
Abstract
Purpose
People with physical disabilities often require lifetime support and experience challenges to maintain or (re)define their level of independence. Assistive living technologies (ALT) are promising to increase independent living and execution of activities of daily living (ADL). This paper provides a systematic literature review that aims to analyse the present state of the literature about the impact of ALT on perceived independence of people with a physical disability receiving long-term care.
Materials and methods
Databases Embase, Medline, and Web of Science were searched for eligible studies from 2010 or later.
Results
Nine studies were included, of which seven qualitative, one quantitative, and one mixed methods. Quality was generally high. ALT enabled participants to execute ADL. We found six themes for the impact of ALT on perceived independence: feeling enabled, choice and control, feeling secure, time alone, feeling less needy, and participation.
Conclusions
ALT appears to impact perceived independence in many ways, exceeding merely the executional aspect of independence. Existing research is limited and quite one-sided. More large-scale studies are needed in order to inform care organisations how to implement ALT, especially considering societal developments and challenges impacting long-term care.
IMPLICATIONS FOR REHABILITATION
People with a physical disability receiving long-term care experience that assistive living technology impacted their independence.
Their independence is increased by making them feel enabled, secure, and less needy and increasing their choice and control, time alone, and participation.
Most studies focused on the use of environmental control systems by people with spinal cord injury.
More research is needed to evaluate long-term effects of diverse assistive living technologies used by people with a physical disability receiving long-term care.
Introduction
Background
The UN Convention on the Rights of Persons with Disabilities states that people with disabilities should have equal opportunity to experience personal autonomy and live independently in the community as every other person [Citation1]. Regardless of the type, complexity or severity of the disability, they deserve the opportunity to decide how to live, work, and participate in society. People with physical disabilities such as multiple sclerosis (MS), amyotrophic lateral sclerosis (ALS), or spinal cord injury (SCI) often require lifetime support and experience challenges to maintain or (re)define their level of independence and autonomy. They may experience that their independence is compromised or restricted because of the actual or apparent conditions deriving from their disability [Citation2,Citation3]. For example, they may need help with activities of daily living (ADL) such as eating, drinking, toileting, clothing or washing themselves, making transfers or walking, social interaction, and managing their living environment (e.g., opening and closing curtains, doors, and windows).
Independence
Multiple studies have shown that independence and having control over their lives and their disability increases the quality of life for persons with a disability [Citation1,Citation4–6]. In the literature, there is no standard definition of independence. Independence is often used as a broad concept involving a wide variety of aspects. Especially for people with a disability, the term “independence” is complex and can mean different things [Citation7,Citation8]. Reindal [Citation7] describes how professionals generally focus on independence in terms of execution of ADL, while people with disabilities themselves tend to define independence as “an ability to be in control of and make decisions about one’s life”. Forber-Pratt [Citation8] studied the meaning of independence for people with physical disabilities that used wheelchairs (including herself), and found that people with a physical disability defined independence as “the ability to manage personal hygiene needs, to navigate the world, and to know one’s equipment”. More importantly it was not necessary to do all this oneself, but rather “having the personal agency and ability to manage one’s own care and having one’s voice heard during these types of tasks.”
Assistive living technology
As a concrete step towards realizing the goals of the UN Convention on the Rights of Persons with Disabilities, the WHO is coordinating the Global Cooperation on Assistive Technology (GATE) to improve access to high-quality affordable assistive technology for people with a disability all over the world [Citation9]. Assistive living technology (ALT) is used by the WHO as an umbrella term covering “any assistive items, services, and any related systems developed to optimize or preserve an individual’s daily functioning” [Citation10]. ALT is expected to have great potential to assist persons with a disability in living independently, to participate in social activities and to promote well-being [Citation11,Citation12]. For example, Brose et al. [Citation13] describe how robotic systems are promising to enable people with physical disabilities such as SCI or neuromuscular disease (e.g., to eat, prepare a meal, brush their teeth, shave, dress themselves, open cabinet doors, load a dishwasher, and fetch items in their daily living environment). ALT is widely studied in elderly people living independently in the community or in care facilities for people with dementia [Citation14,Citation15]. Also, assistive technologies used in rehabilitation in order to enhance strength and to compensate for limitations such as exoskeletons, are a topic of interest in the motor recovery of people with physical disabilities [Citation16]. These studies are mostly conducted in an acute phase after injury [Citation17]. Little is known about the impact of ALT for people with physical disabilities receiving long-term care.
This paper provides a systematic literature review that aims to analyse the present state of the literature about the impact of ALT on perceived independence of people with a physical disability receiving long-term care. The focus of the review is not on the development or technological validation of ALT.
Method
The review is written in accordance with the PRISMA statement for systematic reviews[Citation18]. A detailed protocol is published in the International Prospective Register of Systemic Reviews (PROSPERO 2021 CRD42021265176).
Search strategy
Together with an information specialist, the researchers RB, MG, and KvD developed and finalized a search strategy for the databases Embase (Ovid SP) and Medline (see Supplementary Appendix I online). Snowballing was conducted through references of eligible articles in the database Web of Science. We selected articles that were published between January 1st, 2010 up until May 17th, 2022, when the search was conducted. Because technology is developing rapidly, articles describing technology before 2010 were deemed to be irrelevant and not representative to answer our research question. We included research that met the following inclusion criteria:
original peer reviewed articles in Dutch or English;
qualitative, quantitative or mixed methods research;
research in which participants have a physical disability, are aged 18 years or older, and receive long-term care;
research examining the use of ALT in the daily living environment for execution of ADL (including communication);
self-reported outcomes regarding independence, such as the execution of ADL or perceived independence.
Exclusion criteria were:
review articles and book chapters;
research that focused exclusively on the ALT itself e.g., validation study in an experimental set-up;
ALT that is used only by care providers;
ALT for (gait) training purposes in a rehabilitation setting;
research in which participants are in an (acute) phase of rehabilitation.
Study selection
After conducting the search, duplicate articles were deleted. The articles found were assessed in two steps to ascertain whether they were eligible for inclusion. The first step involved the title and the abstract. When no exclusion criteria were detected here, the second step concerned the full text. The assessment was based on content-analysis and performed independently by two reviewers (RB and KvD). In case of disagreement about eligibility, consensus was reached by consulting a third reviewer (MG).
Data extraction and synthesis
One reviewer (KvD) created a spread sheet and charted information extracted from the included studies that contributed to answering the research question. A second reviewer (MG) checked the extracted information. The following data were extracted: author and year of publication, country where the research was conducted, study design, data collection methods, number and disability of study participants, living situation of study participants, type of technology researched, primary outcome, and main findings. We focused exclusively on research questions and results about independence; whenever other factors were researched (such as user satisfaction or barriers and facilitators for technology uptake), we only mention outcomes regarding independence in this review. To establish themes regarding the impact of ALT on the perceived independence of research participants, themes and quotes described in the included studies were extracted and grouped into categories by one reviewer (KvD) and checked by a second reviewer (MG).
Quality assessment
The scientific quality of the selected studies was evaluated independently by two reviewers (KvD and MG). They matched their results to produce a single score. For most items (84%), the reviewers’ evaluations corresponded. The reviewers discussed the items they judged differently (the other 16%) until consensus was reached. Qualitative studies were assessed on risk of bias using the Critical Appraisal Skills Program [Citation19]. The CASP deploys 10 criteria such as study relevance, design and methods, ethical considerations, reflection on the role of the researcher in relation to participants, rigorousness, and explicitness of findings. Quantitative or mixed studies were assessed using the MMAT (Mixed Methods Appraisal Tool), which contains 2 general screening criteria and 5 criteria to assess either quantitative, qualitative or mixed method research [Citation20]. The criteria for mixed methods research specifically focus on the relevance of using mixed methods and integration of quantitative and qualitative findings. Articles were not excluded based on the quality assessment [Citation21,Citation22]. For both the CASP and MMAT, the compliance of studies with the criteria were judged on the basis of three options: “yes”, “no”, or “can’t tell”.
Results
Study selection
depicts the study selection process. The database searches yielded 824 articles, of which 63 full articles were screened. Additionally, 14 articles were found through snowballing and fully screened for eligibility. We identified 9 studies that met the inclusion criteria. Study characteristics are described in .
Figure 1. Study flowchart.
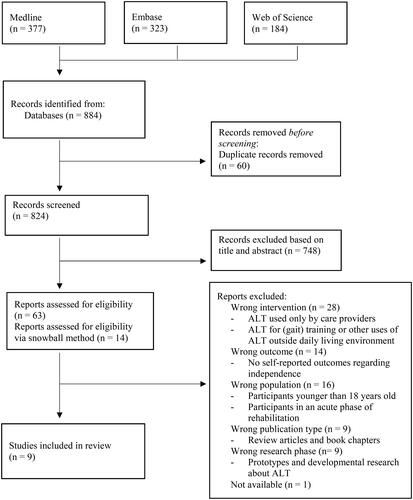
Table 1. Study characteristics.
Description of the selected studies
The selected studies were published between 2011 and 2021. Only two studies were published before 2015 [Citation23,Citation24]. Five studies were executed in Australia [Citation25–29], the other four studies took place in different countries [Citation22,Citation24,Citation30,Citation31]. The number of participants varied from n = 3 to n = 22 (mean n = 10), with a total of n = 91 participants. Participants with SCI were represented in six studies [Citation23–25,Citation27–29], one study studied participants with acquired brain injury [Citation26] and one study participants with ALS [Citation31], while two studies researched heterogenic groups of participants with varying physical disabilities (sclerosis, transverse myelitis, and spasm, MS, Duchenne, and locked-in syndrome) [Citation24,Citation30]. Blach Rossen et al. included both participants with SCI and with progressive diseases. Seven studies used a qualitative methodology [Citation23–25,Citation27–30], there was one mixed methods study [Citation26] and one quantitative study [Citation31]. Data on independence was collected by semi-structured interviews or focus groups and/or questionnaires. Interviews were aimed at how the technology enabled participants to carry out ADL that were meaningful to them, and how they experienced the impact on their independence. For example, Folan et al. [Citation25] asked this question in their semi-structured interviews with participants: “Can you share any stories about how being able to use [the technology] independently has enabled you to do activities that you want to be able to do?” and Blach Rossen et al. [Citation24] asked participants: “What is it like carrying out everyday occupations? Does [the technology] help you or make it harder for you to do such things?” The Psychosocial Impact of Assistive Devices Scale (PIADS) was used in two studies [Citation26,Citation31], and other studies used other scales focusing on ADL (IPPA, CANS). One study used their own developed standardised forms on how participants perceived the technology to impact their independence [Citation30]. The studies evaluated three types of ALTs: five studies examined environmental control systems [Citation23,Citation26–29], three focused on electric wheelchairs (or gaze-driven control systems for electric wheelchairs) [Citation24,Citation30,Citation31], and two included technology for communication aides/computer access [Citation25,Citation26]. In three studies, participants started using the technology for the purpose of the study [Citation25,Citation30,Citation31]. In the other six studies, participants were recruited that already used the technology in their own daily living environment, which was for most participants in their own home (n = 62) versus living in a long-term care facility (n = 29).
Quality of the selected studies
Six of the seven qualitative studies were of good quality and met all or most of the criteria of the CASP (see ). One study roughly met half of the criteria, due to minimal description of methods and results [Citation30]. Together with three other studies [Citation24,Citation27,Citation28,Citation30], they did not thoroughly describe their recruitment strategy. Blach Rossen et al. [Citation24] also scored low on the criteria of critical examination of the researcher’s own role, potential bias and influence in the process of conducting the study.
Table 2. Results of the CASP.
shows the quality assessment of the mixed methods study and the quantitative study. The mixed methods study [Citation26] met the majority of the criteria of the MMAT. However, it did not provide an interpretation of the quantitative data. The quantitative article [Citation31] met three of the five criteria of the MMAT, as it did not describe the sampling strategy and thus provided no information to rule out nonresponse bias.
Table 3. Results of the MMAT.
Impacts of ALT-use on independence
Participants in the included studies mentioned several ADL they were able to perform as the consequence of the ALT they used. depicts an overview of these ADL as they were mentioned in the studies, containing all information the studies gave on this topic.
Table 4. Overview of ADL supported by the use of ALT.
Many studies focused on the impact of ALT-use on perceived independence in daily life rather than focusing on the execution of specific ADL-activities. Participants shared the positive impact of ALT-use on their perceived independence (see ).
Table 5. Impact of ALT on independence.
Feeling enabled
Participants believed ALT increased their ability to independently control their environment and perform and adapt to ADL [Citation26,Citation28]. As Verdonck et al. describe, using ECS enabled participants to experience “pleasure in doing everyday things”. They explain that “ECS evoked an emotional response of feeling good and feeling better about oneself ‘because you are doing it yourself’” [Citation29]. Using ECS and mainstream devices to perform ADL made participants feel better about themselves, more self-confident, skillful and useful [Citation25,Citation26,Citation29].
Choice and control
ALT caused participants to feel empowered and in control over their everyday lives [Citation25,Citation26]. ALT increased their options and their ability to make preferred, spontaneous choices [Citation23,Citation29]. For example when to move, as Wästlund et al. [Citation30] found in participants that used an electric wheelchair: “The new opportunity for independent mobility and actions for individuals who are totally dependent on others, some of whom cannot communicate their wishes, has many important benefits. Psychological and emotional well-being improves with the ability to independently choose when and where to move.”. Hooper et al. [Citation28] describe that ECS enabled participants to choose “when and what they could control” and when they wanted carer assistance [Citation28]. Using ECS and mainstream devices gave participants the opportunity to choose how and when to receive communication, for example through the use of social media [Citation26].
Feeling secure
Participants valued ALT for giving them personal security: using ECS and mainstream devices such as mobile phones made participants feel safe [Citation26,Citation27]. Simply knowing they could use ALT when needed gave participants and their families peace of mind [Citation28]. As Myburg et al. [Citation27] summarise for users of ECS: “All participants, even those most frustrated with their system, placed value on its ability to provide some level of personal security.”
Time alone
Using ALT reintroduced participants to spending time alone, which Myburg et al. [Citation27] mention as one of the most powerful advantages of ALT. Because participants could use ECS to call for help, they did not need a physical presence in the same room anymore: “not a shadow with you” [Citation23,Citation24]. “Having an ECS reintroduced the experience of being alone. Being alone provided “space” and privacy in contrast to having constant company.” [Citation29]. Participants using an electric wheelchair reported the electric wheelchair gave them the ability to be away from home by themselves [Citation23,Citation24].
Less reliance on others
Because users of ECS experience that their (physical) reliance on others decreased, the dynamics of the caregiving relationship changed [Citation23,Citation27–29]. Myburg et al. [Citation27] described: “ECS meant ‘less asking’ and could alleviate participants’ sense of ‘being a pain’ to others. Being able to do things without having to ask a carer decreased frustration and improved participants’ sense of wellbeing.”. Participants reported less apologizing, feeling less frustrated, and reduced annoyance [Citation23,Citation29]. Participants experienced increased freedom, often not only because they themselves feel more independent, but more importantly because using ECS lifted the caregiver from some of their responsibilities [Citation23,Citation27]. The independence and freedom because of using ECS broke the cycle of worry they both experienced: “Caregivers and family members worried about the person with a [physical disability] who in turn was often worried about the caregiver worrying about them.” [Citation23]
Participation
ALT enabled participants to actively participate in their family or community by picking up life roles, such as family member, friend, student, volunteer, and worker [Citation23,Citation26]. ECS and mainstream devices helped them to complete tasks needed for those roles, such as using the computer to arrange the family’s money matters as father or partner [Citation25]. Some participants indicated that using ECS enabled them to contribute to their family or community, which they valued as the most important impact of ALT on their personal lives [Citation27]. Also, using ECS and mainstream devices gave participants the opportunity to (re)connect with friends and family and connect with the outside world [Citation26,Citation28].
Discussion
This review focused on the impact of ALT on independence experienced by people with a physical disability receiving long-term care. We found eligible articles that demonstrated ALT increases their independence, regarding the execution of ADL as well as their perceived independence.
Most studies only briefly mentioned examples of ADL as their main focus was on the impact of ALT on perceived independence of participants in daily life, which could apply to diverse ADL. We established six themes regarding the impact of ALT on perceived independence, being 1) feeling enabled, 2) choice and control, 3) feeling secure, 4) time alone, 5) improved relationship with caregiver, and 6) participation. These results fit the four types of autonomy/independence defined by Van de Ven et al. [Citation32]. The first type they describe is independence in daily life, or executional autonomy. In our study, this is represented by the ADL activities participants could carry out because of the ALT they used. The second type is self-determination, or decisional autonomy. In our review, we found that choice and control was a reoccurring theme in almost all included studies. Participants indicated that they experienced more freedom to make choices and an increased sense of control as a result of using ALT. Closely linked to this, they experienced more space and privacy because ALT enabled them to spend time alone without the presence of a caregiver. The third type van de Ven et al. describe is participation: “the organising of one’s own social roles, affairs, and relationships” [Citation32, p. 250]. We found that because of ALT, participants experienced less reliance on others and more freedom and improved dynamics within their relationship with caregivers. Also, they felt enabled to contribute within their families and communities and connect with others. The fourth type is identification: “the degree to which individuals feel comfortable with their way of living and feel that their way of living befits the person they are” [Citation32, p. 250]. In the studies included in this review, this level of independence was not discussed extensively. However, participants mentioned that because of ALT, they were able to pick up preferred life roles that they were previously not able to perform (anymore) due to their disability.
As such, the results of this review reflect that independence is not limited to just performing ADL, but also impacts more profound aspects of perceived independence which are more related to autonomy and self-esteem.
With our search strategy we found many studies evaluating technology in the development phase. Existing articles about these technologies focus on the functioning of the technology instead of its effects on the user. These technologies are promising for the independence of people with physical disabilities, but not yet used by them in the real-life daily living environments. Examples of such technologies are a rotating spoon to support self-feeding for people with upper limb dysfunction and several robots, robot arms or wearables, to perform ADL such as shaving, brushing, feeding or drinking for people with SCI or other physical disabilities [Citation33–36]. There is a lack of studies that go beyond this development phase and research the effect of the technology for end users.
We were able to include just nine studies in our review. These studies were of good quality, but researched small samples, with a mean of ten participants, and were quite one-sided as most studies used qualitative methodology and examined similar samples (mostly participants with SCI) and technologies. Four of the nine of the studies we found were performed by the same authors for the same type of technology (ECS) in people with the same physical disability (SCI) [Citation23,Citation27–29]. Three of those studies were performed in the same country (Australia) [Citation27–29]. Most studies researched technologies that were already in use by people with a physical disability. However, two studies monitored the experience of people who tested ALT for the sake of their study and did not use it before [Citation30,Citation31] and one study followed people who started using ALT and received training to do so [Citation25].
In conclusion, this topic seems to be an emerging branch of research. However, in practice, ALT is implemented and needed in many long-term care organisations in response to societal developments and challenges such as the increasing costs of care and shortages of healthcare professionals and the focus on independence of people with a physical disability [Citation37]. Solutions such as technology are essential to maintain care for people with (physical) disabilities in the coming years. There is a need for studies that highlight the value of ALT in order for governments to be more willing to invest in and shape ALT markets [Citation38]. Therefore, further published research on pilots and preferably larger studies should report on cost-effectiveness of specific ALTs and how to properly implement these technologies within the care process. That way, care organisations will be in the position to learn from each other and make more considered choices to use technology rather than having to “invent the wheel” themselves over and over again.
Appendix_I__online_._Search_strategies_for_online_databases_Medline__Embase__and_Web_of_Science.docx
Download MS Word (23.4 KB)Acknowledgements
The authors thank Rikie Deurenberg for her assistence with the search strategy and Hendrik Buimer for his feedback during the writing of this paper.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- United Nations [Convention]. Convention on the Rights of Persons with Disabilities. 2006. https://www.un.org/esa/socdev/enable/rights/convtexte.htm.
- Ells C. Lessons about autonomy from the experience of disability. Soc Theory Pract. 2001;27(4):599–615.
- Andrade VS, Faleiros F, Balestrero LM, et al. Social participation and personal autonomy of individuals with spinal cord injury. Rev Bras Enferm. 2019;72(1):241–247.
- McDougall J, Baldwin P, Evans J, et al. Quality of life and self-determination: youth with chronic health conditions make the connection. Appl Res Qual Life. 2016;11(2):571–599.
- Nota L, Soresi S, Ferrari L, et al. A multivariate analysis of the self-determination of adolescents. J Happiness Stud. 2011;12(2):245–266.
- Sandjojo J, Zedlitz A, Gebhardt WA, et al. Training staff to promote self-management in people with intellectual disabilities. J Appl Res Intellect Disabil. 2018;31(5):840–850.
- Reindal SM. Independence, dependence, interdependence: some reflections on the subject and personal autonomy. Disabil Soc. 1999;14(3):353–367.
- Forber-Pratt AJ. (Re)defining disability culture: perspectives from the americans with disabilities act generation. Cult Psychol. 2019;25(2):241–256.
- Khasnabis C, Mirza Z, MacLachlan M. Opening the GATE to inclusion for people with disabilities. Lancet. 2015;386(10010):2229–2230.
- WHO. Assistive technology; 2018. https://www.who.int/news-room/fact-sheets/detail/assistive-technology
- Gentry T. Smart homes for people with neurological disability: state of the art. NeuroRehabilitation. 2009;25(3):209–217.
- Krantz O. Social construction of technical Aids-Personal meaning and interactional effects of disability and assistive devices in everyday life [thesis]. Lund: Lund University; 2009.
- Brose SW, Weber DJ, Salatin BA, et al. The role of assistive robotics in the lives of persons with disability. Am J Phys Med Rehabil. 2010;89(6):509–521.
- Song Y, van der Cammen TJM. Electronic assistive technology for community-dwelling solo-living older adults: a systematic review. Maturitas. 2019;125:50–56.
- Daly Lynn J, Rondón-Sulbarán J, Quinn E, et al. A systematic review of electronic assistive technology within supporting living environments for people with dementia. Dementia. 2019;18(7-8):2371–2435.
- Wang T, Zhang B, Liu C, et al. A review on the rehabilitation exoskeletons for the lower limbs of the elderly and the disabled. Electronics. 2022;11(3):388.
- Khalid S, Alnajjar F, Gochoo M, et al. Robotic assistive and rehabilitation devices leading to motor recovery in upper limb: a systematic review. Disabil Rehabil Assist Technol. 2021;16:1–15.
- Page JM, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. 2021;10(1):1–11.
- CASP Programme [Internet]. 10 questions to help you make sense of qualitative research; 2006. https://casp-uk.net/wp-content/uploads/2018/03/CASP-Qualitative-Checklist-2018_fillable_form.pdf.
- Pace R, Pluye P, Bartlett G, et al. Testing the reliability and efficiency of the pilot mixed methods appraisal tool (MMAT) for systematic mixed studies review. Int J Nurs Stud. 2012;49(1):47–53.
- Boeije HR, van Wesel F, Alisic E. Making a difference: towards a method for weighing the evidence in a qualitative synthesis. J Eval Clin Pract. 2011;17(4):657–663.
- Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. 2008;8:45.
- Verdonck MC, Chard G, Nolan M. Electronic aids to daily living: be able to do what you want. Disabil Rehabil Assist Technol. 2011;6(3):268–281.
- Blach Rossen C, Sørensen B, Würtz Jochumsen B, et al. Everyday life for users of electric wheelchairs–a qualitative interview study. Disabil Rehabil Assist Technol. 2012;7(5):399–407.
- Folan A, Barclay L, Cooper C, et al. Exploring the experience of clients with tetraplegia utilizing assistive technology for computer access. Disabil Rehabil Assist Technol. 2015;10(1):46–52.
- Jamwal R, Callaway L, Ackerl J, et al. Electronic assistive technology used by people with acquired brain injury in shared supported accommodation: implications for occupational therapy. Br J Occup Ther. 2017;80(2):89–98.
- Myburg M, Allan E, Nalder E, et al. Environmental control systems - the experiences of people with spinal cord injury and the implications for prescribers. Disabil Rehabil Assist Technol. 2017;12(2):128–136.
- Hooper B, Verdonck M, Amsters D, et al. Smart-device environmental control systems: experiences of people with cervical spinal cord injuries. Disabil Rehabil Assist Technol. 2018;13(8):724–730.
- Verdonck M, Nolan M, Chard G. Taking back a little of what you have lost: the meaning of using an environmental control system (ECS) for people with high cervical spinal cord injury. Disabil Rehabil Assist Technol. 2018;13(8):785–790.
- Wästlund E, Sponseller K, Pettersson O, et al. Evaluating gaze-driven power wheelchair with navigation support for persons with disabilities. J Rehabil Res Dev. 2015;52(7):815–826.
- Bona S, Donvito G, Cozza F, et al. The development of an augmented reality device for the autonomous management of the electric bed and the electric wheelchair for patients with amyotrophic lateral sclerosis: a pilot study. Disabil Rehabil Assist Technol. 2021;16(5):513–519.
- Van De Ven L, Post M, De Witte L, et al. Strategies for autonomy used by people with cervical spinal cord injury: a qualitative study. Disabil Rehabil. 2008;30(4):249–260.
- Sun JX, Li LF, Zhao YL, et al. CONSORT-Assistive technology-180 degrees rotating eating spoon improves the ability of eating of self-care patients with upper extremity dyskinesia: rotating eating spoon improves eating ability. Medicine. 2019;98(9):e14597.
- Ajani OS, Assal SF. Development of an autonomous robotic system for beard shaving assistance of disabled people based on an adaptive force tracking impedance control. J Mech Eng Sci. 2021;235(21):5758–5775.
- Kronhardt K, Rübner S, Pascher M, et al. Adapt or perish? Exploring the effectiveness of adaptive DoF control interaction methods for assistive robot arms. Technologies. 2022;10(1):30.
- Kang BB, Choi H, Lee H, et al. Exo-Glove poly II: a Polymer-Based soft wearable robot for the hand with a Tendon-Driven actuation system. Soft Robot. 2019;6(2):214–227.
- Dieleman JL, Squires E, Bui AL, et al. Factors associated with increases in US health care spending, 1996-2013. J Am Med Assoc. 2017;318(17):1668–1678.
- Albala SA, Kasteng F, Eide AH, et al. Scoping review of economic evaluations of assistive technology globally. Assist Technol. 2021;33(sup1):50–67.