
Abstract
Purpose: Transcription of speech sounds is a fundamental skill used by speech-language pathologists. Little is known about the impact of professional development courses on transcription accuracy and confidence. This study explored speech-language pathologists’ use and perceptions of transcription and the effect of a professional development course on their transcription accuracy and confidence.
Method: A quasi-experimental, one-group pretest-posttest design was used. Twenty-two Australian speech-language pathologists working with children with speech sound disorders participated in the course. Participants transcribed single words and completed a survey about confidence, perceptions, and the use of transcription at both time points.
Result: The number of participants who reported feeling confident about using transcription significantly increased from 36.84% pre-training to 68.42% post-training. Transcription accuracy of phonemes based on point-to-point accuracy was high pre-training (88.97%) and did not significantly improve. Participants identified strategies to maintain their transcription skills.
Conclusion: This study suggests speech-language pathologists transcribe single words in typical speech with high accuracy using broad transcription, and that participating in a transcription professional development course increases their transcription confidence. Further research is needed to explore different delivery methods of professional development, the impact of professional development on transcription accuracy of disordered speech, and the long-term impacts of professional development on transcription accuracy and confidence.
Introduction
Transcription of speech sounds is the written representation of speech sounds using symbols from the International Phonetic Alphabet (IPA) and Extensions to the International Phonetic Alphabet (extIPA) for disordered speech (Cox & Fletcher, Citation2017; International Phonetic Association, Citation2015; Müller & Ball, Citation2012). Transcription is a core skill for speech-language pathologists (SLPs) working with children with speech sound disorders (SSD) because it allows the SLPs to record how these children speak. Accurate transcription is essential to assess, analyse, and differentially diagnose the type of SSD; identify appropriate intervention; and track intervention progress (Child Speech Disorder Research Network, Citation2017; McLeod & Baker, Citation2017; Olswang & Bain, Citation1994). Transcription is used by 74.9% of SLPs in the UK (Knight et al., Citation2018) and 95.2% of Australian SLPs who work with children with SSD (Nelson et al., Citation2020). This paper will focus on transcription in an Australian English context.
The transcription of speech sounds is different from orthographic transcription, which is the written representation of words using alphabetic symbols (e.g. cat). Speech sounds can be transcribed in two ways. Broad transcription (phonemic transcription) represents phonemes, or sound units (e.g. /kæt/), whereas narrow transcription (phonetic transcription) represents allophones and detailed aspects of speech sounds (e.g. [khæt], where [h] indicates aspiration when [k] is released). Narrow transcription captures more detail than broad transcription but is more time consuming and has reduced interrater reliability (Ball et al., Citation2009; Shriberg & Lof, Citation1991). Transcription of speech sounds is initially taught to speech-language pathology students during their training (Howard & Heselwood, Citation2002) as it is a fundamental “profession-specific competency” (Child Speech Disorder Research Network, Citation2017, p.1).
Learning transcription at university
A small number of studies have surveyed speech-language pathology students and practising SLPs about their perceptions of learning transcription during their training to qualify as SLPs. A survey of 40 final year speech-language pathology students in the Republic of Ireland reported on their current experiences (Shaw & Yanushevskaya, Citation2022) and a larger survey of 759 British practising SLPs reported on their experiences of learning transcription retrospectively (Knight et al., Citation2018). Several barriers to learning transcription at university were identified: poor teaching methods (such as too much emphasis on clinically irrelevant theory), having an accent that differed from the cohort, large class sizes, difficulty remembering the symbol-sound correspondence for IPA symbols and diacritics, and difficulty understanding the relevance of transcription to speech-language pathology (Knight et al., Citation2018; Shaw & Yanushevskaya, Citation2022). Irish speech-language pathology students reported not feeling confident or equipped to use transcription whilst on placement nor ready to enter the workforce due to these barriers, despite using transcription on at least one placement (Shaw & Yanushevskaya, Citation2022).
Few studies have investigated practising SLPs’ self-reported transcription use, and barriers and facilitators to using transcription; yet, transcription is fundamental to the management of children with speech sound disorders. Through transcription, we can understand a child’s speech difficulties, make a plan about how to manage the difficulties, and determine what further assessment is required (Child Speech Disorder Research Network, Citation2017).
SLPs’ use and perceptions of transcription
To the best of our knowledge, the literature is limited to two studies that collected data via online surveys in the UK and Australia. Researchers investigated SLPs’ self-reported current use of transcription; perceived facilitators and barriers to using transcription and maintaining transcription skills; and suggestions for lessening these barriers when working with children with SSD. A large survey of 759 SLPs was conducted in the UK (Knight et al., Citation2018) and a smaller study of 84 SLPs was completed in Australia (Nelson et al., Citation2020).
Of the surveyed Australian SLPs, 39% used a combination of broad and narrow transcription (Nelson et al., Citation2020), compared to 45% of surveyed British SLPs (Knight et al., Citation2018). Exclusive use of broad transcription was reportedly used by 55% of the surveyed Australian SLPs (Nelson et al., Citation2020) and 40% of the surveyed British SLPs (Knight et al., Citation2018). Many SLPs reported using broad transcription for clients with a SSD that was not complex enough to need narrow transcription (i.e. no distortions of speech sounds); however, some SLPs also cited time constraints as a reason for favouring broad over narrow (Knight et al., Citation2018). Diacritics were reportedly used by 39% of surveyed Australian SLPs when further detail was required (Nelson et al., Citation2020). In both countries, 3% of surveyed SLPs reported using narrow transcription exclusively, particularly with cleft palate, atypical speech errors, hearing impairment, or when the SLP wanted a more detailed analysis (Knight et al., Citation2018; Nelson et al., Citation2020).
Like the students, SLPs reported reduced confidence and skill as barriers to effective transcription usage, particularly for narrow transcription. Participants reported these issues were perpetuated by reduced time to practise transcription, competing professional demands, and a lack of support from workplaces (Knight et al., Citation2018; Nelson et al., Citation2020; Shaw & Yanushevskaya, Citation2022).
Transcribing consonants and vowels
To describe the speech system of a child, it is important to record and transcribe both consonants and vowels produced by the child. Both students and practising SLPs reported that when learning to transcribe, vowels were more difficult to transcribe than consonants (Knight et al., Citation2018; Titterington & Bates, Citation2018), a perception shared by expert SLPs in speech sound disorders (Pollock & Berni, Citation2001). Correct transcription of vowels is important for accurate assessment and analysis of vowel production, including vowel errors. Transcription is also essential for analysing consonant-vowel interactions to identify contexts where vowels may facilitate correct consonant production (Pollock & Berni, Citation2001).
In Australia, there are multiple ways to transcribe vowel sounds in Australian English. Vowels can be transcribed directly from the IPA, recommended for transcribing atypical vowel production (Barrett et al., Citation2020), or by using one of two phonemic vowel notation systems. These systems use different IPA vowel symbols to represent the broad vowel production among speakers of Standard Australian English (Cox, Citation2008). One system is the 1965 Mitchell-Delbridge (MD) notation system, based on the Australian vowel production at the time, similar to British English vowel production (Mitchell & Delbridge, Citation1965). The second is the 1997 Harrington, Cox and Evans (HCE) notation system, based on modern Standard Australian English vowel production (Harrington et al., Citation1997). The HCE vowel notation system is arguably a more accurate representation of modern Standard Australian English vowel production than MD (Cox, Citation2008).
Nelson et al. (Citation2020) found that the surveyed Australian SLPs use the following when transcribing: IPA (80%), HCE (27.2%), MD (23.5%), and extIPA (18.5%). As both MD and HCE vowel notation systems are widely used, Australian SLPs reported that the lack of notation consistency between SLPs is a barrier to effective reporting of speech production. SLPs who trained using MD and wanted to upskill to HCE reported difficulty learning and remembering the symbols (Nelson et al., Citation2020). The surveyed Australian SLPs identified vowel notation systems as a topic to address in professional development (Nelson et al., Citation2020).
Professional development for transcription
Professional development postgraduation is routinely used to upskill health professionals, including SLPs (Gibbs, Citation2011). Professional development in transcription is instrumental to ensure practising SLPs maintain their confidence and skills to use transcription clinically (Howard & Heselwood, Citation2002). Despite 69% expressing interest in attending transcription professional development for narrow transcription, HCE, and overall skill improvement, less than 10% of surveyed Australian SLPs reported attending professional development for transcription (Nelson et al., Citation2020). Similarly, 75% of surveyed British SLPs expressed interest in participating in refresher courses (Knight et al., Citation2018). Of the Irish students surveyed, 82% acknowledged needing ongoing practice and maintenance of their transcription skills, including through professional development after graduating (Shaw & Yanushevskaya, Citation2022). The high proportion of SLPs expressing a desire to participate in transcription professional development and the low participation in training raises questions about why such a disparity exists. Investigation of the barriers to SLPs’ engagement with professional development for transcription is warranted.
Only two studies investigated the impact of professional development for practising SLPs on transcription accuracy. These studies used the Cleft Audit Protocol for Speech—Augmented (CAPS-A) (John et al., Citation2006). They reported improved interrater reliability of speech parameter ratings (e.g. resonance, nasal airflow) of the speech of children with cleft lip and palate following training (Chapman et al., Citation2016; Sell et al., Citation2009). Transcription accuracy was not the focus of these study; however, for CAPS-A, participants needed to use narrow transcription and listen to speech parameters to accurately transcribe the speech of children with cleft lip and palate. These findings cannot be assumed to generalise to professional development for transcription of the speech of children from all subgroups of SSD or with typical speech, as speech errors in children with cleft lip and palate are unique and are often transcribed using non-English IPA symbols (Gooch et al., Citation2001). Australian SLPs have a higher proportion of children with SSD of unknown origin in their workloads compared to children with SSD associated with craniofacial impairment (including cleft lip and palate; Nelson et al., Citation2020; Ttofari Eecen et al., Citation2019).
Purpose statement and research questions
Currently, there is limited research on whether and how transcription professional development for practising SLPs may change their transcription accuracy and confidence. SLPs have reported reduced skill and confidence in transcribing, and identified needing professional development to develop their transcription skills. Therefore, the impact of transcription professional development on improving accuracy and confidence in transcribing must be evaluated. The research questions for this study are:
Does a professional development course targeting transcription skills change the accuracy of SLPs’ transcription skills?
Does a professional development course targeting transcription skills change SLPs’ confidence in using transcription?
Do SLPs report that they will change how they use transcription following the completion of a transcription professional development course?
What types of strategies do SLPs report they will employ to maintain their transcription skills following completion of a transcription professional development course?
Method
Ethical permissions
Ethical approval for the study was obtained from Australian Catholic University Human Research Ethics Committee (ACU HREC; 2020-190E). Written informed consent was obtained from participants.
Design
This concurrent mixed methods study used a quasi-experimental, one-group pretest-posttest design (Grbich, Citation2017).
Participant recruitment
Practising SLPs working in Victoria, Australia were invited to attend the course and participate in the study. Participants were required to have primary and/or secondary school-aged students with SSD on their caseloads. Arms-length recruitment, snowball sampling, and convenience sampling were used to recruit participants. Potential participants were recruited by the researchers by emailing their professional networks and asking them to forward the invitation to people who potentially met the inclusion criteria. Researchers posted advertisements for the study on their Facebook and LinkedIn accounts, and advertised through Speech Pathology Australia e-news (Australian national peak body for the speech-language pathology profession). Potential participants read the participant information letter; if they were interested, they completed an expression of interest online and indicated their preferred dates of training.
Participant demographics
Twenty-four SLPs from Victoria participated in the professional development course. Of the attendees, 22 consented to participate in the study. All worked in primary schools and 72% also worked in secondary schools, predominately public or Catholic schools. The majority completed their speech-language pathology training in Australia and had been practising as a SLP for up to 15 years, with the majority practising between 1–10 years. The mean age of participants was 31.55 years (SD 8.13). displays the demographics of the participants.
Table I. Participant demographics.
Professional development course
The professional development course was held twice to maximise the number of participants who could attend, once in February 2021 and once in April 2021. No changes were made to the delivery of the course between the first and second iterations. Five participants attended the course in February and 17 participants attended in April. Each participant attended two 2-hour sessions over two days within the same week. This included time to complete the pre-training survey and post-training survey (20 minutes each), resulting in a total of 3 hours and 20 minutes of training. The course was delivered by the second and third authors via Zoom, due to the COVID-19 pandemic.
The course content was aimed at the transcription of the speech of school-aged children with SSD. The first training session reviewed broad (phonemic) vs. narrow (phonetic) transcription, vowel transcription, different notation systems (HCE vowels, MD vowels, other IPA vowels), and the benefits of using HCE vowels. Participants practised identifying HCE vowel symbols, and transcribing single words and sentences of typical speech synchronously. They graded their accuracy on these exercises using suggested answers. They also explored resources to use for practising transcription (free-to-access websites—IPA charts, recordings of single words, and sentences with suggested answers for practising transcription). The second training session focused on transcribing children’s speech and speech errors (consonant and vowel errors, predominantly SSD of unknown origin), and the benefits of transcribing connected speech (obtaining further information in a more functional context). Content covered included diacritics (e.g. dental [ ̪ ], nasalised [ ̃]) and non-English IPA symbols (e.g. labiodental approximant [ʋ]). Participants practised transcribing words and phrases of disordered speech synchronously, graded their accuracy on these exercises using suggested answers, and explored strategies they could use to maintain their transcription skills. Please see Supplemental Materials for further details on the training.
Data collection
Data were collected from participants at the beginning and end of the course via a Qualtrics survey. The survey included questions exploring participants’ experience and confidence using transcription, and a transcription task assessing broad transcription skills (accuracy). Pre-training data collection occurred during the first 20 minutes of the first day of the course. Post-training data collection occurred during the last 20 minutes of the second day of the course.
Pre-training, participants answered nine closed questions about their demographics. To capture pre-training use and perceptions of transcription, participants completed two closed questions, four Likert scale questions, and one open text question. Post-training, participants answered two Likert scale questions, two open questions about their confidence and likelihood to use transcription following completion of the course, and one closed question about the strategies they would use to maintain their transcription skills. Participants also rated their confidence in use of transcription in clinical settings pre- and post-training on a 5-point Likert scale. These questions asked the participants to reflect on transcription in general and did not specify broad transcription or narrow transcription.
Data on participants’ broad transcription accuracy and confidence to use transcription was collected pre- and post-training. For transcription accuracy, participants were required to transcribe single words using broad transcription, replicating SLPs’ reported current use of transcription in clinical settings (Nelson et al., Citation2020). Pre-training, participants transcribed ten single words from an audio sample of a school-aged child with typical speech development using broad transcription. The sample was recorded using the iPhone audio function. Participants could listen to the audio recording as many times as they wanted during the 20 minutes allocated to data collection. Post-training, participants transcribed ten different words from an audio sample of the same child. The stimuli used pre- and post-training were different from each other, but had similar syllable structures and the same number of consonants and vowels (37 phonemes, 23 consonants, 14 vowels). Participants were given a handout with the HCE vowel symbols and their equivalent MD vowel symbol (to replicate clinical conditions), and an online link to the IPA Character Picker App 27 (r12a, Citation2021; https://r12a.github.io/pickers/ipa/) where they could copy the IPA symbols and paste them in a Microsoft Word document. The Microsoft Word document with the transcribed words was submitted online via the Qualtrics platform.
Data analysis
Quantitative and qualitative data were analysed separately. Analysis of the quantitative data from the participants’ transcriptions and surveys was conducted using the Statistical Program for the Social Sciences (SPSS) Version 28 (IBM Corporation, Citation2021). Participants’ responses were also summarised using descriptive statistics (median, interquartile range [IQR], and frequencies). Qualitative data were analysed using inductive content analysis, as described by Elo and Kyngäs (Citation2008).
Quantitative data
Transcription accuracy was determined by calculating the percentage of correctly transcribed units based on point-to-point agreement with the words transcribed by the researchers. Three of the researchers came up with a transcription for each word via consensus. The percentage of phonemes correct (PPC), percentage of consonants correct (PCC), and percentage of vowels correct (PVC) matrices were used; these are common clinical and research measures of severity for assessing SSD. The accuracy measures were analysed using descriptive statistics, including median and IQR, and inferential statistics to compare the change in transcription accuracy pre- and post-training. Shapiro-Wilk tests indicated the transcription accuracy measures were not normally distributed: pre-training PPC, W = 0.86, p = 0.03; pre-training PCC, W = 0.55, p < 0.01; pre-training PVC, W = 0.84, p = 0.02; post-training PPC, W = 0.83, p = 0.02; post-training PCC, W = 0.52, p < 0.01; and post-training PVC, W = 0.83, p = 0.03. Therefore, Wilcoxon signed-rank tests were performed to examine changes in transcription accuracy pre- and post-training.
Participants were asked to use the same vowel notation system (either MD or HCE) for both their pre- and post-training transcriptions, and note down which one they used. However, some participants did not use the same vowel notation system for both their transcriptions (pre- and post-training). Therefore, transcription accuracy was analysed in two groups. The first group used the same vowel notation system (either HCE or MD) in their pre- and post-training transcription (n = 13). The second group used MD in their pre-training transcription and HCE in their post-training transcription (n = 5). The transcriptions of four participants were not submitted online. This may have been due to technical difficulties with using the online platform or participant choice not to submit their responses.
Participants’ self-rating of confidence was analysed using descriptive (median, IQR) and inferential statistics. Shapiro–Wilk tests also indicated participants’ self-reported confidence was not normally distributed: pre-training confidence, W = 0.85, p < 0.01 and post-training confidence, W = 0.73, p < 0.01. Therefore, Wilcoxon signed-rank tests were performed to examine changes in confidence pre- and post-training.
Additionally, the difference between participants’ transcription scores pre- and post-training, and the difference between their confidence rating pre- and post-training, were further analysed. The aim of this analysis was to determine if there was a relationship between the change in transcription accuracy and the change in confidence pre- and post-training.
Qualitative data
Text responses to the three open survey questions were analysed using inductive content analysis, as described by Elo and Kyngäs (Citation2008). Each question was analysed individually. In the preparation phase, participants’ responses were read to understand their perceptions of transcription and the course. Meaning units (words or groups of words with the same meaning) were selected from the responses. Each meaning unit was coded, counted, and grouped into subcategories. Main categories were formed from the subcategories.
The researchers took measures to ensure the trustworthiness of the data (Lincoln & Guba, Citation1985). Three of the researchers completed the analysis process independently, and then collaborated to come to a consensus on codes that were different, ensuring the credibility of the data. The qualitative data triangulated with the quantitative data, ensuring the confirmability of the data.
Result
The results will be presented in five sections: (a) pre-training use and perceptions of transcription, (b) transcription accuracy, (c) confidence in using transcription, (d) anticipated future use of transcription, and (e) strategies for maintaining transcription skills.
Pre-training use and perceptions of transcription
Prior to the training, participants were asked how often they used transcription when working with children with suspected SSD, and which transcription systems they used (presented in ). All participants used transcription in their clinical practice to inform service delivery. Participants reported that they used transcription for assessment, screening, diagnosis, goal setting, monitoring of therapy progress, and to inform discharge. Half of the participants reported that they used the MD transcription system and approximately one-third of participants used the HCE transcription system for vowels.
Table II. Participants’ current use of transcription pre-training.
Participants rated how much they agreed that time, confidence, and skill impacted their decision to use transcription. Just over two-thirds (68.18%) of participants agreed or strongly agreed that time impacted their decision to use transcription. Four-fifths of participants agreed or strongly agreed that confidence (81.81%) and skill (81.82%) impacted their decision to use transcription.
Seven participants answered an open question where they were required to describe other factors that impact their decision to use transcription. Content analysis revealed the external and internal factors that impacted participants’ decisions to use transcription. The main categories and associated subcategories are presented in . Participants’ quotes supporting these categories are provided, followed by the participant identification number in parentheses.
Figure 1. Participants’ reported additional factors that impact their decision to use transcription. Number in brackets notes the number of meaning units in the main categories and subcategories.
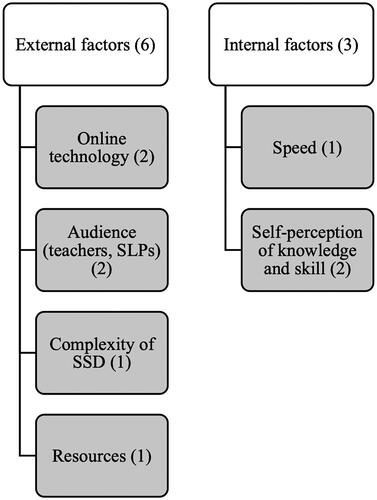
The external factors that participants reported may impact their decision to use transcription included online technology, audience, the complexity of SSD, and resources. One participant reported that their “online system for completing case notes does not allow the use of IPA symbols” (P1). When considering the audience reading documentation that includes transcription, one participant wrote they “use it to maintain consistency with other speech pathologists” but would “convert transcription symbols to phonic spellings” for teachers, as “teachers are unable to read the transcription” (P13). To support their transcription skill, one participant stated that they have “transcription symbols in [their] diary to use if [they] get stuck” (P19).
The internal factors that participants reported may impact their decision to use transcription were transcription speed, and self-perception of transcription skill and knowledge. One participant reflected that they were “unpractised”, causing their transcription to be “very slow” and that the symbols for “long vowels are easily forgotten” (P11). Another commented that their transcription “may not be very accurate at times” (P7).
Transcription accuracy
Seventeen of the 22 participants completed both pre- and post-training transcription. Where participants only completed either the pre- or post-training transcription, this data was not used in the analysis. Thirteen used the same vowel notation for the pre- and post-training transcription; five used MD, and eight used HCE. Four participants used MD for the pre-training transcription and HCE for the post-training transcription. Separate analyses were conducted for each group.
(same transcription system pre- and post-training) and (different transcription system pre- and post-training) show the mean number of correctly transcribed phonemes, consonants, and vowels in the pre- and post-training transcription task for the two groups. Both groups had high transcription accuracy scores for transcribing consonants, with a median of 100% accuracy for both groups pre- and post-training. For vowels, both groups (same vowel transcription system and different vowel transcription systems pre- and post-training) showed improvement in accuracy, but the changes did not reach statistical significance (see and ). Wilcoxon signed-rank tests found no statistically significant changes in transcription accuracy pre- to post-training for phonemes, consonants, or vowels.
Table III. Pre- and post-training comparison of participants’ transcription accuracy (same vowel system).
Table IV. Pre-training (Mitchell-Delbridge) and post-training (Harrington, Cox and Evans) comparison of participants’ transcription accuracy.
Confidence in using transcription
Nineteen of the 22 participants completed pre- and post-training self-ratings of their confidence to use transcription. Pre-training, seven participants (36.84%) agreed they felt confident using transcription with school-aged children with SSD; 0% strongly agreed. Post-training, 68.42% either agreed or strongly agreed that they felt confident using the transcription. The median rating pre-training was 3 (IQR 2), and the median rating post-training was 4 (IQR 1; out of a maximum of 5). A Wilcoxon signed-rank test found participants’ increased confidence was statistically significant (Z = –2.75, p < 0.01).
Table V. Strategies and resources identified for maintaining transcription skills post-training (n = 20).
Participants were asked an open question about whether they had noticed any changes to their confidence post-training. This question was analysed using content analysis and the results will be presented in the categories and subcategories identified. The two most reported categories were: (1) More confident and (2) Improved knowledge, understanding, and awareness. presents the categories and associated subcategories. Participants’ quotes supporting these categories are provided, followed by the participant identification number in parentheses.
Figure 2. Participants’ reported changes in confidence post-training. The number in brackets notes the number of meaning units in the main categories and subcategories.
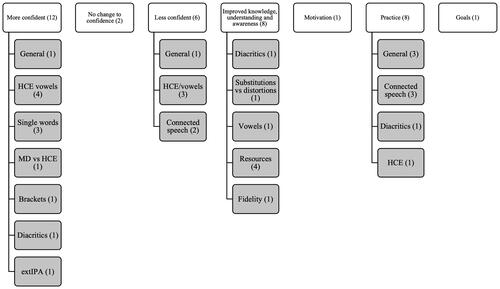
More confident
One participant reported “feeling a little more confident” in general (P15). One participant commented that they felt “more confident knowing the difference between MD and HCE, / /vs [ ] [brackets] and some more about the diacritics” (P16). Others wrote that they felt “more confident using diacritics and extIPA symbols” (P17) and were “able to transcribe single words confidently” (P22). Participants also reported feeling more confident with HCE, such as P1: “a lot more confident with using HCE since doing this course” and P8 who “previously used MD” and was “slowly becoming more confident with some of the HCE vowel transcriptions” (P8).
Improved knowledge, understanding, and awareness
Some participants reported improved knowledge, understanding, and awareness of different transcription elements. One reported that the course had given them “food for thought about [their] fidelity when transcribing” (P9). Others reported a “better understanding of substitutions vs distortions” (P18) and “improved knowledge of using diacritics for transcription of speech sound errors” (P1). Several participants also reported feeling they now knew what to focus on for future learning, such as “better understanding of what areas need to work on” (P15), “upskill on vowel transcription” (P5), and “[knowing] where to turn to access relevant resources” (P21).
Less confident
Contrastingly, one participant reported feeling “confident when transcribing in MD” but being “new to HCE”, they felt “less confident with those vowels” (P4). Another participant wrote they were “struggling to transcribe connected speech in real time” (P13).
Practise
Several participants reflected they needed “much more practice to be confident” (P21) and needed to “practise these skills in order for them to improve” (P20). One who used MD vowels reported wanting to “practise it more regularly with the HCE system” (P9). Another reported they “need to practise with diacritics and connected speech, particularly for students with severe speech disorders” (P22).
Correlation between confidence and transcription accuracy
Statistically significant positive correlations between transcription confidence and accuracy were found in the group that used the same transcription system pre- and post-training. There was a strong correlation between the change in confidence and change in vowel transcription accuracy, r(11) = 0.61, p = 0.03, as well as increased confidence and increased phoneme transcription accuracy, r(11) = 0.62, p = 0.02. The group that used different transcription systems did not show a statistically significant correlation between increased confidence and increased vowel transcription accuracy, r(2) = 0.94, p = 0.06, or increased confidence and increase phoneme transcription accuracy, r(2) = 0.70, p = 0.30. Neither group recorded a statistically significant correlation between increased confidence and increased consonant transcription accuracy—same transcription system, r(11) = 0.38, p = 0.20 and different transcription system, r(2) = –0.91, p = 0.10.
Anticipated future use of transcription
Twenty of the 22 participants completed the post-training survey questions. Participants were asked to rate how likely they were to use transcription with a school-aged child with a suspected SSD in the future. Of these 20 participants, 14 (70%) reported being extremely likely to use it and six (30%) reported being likely to use it.
Participants were asked an open question about whether they had noticed any changes in their likelihood to use transcription since the start of the training course. 30% of these 20 participants indicated they were likely to use transcription more, while 35% reported no change or that they would continue to use transcription in the same way. The 20 participants indicated they aimed to use the following in their clinical practice more: narrow transcription/diacritics (35%), HCE vowels (15%), transcribe connected speech (10%), use extIPA (5%), and record the vowel notation system used (5%). Some participants also made the following transcription goals: increase transcription accuracy (24%), practise transcription more (5%), practise vowel transcription (5%), increase transcription speed (5%), and use resources when practising transcription (5%).
Elements to use more
Several participants who previously used MD vowels reported wanting to begin “transitioning to HCE notation” (P17). One noted that they would “try to be more consistent and note which system [they are] using to transcribe” (P12). Another reflected that they “need to revise and practise the vowels more” (P6). Some reported they could see the benefit to using diacritics, with P8 stating they were “more likely to use some of the diacritics in [their] transcriptions now as [they] can see how this will improve the accuracy of the transcription” and P22 stating that diacritics could be used to “identify patterns in children’s speech”. One noted that they would “make more of an effort to use the extended IPA” (P4).
Participants reported that, since completing the course, they were more likely to “attempt to phonetically transcribe speech samples” (P15) and hoped to be “more accurate and faster” with their transcription (P18). One commented that they intend to use transcription more because they now “know where to go to check if [their] transcription is accurate” and can “access resources” (P20).
Strategies for maintaining transcription skills
Twenty of the 22 participants identified which of the listed strategies and resources they would use to maintain their transcription skills following the course (presented in ). The highest reported strategies and resources that participants identified to maintain their transcription skills were websites (90%), transcription charts (90%), self-practice (85%), and calibration meetings with work colleagues (60%).
Discussion
Professional development is used to continue the education of health professionals after graduation (Gibbs, Citation2011). This study focused on the impact of professional development on the transcription of Standard Australian English, but the findings may be applied to an international context. The findings indicated Australian SLPs who participated in a course on transcription reported increased confidence to transcribe, consistent with previous research.
Changes to transcription confidence
Participants’ increased transcription confidence following the course was statistically significant. Participants reported that their increased confidence came from increased knowledge, understanding, and awareness of transcription elements that were covered in the course, particularly diacritics, extended IPA, vowel transcription systems, substitutions, distortions, and which brackets to use for broad vs narrow transcription. These findings suggest that professional development is beneficial for increasing SLPs’ confidence in clinical skills, and supports the provision of further professional development in transcription by professional associations representing SLPs and/or universities.
The findings about SLPs’ increased confidence after participating in a synchronous training program from this research are consistent with other research on the impact of asynchronous computer-based training of students in transcription. Speech-language pathology students reported increased confidence after completing weekly online modules, including exercises and quizzes (Titterington & Bates, Citation2018), and using computer software (Hillenbrand et al., Citation2015). When working through the course materials at their own pace, these participants reportedly felt more confident after practising transcription elements that they previously found difficult.
While the findings on change in confidence are positive, it must be noted that the participants in this study were asked to rate their confidence about transcription in general, and not specifically their confidence to use broad transcription (as was assessed to assess transcription accuracy) or narrow transcription (as was discussed on the second day of the professional development course). Previous studies such as Knight et al. (Citation2018) specified that SLPs’ lack of confidence was related to their knowledge of narrow transcription.
Changes to transcription accuracy
In this study, there was no statistically significant change in participants’ transcription accuracy pre- and post-training. A ceiling effect may have impacted on the results—the median accuracy of phoneme transcription pre-training was 34/37 correct, and 18.18% of participants scored 37/37 (100% correct) on their transcription of phonemes pre-training. Another factor that may have contributed to high pre-training scores could be the use of a speech sample of a typically developing school-aged child, resulting in a highly accurate transcription of consonants. Despite the high accuracy in transcription, only 36.84% of participants agreed that they felt confident using transcription with school-aged children with SSD pre-training and none strongly agreed. While SLPs’ broad transcription accuracy of typical speech was high, their skill level did not match their confidence in their ability to transcribe. The discrepancy between accuracy and confidence may be because participants were rating their confidence in the transcription of disordered speech, which was not assessed in this study’s accuracy task.
The lack of statistically significant change in accuracy following a transcription course differed from studies on Cleft Audit Protocol for Speech—Augmented (CAPS-A) training, which found improved interrater reliability on rating speech parameters of cleft palate speech following a program of systematic training (Chapman et al., Citation2016; Sell et al., Citation2009). These studies differed from the current research because they measured the rating of speech parameters, whereas the current study investigated transcription accuracy. Furthermore, the current research involved transcription of typically developing speech, whereas Chapman et al. (Citation2016) and Sell et al. (Citation2009) investigated interrater reliability of rating of cleft palate speech. Perceptual assessment of cleft palate speech is more complex than typical speech and involves not just a judgement about phone production, but also compensatory articulations, resonance, and features related to velopharyngeal function (Chapman et al., Citation2016). The training in these studies was provided over 3 days, longer than in this study (4 hours over 2 days) and gave participants greater opportunities for practice than in our study.
Our finding of no statistically significant change in transcription accuracy also differs from the small number of articles that have described using computer-based teaching aids on transcription in speech-language pathology courses. These studies used different delivery methods of content and activities. Titterington & Bates (Citation2018) utilised a self-paced online module that students could access for up to 4 weeks, whereas Krimm et al. (Citation2017) studied the effectiveness of weekly online activities that students independently worked through in conjunction with university coursework. In both studies, activities could be accessed over several weeks, compared to 2 days in the same week in this study. These studies, therefore, allowed time to consolidate learning and spaced repetition, the lack of which likely contributed to no significant changes in this study. Students’ IPA symbol knowledge and transcription ability improved following the completion of online transcription modules, and they performed better on their transcription coursework compared to those who studied coursework without any online content (Krimm et al., Citation2017; Titterington & Bates, Citation2018). These students had no prior knowledge of IPA or transcription, unlike the SLPs from this study, which may explain the difference in study findings.
Australian SLPs who typically use MD vowels previously reported difficulty learning and using HCE vowels (Nelson et al., Citation2020). Median vowel accuracy in the group of participants who used MD pre-training and HCE post-training in the surveys in this study remained the same, despite changing from one notation system to another, suggesting that training was beneficial to transition to a different vowel notation system. This research suggests that, whilst maintaining their transcription accuracy, practising Australian SLPs can upskill from using MD vowels to HCE vowels in a short period of time. When transitioning from one vowel notation system to another, this is best achieved when SLPs are supported with handouts that include both notation systems.
The professional development course in this study provided participants with opportunities to practise their transcription skills and explore transcription elements that may be clinically relevant to their caseloads. Although participants’ increased accuracy in transcription was not statistically significant, a statistically significant positive correlation was found between increased transcription accuracy, particularly accuracy of vowels, and increased confidence. This finding suggests that as participants’ accuracy increased, so did their confidence to use transcription—or the other way around. Therefore, for SLPs to become more confident to use transcription clinically, it is likely they will need to increase their transcription accuracy through opportunities to practise their transcription skills.
Transcription barriers
Factors that influenced participants’ likelihood to use transcription in this research are similar to previous reports in the literature. Like the Australian SLPs in Nelson et al. (Citation2020), most participants in this research agreed that time, confidence, and competence/skills in transcription impacted their likelihood to use transcription. Likewise, UK SLPs reported that confidence impacted their decision to use narrow transcription (Knight et al., Citation2018).
Strategies for transcription practice
At least 85% of participants reported they would use websites, transcription charts, and self-practice to maintain their transcription skills, with 60% of participants reporting they planned to participate in calibration meetings with their work colleagues. These strategies are low cost, easily accessible by SLPs, and have been recommended by Stemberger and Bernhardt (Citation2020) for practising transcription. To engage in self-practice and calibration meetings, SLPs need to dedicate time to this and be supported by their workplace. Australian SLPs previously reported that workplace demands impacted their use of transcription (Nelson et al., Citation2020). British SLPs reported not feeling supported by their workplace to maintain their transcription skills, and indicated wanting transcription training and to practise with colleagues (Knight et al., Citation2018). The findings of this study provide further evidence that SLPs would like employers to allow time for transcription practice to maintain essential skills for clinical work with children with SSD.
In other studies, 69% of surveyed Australian SLPs and 75% of surveyed British SLPs had expressed interest in attending a course on transcription (Knight et al., Citation2018; Nelson et al., Citation2020). In this study, 25% of participants indicated they would use professional development courses to maintain their transcription skills following the completion of this course. This suggests most participants were confident to use the recommended resources and strategies to maintain their skills after this course and did not require attendance at further formal professional development.
Limitations and future research
A small sample of SLPs participated. Therefore, the findings may not be representative of all SLPs in Victoria, Australia, and caution is recommended when generalising the data. Furthermore, the high accuracy of transcription pre-training may be indicative of the sample being biased, i.e. people participating in the study having a particular interest in transcription.
The high accuracy of transcription pre-training could also be an indication that the samples may not have been challenging enough for a large portion of participants and not sensitive enough to identify change. Participants’ transcription accuracy was only assessed by broadly transcribing a small single-word sample of typical speech. Disordered and connected speech, which are crucial clinical skills and more challenging than transcribing typical speech, were not assessed. Future research could include more examples to transcribe, in addition to increasingly complex samples. This could include broad and narrow transcription, transcription of single word samples and connected speech samples, and samples with speech errors of increasing complexity, which may include the speech of children with cleft lip and palate and motor speech disorders.
Whilst acknowledging that this is a limitation of this preliminary study, the authors wanted to first investigate the impact of a professional development program on broad transcription. This is because broad transcription is used exclusively by a large proportion of SLPs (55% of Australian SLPs as reported by Nelson et al., Citation2020; 40% of British SLPs as reported by Knight et al., Citation2018). Therefore, these findings can be applied to real world clinical practice. It is important that future research also investigates the impact of a professional development program on narrow transcription. Both types of studies will contribute to the literature on the impact of professional development on practising SLPs’ knowledge, skills, and confidence in transcribing speech production. They will also inform the teaching of transcription to SLP students at university.
The format of the training could have impacted the research results. The training course in this study was online and synchronous. Further research is needed to explore the fidelity and effectiveness of different delivery methods of professional development for transcription, such as in-person or online asynchronous modules. In addition, participants were given vowel charts to use when transcribing, to mimic clinical practice; their transcription accuracy without such resources is unknown. Finally, the current study did not include any participant follow-up once the course concluded. Therefore, it is unknown what long-term impact the course had on participants’ transcription accuracy and confidence in clinical settings. It is also unknown if participants maintained their transcription skills or implemented the strategies suggested in the course. Future research studies should consider the pace of presentation of the professional development material, the time span of the professional development program, the number of opportunities to practise, and the ability of participants to select the number of practice opportunities based on personal choice. It is important that the mechanisms of change are explored in future professional development programs. Future research should also explore the long-term impact of professional development on transcription accuracy, confidence, and maintenance of transcription skills.
The data collection methods may have also impacted the study results. Some participants transcribed using one vowel notation system pre-training and then transcribed using a different vowel notation system post-training, making it more challenging to analyse the data. Although participants were asked to utilise the same notation system pre- and post-training, more clarity in communication or focusing on only one notation system both pre- and post-training may help with data integrity in future research. Furthermore, some participants experienced technical difficulties because they were unfamiliar with the technology used and some transcribed samples were not submitted. This resulted in data loss. In future online training programs, participants could be given step-by-step guides on the technology used as preparation for course attendance. Given the multiple notation systems used in Australia, future studies could investigate the teaching of transcription for speech-language pathology in Australian universities, including the number of universities that teach transcription using the MD vowel notation, HCE vowel notation, or both.
A final area that could be explored further is the relationship between confidence and accuracy of transcription, and its impact on service delivery and patient outcomes for children with SSD.
Conclusion
This study found SLPs could accurately transcribe typical speech using broad transcription, but were not confident about their transcription skills before the course. A professional development course can have a positive impact on SLPs’ confidence to use transcription, awareness of areas to upskill, and knowledge of strategies and resources to use for practice.
Supplemental Material
Download MS Word (21.9 KB)Acknowledgements
The research team would like to thank: Dr. Megan Willis, a statistician from the Faculty of Health Sciences, ACU; Dr. Anna Cronin, SLP researcher from the Faculty of Health Sciences, ACU; and the SLPs who participated in this study.
Declaration of interest
No potential conflict of interest was reported by the author(s).
References
- Ball, M., Müller, N., Klopfenstein, M., & Rutter, B. (2009). The importance of narrow phonetic transcription for highly unintelligible speech: Some examples. Logopedics, Phoniatrics, Vocology, 34(2), 84–90. https://doi.org/10.1080/14015430902913535
- Barrett, C., McCabe, P., Masso, S., & Preston, J. (2020). Protocol for the connected speech transcription of children with speech disorders: An example from childhood apraxia of speech. Folia Phoniatrica et Logopaedica, 72(2), 152–166. https://doi.org/10.1159/000500664
- Chapman, K. L., Baylis, A., Trost-Cardamone, J., Cordero, K. N., Dixon, A., Dobbelsteyn, C., Thurmes, A., Wilson, K., Harding-Bell, A., Sweeney, T., Stoddard, G., & Sell, D. (2016). The americleft speech project: A training and reliability study. The Cleft Palate-Craniofacial Journal , 53(1), 93–108. https://doi.org/10.1597/14-027
- Child Speech Disorder Research Network. (2017). Good practice guidelines for the analysis of child speech. https://www.nbt.nhs.uk/sites/default/files/BSLTRU_Good%20practice%20guidelines_Transcription_2Ed_2017.pdf
- Cox, F. (2008). Vowel transcription systems: An Australian perspective. International Journal of Speech-Language Pathology, 10(5), 327–333. https://doi.org/10.1080/17549500701855133
- Cox, F., & Fletcher, J. (2017). Australian English pronunciation and transcription. (2nd ed.). Cambridge University Press.
- Elo, S., & Kyngäs, H. (2008). The qualitative content analysis process. Journal of Advanced Nursing, 62(1), 107–115. https://doi.org/10.1111/j.1365-2648.2007.04569.x
- Gibbs, V. (2011). An investigation into the challenges facing the future provision of continuing professional development for allied health professionals in a changing healthcare environment. Radiography, 17(2), 152–157. https://doi.org/10.1016/j.radi.2011.01.005
- Gooch, J. L., Hardin-Jones, M., Chapman, K. L., Trost-Cardamone, J. E., & Sussman, J. (2001). Reliability of listener transcriptions of compensatory articulations. The Cleft Palate-Craniofacial Journal, 38(1), 59–67. https://doi.org/10.1597/1545-1569_2001_038_0059_roltoc_2.0.co_2
- Grbich, C. (2017). Integrated methods in health research. In P. Liamputtong (Ed.), Research methods in health: Foundations for evidence-based practice. (3rd ed., pp. 361–374). Oxford University Press.
- Harrington, J., Cox, F., & Evans, Z. (1997). An acoustic phonetic study of broad, general, and cultivated Australian English vowels. Australian Journal of Linguistics, 17(2), 155–184. https://doi.org/10.1080/07268609708599550
- Hillenbrand, J. M., Gayvert, R. T., & Clark, M. J. (2015). Phonetics exercises using the alvin experiment-control software. Journal of Speech, Language, and Hearing Research, 58(2), 171–184. https://doi.org/10.1044/2014_JSLHR-S-14-0149
- Howard, S. J., & Heselwood, B. C. (2002). Learning and teaching phonetic transcription for clinical purposes. Clinical Linguistics & Phonetics, 16(5), 371–401. https://doi.org/10.1080/02699200210135893
- IBM Corportation. (2021). IBM SPSS statistics (Version 28.0) [Computer software]. https://www.ibm.com/support/pages/downloading-ibm-spss-statistics-280
- International Phonetic Association. (2015). International phonetic alphabet chart. https://www.internationalphoneticassociation.org/content/full-ipa-chart
- John, A., Sell, D., Sweeney, T., Harding-Bell, A., & Williams, A. (2006). The cleft audit protocol for speech-augmented: A validated and reliable measure for auditing cleft speech. The Cleft Palate-Craniofacial Journal : official Publication of the American Cleft Palate-Craniofacial Association, 43(3), 272–288. https://doi.org/10.1597/04-141.116681400
- Knight, R. A., Bandali, C., Woodhead, C., & Vansadia, P. (2018). Clinicians’ views of the training, use and maintenance of phonetic transcription in speech and language therapy. International Journal of Language & Communication Disorders, 53(4), 776–787. https://doi.org/10.1111/1460-6984.12381
- Krimm, H., Schuele, M. C., & Brame, C. (2017). Viability of online learning for ensuring basic skills in speech-language pathology. Perspectives of the ASHA Special Interest Groups, 2(10), 49–58. https://doi.org/10.1044/persp2.SIG10.49
- Lincoln, Y. S., & Guba, E. G. (1985). Naturalistic inquiry. Sage.
- McLeod, S., & Baker, E. (2017). Children’s speech: An evidence-based approach to assessment and intervention. Pearson.
- Mitchell, A. G., & Delbridge, A. (1965). The pronunciation of English in Australia. (Rev. ed.). Angus and Robertson.
- Müller, N., & Ball, M. J. (2012). Linguistics, phonetics, and speech-language pathology: Clinical linguistics and phonetics. In N. Müller & M. J. Ball (Eds.), Research methods in clinical linguistics and phonetics: A practical guide. (Vol. 6, pp. 1–9). John Wiley & Sons. https://ebookcentral.proquest.com
- Nelson, T. L., Mok, Z., & Ttofari Eecen, K. (2020). Use of transcription when assessing children’s speech: Australian speech-language pathologists’ practices, challenges, and facilitators. Folia Phoniatrica et Logopaedica, 72(2), 131–142. https://doi.org/10.1159/000503131
- Olswang, L. B., & Bain, B. (1994). Data collection: Monitoring children’s treatment progress. American Journal of Speech-Language Pathology, 3(3), 55–66. https://doi.org/10.1044/1058-0360.0303.55
- Pollock, K. E., & Berni, M. C. (2001). Transcription of vowels. Topics in Language Disorders, 21(4), 22–40. https://doi.org/10.1097/00011363-200108000-00005
- r12a. (2021). IPA Character App (Version 27.0) [Computer app]. GitHub. https://r12a.github.io/pickers/ipa/
- Sell, D., John, A., Harding-Bell, A., Sweeney, T., Hegarty, F., & Freeman, J. (2009). Cleft audit protocol for speech (CAPS-A): A comprehensive training package for speech analysis. International Journal of Language & Communication Disorders, 44(4), 529–548. https://doi.org/10.1080/13682820802196815
- Shaw, Á., & Yanushevskaya, I. (2022). Students’ views and experiences of the training and use of phonetic transcription in speech and language therapy: The Irish perspective. Clinical Linguistics & Phonetics, 36(2-3), 276–291. Advance online publication. https://doi.org/10.1080/02699206.2021.1874055
- Shriberg, L. D., & Lof, G. L. (1991). Reliability studies in broad and narrow phonetic transcription. Clinical Linguistics & Phonetics, 5(3), 225–279. https://doi.org/10.3109/02699209108986113
- Stemberger, J. P., & Bernhardt, B. M. (2020). Phonetic transcription for speech-language pathology in the 21st century. Folia Phoniatrica et Logopaedica , 72(2), 75–83. https://doi.org/10.1159/000500701
- Titterington, J., & Bates, S. (2018). Practice makes perfect? The pedagogic value of online independent phonetic transcription practice for speech and language therapy students. Clinical Linguistics & Phonetics, 32(3), 249–266. https://doi.org/10.1080/02699206.2017.1350882
- Ttofari Eecen, K., Eadie, P., Morgan, A. T., & Reilly, S. (2019). Validation of Dodd’s model for differential diagnosis of childhood speech sound disorders: A longitudinal community cohort study. Developmental Medicine and Child Neurology, 61(6), 689–696. https://doi.org/10.1111/dmcn.13993