaining an appropriate and satisfyingly “rich” musical outcome.
IMPLICATIONS FOR REHABILITATION
Older adults positively engage with music technology, showing distinct personal preferences for aspects of physical interaction, balance and quality of sound. Rehabilitation and/or wellbeing-based musical activities for older adults in residential care may benefit from considering tools that allow for personal adaptations such as these to be made.
Preferences for musical interaction can be influenced by previous musical experiences, as well as physical and/or cognitive abilities. However, on any given day musical preferences can also be subject to change.
Within a group music-making context, there is a significant capacity for older adults to feel agency in contributing to the overall sound; rehabilitation activities and/or technologies could be designed where this individual contribution to the group can be enhanced.
Group music-making using new digital music interfaces has the potential to encourage interpersonal social connections that are most likely made over repeated sessions.
Introduction
Healthy ageing is described as enabling older people to continue participation in personally meaningful activities, contributing to society for longer, while ensuring equal access to healthcare and other services [Citation1]. Engagement with arts, recreation and leisure activities is highly valued by older adults and is positively related to increased levels of health and wellbeing [Citation2–4]. Over 600 different mechanisms categorised across psychological, biological, social and behavioural processes are thought to be responsible for these gains [Citation5].
Changes in older adults’ health and living situations put them at particular risk of loneliness, which negatively impacts health and wellbeing. This has prompted research into a number of different interventions to improve social connectedness [Citation6]. Research conducted specifically within residential aged-care has demonstrated the potential of participatory arts activities [Citation7,Citation8] and group music-making [Citation9] to improve engagement and wellbeing. Participatory music activity supports mental health and wellbeing through a number of different processes relating to an individual’s sense of identity, processing of emotions, ability to rest (respite), and make connections [Citation10]. There is regular music engagement reported within residential care settings; however, researchers acknowledge that technology can enhance accessibility [Citation11,Citation12].
Embedding new technologies into residential aged-care settings with the purpose of increasing resident engagement and social connectedness has shown positive results in terms of general feasibility. Technologies used successfully across recreation, reminiscence therapy and social communication activities are notably, virtual reality [Citation13,Citation14], social robots [Citation15], touch-screen devices [Citation16] and new communication technologies [Citation17]. These studies highlight the varied needs of people in residential care, especially those living with dementia, and how these might feed into design considerations [Citation18]. When learning to use a new technology there can be both positive and negative outcomes for older adult users. An example of this is Neves and colleagues’ study [Citation17] where in using a new communication technology older adults reported positive outcomes in increased self-efficacy and comfort in using technology. Participants also reported negative outcomes such as increased self-awareness of inadequacy in using technology. The authors noted that even users with high digital literacy still required an adaptation period for getting used to technology. In terms of evaluating how technology could promote engagement, particularly for residents living with dementia, Neal and colleagues [Citation19] recommended that further studies examine interpersonal interactions that were encouraged as a result of using the technology. The authors also drew attention to the personalisation and accommodations for individual preference that may be required for an effective intervention.
Despite the availability and adaptability of new music technology to suit a range of different access and learning needs [Citation20,Citation21], few studies have adapted new technologies for older adult group music-making (notable exceptions are [Citation22–24]; c.f. [Citation25], although as noted in the Appendices section Background, adapting instruments for individuals is well-sourced in music therapy). Only 4.8% of accessible digital music interfaces in a recent review targeted older-adult use; 39.8% targeted general populations with physical impairments [Citation26]. Accessible (or “assistive”) new musical instruments also have a low rate of long-term, sustained use, with up to 50% of technology abandoned within five years [Citation27]. In some cases, having the availability of technology in aged-care for residents does not always lead to their use [Citation12]. Long-term, sustainable access to new musical technology requires financial resources, knowledge, and time [Citation27], which are often in short supply in residential aged-care.
With the aim of designing new digital music instruments for older adults in residential care, this paper examines the music-design and social engagement outcomes of a user-centred design process. This exploratory research project was designed with three distinct research questions: (i) how do older adults wish to interact with digital music instruments?, (ii) which features of group music-making with digital music instruments are important to older adults, and (iii) to what extent can technology-assisted group music-making facilitate social engagement for older adults in residential aged-care?
The user-centred design process for this project has been reported previously by Taylor et al. [Citation24]. Results from the quantitative analysis using a formalised tool to measure engagement in musical activities show that changes made to the interfaces as a result of a user-design process positively affected participants’ overall engagement. This design process, incorporating older adults’ views over a six-month period involving multiple rapid iterations, aimed to position residents in aged-care as design contributors, rather than simply technology users [Citation28]. With an aim to expand on the rich detailed opinions the residents offered regarding the devices and the musical interactions they afford, this paper will focus on the qualitative content of participants’ iterative feedback, providing context to the design process as the participants engaged in the group music-making sessions. The aim of this qualitative analysis is not to provide the viewpoint of one “representative user” from this heterogeneous group of older adults, but instead to explore the diversity of experiences and perspectives in this context [Citation29,Citation30].
Methods
Participants
Staff at an aged-care facility in Western Sydney approached potential participants in person, and through adverts distributed at the facility. Twenty residents (15 F, 5 M, ages 65–96) attended one or more of the twenty on-site technology-assisted group music-making sessions during March–August 2019. Workshop attendance was open-door, so that participants could attend as many (or as few) as they wished. More detail on attendance is provided in the Appendices section Participants. The participants had a range of previous musical experience, as well as differing cognitive and physical abilitiesFootnote1. In terms of experience explicitly playing musical instruments, during the sessions one participant reported having played guitar for a number of years. In contrast, one participant had reported no previous experience of playing any instruments.
Fourteen participants contributed verbal statements during the sessions. The other residents who participated in the sessions either preferred not to verbally engage during the sessions or had barriers to verbal engagement (e.g., medical conditions or English proficiency).
All participants provided informed written consent, and in cases where the resident had reduced capacity to consent, double-consenting procedures were followedFootnote2. The project was approved by the Western Sydney University Human Ethics Committee (H12931).
Prototype instruments
As reported in [Citation24], a number of musical interfaces (a selection of which is shown in ) were used in the group music-making session that fit two distinct categories of “instrument-inspired” (a device that resembles a real musical instrument, but behaves differently); and “alternative” controllers (a completely novel controller unlike any real musical instrument; [Citation31]). All controllers connected to a custom software application that allowed the interfaces to operate in an errorless learning paradigm: essentially, participants could learn to make music together without trial and error – pressing any interface button/surface, or strumming the eGuitar/eBass would unmute a musical stem, allowing all participants to play in time and “in tune” with each other at all times. An exception was the piano interface, developed specifically on request of one participant. Further information is included in the Appendices section Digital Music Interfaces.
Figure 1. A selection of the interfaces used. Our “alternative” music controllers: (a) the commercially available Roli Block; (b) the customised eFlute. Our customised “instrument-inspired” controllers: (c) eGuitar, (d) an iPad based piano interface, and (e) eBass.

Procedure
User design process
After an initial session where the research team and interfaces were introduced to the residents in early March, the subsequent 20 bi-weekly (twice per week) sessions of technology-assisted group music-making followed a user-centred design processFootnote3 (c.f. [Citation24]). Here, participants were exposed to the interfaces and guided to perform well-known songs together. After each session, feedback was collated by the session facilitators from the audio recordings and their own observation notes; this feedback was then passed to the interface development team. Feedback was categorised as either (i) software, (ii) hardware, or (iii) musical content, and an appropriate schedule of developments was enacted for the interfaces in question. Where possible, feedback from one week’s sessions would be coded, implemented and deployed for the following week’s sessions so participants could rapidly experience the requested changes.
The facilitators noted many requests for different songs for future sessions: due to limitations in terms of time and suitabilityFootnote4, there were far more requests for songs than could be managed.
Session facilitators and structure
Each session was conducted by two male facilitators (both currently practicing registered music therapists who were employed as research assistants to the project). Each facilitator was therefore able to continually assess (informally) whether the new interfaces were appropriately challenging for the participants, and able to provide alternative interfaces or activities should the participants indicate (verbally or non-verbally) that they were uncomfortable with the interface or activity presented to them. The content of the sessions was kept flexible in order to allow non-specific therapeutic outcomes for the participants. Participants were made aware of the project aims to have their assistance in adapting new musical instruments for group music-making appropriate for older adults in residential aged-care. Lifestyle coordinators were present during the sessions.
Each session lasted approximately 90 min and began with facilitators welcoming the participants individually and consequently as a group. After collectively choosing which song to begin performing, facilitators then worked with the participants to decide on which interfaces they wanted to use. Once interfaces were assigned, a typical structure would be (i) the facilitators moved sequentially from participant to participant, asking them to play the interface (via a button press, or strum action) and listen to the sound it created. Facilitators took this opportunity to adjust the volume of the individual interfaces if necessary. Once all participants were happy they would proceed to (ii) attempting to perform the song together. During a session, participants could play one song multiple times, or play two to three different songs. Following the group performance of a song, participants were prompted for their feedback. As the sessions went on, participants would often volunteer feedback at any stage during a session. Participants were able to change interfaces at any time if they wished, and this was typically carried out when preparing to play a new song.
Measures
Audio recordings
Participant verbal feedback was collected via an audio recording of each session, using a portable audio recorder placed in the centre of the room. Participants were asked for their opinions during each workshop, using typical user-centred design prompts to generate discussion, e.g., “How do you feel when using the interface?”, “How does it measure up to your expectations?”, “If you had a magic wand, what would you change about the interface?”.
Session facilitator notes
The session facilitators made post-session observational notes that captured not only the facilitators’ perceptions of the sessions, but their observations of participants. These included participants’ non-verbal interactions with the interfaces, and details of any individual conversations with participants during the session which may have not been intelligible from the audio recording.
Staff written post-program feedback
Staff members at the residential aged-care home were asked to complete a short survey regarding their opinions about the program after its conclusion in August 2019. Questions included those regarding their knowledge of residents’ previous musical experiences, social connections they had witnessed between residents or between residents and staff members on account of the program, as well as their thoughts about the activities included in the program, and how this might be supported long-term.
Analysis
The audio recordings of all sessions were transcribed by one of the facilitators, discarding sections where participants were talking to other residents and/or staff about unrelated daily activities (e.g., medicines). The facilitator’s notes were added to this dataset as they often described participant feedback that had been obscured in the original audio recordings. Two researchers (one facilitator, one researcher external to the project) conducted a coding procedure independently, before agreeing and revising the overall themes and sub-themes. The coding procedure followed a hybrid inductive and deductive approach [Citation32]: using initial themes derived from the two broad project objectives to interrogate the data (music-making and social engagement), the two researchers updated the thematic structure using an inductive process driven by the participant statements. The final thematic structure was then further agreed and revised in consultation with the first author. The source of each statement (participant/facilitator) was kept intact throughout coding.
Results and discussion
The themes and sub-themes that resulted from the coding process are presented in a schematic view in . The three main themes identified were:
Figure 2. Scheme of themes and sub-themes arising from qualitative coding process.
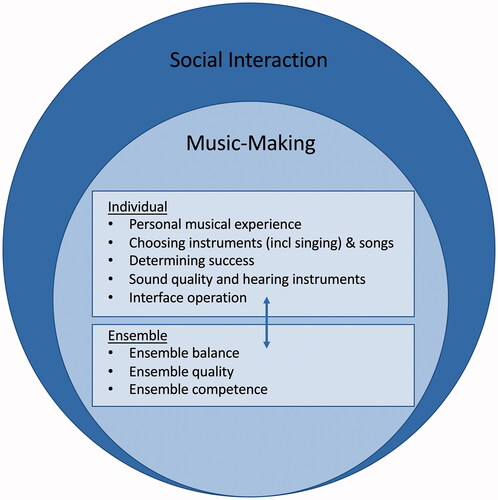
Individual music-making (encompassing five sub-themes)
Ensemble music-making (encompassing three sub-themes)
Social interaction (no sub-themes)
Statements referring to music-making issues for individual participants are contrasted with those affecting the whole group (or ensemble). The music-making on both an individual and group level provided a basis for social interactions to occur. Each theme and their sub-themes are explained below with example quotes provided for each. Parentheses after each quote include a distinct participant identifier.
Individual music-making
This represents the choice of, or preference for, distinct sounds, musical parts (e.g., melody, harmony, and accompaniment) and interfaces that were expressed by individual participants during the sessions. These were typically influenced in part by past experiences and/or aesthetic judgements. Statements here were grouped under five sub-themes (personal musical experience; choosing instruments (including singing) and songs; determining success; sound quality and hearing instruments; interface operation).
Personal musical experience
The participants and facilitators noted a mixture of musical experience in the group, some seasoned musicians, some who learned an instrument at school and then ceased upon leaving school, and others who were having a go for the first time in the current project. Expectations of how a musical interface should afford input from the user were clearly influenced by participants’ previous experiences with other traditional instruments (e.g., piano or guitar). This sometimes led to frustration when the interface did not act as expected or even allow an action that a user was familiar with from past experience:
“the only thing is when you’re used to playing, you tend to want to put your fingers where you think…like you’re playing the violin you’ve got to put your fingers on the note. With [the interfaces] you’re not sure which part is playing at the time” (P05)
The facilitators noted that despite differences in past musical experience, the group was quite musically sophisticated. Participants were all able to engage with music in a nuanced manner. A reflection from the research team was that the participants’ capabilities, and appetites for more engaging sounds and musical parts had possibly been underestimated in the initial prototype design.
Choosing instruments and songs
As participants learned to operate the interfaces, personal preferences were also expressed for how these would operate (e.g., having a sticker or physical surface on the e-guitar, see sub-theme Interface Operation). Participants were for the most part willing to try new controllers and were keen to give things a go:
“I’ll try anything once…who’d like the saxophone? That sounded very, very good actually” (P12)
Over time, facilitators observed participants preferring to use one or two controllers, building knowledge and familiarity with them, and eventually seeing an improvement in the sounds produced. When the technology did not work as expected, participants reported negative experiences. On one occasion, the system connecting the interfaces experienced a malfunction and had to be reset. One participant stated, it “frightened everybody a bit yesterday” (P05) and may have discouraged the others in the group.
Participants made many requests for songs. Participants often sang in the sessions: some preferred only to sing, some played and sang, and some just played the interfaces (some described a lack of confidence singing). Participant preferences for these were fluid:
“just whatever you like on a particular day, you can do both of course, playing around and singing” (P04)
Facilitators noted the benefits of having printed lyrics available, which assisted singing for those who felt they would not be able to remember the words. At times, the participants knew different versions of the same song and so lyrics were also seen as flexible.
Determining success
During the sessions, participants found it difficult to determine what success would look like, and how they could operate the interface to achieve the “right” sound:
“I’m playing good or bad I don’t know” (P02)
Participants wanted to know whether they were succeeding at the task of playing with the interfaces: for those with previous musical experience, they appeared to classify the correctness of their actions by reference to the instrument they used to play (see sub-theme Personal musical experience). Statements included participants talking about learning to listen for the “right” sound. Participants mentioned familiar melodies, lyrics, vocals, or someone acting as a conductor giving them something to “hook” onto. Some mentioned that they would be unaware what they were playing otherwise:
“the only way we distinguish what song’s being played is the singer…now if we only had the music would we have any idea what track we were singing?” (P05)
Sound quality and hearing instruments
Being able to hear their individual instruments was frequently noted by the participants, specifically the volume and timbre of their instrument. Facilitators often noted that this contributed to their feelings of agency both individually and in contributing to the group sound. Furthermore, the instrumental sound quality of the interfaces was commented on by participants, again with personal preferences for specific instruments, and personal dislikes:
“<the flute > is very shrill!” (P09)
Facilitators noted that the potential differences in timbre preference, as well as hearing abilities meant that finding the optimal sound (both controller and volume on that specific controller) for each person often took a lot of work within the session. An illustrative example of this challenge:
“so < participant > is saying < she > can hear the guitar but not the saxophone and you’re saying you can hear the saxophone but not the guitar? (Facilitator)
“That’s correct!” (P04)
Interface operation
The participants made specific comments concerning the gestural control and tactile interaction of the individual interfaces. For example, with the guitar and bass interfaces, which were triggered by passing the hand or finger across an invisible infra-red beam, one participant stated:
“if I pass my hand across it…because I’m not touching anything actually it’s just hit and miss” (P09).
Facilitators noted that sticking a piece of folded electrical tape horizontally across the strumming part of the guitar and bass interfaces was a frequently used tactile element of those interfaces. Similarly, participants noted that the guitar hero controller toggle was easier to use as it was a physical surface.
Participants reported that, in some interfaces, there were limitations on the number of buttons that could be pressed at once (two was the maximum on the flute interface). The amount of tactile pressure required for different surfaces was also mentioned, for example with the Roli block, some participants preferred using drumsticks, while some preferred using their hands.
The piano interface was unique because this was a requested instrument from the participants, one of whom had previously played the piano. It did not have an errorless learning paradigm like the other interfaces, and so caused issues when participants could not easily pick notes of a melody. Although popular, it caused some frustration for participants with and without prior musical experience: the interface was difficult for those with no previous experience of piano playing, as it was complicated to find the right notes “in tune” even though participants were not specifically directed to play the melody of any song. Participants with previous formal music experience found the limited number of piano keys frustrating when wanting to play musical notes outside the available range.
Ensemble music-making
This theme represents thinking of how the individual relates to and thinks about the ensemble (or the group). Statements made under the three sub-themes (ensemble balance; ensemble quality; ensemble competence) and encompassed thinking about the balance of instruments as they create the overall ensemble sound, and how each individual participant’s sound could fit within it.
Ensemble balance
Participants noted limits on the number of instruments and musical parts that could be heard in a group music-making session. Preferences for reduced numbers of musical parts at the same time were stated, to make it easier to hear both the individual and combined parts. Too many instruments and musical parts together sounded like “a jumbled mess” (P05). Participants were also concerned with the overall balance of the instrument sounds, expressing dislike if one instrument sounded louder in volume compared to the others, “taking over” (P12) or that it “just did not seem to blend”(P04). Essentially they liked to hear when the different instruments and musical parts dropped in and out of the song (i.e., the contributions of their fellow participants), and mentioned that having a “solo” for each participant at different times might help:
“if there was something that you played individually yourself that would be alright but it’s all mixed up” (P05)
The desire reported by the participants was for all instruments and musical parts to sound “good” together, with different parts complementing one another, rather than being in competition.
Ensemble quality
Participants again noted the need for a vocal line or conductor to follow so the ensemble could all play together (despite all musical parts being locked to the correct timing, the instrument voices could still “come in” (i.e., unmute) whenever the participant wanted). Nevertheless, participants sometimes requested songs without the backing vocal present, but this depended on the song and the participants.
Participants also made statements noting the quality of their own “part” relating to the whole ensemble sound, what role this played, and whether or not it was interesting. As one participant noted:
“I reckon it should have a couple of extra notes…<it > was quite boring actually…(blows raspberry)” (P04)
Ensemble competence
Participants noted other ensemble members’ sounds and playing and made comments in terms of critiquing and suggestions for improving the ensemble. They often complemented one another and made efforts to help one another with operating the interfaces, e.g., “<referring to another participant’s instrument > that’s a beauty” (P04). Both the facilitators and the participants commented on their perception that the group playing appeared to be improving over subsequent sessions:
“bit better < than last week > I think…it just feels they’re into it this time” (P04).
“my daughter came in yesterday and saw what we were doing and she said to me, Rock on < name>!” (P09)
This may have been influenced by simply the increasing familiarity with the interfaces and the task due to repeated sessions. The facilitators noted generally that the group worked increasingly well together as the sessions progressed, listening to each other, and sharing the interfaces.
Social interactions
Direct interactions between residents in the group sessions often occurred when participants were discussing ensemble competence. Examples include participants suggesting others play certain interfaces, commenting on the clarity and beauty of another participant’s instrument sound, or on how well another participant played. Over time, the participants would start to self-direct the group sessions, suggesting what instrument they wanted to play, what others might want to play.
“this chap should be trying this…yes you!” (P01)
“do you want to have a go at this piano sound? When it comes it’ll be like you’re playing it yourself” (P05)
Throughout subsequent sessions, the facilitators commented on the increasing honesty of responses from participants, leading one participant who drew attention to potential participant biasFootnote5 in the beginning, later took the occasional role of trying to elicit more specific (and honest) in-session responses from other residents.
Generally, some participants reported the workshop series allowed them to become better acquainted, and it was also something they could discuss together. Within the group there were differences in previous social integration within the facility, e.g., some were often spending time together in the various exercise classes, activities, and sitting together at mealtimes. Others had less interaction with group members before the music sessions, which was reflected in different opinions on whether the workshops changed how residents related to one another. For some the change was positive, while others felt there had been no change. From feedback given by the lifestyle coordinators at the facility, it was noted that these other opportunities were often large scale interactions, unlike the smaller group often at the music sessions. Informal indicators of success of the activity are included in the Appendix.
General discussion
This paper investigated the needs and preferences of a group of older adult residents in an aged-care facility when participating together in technology-assisted group music-making. Qualitative analysis of participant statements in the context of a 20-session user-centred design process with iterative adaptations of various digital musical interfaces revealed three main themes: individual music-making, ensemble music-making, and social interaction forming the basis of our discussion. As well as highlighting preferences for interaction, these statements often also reflected some of the challenges the participants experienced when learning how to use the new musical interfaces in a group music-making format.
The first research question asked how older adults wanted to interact with digital music interfaces. The findings reflect the complexities of designing any such interface for a heterogenous group of older adults who comprise a mixture of experiences, abilities, and desires. Finding the “right” interface for each participant is an extremely important issue requiring a great deal of time and effort [Citation33]. From our qualitative findings presented here, the right interface not only addressed the instrumental sound the participant wished to play (e.g., piano, saxophone, guitar), but also the physical gestural control each participant was comfortable with (pressing buttons, or strumming). Although non-tactile interfaces (or empty-handed controllers) such as Soundbeam are often used in music therapy practice [Citation20], we found participants appeared to prefer tactile (or physical) controllers (e.g., placing an additional physical surface on the eGuitar and eBass to touch when strumming), possibly as it allowed them to better connect cause and effect [Citation20]. In line with conclusions by Frid [Citation26], a broad suggestion for consideration is flexible, personalised interfaces that allow for minor adaptations such as fine-tuning the timbre, the tactile interaction and complexity of the part (such as the approaches to making digital music instruments accessible reported in [Citation21]). Although the interfaces may on some level be simpler to physically operate than traditional acoustic instruments, older adults prefer more complex musical output; they appreciate and desire complex and interesting music. This careful attention to the “richness” of sound [Citation22,Citation23] is important for design of these interfaces.
The loudness of each interface was extremely important to the participants as it allowed them to pick out their own individual sound, and be cognisant of their contribution to the ensemble (moreso than for traditional musical instruments, [Citation34]). A design aspect that may have made it difficult for participants to clearly hear their own instrument was that audio from all interfaces was routed through a pair of central speakers in the middle of the group. Flexibility here could be addressed by each participant having individual speakers. Potential solutions for the improvement in older adults’ experience of audio quality in music activities should also consider the effects for those with hearing loss. The type of audio device (e.g., hearing aid, cochlear implant) used to interact with music can significantly affect an older adult’s perception and experience [Citation35]. When using these audio devices, sound quality may be further reduced, and the severity of hearing loss appears to affect which musical genres are appreciated most [Citation36]. In practical terms this could mean that personalisation in terms of listening device as well as the type of music may be necessary for older adults with different levels of hearing loss to participate in the same musical activity.
The second research question asked which features of group music-making with digital music instruments were important to older adults. Participants were very vocal and made numerous requests for different songs to play along with. They were particular about the types of instruments and timbres they preferred, whether a musical part was interesting in both solo and ensemble contexts. The loudness of the sound in the ensemble was important, and too many loud instruments and musical parts could lead to the overwhelming feeling of a “jumbled mess”.
Besides the sense of contributing to the ensemble, participants also expressed interest in being able to have solo parts within the song, or musical parts that came in and out, instead of all instruments playing together all at the same time.
However, these preferences were subject to change: previous musical experiences certainly modulated how participants interacted with the digital music interfaces, but it did not prevent participants from wanting to try something new. This is in line with [Citation12] that participants’ past musical experiences do not necessarily dictate their current musical interests. Participants’ interchangeable attitudes towards interaction with the music interfaces also held true in their propensity to sing along. We note that to some extent, having printed lyrics on hand for all available songs was helpful because singing was often a motivator for engagement. Similarly, we found that unreliable technology can have a detrimental impact on engagement, either because participants felt responsible, or they were reminded of the complexity of the technology.
Our final research question concerned the aspects of technology-assisted group music-making which encouraged social interaction. Group music-making afforded opportunities for residents to get to know each other in smaller social groups than the larger exercise or creative activities available in the facility. Participants increasingly engaged with the activity and became increasingly more honest in their feedback. This suggests that repeated sessions of this type of activity not only facilitates adaptation to new technologies [Citation17] but also builds group rapport and trust, and encourages inter-participant social connection over time. Our results suggest that this increasing social connection between participants was perceived by both the participants and the facilitators. Moreover, at the conclusion of the sessions several participants expressed informally to the facilitators that they were interested in further sessions if these could be arranged.
Implications
Two main implications for the design of technologies supporting older adults’ engagement in arts and leisure activities arise from our results: i) that flexibility may be required both within and across different musical devices, and ii) how interfaces might be simplified without compromising the complexity of the output. Various preferences for physical interaction, instrument sound, and timbre and volume balance, point towards the design of flexible technologies. User-centred customisation and adaptation is promoted in music device research [Citation26] but with limited application for older adults’ use. Older adults, as well as having a range of different abilities, also have a range of motivations for participating in social and leisure activities [Citation37–39] such as digital games [Citation37] and social robot companions for older adults [Citation40], thus, there is naturally no silver-bullet device for older adult group music-making.
Conversely, a peril in designing a tool specifically for older adults is the perception of age appropriateness [Citation38] or that it in some way infantilises them. Our results indicated that older adults can have distinct, “rich” aesthetic preferences for music regardless of their level of musical experience. Activities, tools or apps designed for children may be inappropriate [Citation40], although there may be differences between what adults find child-like for musical instruments depending on experience and preferences (Ibid). Approaching a musical instrument as an older adult will offer different affordances (both physically and socially) than as a child [Citation41]. Our results indicate that including older adults in the design of such instruments can be a successful path to creating musical interactions that are aesthetically satisfying to this particular age group.
Limitations
This study has three main limitations: (i) only fourteen (of 20) participants contributed verbal statements for analysis. Some participants had limited communicative capacity, while others preferred not to talk about their experiences; (ii) although the design of our study incorporated facilitators’ observations, including non-verbal interactions, our user-centred design process relied heavily on verbal statements, potentially excluding the preferences of participants unable to make verbal contributions and discussion on cultural differences that should be heard and incorporated into any design [Citation42]. The use of video-based methods such as those in [Citation43] may be useful to analyse non-verbal gestures or facial expressions from those less likely to communicate verbally; (iii) Although participants were free to comment at any moment, there were general prompts used for discussion: these may have drawn focus to the individual interfaces themselves (and potentially more individual concerns) rather than the wider aspect of musical interaction and the group context. Despite these limitations, we feel this study and its results contribute to literature on designing new technologies for creative activities for older adults. Examining statements and observations made during the music-making process allows evaluation of in-the-moment experiences for older adults. This can be beneficial in exploring older adults’ musical preferences, abilities and opportunities to be creative rather than focussing purely on the effects of musical activity that would be typically evaluated with pre/post measures [Citation44].
Conclusions
To realise the potential of digital music interfaces to enhance accessibility to group music-making for older adults in residential aged-care, further understanding of older adults’ needs and preferences are needed. Our findings show that older adults have particular ideas on what is optimal for both individual and ensemble instrument sound and accessibility. Our results suggest important implications for the design of technology-assisted creative arts and leisure activities for older adults, by considering which features of musical interaction can be made flexible whilst maintaining an appropriate level of engagement.
Research ethics and research participant consent
The project was approved by the Western Sydney University Human Ethics Committee (Approval Number: H12931).
Acknowledgements
The authors acknowledge the contributions of Dave Anthony, Felix Dobrowohl, Alison Short, Ehab Ghobreyal, Khushali Surti and the lifestyle team at the residential aged-care facility in Western Sydney to the delivery of this project.
Disclosure statement
The Authors declare that there is no conflict of interest.
Additional information
Funding
Notes
1 The purpose of the project was to provide group music-making sessions that all residents could attend, so details on the previous experience, and physical/cognitive abilities of the participants were not formally collected as part of the study. The range of experience and abilities were noted by the facilitators of the sessions (two registered music therapists) during their conversations with residents and staff.
2 Consent was sought for the project through the residential aged-care staff. If an individual expressed interest in the project, and the facility knew this individual had a reduced capacity to consent, a family member was then also contacted. Project information was provided to both the individual and the family member and consent sought from both.
3 This project although described as a user-centred design process, could be more accurately described as a co-design project that utilises user-centred design methods. For a discussion on the move from user-centred design to co-design, please see [Citation45] and [Citation46].
4 As detailed in [Citation24], each song was arranged with different musical parts constructed for each interface. This was not the most efficient process, being fairly time-consuming, and this had to be balanced with the time available to respond to software and hardware requests for operation of the interfaces themselves.
5 Participant bias refers to individuals acting in ways they think corresponds with what the researchers are looking for.
6 These measures are detailed and analysed in [Citation24].
References
- World Health Organization. Decade of healthy ageing [Internet]. World Health Organization 2020. https://www.who.int/initiatives/decade-of-healthy-ageing%0Ahttps://www.who.int/initiatives/decade-of-healthy-ageing/connection-series%0Ahttps://www.who.int/ageing/decade-of-healthy-ageing.
- Fraser KD, O'Rourke HM, Wiens H, et al. A scoping review of research on the arts, aging, and quality of life. Gerontologist. 2015;55(4):719–729.
- Rogers NT, Fancourt D. Cultural engagement is a risk-reducing factor for frailty incidence and progression. J Gerontol – Ser B Psychol Sci Soc Sci. 2020;75:571–576.
- Tymoszuk U, Perkins R, Spiro N, et al. Longitudinal associations between Short-Term, repeated, and sustained arts engagement and Well-Being outcomes in older adults. J Gerontol B Psychol Sci Soc Sci. 2020;75(7):1609–1619.
- Fancourt D, Aughterson H, Finn S, et al. How leisure activities affect health: a narrative review and multi-level theoretical framework of mechanisms of action. Lancet Psychiatry [Internet]. 2021;8(4):321–329.
- O’Rourke HM, Collins L, Sidani S. Interventions to address social connectedness and loneliness for older adults: a scoping review. BMC Geriatr. 2018;18(1):13.
- Fraser A, Bungay H, Munn-Giddings C. The value of the use of participatory arts activities in residential care settings to enhance the well-being and quality of life of older people: a rapid review of the literature. Arts Heal. 2014;6(3):266–278.
- Pappne Demecs I, Miller E. Participatory art in residential aged care: a visual and interpretative phenomenological analysis of older residents’ engagement with tapestry weaving. J Occup Sci. 2019;26(1):99–114..
- Paolantonio P, Cavalli S, Biasutti M, et al. Art for ages: the effects of group music making on the wellbeing of nursing home residents. Front Psychol [Internet]. 2020;11:1–14.
- Perkins R, Mason-Bertrand A, Fancourt D, et al. How participatory music engagement supports mental well-being: a meta-ethnography. Qual Health Res. 2020;30(12):1924–1940.
- Garrido S, Dunne L, Perz J, et al. The use of music in aged care facilities: a mixed-methods study. J Health Psychol. 2020;25(10–11):1425–1438.
- Krause AE, Davidson JW. A qualitative exploration of aged-care residents’ everyday music listening practices and how these may support psychosocial well-being. Front Psychol. 2021;12:1–12.
- Baker S, Waycott J, Robertson E, et al. Evaluating the use of interactive virtual reality technology with older adults living in residential aged care. Inf Process Manag [Internet]. 2020;57(3):102105..
- Webber S, Baker S, Waycott J. Virtual visits: reminiscence in residential aged care with digital mapping technologies. Australas J Ageing. 2021;40(3):293–298.
- Fields N, Xu L, Greer J, et al. Shall I compare thee…to a robot? An exploratory pilot study using participatory arts and social robotics to improve psychological well-being in later life. Aging Ment Heal. 2021;25(3):575–584..
- Juul A, Wilding R, Baldassar L. The best day of the week: new technology enhancing quality of life in a care home. Int J Environ Res Public Health. 2019;16:1–17.
- Barbosa Neves B, Franz R, Judges R, et al. Can digital technology enhance social connectedness among older adults? A feasibility study. J Appl Gerontol. 2019;38(1):49–72.
- Tsekleves E. 2021;:63–89. Things: design interventions against dementia. In: Tsekleves E, Keady J, editors. Design for people living with dementia: interactions and innovations. Routledge.
- Neal I, Du Toit SHJ, Lovarini M. The use of technology to promote meaningful engagement for adults with dementia in residential aged care: a scoping review. Int. Psychogeriatr. 2020;32(8):913–935.
- Ward A, Davis T, Bevan A. Music technology and alternate controllers for clients with complex needs. Music Ther Perspect. 2019;37(2):151–168.
- Ilsar A, Kenning G. Inclusive improvisation through sound and movement mapping: from DMI to ADMI. ASSETS 2020 - 22nd Int ACM SIGACCESS Conf Comput Access. 2020. p. 1–8.
- Favilla S, Pedell S. Touch screen ensemble music: Collaborative interaction for older people with dementia. 25th Aust Comput Interact Conf Augment Appl Innov Collab. 2013. p. 481–484.
- Favilla S, Pedell S. Touch screen collaborative music: Designing NIME for older people with dementia. Proc Int Conf New Interfaces Music Expr [Internet]. 2014; p. 35–39.
- Taylor JR, Milne AJ, Macritchie J. New musical interfaces for older adults in residential care: assessing a user-centred design approach. Disabil Rehabil Assist Technol [Internet]. 2021:1–13..
- Creech A. Using music technology creatively to enrich later-life: a literature review. Front Psychol. 2019;10:1–14.
- Frid E. Accessible digital musical instruments—a review of musical interfaces in inclusive music practice. MTI. 2019;3(3):57.
- Lucas A, Ortiz M, Schroeder F. The longevity of bespoke, accessible music technology: a case for community. Proc Int Conf New Interfaces Music Expr [Internet]. 2020. p. 243–248.
- Jiancaro T, Jaglal SB, Mihailidis A. Technology, design and dementia: an exploratory survey of developers. Disabil Rehabil Assist Technol. 2017;12(6):573–584.
- Braun V, Clarke V. Conceptual and design thinking for thematic analysis. Qual Psychol. 2022;9:1–67.
- Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101.
- Miranda ER, Wanderley MM. New digital musical instruments: control and interaction beyond the keyboard (vol. 21). AR Editions, Inc.; 2006.
- Fereday J, Muir-Cochrane E. Demonstrating rigor using thematic analysis: a hybrid approach of inductive and deductive coding and theme development. Int J Qual Methods. 2006;5(1):80–92.
- Gilboa A, Almog Y. Why that instrument? A bibliographic study of the reasons instruments are chosen by music therapy clients. Nord J Music Ther. 2017;26(5):411–431..
- Engelbrecht R, Shoemark H. The acceptability and efficacy of using iPads in music therapy to support wellbeing with older adults: a pilot study. Aust J Music Ther. 2014;26:52–73.
- Fowler SL. The effect of auditory device, onset of hearing loss, and chronologic age on music perception and appreciation in adult listeners. The University of Texas at Dallas; 2021.
- Looi V, Rutledge K, Prvan T. Music appreciation of adult hearing aid users and the impact of different levels of hearing loss. Ear Hear. 2019;40(3):529–544.
- Sayago S, Rosales A, Righi V, et al. Digital games and older people from a theoretical and conceptual perspective: a critical literature review. In: Neves BB, Vetere F, editors. Ageing digit technol des eval emerg technol older adults. Springer; 2019. p. 83–96.
- Lazar A, Nguyen DH. Successful leisure in independent living communities. Proceedings of the 2017 CHI Conference on Human Factors in Computing Systems. 2017. p. 7042–7056.
- Baez M, Nielek R, Casati F, et al. Technologies for promoting social participation in later life. In: Neves BB, Vetere F, editors. Ageing and Digital Technologies. Singapore: Springer Nature; 2019. p. 285–306.
- Coghlan S, Waycott J, Lazar A, et al. Dignity, autonomy, and style of company: Dimensions older adults consider for robot companions. Proc. ACM Hum.-Comput. Interact. 2021;5(CSCW1):1–25.
- Neves BB, Mead G. Digital technology and older people: towards a sociological approach to technology adoption in later life. Sociology 2020. 2021;55(5):888–905.
- Young L. Persons with Alzheimer’s disease and other dementias. In: Eyre L, editor. Guidelines for music practice in mental health. USA: Barcelona Publishers; 2013. p. 718–766.
- Dowlen R, Keady J, Milligan C, et al. In the moment with music: an exploration of the embodied and sensory experiences of people living with dementia during improvised music-making. Ageing Soc. 2021; 1–23.
- Dowlen R, Keady J. Music and dementia: “in the moment” and embodied perspectives. In: Crawford P, Kadetz P, editors. Palgrave encyclopaedia of health humanities. Cham: Springer International Publishing; 2022. p. 1–6.
- Sanders EB-N, Stappers PJ. Co-creation and the new landscapes of design. Co. Design. 2008;4(1):5–18.
- Merkel S, Kucharski A. Participatory design in gerontechnology: a systematic literature review. Gerontologist. 2019;59(1):E16–E25.
- Magee WL, Bertolami M, Kubicek L, et al. Using music technology in music therapy with populations across the life span in medical and educational programs. Music & Medicine. 2011;3(3):146–153.
- Ridder HM, Wheeler BL. Music therapy for older adults. In: Wheeler BL, editor. Music therapy handbook. New York (NY): Guilford Publications; 2015. p. 367–378.
- Abbott EA. Elderly residents in nursing facilities. In: Eyre L, editors. Guidelines for music therapy practice in mental health. Gilsum (NH): Barcelona Publishers; 2013. p. 685–717.
- Kessels RPC, Boekhorst S, Te Postma A, et al. The contribution of implicit and explicit memory to the effects of errorless learning: a comparison between young and older adults. J Int Neuropsychol Soc. 2005;11(2):144–151.
- Mimura M, Komatsu SI. Cognitive rehabilitation and cognitive training for mild dementia. Psychogeriatrics. 2007;7(3):137–143.
- McDermott O, Orrell M, Ridder HM. The development of music in dementia assessment scales (MiDAS). Nord J Music Ther. 2015;24(3):232–251.
Appendices
Background
The idea of adapting interfaces or instruments for musical engagement to suit the needs of the individual is not new; music therapists have long been using new technologies to engage with clients who either have limited capacity, or do not wish to engage with traditional musical instruments [Citation47]. The appropriateness of a musical instrument (and the musical activity) is highly dependent on the individual [Citation48], with therapists working to “match the level” of the client with any intervention [Citation42,Citation49] which can mean both motor and/or cognitive abilities. This can be a delicate problem when entry-level cognitive and motor requirements to playing many traditional instruments are so high (e.g., bowing a note on a violin string). For older adults living with dementia, using accessible traditional instruments such as percussion often brings the unwanted perception of being too simplistic or age-inappropriate [Citation42]. While community music therapy performance focusses on creating new and re-creating past enjoyable musical experiences, such activities are can have detrimental effects to those who are unable to effectively execute their desired level of performance (Ibid).
Participants
Reasons for non-attendance were not formally monitored, although it was anecdotally reported that several participants had periods of ill-health that prevented them from attending. During the span of the project, two participants passed away.
Reduced capacity to consent was determined by the residential care home based on their personal records. Staff at the home were engaged in seeking consent from the participants and relevant family members where appropriate.
Participants did not have the opportunity to review the transcriptions or provide feedback on the findings of the qualitative analysis reported in this paper. However, due to the structure of the project, feedback was given in subsequent sessions.
Materials
Digital music interfaces
For each session, a number of digital music interfaces (a mixture of off-the-shelf commercial products and custom-made interfaces) were made available to the participants (interface selection is explained in [Citation24]. These interfaces encompassed a variety of different levels of tactile interaction, audio-visual display, and gestural control, as well as differences in look, weight and shape (see in the main text). Each musical interface controlled one musical “part” via the MIDI protocol; all parts would play synchronously with the other interfaces. Using an errorless learning paradigm [Citation50,Citation51], all participants would essentially be in control of muting/unmuting their particular “part” in the song being performed. This ensured that no participant, despite different levels of abilities, would be “out of time” or “out of tune” with the group.
Engagement measures
Each participant’s level of engagement was measured using the Music in Dementia Assessment Scale [Citation52] distributed to one facilitator, and one member of staff at the residential aged-care facility for completion before the sessions (facilitator and staff member), during the session (facilitator only) and after each session (staff member only). Other engagement measures collected regarded the interfaces used by each individual participant, as well as the songs performed during the session.Footnote6
Sustainability considerations
A further consideration is how designs for such activities are sustainable for the future. The types of interfaces discussed in this project were centrally controlled from a laptop using custom-designed software, in order to facilitate the rapid prototyping required. Upon study completion, a sustainability placement was conducted by a student music therapist at Western Sydney University, to support the aged-care home’s lifestyle coordinators to continue running the technology-assisted music-making sessions. Despite the success of the activity itself, the following features were identified as barriers to sustainability: i) finances to acquire the equipment necessary outside of the research project, ii) the time required to train facility staff to use the system to a level they felt comfortable with running the activity, iii) continuing support to make changes to the digital music interfaces, or to add more repertoire to suit residents’ desires, iv) continuing maintenance for hardware and software elements of the system. These align with Lucas et al’s dependency model of accessing music through technology [Citation27]. Interfaces which are supported by a wealth of resources are often used more in practice, despite challenges in specialist training required for use, and suitability for different users e.g., the Soundbeam (see Ward et al. [Citation20]). This suggests that the creation of repertoire and supports is of equal importance as the design and function of the interfaces themselves for long-term adoption.
Informal indicators of success
An indicator of success of the technology-assisted group music-making activity (in terms of resident enjoyment) was reported via three separate instances: i) in one session, the facilitator noted that nine residents had shown up to the group without being notified that the activity was on, ii) one participant reported that they had made another resident at the facility aware of the group in hopes they would join, iii) lifestyle coordinators often mentioned informally to the facilitators that the participants had been “excited all week, and looking forward to the sessions”.