
ABSTRACT
Introduction: Children and young people with complex needs (severe motor impairments and without speech) have few opportunities to use alternative devices for communication. Eye-gaze controlled computers (EGCCs) might provide individuals with complex needs increased opportunities for communication and participation in society. Objective: To investigate the impact of EGCCs on communication, functional independence and participation in activities in children and young people with complex needs. Methods: A multicenter intervention study during seven months, measuring outcomes with or without EGCC at four time points, was conducted in Sweden, Dubai, and in USA. Seventeen participants (aged 3–26 years, diagnosis e.g. cerebral palsy, Rett syndrome) were provided with EGCC and services from an Assistive Technology center to implement EGCC in school and/or at home. Results: Participants significantly increased their expressive communication skills and functional independence with EGCC compared to baseline. All but one (16 of 17) increased their activity repertoire and computer use with EGCC. With EGCC, participation in computer activities averaged 4.1 performed activities (e.g. communication, play), with a duration of 70 minutes/day and a frequency of 76% of days. Discussion: The study strengthened the research evidence that EGCC can be an effective intervention in daily life for children and young people with complex needs. Communication and independence, common goals of intervention, were shown to be relevant EGCC outcomes.
Introduction
By providing opportunities for communication and access to a variety of internet activities and digital services, eye-gaze controlled computers (EGCCs) might give individuals with complex needs increased opportunities for participation in society.Citation1–3 Children and young people with complex needs – in this article represented by children and young people with severe motor impairments and without speech – make up a small proportion of the total population of children with disabilities. As a result of their severe motor impairments, they have profound needs for assistance in almost all everyday activities, including communication.Citation4–5 These children and young people often communicate by blinking, eye pointing and using low-tech devices or speech-generating devices with predetermined messages. Like most children, children and young people with complex needs live with their families, attend school and are expected to participate in family-related activities.
For children and young people with complex needs who are unable to operate a computer using gross or fine motor function or voice commands as an alternative method for communication or for other purposes, an EGCC might be an option. Instead of using an ordinary keyboard, mouse or alternative control methods (e.g. head movements, voice recognition), the person controls the computer using their gaze. This is made possible by special software and a camera, typically built-in or mounted on the screen, that emits an infrared light beam and tracks eye movements. The eye gaze controls the cursor on the screen by fixing on an object for a set amount of time (dwelltime).Citation6–7 The EGCC can be used together with software personalized for individual needs (e.g. symbols for communication, school tasks, environmental control) or to control the operating system environment. Being able to use a computer provides opportunities for communication and interaction, as well as participation in a variety of computer-based activities, such as leisure activities, including access to the internet.Citation3 Such opportunities are of utmost importance for a child’s development, health and learning.Citation8
The EGCC can be a relatively expensive assistive technologyCitation1 and clinical experiences indicate that before introduction of an EGCC, other low-tech and high-tech devices for communication have usually been tested without success. Available research shows that the most common diagnoses for children and young people who receive an EGCC as an assistive technology are cerebral palsy (77%) followed by Rett syndrome (17%). These children and young people are dependent on assistance for daily activities and are usually entirely or heavily dependent on assistance from another person for face-to-face communication, with 75% attending special schools.Citation1 Qualitative studies and cases studies have found that an EGCC could be a realistic option for children with complex needs.Citation9–14 Parents have reported that EGCCs provided children with opportunities to demonstrate agency; they could initiate communication and express basic needs, such as thirst and pain. The EGCCs also helped children to express their personality by providing opportunities to make choices and show self-determination.Citation2,Citation9 Furthermore, the possible ways to use an EGCC gave parents and teachers hope for a better future for the children, in which they could communicate independently and make their voice heard.Citation15 A total population study on usability of eye-gaze computers in Sweden, including 171 individuals, of which 60 were children aged 4–18 years of age, found that about two thirds of the children used their EGCC daily and one third used it weekly. More than 80% of the children used the technology during leisure (86%) and school (83%), usually for up to 2 hours a day, with only few high users (more than 4 hours daily).Citation1 The activity repertoire for each child ranged up to 12 activities, with a mean of 4.8. The most common activities when using an EGCC were playing games (78%) followed by talking (72%). Examples of other activities included writing with letters or symbols, watching videos, listening to music/radio, doing homework/school tasks and using social media. Only about one third of the parents agreed that their child used the computer in as many activities as needed (31%) and as often as needed (38%).Citation1
Research in the area is growing more common, but to the best of our knowledge there are few intervention studies examining the effectiveness and usability of EGCCs in everyday life for children and young people with complex needs. In 2018, Karlsson et al.Citation16 conducted a literature review of intervention studies examining the effectiveness of EGCCs for facilitating communication for people with significant physical disabilities. The review did not found any intervention study that examined the effectiveness of EGCCs for communication in children. In fact, they found only one intervention study involving children, which examined the impact of EGCCs on participation in computer activities (duration and frequency of use) and goal attainment in 10 children with complex needs, aged 1–15 years. The identified intervention studyCitation3 showed that children used EGCCs at home and/or in school with a mean activity repertoire of 3.8 activities. The EGCCs were most commonly used for communication, followed by for playing games. The EGCC intervention was successful in increasing achievement of the predefined goals and parents were satisfied with the device and services.
Thus, intervention studies of the effectiveness of EGCCs in everyday life for children and young persons with complex needs remain rare and it is vital that research continues to build evidence in order to support clinical practice. This study has focused on the impact of an EGCC intervention on communication and functional independence in children and young people with complex needs, areas not addressed in previous intervention studies, although they have been emphasized as important in research.Citation2,Citation14 Communication in this study refers to face-to-face communication between individuals in the same room.Citation17 Functional independenceCitation18 refers to stakeholders’ views on the independence of children and young people in daily life, with the EGCC versus without the EGCC. In addition, to build on and validate previous resultsCitation1–,Citation3,Citation12–13 from the research group, the study has also examined participation in computer activities and parental satisfaction with the device and services.
The aim for this multicenter intervention study was to investigate the impact of EGCC intervention on communication, functional independence, and participation in computer activities (type, frequency, and duration) in children and young people with complex needs. In addition, the study investigated stakeholders’ satisfaction with the EGCC as a device and with related services.
Methods
This international multicenter intervention study with a pre- (before EGCC), post- (with EGCC) and without EGCC use design followed 17 children and young people with severe disabilities during seven months when provided with an EGCC for use in school and/or at home. The study was composed of a baseline measurement (T1: before being provided with an EGCC), followed by provision of an EGCC for 6 months and support on how to use it, with intervention measurements at 3 and 6 months after baseline, respectively (T2 and T3: with EGCC), and measurement without the use of the EGCC at 6–7 months from baseline (T4: without EGCC). Each timepoint consisted of 2 weeks of measurements. The participants were permitted to continue using the EGCC following the last timepoint (T4). The procedure for collecting T4 data without the use of the EGCC while participants still had EGCC access was determined based on previous research findings showing limited EGCC use of about 2 hours a day.Citation3 The rationale for a T4 measurement was to verify that intervention with EGCC (T2, T3) did not interfere with their skills in using low tech devices after intervention since they are dependent on low tech devices when not using EGCC in daily life. Thus, the data collection without EGCC at T4 was used to strengthen the design.Citation19
Inclusion and Participants
Inclusion of Assistive Technology Centers
Based on their having the highest number of eye-gaze technology prescriptions in Sweden in past years, seven Swedish assistive technology (AT) centers out of 21 possible centers were invited to participate and 6 agreed. To find potential participants in other countries, the researchers contacted centers that provided EGCC services in Australia, the Netherlands, Hungary, England, the USA and Dubai. The age for inclusion was extended to young people up to 27 years, to accommodate the variety in service delivery in different countries. The centers in Dubai and the USA agreed to participate.
Inclusion of Participants
Children and young people who were assessed by their AT center to be candidates for an EGCC had tried the technology a few times with AT center professionals. Due to severe impairments, they had no or very limited possibilities to control computer software with dynamic pages (e.g. for communication) with input methods other than eye gaze. Inclusion criteria were a) children and young people at pediatric centers with severe motor impairment and without speech, with or without intellectual disabilities (<18 years or <27 years, depending on the country’s service delivery model), and b) candidates for an EGCC, waiting to be provided with an EGCC at home and/or in school. Exclusion criteria were rapidly progressing diseases with expected decline of functions during the study, or serious illness. Six centers in Sweden, one in Dubai, and one in the USA included participants consecutively in the study during the years 2016–2018. Based on previous eye-gaze technology cases at these centers, about 30–40 new cases were estimated during the inclusion period (Sweden 20–30 new cases, the USA 3–6 new cases, Dubai 8 new cases). The Swedish centers included participants during 22 months (2016–2018), the center in Dubai during 2018, and the center in the USA during the school year 2017–2018. All in all, 33 individuals at the eight centers met the inclusion criteria during the inclusion period.
At the six Swedish centers, 22 children and young people met the inclusion criteria. Parents of four individuals were, for unknown reasons, not asked about participation, despite meeting the inclusion criteria. Thus, parents of 18 of the 22 children and young individuals were asked about participation by their AT centers, of whom nine consented to participate and nine declined. Parents who declined did so because of time constraints.
At the center in Dubai, eight children and young people met the inclusion criteria, and all parents consented to participate. However, three individuals declined to participate due to health conditions with frequent absenteeism from school during the intervention and therefore dropped out from the study immediately after baseline. Five children and young people participated in the study.
At the center in the USA, three children met the inclusion criteria, and all parents were asked about participation and consented. All three children were included in the study.
In total, 17 children and young people were included and completed the study (Sweden n = 9, Dubai n = 5, USA n = 3). Two participants (Sweden, USA) used iPads at baseline, and one Swedish participant had access to an EGCC at baseline but had not used it regularly since provision, and was therefore included by the center for a new startup of the intervention. Data on reported hand function and level in the Manual Ability Classification System (MACS)Citation20 indicated that the participants with iPads could only make simple hand movements and thus required continuous support for performing activities on an iPad. Participant characteristics were reported by the centers. Severity of impairments was based on the classification systems Gross Motor Function Classification System (GMFCS),Citation21 MACS,Citation20 and Communication Function Classification System (CFCS).Citation22 All participants had access to low-tech single pictures, communication boards/books and/or a speech-generating device for single or sequential messaging.
Power
A power analysis was performed for the study based on an earlier EGCC intervention studyCitation7 that showed an increase in duration of computer use over time, from baseline to ten months of EGCC intervention. The analysis showed a mean difference of 43 min/day, giving a Cohen’s d [D/SD] of 1.6. To detect such a difference with a before and after design, with 80% power, 16 children would need to be included in the current study. After starting with participants at Swedish centers, centers abroad were also contacted to include the required numbers of participants.
Study Context
Six AT centers located in six of 21 regions in Sweden participated in the study. The AT centers are part of the healthcare system and responsible for providing services to children and young people with disabilities in need of AT in the region. AT team members at the centers are specialized in EGCC services and at least two team members, with any of the following professions, provided EGCC services in the study: occupational therapist, speech-language pathologist, special educator, information technology (IT) support person. These team members had 4–39 years of experience providing services to children and young people with complex needs and 4–18 years of experience with EGCC services. Habilitation centers in a region refer children and young people (<18 years) with disabilities and in need of an EGCC to their regional center to get support in assessing personal needs and adapting an EGCC. Habilitation professionals, who have long-term contacts with the family and teachers at the individual’s school, are invited to participate in the assessment and planning of EGCC use, with the child/young individual and parents. EGCC services may cover the use of an EGCC at home and/or in school.
The center in Dubai is a nonprofit organization, operating under the Ministry of Community Development within the Government of the United Arab Emirates. This center provides services to around 200 children and young people, aged 3–26 years, with various physical and cognitive challenges: autism, cerebral palsy, Down syndrome and/or other developmental disabilities. The center provides daytime services, employing a lifespan approach through a transdisciplinary mode of service delivery. Children and young people with intellectual and developmental disabilities from within the community are eligible to receive services at the center. Various educational and rehabilitation professionals collaborate to deliver services for the holistic development of the children and young adults at the center. EGCC services are related to the use of EGCCs in school. The intervention team is comprised of special educators, speech-language pathologists, occupational therapists, physical therapists, AT specialists, clinical psychologists, information and communication technology teachers, etc. There are two AT specialists, who have 10–15 years’ experience of providing services to the students enrolled at the center and about 5 years’ experience with EGCC services.
The center in the USA is a private nonprofit, non-governmental organization serving approximately 200 children aged 3–8 years with developmental or multiple disabilities and/or autism spectrum disorder, in five state-approved private schools. The center offers preschool classes on its premises. The agency’s AT team, consisting of a speech-language pathologist, an occupational therapist, a special educator and an AT specialist, supports each child’s team in regards to AT upon request. The AT team’s EGCC services may address the use of EGCCs in school and/or at home. AT team members have 20–42 years of experience with children with special needs and 4–12 years of experience with EGCCs. A child’s team includes special educators, speech-language pathologists, occupational and physical therapists, vision specialists and music therapists.
Centers in Sweden supported individuals up to 18 years old, those in Dubai supported individuals up to 26 years old and those in the USA gave support through adulthood.
The Eye-gaze Controlled Computer (EGCC) Interventions
The description of the EGCC interventions follows the Template for Intervention Description and Replication checklist,Citation23 reporting on items 1–10 in the template (brief name, why, what, who provided, how, where, when and how much, tailoring and modifications).
The most common goals of providing EGCCs to participants were communication and social interaction (n = 11) (e.g. making choices, expressing needs, responding to questions), learning to control an EGCC with eye gaze (n = 6), performing school tasks (n = 3) (literacy, writing and learning), and engaging in play and activities (n = 2). The EGCC interventions were followed for six months and consisted of 1) the child or young person getting access to an EGCC device with adapted and personalized software at home and/or in school, and 2) services provided and led by AT team members to the child/young person and to stakeholders (e.g. class teacher, parents, speech-language pathologist, occupational therapist) for implementation of the device in everyday contexts. For participants in Dubai, the EGCC was planned to be used only in school, whereas Swedish and American participants could use the EGCC both in school and at home. The goal of services was to promote the uptake and use of EGCC in school and/or at home. The intervention activities were decided in collaboration between the AT team and each child’s/young person’s team, and based on the respective center’s standard procedures.
Devices and Software
To get access to an EGCC, participants were provided with one of the following Tobii productsCitation24: I12 device (n = 7), I15 device (n = 4), PC Eye Mini (n = 4) or PC EyeGo (n = 2), as shown in . I12 and I15 have a 12” or 15” screen with a built-in eye-gaze device. PC Eye Mini and PC EyeGo are add-on eye-gaze devices for use on a Windows tablet or a laptop. In this study, all devices could be used for eye-gaze control of communication software (e.g. to communicate, play music) and the Windows environment (e.g. to play games, use the internet). Communication software programs reported as used on the EGCCs were Communicator 5Citation24 (n = 10), Grid 3Citation25 (n = 3), Clicker 7Citation26 (n = 3) and Compass with Word powerCitation24 (n = 2). The software was adapted and individualized for each participant by members of the AT team and stakeholders. The adaptations consisted of setting up pages for communication (n = 11) (e.g. choices, greetings, feelings), play and leisure activities (n = 11) (e.g. games, music, YouTube) and/or school activities (n = 5) (e.g. literacy, skills training), to match each participant’s needs. At the end of intervention, the total number of pictures and symbols varied greatly between participants, from about 20 up to several thousand (see Appendix 1 for individual-level data on devices and symbols). The most common symbols were colored photos and colored drawings. Two participants used Blissymbolics. Other software reported as controlled with eye-gaze included Look to LearnCitation24 (n = 6), Scenes and SoundsCitation24 (n = 3), e-books (n = 3) and some software used by a single participant (e.g. Sensory Fix and Eye Play Music from Tobii Dynavox,Citation24 Flame Painter from Escape Motions,Citation27 and other art design software). For one participant, the only software reported was Look to Learn.
Table 1. Overview of EGCC interventions in the study
Services
gives an overview of the provided services. All intervention activities were delivered individually for each participant. The contents of intervention activities were similar between all eight centers and consisted of planning meetings, follow-up meetings and sessions with EGCC use together with stakeholders in everyday contexts. In addition to AT team members, three or four of the following stakeholder categories were reported to be represented in intervention activities for all study participants: parents/guardians, school staff, therapists responsible for the participant’s habilitation, and medical staff.
Planning meetings involved meeting participants to discuss child/young person functioning and needs, goals for EGCC use, and the needs related to adaptations and implementation of a device in school and/or at home. Parents/guardians, teachers and assistants were educated by the centers on the use and handling of the EGCC, the EGCC calibration process, and the use of the software. During follow-up meetings, there were discussions on child/young person’s performance, the need for updated grids in the software, and evaluation of goals. Technical support was provided during intervention by an IT support person or AT specialist. The numbers of planning and follow-up meetings provided to participants are shown in . The median number (range) of meetings held during the 6-month intervention was 3 (1–4) meetings for participants in Sweden, 15 (15) for those in Dubai and 6 (4–13) for those in the USA (see Appendix 2 for individual-level data).
To perform activities with an EGCC in everyday contexts, the EGCC was set up for the participant (e.g. positioning, starting EGCC) by a stakeholder. Occasions of EGCC use were offered in school by teachers (Sweden, Dubai, USA) or specialists (AT specialist, occupational therapist or speech-language pathologist) (Dubai, USA), and at home by parents/guardians (Sweden, USA). Data on how many days each participant had occasions of EGCC use were collected twice during the intervention through structured computer diaries (see Data collection), and are reported in as number of days with EGCC use. For individual-level data, see Appendix 2.
Centers in the USA and Dubai had intensive services with AT professionals providing individual support on the use of EGCC in everyday life during the study. In Sweden, the services were structured so that professionals were responsible for informing and instructing the user’s network (e.g. parents, personal assistants and teachers), who supported the user’s EGCC use in everyday life.
AT team members were all trained in EGCCs and services to individuals with disabilities and delivered services as part of their professional role (see Study context).
Data Collection
Documentation of Services
The intervention activities were monitored by the AT team members during the study and summarized in a protocol developed for the study. They noted type of activity based on a list of predefined activities (e.g. planning meetings, follow-up meetings) and the number of occasions, contents and locations of EGCC use, and who participated in each activity.
Outcome Measurements
The Communication MatrixCitation17 was used to assess participants’ expressive communication skills in everyday life, face to face and in the same room, with and without the use of an EGCC, by interviewing parents/teachers. The instrument includes 24 questions and is specially designed to assess early communication skills in individuals with severe and multiple disabilities, using facial expressions, eye pointing and low- or/and high-tech devices as modes of communication. The use of communication behavior is scored within nine categories (e.g. body movements, facial expressions, concrete or abstract symbols) along with the degree to which the individual has mastered the communication behavior (scored as: not used, emerging, mastered). The total scores range up to 160. Inter-rater observer reliability for the instrument has been shown to be 90%.Citation17
Functional independence in everyday life with and without an EGCC was measured using the Psychosocial Impact of Assistive Devices Scale (PIADS)Citation18 from the perspective of parents and/or teachers, by rating the impact of EGCC versus that of other devices (see Procedure). PIADS is a questionnaire with a total of 26 items (e.g. independence, ability to participate, sense of control). The instrument has three subscales (Competence, Self-Esteem, Adaptability) and items are scored on a seven-point scale from −3 to +3 (“maximum negative impact” to “maximum positive impact”). The subscales measure the perceived impact of AT on productivity and performance (Competence scale), self-confidence and emotional well-being (the Self-esteem scale) and aspects of participation (Adaptability scale).Citation18 Each subscale score (−3 to +3) is obtained by dividing the sum of subscale item scores with the number of items. The instrument has good internal consistency and good reliability (0.77 to 0.85).Citation18,Citation28
A child’s/young person’s participation in computer activities with and without an EGCC was measured based on the computer use diaryCitation3 developed and tested in earlier studies.Citation3Citation29 Parents, personal assistants and teachers observed and documented computer use (type of activities, duration, frequency) during 14 days in a diary at school and another at home. Each day, minutes of computer use were noted for a set of predefined activities; it was also possible to add other activities.
Parents’ and teachers’ satisfaction with the EGCC was evaluated with the Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST 2.0).Citation30 The instrument concerns satisfaction with a device (8 items, e.g. ease of use) and satisfaction with services (4 items, e.g. professional services). All items are rated on a five-point scale (1–5) from “Not satisfied at all” to “Very satisfied”. Psychometric properties have been tested with satisfactory results.Citation30
Health-related quality of life (HRQoL) was measured with the KIDSCREEN-10 proxy version.Citation31 The instrument consists of ten items concerning a child’s/young person’s physical, psychological and social well-being. The instrument was used to capture participants’ mental health during the study and ratings were made by parents or teachers. The ten items are each rated on a five-point scale from “not at all” to “extremely”. The instrument has shown satisfactory reliability (intra-class correlation coefficients for test-retest reliability were 0.56–0.77) and good internal consistency, with a Cronbach’s alpha of 0.77–0.89.Citation31
Procedure
The researchers (MB, HH) visited each center once, before study startup, to describe the study and what was required of the centers. Follow-up meetings were conducted about once a month by phone (Swedish centers) or as web meetings (Dubai, USA) during the study, to support adherence to the study protocol. In addition, e-mails were used to remind centers of specific details and clarify any ambiguities in data collection. Data were collected at four timepoints: at baseline (before provision of the EGCC), at 3 months’ EGCC intervention, at 6 months’ EGCC intervention, and then without EGCC use after the end of the intervention (at 6–7 months after baseline). shows data collection at each timepoint. Data collection was the same for all participants at all timepoints. At baseline (T1) (before provision of EGCC), data collection consisted of stakeholders (parents, teachers, personal assistants) observing and documenting computer use (e.g. iPads) in the computer use diaries for 14 consecutive days in school and at home, and documenting the participant’s HRQoL with KIDSCREEN-10 based on the participant’s mental health during the preceding week. KIDSCREEN was used to understand participants´ HRQoL and to capture greater variations over the study. This was done since reduced HRQoL may compromise participants´ participation in intervention.
Table 2. Data collection at each timepoint (T1–T4)
Functional independence with devices used at baseline (mostly low-tech communication devices) was measured with PIADS. Expressive communication skills (e.g. using limited body movements, facial expressions, gazing at objects, persons, low-tech pictures to communicate) were measured with the Communication Matrix. Both PIADS and the Communication Matrix were administered by an AT specialist/researcher who completed the instrument protocols by interviewing parents or teachers. AT specialists also documented participant characteristics from medical records.
During the EGCC intervention (T2, T3), stakeholders documented EGCC use in computer use diaries at 3 months’ (T2) and 6 months’ (T3) intervention. At T3, interviews based on PIADS were performed with parents and teachers again, this time to measure the functional independence when using an EGCC in everyday life. At T3, expressive communication skills in everyday life were documented (the Communication Matrix) for the EGCC (selecting symbols using eye gaze) and low-tech use. Using QUEST 2.0, stakeholders also rated their satisfaction with the EGCC as a device and with related services at 6 months’ intervention (T3). AT specialists documented all intervention activities in medical records, following standard procedures.
After intervention (T4) (without EGCC use), stakeholders again used diaries to document computer use (e.g. iPads) and rated the participant’s HRQoL (KIDSCREEN-10), and AT team members summarized intervention activities from medical records. As at baseline, an AT team member/researcher interviewed stakeholders at T4 with PIADS, concerning functional independence when using other devices than the EGCC in everyday life (mostly low-tech communication devices). Similarly, the measurement with the Communication Matrix at T4 followed the same procedure as at baseline (T1), documenting expressive communication skills (e.g. use of body movements, facial expressions, low-tech devices) to communicate without using the EGCC, based on interviews with parents or teachers. Completed data for each timepoint were followed up by researchers during the entire study, and stakeholders were reminded repeatedly, if necessary, when data were missing.
Data Analysis
In order to see if there were any differences in ratings on the Communication Matrix over time, with and without the use of an EGCC, paired t-tests were performed between T1 and T3, and between T3 and T4, for total score on the Communication Matrix. Paired t-tests were also performed for each PIADS subscale (Competence, Adaptability, and Self-esteem) between T1 and T3, and between T3 and T4. Based on the multiple analyses, a significant p-value was set to <0.025.Citation32
As regards computer use diaries, 17 participants returned a total of 37 home diaries and 63 school diaries. First, the computer use diaries were summarized for each context (home, school) by calculating frequency of use (days with use in percent) for each activity, and total minutes of use and weekdays with use for each timepoint. Then, total computer use (activity repertoire, duration of use/day, and frequency of use) was calculated for both contexts. Calculations of frequency (days with use) were based on number of days with data in the diaries (maximum no of days: school n = 10, home n = 14). Descriptive statistics (mean, SD, median, range) were calculated for each variable and are presented in boxplots for each timepoint.
Descriptive statistics (mean, SD) were calculated for the QUEST 2.0 subscales Device and Services. Stakeholders’ scoring at an item level was also categorized as satisfied (4 = quite satisfied and 5 = very satisfied) or dissatisfied (1 = not at all, 2 = not very, and 3 = more or less).Citation30
Individual raw scores from KIDSCREEN ratings were transformed into T-scores using the KIDSCREEN Group Europe’sCitation33 reference population data for ages 8–11 years (all participants ≤10 years) and 11–18 years (all participants >10 years). Based on the T-scores, means and standard deviations were calculated for the study sample. As suggested by the KIDSCREEN Group Europe,Citation33 a threshold for judging what to interpret as an average score was set using the mean value plus or minus half a standard deviation for the European reference population data (T-score = 50, SD = 10, threshold 45–55). Higher values indicate better quality of life.
Ethical Considerations
The study was approved by a Regional Ethics Review Board in Sweden (Linköping, dnr 2016/218-31; Stockholm, dnr 2018/1809-32), by a Dubai Scientific Research Ethics Committee (DSREC-11/2017_10), and by an Institution Review Board in the USA (Philadelphia, protocol ESSP-02). Informed parental/guardian consent was obtained for all participants. They were informed that they could withdraw from the study at any time and that doing so would not affect the child’s or young person’s access to services or EGCC support from the center.
Results
Characteristics of Participants
The 17 participants’ age ranged between 3 and 26 years, with mean age 11.4 years (SD = 7.2). The oldest were the participants in the center in Dubai (n = 5, 16–26 years). Most participants were reported to have a cognitive impairment (n = 11) or developmental delay (n = 3), and attended a special school (n = 10) or a special preschool (n = 6), as shown in . Most participants had severe impairments (levels IV–V) in gross motor function (n = 11), manual ability (n = 12) and/or communication ability (n = 11) (see ). Four participants in Sweden (Rett syndrome, mitochondrial disease) were without data because staff deemed scoring with the classification systems (GMFCS, MACS, CFCS) would be inaccurate. The results showed that participants’ quality of life (KIDSCREEN-10) at a group level was at or close to the average of the European norm data. At baseline, the mean value was within the threshold (n = 10, mean T-score = 49.6, SD = 10.1, range 33.9–67.5), at 6 months’ EGCC intervention, it was just below the threshold (T3: n = 14, mean T-score = 44.7, SD = 8.9, range 30.5–65.4) and after intervention and without EGCC, it was within the threshold again (T4: n = 11, mean T-score = 47.6, SD = 9.7, range 28.3–65.4).
Table 3. Participant characteristics
Expressive Communication Skills
shows analyses of the Communication Matrix results. Participants increased in expressive communication skills over time, from before intervention (T1) to at 6 months’ EGCC intervention (T3). There was a significant difference in total score on the Communication Matrix between T1 (M = 39.9) and T3 (M = 52.1) (n = 16, p = .0127). Mean values decreased from T3 to T4, but no significant difference was found between 6 months’ EGCC (T3: M = 49.6) and without EGCC after the end of intervention (T4: M = 45.7) (n = 14, p = .263) (see ).
Table 4. Analysis of PIADS and communication matrix
Functional Independence
also shows an analysis of the PIADS subscales. The analysis revealed that participants increased in functional independence in regard to the subscale Competence (productivity and performance) over time. There was a significant difference between before intervention (T1: M = 0.58) and at 6 months’ intervention (T3: M = 1.21) on the Competence subscale (n = 13, p = .014). No differences were found for the Adaptability subscale (n = 13, p = .039) or the Self-esteem subscale (n = 13, p = .313) between these timepoints. Mean values decreased from 6 months’ EGCC intervention (T3) to after intervention and without an EGCC (T4), but no significant differences were found for any of the subscales between these timepoints (n = 13, T3 and T4) (Competence subscale: p = .033; Adaptability subscale: p = .094; Self-esteem subscale: p = .068).
Repertoire of Computer Activities
Two participants had access to an iPad and performed some activities with this device before and after intervention. Briefly, before intervention, three participants performed computer activities (T1, n = 3, iPads, EGCC), compared with all participants during EGCC intervention (T2, n = 17, EGCC; T3, n = 16, EGCC), and two after the end of the EGCC intervention (T4, n = 2, iPads).
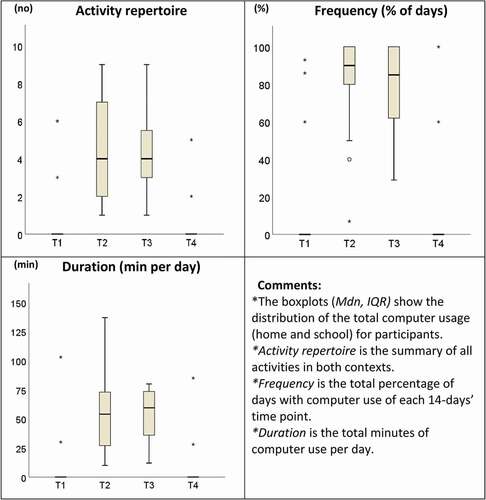
There was an increase in the repertoire of computer activities for 16 of 17 participants during the EGCC intervention. The average activity repertoire was 0.9 activities at baseline (T1: n = 17, SD = 2.1, Mdn = 0), and increased to 4.8 activities at 3 months’ EGCC intervention (T2: n = 17, SD = 2.75, Mdn = 4) and 4.1 activities at 6 months’ EGCC intervention (T3: n = 16, SD = 2.0, Mdn = 4), dropping to 0.4 activities without EGCC after the end of the intervention (T4: n = 17, SD = 1.3, Mdn = 0). shows the distribution of activity repertoires among participants.
Figure 1. Total computer use (activities, frequency and duration) at each time point (T1 n=17; T2 n=17; T3 n=16; T4 n=17). Duration: one participant at T1 (270 min), and another at T2 and T3 (T2: 249 min; T3: 323 min) with extreme values in duration are not shown in the boxplot
At 6 months’ intervention, 14 participants used an EGCC in school and six participants at home. Of these, four participants used it in both contexts, while the others used it in only in school (n = 10) or at home (n = 2). Activities performed with an EGCC by at least three participants in school and/or at home are shown in . In addition, six activities were performed by only one or two participants during school (e.g. participate in circle time, perform tests, conduct searches on the internet, hold presentations), and three activities were performed by only one or two participants at home (write text, write with symbols, read). Across both settings, talking to someone face to face in the same room was the computer activity performed by most participants (n = 10), followed by using the EGCC for games and play (n = 9). In school, the EGCC activity performed by most participants was skills training (n = 9), and at home it was games and play (n = 4). Appendix 3 shows individual-level data.
Table 5. Frequencies (%) of EGCC use in school and at home and activities performed, both predefined and own added. Numbers presented as median values (range)
Duration and Frequency of Computer Use
The duration of computer use was higher during the EGCC intervention than without EGCC. On average, the duration was 24 min per user day at baseline (T1: SD = 68.4, Mdn = 0), and increased to 62 minutes at 3 months’ EGCC intervention (T2: SD = 58.3, Mdn = 54) and to 70 minutes at 6 months’ intervention (T3: SD = 70.9, Mdn = 60), before dropping to 7 min after the intervention and without an EGCC (T4: SD = 21.7, Mdn = 0). Similarly, the average percentage of days with use increased from 14% at baseline (T1: SD = 32, Mdn = 0) to 82% at 3 months (T2: SD = 27, Mdn = 90) and 76% at 6 months (T3: SD = 27, Mdn = 85), dropping to 9% after intervention and without an EGCC (T4: SD = 28, Mdn = 0) (see ).
Satisfaction with Services and Eye-gaze Technology Device
At 6 months’ intervention, parents (n = 7) and teachers (n = 9) were quite satisfied with the EGCC as a device (n = 16, M = 3.64, SD = 0.85) and with the related services (n = 15, M = 3.77, SD = 1.37) (total scale: n = 16, M = 3.63, SD = 0.98). The items with most satisfied stakeholders were Professional Service (13/16), Dimensions (12/16), and Easy to Use (12/16). Most dissatisfied stakeholders were found for Weight (9/16) and Safety (9/16). The three most important items at this timepoint were Easy to Use (15/16), Effectiveness (8/16) and Weight (5/16).
Discussion
Our main reason for conducting this study was to add to the evolving research evidence in the field of EGCCs for children and young people with complex needs. This study provided evidence of increased expressive communication skills with an EGCC among children and young people with complex needs. This is an important finding, since communication and social interaction were major goals with EGCC use for most participants, and talking to others was an activity often performed with an EGCC in this study, as well as in previous research.Citation1–3 Caregivers of children and young people with complex communication needs see communication as a high priority outcome of services and interventions.Citation34–35 Thus, from the stakeholders’ perspectives, the results indicated that EGCCs provided participants with communication opportunities, even though they did not reveal how EGCCs contributed to communication. For example, Dhondt et al.Citation36 found a positive correlation between total score on the Communication Matrix and age, and a case studyCitation37 with a 7-year-old child with disabilities found more advanced communication skills (combining symbols) when the child used a tablet app compared with when using low-tech devices. To explore how EGCCs support functional communication at an individual level, a forthcoming study will use video coding to investigate children and young people with and without the use of an EGCC in communication situations.
Regarding functional independence in everyday life, the current study added to previous research that EGCCs have some positive effects on productivity and performance for participants, based on the results for the Competence scale (PIADS). In line with the current study, a multi-case study with children with Rett syndrome (age 9–15 years) showed positive clinically relevant changes on the Competence scale from EGCC use for all four included children.Citation11 From the stakeholders’ perspectives, increased functional independence with EGCC as regards performance and productivity, which contribute to competence, was probably the most obvious outcome, rather than the two psychosocial areas (Self-esteem, Adaptability) of PIADS. If a device changes a child’s or young person’s status from being totally dependent on stakeholders to being able to perform activities on their own, this would be noticeable by caregivers. Gaining the ability to perform activities, demonstrate skills and initiate activities with an EGCC has been seen in previous qualitative research.Citation2,Citation13 The psychosocial impact of a device is an important outcome as it can predict device retentionCitation18, since utility in everyday life is a prerequisite for sustained use.Citation38 If stakeholders perceive that a device makes a difference in real life, they are more likely to support adoption of an EGCC in school and at home by preparing and setting up the EGCC, to provide opportunities for functional use on a daily basis.
This study supported previous research on the impact of EGCCs on participation in computer activities. The results in this international multicenter study showed that participants had activity repertoires, frequency and duration of EGCC use in school and at home similar to those found in an earlier intervention study in Sweden.Citation3 Mean values of activity repertoires were close to 4 in both studies (M = 4.1 in the current study; M = 3.8 in Borgestig et al.,Citation3) with frequencies ranging from weekly to daily in both studies, and with somewhat longer daily durations in the current study (M = 70 min) than in the previous one (M = 40 min).Citation3 Moreover, talking to someone, participating in games and play, and skills training were common activities in both the current study and in the previous intervention study by Borgestig et al.Citation3 In addition, a survey studyCitation1 showed somewhat higher values, but generally similar results, as regards activity repertoire (M = 4.8), frequency (63% daily use, 33% weekly) and duration of use (mostly up to 2 hours a day); talking to someone and games and play were the activities most often performed with an EGCC. Thus, the current study confirmed previous research and strengthened the evidence concerning usability of EGCCs by children and young people with complex needs to perform important activities in school and at home.
Nevertheless, it was noteworthy that the use of EGCC was limited to 2 hours a day for almost all participants in school and at home, in the current study as well as in previous research, despite a wide range of participant ages. Altogether, comprising results in the current study (17 participants) and the two studies mentioned above, 87 children and young people using an EGCC in everyday life have been included in the research of use and usability (n = 10 in Borgestig et al.Citation3; n = 60 in Hemmingsson and Borgestig.Citation1) Of 87 included children and young people, only seven in school and five at home can be described as high users, with EGCC use of 4 hours or more a day. They were all included in the survey study.Citation1 In fact, only one participant in the current study exceeded a duration of 2.5 hours of EGCC use a day (323 min) during the intervention (see ). Even though an EGCC may create many new opportunities for children and young individuals, the duration of use in everyday life is still limited. The reasons are unknown, but could include the need for parental support or fatiguing demands on the children and young people. Previous research has shown that parents thought EGCCs were not used as much as neededCitation1 and that they needed support to expand activity repertoires in keeping with child development.Citation2 On the other hand, all new opportunities to become more independent with an EGCC may place new demands on children and young people to show skills in school and express themselves without support. Such demands are likely a new situation for a child or young individual who is accustomed to being entirely dependent, and may be fatiguing and reduce the child’s or young person’s attention, energy or interest in using the EGCC. More research is needed to better understand what affects daily EGCC use. Qualitative interviews with parents, teachers, children and young people would provide new insights into this, and also give information about whether EGCC products need to be improved for more functional use and extended duration of use. A recommendation is that service providers use follow-up meetings to ask about the duration of use, the extent to which the EGCC satisfies user needs, and stakeholders’ needs for support.
Limitations
A limitation of the study was the small number of participating children and young people in spite of wide invitations and a long inclusion period. Research into eye-gaze technology has thus far been characterized by small sample sizes.Citation39 The intention of the current study was to include 25–40 participants, to strengthen research evidence in this field. Nevertheless, after 22 months, only 33 children and young individuals were identified as eligible for the study, of whom nine declined, four were not invited for unknown reasons, and three dropped out after baseline for different reasons. One parent’s reason for declining participation was time constraints, which might indicate that the amount of data collection required of the families/teachers was unreasonably high in this study. It is possible that the number of participants was affected by the amount of work they or their family members and teachers were obliged to do if they agreed to participate. For participation in the current study, parents/teachers agreed to be helpful in the rather extensive data collection, as shown in . Conducting a longitudinal intervention study is an expensive project and is time-consuming for both participants and researchers. The amount of data planned for collection was initially justified by the researchers for these reasons. However, some international contacts and parents may have declined participation because of the study requirements putting pressure on the close environment; perhaps participation might have been greater if the work demanded of the participants had been less onerous.Citation40 Parents of children with complex needs may already be exhausted by the high levels of strain from caring for a child with physical and/or intellectual disabilities,Citation41 and they express that they have many family needs.Citation42 In addition, although it has been recommended in research,Citation16 participants did not receive any benefits from participating in the study such as extra training, information or education. A recommendation for future studies for successful inclusion of children and young people with complex needs is to carefully consider how data collection in the everyday environments can be conducted to minimize the extra burden placed on the close environment. Benefits to those involved might also be considered in order to increase participation.
The reason for using a research design following services for six months and then, at the last timepoint, measuring outcomes without the use of an EGCC was to verify that EGCC intervention did not interfere with participants’ skills to use low tech devices after intervention. Since most participants used the EGCC for up to two hours a day, there were many situations involving a need to communicate and participate without EGCC, making it possible to perform measurements without EGCC use at 6–7 months (T4). Although there was a significant increase from T1 (before EGCC) to T3 (with EGCC) in communication and functional independence, the results showed a tendency but no significant decrease from T3 (with EGCC) to T4 (without use of EGCC). One reason for this could be that participants had become trained in eye-gaze pointing by using the EGCC regularly, and thus had also become more competent in pointing with eye gaze on low-tech communication boards and devices. An earlier study showed increases in eye-gaze performance over time among children with severe disabilities using an EGCC regularly.Citation43–44 However, another reason could be that it was difficult for parents and teachers to delimit the positive effects of the EGCC intervention they experienced at T3 when rating other AT devices’ impact on daily life at T4.
Conclusion
This study demonstrated that an EGCC can be an effective intervention in children and young individuals with complex needs, to increase communication and independent performance of and participation in computer activities. It can also inform clinical practice of possible outcomes of EGCC use for young users of varying ages and diagnoses when services are provided by experienced AT teams in pediatric and school settings. This is important, since relevant outcomes may determine adoption and retention of EGCCs in the long term. During follow-up sessions, service providers should pay attention to whether the close environment needs support to increase the duration of EGCC use to meet the child’s and young person’s needs.
In a global perspective, this international project showed that EGCC use and EGCC activities in everyday life have similarities for children and young people with complex needs. A recommendation for future research is to follow participants over several years, since it would be beneficial to learn about long-term effects and continuity in EGCC use. Future studies should also carefully consider the burden of data collection for this specific group of participants. Developing and using technology to electronically log service providers’ activities and stakeholders’ intervention sessions on a daily or weekly basis is recommended.
Declaration of Interest
The authors report no conflict of interest.
Acknowledgments
The authors would like to thank all eight centers, AT teams, families and school personnel for their participation in the study.
Additional information
Funding
- Hemmingsson H, Borgestig M. Usability of eye-gaze controlled computers in Sweden: a total population survey. Int J Environ Res Public Health. 2020;17:1639. doi:https://doi.org/10.3390/ijerph17051639.
- Borgestig M, Rytterström P, Hemmingsson H. Gaze-based assistive technology used in daily life by children with severe physical impairments–Parents’ experiences. Dev Neurorehabil. 2017;20(5):301–08. doi:https://doi.org/10.1080/17518423.2016.1211769.
- Borgestig M, Sandqvist J, Ahlsten G, Falkmer T, Hemmingsson H. Gaze-based assistive technology in daily activities in children with severe physical impairments–An intervention study. Dev Neurorehabil. 2017;20(3):129–41. doi:https://doi.org/10.3109/17518423.2015.1132281.
- Ostensjø S, Carlberg EB, Vøllestad NK. Everyday functioning in young children with cerebral palsy: functional skills, caregiver assistance, and modifications of the environment. Dev Med Child Neurol. 2003;45(9):603–12. doi:https://doi.org/10.1111/j.1469-8749.2003.tb00964.x.
- Rosenbaum P. Cerebral palsy: what parents and doctors want to know. BMJ. 2003;326(7396):970–74. doi:https://doi.org/10.1136/bmj.326.7396.970.
- Karlsson P, Wallen M. Parent perception of two eye-gaze control technology systems in young children with cerebral palsy: pilot study. Stud Health Technol Inform. 2017;242:1095–102.
- Majaranta P, Donegan M. Introduction to gaze interaction. In: Majaranta P, Aoki H, Donegan M, Hansen DW, Hansen JP, Hyrskykari A, Räihä K, editors. Gaze interaction and applications of eye tracking: advances in assistive technologies. Hershey (USA): IGI Global;2012. p. 1–9. doi:https://doi.org/10.3109/17518423.2015.1132281.
- Von Tetzchner S. Utvecklingspsykologi [Developmental psychology]. Ed 2:1. Lund (Sweden): Studentlitteratur; 2016.
- Holmqvist E, Thunberg G, Peny Dahlstrand M. Gaze-controlled communication technology for children with severe multiple disabilities: parents and professionals’ perception of gains, obstacles, and prerequisites. Assist Technol. 2018;30(4):201–08. doi:https://doi.org/10.1080/10400435.2017.1307882.
- Van Niekerk K, Tönsing K. Eye gaze technology: a South African perspective. Disabil Rehabil Assist Technol. 2015;10(4):340–46. doi:https://doi.org/10.3109/17483107.2014.974222.
- Vessoyan K, Steckle G, Easton B, Nichols M, Mok Siu V, McDougall J. Using eye-tracking technology for communication in Rett syndrome: perceptions of impact. Augment Altern Commun. 2018;34(3):230–41. doi:https://doi.org/10.1080/07434618.2018.1462848.
- Hemmingsson H, Ahlsten G, Wandin H, Rytterström P, Borgestig M. Eye-gaze control technology as early intervention for a non-verbal young child with high spinal cord injury: a case report. Technologies. 2018;6(1):12. doi:https://doi.org/10.3390/technologies6010012.
- Rytterström P, Borgestig M, Hemmingsson H. Teachers’ experiences of using eye gaze-controlled computers for pupils with severe motor impairments and without speech. Eur J Spec Needs Educ. 2016;31(4):506–19. doi:https://doi.org/10.1080/08856257.2016.1187878.
- Karlsson P, Bech A, Stone H, Vale C, Griffin S, Monbaliu E, Wallen M. Eyes on communication: trialling eye-gaze control technology in young children with dyskinetic cerebral palsy. Developmental Neurorehabilitation. 2019;22(2):134–40. doi:https://doi.org/10.1080/17518423.2018.1519609.
- Rytterström P, Borgestig M, Hemmingsson H. Hope and technology other-oriented hope related to eye gaze technology for children with severe disabilities. Int J Environ Res Public Health. 2019;16(10):1667. doi:https://doi.org/10.3390/ijerph16101667.
- Karlsson P, Allsop A, Dee-Price BJ, Wallen M. Eye-gaze control technology for children, adolescents and adults with cerebral palsy with significant physical disability: findings from a systematic review. Dev Neurorehabil. 2018;21(8):497–505. doi:https://doi.org/10.1080/17518423.2017.1362057.
- Rowland C, Communication Matrix: F-OM. A clinical and research assessment tool targeting children with severe communication disorders. Journal of Pediatric Rehabilitation Medicine: An Interdisciplinary Approach. 2010;3(4):313–29. doi:https://doi.org/10.3233/PRM-2010-0144.
- Jutai JW, Day H, Gelderblom GJ, De Witte LP. Psychosocial impact of assistive devices scale (PIADS). Technol Disabil. 2002;14(3):107–11. doi:https://doi.org/10.3233/TAD-2002-14305.
- Fok CC, Henry D, Allen J. Research designs for intervention research with small samples II: stepped wedge and interrupted time-series designs. Prev Sci. 2015;16(7):967–77. doi:https://doi.org/10.1007/s11121-015-0569-4.
- Eliasson A-C, Krumlinde-Sundholm L, Rösblad B, Beckung E, Arner M, Öhrvall A-M RP, Rosenbaum P. The Manual Ability Classification System (MACS) for children with cerebral palsy: scale development and evidence of validity and reliability. Dev Med Child Neurol. 2006;48(7):549–54. doi:https://doi.org/10.1017/S0012162206001162.
- Palisano R, Rosenbaum P, Walter S, Russell D, Wood E, Galuppi B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neurol. 1997;39(4):214–23. doi:https://doi.org/10.1111/j.1469-8749.1997.tb07414.x.
- Hidecker MJC, Paneth N, Rosenbaum PL, Kent RD, Lillie J, Eulenberg JB, Chester Jr K, Johnson B, Michalsen L, Evatt M. Developing and validating the communication function classification system for individuals with cerebral palsy. Dev Med Child Neurol. 2011;53(8):704–10. doi:https://doi.org/10.1111/j.1469-8749.2011.03996.x.
- Hoffman TC, Glasziou PP, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. 1975;24(16):1469–74. doi:https://doi.org/10.1016/0006-2952(75)90020-9.
- Tobii Dynavox LLC Assistive technology for communication. Tobii Dynavox; 2020 [accessed 2020 Jun 24] https://www.tobiidynavox.com/en-US/?redirect=true
- Smartbox Assistive Technology. Smartbox communication aids. Malvern (England): Smartbox Assistive Technology Limited; 2020 [accessed 2020 Jun 24] https://thinksmartbox.com/
- Crick Software Ltd. Reading and writing software for all abilities. Crick Software Ltd; 2020 [accessed 2020 Jun 24] https://www.cricksoft.com/uk
- Motions E. Flame Painter 4. Escape Motions; 2020 [accessed 2020 Jun 29] https://www.escapemotions.com/products/flamepainter/
- Pettersson I, Ahlström G, Törnquist K. The value of an outdoor powered wheelchair with regard to the quality of life of persons with stroke: a follow-up study. Assist Technol. 2007;19(3):143–53. doi:https://doi.org/10.1080/10400435.2007.10131871.
- Borgestig M, Falkmer T, Hemmingsson H. Improving computer usage for students with physical disabilities through a collaborative approach: a pilot study. Scand J Occup Ther. 2013;20(6):463–70. doi:https://doi.org/10.3109/11038128.2013.837506.
- Demers L, Weiss-Lambrou R, Ska B, Gelderblom GJ, De Witte LP. The Quebec user evaluation of satisfaction with assistive technology (QUEST 2.0): an overview and recent progress. Technol Disabil. 2002;14(3):101–05. doi:https://doi.org/10.3233/TAD-2002-14304.
- Ravens-Sieberer U, Erhart M, Rajmil L, Herdman M, Auquier P, Bruil J, Power M, Duer W, Abel T, Czemy L, et al. Reliability, construct and criterion validity of the KIDSCREEN-10 score: a short measure for children and adolescents’ well-being and health-related quality of life. Quality of Life Research. 2010;19(10):1487–500. doi:https://doi.org/10.1007/s11136-010-9706-5.
- Ottenbacher KJ. Quantitative evaluation of multiplicity in epidemiology and public health research. Am J Epidemiol. 1998;147(7):615–19. doi:https://doi.org/10.1093/oxfordjournals.aje.a009501.
- The KIDSCREEN Group Europe. The KIDSCREEN Questionnaires - Quality of life questionnaires for children and adolescents. Handbook. Lengerich (Germany): Pabst Science Publishers; 2006.
- Larriba-Quest K, Byiers BJ, Beisang A, Merbler AM, Symons FJ. Special education supports and services for Rett syndrome: parent perceptions and satisfaction. Intellect Dev Disabil. 2020;58(1):49–64. doi:https://doi.org/10.1352/1934-9556-58.1.49.
- Mei C, Reilly S, Reddihough D, Mensah F, Green J, Pennington L, Morgan AT. Activities and participation of children with cerebral palsy: parent perspectives. Disabil Rehabil. 2015;37(23):2164–73. doi:https://doi.org/10.3109/09638288.2014.999164.
- Dhondt A, Van Keer I, Van Der Putten A, Maes B. Communicative abilities in young children with a significant cognitive and motor developmental delay. J Appl Res Intellect Disabil. 2020;33(3):529–41. doi:https://doi.org/10.1111/jar.12695.
- Sreekumar S, Sangeetha GS, Mathew BS. Advancement to higher communicative functions with transition to iPad app - A case report. Disabil Rehabil Assist Technol. 2020;15(4):480–83. doi:https://doi.org/10.1080/17483107.2019.1629116.
- Lenker JA, Paquet VL. A new conceptual model for assistive technology outcomes research and practice. Assist Technol. 2004;16(1):1–10. doi:https://doi.org/10.1080/10400435.2004.10132069.
- Perfect E, Hoskin E, Noyek S, Davies C. A systematic review investigating outcome measures and uptake barriers when children and youth with complex disabilities use eye gaze assistive technology. Dev Neurorehabil. 2020;23(3):145–59. doi:https://doi.org/10.1080/17518423.2019.1600066.
- Polit DF, Beck CT. Nursing research: generating and assessing evidence for nursing practice. 9th. Philadelphia (USA): Lippincott Williams & Wilkins; 2012.
- Kenny K, McGilloway S. Caring for children with learning disabilities: an exploratory study of parental strain and coping. British Journal of Learning Disabilities. 2007;35(4):221–28. doi:https://doi.org/10.1111/j.1468-3156.2007.00445.x.
- Palisano RJ, Almarsi N, Chiarello LA, Orlin MN, Bagley A, Maggs J. Family needs of parents of children and youth with cerebral palsy. Child Care Health Dev. 2010;36(1):85–92. doi:https://doi.org/10.1111/j.1365-2214.2009.01030.x.
- Borgestig M, Sandqvist J, Parsons R, Falkmer T, Hemmingsson H. Eye gaze performance for children with severe physical impairments using gaze-based assistive technology—A longitudinal study. Assist Technol. 2016;28(2):93–102. doi:https://doi.org/10.1080/10400435.2015.1092182.
- Ablenet. Speech generating devices. Roseville (USA): Ablenet Inc; 2020 [accessed 2021 Jan 04] https://www.ablenetinc.com/technology/speech-generating-devices