
ABSTRACT
Background
Dancing is an attractive form of exercise among older adults and may positively influence physical and psychosocial health. The aim of this systematic review was to synthesize the evidence examining the dance prescription and effectiveness of dance in community dwelling older adults.
Methods
Eight databases were searched to identify randomized controlled trials that evaluated the effectiveness of dance programs on community-dwelling older adults from 2007 to December 2020. Data regarding participants, dance programs and outcomes of interest were extracted and narratively synthesized. A meta-analysis was performed on the outcome data where possible.
Results
Twenty-two studies met the inclusion criteria, of those 15 were deemed to be fair quality and 7 high quality using the PEDro scale. Nineteen studies included in the meta-analysis found that dancing can improve mobility and endurance compared to no intervention and afforded equivalent outcomes compared to other exercise programs.
Conclusion
The findings suggest that dance is an effective, safe and viable activity for community-dwelling older adults..
Introduction
Many societies have an ageing population; it is estimated that by 2050, one in six people will be aged 60 years or older (WHO, Citation2016). Most adults (92%) aged 65 years or older have at least one chronic condition, with a significant proportion (62%) presenting with multiple morbidities (Macera et al., Citation2017). If unprecedented demand and pressure on healthcare systems is to be avoided, it is imperative that older adults are encouraged to take an active role in delaying the onset or progression of chronic conditions (WHO, Citation2016).
A growing body of evidence demonstrates that physical activity has multiple health benefits including the prevention and treatment of many chronic diseases and conditions (Hayes & Kriska, Citation2008). Physical activity guidelines recommend that adults aged 65 years and over partake in multi-component recreational activities that include balance training, aerobic exercise and muscle strengthening (Piercy et al., Citation2018). An appropriate dosage and type of physical activity can improve maximal oxygen uptake (Sagiv et al., Citation2010), muscle power, balance (Marques et al., Citation2011), bone density (Bemben & Bemben, Citation2011) and reduce oxidative stress linked to cardiovascular disease in older adults (Roque et al., Citation2013). Studies also show that physical activity has a positive effect on the cognitive health of older adults. Busse et al. (Citation2009) found improvements in attention, cognitive speed, executive functioning, working memory and episodic memory. Hence, an optimally prescribed physical activity program can positively impact the quality of life and physical function of individuals globally. Physical activity, particularly group based, can also provide social connection and lessen the lived-experience of loneliness and social isolation among older adults (Komatsu et al., Citation2017).
Despite the known benefits of physical activity, research suggests that physical inactivity increases with age, with the majority of older adults not meeting the recommended levels of physical activity each week (Bennie et al., Citation2019). Physical inactivity can have a detrimental effect on physical function (Warburton et al., Citation2006) and psychosocial wellbeing (Blanchet et al., Citation2018). Functional decline can result in reduced participation in community activity (Tomioka et al., Citation2015) social isolation and loneliness (Ward et al., Citation2019), with loneliness a significant risk factor for poor health outcomes (Perissinotto et al., Citation2012). Prior to the coronavirus (COVID-19) pandemic, almost one-third of adults aged 50+ in Ireland reported loneliness, which was found to be most prevalent among those over 75 years and those living alone (Ward et al., Citation2019). The unprecedented consequences of the COVID-19 pandemic resulted in limited social contact, reduced physical activity levels and increased sedentary behavior, which can lead to deconditioning, balance deficits, increased falls risk and worsening and/or new mental health problems (De Biase et al., Citation2020), thus increasing the likelihood for further deconditioning, and psychological and cognitive decline. Thus, the consequences of the pandemic have augmented the need for physical activity programs that are effective, fun and support social connectedness for older adults.
Dancing is an attractive and enjoyable form of group-based physical activity among many older adults (Moss et al., Citation2015). Systematic reviews have found that dance can improve physical health with positive effects reported for strength, endurance, functional fitness and some risk factors associated with falls including balance and mobility (Fernández-Argüelles et al., Citation2015; Hwang & Braun, Citation2015; X. Liu et al., Citation2021). Currently, the findings are mixed for gait outcomes (Fernández-Argüelles et al., Citation2015; X. Liu et al., Citation2021). Additionally, a comprehensive review identified that dance and dance movement therapy can improve depression, anxiety, quality of life, interpersonal, cognitive and psychomotor skills (Koch et al., Citation2019).
Given this, research evidence suggests that dance can substantially improve not only physical function but also psychosocial outcomes and cognitive function. Dance may facilitate improvements in cognition through active engagement in physical activity, which has been shown to ameliorate thinking, memory and mood (Mandolesi et al., Citation2018). In addition, learning new motor skills and socialization that are integral to dance participation may contribute to enhancing cognitive function (Kattenstroth et al., Citation2010). These positive effects may enhance psychological wellbeing and encourage long-term participation (Devereux-Fitzgerald et al., Citation2016). While prior reviews on dance for older adults are available (Fernández-Argüelles et al., Citation2015; Hwang & Braun, Citation2015; Xuegang Liu et al., Citation2020; McNeely et al., Citation2015), an updated synthesis is required that includes a detailed examination of the dance intervention exercise prescription and meta-analysis on the main outcomes of interest. Exercise prescription in this context refers to the content of a dance intervention designed to improve health outcomes in older adults. Currently, there is insufficient evidence to inform the prescription and subsequent implementation of effective dance programs for older adults. Several national and international organizations provide guidelines for how to prescribe exercise to improve health. However, to the authors’ knowledge, no published review has explored the literature on dance for older adults in the context of the American College of Sports Medicine (ACSM) recommendations and Physical Activity Guidelines for Americans (PAGA) for older adults (Chodzko-Zajko et al., Citation2009; Piercy et al., Citation2018). The ACSM and PAGA recommend that older adults participate in aerobic, strength, balance and flexibility exercise (Chodzko-Zajko et al., Citation2009; Piercy et al., Citation2018) and different dance genres can offer variable amounts of these forms of exercise. We aim to synthesize the literature evaluating the benefits of dance, identify the exercise prescription of the dance programs according to the ACMS guidelines and the components of each dance program according to the FITT principle (Power & Clifford, Citation2013) by examining the frequency, intensity, duration and type of each dance program.
Thus, the primary aim of this review is to provide a descriptive account of the dance programs and potential benefits of dance for older adults. The review sought to answer the following questions:
What are the frequency, intensity, duration and type of dance programs designed for older adults?
Is dance as effective as other forms of physical activity and more effective than no intervention for improving gait, balance, functional mobility, endurance, flexibility, cognitive function, mood, social isolation and loneliness in older adults?
Methods
The methods of this review conform to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Moher et al., Citation2009).
Inclusion criteria
Study Design: Randomized controlled trials (RCTs) published in the English language (2007–2020) that evaluated the effectiveness of a dance programs on community-dwelling people were included. Participants: Studies that included participants 60 years or older and assessed using at least one of the key outcomes of interest (gait, balance, functional mobility, endurance, flexibility, mood, cognitive function, social isolation and loneliness). Intervention: Studies were included if they reported at least four of the following intervention characteristics: the frequency of the dance classes, the exercise intensity, the duration of the program and the duration of each dance class and the dance genre. Comparisons: the comparator group could be either no intervention or some other form of physical activity.
Exclusion criteria
Studies that were specifically designed to include specific cohorts of people only, for example, those with a neurological (e.g. Parkinson’s disease) cardiopulmonary (e.g. chronic obstructive pulmonary disease) or orthopedic condition were excluded. Studies were also ineligible if they examined dance as an adjunct to another therapy or dance movement therapy as a form of dance.
Literature search
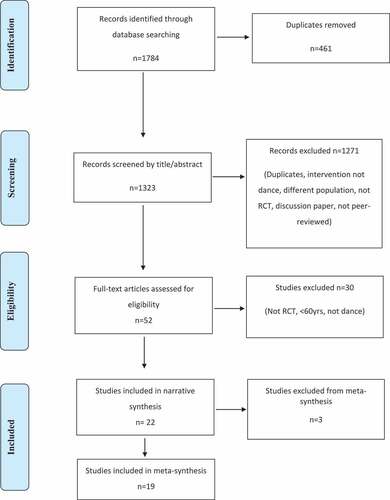
An electronic search was carried out in Embase and EBSCO to search (AMED, Academic Search Complete, CINAHL, MEDLINE, SPORTDiscus, PsychARTICLES and PsychINFO). The search was performed originally to identify eligible articles published from 2007 to January 2019 and again for any recent articles from January 2019 to December 2020. The search terms used were “dance OR dancing” AND “elderly OR aged OR older OR elder OR geriatric OR old OR senior”. Limiters used were study design: RCT and year. Articles retrieved were screened by title and abstract and potentially eligible studies were read by full text. The articles retrieved were initially screened by title. Articles deemed unsuitable clearly stated that the intervention, population or study design were inappropriate for this review. Articles with relevant titles were read by abstract to examine details provided for population, study design, intervention and outcome measures. Any articles that did not meet the inclusion criteria were eliminated at this stage and the remaining articles were examined by full text. A standardised screening checklist, that listed all the inclusion and exclusion criteria, was used to determine an article’s suitability for inclusion. Two reviewers independently completed the original search (JS and MO’G) and one reviewer independently completed the updated search (JMK). Any uncertainties or disagreements were discussed and resolved a second reviewer on both occasions (AC). Any queries about an articles methods or data were confirmed by emailing the authors. Figure A PRISMA flow diagram provides a summary of the search process and Appendix 1 provides an example of a search strategy.
Data extraction
Standardized data extraction forms were used to extract information on participants’ demographics and key outcomes of interest. Characteristics on the dance programs were extracted in the frequency, intensity, duration and type (FITT) format. FITT is a standardized framework used to describe the characteristics and dosage of activity programs. Dance genres were categorized as aerobic, balance, strength or flexibility exercise. Relevant data for the key outcomes of interest including measures of centrality and variability were also extracted.
Outcomes
Primary outcomes of interest included gait, balance, functional mobility, endurance, flexibility, mood, cognitive function, social isolation and loneliness. Due to variability in the measurement tools used in the reviewed studies, only data for the listed physical and psychological measurement tool were extracted. There was broad variability of measurement tools used for cognitive outcomes; therefore, data reported for any tool that measured cognitive outcomes were extracted.
Quality assessment
Quality of the included RCTs was appraised with the PEDro scale (Sherrington et al., Citation2000; displayed in Appendix 2) by two reviewers (TC and JMK), and any uncertainties were discussed with a third reviewer (AC). In addition, a proportion were cross-checked for accuracy resulting in two changes. This is a validated scale used in the completion of previous systematic reviews, including reviews in the area of dance (Aguiar et al., Citation2016; Macedo et al., Citation2010; Maher et al., Citation2003; Shanahan et al., Citation2015).
Data analysis
The effects of dance and the control group were compared using meta-analyses. Analysis required a standardized mean difference (SMD) to be computed, as studies used a number of different measures to measure and report each outcome. A random-effects model was selected for all analyses a priori (Higgins et al., Citation2008). In studies where multiple contrasts were examined (e.g. dancing exercise group compared to stretching exercise group compared to walking group), the sample size in the shared comparison was halved in order to avoid double counting of participants in the analyses. To avoid the dependence of the effect sizes, one effect size per study was selected. We choose the most commonly used outcome measure used among the studies. When a study used a different set of outcome measures, the primary outcome measure from that study was chosen. Pooled 95% confidence intervals (CIs) were computed for standard mean deviation (SMD), and CIs excluding zero were considered statistically significant. Heterogeneity between studies was assessed from the Forest plots, using formal Q-tests (χ2 test statistic and p value) and the I2 statistic. Substantial heterogeneity was determined using the cutoff point I2 ≥ 50%. All analyses were conducted in Review Manager 5.2.
Results
Figure A demonstrates the PRISMA flow diagram. A total of 1090 community-dwelling older adults participated across the 22 studies included in this review. Extracted data are presented for each of the included studies (). Sample sizes ranged from 21 to 115 participants.
Table 1. Study characteristics, program components.
Four of the 22 studies included female participants only (Cepeda et al., Citation2015; Cruz-Ferreira et al., Citation2015; Noopud et al., Citation2019; Rodrigues-Krause et al., Citation2018) and the remaining studies included both males and females, with the majority (80%) of study participants female across most studies that reported gender. The trials were conducted across a wide range of countries and cultures from Canada (McKinley et al., Citation2008), Faroe Islands (Hofgaard et al., Citation2019), Thailand (Areeudomwong et al., Citation2019; Janyacharoen et al., Citation2013; Noopud et al., Citation2019), Australia (Merom et al., Citation2016), Czech Republic (Sejnoha Minsterova et al., Citation2020), Germany (Granacher et al., Citation2012; Hamacher et al., Citation2015; Rehfeld et al., Citation2018, Citation2017), the USA (Aguiñaga & Marquez, Citation2019; Bennett & Hackney, Citation2018; Franco et al., Citation2020; Krampe, Citation2013), Greece (Giorgos Sofianidis et al., Citation2009), Portugal (Cruz-Ferreira et al., Citation2015) and Brazil (Cepeda et al., Citation2015; Rodrigues-Krause et al., Citation2018) and South Korea (Joung et al., Citation2019).
Quality of included studies:
Fifteen studies were of fair quality (4–5/10); and the remaining seven studies were deemed to be of good quality (6–8/10; Cashin & McAuley, Citation2020) using the Physiotherapy Evidence Database Scale (PEDro; Database, Citation1999) detailing the PEDro results can be found in Appendix 2.
Dance prescription:
The frequency, intensity, time (i.e. duration) and type (FITT) of each dance intervention is displayed ().
Frequency:
The number of classes per week varied from a single weekly class to three weekly classes across studies, with the most common frequency of twice weekly.
Intensity:
Units of measurement for intensity varied greatly across studies. Twelve studies did not report any measurement of intensity. Two studies (Müller et al., Citation2017; Giorgos Sofianidis et al., Citation2009) measured intensity as a percentage of maximum heart rate ranging from 50% to 80% between the two studies. Two studies (Rehfeld et al., Citation2018; Rodrigues-Krause et al., Citation2018) used a percentage of maximal oxygen uptake (VO2 max) as a measure of intensity (range 59–69% VO2 max). One study used the BORG Scale (range 11–14; Sejnoha Minsterova et al., Citation2020) and another (Cepeda et al., Citation2015) used a combination of the BORG Scale (range 12–15) and HR reserve (range 60–70%). Other methods were using tempo (beats per minute; Hofgaard et al., Citation2019) or the descriptor moderate intensity (Franco et al., Citation2020).
Time and Duration:
The length of each class ranged from 0.5 to 2 hours. Five studies provided classes that lasted less than 1 hour (Areeudomwong et al., Citation2019; Cruz-Ferreira et al., Citation2015; Hofgaard et al., Citation2019; Janyacharoen et al., Citation2013; Krampe, Citation2013). Eleven studies provided one-hour classes (Aguiñaga & Marquez, Citation2019; Bennett & Hackney, Citation2018; Cepeda et al., Citation2015; Franco et al., Citation2020; Granacher et al., Citation2012; Merom et al., Citation2016; Noopud et al., Citation2019; Rodrigues-Krause et al., Citation2018; Sejnoha Minsterova et al., Citation2020; George Sofianidis et al., Citation2017; Giorgos, Citation2009). Five studies provided 1.5-hour classes (Hamacher et al., Citation2015; Joung et al., Citation2019; Müller et al., Citation2017; Rehfeld et al., Citation2018, Citation2017) and one study’s class duration was 2 hours (McKinley et al., Citation2008). The duration of the intervention varied from 4 weeks to 18 months. The most common program durations were 8 weeks (Bennett & Hackney, Citation2018; Cepeda et al., Citation2015; Granacher et al., Citation2012; Joung et al., Citation2019; Rodrigues-Krause et al., Citation2018) and 6 months (Cruz-Ferreira et al., Citation2015; Hamacher et al., Citation2015; Rehfeld et al., Citation2018; Sejnoha Minsterova et al., Citation2020; George Sofianidis et al., Citation2017). The most common dosage was 22 hours; however, there was a significant variability between studies, ranging from a minimum of 6 hours to a maximum of 144 hours.
Type:
A broad range of dance genres were noted across the studies from ballroom dancing (Cepeda et al., Citation2015; Merom et al., Citation2016) Thai dance (Janyacharoen et al., Citation2013; Noopud et al., Citation2019) Greek dance (Giorgos Sofianidis et al., Citation2009), Tango (McKinley et al., Citation2008), Latin dance (George Sofianidis et al., Citation2017), line dancing (Bennett & Hackney, Citation2018), creative dance (Cruz-Ferreira et al., Citation2015; Joung et al., Citation2019), Salsa (Aguiñaga & Marquez, Citation2019; Granacher et al., Citation2012) and the Lebed method (Krampe, Citation2013). Thai boxing dance (Areeudomwong et al., Citation2019), Folk (Franco et al., Citation2020), Faroese chain dance (Hofgaard et al., Citation2019) and mix of Folk, Country, African, Greek and Tango (Sejnoha Minsterova et al., Citation2020). Six (Hamacher et al., Citation2015; Müller et al., Citation2017; Rehfeld et al., Citation2018, Citation2017; Rodrigues-Krause et al., Citation2018; Sejnoha Minsterova et al., Citation2020) studies offered a combination of different dance genres (see ). Different genres offered different exercise types. All had a significant connection to music. All interventions involved some stepping activity, where stepping sequences were taught and performed to music.
Dance components:
The dance interventions could be classified as aerobic dance, social dance, traditional dance, creative dance or a combination of these genres. All studies had a particular dance structure or codified dance vocabulary. The salient characteristics of these dance types are varied although all interventions offered different levels of difficulty and the possibility to increase level progressively. demonstrates that the majority of dance programs (n = 19) included aerobic and balance components and over half (n = 13) provided strengthening and flexibility components; separate from or part of the warm-up or cool-down. The intervention in nine (Cepeda et al., Citation2015; Franco et al., Citation2020; Granacher et al., Citation2012; Hofgaard et al., Citation2019; Joung et al., Citation2019; McKinley et al., Citation2008; Merom et al., Citation2016; Sejnoha Minsterova et al., Citation2020; Giorgos Sofianidis et al., Citation2009) studies implemented a component of partnered dancing. Partnering is a key component of ballroom, Tango, Latin and Salsa and dancers dance in very close proximity to each other. Several studies included dance that required participants to stand in either a circle or semi-circle holding hands while performing the dance interventions. Some of the dance genres, including Thai, Faroese Chain dance, African dances, a range of folk dances and Greek dance, were culturally significant within their own countries. Line dancing provided a certain kinesthetic empathy through shared rhythmic energy and proprioception even though there is no actual physical contact. Creative dance offered an opportunity for self-expression and creativity through dance. Opportunities for improvization were possible in some of the social dance types. Lebed used activities and exercises prescribed by the physiotherapist to music and presented as a dance activity with set structured sequences and motifs.
Feasibility: dropout and compliance
Attendance rates for the dance interventions ranged from 60% to 100%, with majority of the studies reporting attendance rates above 80% (). Intention to treat was performed in a minority of studies (N = 4). In studies that compared dance to active controls the attendance rates were matched (Areeudomwong et al., Citation2019; Hamacher et al., Citation2015; McKinley et al., Citation2008; Müller et al., Citation2017; Rehfeld et al., Citation2018, Citation2017; George Sofianidis et al., Citation2017). Dropout rates were similar in the dance compared to active control groups. Attrition rates in the dance groups ranged between 0% and 53.9%, with 14 studies reporting attrition rates less than 20%.
Table 2. Feasibility measures, dropouts, attrition and participation in each intervention .
Table 3. Summary of meta-analysis findings for key outcomes of interest.
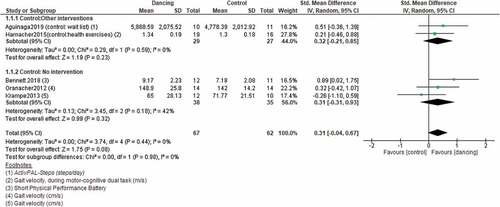
Effects of Dancing versus Control on Gait
Five of the six studies that investigated the effects of dance on gait () were included in a meta-analysis. The subgroup analyses show that dance was marginally insignificant when comparing dance to other interventions and no intervention. The overall effects of dance on gait shows borderline (lower confidence interval is −0.04- see ) favorable effects of dance on gait. Small I2 values indicate that statistically heterogeneity was low for the RCTs at follow-up for gait (I2 = 0%, p = 0.44).
Figure 1. Forest plot of Dancing versus control for Gait.
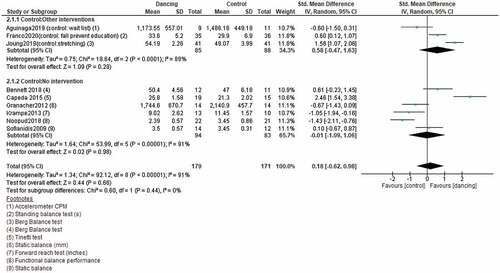
Effects of dancing versus control on balance
Nine out of 12 studies that reported balance-related outcomes were included in the meta-analysis indicates no statistical difference for dance compared to other interventions for improving balance; hence, dance interventions yielded similar balance outcomes compared to other interventions (indicated in ). Dance was however not statistically significant different from no intervention in improving balance (). Large I2 values indicate that statistically heterogeneity was considerably high for the RCTs at follow-up for balance (I2 = 91%, p < 0.001).
Figure 2. Forest plot of dancing versus control for balance.
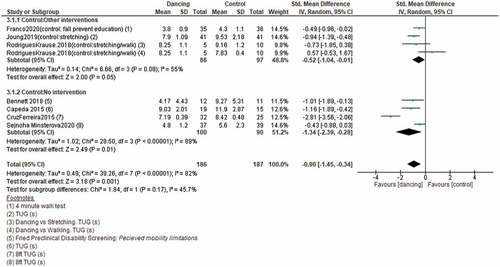
Effects of dancing versus control on mobility
Seven of the eight studies that reported outcomes related to mobility were included in the meta-analysis. shows that dance was significantly better in improving mobility when compared to other interventions () and no control interventions. The overall effect of dance compared to no control intervention was larger than the pooled effect of dance compared to other forms of physical activity. The TUG was the most common outcome measure used to assess functional mobility. Significant statistical heterogeneity was however noted.
Figure 3. Forest plot of dancing versus control for mobility.
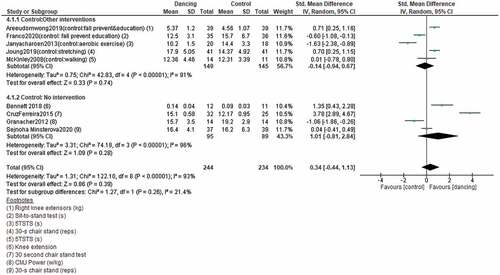
Effects of dancing versus control on strength
Nine of the 11 studies that investigated the effects of dance on strength were included in a meta-analysis (). The subgroup analysis in shows no significant difference between dance and other forms of exercise; hence, dance has similar effects on muscle strength compared to other interventions. Dance was however not statistically better in improving strength compared to no intervention. Large I2 value highlights statistically heterogeneity for this meta-analysis.
Figure 4. Forest plot of dancing versus control for strength.
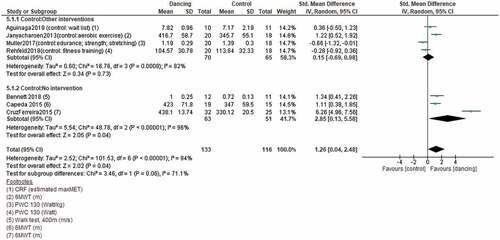
Effects of dancing versus control on endurance
Seven of the nine studies that investigated the effects of dance on endurance were included in a meta-analysis. shows that there was no significant difference in endurance between dance and other forms of exercise (see subgroup analysis). The effect of dance on endurance was statistically better compared to no intervention. The overall effect was also statistically favorable for dance interventions. Large I2 values indicate that statistical heterogeneity was considerably high for the RCTs at all follow-up for endurance.
Figure 5. Forest plot of dancing versus control for endurance.
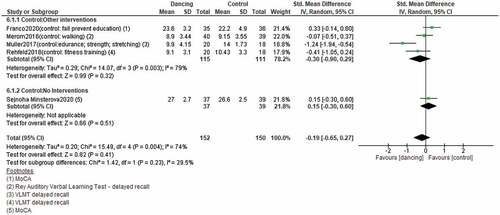
Effects of dancing versus control on cognition
Five studies investigated the effects of dance on cognition (). The subgroup analysis shows that the effect of dance on cognition was not statistically significantly different compared to other exercise interventions. One study compared dance to no intervention and showed statistical insignificance. Statistically heterogeneity was high for the RCTs at follow-up for cognition (I2 = 74%, p = 0.004).
Figure 6. Forest plot of dancing versus control for cognition.
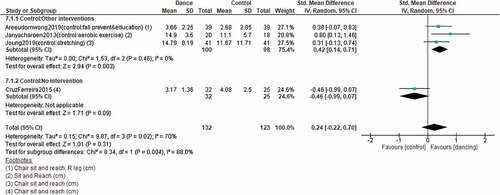
Effects of Dancing versus Control on Flexibility
Effects of dancing versus control on flexibility Four studies investigated the effects of dance on flexibility, of which all were included in the meta-analysis (). As evident in dance was significantly better in improving flexibility compared to other interventions. Only one study compared dance to no intervention and the outcome showed no statistical insignificance. The overall pooled effect also showed no significant difference. Large I2 values indicate that statistically heterogeneity was high (I2 = 70%, p = 0.02).
Figure 7. Forest plot of dancing versus control for flexibility.
Summary of meta- analyses
illustrates that dance did not perform statistically significant worse in any of the comparisons included in the meta-analyses. Dance was either equivalent (no statistical difference) or superior (dance statistically significantly better) compared to the control condition.
Discussion
This review identified substantial variation between the characteristics of the studies included in this review, in terms of study quality, numbers of participants, the dance program characteristics and dance genre. The overall dosage of the interventions varied greatly from a minimum of 6 hours to maximum of 144 hours (median 24 hours). An assortment of dance genres was implemented; each genre was aerobic in nature with most including strength, balance and flexibility components to varying degrees.
Statistically significant improvements were found in functional mobility following participation in the dance intervention, where dance compared favorably to no intervention and other forms of physical activity. The quality of these studies ranged from 4 to 8 on the PEDro Scale. The dance genres also varied, but all programs included aerobic, strength and balance components. Notably, one study reported greater improvements in mobility following participation in the control walking program (Rodrigues-Krause et al., Citation2018), which may be explained by participation in task-oriented motor skill training resulting better task performance (Brach & VanSwearingen, Citation2013) of the Timed up and Go (TUG). Indeed, the TUG was the most commonly used measure of mobility across the studies, which is a reliable and useful outcome measure, as TUG scores (adjusted for age, gender, comorbidities, medications and past history of two falls) are associated with future falls in older adults (Kojima et al., Citation2015).
This study also found significant improvements in endurance following dance, most commonly assessed using the six-minute walk test, a valid measure of functional exercise capacity and endurance. Dance was found to be significantly more effective compared to no intervention and equivalent to the control programs that included elements of strength and endurance training. Thus, similar to the findings of previous research, dance is better than no intervention and equally as good to other forms of exercise for improving aerobic capacity (Hwang & Braun, Citation2015; Xuegang Liu et al., Citation2020). The key studies that identified significant improvements in endurance were mostly of good quality, but varied greatly in total program duration (12–60 hours) and genre (Thai, Ballroom, Line and Creative Dancing).
Improvements in balance were found to be equivalent to the control or physical activity programs offered. The outcome measures used varied significantly across the studies. Although the dance genres differed significantly between the studies, most programs consisted of a balance component, thus it would be expected that improvements in balance would be demonstrated following increased participation. However, the frequency, duration and dosage of the dance interventions varied among the studies. Four of the included studies identified improvements in balance following participating in dance for an average of 22 hours (range, 16–24 hours), when compared to either no intervention, education or a stretching program. Genres varied from line dancing, ballroom, rhythmic folk and creative dance. In contrast, four studies did not identify significant improvements in balance following participation in various dance programs (mean, 18 hours; range, 10.5–32 hours). The dance genres included in these studies were the Merengue, Cha Cha Cha, Salsa, Lebed and Thai dance. Thus, it is recommended that duration and dance movement components are considered when designing a dance program to optimize balance as, for example, 10.5 hours of Thai dance did not lead to improvements in balance compared to 24 hours of ballroom dancing, which did. To target balance, dance programs should include sufficient balance activities that safely and progressively reduce the base of support, such as walking in the tandem position, on toes, on heels and sideways, as well as static standing while on one leg and in the tandem position (Madureira et al., Citation2007). It is recommended that individuals involved in the intervention design should consider the movement components of the dance program prescribed to ensure balance is sufficiently challenged and progressed in line with each individual’s capacity. Research in falls prevention (Sherrington et al., Citation2011) identified that balance exercise should be moderately to highly challenging and undertaken for 2 hours a week for at least 6 months (>50 hour dose) to have the greatest effect on balance and falls prevention. Thus, future research in dance could consider these findings and recommendations if the primary aim of the dance program is to prevent falls in at risk older adults.
Multi-component exercise interventions that include strength, balance and endurance were reported to have the most beneficial effect on strength in the older population (Cadore et al., Citation2013). Dance is a multi-component exercise activity; however, the results of this review found equivalent strength gains following participation in the dance intervention and the control. It is plausible that the intensity of the dance intervention may have been too low to achieve greater strength gains. Research recommends that older adults participate in strength training twice per week at an intensity of 50–85% repetition maximum (Fragala et al., Citation2019). Hence, it is plausible that some dance genres may not achieve sufficient intensity due to the dynamic nature of the activity and bias toward aerobic activity. Strength training may need to be considered during the program design stage or undertaken as a separate activity in order to achieve the required exercise dosage to have an effect on muscle strength. Although the results marginally favored dance compared to the control for gait and cognition, no statistically significant differences were found. Thus, in support of the wider scholarship in the field, we contend that dance may have the potential to maintain or improve cognitive function (Brown et al., Citation2006; Meng et al., Citation2020). The reason for marginal improvements found in this study may be due to the number of studies in the analyses were small and more research may be needed. In addition, dance was compared to other forms of physical activity, which has strong evidence to support its positive biological and psychological effects (Mandolesi et al., Citation2018), which may explain minimal differences between the groups. Only one study assessed the effect of dance on quality of life and no study examined the effect of dance on mood, loneliness or social isolation. Thus, these outcomes could not be assessed. It is recommended that future studies assess the effect of dance on loneliness or social isolation as the health risks associated with loneliness and social isolation are comparable to the dangers of smoking and obesity (Cacioppo et al., Citation2015). Depression and anxiety in older adults are often linked to retirement and may be exacerbated by loneliness, reduced health or loss of social groups. The prevalence of mental health problems may be greater than 50% in the older population and can negatively impact quality of life (Curran et al., Citation2020). Thus, reaffirming the need for future research to include psychosocial measures to assess if arts-based programs can beneficially target physical and emotional aspects of health.
It is essential to carefully select the music accompaniment in accordance with the session’s theme and the participants’ preferences. Different styles of music were used, such as classic, jazz, pop, ethnics, Greek, Portuguese traditional and instrumental music. The significance of music and dancing to specific rhythms and musical beats is highlighted in several of the studies (Areeudomwong et al., Citation2019; Cepeda et al., Citation2015; Cruz-Ferreira et al., Citation2015; Krampe, Citation2013). The complex integration of sensory inputs and rhythm may enhance the benefits gained and provide cultural context to optimize social and group cohesion (Dhami et al., Citation2014). Music can also have an important role in supporting positive aging by improving emotion, increasing social interaction and decreasing social isolation (Hays & Minichiello, Citation2005), which may help to optimize adherence to the dance program.
The average attendance rate among the dance groups are higher than reported in non-dance exercise interventions in older adults (reported as 58–77%; Rivera-Torres et al., Citation2019). Unfortunately, adherence levels were not reported in some studies. This data is required to enable accurate comparisons across studies to establish if adherence is linked to the results of the analysis or if specific dance styles had greater participation. Where reported, dropout rates in the dance groups were slightly higher than reported in aquatic exercise (0–41%) and other land-based exercises (0–36%; Waller et al., Citation2016). The findings indicate that both dropout and attendance rates may be negatively influenced by factors such as duration and if multiple dance genres are taught in one program. Devereux-Fitzgerald et al. (Citation2016) reported that older adults are motivated to participate in activities that promote skill attainment, thus teaching multiple dance genres may be a barrier to accomplishment and continued participation in a program. To encourage older adults to exercise regularly research has found that programs need to be suitable for the individuals’ physical abilities and promote continued support, enjoyment and self-efficacy and social cohesion (O’Regan et al., Citation2020).
At the time of the original search the updated 2020 PRISMA was not published, and thus the original PRISMA was used; however, it is recommended the updated PRISMA 2020 is used in future reviews (Page et al., Citation2021; Yepes-Nuñez et al., Citation2021). The wide variation in quality of the studies and heterogeneity in outcome measures made it more difficult to compare across studies. In addition, the number of studies and pooled sample sizes were relatively small. A gender imbalance was also evident, with women making up the majority of participants in most of the studies. This affects the transferability of the findings to the male population. Hence, future studies should actively engage in public and representative groups to ensure participation of both genders and ensure the study recruitment material is gender sensitive. No study included participants in the design of the dance intervention, which may influence ownership, longer-term participation and sustainability. It is recommended that future studies report the dance prescription adequately to enable further exploration of associations between the dance prescription and improvements in outcome measures post-intervention.
This results of this study suggest that dance is a safe and viable exercise intervention for community-dwelling older adults. Currently, it is not evident which genre of dance is the most effective, however cultural context and participant preference should be considered along with an exercise prescription that is informed by existing literature in falls prevention and physical activity. Further, high-quality RCTs should be conducted using a core set of outcome measures to ensure comparability. There is scope for future studies to investigate the effectiveness of evidence and participant informed dance programs to align with guidelines, participant preference and context. Additionally, studies should attempt to include both men and women as the available evidence is biased towards women and thus limiting translation to practice more widely.
Appendix_2.docx
Download MS Word (17 KB)Appendix_1.docx
Download MS Word (14.5 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Supplementary material
Supplemental data for this article can be accessed online at https://doi.org/10.1080/17533015.2022.2093929
Additional information
Funding
References
- Aguiar, L. P. C., da Rocha, P. A., & Morris, M. (2016). Therapeutic dancing for Parkinson’s disease. International Journal of Gerontology, 10(2), 64–70. https://doi.org/10.1016/j.ijge.2016.02.002
- Aguiñaga, S., & Marquez, D. X. (2019). Impact of Latin dance on physical activity, Cardiorespiratory fitness, and sedentary behavior among latinos attending an adult day center. Journal of Aging and Health, 31(3), 397–414. https://doi.org/10.1177/0898264317733206
- Areeudomwong, P., Saysalum, S., Phuttanurattana, N., Sripoom, P., Buttagat, V., & Keawduangdee, P. (2019). Balance and functional fitness benefits of a Thai boxing dance program among community-dwelling older adults at risk of falling: A randomized controlled study. Archives of Gerontology and Geriatrics, 83(July–August 2019), 231–238. https://doi.org/10.1016/j.archger.2019.04.010
- Bemben, D., & Bemben, M. (2011). Dose–response effect of 40 weeks of resistance training on bone mineral density in older adults. Osteoporosis International, 22(1), 179–186. https://doi.org/10.1007/s00198-010-1182-9
- Bennett, C. G., & Hackney, M. E. (2018). Effects of line dancing on physical function and perceived limitation in older adults with self-reported mobility limitations. Disability and Rehabilitation, 40(11), 1259–1265. https://doi.org/10.1080/09638288.2017.1294207
- Bennie, J. A., De Cocker, K., Teychenne, M. J., Brown, W. J., & Biddle, S. J. H. (2019). The epidemiology of aerobic physical activity and muscle-strengthening activity guideline adherence among 383,928 U.S. adults. The International Journal of Behavioral Nutrition and Physical Activity, 16(1), 34. https://doi.org/10.1186/s12966-019-0797-2
- Blanchet, S., Chikhi, S., & Maltais, D. (2018). The benefits of physical activities on cognitive and mental health in healthy and pathological aging. Geriatrie et psychologie neuropsychiatrie du vieillissement, 16(2), 197–205. https://doi.org/10.1684/pnv.2018.0734
- Brach, J. S., & VanSwearingen, J. M. (2013). Interventions to improve walking in older adults. Current Translational Geriatrics and Experimental Gerontology Reports, 2(4), 230–238. https://doi.org/10.1007/s13670-013-0059-0
- Brown, S., Martinez, M. J., & Parsons, L. M. (2006). The neural basis of human dance. Cerebral Cortex, 16(8), 1157–1167. https://doi.org/10.1093/cercor/bhj057
- Busse, A. L., Gil, G., Santarém, J. M., & Jacob Filho, W. (2009). Atividade física e cognição em idosos: Uma revisão. Dementia & Neuropsychologia, 3(3), 204–208. https://doi.org/10.1590/S1980-57642009DN30300005
- Cacioppo, S., Grippo, A. J., London, S., Goossens, L., & Cacioppo, J. T. (2015). Loneliness: Clinical import and interventions. Perspectives on Psychological Science: a Journal of the Association for Psychological Science, 10(2), 238–249. https://doi.org/10.1177/1745691615570616
- Cadore, E. L., Rodríguez-Mañas, L., Sinclair, A., & Izquierdo, M. (2013). Effects of different exercise interventions on risk of falls, gait ability, and balance in physically frail older adults: A systematic review. Rejuvenation Research, 16(2), 105–114. https://doi.org/10.1089/rej.2012.1397
- Cashin, A. G., & McAuley, J. H. (2020). Clinimetrics: Physiotherapy evidence database (PEDro) scale. Journal of Physiotherapy, 66(1), 59. https://doi.org/10.1016/j.jphys.2019.08.005
- Cepeda, C. C., Lodovico, A., Fowler, N., & Rodacki, A. L. (2015). Effect of an eight-week ballroom dancing program on muscle architecture in older adult females. Journal of Aging and Physical Activity, 23(4), 607–612. https://doi.org/10.1123/japa.2014-0101
- Chodzko-Zajko, W. J., Proctor, D. N., Singh, M. A. F., Minson, C. T., Nigg, C. R., Salem, G. J., & Skinner, J. S. (2009). Exercise and physical activity for older adults. Medicine and Science in Sports and Exercise, 41(7), 1510–1530. https://doi.org/10.1249/MSS.0b013e3181a0c95c
- Cruz-Ferreira, A., Marmeleira, J., Formigo, A., Gomes, D., & Fernandes, J. (2015). Creative dance improves physical fitness and life satisfaction in older women. Research on Aging, 37(8), 837–855. https://doi.org/10.1177/0164027514568103
- Curran, E., Rosato, M., Ferry, F., & Leavey, G. (2020). Prevalence and factors associated with anxiety and depression in older adults: Gender differences in psychosocial indicators. Journal of Affective Disorders, 267(15 April 2020), 114–122. https://doi.org/10.1016/j.jad.2020.02.018
- Database, P. E. (1999). PEDro scale. In School of physiotherapy. University of Sydney. https://pedro.org.au/wp-content/uploads/PEDro_scale.pdf
- De Biase, S., Cook, L., Skelton, D. A., Witham, M., & Ten Hove, R. (2020). The COVID-19 rehabilitation pandemic. Age and Ageing, 49(5), 696–700. https://doi.org/10.1093/ageing/afaa118
- Devereux-Fitzgerald, A., Powell, R., Dewhurst, A., & French, D. P. (2016). The acceptability of physical activity interventions to older adults: A systematic review and meta-synthesis. Social Science & Medicine, 158(June 2016), 14–23. https://doi.org/10.1016/j.socscimed.2016.04.006
- Dhami, P., Moreno, S., & DeSouza, J. F. (2014). New framework for rehabilitation - fusion of cognitive and physical rehabilitation: The hope for dancing. Frontiers in Psychology, 5 , 1478. https://doi.org/10.3389/fpsyg.2014.01478
- Fernández-Argüelles, E. L., Rodríguez-Mansilla, J., Antunez, L. E., Garrido-Ardila, E. M., & Muñoz, R. P. (2015). Effects of dancing on the risk of falling related factors of healthy older adults: A systematic review. Archives of Gerontology and Geriatrics, 60(1), 1–8. https://doi.org/10.1016/j.archger.2014.10.003
- Fragala, M. S., Cadore, E. L., Dorgo, S., Izquierdo, M., Kraemer, W. J., Peterson, M. D., & Ryan, E. D. (2019). Resistance training for older adults: Position statement from the national strength and conditioning association. The Journal of Strength & Conditioning Research, 33(8), 2019–2052. doi:10.1519/JSC.0000000000003230
- Franco, M. R., Sherrington, C., Tiedemann, A., Pereira, L. S., Perracini, M. R., Faria, C. S. G., Negrão-Filho, R. F., Pinto, R. Z., & Pastre, C. M. (2020). Effect of senior dance (DanSE) on fall risk factors in older adults: A randomized controlled trial. Physical Therapy, 100(4), 600–608. https://doi.org/10.1093/ptj/pzz187
- Granacher, U., Muehlbauer, T., Bridenbaugh, S. A., Wolf, M., Roth, R., Gschwind, Y., Wolf, I., Mata, R., & Kressig, R. W. (2012). Effects of a salsa dance training on balance and strength performance in older adults. Gerontology, 58(4), 305–312. https://doi.org/10.1159/000334814
- Hamacher, D., Hamacher, D., Rehfeld, K., Hökelmann, A., & Schega, L. (2015). The effect of a six-month dancing program on motor-cognitive dual-task performance in older adults. Journal of Aging and Physical Activity, 23(4), 647–652. https://doi.org/10.1123/japa.2014-0067
- Hayes, C., & Kriska, A. (2008). Role of physical activity in diabetes management and prevention. Journal of the American Dietetic Association, 108(4, Suppl.), S19–S23. https://doi.org/10.1016/j.jada.2008.01.016
- Hays, T., & Minichiello, V. (2005). The meaning of music in the lives of older people: A qualitative study. Psychology of Music, 33(4), 437–451. https://doi.org/10.1177/0305735605056160
- Higgins, J., Green, S., & Collaboration, C. (2008). Cochrane handbook for systematic reviews of interventions. Wiley Online Library. In.
- Hofgaard, J., Ermidis, G., & Mohr, M. (2019). Effects of a 6-week Faroese chain dance programme on postural balance, physical function, and health profile in elderly subjects: A pilot study. BioMed Research International, 2019, 5392970. https://doi.org/10.1155/2019/5392970
- Hwang, P. W.-N., & Braun, K. L. (2015). The effectiveness of dance interventions to improve older adults’ health: A systematic literature review. Alternative Therapies in Health and Medicine, 21(5), 64. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5491389/
- Janyacharoen, T., Laophosri, M., Kanpittaya, J., Auvichayapat, P., & Sawanyawisuth, K. (2013). Physical performance in recently aged adults after 6 weeks traditional Thai dance: A randomized controlled trial. Clinical Interventions In Aging, 8, 855–859. https://doi.org/10.2147/CIA.S41076
- Joung, H. J., Lee, Y., & Joung, H. J. (2019). Effect of creative dance on fitness, functional balance, and mobility control in the elderly. Gerontology, 65(5), 537–546. https://doi.org/10.1159/000499402
- Kattenstroth, J.-C., Kolankowska, I., Kalisch, T., & Dinse, H. R. (2010). Superior sensory, motor, and cognitive performance in elderly individuals with multi-year dancing activities. Frontiers in Aging Neuroscience, 2, 31. https://doi.org/10.3389/fnagi.2010.00031
- Koch, S. C., Riege, R. F. F., Tisborn, K., Biondo, J., Martin, L., & Beelmann, A. (2019). Effects of dance movement therapy and dance on health-related psychological outcomes. A meta-analysis update. Frontiers in Psychology, 10,1806 . https://doi.org/10.3389/fpsyg.2019.01806
- Kojima, G., Masud, T., Kendrick, D., Morris, R., Gawler, S., Treml, J., & Iliffe, S. (2015). Does the timed up and go test predict future falls among British community-dwelling older people? Prospective cohort study nested within a randomised controlled trial. BMC Geriatrics, 15(1), 38. https://doi.org/10.1186/s12877-015-0039-7
- Komatsu, H., Yagasaki, K., Saito, Y., & Oguma, Y. (2017). Regular group exercise contributes to balanced health in older adults in Japan: A qualitative study. BMC Geriatrics, 17(1), 190. https://doi.org/10.1186/s12877-017-0584-3
- Krampe, J. (2013). Exploring the effects of dance-based therapy on balance and mobility in older adults. Western Journal of Nursing Research, 35(1), 39–56. https://doi.org/10.1177/0193945911423266
- Liu, X., Shen, P.-L., & Tsai, Y.-S. (2020). Dance intervention effects on physical function in healthy older adults: A systematic review and meta-analysis. Aging Clinical and Experimental Research 33(February) 253–263 . https://doi.org/10.1007/s40520-019-01440-y
- Liu, X., Shen, P. L., & Tsai, Y. S. (2021). Dance intervention effects on physical function in healthy older adults: A systematic review and meta-analysis. Aging Clinical and Experimental Research, 33(2), 253–263. https://doi.org/10.1007/s40520-019-01440-y
- Macedo, L. G., Elkins, M. R., Maher, C. G., Moseley, A. M., Herbert, R. D., & Sherrington, C. (2010). There was evidence of convergent and construct validity of physiotherapy evidence database quality scale for physiotherapy trials. Journal of Clinical Epidemiology, 63(8), 920–925. https://doi.org/10.1016/j.jclinepi.2009.10.005
- Macera, C. A., Cavanaugh, A., & Bellettiere, J. (2017). State of the art review: Physical activity and older adults. American Journal of Lifestyle Medicine, 11(1), 42–57. https://doi.org/10.1177/1559827615571897
- Madureira, M. M., Takayama, L., Gallinaro, A. L., Caparbo, V. F., Costa, R. A., & Pereira, R. M. R. (2007). Balance training program is highly effective in improving functional status and reducing the risk of falls in elderly women with osteoporosis: A randomized controlled trial. Osteoporosis International: a Journal Established as Result of Cooperation between the European Foundation for Osteoporosis and the National Osteoporosis Foundation of the USA, 18(4), 419–425. https://doi.org/10.1007/s00198-006-0252-5
- Maher, C. G., Sherrington, C., Herbert, R. D., Moseley, A. M., & Elkins, M. (2003). Reliability of the PEDro scale for rating quality of randomized controlled trials. Physical Therapy, 83(8), 713–721. https://doi.org/10.1093/ptj/83.8.713
- Mandolesi, L., Polverino, A., Montuori, S., Foti, F., Ferraioli, G., Sorrentino, P., & Sorrentino, G. (2018). Effects of physical exercise on cognitive functioning and wellbeing: Biological and psychological benefits. Frontiers in Psychology, 9, 509. https://doi.org/10.3389/fpsyg.2018.00509
- Marques, E. A., Mota, J., Machado, L., Sousa, F., Coelho, M., Moreira, P., & Carvalho, J. (2011). Multicomponent training program with weight-bearing exercises elicits favorable bone density, muscle strength, and balance adaptations in older women. Calcified Tissue International, 88(2), 117–129. https://doi.org/10.1007/s00223-010-9437-1
- McKinley, P., Jacobson, A., Leroux, A., Bednarczyk, V., Rossignol, M., & Fung, J. (2008). Effect of a community-based Argentine tango dance program on functional balance and confidence in older adults. Journal of Aging and Physical Activity, 16(4), 435–453. https://doi.org/10.1123/japa.16.4.435
- McNeely, M., Duncan, R., & Earhart, G. (2015). A comparison of dance interventions in people with Parkinson disease and older adults. Maturitas, 81(1), 10–16. https://doi.org/10.1016/j.maturitas.2015.02.007
- Meng, X., Li, G., Jia, Y., Liu, Y., Shang, B., Liu, P., Bao, X., & Chen, L. (2020). Effects of dance intervention on global cognition, executive function and memory of older adults: A meta-analysis and systematic review. Aging Clinical and Experimental Research, 32(1), 7–19. https://doi.org/10.1007/s40520-019-01159-w
- Merom, D., Grunseit, A., Eramudugolla, R., Jefferis, B., Mcneill, J., & Anstey, K. J. (2016). Cognitive benefits of social dancing and walking in old age: The dancing mind randomized controlled trial. Frontiers in Aging Neuroscience, 8, 26. https://doi.org/10.3389/fnagi.2016.00026
- Moher, D., Liberati, A., Tetzlaff, J., & Altman, D. G. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Annals of Internal Medicine, 151(4), 264–269. https://doi.org/10.7326/0003-4819-151-4-200908180-00135
- Moss, H., Donnellan, C., & O’Neill, D. Hospitalization and aesthetic health in older adults. (2015). Journal of the American Medical Directors Association, 16(2), e111–173. e116. 173. https://doi.org/10.1016/j.jamda.2014.10.019
- Müller, P., Rehfeld, K., Schmicker, M., Hökelmann, A., Dordevic, M., Lessmann, V., Müller, P., Brigadski, T., Kaufmann, J., & Müller, N. G. (2017). Evolution of neuroplasticity in response to physical activity in old age: The case for dancing. Frontiers in Aging Neuroscience, 9, 56. https://doi.org/10.3389/fnagi.2017.00056
- Noopud, P., Suputtitada, A., Khongprasert, S., & Kanungsukkasem, V. (2019). Effects of Thai traditional dance on balance performance in daily life among older women. Aging Clinical and Experimental Research, 31(7), 961–967. https://doi.org/10.1007/s40520-018-1040-8
- O’Regan, A., García Bengoechea, E., Clifford, A. M., Casey, M., Gallagher, S., Glynn, L., Woods, C., & Doyle, C. (2020). How to improve recruitment, sustainability and scalability in physical activity programmes for adults aged 50 years and older: A qualitative study of key stakeholder perspectives. PLoS One, 15(10), e0240974–e0240974. https://doi.org/10.1371/journal.pone.0240974
- Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Brennan, S. E., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J., Grimshaw, J. M., Hróbjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo-Wilson, E., McDonald, S., McGuinness, L. A., andShamseer, L. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. International Journal of Surgery, 88(April), 105906. https://doi.org/10.1016/j.ijsu.2021.105906
- Perissinotto, C. M., Stijacic Cenzer, I., & Covinsky, K. E. (2012). Loneliness in older persons: A predictor of functional decline and death. Archives of Internal Medicine, 172(14), 1078–1083. https://doi.org/10.1001/archinternmed.2012.1993
- Piercy, K. L., Troiano, R. P., Ballard, R. M., Carlson, S. A., Fulton, J. E., Galuska, D. A., … Olson, R. D. (2018). The Physical Activity Guidelines for Americans. Jama, 320(19), 2020–2028. https://doi.org/10.1001/jama.2018.14854
- Power, V., & Clifford, A. M. (2013). Characteristics of optimum falls prevention exercise programmes for community-dwelling older adults using the FITT principle. European Review of Aging and Physical Activity, 10(2), 95–106. https://doi.org/10.1007/s11556-012-0108-2
- Rehfeld, K., Müller, P., Aye, N., Schmicker, M., Dordevic, M., Kaufmann, J., Müller, P., Hökelmann, A., & Müller, N. G. (2017). Dancing or fitness sport? The effects of two training programs on hippocampal plasticity and balance abilities in healthy seniors. Frontiers in Human Neuroscience, 11, 305. https://doi.org/10.3389/fnhum.2017.00305
- Rehfeld, K., Lüders, A., Hökelmann, A., Lessmann, V., Kaufmann, J., Brigadski, T., Müller, N. G., & Müller, P. (2018). Dance training is superior to repetitive physical exercise in inducing brain plasticity in the elderly. PLoS One, 13(7), e0196636. https://doi.org/10.1371/journal.pone.0196636
- Rivera-Torres, S., Fahey, T. D., & Rivera, M. A. (2019). Adherence to exercise programs in older adults: Informative report. Gerontology and Geriatric Medicine, 5, 2333721418823604. https://doi.org/10.1177/2333721418823604
- Rodrigues-Krause, J., Farinha, J. B., Ramis, T. R., Macedo, R. C. O., Boeno, F. P., Dos Santos, G. C., Costa, R. R., Grazioli, R., Costa, R. R., Pinto, R. S., Krause, M., Reischak-Oliveira, A., & Vargas, J. (2018). Effects of dancing compared to walking on cardiovascular risk and functional capacity of older women: A randomized controlled trial. Experimental Gerontology, 114(December), 67–77. https://doi.org/10.1016/j.exger.2018.10.015
- Roque, F. R., Briones, A. M., García‐Redondo, A. B., Galán, M., Martínez‐Revelles, S., Avendaño, M. S., Oliveira, E. M., Vassallo, D. V., Oliveira, E. M., Salaices, M., & Cachofeiro, V. (2013). Aerobic exercise reduces oxidative stress and improves vascular changes of small mesenteric and coronary arteries in hypertension. British Journal of Pharmacology, 168(3), 686–703. https://doi.org/10.1111/j.1476-5381.2012.02224.x
- Sagiv, M., Goldhammer, E., Ben-Sira, D., & Amir, R. (2010). Factors defining oxygen uptake at peak exercise in aged people. Springer.
- Sejnoha Minsterova, A., Klobusiakova, P., Kropacova, S., Novakova, L., Brabenec, L., Balazova, Z., Grmela, R., Skotakova, A., Svobodova, L., & Rektorova, I. (2020). Multishell diffusion MRI reflects improved physical fitness induced by dance intervention. Neural Plasticity 2020 Special Issue , 8836925. https://doi.org/10.1155/2020/8836925
- Shanahan, J., Morris, M. E., Bhriain, O. N., Saunders, J., & Clifford, A. M. (2015). Dance for people with Parkinson disease: What is the evidence telling us? Archives of Physical Medicine and Rehabilitation, 96(1), 141–153. https://doi.org/10.1016/j.apmr.2014.08.017
- Sherrington, C., Herbert, R., Maher, C., & Moseley, A. (2000). PEDro. A database of randomized trials and systematic reviews in physiotherapy. Manual Therapy, 5(4), 223–226. https://doi.org/10.1054/math.2000.0372
- Sherrington, C., Tiedemann, A., Fairhall, N., Close, J. C. T., & Lord, S. R. (2011). Exercise to prevent falls in older adults: An updated meta-analysis and best practice recommendations. New South Wales Public Health Bulletin, 22(4), 78–83. https://doi.org/10.1071/NB10056
- Sofianidis, G., Hatzitaki, V., Douka, S., & Grouios, G. (2009). Effect of a 10-week traditional dance program on static and dynamic balance control in elderly adults. Journal of Aging and Physical Activity, 17(2), 167–180. https://doi.org/10.1123/japa.17.2.167
- Sofianidis, G., Dimitriou, A.-M., & Hatzitaki, V. (2017). A comparative study of the effects of pilates and Latin dance on static and dynamic balance in older adults. Journal of Aging and Physical Activity, 25(3), 412–419. https://doi.org/10.1123/japa.2016-0164
- Tomioka, K., Kurumatani, N., & Hosoi, H. (2015). Social participation and the prevention of decline in effectance among community-dwelling elderly: A population-based cohort study. PLoS One, 10(9), e0164925. https://doi.org/10.1371/journal.pone.0139065
- Waller, B., Ogonowska-Słodownik, A., Vitor, M., Rodionova, K., Lambeck, J., Heinonen, A., & Daly, D. (2016). The effect of aquatic exercise on physical functioning in the older adult: A systematic review with meta-analysis. Age and Ageing, 45(5), 593–601. https://doi.org/10.1093/ageing/afw102
- Warburton, D., Nicol, C., & Bredin, S. (2006). Health benefits of physical activity: The evidence. Canadian Medical Association Journal, 174(6), 801–809. doi:10.1503/cmaj.051351
- Ward, M., Kenny, R., & Layte, R. (2019). Loneliness, social isolation, and their discordance among older adults (Trinity College Dublin). http://hdl.handle.net/2262/89853
- WHO. (2016). Global Strategy and Action Plan on Aging and Health (2016‐2020). Retrieved from
- Yepes-Nuñez, J. J., Urrútia, G., Romero-García, M., Alonso-Fernández, S., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetzlaff, J. M., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J., Grimshaw, J. M., Hróbjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo-Wilson, E., McDonald, S., … Moher, D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. (2021). Revista espanola de cardiologia, 74(9), 790–799. English ed. https://doi.org/10.1016/j.rec.2021.07.010
Appendix 1:
Example of search strategy for PubMed Database
Figure A PRISMA Flow Diagram
Appendix 2.
Critical appraisal and PEDro tables and scores.