
Abstract
Purpose: The achievement of speech intelligibility by persons with Down syndrome facilitates their participation in society. Denial of speech therapy services by virtue of low cognitive skills is a violation of their fundamental human rights as proclaimed in the Universal Declaration of Human Rights in general and in Article 19 in particular. Here, we describe the differential response of an adolescent with Down syndrome to three speech therapy interventions and demonstrate the use of a single subject randomisation design to identify effective treatments for children with complex communication disorders.
Method: Over six weeks, 18 speech therapy sessions were provided with treatment conditions randomly assigned to targets and sessions within weeks, specifically comparing auditory-motor integration prepractice and phonological planning prepractice to a control condition that included no prepractice. All treatments involved high intensity practice of nonsense word targets paired with tangible referents.
Result: A measure of generalisation from taught words to untaught real words in phrases revealed superior learning in the auditory-motor integration condition.
Conclusion: The intervention outcomes may serve to justify the provision of appropriate supports to persons with Down syndrome so that they may achieve their full potential to receive information and express themselves.
Introduction
The Universal Declaration of Human Rights (United Nations, Citation1948) explicitly avoids placing rights in a hierarchy – each is inalienable, that is, must not be denied to any person. At the same time it is recognised that some rights empower others: Article 19, guaranteeing freedom of expression and free access to information, is fundamental to the realisation of the other rights accorded by the declaration. La Rue Lewy (Citation2012) describes how recent interpretations of Article 19 reveal “freedom of speech and communication as a human right and as a way to fight against all forms of discrimination, be they based on race, religion, ethnic group, gender or different physical capabilities” (pp. 57–58). Accordingly, the Convention on the Rights of Persons with Disabilities introduced specific provisions to remedy disadvantages in the exercise of Article 19 rights (Article 19, Citation2016). These include not discriminating against individuals on the basis of disability so that they may enjoy equal opportunity, removing barriers to full participation in society, and providing reasonable accommodations to ensure freedom of expression and access to information.
Persons with intellectual disabilities face many challenges in the exercise of their right to free expression. More specifically, persons with Down syndrome experience persistent delays in language development with expressive abilities being significantly more delayed than receptive abilities (Grieco, Pulsifer, Seligsohn, Skotko, & Schwartz, Citation2015). Severe difficulties with morphosyntax and speech intelligibility can persist into adulthood. In order to achieve their full communicative potential, persons with Down syndrome will require interventions to remediate their specific speech and language disabilities, access to alternative and augmentative forms of communication when necessary, and reasonable accommodations that permit access to information and effective communication. With appropriate supports individuals with Down syndrome can achieve full participation in society, but surveys of their families indicate service provision is typically inadequate.
A Canadian survey revealed that one-third of children with disabilities struggled to obtain special education services and 60% did not obtain speech–language pathology services (Statistics Canada, Citation2003), according to parent report. Furthermore, parents of children with cognitive disabilities were much less likely to believe that their children were being challenged to their full potential in school, compared to parents whose children have physical disabilities or no disabilities. A survey of Canadian adults with disabilities revealed barriers to higher educational attainment, specifically poor access to supports such as tutors and digital technologies as well as school exclusion or bullying. The employment rate for adults with a developmental disability was the lowest of any disability type at only 22% (for US data specific to Down syndrome, see Kumin & Schoenbrodt, Citation2016).
Families in the UK also reported significant difficulties obtaining needed supports for their children with Down syndrome in school, with access to speech and language therapy being a particular concern. Only 58% were scheduled to receive a speech and language service, the frequency of entitlement to that service was not usually specified, and the service was provided by a speech–language pathologist (SLP) in only 14% of cases (Down's Syndrome Association, Citation2004). Surveys of SLPs further reveal inadequate levels of service provision (Meyer, Theodoros, & Hickson, Citation2017), a tendency to treat language over speech intelligibility and insufficient intensity of service.
In the Down’s Syndrome Association (2004) report, parents also indicated distress about discriminatory attitudes by school personnel including SLPs who sometimes discouraged parents from seeking private speech and language therapy. Young children with Down syndrome may be deemed “not ready” for speech therapy if they are unable to imitate speech; however, speech imitation can emerge as an outcome of vocal play therapy that provides the child with the prerequisite internal model of the vocal system (Dethorne, Johnson, Walder, & Mahurin-Smith, Citation2009; Rvachew & Brosseau-Lapré, Citation2018). Older children may be considered poor candidates for speech therapy due to cognitive limits on language learning, but research shows that receptive vocabulary growth can exceed cognitive growth given appropriate environmental inputs to children with Down syndrome (Chapman & Hesketh, Citation2001). In adolescence, speech–language services may be curtailed due to assumptions about a presumed critical period for language development; however, Chapman, Hesketh, and Kistler, (Citation2002) demonstrated that expressive language learning continues into adolescence and recommend continued services during this period for young people with Down syndrome. These forms of “cognitive referencing” have been proscribed by the National Joint Committee for the Communication Needs of Persons With Severe Disabilities (Citation2002) which states that services must be based on “individual student needs”. The type and intensity of services provided may continue to reflect biases about the learning potential of individuals with severe disabilities nonetheless. In this paper, we present a unique research design that permits an objective determination of individual responses to individual therapy approaches or intervention targets.
In the current study, we implemented a single subject randomisation design with a single adolescent with Down syndrome to determine response to speech therapy. Resources for the remediation of speech and language disabilities in persons with Down syndrome are limited in the public and private sectors and the profiles of strengths and needs among this population are heterogeneous. SLPs require tools for deciding how best to target their interventions, choose treatment approaches and organise service delivery components. The ability to conduct short-term experiments with specific cases could support decision making tailored to the learning potential of each individual with Down syndrome.
Speech production accuracy was chosen as the target of this trial as it is the foundation of speech intelligibility (Shriberg & Kwiatkowski, Citation1982), identified as a major concern by parents of 937 persons with Down syndrome (Kumin, Citation2006). Poor speech production accuracy is sometimes attributed to structural impairments in Down syndrome but the severity of the speech problem is more directly related to difficulties with speech motor control, complicated by concomitant hypotonia (Kent & Vorperian, Citation2013; Rupela, Velleman, & Andrianopoulos, Citation2016). Given this profile, one of the treatment conditions assessed in this study addressed motor planning, using sensory-motor procedures designed to improve auditory-motor integration. Speech errors produced by persons with Down syndrome have also been described as atypical and inconsistent (Dodd & Thompson, Citation2001), suggesting difficulties with phonological memory and planning (Rvachew & Matthews, Citation2017a). Difficulties with verbal working memory are characteristic of Down syndrome (Grieco et al., Citation2015) leading to the recommendation that interventions for the treatment of expressive language disabilities employ visual cues as a specific accommodation (Chapman & Hesketh, Citation2001; Chapman et al., Citation2002). Therefore, the second intervention to be used in this trial involved procedures shown effective for improving speech impairment secondary to phonological memory and planning problems (Crosbie, Holm, & Dodd, Citation2005). It was expected that a statistically significant effect would be observed over a six-week treatment interval, indicating superior learning in one or both experimental conditions relative to a control intervention, and that learning would be maintained over a three month follow-up interval.
Method
The method section is organised in accordance with the SCRIBE statement (Tate et al., Citation2016) for describing behavioural intervention trials in a single participant (i.e. research design, participant, measures, interventions and treatment fidelity, and finally, analysis strategy).
Research design
A single subject randomisation design is a form of single case research in which sessions are randomly allocated to treatment conditions within subjects (Edgington & Onghena, Citation2007; Rvachew & Matthews, Citation2017b). Sessions were randomly allocated to the three treatment conditions within weeks. The participant was scheduled to receive 18 one-hour treatment sessions, each occurring on a separate day, three sessions per week, over a six-week period. Research Randomiser software (Urbaniak & Plous, Citation2013) was used to randomly assign the treatment sessions to treatment conditions by generating six sets of three numbers in different independent orders. Furthermore, treatment conditions were randomly assigned to one of three different treatment goals, so that ultimately he received six sessions of treatment for each treatment goal remediated with a different treatment approach. The first author allocated the treatments to sessions and goals while blind to the participant’s assessment profile and uninvolved in the intervention. One experiment is described here in abbreviated form. The reader is strongly encouraged to consult Folden (Citation2016) for further details about the choice and implementation of the experiment treatments and for details regarding two additional replications of this experiment.
Participant
The male participant identified as TASC-DS35, aged 15.08 years, was recruited via referrals from local SLPs, after obtaining approval from the Institutional Review Board of the Faculty of Medicine at McGill University and informed consent from his parents. A written case history and interview with his mother confirmed that he met the inclusion criteria of Down syndrome, severe speech sound disorder and behavioural maturity to cooperate with the intense treatment schedule. Subsequently, TASC-DS35 attended the laboratory clinic at McGill University for direct assessments that included: Diagnostic Evaluation of Articulation and Phonology (DEAP; Dodd, Zhu, Crosbie, Holm, and Ozanne, Citation2006); free speech sample; Kaufman Brief Intelligence Test (KBIT; Kaufman & Kaufman, Citation2004); Peabody Picture Vocabulary Test-III (PPVT; Dunn & Dunn, Citation1997); Maximum Performance Tasks (MPTs; Rvachew, Hodge, and Ohberg, Citation2005); Syllable Repetition Task (SRT; Lohmeier & Shriberg, Citation2011; Shriberg et al., Citation2009). The results of these assessments are presented in and were interpreted in view of the framework presented in Rvachew and Matthew (Citation2017a).
Table I. Pretreatment and follow-up formal assessment scores.
The case history and parent interview revealed a history of multiple therapies including occupational therapy, massage therapy, physiotherapy and speech–language therapy directed at language skills and use of an augmentative and alternative communication device. His mother also reported a past history of pressure equalisation (PE) tubes and ongoing difficulties with swallowing. The speech assessment, as revealed by the DEAP and free speech samples, revealed a severe speech disorder and poor speech intelligibility as well as stuttering (common in Down syndrome, Kent & Vorperian, Citation2013). Error patterns included consonant and syllable harmony and the insertion of extraneous syllables (e.g., shark /ʃa˞k/ → [ka˞k], zebra /zibɹə/ → [ɬæɬæ], umbrella /ʌmbɹεlə/ → [ʌbələlədidə], [ʌmbəbəbəɬæɬə]). Inconsistency within words, oral/nasal, voicing and vowel confusions were observed, along with disrupted transitions between segments and syllables and poor coordination of multiple articulators (e.g. jump /d͡ʒʌmp/ → [map], [bap]). Although his phonetic repertoire included [p,b,t,d,k,m,n,f,v,l,j], none of these sounds were mastered.
Verbal and nonverbal intelligence were significantly delayed with nonverbal skills advanced relative to verbal skills. Oral motor skills were also delayed: specifically, he had difficulty producing combinations of nonspeech movements and was unable to produce trisyllable sequences; simple movements and monosyllable repetition were relatively less impaired. The Syllable Repetition Task yielded scores in the ranges typical of respondents with apraxia of speech in the areas encoding, memory and transcoding (Shriberg, Lohmeier, Strand, & Jakielski, Citation2012).
Treatment goals and speech production probes
The intake assessment provided data for the selection of treatment production goals through a quick multilinear analysis as described in Rvachew and Brosseau-Lapré (Citation2018). Three goals were selected using strengths to supports needs (in other words, targeting known segments in new word shapes and new segments or features in familiar word shapes). This process resulted in three goals: (1) suppress consonant and vowel harmony in two syllable words; (2) stabilise major sound classes in syllable onset (i.e. stop [+consonantal] vs. glide [+sonorant] vs. liquid [+consonantal][+sonorant]) and (3) establish consistent production of /f/. For each goal, five target words were selected to be thematically congruent with a specific play routine. The play routines included the names of nonsense words to name characters, constructed to fit the phonological goal while not inviting interference from misarticulated known words in TASC-DS35’s lexicon. Additional words were selected or created to be congruent with the phonological target and theme so as to support phrase level practice. The three sets of five target words, including nouns, verbs and adjectives, were as follows: [tæmdɑʊ], [bundeɪ], [pɑɡtɑɡ], [dɑʊnʌp], [pinʌt] (Goal 1, monster routine, phonological memory condition); [wit], [lut], [dɜt], [wɑɾə], [jɑd] (Goal 2, alien flower routine, auditory-motor integration condition) and, [pʌf], [fæp], [wʊf], [fuwi], [fud] (Goal 3, dog routine, control condition).
Learning of the specific targets was tracked by coding treatment performance from video recordings of each treatment session. However, the primary outcome was generalisation of learning from the taught words to untaught real words, measured with probes that consisted of short phrases constructed of real words that mirrored the taught phonological structures (e.g. Goal 1: toy bag, onset Cs and Vs expected to be correct; Goal 2: you go, glide and stop manner expected to be matched; Goal 3: two feet, segment /f/ expected to be correct). For each goal a pool of 30 probe items was constructed; from each pool 12 sets of 10 were selected to form six same day probes and six next day probes, each one containing a unique set of items. Same day probes were administered at the end of the session during which the goal was targeted in therapy to assess immediate generalisation from the taught target words to the real word probes. Next day probes were administered at the beginning of the next treatment session to assess maintenance of learning over a short interval. All probes were administered via imitation using a live voice elicitation procedure and recorded using Sony HDR-XR150 camera mounted on a tripod and a Zoom H2 Recorder, placed 53–71 cm from the participant, and set to 4-way stereo recording.
Intervention
The structure of every session was identical regardless of the randomly assigned treatment condition, as follows: (1) introduce session activities using a visual schedule, (2) record 10-item next day probe, (3) prepractice of target words, (4) high intensity practice, (5) record 10-item same day probe, (6) family debrief. Prepractice and practice activities were each scheduled to last 20 min. The remaining activities required an additional 20 min altogether. The accompanying family member observed the sessions through a two-way mirror. Under typical circumstances, home practice and functional words would be chosen as targets and we would advise this for most clinical applications of these procedures. However, in this experiment, home practice was discouraged and the target words and play routines themselves were designed so that spontaneous practice of specific target words was unlikely to occur. This exceptional restriction allowed us to be sure that improvements in speech accuracy and differences across conditions could be attributed to the experimental procedures.
Prepractice procedures
Prepractice is implemented to ensure that the learner is capable of producing the target words and has strategies to maintain a high level of correct production during the practice portion of the treatment session. Prepractice occurs at a relatively slow pace and knowledge of performance feedback is provided as needed (specifically in the form of verbal descriptions of the participant’s articulatory gestures). During auditory-motor integration sessions, the procedures were designed to ensure that TASC-DS35 had a strong auditory-phonetic representation of the target words that was linked to the semantic and articulatory representations of the words. These procedures were also designed to ensure that he could effectively use information provided in audio-visual models to improve production and that he could integrate and use somatosensory and auditory feedback of his own productions in relation to this knowledge of the target to monitor and correct his own productions, specifically auditory bombardment, error detection and focussed stimulation (as described in detail in Chapters 9 and 10 of Rvachew & Brosseau-Lapré, Citation2018). During phonological memory and planning sessions, the procedures were designed to support the independent construction of phonological plans for the production of each target word. Specifically he was taught to associate visual cues with the articulatory gestures for each phoneme in the target word. Using segmentation and chaining techniques, he was taught to produce the target words without the provision of an auditory-visual model, using the visual cues when necessary (as described in more detail in Chapter 11 of Rvachew & Brosseau-Lapré with respect to the procedures for implementing the Core Vocabulary Approach). During control sessions, no prepractice procedures were employed; rather activities that did not involve speech practice were conducted during this segment of the session.
Practice procedures
Regardless of the assigned prepractice condition, the goal of the practice session was to encourage high intensity practice – aiming for at least 100 practice trials – at the highest level of complexity possible while maintaining accuracy “at the challenge point”. In keeping with the challenge point framework (Guadagnoli & Lee, Citation2004; Rvachew & Brosseau-Lapré, Citation2018) practice performance must be neither too high nor too low for optimum learning. Specifically, if responding fell below 4/5 correct responses, practice components were adjusted to make the task easier; when responding rose above this level, practice components were adjusted to make the task more difficult. Adjustable practice components included target complexity (e.g. single word vs. phrase), pre-trial support (e.g. imitative model vs. question prompt), stimulus variability (blocked vs. random presentation) or feedback schedule (e.g., after every trial vs. after a block of five trials). Some aspects of the practice components were unique to the randomised treatment condition as follows: in the auditory-motor integration condition, auditory-visual models were provided frequently and feedback was delayed as much as possible to encourage self-monitoring; in the phonological memory condition, the use of visual cues was encouraged to support spontaneous generation of phonological plans; in the control condition, the feedback schedule was fixed at 60% of trials, congruent with the principles of motor learning (Maas et al., Citation2008; Maas, Butalla, & Farinella, Citation2012).
Treatment fidelity
Treatment sessions were conducted by a student clinician with supervision from the trial coordinator, an ASHA certified speech–language pathologist, both of whom received three days of training in trial procedures prior to implementation. Lesson plans were reviewed by the trial coordinator prior to each session to ensure congruence with the trial protocol. All session videos were coded for compliance by the second author for inclusion of mandated procedures, by randomly allocated condition, using a checklist. Treatment fidelity was 100% for the phonological planning prepractice sessions (meaning that all expected procedures were used during all six sessions) but only 73% during the auditory-motor integration prepractice sessions because activities targeting self-monitoring were often omitted due to the difficulties TASC-DS35 was having detecting errors in the clinician’s speech. During the practice portion of each session, the expectation of at least 100 practice trials was generally achieved on average but not during every session as shown in . The cumulative treatment intensity varied among treatment conditions with total practice trials being 588 in the auditory motor integration condition, 678 in the control condition and 726 in the phonological memory condition. The clinician did not succeed in maintaining practice performance at the challenge point, as shown in , where it can be seen that TASC-DS35 performed below 80% correct during all sessions.
Table II. Total practice trials, percent correct trials, same day (SD) probe scores and next day (ND) probe scores by session and treatment condition.
Analysis strategy
Same day and next day probe scores were transcribed and scored out of 10 points. The probes were transcribed by two independent transcribers with graduate level training in phonetic transcription, using PHON (Rose & McWhinney, Citation2016) to ensure blind transcriptions by multiple coders. Inter-rater agreement for the narrow transcription of probes was 86% for vowels, and 85% for consonants. The inter-scorer agreement for probe item correctness was 97.7%. Probe scores were submitted to a nonparametric randomisation test of the null hypothesis which is that the probe scores are independent of the treatment that was allocated for any given session. This kind of statistical test is performed using only the data obtained in the randomised single case experiment – the obtained data points are permuted repeatedly to represent all possible allocations of treatment conditions to obtained probe scores; the test statistic is recalculated for each possible allocation yielding a test distribution against which to evaluate the significance of the obtained statistic (in this experiment, the test distribution is (3!)6 = 66 = 46,656, F statistics).
Results
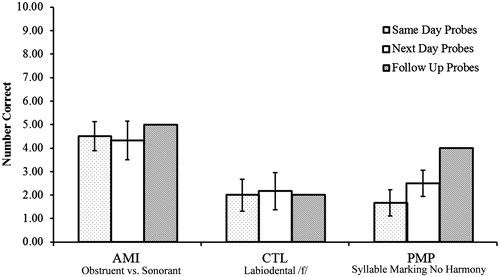
The results by session are presented in which shows the number of practice trials, the number of correctly produced practice trials, the same day probe score and the next day probe score for each session as a function of randomly allocated treatment condition. The next day probe scores are shown adjacent to the session for the associated treatment goal, rather than the “next day” session during which the probe was recorded. TASC-DS35 did not progress beyond the word level with the target words in any condition, although the complexity of practice was generally more complex in the auditory-motor integration sessions (three sessions involving drill-play activities targeting whole words in a delayed imitation or spontaneous word context) when compared to the control and phonological memory and planning sessions during which drill activities targeted direct imitation of part-words or whole words. These differences in practice context explain the variation in number of practice trials by condition because practice intensity is typically higher during simple drill than drill-play activities. Despite these differences in achievement across conditions, the overall impression is that TASC-DS35 was struggling to master all three treatment goals, given that accuracy during practice trials did not reach the goal of 80% correct in any treatment condition. Nonetheless, learning occurred as illustrated in that shows the mean and standard error of these probe scores along with the follow-up probe scores, recorded 84 days following the end of the treatment trial. A significant treatment effect was obtained for the same day probes, as determined by resampling (F = 5.71, p= 0.035, 1000 samples). Mean scores on next day probes show the same pattern of respondings but were not significantly different due to greater variability within and across conditions (F = 4.15, p = 0.056, 1000 samples). Effect sizes (dz for matched samples) were calculated to compare pairs of treatment conditions (Lakens, Citation2013). When comparing probe scores in the auditory motor integration condition to the control condition, the effect size was large for both same day probes (dz = 1.03) and next day probes (dz = 1.18). When comparing probe scores in the auditory motor integration condition to the phonological memory and planning condition, the effect size was large for both same day probes (dz = 1.65) and next day probes (dz = 1.38). When comparing probe scores in the phonological memory and planning condition to the control condition, the effect size was small for both same day probes (dz = −0.13) and next day probes (dz = 0.13). The follow-up assessment showed that gains were maintained for major sound class contrasts in the auditory-motor integration condition and that improvements continued over this interval for the production of multisyllabic words with reduced consonant and vowel harmony. Quick multilinear analysis of the repeat DEAP results also revealed improvements even where perfect accuracy was not achieved: the major class contrasts were better maintained (e.g. elefant /εləfənt/ → [εɬəbələ] at intake, but [alεləvɪt] at follow-up), and consonant and syllable harmony were reduced (e.ɡ. this /ðɪs/ → [ɡɪk] at intake, [dɪs̪] at follow-up).
Figure 1. Mean scores (with standard errors) shown for same day (left patterned bars) and next day probes (middle white bars) by randomly assigned treatment condition and treatment goal. Total score on probes recorded during the follow-up assessment was also shown (right patterned bars). AMI, auditory-motor integration prepractice condition; CTL, no prepractice control condition; PMP, phonological memory and planning prepractice condition.
Discussion
One adolescent with Down syndrome received three interventions, with a schedule of one session per week for six weeks, provided concurrently with randomised order of conditions within weeks. The intention of these interventions was to improve the participant’s speech sound accuracy to foster greater speech intelligibility, thereby facilitating increased success in communication and improved enjoyment of his right to free expression.
Statistically significant improvements in speech sound accuracy were achieved, as measured by same day generalisation probes. The treatment condition designed to remediate his specific underlying impairments in motor planning yielded the best result. Although a statistically significant result was not obtained for next day probes, there is evidence that the interventions facilitated his participation in activities of daily living; specifically, many individuals who interacted with him on a daily basis observed improvements in his ability to communicate verbally with family members, peers and support staff. Although TASC-DS35 did not master the goals taught during the six-week intervention, generalisation from taught to untaught words was observed with maintenance over a three-month interval. Furthermore, the effect size was large and clinically significant, given the discernable impact on intelligibility as reported by his parents and study staff. The findings of this experiment support the claim made by Chapman et al. (Citation2002) that learning continues through adolescence in DS. For public service providers, deciding whether to continue targeting speech intelligibility at this intensity will require an ongoing value judgment – the decision cannot be made on the basis of this evidence alone, without further reflection. However, future decisions about this young man’s treatment program can be made with clear information about his learning potential in the area of speech accuracy. Customising therapy to the individual’s profile of strengths and impairments is crucial in a heterogeneous population that infrequently receives treatment: in adolescents with Down syndrome there is no known blanket approach that can effectively remediate speech impairments.
McDaniel and Yoder (Citation2016) discuss the importance of collaborations among researchers and clinicians for developing precision speech–language services for children with Down syndrome. The single subject randomisation design we describe in this report is a useful tool for such collaborations as it provides high quality research evidence while supporting clinical decision making for individual patients. By pursuing the realisation of freedom of communication and access to information through speech therapy, clinicians hope to empower their clients with developmental disabilities so that they can achieve other fundamental human rights such as those pertaining to education, employment, dignity and security (United Nations, Citation1948). In light of this perspective, evidence that adolescents with Down syndrome can indeed make gains towards effective communication supports the idea that continued access and therapy for this population is warranted.
Limitations
The primary limitation of this study is that a single experiment was conducted with this adolescent, exploring only the relative effectiveness of different treatment approaches with respect to short-term changes in speech accuracy. For example, objective measures of speech intelligibility were not obtained and the study does not reveal the intensity of treatment required to obtain functional improvements in speech communication. The study was not designed to directly explore the relationship between improvements in speech accuracy and the functional outcomes that are ultimately the goal of speech therapy. The design used in this study permits the SLP to choose an intervention that will be effective for improving speech accuracy for a specific client. Larger questions, such as whether a focus on speech accuracy or other means of communication will have a greater impact on participation and inclusion, would require a different design such as a parallel groups randomised control design.
Another limitation is that the study provides no information about optimum intensity or scheduling of intervention. Improvements were observed in the goal of establishing the major sound class contrasts over six one-hour treatment sessions even though he did not master the goal. It is not clear that the same result would be obtained if these six sessions were provided without interleaving of multiple weekly sessions targeting multiple goals: given that variable practice of multiple treatment goals is a predictor of generalisation, it cannot be assumed that sequential rather than concurrent targeting of the three goals would lead to the same result. It is also not known if greater cumulative intervention intensity for each goal would ultimately lead to mastery of any of the goals. It is our sense that if he had received annual six week blocks of intense articulation therapy throughout his 12 years of schooling, his speech intelligibility would be considerably enhanced but it is impossible to be sure. Therefore, without continued clinical research with this young man and other persons with Down syndrome, the choice of speech articulation therapy versus a singular focus on augmentative communication remains a difficult decision for therapists and families.
Conclusion
In this study, we demonstrated that an adolescent with Down syndrome can make changes in speech accuracy, and according to parent report, speech intelligibility, given 6 weeks of intensive speech therapy. Furthermore, we have introduced a research design that permits the SLP to compare an individual’s response to different treatment conditions as a support for decision making about treatment targets, approaches or service delivery models. If we are to properly commit to the realisation of Article 19 rights for persons with Down syndrome much greater efforts must be made to enhance their communication skills in the verbal and nonverbal domains.
Declaration of interest
No potential conflict of interest was reported by the authors.
Acknowledgements
We thank the family that participated in the research project. We are also grateful for the assistance of students and research assistants including Lizzie Carolan, Omar Obregozo Zalava, Melanie Orellana, Pegah Athari and Alexandre Herbay.
Additional information
Funding
Related Research Data
References
- Article 19. (2016). Background paper: Freedom of expression and information and persons with disabilities (Policy Brief). Retrieved from https://www.article19.org/resources.php/resource/38511/en/consultation-open:-principles-on-freedom-of-expression-and-information-and-persons-with-disabilities
- Chapman, R.S., & Hesketh, L.J. (2001). Language, cognition, and short-term memory in individuals with Down syndrome. Down Syndrome Research and Practice, 7, 1–7. doi:10.3104/reviews.108
- Chapman, R.S., Hesketh, L.J., & Kistler, D.J. (2002). Predicting longitudinal change in language production and comprehension in individuals with Down syndrome: Hierarchical linear modeling. Journal of Speech, Language, and Hearing Research, 45, 902–915. doi:10.1044/1092-4388(2002/073)
- Crosbie, S., Holm, A., & Dodd, B. (2005). Intervention for children with severe speech disorder: A comparison of two approaches. International Journal of Language and Communication Disorders, 40, 467–491. doi:10.1080/13682820500126049
- Dethorne, L.S., Johnson, C.J., Walder, L., & Mahurin-Smith, J. (2009). When “Simon Says” doesn't work: Alternatives to imitation for facilitating early speech development. American Journal of Speech-Language Pathology, 18, 133–145. doi:10.1044/1058-0360(2008/07-0090)
- Dodd, B., & Thompson, L. (2001). Speech disorder in children with Down's syndrome. Journal of Intellectual Disability Research, 45, 308–316. doi:10.1046/j.13652788.2001.00327.x
- Dodd, B., Zhu, H., Crosbie, S., Holm, A., & Ozanne, A. (2006). Diagnostic evaluation of articulation and phonology (DEAP). San Antonio, TX: Pearson Education.
- Down's Syndrome Association. (2004). Access to education: A report on barriers to education for children with Down's syndrome. Teddington, Middlesex, UK: Down's Syndrome Association. Retrieved from http://dsagsl.org/wp-content/uploads/2014/04/access_to_education.pdf
- Dunn, L.M., & Dunn, L.M. (1997). Peabody Picture Vocabulary Test (3rd ed.). Circle Pines, MN: American Guidance Service.
- Edgington, E.S., & Onghena, P. (2007). Randomisation tests. New York, NY: Chapman & Hall.
- Folden, M. (2016). Down syndrome and childhood apraxia of speech: Matching a unique psycholinguistic profile to an effective treatment program. Unpublished M.Sc., McGill University, Montréal, Québec. Retrieved from http://digitool.Library.McGill.CA:80/R/-?func=dbin-jump-full&object_id=145539&silo_library=GEN01
- Grieco, J., Pulsifer, M., Seligsohn, K., Skotko, B., & Schwartz, A. (2015). Down syndrome: Cognitive and behavioral functioning across the lifespan. American Journal of Medical Genetics Part C: Seminars in Medical Genetics, 169, 135–149. doi:https://doi.org/10.1002/ajmg.c.31439
- Guadagnoli, M.A., & Lee, T.D. (2004). Challenge point: A framework for conceptualizing the effects of various practice conditions in motor learning. Journal of Motor Behavior, 36, 212–224. doi:10.3200/JMBR.36.2.212-224
- Kaufman, A.S., & Kaufman, N.L. (2004). Kaufman Brief Intelligence Test (2nd ed.). Circle Pines, MN: American Guidance Service.
- Kent, R.D., & Vorperian, H.K. (2013). Speech impairment in Down syndrome: A review. Journal of Speech, Language, and Hearing Research, 56, 178–210. doi:https://doi.org/10.1044/1092-4388(2012/12-0148)
- Kumin, L. (2006). Speech intelligibility and childhood verbal apraxia in children with Down syndrome. Down Syndrome Research and Practice, 10, 10–22. doi:10.3104/reports.301
- Kumin, L., & Schoenbrodt, L. (2016). Employment in adults with Down syndrome in the United States: Results from a national survey. Journal of Applied Research in Intellectual Disabilities, 29, 330–345. doi:https://doi.org/10.1111/jar.12182
- La Rue Lewy, F. (2012). Communication and human rights: The United Nations special rapporteur. In A. V. Montiel (Ed.), Communication and human rights (pp. 55–59). Coyoacán, México: International Association for Media and Communication Research. Retrieved from www.iamcr.org.
- Lakens, D. (2013). Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Frontiers in Psychology, 4, 1–12. doi:https://doi.org/10.3389/fpsyg.2013.00863
- Lohmeier, H.L., & Shriberg, L.D. (2011). Reference data for the Syllable Repetition Task (SRT). Madison, WI: Phonology Project, Waisman Center, University of Wisconsin-Madison.
- Maas, E., Butalla, C.E., & Farinella, K.A. (2012). Feedback frequency in treatment for childhood apraxia of speech. American Journal of Speech–Language Pathology, 21, 239–257. doi:10.1044/1058-0360(2012/11-0119)
- Maas, E., Robin, D.A., Austermann Hula, S.N., Freedman, S.E., Wulf, G., Ballard, K.J., & Schmidt, R.A. (2008). Principles of motor learning in treatment of motor speech disorders. American Journal of Speech–Language Pathology, 17, 277–298. doi:10.1044/1058-0360(2008/025)
- McDaniel, J., & Yoder, P.J. (2016). Pursuing precision speech-language therapy services for children with Down syndrome. Seminars in Speech and Language, 37, 239–251. doi:https://doi.org/10.1055/s-0036-1587708
- Meyer, C., Theodoros, D., & Hickson, L. (2017). Management of swallowing and communication difficulties in Down syndrome: A survey of speech–language pathologists. International Journal of Speech–Language Pathology, 19, 87–98. doi:https://doi.org/10.1080/17549507.2016.1221454
- National Joint Committee for the Communication Needs of Persons With Severe Disabilities. (2002). Access to communication services and supports: Concerns regarding the application of restrictive “eligibility” policies [Technical Report]. Retrieved from www.asha.org/policy
- Rose, Y., & McWhinney, B. (2016). PHON (Version 2.1.8.). Retrieved from https://www.phon.ca/phontrac
- Rupela, V., Velleman, S.L., & Andrianopoulos, M.V. (2016). Motor speech skills in children with Down syndrome: A descriptive study. International Journal of Speech–Language Pathology, 18, 483–492. doi:https://doi.org/10.3109/17549507.2015.1112836
- Rvachew, S., & Brosseau-Lapré, F. (2018). Developmental phonological disorders: Foundations of clinical practice (2nd ed.). San Diego, CA: Plural Publishing.
- Rvachew, S., Hodge, M., & Ohberg, A. (2005). Obtaining and interpreting maximum performance tasks from children: A tutorial. Journal of Speech–Language Pathology and Audiology, 29, 146–156.
- Rvachew, S., & Matthews, T. (2017a). Using the Syllable Repetition Task to reveal underlying speech processes in Childhood Apraxia of Speech: A tutorial. Canadian Journal of Speech–Language Pathology and Audiology, 41, 106–126.
- Rvachew, S., & Matthews, T. (2017b). Demonstrating treatment efficacy using the single subject randomisation design: A tutorial and demonstration. Journal of Communication Disorders, 67, 1–13. doi:https://doi.org/10.1016/j.jcomdis.2017.04.003
- Shriberg, L.D., & Kwiatkowski, J. (1982). Phonological disorders III: A procedure for assessing severity of involvement. Journal of Speech and Hearing Disorders, 47, 256–270. doi:10.1044/jshd.4703.256
- Shriberg, L.D., Lohmeier, H.L., Campbell, T.F., Dollaghan, C.A., Green, J.R., & Moore, C.A. (2009). A nonword repetition task for speakers with misarticulations: The syllable repetition task. Journal of Speech, Language, and Hearing Research, 52, 1189–1212. doi:10.1044/1092-4388(2009/08-0047)
- Shriberg, L.D., Lohmeier, H.L., Strand, E.A., & Jakielski, K.J. (2012). Encoding, memorial and transcoding deficits in Childhood Apraxia of Speech. Clinical Linguistics and Phonetics, 26, 445–482. doi:10.3109/02699206.2012.655841
- Statistics Canada. (2003). Children with disabilities and the educational system-a provincial perspective. Statistics Canada. Retrieved from http://www.statcan.gc.ca/pub/81-004-x/2007001/9631-eng.htm#c
- Tate, R.L., Perdices, M., Rosenkoetter, U., Shadish, W., Vohra, S., Barlow, D.H., … Wilson, B. (2016). The Single-Case Reporting guideline In BEhavioural interventions (SCRIBE) 2016 statement. Journal of School Psychology, 56, 133–142. doi:https://doi.org/10.1016/j.jsp.2016.04.001
- United Nations. (1948). Universal declaration of human rights. Retrieved from http://www.un.org/en/universal-declaration-human-rights/index.html
- Urbaniak, G.C., & Plous, S. (2013). Research randomiser (Version 4.0). [Computer software]. Retrieved from http://www.randomiser.org/