Article title: Finerenone: a mineralocorticoid receptor antagonist for the treatment of chronic kidney disease associated with type 2 diabetes
Authors: Lerma, E. V., & Wilson, D. J.
Journal: EXPERT REVIEW OF CLINICAL PHARMACOLOGY
Bibliometrics: Volume 15, Number 5, pages 501–513
DOI: https://doi.org/10.1080/17512433.2022.2094770
Since the publication of the article, the author wants to add the Plain language summary and graphical abstract as below.
Plain Language Summary:
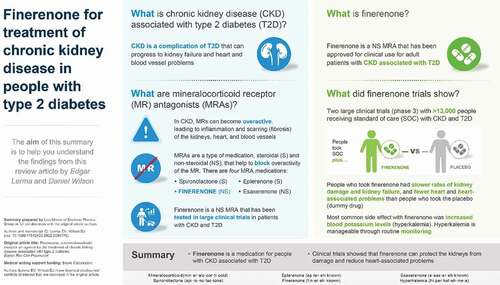
Around 4 in 10 people with type 2 diabetes (T2D) also have a condition called chronic kidney disease (also frequently referred to as diabetic kidney disease). People with T2D and chronic kidney disease have an overactive protein called the mineralocorticoid receptor (MR for short) in their kidney and heart cells. Overactive MRs causes inflammation and cell injury and can eventually cause damage to people’s kidneys and heart. Mineralocorticoid receptor antagonists (MRAs for short) are a type of drug that can be used to block the activity of the MR to reduce inflammation and damage to the kidneys and heart. There are two types of MRA – steroidal MRAs and non-steroidal MRAs. Steroidal MRAs (spironolactone and eplerenone) are an older type of MRA. Finerenone is a non-steroidal MRA and is a newer type of MRA. Researchers studied the effects of finerenone in two clinical trials involving more than 13,000 people withchronic kidney disease and T2D. In these trials people who took finerenone had slower rates of kidney damage and less heart and heart-associated problems than people who took a dummy drug (called a placebo). Some people taking finerenone may have increased blood potassium levels (called hyperkalemia), but this side effect can be managed and so people can continue to take finerenone. Researchers are continuing to research and consider where finerenone “fits best” among the available treatment options for people with T2D and chronic kidney disease.
Graphical Abstract: