


References
- Takai K, Nikkuni K, Shibuya H, et al. Thrombocytopenia with mild bone marrow fibrosis accompanied by fever, pleural effusion, ascites and hepatosplenome-galy. Rinsho ketsueki 2010;51(5):320–5.
- Igawa T, Sato Y. TAFRO Syndrome. Hematol Oncol Clin North Am. 2018 Feb;32(1):107–118. Doi: 10.1016/j.hoc.2017.09.009. PMID: 29157612.
- Castleman B, Iverson L, Menendez VP. Localized mediastinal lymph node hyper-plasia resembling thymoma. Cancer 1956;9(4):822–30.
- Frizzera G, Peterson BA, Bayrd ED, et al. A systemic lymphoproliferative disorder with morphologic features of Castleman’s disease: clinical findings and linic- pathologic correlations in 15 patients. J Clin Oncol 1985;3(9):1202–16.
- Fajgenbaum DC, Uldrick TS, Bagg A, et al. International, evidence-based consensus diagnostic criteria for HHV-8-negative/idiopathic multicentric Castle-man disease. Blood 2017;129(12):1646–57.
- Fujimoto S, Sakai T, Kawabata H, Kurose N, Yamada S, Takai K, Aoki S, Kuroda J, Ide M, Setoguchi K, Tsukamoto N, Iwao-Kawanami H, Kawanami T, Mizuta S, Fukushima T, Masaki Y. Is TAFRO syndrome a subtype of idiopathic multicentric Castleman disease? Am J Hematol. 2019 Sep;94(9):975–983. Doi: 10.1002/ajh.25554. Epub 21 June 2019. PMID: 31222819.
- Thorne I, Sutcliffe N. Sjögren’s syndrome. Br J Hosp Med (Lond). 2 Aug 2017;78(8):438–442. Doi: 10.12968/hmed.2017.78.8.438. PMID: 28783408.
- Grange L, Chalayer E, Boutboul D, Paul S, Galicier L, Gramont B, Killian M. TAFRO syndrome: A severe manifestation of Sjogren’s syndrome? A systematic review. Autoimmun Rev. 2022 Aug;21(8):103137. Doi: 10.1016/j.autrev.2022.103137. Epub 6 July 2022. PMID: 35,803,499.
- Masaki Y, Kawabata H, Takai K, Tsukamoto N, Fujimoto S, Ishigaki Y, Kurose N, Miura K, Nakamura S, Aoki S; Japanese TAFRO Syndrome Research Team. 2019 Updated diagnostic criteria and disease severity classification for TAFRO syndrome. Int J Hematol. 2020 Jan;111(1):155–158. Doi: 10.1007/s12185-019-02780-1. Epub 28 Nov 2019. PMID: 31782045.
- Brito-Zerón P, Baldini C, Bootsma H, Bowman SJ, Jonsson R, Mariette X, Sivils K, Theander E, Tzioufas A, Ramos-Casals M. Sjögren syndrome. Nat Rev Dis Primers. 7 Jul 2016;2:16047. Doi: 10.1038/nrdp.2016.47. PMID: 27383445.
- Yamaguchi Y, Maeda Y, Shibahara T, Nameki S, Nakabayashi A, Komuta K, Mizuno Y, Yagita M, Manabe Y, Morita T, Nishide M, Watanabe A, Takamatsu H, Nishida S, Hirano T, Shima Y, Narazaki M, Kumanogoh A. Recovery from prolonged thrombocytopenia in patients with TAFRO syndrome: case series and literature review. Mod Rheumatol Case Rep. 2020 Jul;4(2):302–309. Doi: 10.1080/24725625.2020.1717747. Epub 3 Feb 2020. PMID: 33087016
Oral Communication
Abstract ID: 5
Chronic reactive arthritis after Neisseria gonorrhoeae infection
Thibault Maerten, Lucie Pothen
Cliniques Universitaires Saint-Luc, Brussels, Belgium
Abstract
Introduction:
Reactive arthritis is a member of the spondyloarthropathy family, presenting as an oligoarthritis mainly affecting the lower limbs after a digestive or genitourinary infection. Extra-articular manifestations are possible (notably the eyes and the skin) and there is an association with HLA B27 which can be found in 50% to 80% of the patients.
Case report:
A 31 years old patient of Romanian origin presented at the emergency room in April 2022 for 48 hours of severe pain in the left buttock region. He described nocturnal recrudescence of the pain and morning stiffness. He also reported mictalgia a week before.
Clinical examination revealed left sacroiliac pain, bilateral conjunctivitis, and circular balanitis.
The patient confirmed recent unprotected sexual intercourse.
Biological tests showed a significant inflammatory syndrome (CRP 100 mg/L) and urinalysis aseptic leukocyturia (2383 GB/µL).
PCR on fresh morning urine was positive for Neisseria gonorrhoeae and negative for Chlamydia trachomatis. Serological tests for other sexually transmitted infections were negative (HIV, HCV, syphilis) and he had vaccine immunity against hepatitis B.
The diagnosis of oculo-urethro-synovial syndrome (formely named Reiter) was retained. The patient was treated with ceftriaxone 2 g once and received NSAIDs for the arthritis. He was discharged from the hospital after a few days.
He was followed in consultation two weeks later. Balanitis and conjunctivitis were resolved and the PCR control on urine for Neisseria gonorrhoeae was negative. However, he still complained about a left sacroiliitis. On physical examination, dactylitis on the left second toe and arthritis of the right tarsus were also appearing. A significant biological inflammatory syndrome persisted (CRP 153 mg/L) accompanied by anemia and a reactive thrombocytosis.
Ultrasound confirmed flexor tenosynovitis of second ray of the left feet and joint swelling in the right tarsus. An attempt at joint puncture failed, probably due to too little intra-articular fluid.
An MRI of the pelvis showed left sacroiliitis. Blood cultures remained sterile. A transthoracic cardiac echocardiogram did not reveal endocarditis or valvular pathology. The ophthalmologic examination was normal.
Because of the suspicion of disseminated gonococcal infection, a 4-week course of ceftriaxone 2 g once a day was decided, while increasing the analgesic treatment (opioids) and continuing the NSAIDs. Unfortunately, there was no improvement of symptoms and inflammatory syndrome. On the contrary, new sites of arthritis appeared on the left hand and knee. The HLA B27 test came back positive. Finally, corticosteroids (maximum dose of 32 mg of methylprednisolone per day and progressively tappered) accompanied by salazopyrine (up to 1000 mg 3 times a day) were started with dramatic improvement of symptoms and inflammatory syndrome.
Conclusion:
Reactive arthritis remains a rare condition (3.5–5/100 000/year). Diagnosis and efficient treatment can be challenging, especially in cases of chronic form or NSAID resistance maintained by carrying the HLA B27.
Oral Communication
Abstract ID: 35
Long-term Protection Against Herpes Zoster (HZ) by the Adjuvanted Recombinant Zoster Vaccine (RZV): Interim Efficacy, Immuno and Safety Results at Approximately 10 Years after Initial Vaccination
Ana Strezovaa, Javier Diez-Domingob, Kamal Al Shawafic, Juan Carlos Tinocod, Meng Shie, Paola Pirrottaf, Angnes Mwakingwe-Omarig, Florence Strubbeh
aGSK, Rixensart, Belgium. bFISABIO Fundación para el Fomento Investigación Sanitaria y Biomédica de la Comunitat Valenciana, Valencia, Spain. cModis, Wavre, Belgium. dHospital General de Durango, Durango, Mexico. eGSK, Rockville, MD, USA. fGSK, Wavre, Belgium. gGSK, Rockville, MD, USA. hOn behalf of authors (GSK), Wavre, Belgium
Abstract
Background: We present data describing vaccine efficacy (VE), immunogenicity persistence and safety up to approximately 10 years after primary vaccination against HZ with RZV. We have previously shown that RZV demonstrated high VE against HZ in adults ≥50 years of age (YOA) participating in two phase 3 clinical trials (ZOE-50, NCT01165177 and ZOE-70, NCT01165229), and VE persisted up to year (Y) 2 in the interim analysis of the extension study (ZOSTER-049, NCT02723773). Here, we describe the interim analysis for Y4 of the extension study. Understanding the persistence of VE and long-term protection against HZ can help to optimize the use of RZV in adults ≥50 YOA.
Methods: Primary objective included VE against HZ over the ZOSTER-049 study. Secondary objectives included VE against HZ from 1 month post-dose 2 in the ZOE-50/-70 studies until the end of Y4 of ZOSTER-049 (Y10 after vaccination), persistence of vaccine-induced humoral immunogenicity (HI) in terms of anti-glycoprotein E (gE) antibody and cell-mediated immune (CMI) response in terms of frequency of gE-specific CD4[2+] T-cells and safety. VE analysis for ZOSTER-049 used historical control estimates from the ZOE-50/-70 placebo groups.
Results: In ZOSTER-049, 7,413 participants were enrolled and 7,277 were included in VE analysis. During 4 years of follow-up in ZOSTER-049, overall VE against HZ was 81.6% (95% confidence interval [CI]: 75.2–86.6). From 1 month post-dose 2 in ZOE-50/-70 until Y4 of ZOSTER-049, the overall VE was 89.0% (95% CI: 85.6–91.3). In ZOSTER-049, anti-gE antibody concentrations persisted >5 times above pre-vaccination up to Y10 after vaccination. The frequency of gE-specific CD4[2+] T-cells remained above pre-vaccination from Y6 to Y10 after vaccination (until the end of Y4 of ZOSTER-049). No safety signals were identified until the end of Y4 of ZOSTER-049.
Conclusion: Efficacy against HZ and immune responses to RZV remained high until the end of the observation period for this Y4 interim analysis suggesting that the clinical benefit of the RZV in adults ≥50 YOA is sustained for at least 10 years after vaccination. RZV safety profile remained clinically acceptable.
Funding: GlaxoSmithKline Biologicals SA (GSK Study identifier: 214093)
Oral Communication
Abstract ID: 25
Familial autoimmune thyrogastric syndrome: clinical, genetic and in vitro studies.
Hernan Valdes-Socina,b, Oriol Calvetec,d, Javier Benitezc, Edouard Louisa,b, Patrick Petrossiansa,b
aCHU de Liège, Liège, Belgium; bUniversité de Liège, Liège, Belgium; cSpanish National Cancer Research Center (CNIO), Madrid, Spain; dNetwork of Research on Rare Diseases (CIBERER), Madrid, Spain
Abstract
Introduction: Autoimmune thyrogastric syndrome (ATGS) is an autoimmune polyendocrinopathy type IIIB that associates autoimmune thyroiditis and chronic gastritis. We previously described eight families with ATGS (Acta Clin Belg 2015). Genetics and physiopathology of ATGS is currently unknown.
Patients and methods: We collected clinical and genetic data (lymphocyte DNA) from four Belgian families (10 females, mean age: 42 ± 11 years). All patients harbored autoimmune gastritis and autoimmune thyroiditis (Hashimoto or Graves disease). Five autoimmune thyrogastric syndrome patients (involving autoimmune gastritis or gNETs, and Graves’ or Hashimoto’s disease) were included in the first gene discovery series and initially studied by Whole Exome Sequencing (WES). WES uncovered different pathogenic variants in SLC4A2, SLC26A7 and SLC26A9, which cotransport together with ATP4A. Preliminary candidate genes found in this study were included in a custom 12 genes achlorhydria panel for targeted Next Generation sequencing (tNGS) studies. Belgian patients and 66 other familial and sporadic Spanish patients (not presented here) were studied with the custom panel. In addition, 40 healthy individuals were recruited as controls. In vitro studies were designed to test the pathogenicity of SLC26A7, SLC26A9 and SLC4A2 genes. Therefore, wild-type HEK293 and knock-out cell lines were cultured in an enriched and a restrictive medium. Moreover, a colony-forming assay and flow cytometry studies were designed to test ROS damage-mediated apoptosis.
Results: The WES study revealed new variants in the ATP4A (c.719C>A, p.Pro240His), SLC26A7 (c.643A>G, p.Ile215Val) and also in SLC26A9 genes (c.514 G > A, p.Val172Met and c.2546 G > A, p.Arg849Gln) in Belgian families. According to in silico analysis, these are possible/probably missense damaging mutations. ATP4A encodes for the gastric hydrogen potassium ATPase, responsible for the acidification of the stomach. SLC26A7 (thyroid and gastric cells) and SLCA4 (gastric cells) are epithelial Solute Carries that regulates chloride and bicarbonate transport. SLC26A9 is another Solute Carrier that regulates iodine, chloride and bicarbonate transport in thyroid cells. The inactivation of SLC26A7, SLC26A9 and SLC4A2 genes in HEK293T cells determined oxidative stress apoptosis (H2O2), suggesting a primary role for these genes in ROS control, cellular acid-base balance and the pathogenesis of ATGS. Previous studies from one of us demonstrated that human mutations in the gastric ATP4A proton pump triggered gastric achlorhydria, activating mucosal autoimmunity (Hum Mol Genet. 2015).
Discussion: The current clinical classification of autoimmune polyendocrinopathy does not assist the patient’s needs. We describe in a large international and collaborative study (Cell 2021 Dec; 10(12): 3500), a constellation of genes in the setting of familial and sporadic autoimmune polyendocrinopathy. These genes are involved in a novel pathogenic mechanism, based in the alteration of cellular acid-base balance and gastric aclhorhydria. Indeed, SLC26A7, SLC26A9 and ATP4A genes are strongly associated with thyroid and gastric disease, suggesting a hereditary autosomal genetic model for ATGS. Our data pave the way for the diagnosis and clinical management of patients with ATGS. Additional studies are needed to precise unsuspected renal and respiratory phenotypes in our patients, and to investigate the pathogenic consequences of gene variants herein described.
Oral Communication
Abstract ID: 61
Recreative drugs: new suspects in the HIV-associated neurocognitive disorders Cluedo game.
Sophie Henrard, MDa,b; Nicola Trottab,c,d PhD, Antonin Rovaib,d PhD; Tim Coolenb,e, MD; Hichem Slamaf, PhD; Julie Bertelsb,f PhD; Delphine Puttaertb PhD; Jean-Christophe Goffarda, MD PhD, Jean-Paul Van Voorena, MD PhD, Serge Goldmanb,c, MD PhD; Xavier De Tiège, MD PhDb,d
aUniversité libre de Bruxelles (ULB), Hôpital Universitaire de Bruxelles (H.U.B.), CUB Hôpital Erasme, Department of Internal Medicine and immunodeficiency, Brussels, Belgium; bLaboratoire de Neuroanatomie et de Neuroimagerie translationnelles (LN2T), UNI – ULB Neuroscience Institute, Université libre de Bruxelles (ULB), Brussels, Belgium; cUniversité libre de Bruxelles (ULB), Hôpital Universitaire de Bruxelles (H.U.B.), CUB Hôpital Erasme, Department of Nuclear Medicine, Brussels, Belgium; dUniversité libre de Bruxelles (ULB), Hôpital Universitaire de Bruxelles (H.U.B.), CUB Hôpital Erasme, Department of translational Neuroimaging, Brussels, Belgium; fUniversité libre de Bruxelles (ULB), Hôpital Universitaire de Bruxelles (H.U.B.), CUB Hôpital Erasme, Department of Radiology, Brussels, Belgium; gUniversité libre de Bruxelles (ULB), Hôpital Universitaire de Bruxelles (H.U.B.), CUB Hôpital Erasme, Department of Clinical Neuropsychology, Brussels, Belgium; fUlBabyLab-Consciousness, Cognition and Computation Group, Center for Research in Cognition and Neurosciences, ULB Neuroscience Institute, Université libre de Bruxelles (ULB), Brussels, Belgium
Abstract
Background Despite the high prevalence of HIV associated neurocognitive disorder (HAND), its pathogenesis remains unclear and efficient diagnostic tools are lacking. This study characterizes the structural and metabolic cerebral correlates of HAND in a preclinical setting that considers the lifestyle of young European men exposed to HIV.
Methods Structural brain magnetic resonance imaging (MRI) and positron emission tomography with [18 F]-fluorodeoxyglucose (FDG-PET) were prospectively acquired simultaneously on a hybrid PET-MR in 23 asymptomatic HIV+ men (mean age: 33.6 years) with a normal CD4+ cell count and undetectable viral load; 26 HIV- men, highly well matched for what concerns lifestyle and age, pre-exposure prophylaxis users (HIV-PrEP), and in 23 undifferentiated young men healthy controls (HC). FDG-PET data were analyzed using a voxel-based approach. Structural MRI data were analyzed using atlas-based brain parcellisation. A comprehensive neuropsychological assessment was also administered to the HIV+ and HIV-PrEP groups.
Results Both HIV+ and HIV-PrEP subjects exhibited asymptomatic neurocognitive impairment based on Frascati criteria. HIV+ had lower performances in executive functions, attentional and working memory functions compared to HIV-PrEP. No brain structural or metabolic differences were found between those two groups. Compared to HC, HIV+ and HIV-PrEP displayed a common frontal hypometabolism in the right dorsolateral and dorso-mesial prefrontal cortex that correlated to the level of recreational drug use but not with the level of dysexecutive deficits.
Conclusion This study disclosed the existence of a dysexecutive syndrome and prefrontal hypometabolism in HIV+ in absence of brain atrophy. Prefrontal hypometabolism was similar to that observed in HIV-PrEP and was related to the use of recreational drug use. Our results support the need for a dynamic prevention of recreative drug use in those populations to cope with their negative impact on brain function and their neurocognitive consequences. A complex interplay between recreative drugs and HIV is involved in the induction and development of HAND in young HIV+ men.
Oral Communication
Abstract ID: 50
Exploring the oligogenic aspects of common variable immunodeficiencies using ORVAL
Marie Nabout, Jean-Christophe Goffard, Isabelle Vandernoot, Sofia Papadimitriou, Youssef Bouysran, Sophie Henrard
ULB Erasme, Anderlecht, Belgium
Abstract
Introduction
Common variable immunodeficiency (CVID), the most common primary humoral immunodeficiency, is a heterogeneous disease with various clinical presentations. Currently, less than 20% of cases of CVID have a known genetic cause, considered as monogenic but not following a mendelian inheritance pattern in most of the cases. More complex genetic scenarios like oligogenic inheritance must be considered. ORVAL, Oligogenic Resource for Variant AnaLysis, is a novel bioinformatics platform designed for the prediction and exploration of candidate disease-causing oligogenic variant combinations. In this study, we aim to unravel networks of candidate pathogenic variant combinations in a cohort of CVID patients.
Materials and Methods
This retrospective study included 35 CVID patients followed up at ULB Erasme Hospital, for whom clinical exome sequencing did not disclose a monogenic cause. Each subject’s clinical exome data, as well as those of a control cohort of 1536 patients, were analysed through ORVAL focusing on 479 genes associated with immune disorders. Combinations found in at least 2 CVID patients, not found in any patient in the control cohort, were then selected as potential candidate pathogenic variant combinations.
Results
The number of variant combinations predicted to be pathogenic was statistically significantly higher among CVID patients compared to controls. In addition, three unrelated couples of patients shared combinations considered as probably pathogenic involving the same gene pair, and none of these combinations were found in the control cohort. These associations involve among others PLCG2, STXBP2 and IL17C genes. Nevertheless, we found clinical similarities in each couple of patients with the same candidate disease-cause associations, as well as similarities into their circulating B cell phenotype.
Conclusion
ORVAL platform seems to be a promising tool to address the oligogenic nature of CVID. Our results need to be replicated in an independent cohort of cases and controls. Furthermore, the real impact of these variant combinations at a molecular level should be then confirmed through functional tests.
Oral Communication
Abstract ID: 3
Diagnostic yield of 18 F-FDG PET in fever versus inflammation of unknown origin
Albrecht Betrainsa, Lennert Boeckxstaensa, Lien Moreela, William Wrightb, Koen Van Laerea, Daniel Blockmansa, Steven Vanderschuerena
aUZ Leuven, Leuven, Belgium; bJohns Hopkins University Hospitals, Baltimore, USA
Abstract
Background Fever of unknown origin (FUO) and inflammation of unknown origin (IUO) are clinical syndromes that share a similar diagnostic spectrum. 18 F-fluorodeoxyglucose positron emission tomography (PET) is an important imaging technique in the diagnostic workup of FUO/IUO. Several studies have investigated the value of PET in FUO and IUO patients, but studies which compare the diagnostic yield of PET imaging between both syndromes are lacking.
Methods Retrospective analysis of adults evaluated for FUO or IUO who underwent PET in our center between 1 January 2000 and 31 December 2019. PET images were rescored and assessed for accuracy and contribution towards the final diagnosis. Logistic regression analyses were performed to evaluate the association of meeting either the FUO or IUO criteria and outcomes of interest with adjustment for combined PET/CT imaging, prior antibiotics or immunosuppressive treatment, and the presence of fever or inflammation at the time of PET imaging.
Results Out of 604 patients, 439 (mean age 56 years, 43% female) underwent PET imaging, including 349 (79%) classified as FUO and 90 (21%) as IUO. IUO patients had a longer time to PET (12 versus 7 days; P = 0.02), more frequent combined PET/CT imaging (52% versus 40%; P = 0.05), and less frequent antibiotics prior to PET (11% versus 29%; P < 0.001). Out of all patients, 51 (12%) had infection, 66 (15%) had malignancy, 119 (27%) had NIID, 46 (10%) had miscellaneous conditions, and 157 (36%) remained undiagnosed. Overall, PET imaging had a sensitivity of 93% (95% confidence interval 89–96%) and a specificity of 34% (28–41%). PET imaging was considered contributive towards the final diagnosis in 25% (21–29%) of cases. Patients with IUO were significantly more likely to have a contributive PET scan compared to those with FUO (IUO 40% versus FUO 21%; aOR 2.68 [1.62–4.40]; P = <0.001). PET was contributive by directly indicating the diagnosis in 25 (23%) and indirectly in 84 (77%) patients by further tissue biopsy (n = 66; 61%), invasive imaging with/without biopsy (n = 6; 5%) serological testing (n = 6; 5%), joint aspiration (n = 5; 5%), and genetic testing (n = 1; 1%). IUO patients more frequently had a direct PET diagnosis compared to those with FUO (IUO 39% versus FUO 15%; aOR 3.80 [1.44–10.4]; P = 0.008).
Conclusion While PET is an excellent diagnostic tool in both FUO and IUO, PET was more frequently contributive and more often directly indicated the final diagnosis among IUO patients.
Poster communications
Abstract ID: 2
Life-threatening hypokaliemia occurring in a patient with adult-onset Still’s disease
Pierre Rossignona, Benoit Rennebooga, Alain Souparta,b
aDepartment of Internal Medicine, Moliere-Longchamp Hospital, Brussels, Belgium; bResearch Unit for the Study of Hydromineral Metabolism, Department of Internal Medicine, Erasmus University Hospital, ULB, Brussels, Belgium
Abstract
Background: Adult-onset Still’s disease (AOSD) is a rare genetic autoinflammatory disease finding its roots in what is nowadays called a cytokine storm : a dysregulation of inflammation leading to an excessive production of well identified cytokines. It most often comes out as fever, polyarthritis and arthralgia, transient erythema, pharyngitis, with inconsistent biological signs; this set can be partial. Acute intestinal pseudo-obstruction denotes an intestinal obstruction occuring in the absence of an anatomic or mechanical cause, with multiple identified etiologies.
Case description: We describe the case of a 62-year-old male who presents himself with signs and symptoms of a mechanical intestinal obstruction, showing severe abdominal distension and watery diarrhea (10–15 stools/day); nausea, vomiting; and high spiking fever >39°C lasting for 3 weeks.
After thorough interrogation, the patient exposes a 1-month history of polyarthralgias, symmetric (shoulders, wrists, metacarpo-phalangial, interphalangeal, and knee articulations). Furthermore, fever is noted to be of vesperal occurrence, and a clinician spotted the emergence of a non pruritic, salmon-colored rash on the patient’s torso. Laboratory data show life-threatening hypokaliemia of 1.7 mEq/L [normal 3.5–4.5 mEq/L] with low kaliuresis (FEK 7%), high white blood cell count (of which 88% were neutrophils) with a CRP level of 207 mcg/L. Antinuclear antibody (ANA) and rheumatoid factors (RF) were negative; ferritin level was high at 810 [normal 20–250 µg/L] while glycosylated ferritin level was low.
At the same time, an abdominal CT shows a small bowel and colonic distension, without anatomic or mechanical cause of obstruction. These findings define an acute intestinal pseudo-obstruction, which have led to the symptoms of watery diarrhea, ultimately leading to severe hypokaliemia.
These findings, alongside with complementary exams to rule out alternative diagnostics, strongly supported the diagnostic of AOSD (whether we use the most recent clinical scale of Crispin et al., or the most used Yamaguchi criteria).
To struggle against stool losses of potassium, the patient needed high intravenous potassium supplementation, up to 440 mEq/day. He furthermore was treated with octreotide, showing no probent effect, before the introduction of corticosteroids. This treatment (methylprednisolone 1 mg/kg/d.) led to a rapid diminution of stool volume and abdominal signs, and hence to progressive correction of the hypokaliemia, but also to an interruption of fever spikes. Methotrexate was then introduced to contend arthritis symptoms.
Progresses were made in the last years, in understanding the AOSD pathogenesis: a dysregulation of inflammation leading to a dysregulation of inflammation leading to a cytokine storm. Dominant cytokines patterns can lead to different clinical phenotypes, ranging from important systemic features to predominant articular involvement.
Conclusion: We described the unusual case of an AOSD presenting with intestinal pseudo-obstruction; this is only the fifth reported case of such a presentation, and the first one presenting with life-threatening hypokaliemia.
Abstract ID: 4
A lymph node in the adrenal
Yassin Akachar, Etienne Delgrange
Université Catholique de Louvain, Bruxelles, Belgium
Abstract
A 53-year-old smoking female patient treated with nebivolol and aldactone for hypertension and with l-thyroxine for a multinodular goiter, without clinical history of acute or chronic infection or lymphoproliferative disorder presented to the outpatient clinic for an adrenal incidentaloma. Known for nephrolithiasis, renal cysts, cervical cancer cured, and polycystic ovary syndrome, she had an injected abdominal MRI for back pain that revealed a left adrenal lesion of 16 mm not present on a computed tomography (CT) six years before, not hyperintense in T2 and without signal drop in T1 out, and with a pathological contrast enhancement. The patient complained of occasional palpitations, hot flashes without real sweating and without fever, dizziness, and loss of appetite. Physical examination revealed moderate weight loss and the presence of centimetric cervical nodes. CRP and LDH levels were normal. A CT scan and a whole-body fluoro-deoxyglucose PET-CT were performed two months after and the nodule was 15x20mm with an average spontaneous density at 43 Hounsfield units and was hypermetabolic (SUV at 7.2). The right adrenal just had a hyperplastic appearance already present six years before and was not hypermetabolic. No other significant lesion was identified. Urinary catecholamines were normal. The 1 mg dexamethasone suppression test was normal with a cortisol of 8 am of 1 µg/dl (<1,8 µg/dl), the ACTH level was also normal (6.24 pg/ml,5–49). The aldosterone/renin ratio (one month after stopping aldactone but under nebivolol) was high: aldosterone was 212 pg/ml (35–300), and renin was 1 pg/ml (3–33) but renin could be reduced by nebivolol. The DHEAS level was normal. After discussion with the patient about the risk-benefit balance of the various therapeutic options, and considering the patient’s desire for a radical treatment, left adrenalectomy was performed. The pathological analysis will reveal in the adrenal medulla a normal lymph node with polarized architecture with germinal center and marginal zone consisting of mature B and T lymphocytes (expressing CD20 and CD3) without other abnormalities. Tissue architecture and normal cortico-medullary differentiation of the adrenal were preserved. The normal histology of the adrenal medulla includes just small perivascular accumulations of lymphocytes and/or plasma cells. Finding a lymph node in the adrenal medulla is extremely rare and has just been described in the literature to our knowledge in one case (Victor E. Nava, Endocrine pathology 2013). This case illustrates that a normal lymph node may have suspicious radiological features and constitutes a rare cause of adrenal incidentaloma.
Abstract ID: 6
The surveillance for hepatocellular carcinoma, it’s fine. To diagnose the cirrhosis, it’s better.
Maxence Lepoura,b, Christophe de Terwangneb, Jean Henriona, Olivier S. Descampsa, Marie de Vosa
aHôpital de Jolimont, La Louvière, Belgium; bUCLouvain, Brussels, Belgium
Abstract
Background
Hepatocellular carcinoma (HCC) is the sixth most common cancer and the third cause of cancer death. Cirrhosis is a major risk factor for HCC in the Western world. International recommendations suggest screening cirrhotic patients twice a year for HCC. This surveillance is associated with early tumor detection, possibility of curative treatment and aims to improve survival. In real life, fewer than one-third of cirrhotic patients undergo screening for HCC in western countries and many patients do not enter into surveillance programs due to undiagnosed cirrhosis. Therefore, the efficacy of this surveillance on mortality is debated.
Aims
We first aimed to assess the quality of surveillance in patients diagnosed with HCC in a background of cirrhosis.
We secondly assessed the efficiency of this surveillance in terms of prognosis of HCC (earlier stage of cancer extension and accessibility to curative treatment).
Methods
In this retrospective single center study, we identified patients with HCC from January 2017 to December 2021 by reviewing reports of multidisciplinary digestive-oncology consultations. We excluded patients without cirrhosis, recurrent diagnosis of HCC and mixed tumors.
We classified the surveillance before the diagnosis of HCC as 3 groups: A) recommended surveillance (patients with known cirrhosis and at least one imaging during the year before diagnosis), B) inconsistent surveillance (patients with known cirrhosis but no imaging during the year before diagnosis) and C) concomitant diagnosis of cirrhosis and HCC. HCC extension (based on the Barcelona Clinic Liver Cancer [BCLC] score) and initial treatment provided were reviewed and compared between group A and groups B + C.
Results
One hundred thirty-six patients were identified with a diagnosis of HCC. We excluded 25 non-cirrhotic patients, 15 recurrences, 3 unclear diagnoses. On the 95 selected patients, 36 (38%) had a recommended surveillance (group A), 17 (18%) had an inconsistent surveillance (group B) and 42 (44%) had a concomitant diagnosis of cirrhosis and HCC (group C).
From the 53 patients with known cirrhosis, 36 (68%) were correctly screened whereas 17 patients did not follow the surveillance program. In this last group, 15 (88%) of them were clearly informed about the utility of the surveillance for HCC.
In group A, 29 patients (80%) had an early-stage disease (BCLC stage 0 or A) and 24 (67%) were eligible for curative treatment (surgery or thermo-ablation). Amongst the patients not correctly screened (from groups B + C), only 18 (30%) had an early-stage disease and 13 (23%) were eligible for a curative treatment.
Conclusion
Amongst the patients with HCC on cirrhosis, almost half of them were diagnosed for the HCC concomitantly with their cirrhosis. For the other patients, with previously known cirrhosis, two-third were correctly followed-up according to current recommendations.
Regular surveillance in cirrhotic patients was associated with an earlier stage diagnosis of HCC and a better access to curative treatment.
We underline the importance to diagnose the pre-existing cirrhosis to implement a correct surveillance program for HCC. Tools like APRI, Fib4-score and fibroscan may help to screen high-risk groups for chronic liver disease in primary care.
Abstract ID: 7
Long-term safety and effectiveness of Alirocumab and Evolocumab in Familial Hypercholesterolemia (FH) in Belgium
Marc Snela, Olivier Descampsb
aPole Hospitalier Jolimont, La Louvière, Belgium; b[email protected], La Louvière, Belgium
Abstract
Background.
Familial Hypercholesterolemia (FH) is an autosomal dominant disease with a prevalence of 1/400. It is caused by a defect in LDL-cholesterol clearance. This results in blood LDL-C levels over twice the usual levels from birth, leading to premature cardiovascular disease (CVD).
Since 2015, monoclonal antibodies against PCSK9 (‘Anti-PCSK9 mAb’, Evolocumab and Alirocumab) which triggers lysosomial destruction of LDL receptor is covered by the national insurance in Belgium under the following conditions: patients with FH (defined by a DLCN score >8) who still have excessive LDL-C values despite treatment of high-intensity statin combined with ezetimibe (LDL-C > 100 mg/dL for patients with a history of cardiovascular disease (CVD), or >130 mg/dL for all other patients)
Our objective is to characterize the patients receiving this new therapy and assess its real-life efficacy.
Methods.
We sourced patients from the EAS Familial Hypercholesterolemia Studies Collaboration (FHSC) database, an international database on FH including 1091 Belgian patients. We selected patients taking anti-PCSK9-mAb treatment followed up at our Lipid Clinic. Patients were divided into three groups following the reimbursement criteria of the National Insurance: a) history of Acute Coronary Syndrome and LDL-C > 100 mg/dL, b) other CVD and LDL-C > 100 mg/dL, c) no CVD history and LDL-C > 130 mg/dL.
Table
Results.
Amongst our 239 FH subjects (56 ± 12 years) receiving anti-PCSK9 mAb (), 25% had a history of acute coronary syndrome, 32% had another CVD history and 43% were on primary prevention. When present, ACS or CVD event occurred early in life. Overall, 85% were at very-high risk of CVD based on the classification of the EAS (history of CVD or multiple risk factors in primary prevention). Despite intense classical therapy, LDL-C were still high (average above 150 mg/dL). Under anti-PCSK9 mAb treatment, LDL-C reduction was above 50% and achieved LDL-C was around 100 mg/dL on average after 1 year of treatment. The patients with ACS had the highest target achievement rates. LDL-C reduction and LDL-C target achievement were lower in patients without statin (). During the follow-up (mean 3,0 ± 1,8 years), 4 patients died (2 CVD, 1 trauma, 1 unknown cause), 4 reported skin rash, 7 had limb pain and one had a new onset of multiple sclerosis. Only 6 patients stopped the anti-PCSK9 mAb due to adverse effects or insurance problem.
Conclusions
Anti-PCSK9-mAb significantly lowered LDL-C and allowed a significant number of patients to reach their lipid targets. The amplitude of LDL-C reduction and the safety profile observed in real life were similar to those from randomized controlled trials. Despite the low LDL-C levels achieved, 50% patients never reached their respective LDL-C targets even once, because the severe phenotype and the very high cardiovascular risk of most of our patients as well as the very stringent LDL-C target (≤55 mg/dL). With the advent of new lipid lowering treatments such as and bempedoïc acid, we can hope for a greater proportion of FH patients to reach their LDL-C targets.
Abstract ID: 8
How the new ESC cardiovascular risk chart, SCORE2, identifies additional high risk patients in a population free of cardiovascular disease with large waist circumference.
Sarah Douharda, Marc Snela, Luc Van Gaalb, Christian Brohetc, André Scheend, Fabian Demeuree, Olivier S. Descampsa
aPôle Hospitalier Jolimont, La Louvière, Belgium; bUAntwerp, Antwerp, Belgium; cUCLouvain, Bruxelles, Belgium; dULiège, Liège, Belgium; eCHU UCL Namur, Namur, Belgium
Abstract
Background
In terms of estimating atherosclerotic cardiovascular disease (ASCVD) risk for primary prevention in Belgium, the European Society of Cardiology (ESC) 2003 guidelines recommended to use the SCORE chart. This was first adapted in 2012 with the weighting of HDL-cholesterol (HDL-C). As recent epidemiological data faced a shift from fatal towards non-fatal ASCD events, in 2021, an update provided a risk estimate combining these two outcomes: the low-risk country SCORE2 and SCORE2-OP (Older Persons). These new charts sort the population into three risk categories, low/moderate, high and very high, with classification cut-offs depending on age, and consider non-HDL-C instead of total cholesterol. Abdominal obesity is both a hint and an alert for greater ASCVD risk. Therefore, we wished to examine how SCORE2 modifies the estimated risk in patients with abdominal obesity.
Methods
In 2004, a Belgian project called ‘BEST study’ aimed to estimate ASCVD risk amongst this population, asked 619 general practitioners to select successive patients aged from 40 to 75 years old, who had increased waist circumference (≥80 cm in women, ≥94 cm in men) and no history of ASCVD. From this cohort (N = 9593), we excluded patients with diabetes and lipid-lowering treatment. The risk categorization was initially performed using the 2012 SCORE-HDL-C and presently with the 2021 low-risk country SCORE2.
Results
Our population consisted of 2720 women (47%) and 3053 men (53%). The distribution of ASCVD classic risk factors and metabolic syndrome is shown in . Compared to the 2012 SCORE-HDL-C, SCORE2 demonstrated a greater proportion of patients in the high and very high risk categories: 27% of the 2177 women and 48% of 1747 men with low/moderate risk shifted to high risk category (). This was due to SCORE2ʹs reclassification based upon age cut-offs. But when limiting analysis to 50–69 years old patients, which accounted for majority of 1782 women and 1894 men, and where risk cut-offs are similar for both charts, numbers were even higher: 36% of the 1496 women and 70% of 888 men in the low/moderate risk shifted to the high risk category. In contrast, none of the men and only three women shifted from high to low/moderate risk. Examining phenotype of these 50–69 years old ‘upward shifter’ patients, prevalence of age, smoking, hypertension, as well as measurement of blood pressure and lipid profile, was greater in those who were reclassified compared to those remaining in the same low/moderate risk. In contrast, there was no difference in body mass index, waist circumference, blood glucose, HDL-C (in men) and triglycerides (in women).
Conclusion
In patients with increased waist circumference, the low-risk country SCORE2 recommended for Belgium identifies a high proportion of patients shifting from the low/moderate ASCVD risk to the high risk category. The most susceptible ‘upward shifter’ patients are, as expected, those owning the greatest classical risk factors, but, surprisingly, not those owning risk factors associated with metabolic syndrome (apart from high blood pressure). Therefore, it is important to re-estimate the cardiovascular risk in most patients.
Table
Abstract ID: 9
Hydralazine hydrochloride-induced p-ANCA vasculitis: a case report
Nicolas Bradta, Laura Bolléa, Elien Mahieub, Anne-Marie Bogaerta
aAZ Sint-Elisabeth, Zottegem, Belgium; bAZ Glorieux, Ronse, Belgium
Abstract
Introduction: Hydralazine hydrochloride remains a widely used therapy for essential hypertension, despite demonstrating no effect on hard cardiovascular endpoints and exhibiting a wide range of side effects. One such side effect is drug-induced vasculitis and lupus-like syndrome.
Case presentation: We present a case of an 81-year-old woman with a history of arterial hypertension and taking Hydralazine hydrochloride who presented with a complaint of general malaise, emaciation and episodes of fever. Biochemically, a positivity test of anti-dsDNA and p-ANCA was seen. As the diagnosis of Hydralazine hydrochloride-induced p-ANCA vasculitis with a lupus-like syndrome was suspected, Hydralazine hydrochloride was discontinued and immunomodulatory medication was started with a clear clinical and biochemical improvement.
Discussion: Hydralazine hydrochloride-induced vasculitis is a rare side effect of this antihypertensive therapy. Due to the possibility of serious complications, the medication should be interrupted. Immunomodulating drugs can also be started in more serious cases.
Abstract ID: 10
Guidelines for the risk stratification of stable patients with pulmonary embolism: the reality of practice
Madeleine Scrivener, Olivier Descamps, Sophia Abdel Kafi
Jolimont, La Louvière, Belgium
Abstract
Background: Evidence-based guidelines are the best way to ensure the quality of patient care. The 2019 European Society of Cardiology (ESC) guidelines were established for the diagnosis and management of acute pulmonary embolism.
Objective: To evaluate the adherence of clinicians to the ESC recommendations in the management of hemodynamically stable patients with pulmonary embolism. To evaluate the identification and orientation of patients at intermediate-high risk of mortality according to the guidelines (sPESI>1 and right ventricle dysfunction and positive troponin test).
Material and Methods: We conducted a retrospective single-centre study on all the patients admitted into the emergency care unit (ECU) and diagnosed for pulmonary embolism from January 2021 to October 2021. Their data were collected from the patient health records of the ECU and the subsequent services where the patients were hospitalized. Hemodynamically unstable patients were excluded (Systolic blood pressure on arrival <90 mmHg, cardiac arrest or use of vasopressors). We evaluated the frequency of use of the recommended tools (PESI or sPESI) as well as the frequency of assessment of right ventricle dysfunction via imaging methods (heart ultrasound or via CT) and of laboratory biomarkers such as Troponin T (cutoff 10 pg/ml) and NT-proBNPs (cutoff 500 ng/L). For all of the selected patients, we retrospectively calculated the sPESI to assign them into three categories of early mortality risk (low, intermediate low and intermediate high) and examined whether the orientations of the patients to the intensive care unit (ICU) or other units were appropriate.
Results: A total of 70 patients with a median age of 64 years were included. Sixteen (23%) patients were SARS-CoV2 positive. Out of the 70 patients,15 (21%) had a documented PESI or sPESI score on arrival, 51 (73%) had a troponin measured and 51 (73%) had a cardiac ultrasound performed of whom 9 (13%) had an ultrasound on arrival and 42 (60%) during their hospital stay. After calculating the sPESI on all patients based on the admission data in the ECU,16 (23%) patients were identified as being at intermediate-high risk. Amongst these 16 severely affected patients,10 had indeed benefitted from surveillance in the ICU whereas one did not benefit from surveillance and five were not transferred to the ICU based on the clinician’s evaluation or the patient’s desire to avoid therapeutic escalation. It appears that sPESI was more frequently calculated (33% vs 4%, p = 0,002) in patients who had certain radiological findings (bilateral embolism or embolism in a main pulmonary artery) compared to patients without radiological signs of severity.
Conclusion: Adherence to the scores recommended by evidence-based guidelines was documented in only 23% of cases. This leaves room for improvement in the use of the PESI score and requires more systematic dosage of Troponins T and faster access to cardiac ultrasound. Our observation showed that even if radiological findings (besides signs of RV dysfunction) are not used in the ESC guidelines, some clinicians are prone to using radiological signs of severity to guide their use of the sPESI score. However, this can lead to a lack of identification and appropriate management of patients at intermediate-high risk of early mortality.
Abstract ID: 11
Stage II colorectal cancer (CRC): does side matter? The role of biomarkers in the prognostic effect of the primary tumor location in stage II colorectal tumors
Brecht Mullebroucka, Jules Colebundersa, Vincent Liégeoisa, Katleen Janssensa,b, Marc Peetersc,a, Nancy Van Dammed, Greetje Vanhouttee
aUniversity of Antwerp, Antwerp, Belgium. bDepartment of Genetics of University Hospital of Antwerp, Antwerp, Belgium; cDepartment of Oncology of University Hospital of Antwerp, Antwerp, Belgium; dBelgian Cancer Registry, Brussels, Belgium; eUniversity Hospital of Antwerp, Antwerp, Belgium
Abstract
Introduction:
Colorectal cancer (CRC) is the second most common tumor in women and the third in men. Treatment of stage II CRC begins with resection of the primary tumor, possibly followed by chemotherapy. The prognosis varies among stage II patients. Some have a higher risk of recurrence than others, and therefore have more relative benefit of adjuvant chemotherapy. This has indicated a need for further stratification of stage II CRC in different risk groups to determine which patients benefit from adjuvant chemotherapy. Hence the need for new biomarkers to further elucidate the prognosis in patients with stage II CRC. One such proposed biomarker is the sidedness (right-sided vs left-sided) of the primary tumor.
Materials and methods:
The study design was an observational study based on a retrospective cohort from data of the Belgian Cancer Registry (BCR). The aim was to collect data on primary tumor location, demographics, stage molecular biomarkers (BRAF or KRAS mutation, …) and survival. We investigated the difference in overall survival in right- vs left-sided stage II CRC patients. Next, we looked into the underlying molecular biomarkers and demographics to see if there could be a confounding effect of these mutations on the prognostic effect of the primary tumor location.
Results:
Pathology reports of all patients from the BCR diagnosed with stage II CRC in 2015–2016 were reviewed, being 3,278 in total. One thousand two hundred and eighty-two patients had a right-sided tumor, 1,351 had a left-sided tumor and 645 had a rectal tumor. 339/1,813 (18.7%) of patients had a tumor with microsatellite instability (MSI), 153/338 (45.3%) had a tumor with a KRAS mutation and 66/251 (26.3%) had a tumor with a BRAF mutation. In univariate analysis, patients with right-sided CRC stage II had a significantly worse overall survival when compared to left-sided stage II CRC patients (HR = 1.23; p-value = 0.0035). Other significant prognostic factors in univariate analysis were pathological T-stage and age. In multivariate analysis only gender, pathological T-stage and age were found to be significant prognostic factors for overall survival. Primary tumor location was not found to be significant in multivariate analysis. Molecular biomarkers (MMR-status, BRAF and KRAS) did not show a significant effect on the overall survival in both univariate and multivariate analyses.
Discussion:
In the literature, right-sidedness is an independent prognostic factor in stage III and stage IV CRC for a worse prognosis. In stage II the literature may indicate that it is the other way around. In our analysis of Belgian stage II CRC patients, right-sided stage II CRC had a worse prognosis in univariate analysis. However, the primary tumor location was not a significant risk factor in our multivariate analysis, indicating that the univariate effect of right-sidedness could be explained by the underlying patient demographics and pathologic T-stage.
Conclusion:
In stage II CRC, the primary tumor location does not seem to be an independent prognostic factor. Molecular biomarkers, such as MSI, BRAF-mutations and KRAS-mutations, had no impact on the prognosis of stage II CRC patients in both uni- and multivariate analysis.
Abstract ID: 12
Where do dialysis catheter infections come from?
Coline Jamez, Olivier S. Descamps, Pauline Biller
Jolimont, La Louvière, Belgium
Abstract
Background
Dialysis catheter is one of the two vascular accesses in patients on hemodialysis. The other one is arterio-venous fistula. One of the biggest differences between these two devices is that dialysis catheters are more likely to become infected than arterio-venous fistulas, which as complications, may lead to catheter-acquired septicaemia and mortality. Several risk factors for dialysis catheter infection are known in the literature. The aim of this study was to identify risk factors that increased catheter-acquired septicaemia in our hospital between 2020 and 2021.
Methods
We conducted a retrospective study including patients on hemodialysis with catheter for vascular access between January 1st, 2020 and 31 December 2021. In our hospital where 140 patients are currently on haemodialysis, 57% have a catheter for vascular access. We excluded patients with non-tunneled dialysis catheters. For patients who developed catheter-acquired septicemia, we studied a 30-day period prior to the first positive blood cultures. For patients who did not develop catheter-acquired septicemia, we studied a 30-day period before a date randomly determined.
Results
During the period of the study, we identified 14 patients (Gp 2) who developed a septicaemia. These patients were compared with the 73 patients without any infection during the same period (Gp 2). The two groups had similar age (69.3 ± 14.4 years vs 65.2 ± 14.4 years), sex distribution (57% vs 55% of males), prevalence of nephropathy (36% vs 25% of diabetic nephropathy) and other dialysis characteristics (months of dialysis and proportion of heparin lock). Between these two groups, we found no statistical difference regarding systemic risk factors of infections such as diabetes (50% vs 38%), MRSA carriage (0% vs 0%), presence of pacemaker, defibrillator or artificial heart valve (7% vs 19%) and immunosuppression (14% vs 21%) as well as no difference regarding local risk factors such as dressing alteration (0% vs 11%), increased manipulations (79% vs 67%), type of dressing and frequency with which the dressing is redone. The only statistically significant difference was the locations of the catheters in the two groups: considering only jugular and subclavian catheters, catheter-acquired septicaemia was more strongly associated (OR: 5.92; p < 0.001) with a left-sided catheter (32%) than with right-sided catheter (7%). The location of femoral catheters could not be statistically examined due to the very low number of patients with such location of catheter (N = 4).
Conclusion
Location of dialysis catheter, more specifically the left-sided location of the jugular and subclavian catheters, appears as one of the main risk factors for catheter-acquired septicaemia. In this study, it was not possible to find any association with other risk factors, suggesting that they are not as strong predictor of septicaemia
Abstract ID: 13
A new interrogation about the value of palliative care
Aurélie Struyfa, Olivier S. Descampsa, Isabelle Hermisseb, Michèle Pieterbourgb
aDepartment of Internal Medicine, Pôle Hospitalier Jolimont, Réseau HELORA, La Louvière, Belgium;bDepartment of Palliative Care, Pôle Hospitalier Jolimont, Réseau HELORA, La Louvière, Belgium.
Background
More and more studies are performed to assess the benefits of palliative care. A large number of tools to estimate quality of life at an individual scale already exist. But what about the assessment of the quality of life of a population? The Federal Center of Expertise of health care (KCE) just published a new tool to facilitate such evaluation: the Belgian valorisation of the EQ-5D-5 L. The advantage of this tool is that it can also give information at a national scale. Although this aspect may appear less important for health-care professionals, good data may motivate change in health policy. The aim of the present study is to assess in real life the feasibility of such tool in evaluating the benefit of our palliative care on the quality of life of our current patients.
Methods
In this prospective study, we selected patients who were followed by our palliative care team between February 1st, 2022 and April 30th, 2022. After informed consent, we asked them to respond to the questions of the EQ-5D-5 L survey at two moments during their follow-up. Our goal was to compare these two numbers. We also attempted to evaluate the reasons why some patients could eventually not answer the survey.
Results
One hundred and five patients were enrolled in our prospective study (50% males; age: 75,1 ± 11,2 years). These patients suffered of cancer (51%), various organ failures (32%; 8% with cardiac insufficiency and 8% kidney disease), infection (14%) for the most frequent causes (median time between start of the disease and the call for palliative team was 6,7 months). Overall, only 11% among these patients could really answer the EQ-5D-5 L questionary. The reasons why we were not able to assess their quality of life on a verbal way were multiple: confusion or dementia (45%), altered state of consciousness (32%), ethical reasons (11%), language barrier (4%) or lack of time for the palliative team (3%). Sixty-one percent of these patients finally died in the hospital (time between first call and death: 12,2 ± 14 days) and the rest quit the hospital (32% in institution, 68% at home where 78% continued with a second line of palliative care).
Discussion
In our study, the EQ-5D-5 L questionary established by the Federal Center of Expertise of health care (KCE) only worked for 11% of the palliative patients. Most of the patients are not able to assess their quality of life on a verbal way. It does not mean that they cannot express it in another way! It is commonly accepted that only 7% of information are transferred in words, the remaining 93% are about para-verbal (38% such as intonation, voice, …) and nonverbal communication (55% such as movements of the hands, the arms, …).
Abstract ID: 14
Impact of Gemcitabine/NAb-Paclitaxel on advanced pancreatic cancer survival: a retrospective case-control study
Fanny Harduin, Olivier Descamps, Hélène Nockerman, Thierry Delaunoit
Hôpital de Jolimont, La Louvière, Belgium
Abstract
Background:
Pancreatic cancer is associated with a high risk of mortality, especially for locally advanced or metastatic disease. For all stages, the 5-year overall survival is around 8%.
Until 1996, fluorouracil (5-FU) had been the most commonly used chemotherapy. Thereafter, gemcitabine, folfirinox and gemox were used with a modest survival improvement.
Since 2018, the first-line metastatic treatment recommended is the combination of gemcitabine and NAb-paclitaxel. In case of major comorbidities, gemcitabine could be utilised alone.
In patients with metastatic or locally advanced pancreatic cancer, we compared, in real life experience, the survival improvement on gemcitabine/nab-paclitaxel versus on gemcitabine.
Methods:
In this retrospective study, we included all patients with locally non resectable and synchronous/metachronous metastatic pancreatic cancer treated with gemcitabine/nab paclitaxel from 01/2018 to 12/2021 and those treated with Gemcitabine from 01/2011 to 12/2014. Patients were identified through the « RCM » (résumé clinique minimum) database of our hospital. Patients with resectable tumour, other neoplasms, unclear histology and treatment discontinuation were excluded from the analysis.
The primary and secondary endpoints were, respectively, overall survival and progression-free survival.
Statistical analyses consisted in Kaplan Meier analysis and Cox regression.
Results:
Seventy eight patients treated with gemcitabine/Nab-paclitaxel (cohort A) and 57 treated with gemcitabine (cohort B) were included in our study.
The two groups were well balanced in terms of gender, location, previous treatments, second-line treatments except for the age: patients in cohort A were younger than patients in cohort B (mean age: 66,9 ± 9,7 versus 71,9 ± 10, p = 0.004).
The hazard ratio in cohort A versus cohort B was 0,68 (95% confidence interval [CI], 0,48–0,98) for overall survival and 0,63 [95% CI, 0,44–0,91] for progression-free survival.
Overall one-year survival rates in the cohorts A and B were, respectively, 40% and 25% (p = 0.03). The progression-free one-year survival rates were 31% in cohort A and 21% in cohort B (p = 0.003).
After age-adjustment, it appeared that progression-free survival was still statistically significantly better in cohort A compared to cohort B (p = 0.03) whereas overall survival was not (p = 0.10).
Conclusions:
Compared to gemcitabine monotherapy, gemcitabine/NAb-paclitaxel improved overall survival and progression-free survival in first-line treatment for metastatic pancreatic cancer.
For cancers that were locally advanced, there was no significant difference in overall survival and progression-free survival.
Grade III/IV toxicities were well balanced between both groups.
Abstract ID: 15
Clinical presentation, etiology, and outcome of infective endocarditis – A retrospective cohort study from 2016 to 2021
Raphaëlle Dermine, Romain Courcelle, Olivier Descamps, Elodie De Groote
Hôpital de Jolimont, La Louvière, Belgium
Abstract
Background
Infective endocarditis (IE) remains a severe disease, associated with high morbidity and mortality. These are influenced by local guidelines and Endocarditis Team consultation. According to recent literature, the 30-day mortality rate is approximately 20%. Little is known about mortality risk factors. The aims of this study were to characterize the population suffering from IE in our hospital, to evaluate the outcome of these patients, and to identify mortality risk factors.
Methods
We conducted an observational retrospective study including all patients diagnosed with IE, during the period between 01/01/2016 and 31/08/2021. We excluded patients with non-infectious endocarditis, with alternative diagnosis, or with missing data. The primary endpoint was the overall survival. The following data were recorded: classical risk factors for IE, comorbidities, clinical presentations, echocardiographic features, causative micro-organisms, antimicrobial therapy, some aspects of the surgical treatment and the 30-day and 6-month mortality.
Results
During this 5,7 years-period, 104 patients were identified. Median age was 71 years. These patients had numerous comorbidities: smoking (52%), heart failure (46%), history of ischaemic heart disease (27%), diabetes (30%), cancer (26%) and chronic kidney disease (35%). The most frequently affected valve was the mitral valve (53%). An abscess was described in 30% as well as severe valvular regurgitation in 25% of all IE. Staphylococcus aureus was the most frequent bacterial cause of IE, followed by streptococcus species and enterococci. When the entrance site of the causative agent was identified, it was mostly the skin or the digestive tract.
The 30-day and 6-month mortality rates reached, respectively, 47% and 56%. Among the survivors, the most common complication of IE was systemic embolization (18%).
None of the comorbidities appeared to be predictive for mortality. We identified as statistically significant mortality risk factors the presence of a valvular abscess, Staphylococcus aureus infection, and the Euroscore II. Conversely, the streptococcus species appeared to be less aggressive than the other micro-organisms.
The 30-day mortality was non significatively higher in medically treated patients (N = 55; 53%) compared to surgical patients (N = 49; 47%). Amongst medically treated patients, those (N = 36) who complied criteria for surgery according to the guidelines but who were not operated due to contraindications to surgery had significantly higher 30-day mortality (69% versus 0%; P < 0.001) than those (N = 19) who were not operated in accordance with the guidelines. Among the patients who underwent surgery, the duration of antibiotherapy before surgery had no significant impact on mortality.
Discussion
In conclusion, in our cohort of IE, the 30-day mortality rate was far higher than described in the literature. Our population was a very high-risk population, with severe comorbidities, serious clinical presentation, valvular abscess and frequent severe valvular regurgitation. This shows the importance of prevention and the need to identify risk patients at an early stage. We identified as risk factors for mortality: presence of an abscess, Staphylococcus aureus infection and the Euroscore II. In the future, it could be interesting to develop and use a mortality risk score to personalize the treatment strategy and improve the quality of care in patients with IE.
Abstract ID: 16
NO elevation’s role in asthma diagnosis
Claire Musquar, Olivier Descamps, Delphine Gouteux
Jolimont, La Louvière, Belgium
Abstract
Background
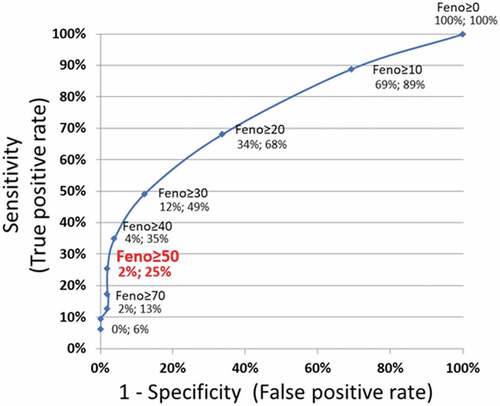
Asthma, which affects about 265 million individuals worldwide, is a disease with a great variability in clinical expression. According to the Global Initiative for Asthma (GINA), ‘asthma is defined by the history of respiratory symptoms that vary over time and in intensity, together with variable expiratory airflow limitation’. The diagnosis can be made with spirometry or with tests of bronchial hyperresponsiveness. However, according to the recent guidelines, the exhaled Nitric Oxyde (FeNO) should not be used in asthma diagnosis. However, our clinical experience tends to show that an elevated FeNO is often associated with a positive challenge test. Therefore, our aim is to explore if there is a FeNO threshold above which the diagnosis of asthma can be confirmed.
Methods
In this retrospective study, we identified from the hospital’s invoicing database, adults who had an exhaled NO measurement and a methacholine challenge test between 2019 and 2021. Another inclusion criteria was that all those patients had to have prior spirometry with results within normal range. The exclusion criteria were: failed FeNO, active smokers, patients already under treatment and those with recent respiratory infection. Using the challenge test as our gold standard to discriminate asthmatic from non-asthmatic, we evaluated specificity and sensitivity (ROC curve) of FeNO as a marker for the diagnosis of asthma. Cofounding factors considered were the Tiffeneau index, past smoking, atopy, obesity as well as levels of eosinophils and total IgE.
Results
Based on our selection criteria, we identified 284 patients, of whom 114 had one or more exclusion criteria. Among the remaining 170 patients, 63 were considered as asthmatic on the basis of a positive challenge test and 107 were non asthmatic. These two groups had similar characteristics regarding sex, obesity (BMI >30), IgE levels and atopy, whereas asthmatic patients were older on average (49 ± 14 vs 46 ± 16 years; p = 0,04), had higher counts of eosinophils (268 ± 200 vs 185 ± 152/mmc; p = 0.004) and had a lower prevalence of past smokers (13% vs 26%; p = 0,04). ROC curve () showed the specificity and sensitivity of various cut off of FeNO as a marker for the diagnosis of asthma.
Choosing 50 ppb as the threshold above which asthma can be assumed (sensitivity: 25% and false-positive rate: 2%), we searched for possible confounding factors by comparing patients above (N = 18) this threshold and below (N = 152). The only significant differences were a greater proportion of men (61% vs 35%, p = 0,03) and a higher count of eosinophils (424 ± 241 vs 189 ± 146/mm3; p < 0.001).
Discussion
A threshold of exhaled NO of 50 ppb which yields a sensitivity of 25% in asthma diagnosis with a false-positive rate of only 2% may be a good alternative to the challenge test. Challenge test is indeed more time consuming and stressful: it may lead to an asthma attack and is sometimes refused by the patient. However, the sensitivity was lower than expected. Therefore, the methacholine challenge test remains of application in routine diagnosis of asthma, which is consistent with the European guidelines.
Abstract ID: 17
DRY WEIGHT CHANGES IN HAEMODIALYSIS PATIENTS DURING THE COVID-19 PANDEMIC
François Collard, Olivier Descamps, Benjamin Seront
Pôle Hospitalier Jolimont, La Louvière, Belgium
Abstract
Background
Dry weight is defined as the lowest tolerated post-dialysis weight at which there are minimal signs or symptoms of hypovolemia or hypervolemia. Achieving dry weight is a goal for each dialysis session. That improves blood pressure control and reduces cardiovascular risk in dialysis patients.
Haemodialysis patients may experience weight loss likely related to a reduction of dry mass when catabolic reactions and inflammation occur. Our aim was to assess the impact of SARSCov-2 infection on haemodialysis patients and analyse factors associated with dry weight variations observed during the COVID-19 pandemic.
Methods
In this retrospective observational single-centre study, we analysed the clinical characteristics of all patients undergoing haemodialysis at the Pôle Hospitalier Jolimont during COVID-19 pandemic from 1 March 2020 to 28 February 2022.
We determined dry weight at day 1 after diagnosis of SARSCov-2 infection or at day 1 of a randomly assigned 28-days observation period and at 2, 3 and 4 weeks later.
We compared infected and uninfected patients and examined the clinical features associated with SARSCov-2 infection and those associated with changes in dry weight.
Results
Within the observation period, among the 162 haemodialysis patients, 47 patients were infected with SARSCov-2. Three patients were excluded because they have been infected before the first dialysis session and seventeen others due to missing data. Two patients were infected twice but we considered the second episodes as relevant and had therefore 144 observations.
Dry weight variation ratio (dry weight variation divided by dry weight at day 1) was a continuous non normally distributed variable for which we performed Wilcoxon rank sum tests and Student’s t-tests.
Dry weight variations were bigger in patients infected with SARSCov-2 compared to non-infected patients: the mean dry weight variation ratio was – 2,4 ± 2,2% (SD) in the infected dialysis patients and – 0,6 ± 2,0% in the uninfected patients (p < 0.001). A very strong association was found between SARSCov-2 infection and loss of dry weight (0,5 kg and more) with odds ratio = 21,89; 95% CI [7,17–66,85]. No difference was found whether infected patients were symptomatic or not (–2,6 ± 2,2% vs – 2,3 ± 2,3%; p = 0,662).
Infected patients and non-infected patients significantly differ by the sex distribution (76% vs 52% males; p = 0,008). We performed a Cochran-Mantel-Haenszel stratified analysis and confirmed the association between loss of dry weight and SARSCov-2 infection after controlling for effect modification or confounding by sex. Furthermore, dry weight often varies during early haemodialysis sessions and a bias such as a short dialysis duration was also ruled out. Indeed, no correlation was found between the shortest dialysis durations (less than 2 months) and the dry weight variations observed in our population.
Discussion
SARSCov-2 infection is associated with decreases of dry weight in haemodialysis patients. Systemic effects of SARSCov-2 infection are suspected since dry weight changes are quite similar both in symptomatic and asymptomatic infected dialysis patients.
Only 2 patients in our population died from complications related to SARSCov-2 infection. Adapting dry weight may be a major element in lowering mortality in infected dialysis patients.
Abstract ID: 18
Is there a connection between the severity of high cobalamin serum levels and underlying diseases in hospitalized patients?
Sophie Dupont, Helene Nokerman, Stephan Frederic, Alain Kentos, Olivier Descamps
Pôle Hospitalier Jolimont, La Louvière, Belgium
Abstract
Background
Elevated serum levels of cobalamin (B12) are frequently observed in hospitalized patients. Some studies have reported an association between patient mortality and high B12 levels in hospitalized patients. Many pathologies, including acute and chronic liver diseases, neoplasia, malignant hemopathies, renal failure and auto-inflammatory disease are associated with B12 elevation. The aim of our study was to examine whether, amongst patients with elevated B12, the severity of this one (high B12) is more specifically associated with one of these diseases. This could refine the clinical attitude to have in front of high cobalamin blood level.
Methods
In this retrospective study, we selected patients admitted between October 2021 and November 2021 where routine admission blood test showed serum cobalamin levels (B12) above 770 pg/ml. We excluded patients under 18 years old, patients with cobalamin supplementation and patients with cobalamin levels above 2000 pg/ml (as such levels may result from immunologic complexes, IgG-vitB12, interfering with the dosage of B12). Our primary endpoint was the association between the severity of high B12 levels and the presence of pathologies generally associated with high B12 levels. The secondary endpoint was its association with the mortality.
Results
Amongst the 247 patients we selected during the period of our study, 45% had chronic or acute renal failure, 23% hepatopathies, 11% malignant hemopathies, 21% others neoplasia and 5% an auto-inflammatory disease. Twenty-five percent had more than one of these pathologies. Thirty-two percent of these patients died within the following 8 months.
Comparing the patients with B12 levels below or above the median (1071 pg/ml), the prevalence of the pathologies of interest (or the 8-month mortality) did not differ except for hepatopathies (15% versus 30%; p = 0,006). In addition, there was a trend to statistical significance association in patients having more than one of these pathologies of interest (20% versus 31%; p = 0,06). Comparing three groups split based on the tertiles of B12 levels (950 pg/ml and 1258 pg/ml), only the same association with hepatopathies was found statistically significant with a continuous gradient (13%, 23% and 31%, respectively, in the first, second and third tertile; p = 0,02). To attempt to discriminate a cut off for suspecting hepatopathies, we performed a ROC-curve analysis, but found no efficient diagnostic test for hepatopathies using B12 levels.
Conclusion
Extremely high cobalamin serum levels are associated with hepatopathies in hospitalized patients. However, such levels are not efficient to diagnose hepatopathies. There was no association between the severity of high cobalamin serum levels and other diseases. The mortality is not higher when cobalamin serum levels are severely high.
The 8-month mortality of our cohort was very high (32%), it could indicate a poor prognostic in our hospitalized patients. More studies with comparison to a control population are required.
Abstract ID: 19
Incidence of hypokalemia in patients under intravenous flucloxacillin versus intravenous amoxicillin therapy – a retrospective study
Arnaud Lorge, Olivier Descamps, Élodie De Groote
Pôle Hospitalier Jolimont, Réseau HELORA, La Louvière, Belgium
Abstract
Background
When administered intravenously at high doses, penicillin and its derivatives may lead to renal loss of potassium by non-absorbable ion effects in the distal tubule and/or intracellular redistribution. Flucloxacillin, a narrow-spectrum beta-lactam antibiotic is commonly indicated for infection caused by methicillin-sensitive Staphylococcus aureus, and must be prescribed at high dosages and long-term intravenous therapy in special circumstances including bacteriemia prosthesis-related infection, osteomyelitis or endocarditis. Amoxicillin is a beta lactam anti-microbial therapy, active against gram-positive cocci, including nonpenicillin resistant streptococcal, staphylococcal, and enterococcal species. It is commonly used for multiple infections and following the antimicrobial susceptibility of the causative microorganisms (mastoiditis, epiglottitis, community pneumonia, …).
Little is known about the difference in hypokalemic effect of each type of these penicillin derivatives. The aim of this study is to compare the incidence of hypokalemia in patients receiving intravenous flucloxacillin or intravenous amoxicillin.
Methods
In this retrospective study, data were collected from the pharmacy record of HELORA Network (RCM Database). We included all patients hospitalized from January 2021 to December 2021, and who received intravenous flucloxacillinor amoxycillin for at least 5 days. Exclusion criteria were: age under 18 years, therapy with premature shift to oral therapy, potential disease known to induce hypokalemia, dialyzed patients. Confounding factors were recorded such as diuretics, insulin therapy, antibiotic dilution (glucose 5% versus NaCl 0,9%) and diarrhea which could be associated to antibiotic therapy.
Results
Amongst the 1044 patients found in the database, 150 patients could be selected based on our criteria: 56 (38%) were treated by intravenous amoxicillin and 94 (62%) by intravenous flucloxacillin. Ages (68 versus 69 years) and sex distribution (68% vs 69% males) were similar as well as the proportion of potassium-influencing factors: diarrhea and others digestives conditions (5.4% vs 5.3%), insulin therapy (21% vs 24%), loop diuretic (30% vs 27%) and potassium sparing-diuretic (5% vs 11%), ACE/sartan (16% vs 28%, P = 0.09), proportion of diabetes and renal dysfunction. The only significant difference between the two groups was the support for antibiotic dilution composed of NaCl 0.9% (84% vs 60%; p < 0.05) rather than Glucose 5% dilution. The change of potassium between hospital admission and the lowest level in the course of hospitalization was greater (p = 0.02) in the flucloxacillin group (−0,7 mEq/l) versus amoxicillin group (−0.49 mEq/l). Using a cut-off of 3,3 mEq/l potassium to define hypokalemia, hypokalemia occurred with a significantly higher proportion (P = 0.005) in patients in the flucloxacillin group (49%) than in the amoxicillin group (26%). In separate analysis taking into account the dilution, hypokalemia occurred was also significantly greater between these two antibiotic regimens using dilution with NaCl 0.9% (28% vs 50%; p = 0.02) as well as with glucose 5% (25% vs 47%, p < 0.05).
Conclusion
Intravenous flucloxacillin induces more frequently hypokalemia than intravenous amoxicillin. This difference between these two penicillin derivatives could be due to the non absorbable ion effects in the distal tubule and/or intracellular redistribution, more important with flucloxacillin than amoxicillin, potentially due to the molecular conformation of metabolites.
Abstract ID: 20
Cerebral air embolism as a complication of esophagogastroduodenoscopy.
Hans Buelensa, Merel Van Parijsb, Evien Alic, Pascale Abramsd,e, Frank Van De Mierope, Isabelle Maurissene
aUniversity of Antwerp, Antwerp, Belgium; bGhent University, Ghent, Belgium; cKU Leuven, Leuven, Belgium; dSint-Vincentius, Antwerp, Belgium; eSint-Augustinus, Antwerp, Belgium
Abstract
Introduction
Cerebral air embolism is a rare complication following gastrointestinal endoscopic investigations. Symptoms are cardiovascular or pulmonary (hypoxia, hypotension, collapse, cardiac arrest, etc.) and deterioration of neurological functions. Treatment includes supportive therapy and hyperbaric oxygen. (1–2) Decreased neurological status after endoscopy should never be solely attributed to the effects of sedation. Because of potential mortality, it is crucial to recognise this complication and take appropriate action.
Case description
An 85-year-old woman presented with one episode of hematemesis. The patient’s history included liver cirrhosis (alcoholic etiology), hypertension, hypercholesterolaemia and breast ductal adenocarcinoma. She takes propranolol for prevention of variceal bleeding. She had a DNR-1 code.
The patient was hemodynamically stable with a slightly painful epigastric palpation. Lab results showed a hemoglobin of 13,5 g/dl, other tests were also normal. She had a prolonged QTc interval of 506 ms, taking trazodone, citalopram and zolpidem. Therapy included fluid and pantoprazole 40 mg twice a day intravenously. Abdominal ultrasound showed liver cirrhosis. Esophagogastroduodenoscopy reveals remarkable esophagitis and a distal esophageal bleeding (without a direct visualisation of varices or the bleeding origin). At the end of the examination, the patient was suddenly not responsive, despite not receiving any sedatives.
Therapy was started with a mayo cannula and oxygen. Vital signs and glycaemic level were normal. She had a Glasgow Coma Scale of 3/15 with miotic pupils and eyes deviated to the left. Although no convulsions were seen, lorazepam 2 mg was administered to treat possible underlying epileptic activity. CT scan showed multiple air embolisms in both hemispheres. Somatostatin was started to treat possible variceal bleeding.
Although non-responsive, she was spontaneously moving her legs. Hyperbaric oxygen therapy was considered, but decided against for multiple reasons. Later, there was some neurological recovery; following commands, minimal speech and left-sided hemineglect. Sudden respiratory deterioration with pneumothorax occurred, treated by needle decompression. Cardiac ultrasound showed no signs of a patent foramen ovale or other transseptal passage. Placing the patient’s comfort first, only oxygen was given. The left-sided hemiparesis persisted. Her general condition further decreased. A DNR-3 code was introduced and palliative sedation was started. Sadly, the patient died.
Discussion
Air embolism is more frequently associated with ERCP, but can also happen during other gastrointestinal endoscopy such as esophagogastroduodenoscopy with an incidence of around 0,00056%. (1–3) The proposed mechanism in this patient is insufflation of air, entering through the esophageal varix into the portal venous system. For a cerebral air embolism to occur, an intracardiac shunt could be present, but was not seen on echocardiography. Other mechanisms mentioned in previous literature include intrapulmonary shunts (often seen with chronic liver disease), passage from the superior caval vein to the cerebral veins by retrograde flow, etc. (1–2, 4). No autopsy was performed in discovering the exact mechanism. Therapy options are supportive (Trendelenburg or left lateral decubitus position, oxygen, IV fluids, vasopressors) and hyperbaric oxygen. (1–3) Using carbon dioxide for insufflation can lower the risk of an air embolism. (3, 5) A pre-endoscopic echocardiography could prevent some cases but is not cost-effective.
Abstract ID: 21
Monkeypox and co infections presenting as a painful genital rash
Maja Kiselinova, Sanne De Smet, Linos Vandekerckhove, Marie Angelique De Scheerder
UZ Gent, Gent, Belgium
Abstract
Since May 2022, there is an ongoing monkeypox (MPX) outbreak that has been declared as a public health emergency of international concern by WHO. Most of the cases are men who have sex with men, frequently presenting to the clinic with one or more sexually transmitted diseases (STDs).
We present one of the first cases admitted to our hospital ward with a clinical image of multiple painful peri anal lesions. To our experience, even most extensive cases can be treated with symptomatic and directed therapy. Screening and treatment for concomitant STDs is mandatory.
The MPX outbreak has become a public health concern for which the best preventive options are actively discussed. Currently, pre-exposure and post-exposure vaccination are available in Belgium, but vaccines are scarce. Pre-exposure vaccination may be effective in the transmission of MPX virus, but probably insufficiently in the current ongoing epidemic. Therefore, there is an urgent need for structured prevention programs, improved diagnostic strategies and systematic clinical management.
Abstract ID: 22
When you hear hoofbeats, you might want to think about zebras too
Pauline Vermoesena,b, Charlotte Stegerb, Jeroen Mausb
aUniversity of Antwerp, Antwerp, Belgium. bZNA Middelheim, Antwerp, Belgium
Abstract
Introduction
Drug Reaction with Eosinophilia and Systemic Symptoms Syndrome (DRESS syndrome) is a potentially life-threatening systemic reaction linked to a variety of medication (1). Although it is considered rare with a prevalence of 1/1.000 to 1/10.000 drug exposures, it carries a great disease burden due to its high mortality which can lead up to 20% (2). We recently encountered a case that underlines how correct diagnosis and quick withdrawal of the causal drug are essential in the prognosis of this syndrome.
Case
An 82-year-old woman was admitted because of a pruritic generalized rash and fatigue since a couple of days. Clinical investigation showed axillary lymphadenopathy and multifocal neurological symptoms. Laboratory investigation showed leukocytosis of 15,1 x10^9/L (3,45–9,76 x10^9/L) with a significant eosinophilia of 11.3% (0.9–8.4%), a mildly disturbed liver set and an elevated high-sensitivity troponin of 1096 ng/L (<12 ng/L). Further anamnesis revealed the intake of carbamazepine for trigeminal neuralgia since 6 weeks. Skin biopsy revealed a perivascular lymphocytic infiltrate with eosinophilia. Additional serology was positive for Human Herpesvirus 6 (HHV-6). No clear coloring of the hearth muscle was seen on MRI of the heart. MRI of the brain showed multiple emboligenic infarctions.
On the RegiSCAR inclusion criteria for DRESS syndrome, the patient scored 6, which made the case definite (3).
Carbamazepine was immediately stopped and high doses of IV steroids (2 mg/kg/d) were given. A topical steroid was prescribed until skin symptoms resolved. Our patient fully recovered when she was discharged 3 weeks later.
Conclusion/Discussion
We present a case of DRESS syndrome caused by carbamazepine intake. It is known that aromatic anticonvulsants are the most common cause of DRESS syndrome, but only recently we began to understand that DRESS syndrome is more than a hypersensitivity reaction to drugs (4–6). It is now seen as an interplay among drugs, viruses and the immune system which is illustrated in this case by the positive serology for HHV6 (7, 8).
Furthermore, this presentation of DRESS syndrome was complicated with myocarditis and emboligenic infarction, a severe and under-recognized complication with a mortality up to 45% (7, 8). Due to the RegiSCAR criteria, we were able to quickly recognize the syndrome and to start systemic therapy, improving the patients’ outcome.
Abstract ID: 23
How to predict mortality in elderly population with pneumonia ?
Justin Kroemmer, Olivier Descamps, Pierre Hanotier, Nokerman Hélène
Jolimont, La louvière, Belgium
Abstract
Background
Pneumonia is a major cause of mortality and morbidity amongst elderly populations. There are several scores designed to predict the disease severity but they are more often studied in general adults rather than in geriatric populations.
Method
In this retrospective study, we included all patients aged over 75 years hospitalised with Community Acquired Pneumonia (CAP) between 1 January 2021 and 31 December 2021 selected in the databank of department of medical information, « RCM ». Patients with non-bacterial agent, nosocomial pneumonia, missing data, lost of follow-up, outpatient treatment, different or uncertain final diagnosis were excluded. CURB-65 score, Pneumonia Severity Index (PSI) and Charlson Comorbidity Index were calculated for all patients when sufficient data allowed doing so. Minimal Mental State Evaluation (MMSE), KATZ score and Mini Nutritional Assessment (MNA) were collected from medical record when available. Primary endpoint consisted in 30-day mortality after the diagnosis, secondary endpoints were transferred to the intensive care unit (ICU) and new institutionalisation after hospitalisation.
Results
During the period of the study, occurred 133 admissions for CAP: 59% were men and mean age at admission was 84,6 ± 6,1 years. CURB-65 and Charlson Comorbidity Index could be calculated in all patients whereas PSI in only 109 patients. MMSE was documented in 72 records, KATZ score in 33 and MNA in 66.
The 30-day mortality rate was significantly associated with the classical score for pneumonia: CURB-65 score (p < 0,001), PSI score (p = 0,012). Interestingly, it was also associated with the Charlson Comorbidity Index. In contrast, none of the other usual geriatric scores (Katz score, MMSE, MNA) nor prior institutionalisation was statistically associated with higher 30-day mortality.
No statistical associations were found between those scores versus ICU admission or new institutionalisation.
Discussion
In our elderly patients with Community Acquired Pneumonia, higher PSI score and CURB-65 score are associated with higher 30-day mortality. Interestingly, the Charlson Comorbidity Index which is usually used to predict 10-year survival in patients with multiple comorbidities was also strongly associated with higher 30-day mortality. Such association was not found for the other geriatric score studied in our cohort. There are some limitations: small number of patients, monocentric study, lack of some geriatric data in some deceased patients.
Abstract ID: 24
Clinical applications of rescue strategies in extensively drug-resistant HIV-1, a case report
Marco Morettia, Karolien Stoffelsb, Sigi VAN DEN WIJNGAERTb, Charlotte Martinc
aVrije Universiteit Brussel, UZ Brussel, Brussels, Belgium; bAIDS Reference Laboratory, Centre Hospitalier Universitaire St. Pierre, Brussels, Belgium; cUniversity Hospital Center (CHU) Saint Pierre, Brussels, Belgium
Abstract
Background: The availability of antiretroviral therapy for people living with HIV is increasing worldwide. However, limited therapeutical options are available for patients with multi-drug resistant HIV.
Purpose: To describe the clinical management and potential rescue strategies for a patient with extensively drug-resistant HIV-1 strains. Virological failures were followed by serial genotyping analyses showing the evolution of the mutations and resistances.
Methods: Serial genotyping analyses were carried out with Sanger sequencing techniques followed by resistance prediction using Stanford HIV Drug Resistance Database (HIVdb algorithm version 9.1). Drug susceptibility testing was performed by phenotyping through PhenoSense® (Monogram Biosciences Inc.). Tropism analyses were carried out by Trofile® (Monogram Biosciences Inc.).
Results: A 38-year-old female, perinatally HIV-1 infected, has been treated with 14 different antiretroviral regimens over 27 years at our HIV reference clinic. From 2009 to 2012, she was treated with a regimen containing integrase strand transfer inhibitors (INSTI), which progressively induced high-level resistance to all INSTIs. Thereafter, various attempts have been made to suppress the virus with an intravenous anti-viral induction, containing intravenous Foscarnet and Enfuvirtide. Finally, maintenance therapy was reinforced by adding Fostemsavir and Lenacapavir to the regimen, combined with efforts to improve compliance through multidisciplinary patient-tailored strategies.
Conclusion: The patient described in this report progressively evolved to a fully four-class drug-resistance HIV-1 infection due to suboptimal virological HIV control for years. Induction with off-label intravenous Foscarnet and Enfuvirtide, but also the availability of new first-in-class drugs Fostemsavir and Lenacapavir might be a game-changer for patients without alternative validated treatment.
Abstract ID: 26
Campylobacter fetus aortitis
Damien Hoolansa, Thierry Deremeb, Vincent Gerina, Louise Doyena, Jean-Christophe Marota, Grégoire Wieërsa
aClinique Saint-Pierre Ottignies, Ottignies, Belgium; bCentre hospitalier regional de Namur, Namur, Belgium
Abstract
Introduction:
Campylobacter fetus infections mostly occur in immunocompromised patient or patient exposed to infected cattle or sheep and can cause intestinal illness or systemic infection. This germ is characterized by a vascular tropism which can lead to rarely described infective aortitis at the occasion of a bacteriemia.
Case presentation:
An 85-year-old immunocompetent patient initially presented with diarrhea, asthenia, loss of weight, fever and an elevation of the CRP at 215 mg/dL. His medical history is marked by an abdominal aneurysm treated by an aorto-biiliac endoprosthesis in 2005. Abdominal CT-scan showed an increase in the abdominal aortic aneurysm size associated with peri-aortic infiltration (). PET-CT showed a perianeurysmal hypermetabolism compatible with a septic phenomenon (). Transesophageal echocardiogram revealed no vegetations and colonoscopy revealed no colic lesion. Resistant Campylobacter fetus was identified in the blood cultures leading to the diagnosis of infective aortitis. The patient was empirically treated by a 6-weeks course of meropenem IV (CMI 0,047 µg/mL).
Favorable clinical and biological evolution led to the patient discharge after 44 days.
Conclusion:
Campylobacter fetus infective aortitis is a rare but life-threatening disease. This case underlines the importance of considering this germ even in immunocompetent patients presenting a non-specific febrile illness with no history of exposure to infected animals. This will ensure adequate antibiotic therapy is set-up and fatal complications such as rupture of the aneurysm are prevented. Additionally, resistance of this germ should not be overlooked as suggested by this case which highlights the importance of using broad spectrum antibiotics such as meropenem as empirical treatment.
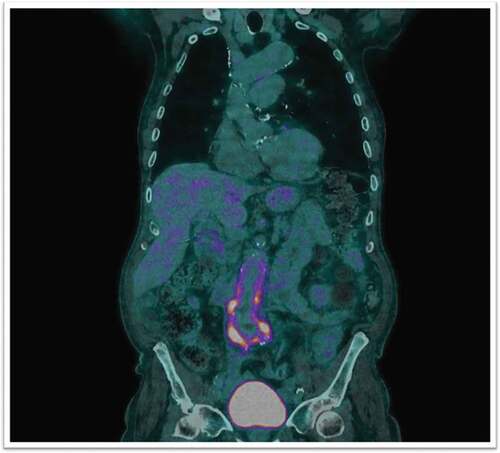
Abstract ID: 27
Altered consciousness and coma in a case of urea cycle disorder
Milad Ahadi, Dana Pencu
GHDC, Charleroi, Belgium
Abstract
Background: the urea cycle is a metabolic reaction that allows the transformation of nitrogen into urea in order to excrete it from the body. Genetic deficiency in an enzyme of this cycle lead to a urea cycle disorder (UCD). This pathology is mainly found in children but cases are described in adult patients, especially ornithine transcarbamylase (OTC) deficiency.
Case report: A 66-years-old female with no relevant medical history was admitted for deterioration of general condition in the emergency room. She was complaining of asthenia and vomiting starting several weeks before. During her stay in the emergency department she developed gradually an impaired consciousness followed by a coma. An initial work up with brain scan, blood test and gas analysis (showing respiratory alkalosis), electroencephagram and lumbar punction revealed no precipitant factor. Afterward, blood ammonium was measured and showed hyperamoniemia although there was no biological or iconographic argument for a hepatic insufficiency. Later on, in the presence of the triad of encephalopathy, hyperamoniemia and respiratory alkalosis the hypothesis of UCD was proposed. In order to confirm the diagnostic plasma and urinary amino acids levels and genetic testing were requested.
Discussion: Urea cycle disorder is genetic enzyme deficiency in one of the urea cycle metabolic pathway. Although these defects are mainly found in children, cases are described in adult patients, especially ornithine transcarbamylase (OTC) deficiency which is X linked. Clinical features presented by patients range from psychiatric abnormalities, recurrent vomiting and lethargy. Unlike children, adults can manifest an atypical presentation with delayed symptoms and hyperamoniemia may only occur during metabolic decompensations due to a catabolic stress (infection, gastro-intestinal bleeding, post-operative, myocardial infraction, chemotherapy …). Encephalopathy, elevated plasma ammonia, normoglycemia and respiratory alkalosis strongly bring to mind an UCD. Further investigations are needed to confirm the diagnosis, and imply amino acid profiles associated to molecular genetic testing. Quantitative plasma amino acid allows to distinguish between UCD subtypes. Genetic testing is beginning to take the place of tissue biopsies (that allows the analysis of enzymatic activity), and is now considered as a first-line approach for diagnosis. Patients with UCDs should be transferred to a Centre of Expertise after the diagnosis was confirmed for acute and long-term management.
Abstract ID: 28
A recovery rash: white islands in a sea of red
Liselot Vandenbergen, Halil Yildiz
Cliniques Universitaires Saint-Luc, Bruxelles, Belgium
Abstract
Introduction
People are travelling to regions where Dengue fever is endemic. Physicians should be able to recognize the clinical presentation of this viral infection. Dengue fever is associated with mucocutaneous manifestations such as flushing erythema and maculopapular or morbilliform eruption during the acute phase. However, in rare cases, a rash may occur during the recovery phase and seems to be due to an immune reaction.
Case description
A 33-year-old woman was evaluated for high fever (T: 39–40°C) since 5 days. Her main complaints were headache, muscle pain and dry cough. There were no dyspnea, gastro-intestinal or urinary symptoms.
She had no relevant past medical history and was not taking any medication. She returned from a 3-week holiday in Thailand 6 days before. She mentioned mosquito bites during her holiday and did not use repellent or prophylaxis for malaria.
On physical examination, temperature was 37.2°C, blood pressure 100/50 mmHg, heart rate 61 beats per minute and oxygen saturation 99% while breathing ambient air. Cardio-respiratory auscultation and abdominal examination were normal. She had no skin rash and no arthritis. She did not had signs of throat infection. Neurological examination was normal.
The neutrophil count was 590/mmc, lymphocyte count 580/mmc and the platelet count 78.000/mmc. CRP was 1 mg/L. LDH was slightly elevated (267 U/L) and GOT (44 U/L). Urine analysis was negative (44 white blood cells/µL). Blood cultures were taken. Nasopharyngeal swab for SarsCov2 (PCR) was negative. Two tick blood smears at 12 h interval were negative for malaria parasites. Serology for EBV was positive (but with presence of anti EBNA). Serology for CMV was negative for acute infection. The patient was immune for Hepatitis A and negative for Hepatitis B/C, Syphilis and HIV.
Chest X-ray was normal and the patient was discharged with a prescription of Paracetamol with a follow-up consultation in 1 week.
Five days later, the patient came back to the emergency ward because of a rash that was evolving since 3 days on her legs, arms, thorax and abdomen. The skin rash was not itchy or painful and was characterized by a confluent erythema with several white spots. She mentioned no more fever or muscle pain.
Her neutrophil count was 1000/mmc, lymphocyte count 1220/mmc and platelet count 165.000/mm3. There was still no elevation of CRP level. Liver enzymes were higher (GOT 69 U/L, GPT 62 U/L) and LDH 480 U/L.
The patient was discharged with no extra measures but a follow-up consultation. Based on the skin manifestation (erythematosus rash with island of sparing), a Dengue infection was suspected.
One week later, she was evaluated on the internal medicine consultation. She had no persistent complaints. There was still a skin hyperpigmentation, particularly on the legs and serology for Dengue came back positive.
Conclusion
When faced with an erythematous or petechial rash with areas of normal skin (isles of white in a sea of red) in a patient with a history of traveling, a Dengue infection should be highly suspected.
Abstract ID: 29
Multiple opportunistic infections complicating a paraneoplastic Cushing syndrome
Igor Maleca, Michaël Piagnerellib, Sandrine Milasb, Isolde Ramonb, Soraya Cherifib
aUniversité libre de Bruxelles, Bruxelles, Belgium; bCHU Charleroi, Charleroi, Belgium
Abstract
Cushing’s syndrome, an endocrine disorder characterized by excessive levels of cortisol is often associated with many complications including opportunistic infections. In this case report, we describe multiple severe opportunistic infections, including invasive disseminated aspergillosis with central nervous system involvement and Pneumocystis jirovecii pneumonia, due to endogenous uncontrolled hypercortisolism.
A 55-year-old woman, who presented with leg swelling for a few months, was hospitalized in CHU de Charleroi for severe hypokaliemia and uncontrolled hypertension. Clinical work-up showed severe hypercortisolism secondary to ectopic ACTH secretion. An abdominal MRI revealed a voluminous expansive intra-vaginal neoplastic process. A biopsy showed a neuroendocrine small cell carcinoma of cervical origin. High volume infusion of potassium must be used under monitoring in intensive care unit. Ketoconazole treatment was started, followed by ethomidate. Finally, a ‘rescue’ bilateral adrenalectomy in order to control hypercortisolism was performed.
The case was regularly discussed with Endocrinology, Intensive care and Infectious diseases.
The patient developed a respiratory distress and a bronchoscopy bronchoalveolar lavage was performed with a positive culture for Aspergillus fumigatus and a positive aspergillus galactomanan. Chest CT-scan was also typical of pulmonary aspergillosis
The day after surgery, the patient developed a paresis of the left arm and a left facial paresis.
A brain MRI showed multiple ischemic embolic stroke with predominantly right hemispherical lesions and a positive aspergillus galactomanan in the cerebrospinal fluid at 7, leading to a diagnosis of invasive disseminated aspergillosis with central nervous system involvement. A second bronchoalveolar lavage revealed the presence of Pneumocystis jirovecii and a positive culture for Klebsiella pneumoniae ESBL (Extended-Spectrum Beta-Lactamases). Despite administration of large antibiotics and antifungal treatments, the patient died.
Paraneoplastic Cushing syndrome is a real diagnostic and therapeutic challenge.
Screening of opportunistic infections in uncontrolled hypercortisolism should be done actively.
A multidisciplinary approach is required to improve the management of a complicated case of polymicrobial infection in the setting of hypercortisolism
Abstract ID: 30
Epidemiology and management of viral meningoencephalitis identified by multiplex PCR in a tertiary hospital between 2018 and 2022
Marie Heijmans, Christophe Lelubre, Soraya Cherifi
CHU de Charleroi, Charleroi, Belgium
Abstract
Introduction:
The epidemiology of viral meningitis and encephalitis (ME) is less known than that of bacterial origin. This retrospective study was performed at the University Hospital of Charleroi from 01/02/2018 to 01/02/2022. The only inclusion criteria was a positive PCR for one of the viruses on cerebrospinal fluid (CSF) analysis (via lumbar puncture) detected by the Filmarray® ME panel. The objectives of the study were to analyze the epidemiology and management of patients with viral meningoencephalitis by comparing adults and children under the age of 16.
Results:
A total of 61 patients were included: 40 adults (66%) and 21 children (<16 years) (34%).
Pathogens identified were: 31 (51%) Enterovirus, 14 (23%) Varicella zoster virus, 8 (13%) Human herpesvirus 6, 5 (8.2%) Herpes simplex virus type 1, 2 (3.3%) Herpes simplex virus type 2 and 1 (1.6%) Human parechovirus. The median time from admission to getting the lumbar puncture was 3h46min (2h20-6h36) and tended to be shorter in children (p = 0.086). Pyrexia and respiratory prodromes were more frequent in children (respectively, p = 0.008 and p = 0.031), in contrast to acute neurological deficits that were more frequent in adults (p = 0.032). A total of 40 (71%) empirical treatments (prior to PCR results) were initiated. Children tended to be more frequently treated empirically with antibiotics (p = 0.059), but adults were more likely to receive antiviral treatment (p < 0.001). Empirical treatments were adapted for 67% of patients within the first 24 hours and more rapidly in adults (p = 0.007), 26 (65%) were stopped and 11 (20%) were modified. Six (11%) patients received aciclovir treatment following PCR results. The median length of hospital stay was 4 days (2–14). Four (7.0%) patients were admitted to intensive care and 1 (1.8%) patient died during hospitalization.
Conclusions:
Enteroviruses are the most commonly identified cause of viral central nervous system infection. Clinical presentation and management differ significantly between adults and children. The use of a multiplex PCR has had a positive impact on the adaptation of empirical treatments, especially in the adult population.
Keywords: Viral Meningoencephalitis-Multiplex PCR
Abstract ID: 32
Digestive melanoma metastasis mimicking Kaposi sarcoma in HIV-1 infected patient.
Xavier Gilis, Jean-François Baurain, Bénédicte Delire, Jean Cyr Yombi, Halil Yildiz
Cliniques Universitaires Saint-Luc, Brussels, Belgium
Abstract
Introduction
Cytomegalovirus colitis is the main cause of gastrointestinal (GI) bleeding in HIV-infected patient. Other reasons include cancer, colonic ulcers, and idiopathic colitis, depending on the cohort examinedCitation1,Citation2. Kaposi sarcoma is rarely the origin of lower gastrointestinal hemorrhage. We would like to describe here an unusual cause of GI bleeding in an HIV-1 infected patient.
Case report
A 69-year-old caucasian man living in South Africa came in Belgium with unexplained anemia, rectal bleeding and acute confusion. His relevant medical history includes an HIV diagnosis treated with Efavirenz/Emtricitabine/Tenofovir and a localized cutaneous melanoma treated 3 years ago with a combination of surgery and radiotherapy.
Confusion arose in 2 weeks, while at the same time he noticed the appearance of right hemiparesis and dyspnea. He admitted that he had not taken his antiretrovial therapy for 2 weeks.
An aregenerative microcytic grade 4 anemia linked to an iron shortage was detected in the initial blood test. The CD4 cell count was normal (502/µL) and the HIV viral load was undetectable (<40 copies/mL). A right hemiparesis (4/5), a walking deviation to the right, and a right hemianopsia were observed on neurological examination, but no skin lesions were found.
Multiple lesions suggestive of Kaposi sarcoma were discovered in the stomach and colon during gastroscopy and colonoscopy. Multiple metastatic lesions surrounded by edema were visible in the left parieto-occipital and right parietal lobes on the cerebral CT scan and MRI. A [18 F]FDG-PET/CT was performed and revealed pulmonary nodules, lymph nodes, peritoneal carcinomatosis, pancreatic, adrenal, subcutaneous and bone hypermetabolic lesions.
The histology of the intestinal biopsy confirmed the metastatic relapse of malignant melanoma.
Discussion
Gastrointestinal tract metastatic lesions are a rare presentation for cancer spreading. Malignant melanoma, breast cancer and pancreatic cancer are the predominant primary sitesCitation3. Patients with gastrointestinal metastasis are diagnosed at advanced-stage. The entire digestive tract may be affected, but the stomach, colorectal section, and small intestine remain the primary sites3,Citation4.
Conclusion
We describe here a rare cause of digestive bleeding in HIV-1 infected patient secondary to digestive tract metastasis of melanoma. The visual characteristics of the intestinal lesions were consistent with Kaposi sarcoma. However, given his high CD4 cell count and an undetectable viral load, this diagnosis appeared unlikely.
References
- Chalasani, N., & Wilcox, M. (1998). Etiology and outcome of lower gastrointestinal bleeding in patients with AIDS. The American Journal of Gastroenterology, 93(2), 175–178. https://doi.org/10.1016/S0002-9270(97)00090–7
- Bini, J., Weinshel, E., & Falkenstein, D. (1997). Risk factors for recurrent bleeding and mortality in human immunodeficiency virus–infected patients with acute lower GI hemorrhage. Gastrointestinal endoscopy, 49(6), 748–753. https://doi.org/10.1016/S0016-5107(99)70294–4
- Gilg, M., Gröchenig, H-P., Schlemmer, A., Eherer, A., Högenauer, C., & Langner, C. (2018). Secondary tumors of the GI tract: origin, histology, and endoscopic findings. Gastrointestinal endoscopy, 88(1), 151–158. https://doi.org/10.1016/j.gie.2018.02.019
- Kaila, V., Jain, R., Lager, D., Jensen, P., & Feldman, M. (2021). Frequency of metastasis to the gastrointestinal tract determined by endoscopy in a community-based gastroenterology practice. Baylor University Medical Center Proceedings, 34(6). https://doi.org/10.1080/08998280.2021.1936361
Abstract ID: 34
Adrenal incidentaloma in the 3rd trimester of pregnancy followed by gravid uterus rupture.
Tiphaine Cartona, Irène Assafb, Ahmad Awadab, Martina Pezzulloa, Clotilde Lamya, Anne-Céline Cheronc, Julie Désird, Natacha Driessensa
aHUB-hôpital Erasme, Brussels, Belgium; bHUB-hôpital Bordet, Brussels, Belgium; cGHdC Grand Hôpital de Charleroi, Charleroi, Belgium; dInstitut de Pathologie et de Génétique, Gosselies, Belgium
Abstract
It is rare to discover an adrenal lesion during pregnancy. Before the age of 30, the risk of carcinoma increases and warrants a quick management. Pregnancy is also a challenge for the management of adrenal lesions because maternal physiological changes make test interpretation difficult, imaging studies are limited, and many treatments are contraindicated. Trans-abdominal laparoscopic surgery is technically feasible by expert teams and should ideally be performed during the first or second trimester. Maternal prognosis is conditioned by the nature of the lesion and that of the fetus is less favorable in cases of Cushing’s syndrome.
We report the case of a 23-year-old woman, with no previous history, pregnant with 27 weeks of gestation (G1P0) in whom an adrenal incidentaloma (45x27x63mm) was demonstrated on an ultrasound performed 3 days after a moderate-intensity car crash.
The characteristics of the lesion on MRI, performed 6 days after the accident, were in favor of a neoplastic lesion: hyposignal in T1, heterogeneous in T2 and in diffusion. There was no argument for an adenoma (no fat contained) or for a hematoma (no hypersignal in T1). Given its size (>4 cm) and heterogeneity, this adrenal mass was suspicious of an expansive lesion. The left adrenal was unremarkable and there was no macroadenomegaly in the upper abdominal.
There were no symptoms, clinical signs or biological elements suggestive of a functional tumor.
Because this expansive mass was non-functional in an asymptomatic patient in the third trimester of pregnancy, it was decided to monitor the lesion by MRI at 1 month. MRI monitoring showed a reduction in size by half (32x11x25mm) as well as a T1 signal change arguing, this time, for the diagnosis of hematoma. A final ultrasound at 35 weeks of gestation confirmed the resorption of the hematoma. We retained trauma as the cause of the adrenal hemorrhage.
The obstetrical follow-up continued without any particularity until the delivery.
The delivery was complicated by fetal distress in late labor, leading to an emergency cesarean section during which the obstetricians discovered a spontaneous posterior uterine rupture with hemoperitoneum that required a hysterectomy. On review, the patient had no hypertensive peak and labor had normal kinetics. The patient also had no history of curettage, uterine surgery or previous cesarean section.
The occurrence of a spontaneous adrenal hemorrhage followed by a rupture of a gravid uterus was suspected of a collagen disease in its most severe form of vascular Ehlers Danlos syndrome (vEDS). A targeted genetic analysis was proposed to our patient and is still in progress.
The occurrence of spontaneous adrenal hemorrhage should systematically lead to a workup for vEDS (first serious manifestation in our case).
The prevalence of vEDS is estimated between 1/50,000 and 1/200,000 but is probably underdiagnosed, especially in milder forms of the disease. The prognosis varies depending on the type of pathogenic variant of COL3A1.
Genetic diagnosis is essential to propose prophylactic measures to clinically silent patients and to ensure expert multidisciplinary management in case of complications.
Abstract ID: 36
Fibrosis stage is the main driver of liver-related events in adults with biopsy-proven Nonalcoholic Fatty Liver Disease
Adrien Bocquillona,b, Lukas Otero Sanchezc, Delphine Degréc, Antonia Lepidac, Antonella Putignanoc, Nathalie Boonc, Thierry Gustotc, Eric Trépoc, Christophe Morenoc
aCUH Erasme, Anderlecht, Belgium. b. cCUB Erasme, Anderlecht, Belgium
Abstract
Background
Patients with Nonalcoholic Fatty Liver Disease (NAFLD) have a greater risk of hepatic decompensation and a higher overall mortality rate than the general population. Risk factors associated with these complications and mortality are not well established.
Method
We conducted a single-center retrospective study including 228 patients with biopsy proven NAFLD, performed at Erasme Hospital in Belgium between 2009 and 2019. The main inclusion criteria were: ≥18 years old, biopsy-proven NAFLD (≥5% macrovesicular steatosis); exclusion criteria were: other causes of chronic liver diseases, excessive alcohol consumption (>20 g of alcohol/day for women and >30 g/day for men). We studied the incidence of liver-related events (hepatocellular carcinoma, clinical apparent ascites, hepatic encephalopathy, variceal hemorrhage) and their associated risk factors using Fine and Gray competing risk model. Risk factors associated with mortality were studied using COX regression.
Results
A total of 228 patients, 48% men and 52% women, with a median age of 63 years were included. Patients were followed for a median of 2,7 years. 36% of patients had a NAS (NAFLD Activity Score) 1–2, 42% had a NAS 3–4 and 22% had a NAS ≥5 at baseline. Cardiovascular events occurred in 9,57% of the patients during the study period (30% myocardial infarction, 30% stroke and 30% acute hearth failure). The main causes of mortality were cardiovascular events (25%) and infections (11%). Liver-related events increased with fibrosis stage (2,3% at 10 years for F0-F2 vs 17,5% at 10 years for F3-F4). It should be noted that all the patients with a liver-related event were diabetic. In the multi-state model, only fibrosis stage F3-F4 is a significant risk factor associated with LRE (HR = 6.95, 95% CI [1.45–33.2], p = 0.015). Risk factors associated with mortality in the multi-state model were: albumin (HR = 0.81, 95% CI [0.83–0.91], p < 0.001), GGT (HR = 1.01, 95% CI [1.00–1.01], p < 0.001), HDL-cholesterol (HR = 1.04, 95% CI [1.01–1.06], p = 0.003), ALP (HR = 0.98, 95% CI [0.97–1.00], p = 0.017).
Conclusion
In this cohort of biopsy-proven NAFLD patients, we have confirmed that the first cause of death in NAFLD is related to cardiovascular events. Advanced fibrosis and cirrhosis are the main risk factors of liver-related events. These results also highlight the importance of systematic cardiovascular screening in this population and identify the target population for a follow-up by the liver specialist.
Abstract ID: 37
On paraneoplastic cushing in prostatic neuro-endocrine carcinoma: a case report
Denis Gosselin
Jolimont, La Louvière, Belgium
Abstract
Background:
Cushing syndrome associated with neuro-endocrine carcinoma of prostate is a rare and difficult diagnosis cause of paraneoplastic syndrome. This is partly due to the rarity of neuroendocrine prostate cancer (less than 1% of prostate cancers) and that the extra-pulmonary location of neuroendocrine tumours is less known. This can lead to a delay in diagnosis.
Case presentation:
A 58-year-old man was admitted for sudden muscle weakness in the context of an infection with Sars-cov2. The systematic history did not highlight any other complaint. His physical examination revealed swollen legs with godet sign and symmetrical proximal strength deficit. The rest of the clinical examination was unremarkable. The patient is known for a total radical prostatectomy in the context of a neuro-endocrine carcinoma with small cells of the prostate with multiple metastasis. His chronic treatment consisted of alizapride, métoclopramide and lormétazépam. Initial blood testing revealed an anemia with lymphopenia and eosinopenia, hypokaliemia (2.3 mmol/l), hypo-proteinemia, high level of LDH. CRP and creatinine were within standards.
In the light of his muscle weakness, severe hypokaliemia refractory to IV KCl high dose and oncological history, a cushing syndrome was suspected. Which was confirmed with cortisoluria (31,272.1 nmol/24 h) and a high level of serum ACTH (582 pg/ml). An ACTH adenoma was reasonably excluded by a pituitary-MRI.
With all of these elements, we conclude at a paraneoplasic cushing syndrome arising of a recidivism of his prostatic neuro-endocrine carcinoma.
Discussion:
In a neoplasic contexte with none pituitary adenoma, the ACTH-dependent cushing syndrome is due to an ectopic secretion of ACTH (rarely CRH) in a context of paraneoplasic syndrome.
Patients with suggestive signs or symptoms should alert us as complications of cushing syndrome are fatal by an increased cardiovascular risk, a prothrombophilic state, suicidal ideation and immunosupression. In our patient’s case, the clinic was poor because of the rapidity with which the pathology sets in, and the blood test was the most evocative. It can also be the point of call for the fortuitous discovery of a neoplasia of the neuro-endocrine or carcinoid type. We rely on cortisoluria or the short dexamethasone test and the ACTH to suspect the diagnosis. If there is any doubt about the neoplastic origin or in the absence of a history, an octreotide scan can be performed to locate the ectopic secretion of ACTH.
Cancer treatment remains the main therapy. With regard to the actual treatment of the cushing syndrome, there is debate. We can inhibit steroid production (ketoconazole, metyrapone, etomidate, …) or make bilateral adrenalectomy (surgery, mitotane).
Conclusion:
The paraneoplastic cushing syndrome may be difficult in early state with just some aspecific abnomalies at the blood testing. In our case, the patient initially had only hypokalemia associated with proximal muscle weakness. We must keep in mind that Cushing’s syndrome is a fatal disease. Increased cardiovascular risk, hypertension and prothrombotic state are the major causes of death associated with cushing syndrome. Hypoproteinemia leading to a decrease in immune defences leads to severe infections and even septic shock.
Abstract ID: 38
The triad of Legionnaires’ disease: a case report
Celien Claes, Marie Schouterden, Liesbet Henckaerts
University Hospitals Leuven, Leuven, Belgium
Abstract
Legionnaires’ disease is an atypical and severe pneumonia caused by environmental gram-negative bacteria called Legionella species. Typical symptoms include fever, cough and shortness of breath. Moreover, Legionnaires’ disease can present with extrapulmonary manifestations including gastro-intestinal symptoms and rhabdomyolysis resulting in renal failure. In this case report, we describe a 43-year-old female patient with a history of HIV, latent tuberculosis and a recent covid-infection who presented with shortness of breath, chest pain, myalgias and diarrhea for 3 days. She was admitted with a left lower lobe pneumonia and acute kidney injury, initially consigned to a prerenal cause. She also had abnormal liver function tests; however, a liver ultrasound showed no dilated bile ducts or focal lesions. Empirical treatment with Amoxicillin/clavulanic acid was started at the emergency ward, besides supportive therapy with IV fluids and antipyretics. At admission, she required 2 liters of supplemental oxygen via nasal cannula and was hemodynamically stable. On day 2 of hospitalization, our patient developed oliguria. Laboratory tests revealed a serum creatinine of 6.08 mg/dL, a C-reactive protein of 528 mg/L and creatinine kinase of128100U/L. Urine analyses showed proteinuria and hematuria. The urinary Legionella Antigen test was positive. Clarithromycin was added to the treatment and aggressive IV hydration was started with crystalloids, besides the administration of sodium bicarbonate to alkalize the urine. The following days the patient’s general condition improved rapidly. Eventually she could be discharged 10 days after her admission, completely recovered. This case report outlines the importance for clinicians to early recognize this rare but severe triad of Legionnaires’ disease, with pneumonia, rhabdomyolysis and renal failure to reduce morbidity and mortality.
Abstract ID: 39
Pulmonary artery stenosis and Fontan-associated liver disease are long-term complications of the Fontan-palliation procedure. A case report.
Abdoul Aziz Karenzi, Agnes Pasquet
Division of Cardiology, Department of Cardiovascular disease, Cliniques Saint-Luc UCL, Brussels, Belgium
Abstract
A 57-year-old man of Caucasian origin, known to have single-ventricle congenital heart disease, had been admitted to our hospital due to refractory ascites. He was born with L-Transposition of Great Arteries (L-TGA), pulmonary valve stenosis, and a double inlet left ventricle (DILV). His first palliative surgery was during the neonatal period, when a left Blalock-Thomas-Taussig shunt was performed. At 4 years old, he underwent a bi-direction cavo-pulmonary anastomosis (Glenn shunt), followed by a hemi-Fontan procedure in which the superior vena cava was connected to the right pulmonary artery, via Rygg’s valved conduit. The tricuspid valve was closed, the patent foramen ovale was closed, and the Blalock shunt was excluded. At 7 years old, he had re-do Fontan procedure due to postoperative graft thrombosis and tricuspid residual leakage. At 36 years old, pacemaker implantation (VVIR) was performed after a third-degree atrioventricular block diagnosis. He then developed typical atrial flutter at the age of 48. Issues began when he was admitted to the emergency room for severe asthenia. The assessment showed third-degree atrioventricular block recurrency due to pacemaker lead fracture. Epicardial ventricular lead placement via left thoracotomy was performed. Unfortunately, atrial lead placement was not possible due to extremely dilated mediastinal veins and extensive thoracic post-surgical adhesions. Post-operative surveillance was marked by ascites accumulation and was managed by abdominal paracentesis. Three months later, he was readmitted to the emergency department due to diffuse abdominal pain caused by a strangulated umbilical hernia favored by recurrent ascites. During the umbilical hernia surgery, the surgeon noticed a considerable volume of ascites. Assessment of the ascites etiology showed no evidence of prolonged alcoholism, nor viral hepatitis, nor autoimmune hepatitis, nor any other prevalent etiology of liver cirrhosis. He was discharged on diuretics after his ascites was determined to be secondary to the ‘Fontan evolution’. Five months later, and despite taking significant doses of diuretics, he was hospitalized at our center with refractory ascites. Diagnostic cardiac catheterization was performed under local anesthesia. Fontan angiography [] demonstrated severe stenosis between right atrium (RA) and the origin of the left pulmonary artery (LPA). Baseline mean right atrium pressure and left pulmonary artery pressure were 26 mmHg and 16 mmHg, respectively.
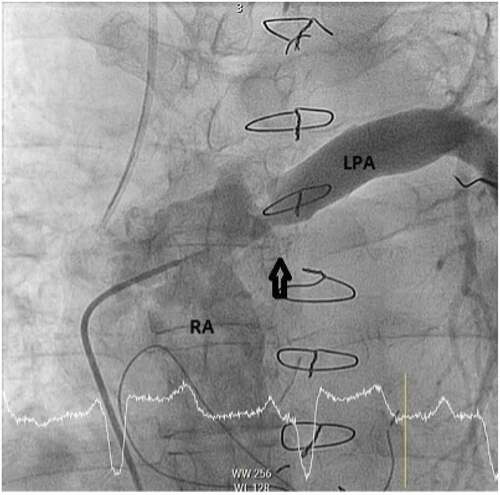
Trans-stenotic gradient pressure was 10 mmHg. What would be the most appropriate management for you at this step. After decision was made to treat the lesion percutaneously. Cardiac catheterization was performed under general anaesthesia. A 6 F sheath was placed in the right femoral vein. The stenosis between right atrium and left pulmonary artery was crossed using specific catheters. Pre-dilatation of the lesion was done using a 20 mm balloon [], a covered Stent was then deployed.
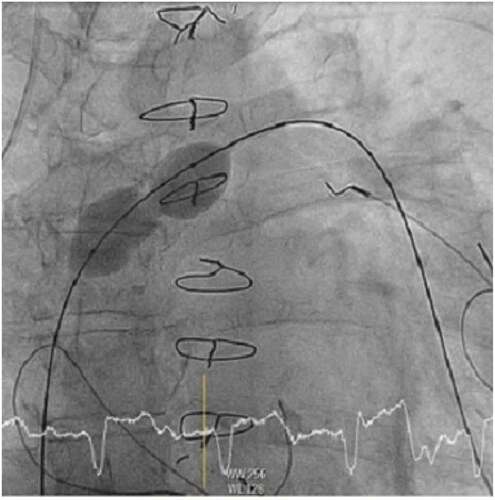
Distal flow was found to be satisfactory after stent deployment [], with improved hemodynamic measures; the pressures in the right atrium and left pulmonary artery were 22 mmHg and 22 mmHg, respectively.

At discharge, ascites and lower limbs oedema had disappeared, with a stable low dose of diuretics indicating clinical improvement. Iterative ascites punctures were scheduled in his local hospital.
Abstract ID: 40
Could biological factors predict adverse outcomes in a well-defined population referred for a coronary angiogram? Follow-up of 188 patients from a Coronary Angiography Prospective Trial.
Abdoul Aziz Karenzi
Division of Cardiology. Cliniques Universitaires Saint-Luc, Brussels, Belgium
Abstract
Background/Introduction
The World Health Organization (WHO) has identified cardiovascular disease as the leading cause of death in the world. An estimated 18 million people have died of CVD in 2019, which accounts for 32% of all worldwide deaths. Of these deaths, the overwhelming majority (85%) are due to ischemic heart disease (IHD) or stroke.
Ischemic heart disease is a chronic, progressive disease. It may remain in a quiescent state for some time, but most patients will eventually experience flare-ups, such as acute coronary syndrome or death. This is the concept of residual risk. This progression of the disease persists despite optimal management of cardiovascular risk factors, complete revascularization or any other treatment that is considered up to date.
Purpose
The objective of this single-center retrospective study was to identify biological prognostic factors for adverse outcomes, such as all-cause mortality and the occurrence of acute coronary syndrome, in a clinically and biologically well-characterized cohort whose coronary anatomy is known.
Methods
Patients investigated in this study were initially recruited in the prospective ACCTHEROMA Trial. The study population included 188 patients who underwent coronary angiography for various purposes. Blood samples (platelet isolation, protein extraction) and analyses were performed. Investigators performed routine and more specific biological analyses. They examined oxidized LDL and PCSK9 proteins, markers of platelet function (TRAP test), intra-platelet lipid metabolism (phosphorylated-Acetyl-CoA Carboxylase), and markers of coagulation activation (D-dimers, thrombin-antithrombin complex, endogenous thrombin potential, and fibrinogen). The follow-up was done over a median of 6.25 years. The information gathered was primarily for the following events: death, acute coronary syndrome episodes, and coronary revascularization. We then performed a principal component analysis of thrombotic and inflammatory specific biological factors according to the accomposit outcome of death and myocardial infarction
Results
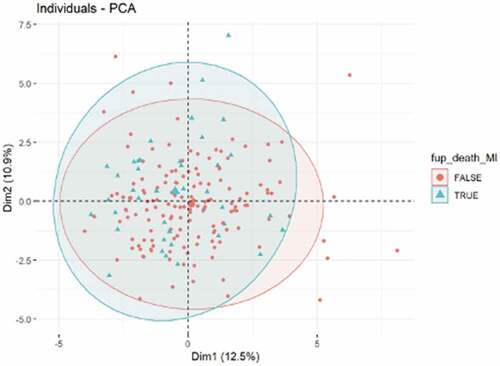
Principal component analysis of biological factors according to a composite outcome of death and myocardial infarction during follow-up shows no discrimination between patients with a favourable or unfavourable outcome.
Conclusion
In a well-characterized population referred for coronary angiography, the principal component analysis of biological factors did not differentiate patients who experienced unfavorable outcomes from those who experienced favorable outcomes. These specific analyses did not allow us to estimate residual risk.
Abstract ID: 41
To treat or not to treat acne, that was the question
Flavien Randazzoa, Abeline Kapuczinskib, Nathalie Demeulenaereb, Marc Léonb, Evelyne Berlinginc, Camélia Rossid
aAmbroise Paré – infectious disease department, Mons, Belgium; bAmbroise Paré – rheumatology department, Mons, Belgium; cAmbroise Paré – dermatology department, Mons, Belgium; dAmbroise Paré – infectious disease department, Mons, Belgium
Abstract
Background
Minocycline is a synthetic tetracycline-derived antibiotic which is widely used for acne vulgaris. Chronic exposure to minocycline can be associated with the development of autoimmune disorders including drug-induced lupus, autoimmune hepatitis and vasculitis. Minocycline-induced vasculitis most commonly present with skin lesions mimicking livedo reticularis and/or subcutaneous nodules that resemble cutaneous polyarteritis nodosa.
Case Report
A 19-year-old male came to the Rheumatology Department outpatient clinic for arthralgia (affecting wrists, elbows and ankles), weight loss and subcutaneous nodules on his legs, arms and neck lasting for a few days with functional impairment, waking up at night and joints morning stiffness. Medical history was unremarkable. Ultrasound of the wrists and hands showed a radio-ulnar tenosynovitis without erosions. Blood test revealed moderate inflammatory syndrome with increased sedimentation rate (31 mm/h), C-Reactive Protein (CRP) level (39 mg/l) and positive anti-nuclear factors (FAN) 1:320 titer without identification. Both rheumatoid factor (RF) and anti-CCP antibodies were tested negative. Corticoids were started with fast tapering dosage. Three days after tapering corticoids, the patient presented to the Emergency Department because of important functional impairment, arthralgia and night sweats. He was then admitted for further investigations. CRP level was higher (185 mg/l), infectious serologies were negative, including screening for hepatitis B, C and HIV. Blood cultures were all negative. Screening for angiotensin-converting enzyme inhibitor (ACE), HLA B27 and ANCA were also negative. Thoracic and abdominal CT scan were normal. CT angiography excluded arteritis. After repeated questioning, patient reported to take minocycline since a month to treat his acne. Minocycline was stopped and methylprednisolone was started at 1 mg/kg/day with rapid clinical improvement and decrease of CRP level. Skin biopsy performed before starting high dose corticoids was suggestive of vasculitis with inflammatory involvement and subsequent necrosis of the surrounding adipose tissue.
Discussion and conclusion
Minocycline is associated with the development of various autoimmune syndrome. Improvement of the symptoms generally occurs after stopping the medication, but some patients need non-steroid anti-inflammatory drug or low dose steroid. The causal link between minocycline treatment and the symptoms developed by the patient cannot be excluded. The use of non – minocycline tetracyclines for the treatment of acnes vulgaris should be preferred. This case highlights the importance of considering minocycline-induced vasculitis especially in young patients presenting auto-immune manifestations.
Abstract ID: 42
Repeating a renal biopsy: indication in acute kidney failure with a patient suffering from an unusual association between Sharp’s syndrome and Berger’s disease.
Thibault Gennarta, Fozi Moussab, Sophie Lefèbvrec, Yves Pottiezc
aUCL, Bruxelles, Belgium; bCHU Tivoli, La Louvière, Belgium; cCHMouscron, Mouscron, Belgium
Abstract
Background:
Kidney injury in mixed connective tissue disease can be severe in a minority of cases. IgA nephropathy is part of the differential diagnosis. We report a case showing this unusual association and the implications in care. The risk factors for this association are unknown. An incidental association cannot be excluded.
Clinical case:
A 28-year-old Belgian patient with mixed connective tissue disease and IgA nephropathy with normal renal function. He is not taking hydroxychloroquine due to intolerance (unspecified).
The patient was admitted to the nephrology department for macroscopic haematuria, proteinuria at 5 g/24 h, AKIN stage 1 acute kidney failure and uncontrolled hypertension on ramipril. The CRP has increased to 97 mg/L. The patient had arthralgias and headaches. Neither a frank clinical infection nor a PET-CT scan showed any evidence of infection. Abdominal CT scan showed splenomegaly with centimetric lymph nodes in front of the left renal artery. Treatment with macrolides for suspected atypical pneumonia, based on a discrete cough and equivocal chlamydia pneumoniae serology, was started. Bacterial and viral tests (HCV, HBV, HIV, hantavirus, tuberculosis …) were negative. Antibiotic therapy did not improve the clinical picture or the renal function. Autoimmune serologies (FAN, ANCA, cryoglobulins, complement) were negative. Ferritin and triglycerides were within normal limits. A bicytopenia (microcytic anaemia and low-grade thrombopenia) was also noted. A renal biopsy was proposed to rule out the possibility that the renal involvement was caused by the connectivitis (typically extra-membranous glomerulonephritis) or due to IgA nephropathy or other.
Renal biopsy showed crescentic glomerulonephritis in ±50% of glomeruli, with mesangial IgA deposits. Treatment with methylprednisolone in decreasing doses, combined with IV cyclophosphamide, was started with rapid resolution of the inflammatory syndrome and fever, normalisation of renal function and a decrease in proteinuria to 1.39 g/g and haematuria, and normalisation of thrombocytopenia.
Literature key points:
The absence of severe kidney involvement is a characteristic of mixed connective tissue disease, although renal involvement, mostly subclinical and with a good prognosis, is found in up to ±20–25% of patients: membranous involvement is the most common, followed by mesangial glomerulonephritis. Other types of involvements are possible: proliferative glomerulonephritis, scleroderma pattern, ANCA glomerulonephritis association, Castleman’s disease, tubulo-interstitial nephritis, thrombotic thrombocytopenic purpura, glomerulonephritis (mostly ISN/RPS 2003 class II mesangial GN), collapsing nephropathy.
Rarely, patients develop acute kidney failure in IgA nephropathy, secondary to crescentic nephropathy or haematuria causing tubular obstruction and/or red cell injury (acute tubular necrosis). If it is a shift to crescentic glomerulonephritis, immediate treatment is required.
Conclusion:
Do not hesitate to repeat a renal biopsy to specify the mechanism in a patient suffering from two autoimmune diseases with (sub)acute kidney involvement. It changes the treatment and therefore the prognosis.
Abstract ID: 43
The nephrologist facing end-stage kidney disease in underprivileged populations: a 10-year observational retrospective study
Lucas Jacobs, Maria Mesquita, Frederic Collart, Joelle Nortier
CHU Brugmann, Brussels, Belgium
Abstract
Introduction
Belgium has a multicultural landscape. Our hospital and its dialysis unit is one of the largest centers in Brussels, entirely public-funded, partnering ‘Fedasil’ and ‘Médecins du Monde’, often welcoming the most underprivileged population. We studied our epidemiology and patient survival over the last 10 years.
Material and Method
We conducted a 10-year observational retrospective study, on 321 incident patients (pts) starting dialysis from the 1st of January 2010 to the 31st of December 2019 using the ‘Groupement des Néphrologues Francophones de Belgique’ end stage renal disease database. Pts were divided into four groups: Western Europe (Belgium, France, Italy, Spain), Eastern Europe (Armenia, Poland, Roumania, Ukraine), North-Africa (Morocco, Algeria), sub-Saharan Africa (DR Congo, Rwanda, Cameroon). Pts were followed from day 1 after the initiation of dialysis until death or censoring (at time of transplantation, lost to follow-up or transfer). Incident dialysis modality represents the modality at start or after a brief period of urgent-dialysis. We studied basic pts characteristics, primary renal diseases (prd), pre-dialysis follow-up duration, comorbidities (Charlson index), survival, and time to transplantation.
Results
Basal characteristics. Our pts population is made of 33% Western European (WE), 22% Eastern European (EE), 24% North African (NA), 21% sub-Saharan Africans (SSA). Notably, EE and SSA are less comorbid than WE and NA. Type 2 diabetes represents 50% of prd in NA. Renal vascular disease represents 55% of prd in WE. In EE and SSA, prd are more diverse. WE have a longer median pre-dialysis follow-up (7 months, IQR: 29.7) than EE, NA, and SSA (each <1 months, IQR: 8–14). At start of dialysis, WE are roughly 15 years older than EE and SSA, and 7 years older than NA.
Practice patterns. Our center provides greater access to PD in particular for EE and SSA (33%) but also for WE and NA (25%).
Survival analysis. Univariate analysis shows a significant correlation between survival and geographic origin; significant variables being age, comorbidity, and geographic origin. However, multivariate analysis demonstrates that survival solely depends on age and comorbidity. SSA and EE have a double median survival time (SSA: 1121 months, IQR: 1314; EE: 1189 months, IQR: 1615), than NA and WE (NA: 698 months, IQR: 690; WE: 639 months, IQR: 1167).
Transplantation access. Time to transplantation is double for EE and SSA (4 years) compared to WE and NA. However, SSA have the highest transplantation rate with 30% (15–20% in other groups). Variables influencing transplantation are age and pre-dialysis follow-up
Discussion and Conclusion
We highlight the high prevalence of PD in SSA and EE (many asylum seekers), showing that the lack of home-facilities, and language barriers do not prevent higher PD use. Pts from NA, EE, and SSA are generally started more urgently when WE have a longer pre-dialysis follow-up. Geographic origin does not influence survival. SSA and EE immigrants have a longer (administrative) delay before transplantation. Nevertheless, given their young age and less comorbidities, SSA catch up with WE and NA and are on average more transplanted while EE remain similar.
Abstract ID: 44
Peritoneal carcinomatosis with malignant small bowel obstruction: an atypical presentation of breast cancer
Vincenzo Delsinne, Victor Chua, Julien Compere, Yannick Gombeir
EpiCURA, Hornu, Belgium
Abstract
Background
Breast cancer (BC) is the most common malignancy among women, but only 6% of newly diagnosed patients encounter distant metastasis at diagnosis. Invasive lobular carcinoma (ILC) comprises 4–15% of all malignant neoplasms of the breast. The most common metastatic sites of ILC are bones, gastrointestinal tract, uterus and ovaries. Small bowel obstruction is a rare initial presentation of breast cancer with only a few cases reported in the literature. We report a case of ILC presenting as bowel obstruction.
Case presentation
A 64-year-old woman presented to the emergency clinic with abdominal pain. She had a 1-week history of nausea, vomiting and constipation. Physical examination revealed diffuse abdominal tenderness and hirsutism. Abdominal CT scan revealed a small bowel obstruction and a 5-cm mass in the left breast. Laparotomy revealed a small fibrotic intestinal segment and peritoneal nodules. A small bowel resection and biopsies were performed. Laboratory tests showed a CA15.3 of 480 kU/L (0.0–35.0). Histopathological analysis tested positive for CK AE1+ AE3, and negative for CD45, evoking a carcinoma. Tumoral cells were present at the serosa with perineural and lymphovascular invasion. Immunostaining showed E R(8/8), PgR(8/8), and HER2(1+), characterizing the lesions as bowel metastasis of breast cancer with peritoneal carcinomatosis. Breast biopsy confirmed an invasive lobular carcinoma. FDG-PET also revealed diffuse bone uptake. A treatment with Letrozole and Palbociclib was initiated. The outcome was favorable at 4 months.
Discussion
According to the last exhaustive literature reviews on BC, the most common gastrointestinal metastatic sites are the large bowel and small bowel (>95% of cases), with rare case reports of lesions in stomach, anus and peritoneum. The latter is mostly due to ductal carcinomas (>75%), unlike our case. Median age of patients was 61-years with female predominance, with a median time of evidence of intestinal involvement 7 years after the diagnosis of breast cancer. The first clinical presentation was bowel obstruction (40–50% of cases), followed by gastrointestinal bleedings. The main problem is to distinguish primary and secondary gastrointestinal tumors to provide the optimal care. As for our patient, reviews show a majority of lobular carcinoma (50–60%) at histopathological findings; this could be related to a particular tropism of lobular cells. While the median survival estimated from the available data was around 12 months, the median survival of patients with peritoneal disease was 1.5 months. In a large autopsy series [Citation1] of patients who died of breast cancer, intestinal metastasis presented an incidence of 16.4% and only 20% of these patients complained of having symptoms. This supposes a lot of under-diagnosis.
Conclusions
Intestinal metastasis should be considered in the differential diagnosis of patients with intestinal symptoms and history of breast cancer, especially with a histology of lobular carcinoma. Treatment strategies include palliative surgery, chemotherapy and hormone therapy. The prognosis of patients is significantly reduced in comparison with other metastatic sites.
Reference
- Asch, M.J., Wiedel, P.D., Habif, D.V. (1968). Gastrointestinal metastases from carcinoma of the breast. Autopsy study and 18 cases requiring operative intervention. Arch Surg;96:840–843.
Abstract ID: 45
Isolated oral histoplasmosis
Vincenzo Delsinne, Victor Chua, Vic Arendt, Thérèse Staub
CHL, Luxembourg, Luxembourg
Abstract
Background
Histoplasmosis is a rare endemic systemic mycosis, usually asymptomatic. Its presentation is characterized by pulmonary disease, mediastinitis, pericarditis and rheumatologic manifestations. Patients with advanced AIDS usually develop progressive disseminated histoplasmosis. Localized histoplasmosis in HIV patients occurs in only 8,3% of reported cases in Europe and are mostly skin-related.[Citation1] Head and neck involvement generally occurs as a part of the disseminated illness. To our knowledge, there are only four reported cases of isolated oral histoplasmosis in HIV-infected patient. We present a new atypical case of this disease.
Case presentation
A 40-year-old female, living in Luxembourg for 7 years and returning once a year in her country of origin Cameroon, presented to her dentist for mouth pain. Clinical examination showed an irregularly shaped ulcer of the left hard and soft palate and left maxillary gingiva. Biopsy of the lesion was performed. Serologic studies for exposure to HIV were positive. Her CD4 cell count was 27 cells/µl.
Results
Biopsy shows sheets of histiocytes containing small intracellular yeasts. PCR identified Histoplasma capsulatum. The patient was initially treated with amphotericin B. After identification of Histoplasma capsulatum and considering the lack of compliance with oral itraconazole, treatment was maintained with amphotericin B once a week, for 6 months. The oral lesion and the pain disappeared in a few weeks.
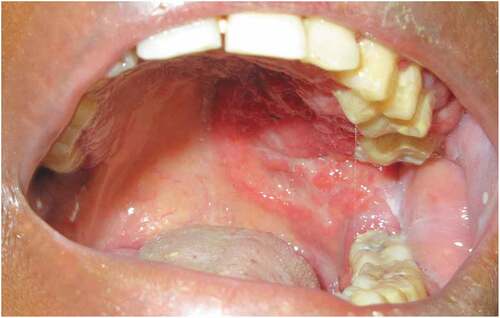
Conclusions
Histoplasmosis should be included in the differential diagnosis of oral ulcers. Infectious causes can be bacterial (syphilis, atypical mycobacterium species, Helicobacter pylori), viral (HSV, VZV, CMV, VIH-linked, Coxsackie …), mycotic (candida, cryptococcosis, mucormycosis, aspergillosis, penicilliosis, histoplasmosis …) or parasitic (leishmaniosis). Oral histoplasmosis is more associated with immunocompromised state and with disseminated illness. Biopsy is the gold standard for this rare diagnosis.
Reference
- Antinori, S., Magni, C., Nebuloni, M., Parravicini, C., Corbellino, M., Sollima, S., Galimberti, L., Ridolfo, A. L., Wheat, L. J.(2006). Histoplasmosis Among Human Immunodeficiency Virus-Infected People in Europe. Report of 4 Cases and Review of the Literature. Medicine (Baltimore);85(1):22–36.
Abstract ID: 47
Atypical presentation of Dunbar syndrome: about a case
Vincenzo Delsinne, Victor Chua
CHMouscron, Mouscron, Belgium
Abstract
BACKGROUND
Dunbar syndrome or median arcuate ligament syndrome (MALS) is a rare pathology typically seen in young and thin adult females, with the following triad: postprandial pain, weight loss and epigastric bruit. The pathophysiology of this syndrome would involve both ischemic and neuropathic mechanisms. During expiration, an abnormal position of the arcuate ligament could lead to the compression of the celiac axis.
We report a case of Dunbar syndrome, with non-specific symptoms and no typical triad, showing the importance of vascular imaging in this unrecognized disease.
CASE PRESENTATION
A 52-year-old female presents to the gastroenterology clinic with continuous diffuse abdominal pain, nausea, and weight loss of 16 kg within the last 2 years. The patient has no medical history except hypothyroidism. The clinical examination only shows an epigastric sensitivity. Exhaustive laboratory blood, stool and urine tests were unremarkable. Abdominal echography and CT scan without contrast, gastroscopy, colonoscopy, echo-endoscopy and gastric emptying scintigraphy were normal. The patient underwent a contrast-enhanced abdominal CT scan, which showed a focal stenosis of the celiac artery with normal mesenteric arteries. Doppler echography demonstrated an increasing peak flow velocity on expiration. Aortic arteriography confirmed an extrinsic compression by the median arcuate ligament. Surgical ligament release by laparoscopy was performed. The outcome of our patient was favorable with post-operative total symptoms relief.
DISCUSSION
An abnormal position of the celiac artery or the median arcuate ligament is found in about 10% to 24% of the general population. However, only a small proportion of people show symptoms of MALS. With an incidence of one per 50,000, Dunbar syndrome is characterized by the triad: post-prandial pain, weight loss and abdominal bruit. [Citation1] This triad is, as for our patient, usually incomplete. Indeed, weight loss is found in only 50% of cases and abdominal pain is not post-prandial in 20% of cases. Abdominal pain can occur during effort, vary with position, be permanent or intermittent. [Citation2] Nausea is described in 10% of cases and abdominal murmur in only 30%. As for our patient, immediate post-surgery relief of symptoms is described in 78 to 96% of cases. [Citation3]
CONCLUSION
This presentation shows the common misdiagnosis of MALS due to its nonspecific symptoms and the lack of awareness of this syndrome among physicians. It should be included in the differential diagnosis of chronic abdominal pain, especially in young and thin adult females. This case also highlights the importance of vascular and inspiratory-expiratory imaging, when the basic diagnostic workup remains unresolved. Treatment involves surgical release of the median arcuate ligament. Revascularization of the celiac artery can be considered if symptoms persist.
References
- Kakar et al.(2022). Severe Post-prandial Pain: A Case Report. Cureus; 14(2): e22448.
- Reilly et al. (1985). Late results following operative repair for celiac artery compression syndrome. J Vasc Surg; 2(1):79–91.
- Jimenez et al.(2012). Open and laparoscopic treatment of median arcuate ligament syndrome. J Vasc Surg; 56(3):869–73. DOI: 10.1016/j.jvs.2012.04.057.
Abstract ID: 48
One pneumonia may hide another – a case report in a lung transplant recipient
Laurence Bampsa, Lorena van den Bogaarta, Mathias Van Singera, Angela Koutsokeraa, Alessio Casutta, Christophe Abellana, Gregory Berrab, Thorsten Kruegera, Celine Forstera, Fabio De Carvalho Pavaoa, Leonie Badertschera, Jean-Luc Pagania, Michel Gonzaleza, Oriol Manuela
aCentre Hospitalier Universitaire Vaudois, Lausanne, Switzerland; bHôpitaux Universitaires de Genève, Genève, Switzerland
Abstract
CASE:
We report here the case of a 24-year-old female with a history of liver transplantation 7 years prior for a congenital biliary atresia, with a secondary severe portopulmonary hypertension despite medical treatment leading to a bipulmonary transplantation.
On day 3 after lung transplantation, she was diagnosed with a donor-derived polymicrobial pneumonia with the samples collected on the donor lung fragments and bronchial aspiration showing Klebsiella oxytoca, Hafnia alvei and Staphylococcus aureus. She was treated with cefepime 2 g tid according to the antimicrobial susceptibility testing. On day 6, her clinical condition worsened with high fever, increasing PaO2/FiO2 ratio, need for ventral decubitus and vasopressor support. The thoracic CT scan showed bilateral basal condensations and ground-glass opacities. Bronchoscopy showed abundant purulent secretions. The treatment was empirically broadened to meropenem 2 g tid. The bacterial and fungal cultures performed on bronchial aspiration were negative, as well as the molecular analyses (including a broad respiratory viral PCR panel and PCR for Chlamydia pneumoniae, Mycoplasma pneumoniae, Aspergillus fumigatus). Mycoplasma hominis and Ureaplasma urealyticum were detected by PCR on the respiratory samples, with, respectively, 6,000,000 DNA copies/ml and 6,810,900 DNA copies/ml. The patient was treated with a combination of doxycyclin and levofloxacin for 4 weeks, and the outcome was favorable, allowing extubation by day 12. Her blood ammonia level at diagnosis was normal. Subsequent bronchial aspirations showed a progressive decrease then negativization of DNA copies of both pathogens. A PCR was performed on the donor samples and was negative, allowing to exclude a donor-derived infection.
DISCUSSION:
Mollicutes like U. urealyticum and M. hominis infections in lung transplant recipients can lead to hyperammonemia syndrome (HS), a rare but life-threatening complication occurring during the first weeks following transplantation, in the absence of any hepatic dysfunction. They are mostly donor-acquired infections. Hyperammonemia syndrome is primarily described with U. urealyticum; M. hominis is mainly associated with wound infections after thoracic surgery but one case of a disseminated infection with hyperammonemia in a lung transplant recipient has been reported. Both pathogens may cause infections even if in the absence of HS. Antimicrobial susceptibility testing is usually not available at the time of diagnosis, but variable resistance rates have been described for both organisms (resistance to doxycyclin and macrolides for U. urealyticum, resistance to macrolides and quinolones for M. hominis). For this reason, a dual antimicrobial therapy might be warranted.
CONCLUSION AND PERSPECTIVES:
Ureaplasma urealyticum and Mycoplasma hominis are involved in severe complications in lung transplant recipients, associated with high morbidity and even mortality. Clinician suspicion should arise in patients presenting with unexplained pulmonary infiltrates or neurologic complications following transplantation, and a confirmed infection should be aggressively treated.
Further studies are needed to determine if universal donor screening or antimicrobial prophylaxis targeting these pathogens should be recommended, according to local epidemiology and to potential risk factors of the organ donor of carrying U. urealyticum in their lower respiratory tract (young, male, sexually active donors having an aspiration event prior to death).
Abstract ID: 49
Periarteritis nodosa unveiling myelodysplastic syndrome with multilineage dysplasia
Louis Wolffa, Frederic Vandergheynstb, Athanassios Kolivrasc, Isabelle Nubourgha
aDepartment of Internal Medicine, Saint-Pierre University Hospital, Université Libre de Bruxelles, Brussels, Belgium. bDepartment of Internal Medicine, CUB Hôpital Erasme, Université Libre de Bruxelles, Brussels, Belgium. cDepartment of Dermatology, Saint-Pierre University Hospital, Université Libre de Bruxelles, Brussels, Belgium
Abstract
A 68-year-old male patient with known ischemic cardiopathy with preserved ejection fraction, transient ischemic attack and hypercholesterolemia was treated with aspirine, atorvastatine, bisoprolol and venlafaxine. He presented with fatigue, nocturnal sudation and loss of more than 10% of his weight over the previous month. Physical examination revealed a macular erythematous lesion of the right eyelid. Blood sample demonstrated a normocytic normochromic non-regenerative anemia at 9 g/dl, neutropenia at 1.1 G/l, CRP at 60 mg/l and natremia at 130 mmol/l. Initial work up including the search for infections and deficiencies (thyroid, B9, B12, copper and zinc) and thoraco-abdominal computed tomography (CT) were within normal range. A bone marrow biopsy demonstrated hypoplasia. Venlafaxine, which was initiated 6 weeks earlier, was discontinued and neutropenia resolved. Six months later, he presented the same symptoms. We repeated the same work up except the bone marrow biopsy and also performed a PET-CT. Everything remained unremarkable. Due to dysuria during hospitalization, biopsy of a prostatic lesion revealed by magnetic resonance showed no sign of malignancy. Three months later, he complained of vision loss and a retinal artery occlusion was diagnosed. A temporal artery biopsy was unremarkable. A year later, he suffered another similar exacerbation of symptoms added with abdominal pain and diarrhea. Initial blood sample revealed inflammation, anemia, neutropenia and a thrombopenia. Work up included thoraco-abdominal CT, exclusion of infections (repeated urine and blood cultures, EBV, CMV, hepatitis, syphilis, Q fever, cryptococcus antigen) and immunological tests (protein electrophoresis, C3, C4, anti-nuclear antibodies, anti-neutrophil cytoplasmic antibodies, anti-cyclic citrullinated peptide, rheumatoid factor and IgG4) which were unremarkable. Coloscopy revealed colitis without signs of amyloidosis. Empirical antibiotics did not improve symptoms. Repeated bone marrow biopsy demonstrated red blood cell dysplasia and next generation sequencing was pending. He then developed testicular pain without local inflammation. Beta HCG and echography were within normal range. He presented erythematous papules and nodules on his lower limbs and face. Skin biopsy demonstrated medium-sized arteritis with fibrinoid necrosis within the vessel wall. IgA, IgG, IgM, C3 and fibrinogen were absent on direct immunofluorescence. Repeated immunological work-up remained unremarkable. Bone marrow oncogenomic results later revealed TP53 and ASLX1 mutations. Patient was diagnosed with periarteritis nodosa secondary to myelodysplastic syndrome with multilineage dysplasia. VEXAS (Vacuoles, Enzyme E1, X-linked, Autoinflammatory, Somatic) syndrome was ruled out. Steroids were given with rapid improvement of symptoms. The patient suffered from multiple complications, including intestinal perforation, and unfortunately died a year later.
Abstract ID: 51
Prescribing modalities and efficacy of Canakinumab for the treatment of Autoinflammatory Recurrent Fever Syndromes in Belgium
Jeremiah Nagar
Erasme, Brussels, Belgium
Abstract
1. Introduction
Familial Mediterranean fever (FMF), mevalonate kinase deficiency (MKD) and ‘tumor necrosis factor receptor-associated periodic syndrome’ (TRAPS) are autoinflammatory diseases characterized by recurrent attacks of systemic inflammation including fever and elevated biomarkers, variably associated with skin, joint and serosal involvement. In these diseases, the cytokine interleukin-1β plays a prominent role.
In 2018, the ‘CLUSTER’ study by De Benedetti et al. demonstrated the efficacy of Canakinumab, a monoclonal antibody directed against interleukin-1β, for the control and prevention of attacks in patients with cr-FMF, TRAPS and MKD. The results of this study contributed to the adoption of Canakinumab reimbursement in Belgium.
The aim of the present work is to study the demographic and clinical characteristics of cr-FMF, TRAPS and MKD, as well as to investigate the treatment modalities and efficacy of Canakinumab in Belgium.
2. Material and method
We conducted a retrospective study of 23 patients who received Canakinumab treatment for colchicine-resistant FMF (cr-FMF), TRAPS or MKD prescribed by a physician affiliated with the Erasmus Hospital or the Jessa Ziekenhuis. We collected demographic data, clinical data, biologic and radiographic data, complications and treatment data.
3. Results & Discussion
Disease manifestation
The clinical manifestations were mainly fever, abdominal symptoms and arthralgia during attacks. Disease-specific manifestations were present. However, the symptomatology was not specific resulting in a significant diagnostic delay. Diagnostic delay is important to reduce because it is associated to a high risk of complications, the most severe being AA amyloidosis, and a significant decrease in quality of life. The efficacy of colchicine in the prevention of amyloidosis is well established, but we lack of hindsight to say the same about biological agents. It is thus advisable to continue to give patients a dose of colchicine in parallel with the biological treatment.
Prescribing modalities
The RIZIV reimbursement criteria for the cr-FMF differ slightly from the inclusion criteria of the ‘CLUSTER’ study, but are the same for the TRAPS and MKD.
In our cohort, three patients with cr-FMF received, before starting Canakinumab, treatment with Anakinra, an anti-IL1 with proven efficacy for the treatment of cr-FMF. Anakinra has the advantage of being much cheaper than Canakinumab, but requires a daily injection. No large-scale study has been able to prove the superiority of one anti-IL1 agent over the others. It would thus be interesting to add an Anakinra failure for the reimbursement criteria for Canakinumab, as well as comparing the efficacy of Anakinra and Canakinumab in large-scale studies.
Efficacy
In our cohort, a complete response was found in 77.3% of patients and 18.2% showed a partial response. In cr-FMF, complete efficacy was found in 73.7% of patients, a result statistically comparable to the literature. In TRAPS and MKD, complete response was found in 100% of patients. In this study, 7 patients suffered from mild side effects.
4. Conclusion
Both in terms of clinical manifestations and treatment efficacy, our results confirm the data in the literature. There is still much progress to be made in the management of these diseases, both at the diagnostic and therapeutic levels.
Abstract ID: 52
Rare case of infectious staphylococcus aureus colitis: endoscopic appearance and review of literature
Ihsane Eljaadi, Aicha Akjay, Laila Grihe, Houda Meyiz, Ihsane Mellouki
Gastroenterology Department university hospital, tangier, Morocco
Abstract
Staph aureus Colitis was discovered for the first time as a complication of antibiotic therapy with or without risk factors. However, he was recognized as the prinicipal agent of infectious colitis before its eclipse by the clostr in the 1970s. We report a rare case of mehicilline-resistant staph MRSA colitis in an adult with non-significant risk factors.
We report a rare case of a 42 years old patient with no pathological history. He consults for acute bloody diarrhea associated with abdominal pain evolving in a context of fever and deterioration of his general state. There was an infectious syndrome in clinical and biological assessment. The CT scan showed signs of non specific inflamation with presence of ulceration in endoscopic exploration without any severity signs.
The patient was treated empirically by dual antibiotic therapy.
The evolution was marked by a clear improvement of symptoms since the third day. The stool culture results came back positive of MRSA and a treatment with trimethoprim-sulfamethoxazole was initiated due to a vancomycin supply shortage.
The control was favorable with healing of clinical and endoscopic signs.
MRSA Endotoxin producing remains a significant etiology of infectious colitis, which must be systematically suspected in front of each bloody diarrhea especially in patients with risk factors.
Abstract ID: 53
Liquorice-induced pseudohyperaldosteronism: the importance of dietary intake in the differential diagnosis of hypokalaemia, a case report
Sophie Vanhoof
UZA, Antwerpen, Belgium
Abstract
Introduction: Hypokalaemia is a common electrolyte disorder and mild imbalances are frequently found in routine outpatient blood testing. However, severe potassium deficiency (<2,5 mmol/L) is rare and could provide a diagnostic challenge for clinicians. This report describes a case of hypokalaemia due to pseudohyperaldosteronism caused by the ingestion of liquorice, and demonstrates the importance of dietary intake assessment in hypokalaemia patients.
Case presentation: A 45-year-old female without a notable medical history was admitted to the hospital with severe hypokalaemia (2.3 mmol/L) on laboratory testing. Two years earlier, her serum potassium level was adequate (3.8 mmol/L). She denied diarrhea and her only complaint was fatigue. Save for oral contraceptives, she reported no use of medications. On examination, she appeared malnourished and had high blood pressures. Although dietary intake was not evaluated at the time of presentation, it was eventually discovered she consumed liquorice daily since childhood. Furthermore, she tested positive for COVID-19 and had low serum magnesium and phosphate levels as well. Urine potassium excretion was never measured. Intravenous potassium phosphate was administered in high doses, in addition to magnesium supplementation and spironolactone, with eventual correction of the hypokalaemia and resolution of hypertension. The patiënt was advised to refrain from further liquorice consumption.
Discussion: This case of hypokalaemia is thought to be induced by excessive liquorice ingestion, which can cause pseudohyperaldosteronism by inhibiting the conversion of cortisol to cortisone, thus increasing the cortisol levels which bind the mineralocorticoid receptor similarly to aldosterone, subsequently activating the renin-angiotensin-aldosterone system (RAAS) and causing features of mineralocorticoid excess, including hypokalaemia and hypertension.
This patient also presented with aggravating factors. First, a magnesium deficit, which is known to impair potassium reabsorption across the renal tubules. Therefore, magnesium should be replaced to facilitate potassium correction, especially in hypokalaemia refractory to supplementation, as was done here. Second, concomittant COVID-19 infection could have contributed to the severity of hypokalaemia in this patient, as COVID-19 is thought to downregulate ACE2 expression, consequentially increasing angiotensin II, which will augment the potassium excretion in the urine.
In conclusion, dietary preferences and nutritional status should be assessed in all patients presenting with hypokalaemia, as this could provide important clues for differential diagnosis and etiology of hypokalaemia. In this patient, electrolyte imbalances caused by malnutrition, and concomitant COVID-19 infection could explain why her liquorice consumption only now proved to be problematic after years of excessive intake.
Abstract ID: 54
Ethionamide and ethionamide sulfoxide pharmacokinetics in patients with drug resistant tuberculosis, preliminary results.
Fanya Laure Bouloua, Pierre Mugabob, Danie Theronc
aSchool of Pharmacy, University of the Western Cape, Cape Town, South Africa. bSchool of Pharmacy, University of the Western cape, Cape Town, South Africa. cBrewelskloof Hospital, Department of Health, Worcester, South Africa
Abstract
Background and objective: Ethionamide (ETH) is one of the medicines used for treatment of drug-resistant tuberculosis (DR-TB). Ethionamide sulfoxide (ETH-SO), one of ETH metabolites, is believed to be more active than the parent drug against Mycobacterium tuberculosis (MTB). Ethionamide and ETHSO pharmacokinetic parameters have been described in healthy volunteers. However, the pharmacokinetics of ETH-SO in patients with DR-TB with and without HIV co-infection is unknown. The aims of this study were to determine and compare ETH and ETH-SO pharmacokinetic parameters, to assess the effect of HIV-infection and antiretroviral medicines (ARVs) on ETH-SO pharmacokinetics, and to determine the amount of ETH-SO that emanates from ETH.
Methods: After informed and written consent, male and female DR-TB patients, 18–65 years old, with and without HIV-infection, at least 2 weeks after starting DR-TB were involved in the study. On the study day, after an 8-hour overnight fast, blood samples were collected in a heparinised tube via an intravenous catheter fixed on the forearm before (baseline) and 1, 2, 2.5, 3, 3.5, 4, 5, 8 and 24 hours after dosing. Ethionamide and ETH-SO plasma levels were quantified using LC-MS/MS. Pharmacokinetic parameters were determined using PKanalix 2019R1. The correlation and regression analysis between HIV infection, age, sex, weight, and creatinine clearance (CrCl) and the pharmacokinetics parameters were assessed. The amount of ETH-SO that emanated from ETH was calculated.
Results and discussion: Thirty-one patients, 32 (18–54) years old, 52.32 (27–54) kg body weight, 11 HIV-positive and 17 males participated in the study. The dose of all anti-TB drugs was determined according to the South African TB treatment guidelines. Each patient received ethambutol, kanamycin (29/31) or amikacin (2/31), ofloxacin (8/31) or moxifloxacin (23/31), pyrazinamide and terizidone. Seven male and 9 female patients received ethionamide 500 mg due to side effects associated with ethionamide 750 mg tablet. Ten male and five female patients were prescribed ethionamide 750 mg tablet. Isoniazid was added to the treatment in 20/31 patients who were rifampicin-mono-resistant. The following antiretroviral drugs were administered to HIV-positive patients: abacavir (4/11), stavudine (3/11), efavirenz (6/11) and lamivudine (7/11). Out of 31 patients, 26 had mild (Child-Pugh Class A) and 5/31 had moderate (Child-Pugh Class B) hepatic impairment. Twenty six patients had a normal renal function, 4 patients had mild renal impairment and one had a moderate renal failure. Ethionamide sulfoxide plasma levels were significantly higher than ETH concentrations. Ethionamide and ETH-SO pharmacokinetic parameters obtained are shown in the table below.
Table 1. Median (range) pharmacokinetics parameters of ethionamide and ethionamide sulfoxide.
Large variations were observed in the clearance (Cl) and volume of distribution (Vd) of ethionamide and ETH-SO. There was no significant correlation between age, sex, weight, CrCl and the pharmacokinetics of ETH-SO and ethionamide. A total of 472.63 (21.85–9715.78) mg, and 747.79 (598.61–1156.16) mg of ETH-SO, respectively, emanated from ETH 500 mg dose and 750 mg dose.
Discussion and conclusion: This study determined for the first time, the pharmacokinetic parameters of ETH-SO in DR-TB patients with and without HIV infection. The large ‘inter-subject variations’ observed in the clearance (Cl) and Vd of ethionamide and ETH-SO may be due to the genetic polymorphism underwent by the enzymes responsible for ETH metabolism, the flavin containing monooxygenases (FMOs) and to isoniazid co-administration which has been previously found to reduce ethionamide clearance and consequently increase its AUC.
The patients‘ median exposure to ETH – SO is about ±40 times higher than the exposure to ETH. However, their respective half-life and mean residence time are short. Further studies evaluating the impact of ETH-SO on ETH efficacy and safety in patients with DR-TB are recommended.
Acknowledgement:
(1) Patients involved in this study.
(2) South African Medical Research Council (SAMRC) and the University of the Western Cape for funding.
(3) The Department of Health (Province of Western Cape, South Africa) for granting permission to conduct the study.
Abstract ID: 55
Plummer Vinson syndrome: atypical clinical presentation. Do patients get used to their dysphagia?
Ihsane Eljaadi, Houda Meyiz, Aicha Akjay, Khaoula Attaqi, Ihsane Mellouki
Gastroenterology Department University Hospital, Tangier, Morocco
Abstract
Plummer Vinson syndrome (PVS) is a rare disease. Dysphagia remains his principal symptom. However, the clinical presentation is not always typical. We report three observations of SPV with unusual revelation, collected over 1 year.
It is about two young people aged 27 and 18 years old, who consulted for an endoscopic exploration of an iron deficiency anemia evolving in a context of deterioration of the general state and suspicion of celiac disease. However, the third case is about 60-year-old woman, who presented a chronic vomiting complicated by melena on a gastric adenoracinoma. Gastroscopy revealed the presence of upper esophageal webs in all the three cases. However, the review of the questioning objectified a notion of chronic dysphagia to which the patients are accustomed.
To our knowledge, a handful of cases have been reported in the literature of such association. Our three cases remain unusual by the mode of revelation and the progressive adaptation to dysphagia.
Abstract ID: 56
Ptosis and hyponatremia: a diagnosis not to miss
Remy Ponsa, Christophe De Terwangneb, Cédric Mahiatc
aStudent of the Catholic University of Louvain, Hopital universitaire Saint-Luc, Bruxelles, Belgium. bDepartment of geriatric medecine, Hopital universitaire Saint-Luc, Bruxelles, Belgium. cIntensive Care Unit, Hopital universitaire Saint-Luc, Bruxelles, Belgium
Abstract
Introduction:
Pituitary apoplexy (PA) is a rare but life-threatening condition. Sometimes, atypical clinical presentations can be misleading and delay the diagnosis.
Case report:
An 86-year-old women presented at our emergency department (ED) with asthenia, nausea, vomiting, diarrhea.
Ten days earlier, she presented at the ED of another hospital with complaints of right eye ptosis, headaches, myalgia and lower extremity edema. She was discharged with diagnosis of SARS-Cov-2 (positive PCR) and congestive heart failure and treated with diuretics.
She had a medical history of arterial hypertension, type II diabetes, chronic kidney failure and a history of benign non-functional pituitary macroadenoma that was surgically removed in 1994. To note, atrial fibrillation was recently discovered, and she was taking oral anticoagulant therapy. The physical examination showed right eye ptosis, unstable gait, and lower extremity edema.
Initial biology tests showed severe hypotonic hyponatremia (117 mmol/L, 238mOsm/kg) with decreased natriuresis (<10mmol, <9 mmol/24h, 183mOsml/kg). Brain CT scan was normal.
The patient was admitted in the geriatric ward for further management of supposed syndrome of inappropriate antidiuretic hormone secretion (SIADH). Evolution during the first days was unsatisfactory with persistent hyponatremia despite well conducted fluid restriction. Six days after her admission, she developed acute right ophthalmoplegia, right visual loss, areactive mydriasis, complete right ptosis and worsening of headaches. An urgent brain MRI led to the diagnosis of macroadenoma with intra-adenomal hemorrhage. Recent introduction of anticoagulation therapy could have precipitate adenomal hemorrhage.
Pituitary hormone function tests confirmed the diagnosis of PA. Urgent surgery was performed and the patient was discharged a few days later.
Discussion:
PA is a rare disease and most usually occurs due to sudden hemorrhage of non-functioning pituitary adenoma. This sudden hemorrhage causes an enlargement of the pituitary gland and subsequent pituitary stalk compression. This can lead to a large panel of symptoms (headaches, visual field impairment and decreased visual acuity) and biological findings (hypopituitarism and rarely acute cortisol deficiency).
Our case presented early signs of compressive macroadenoma i.e., palpebral claudication and biological findings of SIADH. The latter has been described in cases of pituitary insufficiency and PA but is rather an uncommon initial finding. This atypical presentation could therefore have delayed the diagnosis in our patient. Moreover, hyponatremia is a frequent disorder which is commonly associated to more frequent diseases or medications and PA is a rather rare condition. The initial cerebral CT-scan performed in the ED was also misleading as it described enlargement of the pituitary gland without signs of compression.
In conclusion, physicians should also think of PA in case of severe hyponatremia. MRI is the preferred technique for pituitary imaging.Citation1,Citation2,Citation3,Citation4,Citation5
References
- Capatina C, Inder W, Karavitaki N, Wass JA. Management of endocrine disease: pituitary tumour apoplexy. Eur J Endocrinol. 2015;172(5):R179–R190. doi:10.1530/EJE-14-0794
- Randeva HS, Schoebel J, Byrne J, Esiri M, Adams CB, Wass JA. Classical pituitary apoplexy: clinical features, management and outcome. Clin Endocrinol (Oxf). 1999;51(2):181–188. doi:10.1046/j.1365-2265.1999.00754.x
- Oelkers W. Hyponatremia and inappropriate secretion of vasopressin (antidiuretic hormone) in patients with hypopituitarism. N Engl J Med. 1989;321(8):492–496. doi:10.1056/NEJM198908243210802
- Vargas G, Gonzalez B, Guinto G, et al. Pituitary apoplexy in nonfunctioning pituitary macroadenomas: a case-control study. Endocr Pract. 2014;20(12):1274–1280. doi:10.4158/EP14120.OR
- Smedegaard SB, Jørgensen JO, Rittig N. Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) and Subsequent Central Diabetes Insipidus: A Rare Presentation of Pituitary Apoplexy. Case Rep Endocrinol. 2019;2019:7592648. Published 2019 Apr 2. doi:10.1155/2019/7592648
Abstract ID: 57
Migration of a Hot AXIOS™ Stent causing small bowel obstruction
Sven Van Laera,b, Louis Werpina,c, Arne Balleta,b, Steven Dockxa, Schalk Van der Merwed,c
aDepartment of Gastroenterology, Ziekenhuis Geel, Geel, Belgium. bFaculty of Medicine and Health Sciences, University of Antwerp, Antwerp, Belgium. cFaculty of Medicine, KU Leuven, Leuven, Belgium. dDepartment of Gastroenterology and Hepatology, University Hospitals Leuven, Leuven, Belgium
Abstract
Background: Lumen-apposing metal stents (LAMS), such as the Hot AXIOS™ Stent, are devices approved for endoscopic drainage of a pancreatic pseudocyst, the gallbladder in patients with acute cholecystitis, and the bile duct after failed endoscopic retrograde cholangiopancreatography (ERCP). Due to their success and safety, LAMS are increasingly used for off-label indications including gastrojejunostomy, gastro-gastrostomy and drainage of postsurgical collections. The complication rates for these indications are not well known. We present the case of a 68-year-old female patient with a small bowel obstruction caused by migration of LAMS after endoscopic gastro-gastrostomy with a Hot AXIOS™ Stent after Roux-en-Y gastric bypass.
Case presentation: A 68-year-old woman presented to the emergency department with severe abdominal pain and nausea. Her medical history included a Roux-en-Y gastric bypass and nonalcoholic steatohepatitis (NASH) liver cirrhosis treated with an orthotopic liver transplant, complicated by a transverse colon perforation with the need for extended right hemicolectomy with a terminal ileostomy. A few months back she underwent an endoscopic gastro-gastrostomy with a Hot AXIOS™ Stent for a later ERCP. The patient described periumbilical cramping, nausea and cessation of the passage of stool for 2 days. Physical examination revealed an elevated heart rate of 107/min, a blood pressure of 136/85 mmHg, dry mucous membranes, and abdominal distention. Blood tests showed an acute kidney injury and hypokalaemia. An abdominal X-ray showed dilated bowel loops with air-fluid levels, with a foreign object at the level of the right flank. An abdominal CT scan confirmed migration of the Hot AXIOS™ Stent to just before the stoma with the presence of faecal bowel sign. The patient underwent ileoscopy through the ileostomy, which confirmed the presence of a Hot AXIOS™ Stent near the end of the ileostomy. The Hot AXIOS™ Stent was rotated inside the bowel, with both ends facing the bowel wall, causing mechanical small bowel obstruction. The stent was endoscopically removed, followed by rapid clinical recovery.
Discussion: The use of LAMS in daily practice has increased significantly in recent years. The literature shows that there is a technical success rate of 98% and a clinical success rate of 95% for approved indications. These impressive findings are responsible for the increase in off-label indications, such as gastro-gastrostomy as in our case. Stent migration in approved indications is a known adverse event occurring in approximately 3–5% of patients. Migration to the bowel, however, is a very rare complication. Previously published case reports include the presentation of a patient with migration of a Hot AXIOS™ Stent, implanted to drain a pancreatic pseudocyst, into the colon. Spontaneous evacuation occurred and no endoscopic intervention was required. Another case report describes the migration of a LAMS into the colon with elective endoscopic removal without gastrointestinal obstruction.
Conclusion: To our knowledge, this is the first reported case of a migrating LAMS causing a gastrointestinal obstruction. Given the rapid increase in (off-label) indications for LAMS implantation, migration and subsequent possible obstruction should be considered in the differential diagnosis in patients with abdominal pain and a history of LAMS implantation.
Abstract ID: 58
Chilaïditi syndrome: the false pneumoperitoneum not to be ignored
Ihsane Eljaadi, Ibtissam Meriai, Ahmed Kalai, Morgan Andre
Hospital of Layné, Mont de Marsan, France
Abstract
The Chilaïditi syndrome is a set of clinical and radiological signs characterized by the interposition of the colon or the small intestine between the lower face of the diaphragm and the liver. It is a rare entity often fortuitously discovered.
We report the case of two patients admitted to the emergency room, the first 74 years old for exploration of acute epigastric pain with dyspnea in a covid positive context while the second 66 years old for an occlusive syndrome with a history of chronic constipation. The scannographic exploration finds colonic anses in the interhepatodiaphragmatic space making evoke a Chilaiditi syndrome
Chilaiditi syndrome represents the classic trap of false right pneumoperitoneum as it can mask a true pneumoperitoneum. The treatment is often conservative and surgery is reserved in case of complications
Abstract ID: 59
Primary rectal linitis: a rare entity of difficult diagnosis
Ihsane Eljaadi, Patrick Texereau, Morgan Andre
Hospital of Layné, Mont de Marsan, France
Abstract
Primary rectal linitis is a rare neoplasia with a poor prognosis. It is often associated with a gastric location. The management of the treatment is codified
We report the case of a 65-year-old patient who consulted for chronic diarrhea that was resistant to symptomatic treatment. A series of three endoscopic examinations always showed the same endoscopic appearance. The two biopsies always came back non-specific and it was only at the third biopsy that the diagnosis of an adenocarcinoma with ring pattern cells was made. The patient was put on chemotherapy.
Abstract ID: 60
Phenotypic and genotypic characterization of the population affected by Transthyretin amyloidosis at the ‘Erasme’ hospital and search for genotype-phenotype associations
Fromont Margaux, Vandergheynst Frédéric, Remiche Gauthier, Bondue Antoine
ULB (Erasme), Anderlecht, Belgium
Abstract
Introduction
Transthyretin (ATTR) amyloidosis is an infiltrating disease associated with the deposition of transthyretin (TTR) amyloid fibrils. It is subdivided into two entities according to the amino acid sequence of TTR. The finding of a pathogenic variant leads to the diagnosis of hereditary ATTR (hATTR) whereas the lack of such a variant corresponds to senile ATTR (wtATTR). Although systemic, ATTR preferentially affects the myocardium and peripheral nerves.
The main objective of this study is the genotypic characterization of hATTR subjects as well as the phenotypic characterization of ATTR patients and thereby, to explore the genotype-phenotype associations.
Methods
This is a monocentric descriptive retrospective study carried out at Erasmus Hospital on the demographic, clinical and genetic characteristics of hATTR and wtATTR subjects. The statistical methods used are essentially descriptive. Comparisons were also made using Fisher’s exact test or Wilcoxon’s test.
Results
A total of 22 wtATTR subjects and 26 hATTR subjects were included. The hATTR group was divided into 2 subgroups according to the variant found: ‘V50M’ (n = 14) and ‘non-V50M’ (n = 12).
The variants found are: ‘V50M’ (n = 14), ‘Thr80Ala’ (n = 3), ‘Lys90Asn’ (n = 1), ‘Val142del’ (n = 1), ‘Ile88Leu’ (n = 3), ‘Val142Ile’ (n = 3) and ‘Asp58His’ (n = 1).
100% of V50M patients have neurological involvement as the first clinical presentation.
80% of non-V50M subjects have cardiological involvement as the first clinical presentation.
At present, 100% of symptomatic ‘V50M’ patients present with neurological impairment (n = 7) and 42.9% with cardiomyopathy (n = 3). 80% of symptomatic ‘non-V50M’ patients present with cardiomyopathy (n = 8) and 80% with neurological involvement (n = 8).
Patients with cardiomyopathy are exclusively male.
The significant differences between the ‘V50M’ and ‘non-V50M’ subgroups relate to gender (p = 0.014), first clinical presentation (neurological versus cardiological) (p = 0.002) and age of onset (p = 0.02). The ‘non-V50M’ subgroup presents for the majority a cardiomyopathy as first clinical presentation and is composed mainly of men. Conversely, the ‘V50M’ subgroup all have neurological involvement as the first clinical presentation and an equivalent gender distribution.
The wtATTR group is composed of 68% men (n = 15) and 32% women (n = 7). Among those referred to a neurologist, all had a distal sensory-motor polyneuropathy (n = 9).
Conclusion
The genotypic distribution of hATTR subjects is very heterogeneous and mainly includes the ‘V50M’ variant. Our results highlight the presence of an association between genotype and phenotype regarding the first neurological versus cardiological clinical presentation, age of onset and gender.
Our wtATTR group includes more women than in previous series.