
Abstract
Purpose
To explore accessibility challenges encountered by smartphone users with cervical spinal cord injuries (C1-C8). To investigate the suitability of current technology and make recommendations to help future technology meet user needs.
Methods
The study uses a mixed-method approach combining an inductive thematic analysis of nine semi-structured interviews with a quantitative analysis of thirty-nine questionnaires.
Results
The analysis generated four themes: 'the drive for independence and self-efficacy'; 'trying to make it work'; 'getting the right technology for me'; 'using the phone as and when I want to'. These themes highlighted how unresolved access issues and situational barriers limited independence and created unwanted privacy compromises for effective communication. There was a lack of information or support on available smartphone accessibility features and assistive technology (AT). Smartphone AT was regarded as overpriced, poorly designed and lacking the voices of people with disabilities.
Conclusions
The smartphone’s potential to improve quality of life, participation, and well-being is limited by accessibility challenges hindering independent and private smartphone use. Future design work should focus on improving accessibility, investigating reasons for AT's poor quality and high cost, and removing barriers to end-user inclusion. To enhance user awareness of available technology, stakeholders should build and maintain an open platform to act as an information source for peer and professional support on assistive technology.
IMPLICATIONS FOR REHABILITATION
A smartphone’s potential to empower, connect, and improve the quality of life of people with a cervical spinal cord injury (SCI) is limited by unresolved accessibility barriers, causing isolation.
Standard interaction methods used by people with a cervical SCI to mitigate smartphone access barriers can require unwanted privacy compromises and limit independence.
Participants struggled to find information and support on available accessibility solutions and assistive technologies that might enable easier smartphone use.
Participants rarely used assistive technology (AT) to facilitate smartphone use, and available AT was regarded as expensive and poorly designed.
Introduction
The World Health Organization (WHO) estimates between 250,000 and 500,000 people globally are diagnosed with a spinal cord injury (SCI) each year [Citation1]. SCIs can result in various types of impairment depending on the level and severity of the injury. Alongside physical disabilities, people with SCIs often face challenges with successful community involvement [Citation2], barriers related to employment [Citation3], social engagement [Citation4], and the ability to lead an active lifestyle [Citation5]. A review paper by Hammel [Citation6] found positive correlations between Quality of Life (QoL) and self-assessed health, social support and participation, relationships, autonomy, and employment. Thereby indicating social disadvantage negatively influences QoL after an SCI rather than injury characteristics such as level of injury.
Technology can improve the Quality of Life (QoL) of people with disabilities by addressing factors Hammell [Citation6] found to influence QoL scores, enabling participation in society by facilitating access to education and healthcare and assisting communication with others [Citation7–11]. A smartphone could help users with a cervical SCI participate in everyday indoor and outdoor activities [Citation12], control their environment (environmental control system) [Citation13] and access the internet [Citation14]. The potential of smartphones to enable independent participation gives rise to a vitally important sense of self-efficacy and personal autonomy for people with cervical SCIs [Citation15]. Thereby helping avoid the embarrassment associated with dependence on others while inducing feelings of safety, security, competence, confidence, and control [Citation10].
Unfortunately, while the potential benefits are evident, smartphone users with a cervical SCI often struggle to use their devices effectively. Phone ownership rates of 33.3% C1–C4 (n = 42) and 47.7% (n = 75) C5–C8 (complete) are in stark contrast to ownership rates of the general population of 95% [Citation16]. Such a disparity could arise from the expenses associated with smartphones and assistive technology and the higher living costs of people with an SCI [Citation17,Citation18]. These values contrast the comparatively high cervical SCI ownership rates of computers, 92.9% C1–C4, and 89.2% C5–C8 (complete) [Citation16]. The preference for computers indicates a discrepancy in accessibility, potentially because of a lack of assistive technology, support, or physical factors which increase smartphone interaction difficulties [Citation19–21]. To improve accessibility, users with cervical SCIs may benefit from assistive technology (AT), which has been shown to improve QoL when used for computer [Citation22–24] and mobile phone [Citation9] access. The study uses the UK Medicines and Healthcare products Regulatory Agency (MHRA) definition of assistive technology: a specific product or system designed to support and help individuals with disabilities perform a function that might otherwise be difficult or impossible [Citation25]. However, our definition does not include features included as standard in smartphone operating systems, such as assistive touch.
Improvements in smartphone accessibility have come incrementally from in-built accessibility features and assistive technology. These adaptations assist both users with disabilities and the general population, making them accessible to all [Citation20]. By taking an inclusive design approach – developing products and services to meet the needs of the whole population and lessening capability demand - they can expand the target user group [Citation26]. Smartphone manufacturers have embraced this approach by improving switch access, voice-to-text, text-to-speech, and voice access technology [Citation27–29]. However, these developments may not help those with more complex needs.
Research and development (R&D) in this field is gaining traction, although it is often expensive and poorly supported. Research has been conducted into access methods designed to interact with smartphones or computers, incorporating users’ functional abilities, e.g. using their tongue [Citation9,Citation30], lips [Citation31], and electromyography (EMG) [Citation32]. However, high-tech solutions rarely become commercially available for use with smartphones. While AT can allow people with disabilities to present themselves as befitting their values, AT can mark a user as ‘different’ or ‘lacking’ and thereby act as a barrier to achieving and presenting their preferred self [Citation10]. Consequently, users can reject AT outright, even though it may enhance functional capabilities.
This study contributes to the literature by striving to understand the causes of the disability phone-use gap, which suggests smartphones do not meet the needs of many people with a cervical SCI. Using a mixed-methods approach, we aim to understand the user experience, trends, challenges, and motivations through a qualitative thematic analysis of semi-structured interviews and a quantitative survey of smartphone and AT use () to answer the research questions below. We focus on cervical-level injuries (C1-C8), which involve complete or incomplete paralysis of sensory and motor function below the injury site [Citation33], as at this level gross and fine upper-limb function is affected, which is crucial for interacting with smartphone touch screens. The quantitative analysis distinguishes between injuries at high cervical level (C1-C4) and those at low cervical level (C5-C8) (, ), as complete injuries above C4 would result in complete paralysis of upper limbs.
Figure 1. Diagram of the study’s mixed-methods convergent, parallel databases design.
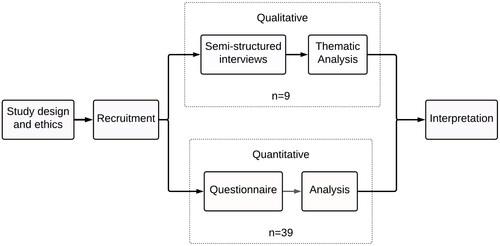
Figure 2. The study's thematic analysis plan. Adapted from the 6-phase approach to thematic analysis Braun & Clarke [Citation42,Citation43].
![Figure 2. The study's thematic analysis plan. Adapted from the 6-phase approach to thematic analysis Braun & Clarke [Citation42,Citation43].](/cms/asset/ec584ba9-c38a-42db-b014-b47ca154f6b5/iidt_a_2192246_f0002_c.jpg)
Study research questions (RQs)
The study’s overarching aim is to improve understanding of smartphone accessibility so future technology can better meet the needs of people with cervical SCIs. To achieve this we use three RQs adapted from the aims of qualitative HCI studies proposed by Blandford et al. [Citation44]:
RQ1: What effect do smartphones have on people with a cervical SCI, and how do smartphones integrate into their lives?
RQ2: How well do smartphones work for people with cervical SCIs, and what are the pressing practical problems?
RQ3: How well do smartphones meet the needs of people with cervical SCIs?
Methods
Study design
The study combined independent quantitative and qualitative analysis using a mixed-methods, convergent, parallel database design () and a pragmatist research paradigm [Citation34]. The inductive thematic analysis was conducted from an interpretivist perspective, while the statistical analysis of questionnaire data used a positivist approach. This combination of rich descriptive data from the thematic analysis and statistical data from the questionnaires allowed data interpretation from several different perspectives and provided a more comprehensive account with possibilities for triangulation [Citation35], adding credibility and allowing an in-depth insight into smartphone usability issues for people with cervical SCIs.
Ethics and data protection
The study participants were adults with no known cognitive impairments, and each gave informed consent. The study was approved on 01/02/2021 by University College London (UCL) Research Ethics Committee, Project ID: 6860/013 and registered with UCL Data protection (Z6364106 2020 11 89). The data was anonymised, and interview recordings were deleted after transcription and a familiarisation period.
Recruitment
Participants were recruited for the interview and questionnaire independently and simultaneously with the same inclusion criteria (). Due to anonymity, participation in both activities was impossible to record, though not restricted. Adverts were posted on social media platforms (Facebook, Twitter, Instagram, Reddit, and LinkedIn) in partnership with relevant charities and organisations. The study had a dedicated website with participant information sheets, consent forms, and researcher contact details.
Table 1. Inclusion criteria and study incentives.
The semi-structured interviews had a target sample size of ≥6 and ≤12, determined through a literature review [Citation36,Citation37]. The target number of questionnaire respondents was 100, derived by estimating a population > 100,000 with a 95% confidence interval and a 10% margin of error set by Yamane [Citation38]. We met our interview target with 9 participants; however, due to difficulties in recruiting participants with a cervical SCI and time constraints, we stopped recruiting at 39 questionnaire respondents.
Demographics
Demographics were taken at the start of the questionnaire and asked verbally before the interviews. Questionnaire data were collected on age, gender, SCI level, living situation, domicile country, SCI type (complete/incomplete), time since injury, and phone make and model. The interviewers asked participants for their age, gender, SCI level, SCI type, The American Spinal Injury Association Impairment Scale (AIS), and phone make and model.
Thematic analysis of semi-structured interviews
Nine participants took part in semi-structured interviews conducted remotely using Microsoft Teams due to Covid-19 restrictions. Two interviewers conducted each interview using a pre-prepared guide, which was tested before use, and the completed interviews were transcribed professionally (full verbatim). Verbal consent was obtained at the start of each interview, and participants had the opportunity to ask questions. The interviewers asked non-leading questions, actively listened, left silence, and encouraged elaboration [Citation39–41].
Analysis
The thematic analysis was inductive and data-driven, following the 6-steps described by Braun & Clarke [Citation42,Citation43]. This interpretivist method assumes a subjective reality constructed through participant and researchers’ interpretations [Citation44]; it is flexible and not reliant on theory [Citation39]. The process was non-linear, with reflection, debriefing, and review sessions after each phase to discuss progress, possible bias, and patterns in the data. One researcher coded the interviews semantically, including latent coding where possible, based on the research questions and generated a set of initial themes based on the codes. A second researcher familiarised themselves with the interviews so they could collaborate in six peer debriefing and theme review sessions. NVivo 12 was used for coding without corpus tools for prior lexical analysis, and DrawIO software was used to create thematic maps for reflection, debriefing, and theme review sessions ().
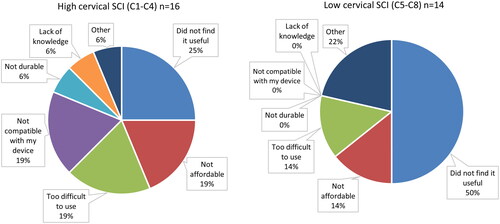
Figure 3. Reasons for abandoning Assistive Technology (AT) high cervical, C1-C4 (left) and low cervical, C5-C8 (right) SCI. Blank or N/A respondents were removed.
Steps were taken to meet the trustworthiness criteria [Citation45,Citation46]: Storing auditable notes, including reflections on the interviews, methodological decisions, and analysis. Peer debriefing sessions involved the researchers, a professor specialising in assistive technology, and a PhD student with experience in qualitative analysis. One of the interviewers had clinical experience working with AT for people with disabilities.
Quantitative analysis of questionnaire
Over two months thirty-nine participants took part in an online questionnaire using Microsoft Forms. Responses were anonymous, participants could skip questions, and drop-down menus were used for multiple-choice questions. Demographics and health information were collected alongside data on current assistive technology and smartphone use and level of satisfaction. Responses were anonymous, participants could skip questions, and drop-down menus were used for multiple-choice questions. To improve questionnaire usability, we used predetermined selectable categories for all questions. These categories were created by researching smartphone, tablet, and computer accessibility studies for people with upper limb impairments [Citation9,Citation12,Citation47], then adjusted to suit current technology and help answer the research questions.
Data analysis of questionnaire
Self-reported upper-limb mobility, sense of touch, and grip strength as a 5-point Likert scale (1= very poor, 5= very good). Five-point Likert scales were also employed to measure opinions on AT used to access smartphones (opinion scores: satisfaction, ease of use, agreement that “AT provided a greater sense of independence.”) as well as usage scores (frequency of AT use). The data were analysed with descriptive and inferential statistics using SPSSFootnote1 and MatlabFootnote2.
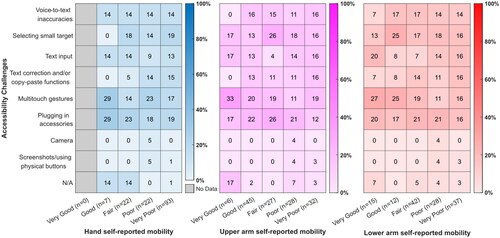
There may be a high variability between participants with an incomplete injury which may distort or skew participant data for different injury levels. So, we used a Somer’s d trend analysis to determine whether injury could be accurately characterised by self-reported upper limb mobility and grip strength scores without controlling for completeness of injury (). As a linear trend was found for each case, we separated smartphone accessibility challenges and smartphone interaction methods selected by these self-reported values ( and ). Cochran-Armitage tests of trend were then performed to investigate whether linear trends existed between upper limb mobility ratings and the ability to send and receive texts and calls or use the internet.
Figure 4. Smartphone interaction methods separated by self-reported upper-limb mobility. As the question allowed for multiple selections, n is the total number of selections by self-reported mobility category, and values denote % of selections for each interaction method.
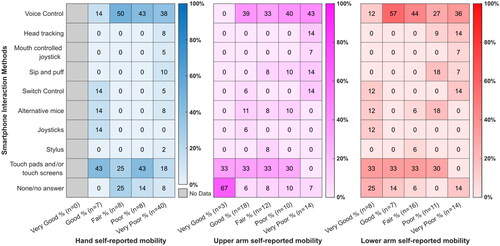
Figure 5. Smartphone accessibility challenges separated by self-reported upper-limb mobility. As the question allowed for multiple selections, n is the total number of selections by self-reported mobility category, and values denote % of selections for each accessibility challenge.
Results
Qualitative thematic analysis (n = 9) results are presented first, followed by quantitative study (n = 39) results () with participant demographics set out in and , respectively.
Table 2. Qualitative study participant demographics (n = 9).
Table 3. Quantitative study participant demographics (n = 39).
Table 4. Somer’s delta trend analysis to determine whether functional ability scores can characterise injury without splitting by complete or incomplete.
Thematic analysis
We generated four themes describing the qualitative study participant’s user experience (demographics detailed in ). Some felt their smartphone was a “lifeline” (P1, P3) and a “life-changing” piece of technology (P6), with “emotional value” (P1) used for a variety of purposes in both work and social contexts (P4, P6, P8), a source of “escapism”, “companionship”, or something providing “security” (P1, P3) thereby allowing more freedom and independence. This perceived value heightens both successes and failures when using a smartphone.
Theme 1: The drive for independence and self-efficacy
Independence was “core” aspect of P9’s identity before his cervical SCI. Transitioning from independence to dependence on others was challenging for many participants (P4, P7, P9) “The most difficult part for me after the accident wasn’t the fact that I could not walk, run or use the bike anymore…, it was the fact that I had to rely on other people for help” (P9). “I can see it there, and I just can’t physically get my hand to the position to get it…. You get thoroughly miserable just having to ask them (carers) to reach forward” (P7). Successful smartphone use gave some participants a sense of autonomy and connection to the outside world (P1, P3, P9). A few participants described how their phones had added importance during rehab, as it was an intense experience punctuated with loneliness and boredom (P1, P8). This meant learning to use a phone while in hospital was a priority for one participant following his injury, and how independently using this technology at an early stage was motivating “It did help to the extent that I could actually do things for myself even at that early stage… A sense of achievement” (P8). Participants regarded their smartphone as life-changing, “Before I was not able to write anything down, physically myself. Now I can tap on an app, open up notes, type in what I need.” (P6) and a source of encouragementdue to the potential for autonomy. “What encouraged me? Realising that I could actually do something with my hands and that I didn’t need to call somebody else to do it for me.” (P6).
The inability to use their phones independently had consequences for other participants. Often it would mean relying on the technical skills of the carers or personal assistants (P1, P4, P7) and a loss of privacy when composing messages (P2, P4, P7, P5). One participant described their sense of “isolation” (P1) when an unreliable nursing team did not help him use his phone during rehabilitation.
All participants devised solutions to improve their smartphone use, from using their noses to activate a camera (P3) to creating a Velcro hand strap to enable outside use (P9). They spoke proudly of their successes, indicating the importance of self-efficacy. These solutions were driven by “need” and “necessity” (P2) or “for my little bit of independence” (P6). The technological solutions devised for environmental control further indicate a drive for independence. Some participants used specially designed smartphone apps as a control system (P1, P9). In contrast, others (P2, P4) described a preference for mainstream solutions such as AlexaFootnote3 due to its relative ease of use “I’ve got some of the lights working through Alexa, and again, just the fact that it’s voice-activated” (P4).
Theme 2: Trying to make it work
Differing views were expressed on phone interaction methods. All participants used direct access and voice control, individually or in combination. However, they were rarely satisfied with their chosen method. One individual explained his difficulties writing with voice dictation, describing “silly errors” (P1) or false interpretations, while another blamed technology (P7) “It doesn’t pick you up, or it misses bits. It’s not like I'm slurring my words or anything” (P3). Despite these issues, they spoke of the merits of using voice to control their phones as “a real game-changer” (P1). Some participants felt uncomfortable speaking their messages aloud, feeling it infringed their privacy (P2, P3, P4). Others distrusted speech recognition technology (P3, P8, P5). P1 and P5 wanted voice control to do more; seeing its merits even though it proved unusable for them, “using a kindle at night so I could say just turn the page over, would be fantastic” (P5).
Participants not using voice control could directly access their phones via the touch screen. However, those with poor hand function felt frustrated by this process “It’s just ten times easier replying to an email via voice than it is typing it in because it takes bloody ages.” (P3). Physical characteristics, such as screen size, influenced access possibilities and could determine a device’s usefulness for certain activities “it’s much easier for me to use for swiping and texting” (P1), sometimes the determining factor for independent access (P4). Some participants adopted a flexible approach, such as tapping to navigate and incorporating voice recognition to compose messages (P9). Switching between methods could be due to fatigue and variability in hand function. “I use the voice function more when I'm tired or my hands are hurting” (P1).
Participants had different strategies to stabilise their phones. Many participants used a stand (P2, P4, P5, P6, P8), rested their phones on a table (P8), or used their bodies (legs, laps, stomachs). Some made adaptations (P9, P6). A stable position could liberate their hands, and the addition of a speakerphone meant they could use their wheelchair or perform other tasks requiring hand function. Some participants could not sufficiently grip and therefore access their phone (P1, P2, P3), often due to the changes in or loss of tactile sensation. However, simple rubber covers offered greater friction and tactile feedback, making a “massive difference” (P2). P1 incorporated his permanent hand flexion as a natural phone grip posture. In contrast, others found their fingers got in the way, hindering their use “they’re literally covering about half of the screen” (P7).
Many of the phone’s functions required two hands “you don’t realise how many two-handed operations you do with your phone” (P3), indicating frustration at a lack of awareness of users unable to use both hands. In this instance, P3 always needed one hand to support their balance and posture, leaving only one hand free to use their phone. Some participants were resigned to struggling to use their phones. “It is what it is. There’s nothing I could immediately do to change the situation. So, I just have to live with it.” (P5).
Theme 3: Getting the right technology for me
Nearly all our participants described difficulties in finding suitable technology and accessibility features “I think the biggest problem is the lack of knowledge” (P4), “I just didn’t know there was any more stuff out there” (P7). They felt they needed a central location “one-stop-shop” to buy and learn about technology (P1, P2, P4, P5, P8). This lack of available information caused one participant to stop searching “I didn’t know there was anything left… anything more a smartphone could do” (P7), affecting their motivation to use their phones fully. Some participants suggested that only people with similar disabilities would “fully understand” their needs (P1, P8).
Participants reported dissatisfaction with the poor design and high cost of what they considered AT. One described AT as “not very well designed for anyone really, non-disabled, paras, but particularly tetras” (P8), and he felt “the voices of disabled people” (P8) were absent from the design of smartphone technology. Another felt the price of AT to was “astronomical” (P6), while another explained that “disabled people have more financial problems than non-disabled people” (P8). This resulted in financial compromises to pay for their technology “I won’t be able to afford a pizza this month because I’m saving for the phone next month” (P9).
Smartphones were integrated into a system of interconnected devices, where individuals could choose their preferred device for a given situation. One participant described setting up his devices as “part of getting dressed in the morning, put the tray on and it’s all on there.” (P5), showing its value alongside his activities of daily living. This interconnectivity allowed deficiency in their phones, such as a small screen, to be mitigated by a different device, e.g. screen sharing to a television, connecting to a stereo system of a car (P7, P2), or linking an Alexa to a phone to make a call (P6). The level and ease of interconnectedness were reasons for buying a particular smartphone: someone with an iPad or iWatch would have an iPhone, which was also true for Samsung devices. Brand loyalty with devices from the same manufacturer went “hand-in-hand” (P4).
Theme 4: Using the phone as and when I want to
Many participants admitted they could not access their phone as they wished “I find it really difficult to use it anywhere” (P7). They described the difficulties of using their phones on the move, such as in a moving car or wheelchair (P7). All participants described dropping their phones as a persistent issue, resulting in a feeling of powerlessness at being unable to resolve the issue themselves (P2, P3, P6, P8). They accepted this situation as a fact and out of their control. “if it happens, it just becomes the next problem” (P2). Another issue was fear of theft when on display (P6, P7), “If it was permanently on a stand, I don’t know how confident I would be to have it out in public the whole time.” (P4), which resulted in them not using technology designed to aid one-handed use, such as a stand. These issues meant participants stored their phones away in their bags or pockets, and upper-limb functional mobility problems meant they struggled to retrieve them when needed (P2, P1, P7).
These factors limited the situations where they could use their smartphones and sometimes opportunities to participate (P2). Participants missed calls, “it’ll ring out; guaranteed that I’ll end up missing the message” (P4), and there was a sense of missing out “I’m not very good at sporting events. The goal’s been scored by the time I’ve got my phone out” (P2). To overcome this, some participants developed strategies for outside phone use, such as connecting it with their “iWatch” (P1, P9), attaching it to their wrist using a self-made strap (P6, P9) or even “wearing a larger pair of jeans” (P1).
Participants were forced to make unwanted compromises while using their phones. One participant had to shorten their communication style due to difficulty writing messages (P3). Others avoided using voice dictation to write messages due to privacy concerns about being overheard. Instead, they used the touch screen, which they perceived as less reliable (P2, P3). P7 felt obligated to use voice recognition despite their security concerns “I just don’t trust them… but it’s getting to the point where I might have to start using them.” (P7).
Questionnaire analysis
We received 46 survey responses. However, four were discarded for breach of inclusion criteria. An inspection of data revealed inconsistencies in the answers of three participants (two with complete C4 injuries and one with an incomplete C2 injury), leaving 39 participants (demographics described in ).
Descriptive statistics
Inferential statistics on questionnaire responses
Using a Cochran-Armitage test of trend we found lower self-reported mobility ratings for upper and lower arm and grip strength were associated with a higher proportion of participants who could not make or receive calls (p < 0.05). However, sending and receiving texts, or browsing the internet, had no associated linear trend with any function scores. Additionally, there was a statistically significant positive correlation between the number of assistive technology solutions previously tried and level of satisfaction with current solutions (d = 0.274, p < 0.05). We found a linear trend with a statistically significant positive correlation between an agreement that assistive technology facilitated independence and the frequency AT was used for smartphone access (d = 0.514, p < 0.05). Participants whose choice of smartphone was not influenced by assistive technologies’ availability or compatibility reported lower levels of satisfaction (p < 0.05) and used AT less frequently (p < 0.05) and with greater difficulty (p < 0.05).
Discussion
We aimed to identify how smartphones can better meet the needs of people with a cervical SCI. This analysis highlights the diversity of opinions, methods, and solutions, suggesting there is not a one-size-fits-all approach to smartphone usability. The findings are presented below in answer to the research questions.
RQ1: What effect do smartphones have on people with a cervical SCI, and how do smartphones integrate into their lives?
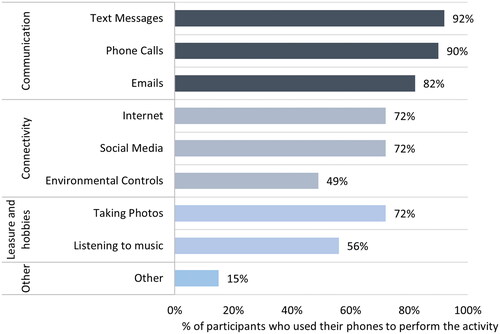
Participants considered their smartphone to be an integral part of daily life (theme 1) and “part of their getting dressed routine” (theme 3), linking to McRae et al. [Citation15], who stated: “smartphones can be seen as an extension of the disabled body”. Communication and connectivity were the most prevalent phone use (), as they others provided a feeling of safety and confidence and allowed contact in case of emergency, thereby facilitating greater independence, e.g. driving independently or going out on a recumbent bike (theme 1) [Citation10,Citation12,Citation15]. Phones allowed users to work remotely, sidestepping transportation requirements - the largest barrier to returning to work found by Lidal et al. [Citation3]. A smartphone’s potential to improve quality of life [Citation6] by providing a sense of autonomy and motivation through independent use [Citation8, Citation9] and enabling participation in social and professional contexts had a considerable impact. These findings suggest successful smartphone use can help overcome challenges preventing community involvement [Citation2] and help meet the priorities set out by Simpson et al. [Citation64].
Figure 6. Activities performed on a smartphone by questionnaire study participants.
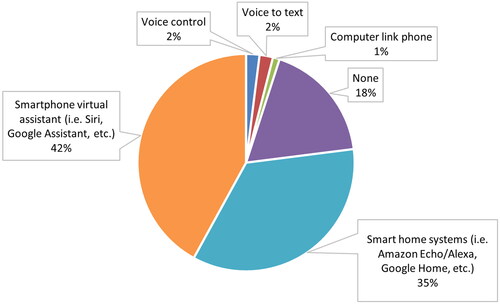
Participants integrated their phones into systems of compatible technology, giving an added layer of security in case of a device failure and allowing for a device’s limitations to be compensated by another device in the system. For example more reliable voice-activated calling could be initiated by connecting a smartphone to an Alexa-enabled device or using a tablet with a more accessible larger screen to send WhatsApp messages [Citation48]. Many interview participants positively described their environmental control systems, with 35% of questionnaire participants integrating their phones with a smart-home system ().
Figure 7. Hands-free technology used to help smartphone access n = 68 (multiple selection).
Device compatibility was a factor in smartphone brand choice (theme 3). Participants often connected multiple products from the same manufacturer, possibly due to reduced learning requirements of similar interfaces and the relative ease of interconnecting these devices. While these systems of devices allowed greater autonomy, added functionality and robustness, they also required technical knowledge and adequate support to set them up. Such requirements risk in-group inequalities due to differences in technical ability, living situation () and the variable quality of available support and care for people with a cervical SCI. In future, it would be valuable to explore the connectivity and interoperability of different brand smartphones with other devices, especially concerning accessibility.
RQ2: How well do smartphones work for people with a cervical SCI, and what are the pressing practical problems?
Participants experienced smartphone accessibility challenges, such as phone stabilisation and positioning; quality of voice activation; the need to use two hands; and the unreliability of directly accessing the touch screen (theme 2). Interestingly the principal device interaction methods used were standard smartphone features, such as voice control or direct touchscreen access, rather than AT (). However, access method preference changed depending on self-reported upper-limb mobility. No participants who self-reported their upper and lower arm mobility as ‘very poor’ used a touch screen. Nevertheless, touchscreens were used by participants self-reporting ‘very poor’ hand mobility and ‘poor’ upper and lower arm mobility (), thereby indicating a desire to use hands where possible, regardless of reliability issues highlighted in theme 2. Even with good self-reported mobility, usability problems arose when interactions required dexterity (), whereas actions achieved through assistive touch (screenshots and taking photos) were less problematic. There was a correlation between lower mobility and grip strength ratings and a decreased likelihood of making and receiving calls (p < 0.05). The phone’s small screen sizes exacerbated these issues, resulting in a conflict between the desire for a more accessible device and portability [Citation12,Citation48,Citation49]. Voice control allowed some users to access their phones without a touchscreen’s dexterity and stabilisation requirements (). However, participants reported frustration due to errors, output inaccuracies, and privacy concerns (theme 2). Additionally, over half of the questionnaire respondents, rated voice-to-text inaccuracies as a challenge. In some cases, dissatisfaction related to these issues led to the abandonment of voice activation technology.
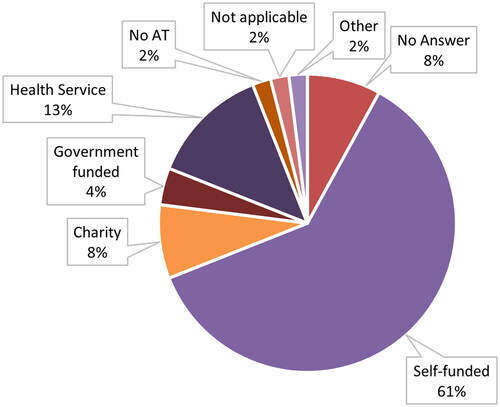
Portability is a core design principle of smartphones; however, situational barriers prevented their use outside. A prominent barrier to outside use stemmed from fears of theft and the risk of it dropping and getting damaged (theme 4). These fears would be made more acute because of the higher living expenses associated with SCIs [Citation50], the high cost of mobile and assistive technology [Citation48], and because technology is predominantly self-funded ( and ). This fear meant participants were reluctant to use visible mounting systems, as they could draw attention to the user’s disability and result in stigma [Citation51], thereby removing one of the key benefits of a smartphone [Citation15] “offer assistance without marking difference”. The lack of a mounting system meant participants needed two hands to use their phones. Therefore, using a touch screen was challenging as one hand was often required for body stabilisation. As a result, users would stow away their phones, countering findings by Naftali & Findlater [Citation12]. In addition, the difficulties retrieving stowed-away phones (from pockets or bags) resulted in missed calls and messages, further limiting efficacy and communication possibilities (theme 4), limiting their phone use. Potential alternative phone access methods such as voice activation or speech-to-text were considered inaccurate and unreliable, and participants were conscious of being overheard in public, which would infringe on their privacy [Citation12,Citation52]. These barriers meant many participants could not effectively use their phones as intended by the manufacturer and they showed a preference for use more accessabile devicesat home, such as a tablet or a smart home device.
RQ3: How well do smartphones meet the needs of people with cervical spinal cord injuries?
Smartphones and available AT fail to meet the needs of people with a cervical SCI in a range of areas: independence (theme 1), autonomy in their smartphone use (theme 1), and privacy in their communication (themes 1 and 4). While many participants were aware of the potential benefits of their phones, they were frustrated by their inability to achieve their ambitions. Access problems meant many participants sacrificed their privacy for phone use (theme 4) [Citation52] or participants were forced to adapt their communication style to shorter, less expressive forms (theme 4),highlighting a forced compromise, sacrificing privacy for a need to communicate. McRae et al. [Citation15] describe a similar sacrifice for people with disabilities - paying for independence with a loss of privacy. These issues are made more salient as people with a disability already feel a loss of privacy, and their sense of autonomy depends on having control over their private information [Citation53,Citation54]. These findings emphasise the need to design technology that facilitates independent and private smartphone use and highlight inequalities in mainstream technology access between users living with a disability and those without a disability, limiting opportunities to improve the well-being of an individual with a cervical SCI.
Participants predominantly relied on standard smartphone technology or built-in accessibility features (), used by non-disabled individuals and those with a disability, over assistive technology (AT). Even though, these modes of interaction were considered unreliable, frustrating, and often a cause of accessibility issues described in theme 2, indicating an underlying problem with available AT. This finding is supported by Kane et al. [Citation52], who found that people with disabilities used mass-market devices over specialised devices even when specialist access methods were available, possibly due to concerns of AT drawing attention to a user’s disability and stigmatisation [Citation10,Citation15]. The few interview participants who used AT had designed it themselves to solve a specific need (theme 1), further indicating a lack of faith in the technology. The sense of pride in this self-sufficiency shows the importance of self-efficacy and its role in motivation and empowerment [Citation55]. However, a situation where users must design their own AT results in further inequalities within the user group as it relies on functional capability, technical ability, and assistance from others. Our questionnaire found 12% of 39 people surveyed lived alone, while Carpenter et al. [Citation2] reported 8% of 357 people with a SCI did not have anyone to rely on for help and living alone made them more likely to be dissatisfied with their support.
A lack of available information and support for AT (highlighted by nearly all interview participants, theme 3) limits its potential benefits [Citation9,Citation23,Citation24,Citation56]. Participants wanted a single, easily accessible information source, a one-stop shop, where individuals with cervical SCIs could explore possible AT and learn about accessibility options (theme 3). They wanted to learn from peer experience and access professional support. Despite a lack of knowledge, there was still an appreciation that AT could be beneficial, and the questionnaire indicated experience using AT could positively impact smartphone use, leading to higher satisfaction (d = 0.274, p < 0.05) and greater autonomy, which would encourage use (d = 0.514, p < 0.05). Therefore users would benefit from testing prospective technology before purchase. It would expedite a trial-and-error process, reduce the risk of buying unsuitable technology (), and allow greater involvement in user decision-making around AT, a factor in abandonment [Citation57].
The current design, quality, cost and support issues highlighted in Theme 3 and indicate underlying problems within the AT ecosystem, which require further exploration. Active participation with end-users and key stakeholders early in the design can help ensure the quality and efficacy of AT [Citation58], improving the cost/benefits of AT and reducing abandonment [Citation57] and the risk of stigma, thereby improving user self-esteem [Citation51].
AT classification depends on manufacturer claims and intended use. If a product is designed to compensate for a specific disability or injury, it can be categorised as a medical device [Citation25], resulting in greater regulatory requirements. These requirements can result in higher development costs, barriers between end-users, designers and researchers, and require a clinical evaluation to prove efficacy [Citation59]. In contrast, products designed for computer access, such as a mouse, keyboard or an accessibility feature, would avoid additional regulation and more easily involve users in the design. Arguably, both AT for computer access and standard computer access devices (such as a mouse or keyboard) perform the same task; only differentiated by the user’s disability. As AT is predominantly self-funded (), end users pick up the extra cost.
Figure 8. AT funding n = 48 (multiple selection).
Relevance for users with other disabilities
The study results are relevant for other disability populations. As in theme 1, studies on other disability populations have also highlighted the importance of smartphone use. Participants who had a stroke showed greater phone use following their injury [Citation60]. In another study, participants saw their phones as a lifeline, enabling a sense of belonging and agency [Citation61]. The issues with smartphone accessibility (theme 2,) described in this study would also be relevant. Another study showed how people with a traumatic brain injury (TBI) struggled to learn how to use their phones [Citation62] and, finally, how caregivers influenced smartphone use for people with cognitive disabilities [Citation63]. This overlap between smartphone accessibility needs of people with cervical SCIs and those with other disabilities further emphasises the importance of making smartphones more accessible and suitable AT more available and appropriate.
Study limitations
Online recruitment and involvement methods meant participants required a degree of technical aptitude and access to social media platforms, the internet, and Microsoft Teams. This possible bias could be reflected in the younger population of interview participants (predominantly 30-39), resulting in the potential under-representation of accessibility issues from older individuals with an SCI. Also, some interview participants were directly involved with SCI charities, supporting others with an SCI, potentially resulting in more knowledge of and exposure to AT than the cervical SCI population. Future studies could include physical posters, flyers and other in-person recruitment measures to mitigate this potential bias.
Further limitations arise from the underpowered nature of the quantitative study, affecting generalisability and restricting possibilities to subdivide data by injury type or AIS. Time since injury was not recorded for interview participants, and neither group undertook a neuropsychological test, which would have been beneficial in understanding user experience. Additionally, the COVID-19 pandemic meant participants spent more time at home and had easier access to their computers and tablets. As a result, mobile phone use was reduced, and some participants had to recall using their phones outside pre-pandemic.
Conclusions and future work
Our results show the importance of smartphones for users with spinal cord injuries and how usability issues restrict the smartphone’s potential to enable participation and improve the quality of life. There was considerable variability between the participants, highlighting the importance of catering to individual needs arising from functional ability, environmental context, care situation, motivations, preferences, and interests. This heterogeneity highlights a need for flexible and adaptable solutions.
New technological developments should focus on enabling independent smartphone interactions for users with upper limb impairments inside and outside the home without compromising privacy and functionality. Users should also be able to set up their phones and necessary AT independently. These changes would reduce the reliance on carers’ technical skills and motivation, a current source of inequality.
While progress has been made, this study indicates a gap between users with disabilities, researchers and manufacturers, resulting in low uptake and a lack of confidence in available assistive technology. Barriers within the AT ecosystem preventing the involvement of users living with a disability early in the research and design process should be investigated. In addition, further research should aim to understand the root of AT’s high cost and the user’s perception of poor, uninformed design.
The lack of support and information on available technology solutions should be addressed by developing and maintaining a platform to allow users with a disability, caregivers and key stakeholders to discover available technology suitable for their specific needs. End users and caregivers could share their experiences and exchange information with professionals or peers. They should have an opportunity to trial equipment before purchase, reducing the risk and cost of purchasing inappropriate technology. Caregivers should be encouraged and supported to improve their technical capabilities and be suitably matched [Citation63] to help meet their client’s technological and care needs. Finally, ongoing technical assistance should be available for end-users and caregivers as the set-up, learning and support of any new technology are crucial to facilitate widespread uptake.
Acknowledgements
We would like to acknowledge the Aspire CREATe Lab for their help in organising the project, the Aspire charity, Andrew Kell, and the Spinal Cord Injury Association (SIA) for highlighting the need for the study and enabling us to reach people with a spinal cord injury; and Cathy Morand for her support, excellent feedback, and advice.
Disclosure statement
The authors declare that they have no known competing financial interests or personal relationships that could have influenced the work reported in this paper.
Additional information
Funding
Notes
1 SPSS version 27 (IBM Corp, 2020)
2 Matlab 2020.
References
- World Health Organization. Spinal cord injury; 2013. November 19 [cited 2021 Nov 27]. Available from https://www.who.int/news-room/fact-sheets/detail/spinal-cord-injury.
- Carpenter C, Forwell SJ, Jongbloed LE, et al. Community participation after spinal cord injury. Arch Phys Med Rehabil. 2007;88(4):427–433.
- Lidal IB, Huynh TK, Biering-Sørensen F. Biering-Sørensen F. Return to work following spinal cord injury: a review. Disabil Rehabil. 2007;29(17):1341–1375.
- Noreau L, Fougeyrollas P. Long-term consequences of spinal cord injury on social participation: the occurrence of handicap situations. Disabil Rehabil. 2000;22:170–180.
- Fernhall BO, Heffernan K, Jae SAEY, et al. Health implications of physical activity in individuals with spinal cord injury: a literature review. J Health Hum Serv Adm. 2008;30:468–502.
- Hammell KW. Exploring quality of life following high spinal cord injury: a review and critique. Spinal Cord. 2004;42(9):491–502.
- Tyagi N, Amar Goel S, Alexander M. Improving quality of life after spinal cord injury in India with telehealth. Spinal Cord Ser Cases. 2019;5(1):1–5.
- Goldner M. Using the internet and email for health purposes: the impact of health status. Social Science Q. 2006;87(3):690–710.
- Kim S, Lee BS, Kim JM. Comparison of the using ability between a smartphone and a conventional mobile phone in people with cervical cord injury. Ann Rehabil Med. 2014;38(2):183–188.
- Lupton D, Seymour W. Technology, selfhood and physical disability. Soc Sci Med. 2000;50(12):1851–1862.
- Shem K, Irgens I, Skelton F, et al. Telerehabilitation in Spinal Cord Injury. Telerehabilitation: principles and Practice 2022. January 1 [cited 2022 October 8]:23–42.
- Naftali M, Findlater L. Accessibility in context: understanding the truly mobile experience of smartphone users with motor impairments In ASSETS14 - Proceedings of the 16th International ACM SIGACCESS Conference on Computers and Accessibility. Association for Computing Machinery, Inc; 2014. p. 209–216.
- Hooper B, Verdonck M, Amsters D, et al. Smart-device environmental control systems: experiences of people with cervical spinal cord injuries. Disabil Rehabil Assist Technol. 2018;13(8):724–730.
- Rigot SK, Worobey LA, Boninger ML, et al. Changes in internet use over time among individuals with traumatic spinal cord injury. Arch Phys Med Rehabil. 2022;103(4):832–839.e2.
- McRae L, Ellis K, Kent M, et al. Privacy and the ethics of disability research: changing perceptions of privacy and smartphone use. Second international handbook of internet research. Dordrecht: Springer; 2020. p. 413–429.
- Williams T. Percentage of households with durable goods: Table A45 - Office for National Statistics. Office for national statistics [Internet]; 2018. [cited 2021 April 29]. Available from https://www.ons.gov.uk/peoplepopulationandcommunity/personalandhouseholdfinances/expenditure/datasets/percentageofhouseholdswithdurablegoodsuktablea45.
- John E, Thomas G, Touchet A. The disability price tag 2019 Policy report. 2019.
- McDaid D, Park A, la Gall A, et al. Understanding and modelling the economic impact of spinal cord injuries in the United Kingdom. Spinal Cord. 2019;57(9):778–788.
- Adams MM, Hicks AL. Spasticity after spinal cord injury. Spinal Cord. 2005;43(10):577–586.
- Kaye HS, Yeager P, Reed M. Disparities in usage of assistive technology among people with disabilities. Assist Technol [Internet]. 2008;20(4):194–203.
- Elbasiouny SM, Moroz D, Bakr MM, et al. Management of spasticity after spinal cord injury: current techniques and future directions. Neurorehabil Neural Repair. 2010;24(1):23–33.
- Baldassin V, Shimizu HE, Fachin-Martins E. Computer assistive technology and associations with quality of life for individuals with spinal cord injury: a systematic review. Qual Life Res. 2018;27(3):597–607.
- Folan A, Barclay L, Cooper C, et al. Exploring the experience of clients with tetraplegia utilising assistive technology for computer access. Disabil Rehabil Assist Technol. 2015;10(1):46–52.
- Mattar AAG, Hitzig SL, McGillivray CF. A qualitative study on the use of personal information technology by persons with spinal cord injury. Disabil Rehabil. 2015;37(15):1362–1371.
- MHRA. Assistive technology: definition and safe use - GOV.UK. GOVUK [Internet]. 2021. October 28 [cited 2021 November 30]. Available from: https://www.gov.uk/government/publications/assistive-technology-definition-and-safe-use/assistive-technology-definition-and-safe-use#assistive-technology-medical-device-or-not.
- Coleman R, Lebbon C, Clarkson J, et al. From margins to mainstream. In: Inclusive Design, Design for the Whole Population. 1st ed. London, Springer; 2003. pp 1–25.
- AbleNet. iOS 11 Accessibility Switch Control-The Missing User Guide. 2017. Available from https://www.ablenetinc.com/hook-switch-interface.
- Google. Accessibility | Android. 2021. [cited 2021 November 30]. Available from https://www.android.com/intl/en_uk/accessibility/.
- Apple. Inclusion - Technologies - Human Interface Guidelines - Apple Developer. 2021. [cited 2021 November 30]. Available from: https://developer.apple.com/design/human-interface-guidelines/inclusion/overview.
- Kong F, Sahadat MN, Ghovanloo M, et al. A Stand-Alone intraoral Tongue-Controlled computer interface for people with tetraplegia. IEEE Trans Biomed Circuits Syst. 2019; 13(5):848–857.
- José MA, de Deus Lopes R. Human-computer interface controlled by the lip. IEEE J Biomed Health Inform. 2015;19(1):302–308.
- Cotton RJ. Smartphone control for people with tetraplegia by decoding wearable electromyography with an on-device convolutional neural network. Proceedings of the IEEE RAS and EMBS International Conference on Biomedical Robotics and Biomechatronics; 2020. Nov 1; [cited 2022 October 8];2020-November. p. 1140–1145.
- Torlincasi AM, Waseem M. Cervical injury. Treasure Island (FL): StatPearls Publishing; 2019. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28846253
- Creswell J, Plano Clark V. Chapter 3. Choosing a mixed methods research design. In Designing and conducting mixed methods research. Thousand Oaks (CA): SAGE Publications; 2006. p. 53–105.
- Bryman A. Integrating quantitative and qualitative research: how is it done? Qualitative Research [Internet]. 2006;6(1):97–113.
- Onwuegbuzie A, Collins K. A typology of mixed methods sampling designs in social science research. TQR. 2007;12 (2):281–316.
- Guest G, Bunce A, Johnson L. How many interviews are enough? An experiment with data saturation and variability. Field Methods. 2006;18(1):59–82.
- Yamane T. Statistics : an introductory analysis. New York (N.Y.): Harper and Row; 1973.
- Braun V, Clarke V. Successful qualitative research: a practical guide for beginners. 1st ed. London: SAGE Publications; 2013.
- Legard R, Keegan J, Ward K. Qualitative research practice: a guide for social science students and researchers; 2003.
- Ryan F, Coughlan M, Cronin P, et al. The one-to-one interview. Int J Ther Rehabil. 2009;16(6):309–314.
- Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101.
- Braun V, Clarke V. Reflecting on reflexive thematic analysis. Qual Res Sport Exerc Health. 2019;11(4):589–597
- Blandford A, Furniss D, Makri S. Qualitative HCI Research Going Behind the Scenes. 1st ed. Cham: Springer Cham; 2016.
- Lincoln YS, Guba E. Naturalistic Inquiry. 1985.
- Nowell LS, Norris JM, White DE, et al. Thematic analysis: striving to meet the trustworthiness criteria. Int J Qual Methods. 2017;16:1–13.
- Guerreiro TJV, Nicolau H, Jorge J, et al. Assessing mobile touch interfaces for tetraplegics. ACM International Conference Proceeding Series 2010. p. 31–34.
- Trewin S, Swart C, Pettick D. Physical accessibility of touchscreen smartphones Proceedings of the 15th International ACM SIGACCESS Conference on Computers and Accessibility, ASSETS 2013. 2013.
- Nicolau H, Guerreiro J, Guerreiro T. Stressing the Boundaries of Mobile Accessibility. 2014. February 5 [cited 2021 November 30]. Available from: https://arxiv.org/abs/1402.1001v1.
- National SCI Statistical Center. Facts and figures at a glance. Birmingham; 2018.
- Parette P, Marcia S. Assistive technology use and stigma. Educ Train Dev Disabil. 2004;39:217–226.
- Kane SK, Jayant C, Wobbrock JO, et al. Freedom to roam: a study of mobile device adoption and accessibility for people with visual and motor disabilities. ASSETS’09 - Proceedings of the 11th International ACM SIGACCESS Conference on Computers and Accessibility. New York, New York, USA: ACM Press; 2009. p. 115–122.
- Braithwaite DO. Just how much did that wheelchair cost? Management of privacy boundaries by persons with disabilities. Western J Speech Commun. 1991;55(3):254–274.
- Bland R. Independence, privacy and risk: two contrasting approaches to residential care for older people. Ageing Soc. 1999;19(5):539–560.
- Hurst A, Tobias J. Empowering individuals with do-it-yourself assistive technology ASSETS’11: Proceedings of the 13th International ACM SIGACCESS Conference on Computers and Accessibility. Dundee Scotland, UK; 2011. p. 11–18.
- Scherer MJ, Cushman LA. Predicting satisfaction with assistive technology for a sample of adults with new spinal cord injuries. Psychol Rep. 2000;87(3 Pt 1):981–987.
- Riemer-Reiss ML, Wacker RR. Factors associated with assistive technology discontinuance among individuals with disabilities - ProQuest. J Rehabil. 2000;66:45–50.
- García TP, Garabal-Barbeira J, Trillo PP, et al. A framework for a new approach to empower users through low-cost and do-it-yourself assistive technology. Int J Environ Res Public Health [Internet]. 2021;18:1–17.
- MHRA. Guidance on Class I medical devices - GOV.UK. GOVUK [Internet]. 2020. December 31 [cited 2021 December 18]. Available from: https://www.gov.uk/government/collections/guidance-on-class-1-medical-devices.
- Burns SP, Terblanche M, MacKinen A, et al. Smartphone and mHealth use after stroke: results from a pilot survey. OTJR. 2022;42(2):127–136.
- Kamwesiga JT, Tham K, Guidetti S. Experiences of using mobile phones in everyday life among persons with stroke and their families in Uganda – a qualitative study. Disabil Rehabil. 2017;39(5):438–449.
- Wong D, Sinclair K, Seabrook E, et al. Smartphones as assistive technology following traumatic brain injury: a preliminary study of what helps and what hinders. Disabil Rehabil. 2017;39(23):2387–2394.
- Heitplatz VN, Bühler C, Hastall MR. Caregivers’ influence on smartphone usage of people with cognitive disabilities: an explorative case study in Germany. Lecture Notes in Comp Sci. 2019;11573:98–115.
- Simpson LA, Eng JJ, Hsieh JTC, et al. The health and life priorities of individuals with spinal cord injury: a systematic review. J Neurotrauma. 2012;29(8):1548–1555.