
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
Rett syndrome is a neurodevelopmental disorder in which scoliosis is a common orthopedic complication. This explorative study aims to identify predictors for rapid progression of scoliosis in Rett syndrome to enable variable selection for future prediction model development. A univariable logistic regression model was used to identify variables that discriminate between individuals with and without rapid progression of scoliosis (>10Cobb angle/6 months) based on multi-center data. Predictors were identified using univariable logistic regression with OR (95% CI) and AUC (95% CI). Age at inclusion, Cobb angle at baseline and epilepsy have the highest discriminative ability for rapid progression of scoliosis in Rett syndrome.
Introduction
Rett syndrome (RTT) is an X-linked dominant neurodevelopmental disorder that evolves from a defect in the Methyl-CpG binding protein 2 (MECP-2). Citation1–3 It predominantly affects women with a prevalence of 1 in 10,000 births.Citation1,Citation4–6 Rett syndrome is characterized by a regression of acquired skills after a period of 6–18 months postpartum of seemingly normal development.Citation7 Clinical symptoms include loss of expressive language skills, development of hand stereotypes and impaired gross motor skills. Multiple comorbidities are recognized in Rett syndrome, of which scoliosis is the deformity most commonly urging to orthopedic care; it appears in 75% of individuals with Rett syndrome of which 50% develops scoliosis before the age of 11 years.Citation1,Citation5,Citation8
It is usually assessed using posteroanterior (PA) and lateral X-ray imaging of the cervical, thoracic and lumbar spine, and is diagnosed when the Cobb angle, in the frontal plane, exceeds 10.Citation9 Scoliosis in Rett syndrome is thought to be of neuromuscular origin; it can occur early in a child’s life, is often progressive, and does not necessarily cease when skeletal maturation has finished.Citation8,Citation10 It could lead to secondary symptoms such as discomfort, deterioration of mobility and a decrease in physical function.Citation8 Despite these major implications, the evidence base concerning factors that influence progression is limited, consequently resulting in uncertainty about treatment pathways and timing of interventions in females with RTT for parents as well as clinicians.Citation11
The management of scoliosis in children can roughly be divided into conservative or operative management, depending on the severity of progression.Citation9 Surgery is indicated in case of severe scoliosis to regain spinal symmetry, improve mobility, improve sitting balance, decrease pain, and treat/prevent progressive lung compression.Citation2,Citation11 Orthotic treatment and physiotherapy are part of the conservative management approach of scoliosis. Bracing has been shown to be effective in reducing the risk of curve progression in idiopathic scoliosis, especially in young children with a low skeletal maturity.Citation9 Inconclusive evidence exists concerning the effectiveness of conservative management in the form of bracing for scoliosis in Rett syndrome. For physiotherapy however, evidence shows improved mobility, flexibility of the spine, and increased comfort. Nonetheless, neither bracing nor physiotherapy seems to be able to reduce progression of scoliosis in RTT.Citation8,Citation12
Several predictors for the progression of scoliosis have been identified in the literature. Prognosis of a more severe scoliosis was found to be related to earlier onset of puberty, as the onset of puberty in females with Rett syndrome is premature compared to females that develop typically.Citation12 Evidence suggests that certain genotypes are associated with milder forms of scoliosis (p.Arg133Cys and p.Arg306Cys) and some genotypes are known to be associated with a higher risk of developing severe scoliosis (p.Arg270X).Citation1,Citation11,Citation12 In addition, multiple studies showed that a higher level of walking ability is associated with a lower severity of scoliosis.Citation1,Citation2,Citation11 Age at regression (phase two Rett syndrome) and Cobb angle in the frontal plane are also mentioned as possible predictors in the current body of evidence, in which an earlier age at regression could lead to more severe scoliosis.Citation1,Citation12–14 Previous small case studies indicate an average progression of scoliosis of 14 degrees per year, although patient characteristics contributing to this progression in individuals with Rett syndrome are uncertain.Citation15 Since evidence about the management of scoliosis in individuals with Rett syndrome is mostly lacking, insight into factors that predict rapid progression of scoliosis by means of a clinical prediction model is crucial. Furthermore, insight in these factors aids parents and clinicians to predict the chance of progression of scoliosis specific to the individual with Rett syndrome.Citation11 However, a sufficiently large Dutch cohort with extensively described patient characteristics that is needed to create a prediction model is not available.Citation16
This study aims to explore factors with discriminative ability to identify progression of scoliosis in individuals with Rett syndrome.
Materials and Methods
Study Design
A longitudinal analysis was performed based on prospectively collected multi-center data. As this study precedes prediction research, the TRIPOD statement was used as reporting guideline.
In- and Exclusion Criteria
For this study, exclusively females with clinically or genetically confirmed Rett syndrome and scoliosis between the age of 2–16 were selected. As only few cases of males with Rett syndrome have been described and the clinical presentation in males is not yet fully understood, male participants were excluded from this study. Citation17–20 To measure scoliosis progression, at least two subsequent Cobb angle measurements are required with 6 months or more in between. Therefore, participants with less than two subsequent X-rays were excluded from this study. Further exclusion criteria were as follows: commencement of menarche prior to the first measurement and previously performed scoliosis surgery.
Data Collection
To acquire a sufficient sample size, data of the Dutch Rett syndrome Association (NRSV) and of the Maastricht University Medical Centre (MUMC+) Rett expertise center were combined. Data from the NRSV consisted of written questionnaires completed by members of the NRSV – parents/caregivers of individuals with Rett syndrome – between 2008 and 2013. During this timeframe, parents and/or caregivers were approached by the NRSV through written request and were asked to fill out questionnaires and include X-ray images after written consent. A response of 95 members and their respective children was obtained. Only data from included children with two or more sequential X-ray images was used for the dataset which led to a sample size of 27 participants. Furthermore, data from the MUMC+ was obtained by researchers from medical records and accompanying X-ray images of individuals with Rett syndrome at the department of orthopedic medicine. All eligible participants were screened on the availability of sequential X-ray images which led to a sample size of 50 participants.
Information about current age, age at RTT diagnosis, type of mutation, age at (first) regression, level of walking ability, level of sitting ability, epilepsy, respiratory problems, constipation, low bone density, physiotherapy, bracing, and surgical correction were obtained from both data sources using the questionnaires or medical records, respectively (app 1). Sequential hip and spine X-ray assessment was performed by professionals and provided information about the Cobb angle (position X-ray, type of curve, apex curve), kyphosis, subluxation of the hip, Risser’s sign and leg length difference of the participants (app 1). The professional rater team included an orthopedic surgeon and an experienced physical therapist trained in spine X-ray readings by an orthopedic spine surgeon.
Subsequently, all collected data originating from the two sources were combined into one dataset, resulting in 64 unique participants ().
Figure 1. Flow chart participant selection.
Outcome
The primary outcome of this study, rapid progression of scoliosis, was operationalized as the change in Cobb angle per time unit (/half a year). Cobb angle measurements in the frontal plane of the scoliosis curve were performed at each available sequential X-ray for every participant, to quantify the magnitude of the curve.Citation21 Multiple actions were undertaken to optimize reliability of Cobb angle measurements in this study.Citation22,Citation23 All Cobb angle measurements of the sequential X-rays were performed twice with standardization of the end vertebrae of the curvature. In addition, the position of the participant was recorded for every X-ray. For the NRSV data, two independent blinded expert raters assessed all Cobb angles independently whereas the Cobb angles rated by an expert in the MUMC+ data source were compared to the Cobb angles extracted from the medical files. The mean value of the two independent measurements reflects the “true” Cobb angle of the participant per X-ray at a timepoint. A difference in Cobb angle was suspected for measurements performed in supine positioning relative to a seated or standing X-ray. To uniform the sequential Cobb angle measurements in order to enable comparison between the supine and standing X-ray images, a systematic correction of 10
degrees was included for every measurement assessed in supine position.Citation24,Citation25 Subsequent Cobb angle measurements were available between 3 months and 2 years, varying per participant. The median time between the initial and subsequent spinal X-rays was 10 months (IQR: 6–16 months).
To obtain the progression of the scoliosis per half-year, the difference in Cobb angle between sequential measurements was calculated using change scores. In clinical practice, an increase of >5 suggests a progression of the curve.Citation22 However, diurnal variation, physical disabilities, walking/sitting aids, positioning during X-ray, and energy capacity of children with Rett Syndrome are likely to increase heterogeneity in X-ray images.Citation24 To take these sources of measurement error into account, the cutoff point for progression of the scoliosis was set at >10
.Citation24 Therefore, the binary outcome variable progression of scoliosis was defined as a change score exceeding a Cobb angle progression of 10
per half-year.
Predictor Variables
All potential predictors derived from the cohort were discussed in clinical expertise consensus meetings. This led to a total of 19 candidates predictor variables that were collected for all participants, of which four originated from the X-ray images. First, the Cobb angle in the frontal plane () at the initial visit to the specialist was recorded for every participant. In addition, the apex of the curve was reported, divided in high thoracic (T1–T6), low thoracic (T7–T12) and lumbar (L1–L5). Second, the Cobb angle in the sagittal plane was recorded, indicating presence of hyper kyphosis of the thoracic spine. Presence of thoracic hyper kyphosis was defined as a curve that exceeds 50
and dichotomized accordingly (yes/no). Next, the position of the hip joint was dichotomized into presence or absence of a (sub)luxation, defined as a central edge-angle larger than 15
. All variables extracted from the X-rays were assessed by the same expert raters that assessed the Cobb angle.
Further collection of candidate predictors originated from questionnaires or medical files, based on their data source being the NRSV or the MUMC+, respectively. For predictors that could fluctuate over time, initial measurement values were leading. Predictors included the continuous variables age at regression (months), age at diagnosis (years) and age at inclusion (years). The dichotomous predictor menarche (yes/no) was included due to its suggested relationship between severe scoliosis and puberty.Citation12 Another predictor that is thought to be associated with the progression of scoliosis is type of mutation on the MECP2.Citation1,Citation12,Citation26 This variable was categorized in two groups based on similarities of the phenotype: severe mutations of the MECP2 gene and mild mutations of the MECP2 gene.Citation12 Severe mutations included p.Arg106Trp, p.Thr158Met, p.Arg168X, p.Arg255X, p.Arg270X or large deletions,Citation1,Citation12,Citation26,Citation27 mild mutations included p.Arg306Cys, p.Arg133Cys, p.Arg294X and C-terminal deletions.Citation1,Citation27 Previous evidence suggests that independent walking is a protective factor for progression of scoliosis.Citation1,Citation12 Therefore, the level and quality of walking was included as predictor based on a preliminary version of the Dutch Rett Syndrome Gross Motor Scale (RSGMS-NL), as this measurement instrument was not yet developed at the time of data collection.Citation28,Citation29 The RSGMS-NL assesses gross motor abilities in children with Rett syndrome based on the level of assistance needed to perform the item. With the available data, a construct of the RSGMS-NL items “level of walking ability” and “level of sitting ability” were assessed using the dichotomized score “no assistance required” and “assistance required.”
Multiple comorbidities are prevalent in females with Rett syndrome. Constipation, low bone density, lung disorders and epilepsy were included in the model. In addition, presence of a gastro intestinal tube, vitamin-D use and a brace were included as binary predictors (present/absent). The last variable is binary and encompasses presence of a current physiotherapy treatment, as this might influence curve progression (present/absent).Citation8,Citation12
Statistical Analyses
Descriptive statistics of candidate predictors and other baseline characteristics were described as mean and standard deviation (SD) and range for continuous variables, and count and proportion for categorical variables.
Univariable logistic regression was used to assess the discriminative ability of 19 individual variables. Results were expressed as odds ratio (OR) with 95% confidence interval (CI), the p-value, and the area under the receiver operating characteristic curve (AUC). All data were analyzed using IBM SPSS version 27.
To obtain the estimated change in Cobb angle half a year after the initial first visit to the specialist for all participants, linear regression analyses were performed on a per person level on all available measurements, enabling interpolation of the Cobb angle to estimate the change score after 6 months. Hereafter, progression of the scoliosis curve was assessed based on the 6 months change scores. To prevent loss of power accompanying complete-case analysis, a simple imputation strategy (stochastic regression imputation) was used to impute missing values on candidate predictor variables.
Ethics Statement
Correspondence with the ethical committee of the general hospital Maastricht/University of Maastricht at April 30, 2021 confirmed that the Medical Research Involving Human Subjects Act (WMO) did not apply to this study (METC 2021–2615). Approval by the committee was granted.
Results
The study population consisted of 64 females with Rett syndrome between the age of 2–16 years. Characteristics are shown in . There were some values missing for low bone density (7.9%), hip subluxation (7.9%), and kyphosis (26.0%). Progression of scoliosis occurred in seven cases (10.9% during half a year). There was much heterogeneity in participants’ initial Cobb angle at baseline. The median time between the initial and subsequent spinal X-rays was 10 months (IQR: 6–16 months).
Table 1. Baseline characteristics and candidate predictors of the study cohort at inclusion.
The highest AUC (95% CI) values included: age at inclusion 0.677 (0.471–0.882), Cobb angle at baseline 0.675 (0.439–0.912) and epilepsy 0.662 (0.422–0.821). Therefore, these showed to have the highest discriminative ability and thus are the strongest predictors for rapid progression of scoliosis in Rett syndrome (). An exemplary ROC curve of the predictor Cobb angle at baseline is shown in .
Figure 2. ROC curve predictor “Cobb angle at baseline”.
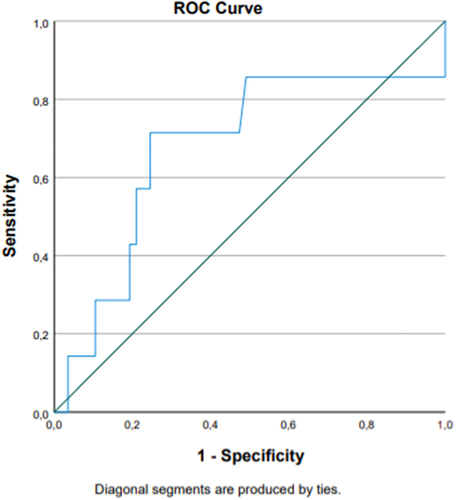
Table 2. Associations of predictor variables with progression of scoliosis.
Discussion
In this exploratory study, we estimated what predictors could be of influence on rapid progression of scoliosis. As the size of the current database is not sufficiently large for associations that are clinically relevant, this study enables predictor selection for future prediction model development for identification of rapid progression of scoliosis. Age at inclusion, Cobb angle at baseline and epilepsy were shown to have the highest discriminative ability for rapid progression of scoliosis in Rett syndrome with AUC values of 0.677, 0.675, and 0.662, respectively.
Clinical suspicion concerning progressive scoliosis in Rett syndrome is accompanied by intensive monitoring, frequent visits to the hospital, initiation of intensive conservative therapy and ultimately surgical correction, which is burdensome for both children and parents. However, clinicians as well as parents are often left in the dark about the risk of development of scoliosis after the initial visit to the specialist. This leads to uncertainty about treatment pathways and timing of interventions and leaves parents insecure. This study lays basis for a tentative prediction model that could enable identification of individuals with Rett syndrome with a high risk of rapid scoliosis progression to initiate immediate treatment. Furthermore, the model potentially decreases the need for intensive monitoring and treatment of females that are at low risk for scoliotic progression and eliminates uncertainty in parents.
The latest guidelines on the development of prediction models encourages inclusion of predictors not on statistical significance but based on expert opinion and clinical relevance 30,31To take these guidelines into account for future prediction model development, the predictors used in this study are based on the current literature base and expert opinion and are being routinely collected during Rett consultation. In this study, data was collected from two sources, enabling a good reflection of the patient population in the Netherlands.
Some challenges were present in this study. Due to the explorative nature and small sample size of the study cohort (n = 64) the statistical analysis was restricted to univariable analyses. From a statistical point of view the sample size of this study is limited, which renders statistical testing rather meaningless. The low statistical power may have caused clinical meaningful associations to go undetected. In this field however, given the rarity of the syndrome, a sample size of 64 participants is large. In addition, we were limited to the variables that were included in the combined dataset. By choosing a pragmatic approach, optimal use of all available data was enabled. The focus of this study was on assessing the discriminative ability of the predictors for future model development, therefore using univariable analyses exclusively was a suiting pragmatic solution that enabled the use of all available data.
Second, Cobb angle measurements in this study population were prone to a decreased interrater and intra-rater reliability due to physical disabilities, walking/sitting aids, variability in positioning and energy capacity. Therefore, we aimed to standardize the measurements and corrected for positioning to optimize the reliability of the Cobb angle measurements.
This study generates recommendations for future prediction model development research. In individuals with Rett syndrome one should routinely collect data concerning the age at inclusion, Cobb angle at baseline and epilepsy. A large part of the participants in both data sources lacked sequential X-ray images or included solely one X-ray. To optimize sample size in future studies, all hospitals in the Netherlands should be contacted to find all sequential X-ray images of the study population.
To optimize Cobb angle measurement in the future, X-ray positioning in individuals with Rett syndrome should be standardized. All X-rays should be performed using the same positioning considering the influence on the measured Cobb angle. Lastly, all females should undergo a total of three X-rays at their initial visit in the first year to monitor progression of scoliosis in a standardized and detailed manner. This enables creation of a more precise prediction model that could predict progression at one year after the initial visit to the specialist, without the risk on confounding on indication.
Conclusion
We explored the discriminative ability of 19 predictors to identify rapid progression of scoliosis in individuals with Rett syndrome aged 2–16 that should be collected for future prediction model development based on Dutch multi-center data. Age at inclusion, Cobb angle at baseline and epilepsy were shown to have the highest discriminative ability for rapid progression of scoliosis in Rett syndrome. Future research should focus on the development of a reliable and valid prediction model using the latest guidelines which encourage inclusion of predictors not on statistical significance but based on expert opinion and clinical relevance and should include the strongest predictors that were explored in this study.Citation30
Acknowledgments
The authors would like to express their gratitude to all the individuals and their parents and/or caregivers for participating in this study; to Tjeerd Jan van Woensel, this paper could not have been accomplished without his help; to Ellen Heerdt for her contributions during the data collection process and lastly, to Prof. Dr. van Royen and Paul van Urk for their efforts.
Disclosure Statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Downs J, Torode I, Wong K, Ellaway C, Elliott EJ, Christodoulou J, Jacoby P, Thomson MR, Izatt MT, Askin GN. et al. The natural history of scoliosis in females with rett syndrome. Spine (Phila Pa 1976). 2016 May. 41(10):856–63. doi:10.1097/brs.0000000000001399.
- Downs J, Torode I, Wong K, Ellaway C, Elliott EJ, Izatt MT, Askin GN, Mcphee BI, Cundy P, Leonard H. et al. Surgical fusion of early onset severe scoliosis increases survival in Rett syndrome: a cohort study. Dev Med Child Neurol. 2016 June. 58(6):632–38. doi:10.1111/dmcn.12984.
- Giudice-Nairn P, Downs J, Wong K, Wilson D, Ta D, Gattas M, Amor D, Thompson E, Kirrali‐Borri C, Ellaway C. et al. The incidence, prevalence and clinical features of MECP2 duplication syndrome in Australian children. J Paediatr Child Health. 2019 Nov. 55(11):1315–22. doi:10.1111/jpc.14399.
- Downs JA, Bebbington A, Jacoby P, Msall ME, McIlroy O, Fyfe S, Leonard H, Kaufmann W, Leonard H. Gross motor profile in Rett syndrome as determined by video analysis. Neuropediatrics. 2008;29(4):205–10. doi:10.1055/s-0028-1104575.
- Borst HE, Townend GS, van Eck M, Smeets E, van den Berg M, Laan A, Curfs LMG. Abnormal foot position and standing and walking ability in rett syndrome: an exploratory study. J Dev Phys Disabil. 2018;30(2):281–95. doi:10.1007/s10882-017-9585-6.
- Hagberg B. Clinical manifestations and stages of Rett syndrome. Ment Retard Dev Disabil Res Rev. 2002;8(2):61–65. doi:10.1002/mrdd.10020.
- Einspieler C, Marschik PB. Regression in Rett syndrome: developmental pathways to its onset. Neurosci Biobehav Rev. 2019 [2019 03 1]. 98:320–32. doi:10.1016/j.neubiorev.2019.01.028.
- Ager S, Downs J, Fyfe S, Leonard H. Parental experiences of scoliosis management in Rett syndrome. Disabil Rehabil. 2009;31(23):1917–24. doi:10.1080/09638280902846392.
- Sheehan DD, Grayhack J. Pediatric scoliosis and kyphosis: an overview of diagnosis, management, and surgical treatment. Pediatr Ann. [2017 Dec 1]. 46(12):e472–80. doi:10.3928/19382359-20171113-01.
- Murphy RF, Mooney JF. Current concepts in neuromuscular scoliosis. Curr Rev Musculoskelet Med. 2019 June. 12(2):220–27. doi:10.1007/s12178-019-09552-8.
- Downs J, Bergman A, Carter P, Anderson A, Palmer GM, Roye D, van Bosse H, Bebbington A, Larsson EL, Smith BG. et al. Guidelines for management of scoliosis in Rett syndrome patients based on expert consensus and clinical evidence. Spine (Phila Pa 1976). [2009 Aug 1]. 34(17):E607–17. doi:10.1097/BRS.0b013e3181a95ca4.
- Killian JT, Lane JB, Lee HS, Skinner SA, Kaufmann WE, Glaze DG, Neul JL, Percy AK. Scoliosis in Rett syndrome: progression, comorbidities, and predictors. Pediatr Neurol. 2017 May. 70:20–25. doi:10.1016/j.pediatrneurol.2017.01.032.
- Ager S, Fyfe S, Christodoulou J, Jacoby P, Schmitt L, Leonard H. Predictors of scoliosis in Rett syndrome. J Child Neurol. 2006 Sep. 21(9):809–13. doi:10.1177/08830738060210091501.
- Rumbak DM, Mowrey W, Ws S, Sarwahi V, Djukic A, Killinger JS, Katyal C. Spinal fusion for scoliosis in Rett syndrome with an emphasis on respiratory failure and opioid usage. J Child Neurol. 2016 Feb. 31(2):153–58. doi:10.1177/0883073815585352.
- Harrison DJ, Webb PJ. Scoliosis in the Rett syndrome: natural history and treatment. Brain Dev. 1990;12(1):154–56. doi:10.1016/s0387-7604(12)80200-2.
- Steyerberg E. Clinical prediction models: apractical approach to development, validation, and updating. Springer; 2009. 19.
- Pitzianti MB, Santamaria Palombo A, Esposito S, Pasini A. Rett syndrome in males: the different clinical course in two brothers with the same microduplication MECP2 Xq28. Int J Env Res Pub He. 2019;16(17):3075. doi:10.3390/ijerph16173075.
- Chahil G, Yelam A, Bollu PC. Rett syndrome in males: a case report and review of literature. Cureus. 2018;10(10):e3414–3414. doi:10.7759/cureus.3414.
- Budden SS, Dorsey HC, Steiner RD. Clinical profile of a male with Rett syndrome. Brain Dev. 2005 [2005 November 1]. 27:S69–71. doi:10.1016/j.braindev.2005.03.018.
- Leonard H, Silberstein J, Falk R, Houwink-Manville I, Ellaway C, Raffaele LS, Witt Engerström I, Schanen C. Occurrence of Rett syndrome in boys. J Child Neurol. 2001 May 01. 16(5):333–38. doi:10.1177/088307380101600505.
- Stokes I. Three-dimensional terminology of spinal deformity. Scoliosis Research Society; https://www.srs.org/professionals/online-education-and-resources/glossary/three-dimensional-terminology-of-spinal-deformity#40.
- Chockalingam N, Dangerfield PH, Giakas G, Cochrane T, Dorgan JC. Computer-assisted Cobb measurement of scoliosis. Eur Spine J. 2002 Aug. 11(4):353–57. doi:10.1007/s00586-002-0386-x.
- Tanure MC, Pinheiro AP, Oliveira AS. Reliability assessment of Cobb angle measurements using manual and digital methods. Spine J. 2010 Sep. 10(9):769–74. doi:10.1016/j.spinee.2010.02.020.
- Kim H, Kim HS, Moon ES, Yoon C-S, Chung T-S, Song H-T, Suh J-S, Lee YH, Kim S. Scoliosis imaging: what radiologists should know. Radiographics. 2010 Nov. 30(7):1823–42. doi:10.1148/rg.307105061.
- Torell G, Nachemson A, Haderspeck-Grib K, Schultz A. Standing and supine Cobb measures in girls with idiopathic scoliosis. Spine (Phila Pa 1976). 1985 June. 10(5):425–27. doi:10.1097/00007632-198506000-00004.
- Percy AK, Lee HS, Neul JL, Lane JB, Skinner SA, Geerts SP, Annese F, Graham J, McNair L, Motil KJ. et al. Profiling scoliosis in Rett syndrome. Pediatr Res. 2010 Apr. 67(4):435–39. doi:10.1203/PDR.0b013e3181d0187f.
- Cuddapah VA, Pillai RB, Shekar KV, Lane JB, Motil KJ, Skinner SA, Tarquinio DC, Glaze DG, McGwin G, Kaufmann WE. et al. Methyl-CpG-binding protein 2 (MECP2) mutation type is associated with disease severity in Rett syndrome. J Med Genet. 2014 Mar. 51(3):152–58. doi:10.1136/jmedgenet-2013-102113.
- Downs J, Stahlhut M, Wong K, Syhler B, Bisgaard A-M, Jacoby P, Leonard H. Validating the Rett syndrome gross motor scale. PLoS One. 2016;11(1):e0147555. doi:10.1371/journal.pone.0147555.
- Borst H, Weeda J, Downs J, Curfs L, de Bie R. The rett syndrome gross motor scale - dutch version (RSGMS-NL) can reliably assess gross motor skills in dutch individuals with rett syndrome. Dev Neurorehabil. 2022 Feb. 25(2):133–39. doi:10.1080/17518423.2021.1960920.
- Wynants L, Collins GS, Van Calster B. Key steps and common pitfalls in developing and validating risk models. Bjog. 2017 Feb. 124(3):423–32. doi:10.1111/1471-0528.14170.