

ABSTRACT
Introduction
Atherosclerotic cardiovascular disease (ASCVD) and heart failure (HF) are two major complications of type 2 diabetes (T2DM). Cardiovascular protection is a key objective, yet not fully reached in clinical practice.
Areas covered
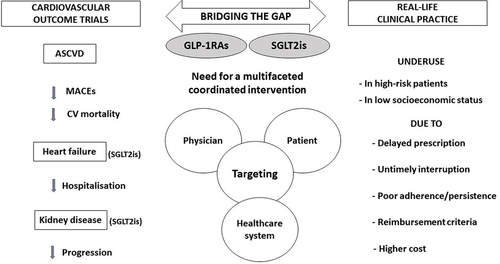
Both glucagon-like peptide-1 receptor agonists (GLP-1RAs) and sodium-glucose cotransporter 2 inhibitors (SGLT2is) have proven their efficacy in reducing major cardiovascular events in high-risk patients with T2DM and SGLT2is in reducing hospitalization for HF in placebo-controlled randomized trials. However, real-life studies worldwide revealed that only a minority of patients with T2DM receive either a GLP-1RA or an SGLT2i and surprisingly even less patients with established ASCVD or HF are treated with these cardioprotective antihyperglycemic agents.
Expert opinion
Bridging the gap between evidence-based cardiovascular protection with GLP-1RAs and SGLT2is and their underuse in daily clinical practice in patients with T2DM at high risk is crucial from a public health viewpoint. However, the task appears hazardous and the goal not attained considering the current failure. Education of specialists/primary care physicians and patients is critical. Multifaceted and coordinated interventions involving all actors (physicians, patients and broadly health-care system) must be implemented to stimulate the adoption of these cardioprotective antihyperglycemic medications as part of routine cardiovascular care among patients with T2DM.
Plain Language Summary
Type 2 diabetes can lead to major cardiovascular complications including cardiovascular disease linked to narrowing of the arteries (atherosclerosis), and heart failure. These complications are associated with lower quality of life and life expectancy. Thus, cardiovascular protection in people with type 2 diabetes is an important objective. However, clinical practice often fails in fully achieving this goal.
Two types of medications that lower blood sugar (so-called antidiabetic agents) have shown efficacy in reducing major cardiovascular events (such as strokes and heart attacks) in high-risk patients with type 2 diabetes. One of them has also shown effectiveness in decreasing hospitalizations due to heart failure. However, in clinical practice, most patients with type 2 diabetes do not receive these medications, even people with known cardiovascular disease or heart failure, despite the proven effectiveness of these drugs. Many studies worldwide have highlighted socioeconomic inequities regarding the use of these medications, which can be expensive.
From a public health perspective, it is imperative to bridge the gap between the under-use of cardioprotective antidiabetic agents in routine daily practice among high-risk patients with type 2 diabetes and the clear-cut recommendations of international guidelines. Given the current limitations, this task appears challenging. Education of physicians (both primary care practitioners and specialists, including cardiologists) and patients is most important in addressing this issue. Finally, in every country, the global health-care system should facilitate the use of these agents among patients with type 2 diabetes at high risk of atherosclerotic cardiovascular disease and heart failure.
GRAPHICAL ABSTRACT
Article highlights
People with type 2 diabetes are exposed to a high risk of atherosclerotic cardiovascular disease and heart failure
Both GLP-1 receptor agonists and SGLT2 inhibitors have demonstrated cardioprotective effects in dedicated outcome trials and observational studies
Nevertheless, numerous real-world studies reported an underuse of these agents, even and especially in patients with type 2 diabetes at high cardiovascular (and renal) risk
Numerous factors may explain this deficit and they concern not only medical doctors and patients, but also the global health-care system
A well-coordinated and multifaceted approach targeting prescribers, patients, and health-care system is warranted to succeed in bridging the current gap seen in clinical practice
Disclosure statement
AJ Scheen has received lecturer/scientific advisor/clinical investigator fees from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp & Dohme, NovoNordisk and Sanofi. He worked as clinical investigator in the EMPA-REG OUTCOME, CANVAS-R, DECLARE-TIMI 58, LEADER, and HARMONY Outcomes cardiovascular outcome trials. The author has no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Reviewer disclosures
Peer reviewers on this manuscript have no relevant financial or other relationships to disclose.